Abstract
Eosinophilic esophagitis (EE) is a chronic, immune-mediated or antigen-mediated esophageal disease. Treatment for patients with EE can be challenging with no previously approved medications. Current management strategies follow the four D’s paradigm of drugs, dietary elimination, dilation, and disease anxiety and hypervigilance therapy. On 20 May 2022, dupilumab was approved by FDA for EE. A dose of 300 mg dupilumab weekly significantly improved signs and symptoms of EE compared to placebo in a phase 3 trial. The approval of dupilumab will fulfill an unmet need for the increasing number of patients with EE.
1. Introduction
1.1. Definition and Symptoms
Eosinophilic esophagitis (EE) is a chronic, immune-mediated or antigen-mediated esophageal disease. In EE, large numbers of eosinophils are found in the inner lining of the esophagus [1,2]. The chronic inflammation of EE leads to several symptoms. EE is characterized by symptoms relevant to eosinophil-predominant inflammation and esophageal dysfunction. The prevailing antigens that trigger EE seem to be food related. Other causes of EE include allergic vasculitis, parasitic infection, esophageal leiomyomatosis, and Crohn’s disease of the esophagus [3]. Symptoms of EE include vomiting, feeding problems, and dysphagia and food impaction in adults and adolescents and abdominal pain in children. Present also is esophageal mucosal eosinophilia of ≥15 eosinophils per high-power field [1,2].
1.2. Pathogenesis
Premature delivery, birth by caesarean, lack of breast-feeding, antibiotic exposure during infancy, food allergy, and living in low population density areas have all been associated with EE. Studies have also indicated that the absence of early exposure to microbes or the altered microbiome in vulnerable patients may play a role [4,5,6]. The male predominance of EE and studies of genome-wide association and family history indicate that there is a genetic component to EE. In fact, three genes encoding thymic stromal lymphopoietin, eotaxin-3, and calpain-14 are altered in EE [7,8,9,10,11,12]. Furthermore, dilated interepithelial spaces, altered function of epithelial barrier, and down-regulation of filaggrin, zonulin-1, and desmoglein-1 have been found upon assessing esophageal tissue of EE patients. Altered epithelial permeability leads to an uncontrolled environment, enhances antigen presentation, and results in recruitment of eosinophils [13,14,15,16,17].
Several lines of evidence also suggest that EE can be mediated by type 2 helper T (Th2) cell activity and promoted largely by food antigens [3]. Specifically, interleukin-5 and interleukin-13 may play a role in the pathogenesis of EE [18]. There are also thymic stromal lymphopoietin-directed and cytokine-directed proliferation and recruitment of eosinophils, IgE-bearing mast cells, Th2 lymphocytes, natural killer cells, and basophils in EE patients [19,20,21,22]. Interestingly, food-specific IgG4 was shown to be present in the esophageal epithelium and to be reactive to the four most common food-antigen triggers in EE patients [23].
1.3. Prevalence
EE has been described in all age groups. Nevertheless, it mainly impacts white men with an onset from school age to midlife [24]. A history of atopic disorders, such as eczema, rhinitis, asthma, and anaphylactic food allergy is widespread among patients predisposed to EE [25]. Patients undergoing endoscopy owing to food impaction history have a significantly higher incidence of up to 54% [26]. Studies have estimated the prevalence of EE as 1–5 per 10,000 people in the western hemisphere, with increased prevalence in Asia [27,28,29,30].
1.4. Complications
EE is a long-lasting inflammatory condition with a persistent course of instability. Life expectancy does not appear to be affected, but EE often affects the life quality. Furthermore, there appear no association between EE and esophageal cancer; nevertheless, there are serious concerns that the uncontrolled, prolonged inflammation may lead to irreversible structural changes resulting in stricture formation, tissue fibrosis, and impairment of the esophageal function. Other complications of EE include esophageal perforation, food impaction, malnutrition, hepatic portal venous gas, achalasia-like changes, and adrenal insufficiency. Concurrent conditions that have been associated with patients with EE include connective tissue diseases [31], Crohn’s disease [32], and celiac disease [33].
1.5. Current Treatment Strategies
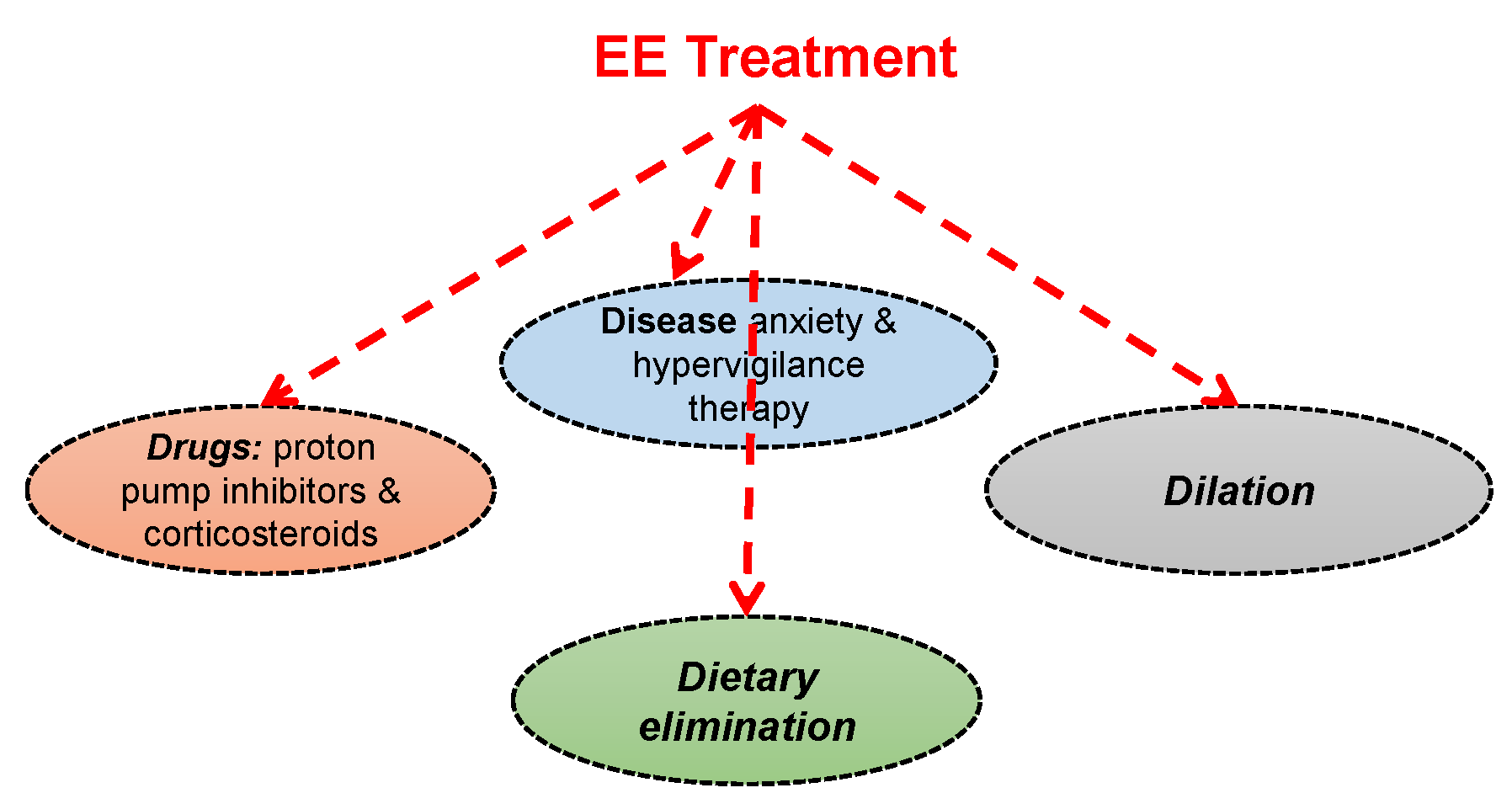
Some adults and many children with EE show improvement with proton pump inhibitors [34,35,36] as well as diet modification so that the food that triggers allergy is removed, particularly egg, milk, wheat, soy, nuts, and fish [37,38]. Some patients require a liquid formula diet provided via a feeding tube. Steroid medications can be used to control inflammation [39,40]. Esophageal dilation to relieve esophageal narrowing is also an established strategy for EE, especially in older adults and teenagers [41]. Generally, the current paradigm of EE treatment is depicted in Figure 1. The paradigm revolves around the four Ds concept of drugs (proton pump inhibitors or corticosteroids), dietary elimination, dilation, and disease anxiety and hypervigilance therapy.
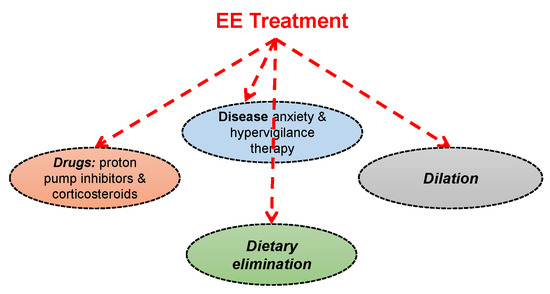
Figure 1.
The current paradigm of EE treatment. The treatment follows the 4 Ds concept.
2. Dupilumab (Dupixent®, Regeneron)
The drug was jointly developed by Sanofi Genzyme and Regeneron Pharmaceuticals. Dupilumab has an approximate molecular weight of 147 kDa. Dupilumab is produced by recombinant DNA technology in Chinese Hamster Ovary cell suspension culture. Dupilumab is a human monoclonal IgG4 antibody that inhibits both interleukin-13 (IL-13) and interleukin-4 (IL-4) signaling by binding to the IL-4Rα subunit. Such binding inhibits IL-13 and IL-4 cytokine-induced inflammatory responses, including the release of proinflammatory cytokines, chemokines, immunoglobulin E, and nitric oxide [42,43]. It was previously approved for moderate to severe eosinophilic or oral glucocorticoid-dependent asthma, moderate to severe atopic dermatitis, and chronic rhinosinusitis with nasal polyposis [44].
Following subcutaneous administration, its bioavailability is 61% to 64%. Its time to peak is ~1 week. Its Vd is ~4.8 ± 1.3 L. Monoclonal antibodies are primarily cleaved to short peptides and individual amino acids by catabolism. The median times to reach nondetectable levels are 10 to 11 weeks (for 300 mg every 2 weeks), 13 weeks (for 300 mg weekly), and 9 weeks (for 200 mg every 2 weeks) [45,46].
On 20 May 2022, the indication for dupilumab was expanded to include treating EE in people aged 12 years or older and weighing at least 40 kg. The efficacy and safety of dupilumab in EE was exhibited in a randomized, double-blind, parallel-group, multicenter, placebo-controlled trial that included two 24-week treatment periods (Parts A and B, phase 3, n = 321) that were independently conducted in separate groups of patients. In both Parts A and B, patients received 300 mg dupilumab or placebo every week. The primary outcome measures were the proportion of patients achieving peak esophageal intraepithelial eosinophil count of ≤6 eosinophils per high-power field at week 24 and the absolute change in Dysphagia Symptom Questionnaire (DSQ) score. In Part A, 60% of the patients who received dupilumab achieved the pre-determined level of decrease of eosinophils in the esophagus in relative to only 5% of those in the placebo group. Patients who received dupilumab also had an average improvement of 22 points in the DSQ score relative to only 10 points for patients in the placebo group. In Part B, 59% of patients who were treated with dupilumab attained the pre-determined level of decrease of eosinophils in the esophagus relative to 6% of those in the placebo group. Overall, in this phase 3 trial, dupilumab 300 mg weekly substantially alleviated signs and symptoms of EE compared to placebo [47].
There are no dosage adjustments provided in the manufacturer’s labeling for patients with altered kidney or liver functions. Dupilumab can cause allergic reactions, keratitis, and conjunctivitis because of its immunosuppressive effects. It can also reactivate cold sores. Patients who had been treated with dupilumab had decreased levels of T helper cells [42,43,44]. No animal studies have been performed to evaluate the mutagenic or carcinogenic potential of dupilumab. No effects on fertility parameters such as menstrual cycle length, reproductive organs, or sperm analysis were detected in sexually mature mice that were injected with a homologous antibody against IL-4Rα at doses up to 200 mg/kg/week.
3. Discussion of the Study
The FDA approval was based on results of a phase 3 trial with two parts evaluating the efficacy and safety of Dupixent 300 mg weekly compared with placebo. A single randomized, double-blind, multicenter, parallel-group, placebo-controlled trial, including two 24-week treatment periods (Parts A and B), was conducted in adult and pediatric subjects 12 to 17 years of age, weighing at least 40 kg, with EE (NCT03633617). In the two parts, subjects were randomized to receive 300 mg dupilumab every week or placebo. Eligible subjects had ≥15 intraepithelial eosinophils per high-power field following a treatment course of a proton pump inhibitor either prior to or during the screening period and symptoms of dysphagia as measured by the DSQ. At baseline, 43% of subjects in Part A and 37% of subjects in Part B had a history of prior esophageal dilations.
Baseline characteristics and demographics were similar in the two parts. A total of n = 81 subjects (61 adults and 20 pediatric subjects) were enrolled in Part A and n = 159 subjects (107 adults and 52 pediatric subjects) were enrolled in Part B. The mean age in years was 32 years (range of 13–62 years) in Part A and 28 years (range of 12–66 years) in Part B. Most of subjects were male (60% in Part A and 68% in Part B) and white (96% in Part A and 90% in Part B). The mean baseline DSQ score (standard deviation) was 33.6 (12.4) in Part A and 37.2 (10.7) in Part B.
As mentioned above, the primary efficacy endpoints were the proportion of subjects achieving histological remission defined as peak esophageal intraepithelial eosinophil count of ≤6 eosinophils per high-power field at week 24 and the absolute change in the subject-reported DSQ score from baseline to week 24. Efficacy results are reported in Table 1 [48].

Table 1.
Efficacy results of dupilumab at week 24 in subjects 12 years of age and older with EE.
In the two parts, a larger proportion of participants randomized to dupilumab achieved histological remission compared to placebo. At week 24, treatment with the drug also led to a significant improvement in LS mean change in DSQ score compared to placebo. The results of the anchor-based analyses that incorporated the participants’ perspectives suggested that the observed improvement in dysphagia from the two parts is representative of a clinically meaningful within-subject improvement.
In the above trial, the proportion of participants who discontinued treatment due to adverse events was 2% of the placebo group and 2% of the dupilumab 300 mg QW group.
Table 2 summarizes the adverse reactions that occurred at a rate of at least 2% in participants treated with dupilumab and at a higher rate than in their respective comparator group in the two parts.
Table 2.
Adverse reactions occurring in ≥2% of patients with EE treated with dupilumab in a placebo-controlled trial (Parts A and B; 24-week safety pool).
Generally speaking, the safety profile of dupilumab in 72 pediatric subjects 12 to 17 years of age, weighing at least 40 kg, and adults in Parts A and B was similar.
It is important to mention here that a phase 2 trial of adults with active EE (two episodes of dysphagia per week with peak esophageal eosinophil density of ≥15 eosinophils per high-power field) was conducted earlier from 12 May 2015 through 9 November 2016, at multiple sites (NCT02379052) [49]. For 12 weeks, the adults were randomly assigned to two groups: the first group was the patients who received weekly subcutaneous injections of dupilumab (300 mg, n = 23) and the second group was the placebo group (n = 24). The primary endpoint was changed from baseline to week 10 in Straumann Dysphagia Instrument patient-reported outcome score. At the conclusion of the study, it was found that dupilumab significantly decreased dysphagia, histologic features of disease (including eosinophilic infiltration and a marker of type 2 inflammation), and abnormal endoscopic features compared with placebo. Dupilumab also significantly increased esophageal distensibility and was generally well-tolerated [49].
4. Conclusions
There are about 160,000 patients in the US living with EE who are currently using therapeutics not necessarily approved for the disease. Among them, about 48,000 continue to experience EE symptoms regardless of several treatments. The FDA granted dupilumab priority review and breakthrough therapy designations for EE, and on 20 May 2022 it was approved by the FDA for EE. Treatment for patients with EE can be challenging with no previously approved medications. Patients now have a treatment available to control their symptoms, improve inflammation, and heal the changes in the esophagus. Importantly, the approval of this drug for EE underscores the role of type 2 inflammation in this disease [47,49,50]. The recommended dosage of dupilumab for adult and pediatric patients 12 years of age and older, weighing at least 40 kg, is 300 mg given every week (QW).
Author Contributions
R.C. and R.A.A.-H.; writing—original draft preparation, R.C. and R.A.A.-H.; writing—review and editing, R.A.A.-H.: funding. All authors have read and agreed to the published version of the manuscript.
Funding
R.A.A.H. is supported by NIGMS of the National Institute of Health under award number SC3GM131986 to R.A.A.H. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding institutions.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Provided in the manuscript.
Conflicts of Interest
The authors declare no conflict of interest with the work being reported here. The authors have no conflict of interest about Dupixent®, Regeneron.
References
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 2011, 128, 3–20.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellon, E.S.; Gonsalves, N.; Hirano, I.; Furuta, G.T.; Liacouras, C.A.; Katzka, D.A. ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of Esophageal Eosinophilia and Eosinophilic Esophagitis (EoE). Am. J. Gastroenterol. 2013, 108, 679–692. [Google Scholar] [CrossRef] [PubMed]
- Furuta, G.T.; Katzka, D.A. Eosinophilic Esophagitis. N. Engl. J. Med. 2015, 373, 1640–1648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, E.T.; Hoffman, K.; Shaheen, N.J.; Genta, R.M.; Dellon, E.S. Esophageal Eosinophilia is Increased in Rural Areas With Low Population Density: Results From a National Pathology Database. Am. J. Gastroenterol. 2014, 109, 668–675. [Google Scholar] [CrossRef] [Green Version]
- Jensen, E.T.; Kappelman, M.D.; Kim, H.P.; Ringel-Kulka, T.; Dellon, E.S. Early Life Exposures as Risk Factors for Pediatric Eosinophilic Esophagitis. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 67–71. [Google Scholar] [CrossRef] [Green Version]
- van Nimwegen, F.A.; Penders, J.; Stobberingh, E.E.; Postma, D.S.; Koppelman, G.H.; Kerkhof, M.; Reijmerink, N.E.; Dompeling, E.; van den Brandt, P.A.; Ferreira, I.; et al. Mode and place of delivery, gastrointestinal microbiota, and their influence on asthma and atopy. J. Allergy Clin. Immunol. 2011, 128, 948.e3–955.e3. [Google Scholar] [CrossRef]
- Kapel, R.C.; Miller, J.K.; Torres, C.; Aksoy, S.; Lash, R.; Katzka, D.A. Eosinophilic Esophagitis: A Prevalent Disease in the United States That Affects All Age Groups. Gastroenterology 2008, 134, 1316–1321. [Google Scholar] [CrossRef] [Green Version]
- Alexander, E.S.; Martin, L.J.; Collins, M.H.; Kottyan, L.C.; Sucharew, H.; He, H.; Mukkada, V.A.; Succop, P.A.; Abonia, J.P.; Foote, H.; et al. Twin and family studies reveal strong environmental and weaker genetic cues explaining heritability of eosinophilic esophagitis. J. Allergy Clin. Immunol. 2014, 134, 1084–1092.e1. [Google Scholar] [CrossRef] [Green Version]
- Sherrill, J.D.; Gao, P.-S.; Stucke, E.M.; Blanchard, C.; Collins, M.H.; Putnam, P.E.; Franciosi, J.P.; Kushner, J.P.; Abonia, J.P.; Assa’Ad, A.H.; et al. Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. J. Allergy Clin. Immunol. 2010, 126, 160–165.e3. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, C.; Wang, N.; Stringer, K.F.; Mishra, A.; Fulkerson, P.C.; Abonia, J.; Jameson, S.C.; Kirby, C.; Konikoff, M.R.; Collins, M.H.; et al. Eotaxin-3 and a uniquely conserved gene-expression profile in eosinophilic esophagitis. J. Clin. Investig. 2006, 116, 536–547. [Google Scholar] [CrossRef] [Green Version]
- Kottyan, L.C.; Davis, B.P.; Sherrill, J.D.; Liu, K.; Rochman, M.; Kaufman, K.; Weirauch, M.T.; Vaughn, S.; Lazaro, S.; Rupert, A.M.; et al. Genome-wide association analysis of eosinophilic esophagitis provides insight into the tissue specificity of this allergic disease. Nat. Genet. 2014, 46, 895–900. [Google Scholar] [CrossRef] [Green Version]
- Sleiman, P.M.A.; Wang, M.-L.; Cianferoni, A.; Aceves, S.; Gonsalves, N.; Nadeau, K.; Bredenoord, A.J.; Furuta, G.T.; Spergel, J.M.; Hakonarson, H. GWAS identifies four novel eosinophilic esophagitis loci. Nat. Commun. 2014, 5, 5593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzka, D.A.; Tadi, R.; Smyrk, T.C.; Katarya, E.; Sharma, A.; Geno, D.M.; Camilleri, M.; Iyer, P.G.; Alexander, J.A.; Buttar, N.S. Effects of Topical Steroids on Tight Junction Proteins and Spongiosis in Esophageal Epithelia of Patients With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 2014, 12, 1824–1829.e1. [Google Scholar] [CrossRef] [PubMed]
- Katzka, D.A.; Ravi, K.; Geno, D.M.; Smyrk, T.C.; Iyer, P.G.; Alexander, J.A.; Mabary, J.E.; Camilleri, M.; Vaezi, M.F. Endoscopic Mucosal Impedance Measurements Correlate With Eosinophilia and Dilation of Intercellular Spaces in Patients With Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 2015, 13, 1242–1248.e1. [Google Scholar] [CrossRef] [PubMed]
- van Rhijn, B.D.; Weijenborg, P.W.; Verheij, J.; van den Bergh Weerman, M.A.; Verseijden, C.; van den Wijngaard, R.M.; de Jonge, W.J.; Smout, A.J.; Bredenoord, A.J. Proton pump inhibitors partially restore mucosal integrity in patients with proton pump inhibitor-responsive esophageal eosinophilia but not eosinophilic esophagitis. Clin. Gastroenterol. Hepatol. 2014, 12, 1815.e2–1823.e2. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, C.; Stucke, E.M.; Burwinkel, K.; Caldwell, J.M.; Collins, M.H.; Ahrens, A.; Buckmeier, B.K.; Jameson, S.C.; Greenberg, A.; Kaul, A.; et al. Coordinate Interaction between IL-13 and Epithelial Differentiation Cluster Genes in Eosinophilic Esophagitis. J. Immunol. 2010, 184, 4033–4041. [Google Scholar] [CrossRef] [PubMed]
- Sherrill, J.D.; Kc, K.; Wu, D.; Djukic, Z.; Caldwell, J.M.; Stucke, E.M.; Kemme, K.A.; Costello, M.; Mingler, M.K.; Blanchard, C.R.; et al. Desmoglein-1 regulates esophageal epithelial barrier function and immune responses in eosinophilic esophagitis. Mucosal Immunol. 2013, 7, 718–729. [Google Scholar] [CrossRef] [PubMed]
- Kc, K.; Rothenberg, M.E.; Sherrill, J.D. In vitro model for studying esophageal epithelial differentiation and allergic inflammatory responses identifies keratin involvement in eosinophilic esophagitis. PLoS ONE 2015, 10, e0127755. [Google Scholar] [CrossRef] [PubMed]
- Mulder, D.J.; Mak, N.; Hurlbut, D.J.; Justinich, C.J. Atopic and non-atopic eosinophilic oesophagitis are distinguished by immunoglobulin E-bearing intraepithelial mast cells. Histopathology 2012, 61, 810–822. [Google Scholar] [CrossRef]
- Straumann, A.; Bauer, M.; Fischer, B.; Blaser, K.; Simon, H.U. Idiopathic eosinophilic esophagitis is associated with a T(H)2-type allergic inflammatory response. J. Allergy Clin. Immunol. 2001, 108, 954–961. [Google Scholar] [CrossRef]
- Noti, M.; Wojno, E.T.; Kim, B.S.; Siracusa, M.C.; Giacomin, P.; Nair, M.; Benitez, A.J.; Ruymann, K.R.; Muir, A.B.; Hill, D.; et al. Thymic stromal lymphopoietin–elicited basophil responses promote eosinophilic esophagitis. Nat. Med. 2013, 19, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Lexmond, W.S.; Neves, J.F.; Nurko, S.; Olszak, T.; Exley, M.A.; Blumberg, R.S.; Fiebiger, E. Involvement of the iNKT Cell Pathway Is Associated With Early-Onset Eosinophilic Esophagitis and Response to Allergen Avoidance Therapy. Am. J. Gastroenterol. 2014, 109, 646–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayton, F.; Fang, J.C.; Gleich, G.J.; Lucendo, A.J.; Olalla, J.M.; Vinson, L.A.; Lowichik, A.; Chen, X.; Emerson, L.; Cox, K.; et al. Eosinophilic Esophagitis in Adults Is Associated With IgG4 and Not Mediated by IgE. Gastroenterology 2014, 147, 602–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellon, E.S.; Jensen, E.T.; Martin, C.F.; Shaheen, N.J.; Kappelman, M.D. Prevalence of Eosinophilic Esophagitis in the United States. Clin. Gastroenterol. Hepatol. 2014, 12, 589–596.e1. [Google Scholar] [CrossRef] [Green Version]
- Aceves, S.S. Food Allergy Testing in Eosinophilic Esophagitis: What the Gastroenterologist Needs to Know. Clin. Gastroenterol. Hepatol. 2013, 12, 1216–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Desai, T.K.; Stecevic, V.; Chang, C.-H.; Goldstein, N.S.; Badizadegan, K.; Furuta, G.T. Association of eosinophilic inflammation with esophageal food impaction in adults. Gastrointest. Endosc. 2005, 61, 795–801. [Google Scholar] [CrossRef]
- Hruz, P.; Straumann, A.; Bussmann, C.; Heer, P.; Simon, H.-U.; Zwahlen, M.; Beglinger, C.; Schoepfer, A.M.; Swiss EoE Study Group. Escalating incidence of eosinophilic esophagitis: A 20-year prospective, population-based study in Olten County, Switzerland. J. Allergy Clin. Immunol. 2011, 128, 1349–1350.e5. [Google Scholar] [CrossRef]
- Ronkainen, J.; Talley, N.J.; Aro, P.; Storskrubb, T.; Johansson, S.-E.; Lind, T.; Bolling-Sternevald, E.; Vieth, M.; Stolte, M.; Walker, M.M.; et al. Prevalence of oesophageal eosinophils and eosinophilic oesophagitis in adults: The population-based Kalixanda study. Gut 2007, 56, 615–620. [Google Scholar] [CrossRef] [Green Version]
- Mansoor, E.; Cooper, G.S. The 2010–2015 Prevalence of Eosinophilic Esophagitis in the USA: A Population-Based Study. Dig Dis Sci. 2016, 61, 2928–2934. [Google Scholar] [CrossRef] [Green Version]
- Ishimura, N.; Shimura, S.; Jiao, D.; Mikami, H.; Okimoto, E.; Uno, G.; Aimi, M.; Oshima, N.; Ishihara, S.; Kinoshita, Y. Clinical features of eosinophilic esophagitis: Differences between Asian and Western populations. J. Gastroenterol. Hepatol. 2015, 30, 71–77. [Google Scholar] [CrossRef]
- Abonia, J.P.; Wen, T.; Stucke, E.M.; Grotjan, T.; Griffith, M.S.; Kemme, K.A.; Collins, M.H.; Putnam, P.E.; Franciosi, J.P.; von Tiehl, K.F.; et al. High prevalence of eosinophilic esophagitis in patients with inherited connective tissue disorders. J. Allergy Clin. Immunol. 2013, 132, 378–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulder, D.J.; Hookey, L.C.; Hurlbut, D.J.; Justinich, C.J. Impact of Crohn disease on eosinophilic esophagitis: Evidence for an altered T(H)1-T(H)2 immune response. J. Pediatr. Gastroenterol. Nutr. 2011, 53, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Jensen, E.; Lebwohl, B.; Genta, R.; Dellon, E. Increased Risk of Eosinophilic Esophagitis in Patients With Active Celiac Disease on Biopsy: Results From a National Pathology Database. Am. J. Gastroenterol. 2014, 109, S21. [Google Scholar] [CrossRef]
- Cheng, E.; Zhang, X.; Huo, X.; Yu, C.; Zhang, Q.; Wang, D.H.; Spechler, S.J.; Souza, R.F. Omeprazole blocks eotaxin-3 expression by oesophageal squamous cells from patients with eosinophilic oesophagitis and GORD. Gut 2013, 62, 824–832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thakkar, K.P.; Fowler, M.; Keene, S.; Iuga, A.; Dellon, E.S. Long-term efficacy of proton pump inhibitors as a treatment modality for eosinophilic esophagitis. Dig. Liver Dis. 2022, in press. [Google Scholar] [CrossRef] [PubMed]
- Wen, T.; Dellon, E.S.; Moawad, F.J.; Furuta, G.T.; Aceves, S.S.; Rothenberg, M.E. Transcriptome analysis of proton pump inhibitor–responsive esophageal eosinophilia reveals proton pump inhibitor–reversible allergic inflammation. J. Allergy Clin. Immunol. 2014, 135, 187–197.e4. [Google Scholar] [CrossRef] [Green Version]
- Votto, M.; De Filippo, M.; Lenti, M.V.; Rossi, C.M.; Di Sabatino, A.; Marseglia, G.L.; Licari, A. Diet Therapy in Eosinophilic Esophagitis. Focus on a Personalized Approach. Front. Pediatr. 2022, 9, 820192. [Google Scholar] [CrossRef]
- Arias, Á.; González-Cervera, J.; Tenias, J.M.; Lucendo, A.J. Efficacy of Dietary Interventions for Inducing Histologic Remission in Patients With Eosinophilic Esophagitis: A Systematic Review and Meta-analysis. Gastroenterology 2014, 146, 1639–1648. [Google Scholar] [CrossRef] [PubMed]
- Główczewski, A.; Krogulska, A. Formulations of Topical Steroids in Eosinophilic Esophagitis—Current Treatment and Emerging Possibilities. J. Clin. Med. 2022, 11, 1454. [Google Scholar] [CrossRef]
- Dellon, E.S.; Lucendo, A.J.; Schlag, C.; Schoepfer, A.M.; Falk, G.W.; Eagle, G.; Nezamis, J.; Comer, G.M.; Knoop, K.; Hirano, I. Fluticasone Propionate Orally Disintegrating Tablet (APT-1011) for Eosinophilic Esophagitis: Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2022, in press. [Google Scholar] [CrossRef]
- Muir, A.; Falk, G.W. Eosinophilic Esophagitis: A Review. JAMA 2021, 326, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Shirley, M. Dupilumab: First Global Approval. Drugs 2017, 77, 1115–1121. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves New Eczema Drug Dupixent. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-new-eczema-drug-dupixent (accessed on 21 May 2022).
- Highlights of Prescribing Informat. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/761055s014lbl.pdf (accessed on 21 May 2022).
- Li, Z.; Radin, A.; Li, M.; Hamilton, J.D.; Kajiwara, M.; Davis, J.D.; Takahashi, Y.; Hasegawa, S.; Ming, J.E.; DiCioccio, A.T.; et al. Pharmacokinetics, Pharmacodynamics, Safety, and Tolerability of Dupilumab in Healthy Adult Subjects. Clin. Pharmacol. Drug Dev. 2020, 9, 742–755. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Gao, Y.; Li, M.; Xu, C.; Davis, J.D.; Kanamaluru, V.; Lu, Q. Population pharmacokinetic analysis of dupilumab in adult and adolescent patients with asthma. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 941–952. [Google Scholar] [CrossRef]
- FDA Approves First Treatment for Eosinophilic Esophagitis, a Chronic Immune Disorder. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-eosinophilic-esophagitis-chronic-immune-disorder (accessed on 21 May 2022).
- Highlights of Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/761055s042lbl.pdf (accessed on 29 June 2022).
- Hirano, I.; Dellon, E.S.; Hamilton, J.D.; Collins, M.H.; Peterson, K.; Chehade, M.; Schoepfer, A.M.; Safroneeva, E.; Rothenberg, M.E.; Falk, G.W.; et al. Efficacy of Dupilumab in a Phase 2 Randomized Trial of Adults With Active Eosinophilic Esophagitis. Gastroenterology 2020, 158, 111–122.e10. [Google Scholar] [CrossRef] [Green Version]
- Press Release: FDA Approves Dupixent® (dupilumab) as First Treatment for Adults and Children Aged 12 and Older with Eosinophilic Esophagitis. Available online: https://www.sanofi.com/en/media-room/press-releases/2022/2022-05-20-21-15-00-2447906 (accessed on 21 May 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).