
Phantosmia in Parkinson’s Disease: A Systematic Review of the Phenomenology of Olfactory Hallucinations

 ,
,  ,
,  ,
,  , and
, and
Abstract
:1. Introduction
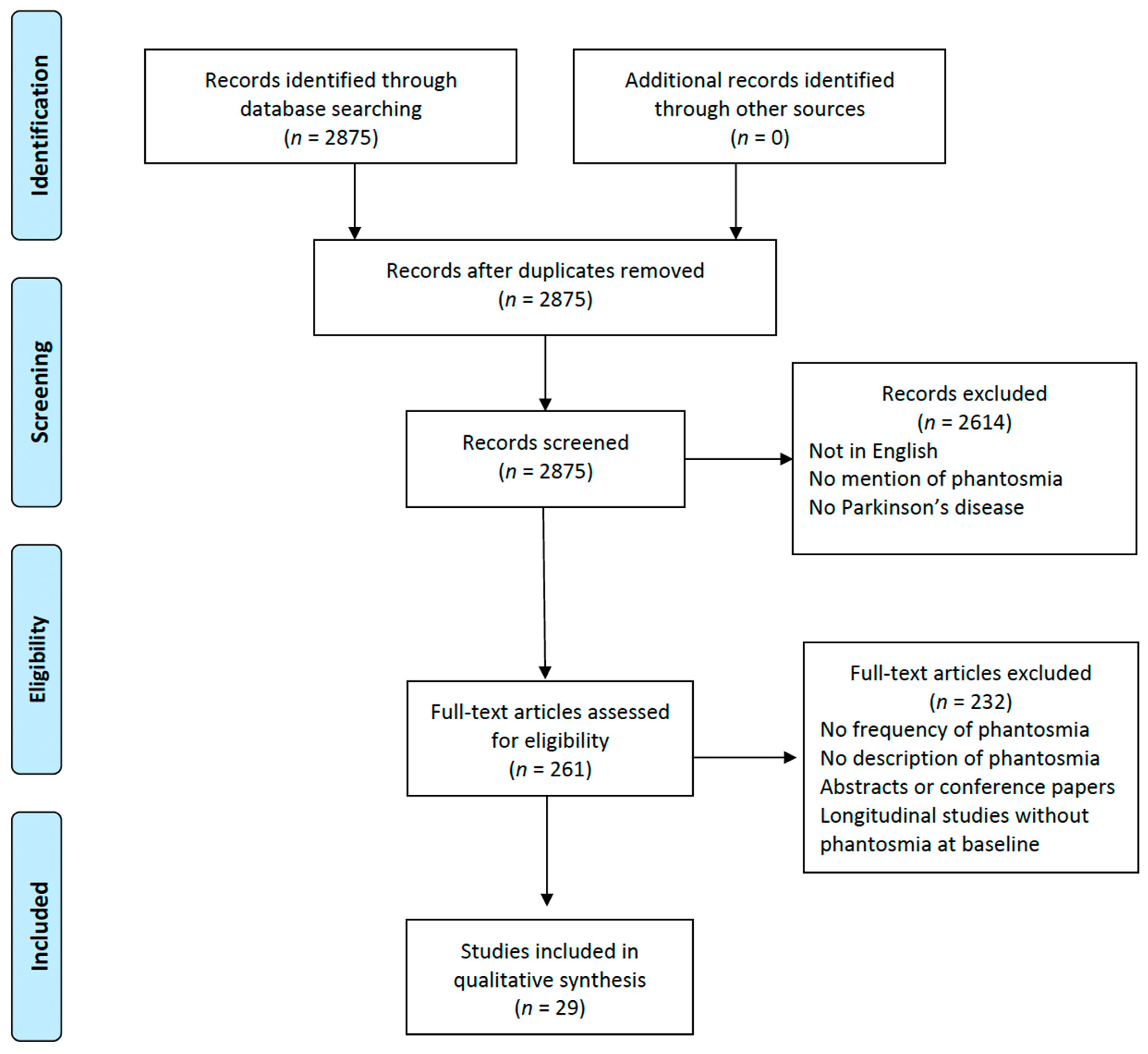
2. Methods
3. Results
3.1. Frequency of OHs and Gender Distribution
3.2. OHs Features (Pleasant vs. Unpleasant)
3.3. Assessment of OHs
3.4. Quantitative Evaluation of Olfactory Function
3.5. Associated Hallucinations
3.6. Impact on Quality of Life
3.7. Treatment of OHs
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| eSAPS-PD | Enhanced Scale for Assessment of Positive Symptoms in Parkinson’s Disease |
| NMSs | non-motor symptoms |
| NMFs | non-motor fluctuations |
| NPI | Neuropsychiatric Inventory |
| OHs | olfactory hallucinations |
| PD | Parkinson’s disease |
| PSAS | Psycho-Sensory hAllucinations Scale |
| PsycH-Q | Psychosis and Hallucinations Questionnaire |
| RBD | rapid eye movement sleep behavior disorder |
| SAPS | Schedule for Assessment of Positive Symptoms |
| TDI | threshold–discrimination–identification |
| UM-PDHQ | University of Miami Parkinson’s disease Hallucinations Questionnaire |
| UPSIT | University of Pennsylvania Smell Identification Test |
References
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease. JAMA 2020, 323, 548. [Google Scholar] [CrossRef]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s Disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abbasi, N.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; et al. Global, Regional, and National Burden of Parkinson’s Disease, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- de Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s Disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef]
- Belvisi, D.; Pellicciari, R.; Fabbrini, A.; Costanzo, M.; Pietracupa, S.; De Lucia, M.; Modugno, N.; Magrinelli, F.; Dallocchio, C.; Ercoli, T.; et al. Risk Factors of Parkinson Disease: Simultaneous Assessment, Interactions, and Etiologic Subtypes. Neurology 2020, 95, e2500–e2508. [Google Scholar] [CrossRef]
- Schapira, A.H.V.; Chaudhuri, K.R.; Jenner, P. Non-Motor Features of Parkinson Disease. Nat. Rev. Neurosci. 2017, 18, 435–450. [Google Scholar] [CrossRef]
- Belvisi, D.; Pellicciari, R.; Fabbrini, A.; Costanzo, M.; Ressa, G.; Pietracupa, S.; De Lucia, M.; Modugno, N.; Magrinelli, F.; Dallocchio, C.; et al. Relationship between Risk and Protective Factors and Clinical Features of Parkinson’s Disease. Park. Relat. Disord. 2022, 98, 80–85. [Google Scholar] [CrossRef]
- Boesveldt, S.; Verbaan, D.; Knol, D.L.; Visser, M.; Van Rooden, S.M.; Van Hilten, J.J.; Berendse, H.W. A Comparative Study of Odor Identification and Odor Discrimination Deficits in Parkinson’s Disease. Mov. Disord. 2008, 23, 1984–1990. [Google Scholar] [CrossRef]
- Haehner, A.; Boesveldt, S.; Berendse, H.W.; Mackay-Sim, A.; Fleischmann, J.; Silburn, P.A.; Johnston, A.N.; Mellick, G.D.; Herting, B.; Reichmann, H.; et al. Prevalence of Smell Loss in Parkinson’s Disease—A Multicenter Study. Park. Relat. Disord. 2009, 15, 490–494. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Ercoli, T.; Frau, C.; Bagella, C.; Pinna, I.; Loy, F.; Defazio, G. Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease. Biology 2023, 12, 112. [Google Scholar] [CrossRef]
- Hummel, T.; Whitcroft, K.L.; Andrews, P.; Altundag, A.; Cinghi, C.; Costanzo, R.M.; Damm, M.; Frasnelli, J.; Gudziol, H.; Gupta, N.; et al. Position Paper on Olfactory Dysfunction. Rhinol. J. 2017, 54, 1–30. [Google Scholar] [CrossRef]
- Pellegrino, R.; Mainland, J.D.; Kelly, C.E.; Parker, J.K.; Hummel, T. Prevalence and Correlates of Parosmia and Phantosmia among Smell Disorders. Chem. Senses 2021, 46, bjab046. [Google Scholar] [CrossRef]
- Savage, S.A.; Butler, C.R.; Milton, F.; Han, Y.; Zeman, A.Z. On the Nose: Olfactory Disturbances in Patients with Transient Epileptic Amnesia. Epilepsy Behav. 2017, 66, 113–119. [Google Scholar] [CrossRef]
- Ercoli, T.; Masala, C.; Pinna, I.; Orofino, G.; Solla, P.; Rocchi, L.; Defazio, G. Qualitative Smell/Taste Disorders as Sequelae of Acute COVID-19. Neurol. Sci. 2021, 42, 4921–4926. [Google Scholar] [CrossRef]
- Stevenson, R.J.; Langdon, R.; McGuire, J. Olfactory Hallucinations in Schizophrenia and Schizoaffective Disorder: A Phenomenological Survey. Psychiatry Res. 2011, 185, 321–327. [Google Scholar] [CrossRef]
- Aarsland, D.; Ballard, C.; Larsen, J.P.; McKeith, I. A Comparative Study of Psychiatric Symptoms in Dementia with Lewy Bodies and Parkinson’s Disease with and without Dementia. Int. J. Geriat. Psychiatry 2001, 16, 528–536. [Google Scholar] [CrossRef]
- Amar, B.R.; Yadav, R.; Janardhan Reddy, Y.C.; Pal, P. A Clinical Profile of Patients with Parkinson′s Disease and Psychosis. Ann. Indian Acad. Neurol. 2014, 17, 187. [Google Scholar] [CrossRef]
- Arnulf, I.; Bonnet, A.M.; Damier, P.; Bejjani, B.P.; Seilhean, D.; Derenne, J.P.; Agid, Y. Hallucinations, REM Sleep, and Parkinson’s Disease. Neurology 2000, 55, 281–288. [Google Scholar] [CrossRef]
- Bannier, S.; Berdagué, J.L.; Rieu, I.; De Chazeron, I.; Marques, A.; Derost, P.; Ulla, M.; Llorca, P.-M.; Durif, F. Prevalence and Phenomenology of Olfactory Hallucinations in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2012, 83, 1019–1021. [Google Scholar] [CrossRef]
- Barrett, M.J.; Smolkin, M.E.; Flanigan, J.L.; Shah, B.B.; Harrison, M.B.; Sperling, S.A. Characteristics, Correlates, and Assessment of Psychosis in Parkinson Disease without Dementia. Park. Relat. Disord. 2017, 43, 56–60. [Google Scholar] [CrossRef]
- Chou, K.L.; Messing, S.; Oakes, D.; Feldman, P.D.; Breier, A.; Friedman, J.H. Drug-Induced Psychosis in Parkinson Disease. Clin. Neuropharmacol. 2005, 28, 215–219. [Google Scholar] [CrossRef]
- Factor, S.A.; Scullin, M.K.; Sollinger, A.B.; Land, J.O.; Wood-Siverio, C.; Zanders, L.; Freeman, A.; Bliwise, D.L.; McDonald, W.M.; Goldstein, F.C. Cognitive Correlates of Hallucinations and Delusions in Parkinson’s Disease. J. Neurol. Sci. 2014, 347, 316–321. [Google Scholar] [CrossRef]
- Fénelon, G.; Soulas, T.; Zenasni, F.; De Langavant, L.C. The Changing Face of Parkinson’s Disease-Associated Psychosis: A Cross-Sectional Study Based on the New NINDS-NIMH Criteria. Mov. Disord. 2010, 25, 763–766. [Google Scholar] [CrossRef]
- Gu, R.; Zhu, J.; Zhong, M.; Jiang, Y.; Zhu, S.; Wang, Y.; Jiang, X.; Shen, B.; Yan, J.; Zhang, L.; et al. Characteristics of Sleep Structure in Parkinson’s Disease Patients with Hallucinations Based on Polysomnography. Front. Neurol. 2022, 13, 929569. [Google Scholar] [CrossRef]
- Hirsch, A.R. Parkinsonism: The Hyposmia and Phantosmia Connection. Arch. Neurol. 2009, 66, 538. [Google Scholar] [CrossRef]
- Kulick, C.V.; Montgomery, K.M.; Nirenberg, M.J. Comprehensive Identification of Delusions and Olfactory, Tactile, Gustatory, and Minor Hallucinations in Parkinson’s Disease Psychosis. Park. Relat. Disord. 2018, 54, 40–45. [Google Scholar] [CrossRef]
- Landis, B.N.; Burkhard, P.R. Phantosmias and Parkinson Disease. Arch. Neurol. 2008, 65, 1237–1239. [Google Scholar] [CrossRef]
- Lenka, A.; George, L.; Arumugham, S.S.; Hegde, S.; Reddy, V.; Kamble, N.; Yadav, R.; Pal, P.K. Predictors of Onset of Psychosis in Patients with Parkinson’s Disease: Who Gets It Early? Park. Relat. Disord. 2017, 44, 91–94. [Google Scholar] [CrossRef]
- Mack, J.; Rabins, P.; Anderson, K.; Goldstein, S.; Grill, S.; Hirsch, E.S.; Lehmann, S.; Little, J.T.; Margolis, R.L.; Palanci, J.; et al. Prevalence of Psychotic Symptoms in a Community-Based Parkinson Disease Sample. Am. J. Geriatr. Psychiatry 2012, 20, 123–132. [Google Scholar] [CrossRef]
- Marques, A.; Taylor, N.L.; Roquet, D.; Beze, S.; Chassain, C.; Pereira, B.; O’Callaghan, C.; Lewis, S.J.G.; Durif, F. Structural and Functional Correlates of Hallucinations and Illusions in Parkinson’s Disease. JPD 2022, 12, 397–409. [Google Scholar] [CrossRef]
- Marsh, L.; Williams, J.R.; Rocco, M.; Grill, S.; Munro, C.; Dawson, T.M. Psychiatric Comorbidities in Patients with Parkinson Disease and Psychosis. Neurology 2004, 63, 293–300. [Google Scholar] [CrossRef]
- McAuley, J.H.; Gregory, S. Prevalence and Clinical Course of Olfactory Hallucinations in Idiopathic Parkinson’s Disease. J. Park. Dis. 2012, 2, 199–205. [Google Scholar] [CrossRef]
- Mehanna, R.; Chandra, S.; Furr-Stimming, E.; Schiess, M. Olfactory Hallucinations as a Non-Motor Sign of Parkinson’s Disease—A Cross Sectional Study amongst Patients in a Tertiary Movement Disorder Center. Park. Relat. Disord. 2022, 99, 30–32. [Google Scholar] [CrossRef]
- Muller, A.J.; Mills, J.M.Z.; O’Callaghan, C.; Naismith, S.L.; Clouston, P.D.; Lewis, S.J.G.; Shine, J.M. Informant- and Self-Appraisals on the Psychosis and Hallucinations Questionnaire (PsycH-Q) Enhances Detection of Visual Hallucinations in Parkinson’s Disease. Mov. Disord. Clin. Pract. 2018, 5, 607–613. [Google Scholar] [CrossRef]
- Omoto, S.; Murakami, H.; Shiraishi, T.; Bono, K.; Umehara, T.; Iguchi, Y. Risk Factors for Minor Hallucinations in Parkinson’s Disease. Acta Neurol. Scand. 2021, 143, 538–544. [Google Scholar] [CrossRef]
- Pagonabarraga, J.; Martinez-Horta, S.; Fernández de Bobadilla, R.; Pérez, J.; Ribosa-Nogué, R.; Marín, J.; Pascual-Sedano, B.; García, C.; Gironell, A.; Kulisevsky, J. Minor Hallucinations Occur in Drug-Naive Parkinson’s Disease Patients, Even from the Premotor Phase: Minor Hallucinations in Untreated PD Patients. Mov. Disord. 2016, 31, 45–52. [Google Scholar] [CrossRef]
- Papapetropoulos, S.; Katzen, H.; Schrag, A.; Singer, C.; Scanlon, B.K.; Nation, D.; Guevara, A.; Levin, B. A Questionnaire-Based (UM-PDHQ) Study of Hallucinations in Parkinson’s Disease. BMC Neurol. 2008, 8, 21. [Google Scholar] [CrossRef]
- Rai, N.; Goyal, V.; Kumar, N.; Shukla, G.; Singh, S.; Behari, M.; Srivastava, A. Neuropsychiatric Co-Morbidities in Non-Demented Parkinson′s Disease. Ann. Indian Acad. Neurol. 2014, 26, 619–620. [Google Scholar] [CrossRef]
- Shine, J.M.; Mills, J.M.Z.; Qiu, J.; O’Callaghan, C.; Terpening, Z.; Halliday, G.M.; Naismith, S.L.; Lewis, S.J.G. Validation of the Psychosis and Hallucinations Questionnaire in Non-demented Patients with Parkinson’s Disease. Mov. Disord. Clin. Pract. 2015, 2, 175–181. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Pinna, I.; Ercoli, T.; Loy, F.; Orofino, G.; Fadda, L.; Defazio, G. Frequency and Determinants of Olfactory Hallucinations in Parkinson’s Disease Patients. Brain Sci. 2021, 11, 841. [Google Scholar] [CrossRef]
- Svetel, M.; Smiljković, T.; Pekmezović, T.; Kostić, V. Hallucinations in Parkinson’s Disease: Cross-Sectional Study. Acta Neurol. Belg. 2012, 112, 33–37. [Google Scholar] [CrossRef]
- Tousi, B.; Frankel, M. Olfactory and Visual Hallucinations in Parkinson’s Disease. Park. Relat. Disord. 2004, 10, 253–254. [Google Scholar] [CrossRef]
- Whitehead, D.L.; Davies, A.D.M.; Playfer, J.R.; Turnbull, C.J. Circadian Rest-Activity Rhythm Is Altered in Parkinson’s Disease Patients with Hallucinations. Mov. Disord. 2008, 23, 1137–1145. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, G.Y.; Zhu, X.B.; Zhang, Z.E.; Gan, J.; Liu, Z.G. Clinical Characteristics of Minor Hallucinations in Chinese Parkinson’s Disease Patients. Front. Aging Neurosci. 2022, 13, 723405. [Google Scholar] [CrossRef]
- Schutte, M.J.L.; Linszen, M.M.J.; Marschall, T.M.; Ffytche, D.H.; Koops, S.; Van Dellen, E.; Heringa, S.M.; Slooter, A.J.C.; Teunisse, R.; Van Den Heuvel, O.A.; et al. Hallucinations and Other Psychotic Experiences across Diagnoses: A Comparison of Phenomenological Features. Psychiatry Res. 2020, 292, 113314. [Google Scholar] [CrossRef]
- Llorca, P.M.; Pereira, B.; Jardri, R.; Chereau-Boudet, I.; Brousse, G.; Misdrahi, D.; Fénelon, G.; Tronche, A.-M.; Schwan, R.; Lançon, C.; et al. Hallucinations in Schizophrenia and Parkinson’s Disease: An Analysis of Sensory Modalities Involved and the Repercussion on Patients. Sci. Rep. 2016, 6, 38152. [Google Scholar] [CrossRef]
- Toh, W.L.; Yolland, C.; Gurvich, C.; Barnes, J.; Rossell, S.L. Non-Visual Hallucinations in Parkinson’s Disease: A Systematic Review. J. Neurol. 2023, 270, 2857–2889. [Google Scholar] [CrossRef]
- Goetz, C.G.; Stebbins, G.T.; Ouyang, B. Visual plus Nonvisual Hallucinations in Parkinson’s Disease: Development and Evolution over 10 Years: Visual Plus Nonvisual Hallucinations in PD. Mov. Disord. 2011, 26, 2196–2200. [Google Scholar] [CrossRef]
- Goetz, C.G.; Vogel, C.; Tanner, C.M.; Stebbins, G.T. Early Dopaminergic Drug-Induced Hallucinations in Parkinsonian Patients. Neurology 1998, 51, 811–814. [Google Scholar] [CrossRef]
- Mehanna, R.; Furr-Stimming, E.; Schiess, M. Not Just a Difference in Perception: What If Olfactory Hallucinations Are More Frequent That Previously Reported in Parkinson’s Disease Patients? Park. Relat. Disord. 2022, 102, 142–143. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Pinna, I.; Frau, C.; Ercoli, T.; Defazio, G. Olfactory Hallucinations in Parkinson’s Disease Patients and the Role of Their Evaluation in Clinical Practice. Park. Relat. Disord. 2022, 102, 141. [Google Scholar] [CrossRef] [PubMed]
- Scarmeas, N.; Brandt, J.; Albert, M.; Hadjigeorgiou, G.; Papadimitriou, A.; Dubois, B.; Sarazin, M.; Devanand, D.; Honig, L.; Marder, K.; et al. Delusions and Hallucinations Are Associated with Worse Outcome in Alzheimer Disease. Arch. Neurol. 2005, 62, 1601–1608. [Google Scholar] [CrossRef] [PubMed]
- El Haj, M.; Larøi, F. Olfactory Hallucinations in Alzheimer’s Disease. Acta Neuropsychiatr. 2021, 33, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, T.; Miyamoto, M.; Iwanami, M.; Hirata, K.; Kobayashi, M.; Nakamura, M.; Inoue, Y. Olfactory Dysfunction in Idiopathic REM Sleep Behavior Disorder. Sleep Med. 2010, 11, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Abraham, A.; Bay, A.A.; Ni, L.; Schindler, N.; Singh, E.; Leeth, E.; Bozorg, A.; Hart, A.R.; Hackney, M.E. Gender Differences in Motor and Non-Motor Symptoms in Individuals with Mild-Moderate Parkinson’s Disease. PLoS ONE 2023, 18, e0272952. [Google Scholar] [CrossRef] [PubMed]
- Santos-García, D.; Laguna, A.; Hernández-Vara, J.; De Deus Fonticoba, T.; Cores Bartolomé, C.; Feal Painceiras, M.J.; Íñiguez-Alvarado, M.C.; García Díaz, I.; Jesús, S.; Boungiorno, M.T.; et al. Sex Differences in Motor and Non-Motor Symptoms among Spanish Patients with Parkinson’s Disease. J. Clin. Med. 2023, 12, 1329. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Liscia, A.; Piras, R.; Ercoli, T.; Fadda, L.; Hummel, T.; Haenher, A.; Defazio, G. Sex-Related Differences in Olfactory Function and Evaluation of Possible Confounding Factors among Patients with Parkinson’s Disease. J. Neurol. 2019, 267, 57–63. [Google Scholar] [CrossRef]
- Thomas, G.E.; Zeidman, P.; Sultana, T.; Zarkali, A.; Razi, A.; Weil, R.S. Changes in Both Top-down and Bottom-up Effective Connectivity Drive Visual Hallucinations in Parkinson’s Disease. Brain Commun. 2023, 5, fcac329. [Google Scholar] [CrossRef]
- Weil, R.; Reeves, S. Hallucinations in Parkinson’s Disease: New Insights into Mechanisms and Treatments. ACNR 2020, 19, 20–22. [Google Scholar] [CrossRef]
- Powell, A.; Matar, E.; Lewis, S.J.G. Treating Hallucinations in Parkinson’s Disease. Expert Rev. Neurother. 2022, 22, 455–468. [Google Scholar] [CrossRef]
- Franke, C.; Storch, A. Nonmotor Fluctuations in Parkinson’s Disease. In International Review of Neurobiology; Elsevier: Amsterdam, The Netherlands, 2017; Volume 134, pp. 947–971. ISBN 978-0-12-812603-5. [Google Scholar]
- Ercoli, T.; Masala, C.; Cadeddu, G.; Mascia, M.M.; Orofino, G.; Gigante, A.F.; Solla, P.; Defazio, G.; Rocchi, L. Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature. Brain Sci. 2022, 12, 513. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Ref | Authors | Year of Publication | Study Design | Sample Size | Number of Patients with OHs (%) |
|---|---|---|---|---|---|
| [16] | Aarsland et al. | 2001 | cross-sectional | 83 PD without dementia and 48 PDD | 1 (1%) PD and 3 PDD (6%) |
| [17] | Amar et al. | 2014 | cross-sectional | 40 PD | 1 (2.5%) |
| [18] | Arnulf et al. | 2000 | case report | 1 PD | 1 |
| [19] | Bannier et al. | 2012 | cross-sectional | 87 PD | 9 (10%) |
| [20] | Barrett et al. | 2017 | cross-sectional | 101 PD | 4 (4%) |
| [21] | Chou et al. | 2005 | baseline data from 2 studies on PD patients with drug-induced psychosis | 160 PD | 25 (16%) |
| [22] | Factor et al. | 2014 | cross-sectional | 144 PD | 7 (4.9%) |
| [23] | Fenelon et al. | 2010 | cross-sectional | 116 PD | 13 (11%) |
| [24] | Gu et al. | 2022 | cross-sectional | 278 PD | 4 (5.2%) |
| [25] | Hirsch et al. | 2009 | case report | 1 PD | 1 |
| Burkhard and Landis | 2009 | case report | 1 PD | 1 | |
| [26] | Kulick et al. | 2018 | cross-sectional | 199 PD | 11 (5.5%) |
| [27] | Landis and Burkhard | 2008 | case series | 1 PD | 1 |
| 1 PD | 1 | ||||
| [28] | Lenka et al. | 2017 | cross-sectional | 51 PD | 1 (1.9%) |
| [29] | Mack et al. | 2012 | cross-sectional | 250 PD | 5 (2%) |
| [30] | Marques et al. | 2022 | cross-sectional | 62 PD | 5 (8%) |
| [31] | Marsh et al. | 2004 | cross-sectional | 116 PD | 3 (2.6%) |
| [32] | McAuley and Gregory | 2012 | cross-sectional plus case description | 188 PD | 4 (2.1%) at baseline and 2 (1%) at follow-up |
| [33] | Mehanna et al. | 2022 | cross-sectional | 137 PD | 25 (18.2%) |
| [34] | Muller et al. | 2018 | cross-sectional | 163 PD | 15 (9%) |
| [35] | Omoto et al. | 2020 | cross-sectional | 100 PD | 2 (2%) |
| [36] | Pagonabarraga et al. | 2015 | baseline data from a longitudinal study | 50 PD | 2 (4%) |
| [37] | Papapetropoulos et al. | 2008 | cross-sectional | 70 PD | 5 (7.1%) |
| [38] | Rai et al. | 2015 | cross-sectional | 126 PD | 2 (1.6%) |
| [39] | Shine et al. | 2014 | cross-sectional | 197 PD | 18 (9%) |
| [40] | Solla et al. | 2021 | cross-sectional | 141 PD | 16 (11.3%) |
| [41] | Svetel et al. | 2012 | cross-sectional | 180 PD | 1 (0.5%) |
| [42] | Tousi and Frankel | 2004 | case report | 1 PD | 1 |
| [43] | Whitehead et al. | 2008 | case series | 50 PD | 3 (6%) |
| [44] | Zhang et al. | 2022 | cross-sectional | 149 | 8.1% |
| Question Category | Question | Scoring |
|---|---|---|
| Symptom Assessment | Have you experienced any unusual or abnormal smells that others do not seem to notice? (Yes/No) | Yes: 1 point; No: 0 points |
| Symptom Description | Describe whether these smells are pleasant or unpleasant. | N/A |
| Describe the nature of these smells (e.g., foul, sweet, burning, chemical). | N/A | |
| Frequency | How often do you experience these smells? (Daily, Weekly, Monthly) | Daily: 3 points; Weekly: 2 points; Monthly: 1 point; Never: 0 points |
| Onset | How long have you noticed these smells? | <6 months: 1 point; 6–12 months: 2 points; >12 months: 3 points |
| Consistency | Do these smells occur at specific times, or are they random? (Specific Times/Random) | Specific Times: 2 points; Random: 1 point |
| Correlation with PD | Do you notice these smells more during certain states of your PD (e.g., ON/OFF states)? (Yes/No) | Yes: 2 points; No: 0 points |
| State Description | If yes, please describe these states and their relation to the smells. | N/A |
| Impact on Daily Life | Do these smells affect your eating habits? (Yes/No) | Yes: 1 point; No: 0 points |
| Do these smells interfere with daily activities? (Yes/No) | Yes: 1 point; No: 0 points | |
| Distress Level | Rate the distress caused by these smells on a scale of 0 to 10. | 0–10 scale |
| Associated Symptoms | Do you experience any other symptoms along with the smells? (Please describe, e.g., headaches, dizziness, pain, sweating.) | N/A |
| Treatment and Management | Have you noticed any factors or conditions that seem to trigger or worsen these unusual smells? (Please describe.) | N/A |
| Are there any activities, treatments, or conditions that appear to alleviate or reduce these smells? (Please describe.) | N/A | |
| Are you currently receiving any treatment specifically for these smells? | N/A | |
| Additional Comments | Please provide any additional information or comments regarding your experience with phantosmia. | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ercoli, T.; Bagella, C.F.; Frau, C.; Ruiu, E.; Othmani, S.; Gusinu, G.; Masala, C.; Sechi, L.A.; Solla, P.; Defazio, G. Phantosmia in Parkinson’s Disease: A Systematic Review of the Phenomenology of Olfactory Hallucinations. Neurol. Int. 2024, 16, 20-32. https://doi.org/10.3390/neurolint16010002
Ercoli T, Bagella CF, Frau C, Ruiu E, Othmani S, Gusinu G, Masala C, Sechi LA, Solla P, Defazio G. Phantosmia in Parkinson’s Disease: A Systematic Review of the Phenomenology of Olfactory Hallucinations. Neurology International. 2024; 16(1):20-32. https://doi.org/10.3390/neurolint16010002
Chicago/Turabian StyleErcoli, Tommaso, Caterina Francesca Bagella, Claudia Frau, Elisa Ruiu, Sabrine Othmani, Giansalvo Gusinu, Carla Masala, Leonardo Antonio Sechi, Paolo Solla, and Giovanni Defazio. 2024. "Phantosmia in Parkinson’s Disease: A Systematic Review of the Phenomenology of Olfactory Hallucinations" Neurology International 16, no. 1: 20-32. https://doi.org/10.3390/neurolint16010002
APA StyleErcoli, T., Bagella, C. F., Frau, C., Ruiu, E., Othmani, S., Gusinu, G., Masala, C., Sechi, L. A., Solla, P., & Defazio, G. (2024). Phantosmia in Parkinson’s Disease: A Systematic Review of the Phenomenology of Olfactory Hallucinations. Neurology International, 16(1), 20-32. https://doi.org/10.3390/neurolint16010002