
Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis

 , , ,
, , ,
Abstract
1. Background
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Patient Selection
2.4. Outcomes and Variables
2.5. Statistical Analysis and Visualisation
3. Results
3.1. Study Sample Characteristics
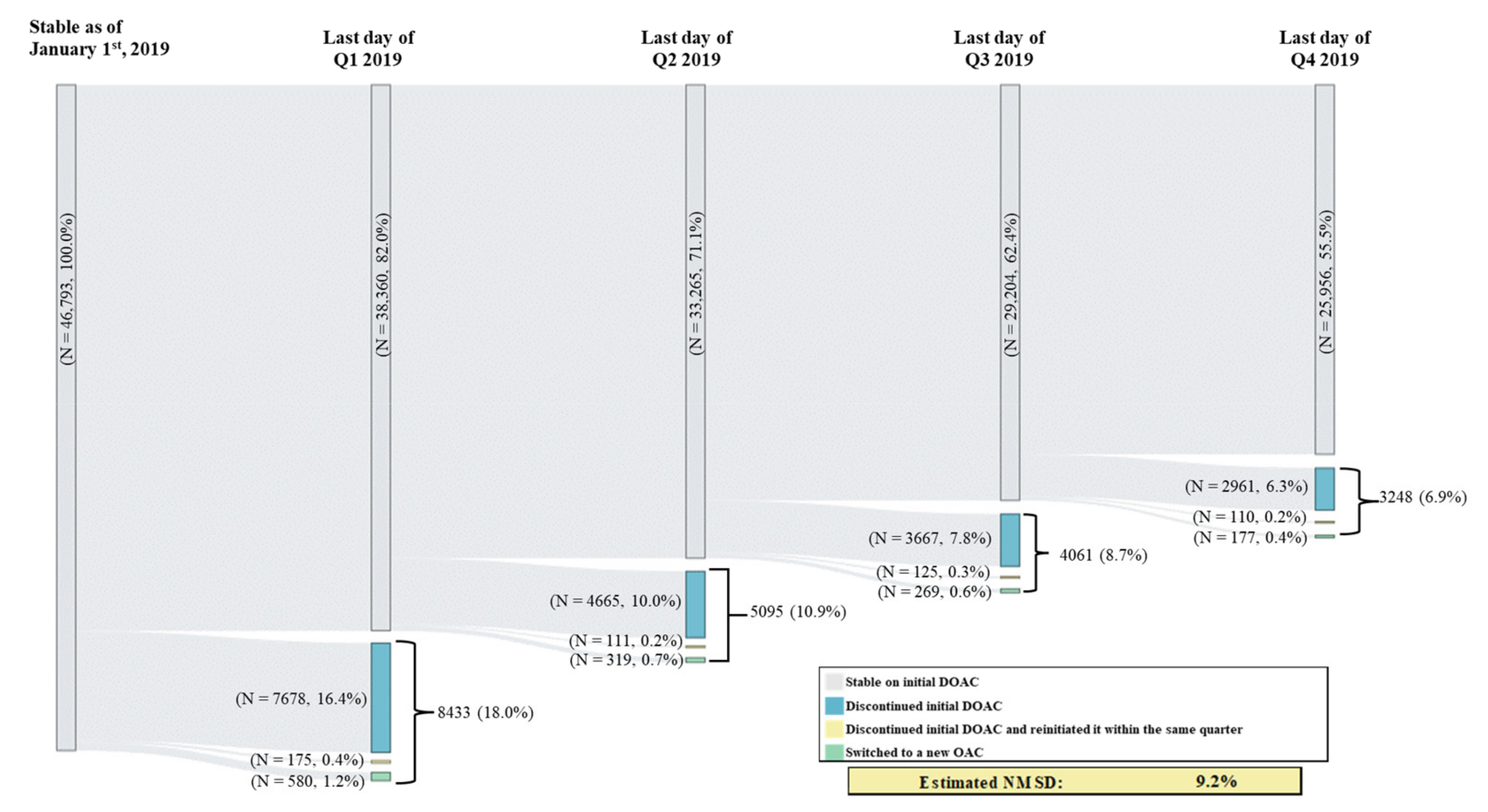
3.2. Switching and Discontinuation Patterns
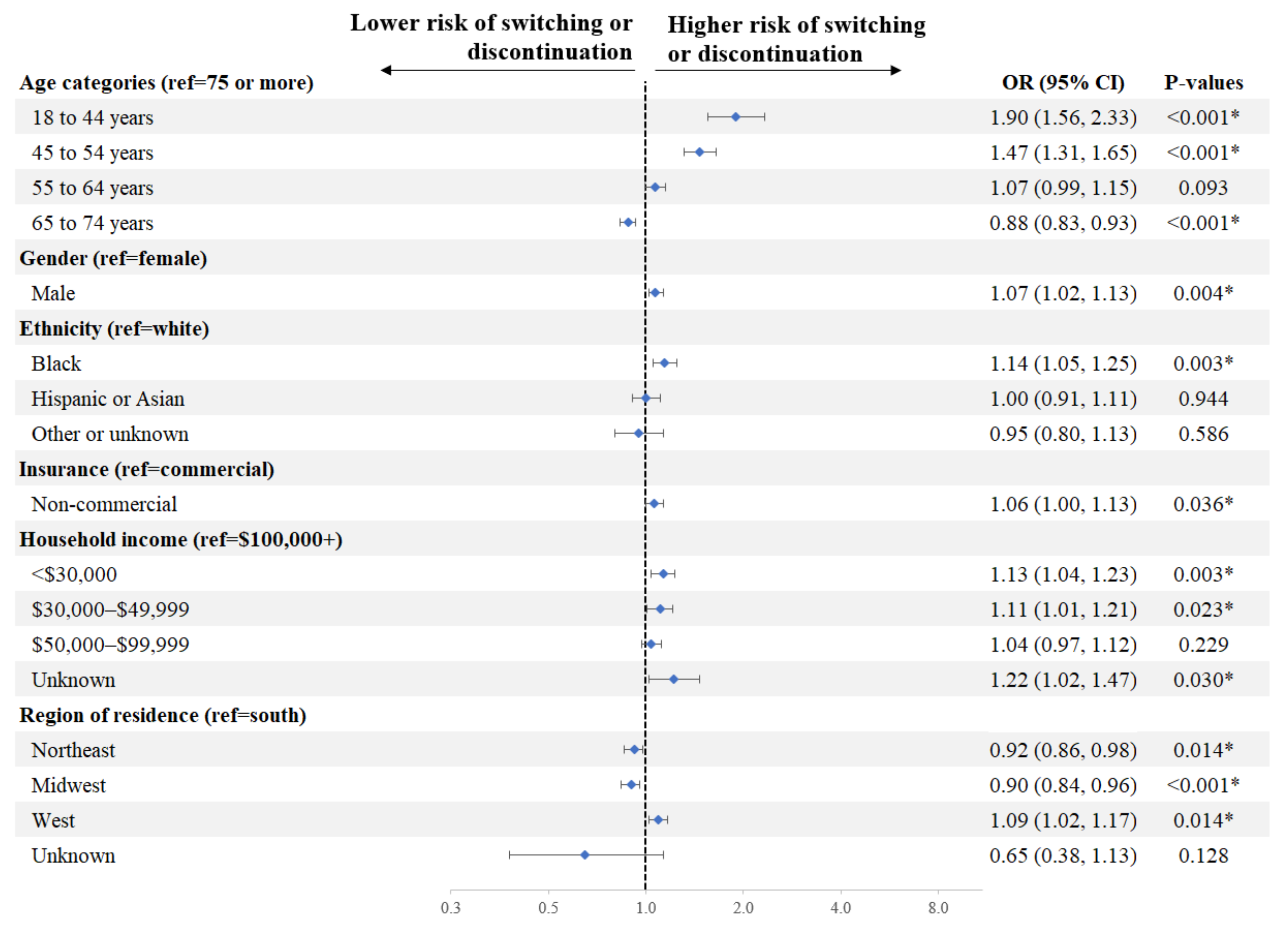
3.3. Demographic and Socioeconomic Factors Associated with Switching or Discontinuation of Initial DOAC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AF | Atrial fibrillation |
| DOAC | Direct-acting oral anticoagulant |
| NMSD | Non-medical switching or discontinuation |
| NVAF | Non-valvular atrial fibrillation |
| OAC | Oral anticoagulant |
| OR | Odds ratio |
| US | United States |
References
- Kornej, J.; Borschel, C.S.; Benjamin, E.J.; Schnabel, R.B. Epidemiology of atrial fibrillation in the 21st century: Novel methods and new insights. Circ. Res. 2020, 127, 4–20. [Google Scholar] [CrossRef]
- Reiffel, J.A. Atrial fibrillation and stroke: Epidemiology. Am. J. Med. 2014, 127, e15–e16. [Google Scholar] [CrossRef]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef]
- January, C.T.; Wann, L.S.; Calkins, H.; Chen, L.Y.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; Furie, K.L.; et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2019, 74, 104–132. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic therapy for atrial fibrillation: CHEST guideline and expert panel report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [PubMed]
- American College of Cardiology Foundation; American Heart Association; European Society of Cardiology; Heart Rhythm Society; Wann, L.S.; Curtis, A.B.; Ellenbogen, K.A.; Estes, N.A.; Ezekowitz, M.D.; Jackman, W.M.; et al. Management of patients with atrial fibrillation (compilation of 2006 ACCF/AHA/ESC and 2011 ACCF/AHA/HRS recommendations): A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 2013, 127, 1916–1926. [Google Scholar] [CrossRef]
- Gupta, K.; Trocio, J.; Keshishian, A.; Zhang, Q.; Dina, O.; Mardekian, J.; Nadkarni, A.; Shank, T.C. Effectiveness and safety of direct oral anticoagulants compared to warfarin in treatment naive non-valvular atrial fibrillation patients in the US Department of Defense population. BMC Cardiovasc. Disord. 2019, 19, 142. [Google Scholar] [CrossRef] [PubMed]
- Pirlog, A.M.; Pirlog, C.D.; Maghiar, M.A. DOACs vs. vitamin K antagonists: A comparison of phase III clinical trials and a prescriber support tool. Open Access Maced. J. Med. Sci. 2019, 7, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.G.; Aguilar, M.; Atzema, C.; Bell, A.; Cairns, J.A.; Cheung, C.C.; Cox, J.L.; Dorian, P.; Gladstone, D.J.; Healey, J.S.; et al. The 2020 Canadian Cardiovascular Society/Canadian Heart Rhythm Society comprehensive guidelines for the management of atrial fibrillation. Can. J. Cardiol. 2020, 36, 1847–1948. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Klijn, C.J.; Paciaroni, M.; Berge, E.; Korompoki, E.; Korv, J.; Lal, A.; Putaala, J.; Werring, D.J. Antithrombotic treatment for secondary prevention of stroke and other thromboembolic events in patients with stroke or transient ischemic attack and non-valvular atrial fibrillation: A European Stroke Organisation guideline. Eur. Stroke J. 2019, 4, 198–223. [Google Scholar] [CrossRef] [PubMed]
- Navar, A.M.; Kolkailah, A.A.; Overton, R.; Shah, N.P.; Rousseau, J.F.; Flaker, G.C.; Pignone, M.P.; Peterson, E.D. Trends in oral anticoagulant use among 436 864 patients with atrial fibrillation in community practice, 2011 to 2020. J. Am. Heart Assoc. 2022, 11, e026723. [Google Scholar] [CrossRef] [PubMed]
- Adelakun, A.R.; Turgeon, R.D.; De Vera, M.A.; McGrail, K.; Loewen, P.S. Oral anticoagulant switching in patients with atrial fibrillation: A scoping review. BMJ Open 2023, 13, e071907. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, A.F.; Choi, A.S.; Le, Q.T.; Ko, D.T.; Han, J.K.; Park, S.S.; Jackevicius, C.A. Real-world adherence and persistence to direct oral anticoagulants in patients with atrial fibrillation: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e005969. [Google Scholar] [CrossRef]
- Kirley, K.; Rao, G.; Bauer, V.; Masi, C. The role of NOACs in atrial fibrillation management: A qualitative study. J. Atr. Fibrillation 2016, 9, 1416. [Google Scholar] [CrossRef]
- Nguyen, E.; Weeda, E.R.; Sobieraj, D.M.; Bookhart, B.K.; Piech, C.T.; Coleman, C.I. Impact of non-medical switching on clinical and economic outcomes, resource utilization and medication-taking behavior: A systematic literature review. Curr. Med. Res. Opin. 2016, 32, 1281–1290. [Google Scholar] [CrossRef]
- Dolinar, R.; Kohn, C.G.; Lavernia, F.; Nguyen, E. The non-medical switching of prescription medications. Postgrad. Med. 2019, 131, 335–341. [Google Scholar] [CrossRef]
- Pearson, S.D.; Lowe, M.; Towse, A.; Segel, C.S.; Henshall, C. Cornerstones of “fair” drug coverage: Appropriate cost-sharing and utilization management policies for pharmaceuticals. J. Comp. Eff. Res. 2021, 10, 537–547. [Google Scholar] [CrossRef]
- American Society for Preventive Cardiologist (ASPC). Total Fear & Stress: The Impact of Non-Medical Switching on Patients Taking a Blood Thinner; ASPC: Kingwood, TX, USA, 2022; pp. 1–6. [Google Scholar]
- Happe, L.E.; Clark, D.; Holliday, E.; Young, T. A systematic literature review assessing the directional impact of managed care formulary restrictions on medication adherence, clinical outcomes, economic outcomes, and health care resource utilization. J. Manag. Care Spec. Pharm. 2014, 20, 677–684. [Google Scholar] [CrossRef]
- Coleman, C.; Salam, T.; Duhig, A.; Patel, A.A.; Cameron, A.; Voelker, J.; Bookhart, B. Impact of non-medical switching of prescription medications on health outcomes: An e-survey of high-volume Medicare and Medicaid physician providers. J. Mark. Access Health Policy 2020, 8, 1829883. [Google Scholar] [CrossRef]
- Costa, O.S.; Salam, T.; Duhig, A.; Patel, A.A.; Cameron, A.; Voelker, J.; Bookhart, B.; Coleman, C.I. Specialist physician perspectives on non-medical switching of prescription medications. J. Mark. Access Health Policy 2020, 8, 1738637. [Google Scholar] [CrossRef] [PubMed]
- Baum, D.S.J. Non-medical switching an unmitigated threat to patient care. Am. J. Prev. Cardiol. 2023, 13, 100470. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.L.; Dhamane, A.D.; Mardekian, J.; Dina, O.; Russ, C.; Rosenblatt, L.; Lingohr-Smith, M.; Menges, B.; Lin, J.; Nadkarni, A. Comparison of drug switching and discontinuation rates in patients with nonvalvular atrial fibrillation treated with direct oral anticoagulants in the United States. Adv. Ther. 2019, 36, 162–174. [Google Scholar] [CrossRef] [PubMed]
- Jackson, L.R., 2nd; Kim, S.; Blanco, R.; Thomas, L.; Ansell, J.; Fonarow, G.C.; Gersh, B.J.; Go, A.S.; Kowey, P.R.; Mahaffey, K.W.; et al. Discontinuation rates of warfarin versus direct acting oral anticoagulants in US clinical practice: Results from Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II (ORBIT-AF II). Am. Heart J. 2020, 226, 85–93. [Google Scholar] [CrossRef]
- Willey, V.; Franchino-Elder, J.; Fu, A.C.; Wang, C.; Sander, S.; Tan, H.; Kraft, E.; Jain, R. Treatment and persistence with oral anticoagulants among newly diagnosed patients with non-valvular atrial fibrillation: A retrospective observational study in a US commercially insured and Medicare Advantage population. BMJ Open 2018, 8, e020676. [Google Scholar] [CrossRef]
- Centers for Medicare & Medicaid Services (CMS). Chapter 6–Part D drugs and formulary requirements. In Medicare Prescription Drug Benefit Manual; CMS: Baltimore, MD, USA, 2016; pp. 1–83. [Google Scholar]
- Rae, M.; Cox, C.; Levitt, L. Deductible Relief Day: How Rising Deductibles Are Affecting People with Employer Coverage. Available online: https://www.healthsystemtracker.org/brief/deductible-relief-day-how-rising-deductibles-are-affecting-people-with-employer-coverage/ (accessed on 12 May 2023).
- Essien, U.R.; Holmes, D.N.; Jackson, L.R., II; Fonarow, G.C.; Mahaffey, K.W.; Reiffel, J.A.; Steinberg, B.A.; Allen, L.A.; Chan, P.S.; Freeman, J.V.; et al. Association of race/ethnicity with oral anticoagulant use in patients with atrial fibrillation: Findings from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation II. JAMA Cardiol. 2018, 3, 1174–1182. [Google Scholar] [CrossRef]
- Wharam, J.F.; Zhang, F.; Landon, B.E.; Soumerai, S.B.; Ross-Degnan, D. Low-socioeconomic-status enrollees in high-deductible plans reduced high-severity emergency care. Health Aff. 2013, 32, 1398–1406. [Google Scholar] [CrossRef]
- Dhamane, A.D.; Hernandez, I.; Di Fusco, M.; Gutierrez, C.; Ferri, M.; Russ, C.; Tsai, W.-L.; Emir, B.; Yuce, H.; Keshishian, A. Non-persistence to oral anticoagulation treatment in patients with non-valvular atrial fibrillation in the USA. Am. J. Cardiovasc. Drugs 2021, 22, 333–343. [Google Scholar] [CrossRef]
- Essien, U.R.; Lusk, J.B.; Dusetzina, S.B. Cost-sharing reform for chronic disease treatments as a strategy to improve health care equity and value in the US. JAMA Health Forum 2022, 3, e224804. [Google Scholar] [CrossRef]
- Dusetzina, S.B.; Besaw, R.J.; Whitmore, C.C.; Mattingly, T.J., II; Sinaiko, A.D.; Keating, N.L.; Everson, J. Cost-related medication nonadherence and desire for medication cost information among adults aged 65 years and older in the US in 2022. JAMA Netw. Open 2023, 6, e2314211. [Google Scholar] [CrossRef]
- Mykyta, L.; Cohen, R.A. Characteristics of adults aged 18–64 who did not take medication as prescribed to reduce costs: United States, 2021. NCHS Data Brief 2023, 470, 1–8. [Google Scholar]
- Agarwal, R.; Mazurenko, O.; Menachemi, N. High-deductible health plans reduce health care cost and utilization, including use of needed preventive services. Health Aff. 2017, 36, 1762–1768. [Google Scholar] [CrossRef] [PubMed]
- Eaddy, M.T.; Cook, C.L.; O’Day, K.; Burch, S.P.; Cantrell, C.R. How patient cost-sharing trends affect adherence and outcomes: A literature review. Pharm. Ther. 2012, 37, 45–55. [Google Scholar] [PubMed]
- Toorop, M.M.A.; Chen, Q.; Tichelaar, V.; Cannegieter, S.C.; Lijfering, W.M. Predictors, time course, and outcomes of persistence patterns in oral anticoagulation for non-valvular atrial fibrillation: A Dutch nationwide cohort study. Eur. Heart J. 2021, 42, 4126–4137. [Google Scholar] [CrossRef] [PubMed]
- Nathan, A.S.; Geng, Z.; Dayoub, E.J.; Khatana, S.A.M.; Eberly, L.A.; Kobayashi, T.; Pugliese, S.C.; Adusumalli, S.; Giri, J.; Groeneveld, P.W. Racial, ethnic, and socioeconomic inequities in the prescription of direct oral anticoagulants in patients with venous thromboembolism in the United States. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005600. [Google Scholar] [CrossRef]
- Cools, F.; Johnson, D.; Camm, A.J.; Bassand, J.P.; Verheugt, F.W.A.; Yang, S.; Tsiatis, A.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Kayani, G.; et al. Risks associated with discontinuation of oral anticoagulation in newly diagnosed patients with atrial fibrillation: Results from the GARFIELD-AF Registry. J. Thromb. Haemost. 2021, 19, 2322–2334. [Google Scholar] [CrossRef]
- Farinha, J.M.; Jones, I.D.; Lip, G.Y.H. Optimizing adherence and persistence to non-vitamin K antagonist oral anticoagulant therapy in atrial fibrillation. Eur. Heart J. Suppl. 2022, 24, A42–A55. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Saya, U.Y.; Shrank, W.H.; Greenberg, J.O.; Melia, C.; Bilodeau, A.; Kadehjian, E.K.; Dolan, M.L.; Dudley, J.C.; Kachalia, A. Cost-related medication underuse: Prevalence among hospitalized managed care patients. J. Hosp. Med. 2012, 7, 104–109. [Google Scholar] [CrossRef]
- Gellad, W.F.; Haas, J.S.; Safran, D.G. Race/ethnicity and nonadherence to prescription medications among seniors: Results of a national study. J. Gen. Intern. Med. 2007, 22, 1572–1578. [Google Scholar] [CrossRef]
- Kachroo, S.; Hamilton, M.; Liu, X.; Pan, X.; Brixner, D.; Marrouche, N.; Biskupiak, J. Oral anticoagulant discontinuation in patients with nonvalvular atrial fibrillation. Am. J. Manag. Care 2016, 22, e1–e8. [Google Scholar]
- Doehner, W.; Bohm, M.; Boriani, G.; Christersson, C.; Coats, A.J.S.; Haeusler, K.G.; Jones, I.D.; Lip, G.Y.H.; Metra, M.; Ntaios, G.; et al. Interaction of heart failure and stroke: A clinical consensus statement of the ESC Council on Stroke, the Heart Failure Association (HFA) and the ESC Working Group on Thrombosis. Eur. J. Heart Fail. 2023, 25, 2107–2129. [Google Scholar] [CrossRef] [PubMed]
- Tsimihodimos, V.; Gonzalez-Villalpando, C.; Meigs, J.B.; Ferrannini, E. Hypertension and diabetes mellitus: Coprediction and time trajectories. Hypertension 2018, 71, 422–428. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| N = 46,793 | |
|---|---|
| Age categories, N (%) | |
| 18 to 44 years | 474 (1.0) |
| 45 to 54 years | 1841 (3.9) |
| 55 to 64 years | 7665 (16.4) |
| 65 to 74 years | 14,549 (31.1) |
| 75 years or more | 22,264 (47.6) |
| Gender, N (%) | |
| Male | 24,617 (52.6) |
| Female | 22,176 (47.4) |
| Ethnicity, N (%) | |
| White | 30,982 (66.2) |
| Black | 3623 (7.7) |
| Hispanic or Asian | 2716 (5.8) |
| Other or unknown | 9472 (20.2) |
| Insurance, N (%) | |
| Non-commercial | 31,946 (68.3) |
| Medicare | 28,736 (61.4) |
| Medicaid | 2980 (6.4) |
| Other | 230 (0.5) |
| Commercial | 14,847 (31.7) |
| Household income, N (%) | |
| <$30,000 | 8273 (17.7) |
| $30,000–$49,999 | 6091 (13.0) |
| $50,000–$99,999 | 14,674 (31.4) |
| $100,000+ | 9272 (19.8) |
| Unknown | 8483 (18.1) |
| Education, N (%) | |
| High school or less | 10,680 (22.8) |
| Some college | 16,651 (35.6) |
| Associate degree and above | 10,940 (23.4) |
| Unknown | 8522 (18.2) |
| Census region of residence, N (%) | |
| Northeast | 9942 (21.2) |
| Midwest | 11,037 (23.6) |
| West | 6946 (14.8) |
| South | 18,760 (40.1) |
| Unknown | 108 (0.2) |
| Month of initiation in 2018, N (%) | |
| Jul | 10,105 (21.6) |
| Aug | 11,190 (23.9) |
| Sep | 10,869 (23.2) |
| Oct | 13,259 (28.3) |
| Nov | 1370 (2.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Published by MDPI on behalf of the Market Access Society. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ingham, M.; Romdhani, H.; Patel, A.; Ashton, V.; Caron-Lapointe, G.; Tardif-Samson, A.; Lefebvre, P.; Lafeuille, M.-H. Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis. J. Mark. Access Health Policy 2024, 12, 252-263. https://doi.org/10.3390/jmahp12030020
Ingham M, Romdhani H, Patel A, Ashton V, Caron-Lapointe G, Tardif-Samson A, Lefebvre P, Lafeuille M-H. Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis. Journal of Market Access & Health Policy. 2024; 12(3):252-263. https://doi.org/10.3390/jmahp12030020
Chicago/Turabian StyleIngham, Michael, Hela Romdhani, Aarti Patel, Veronica Ashton, Gabrielle Caron-Lapointe, Anabelle Tardif-Samson, Patrick Lefebvre, and Marie-Hélène Lafeuille. 2024. "Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis" Journal of Market Access & Health Policy 12, no. 3: 252-263. https://doi.org/10.3390/jmahp12030020
APA StyleIngham, M., Romdhani, H., Patel, A., Ashton, V., Caron-Lapointe, G., Tardif-Samson, A., Lefebvre, P., & Lafeuille, M.-H. (2024). Non-Medical Switching or Discontinuation Patterns among Patients with Non-Valvular Atrial Fibrillation Treated with Direct Oral Anticoagulants in the United States: A Claims-Based Analysis. Journal of Market Access & Health Policy, 12(3), 252-263. https://doi.org/10.3390/jmahp12030020