
Market Access Challenges and Solutions in Cell and Gene Therapy in The Netherlands

Abstract
1. Introduction
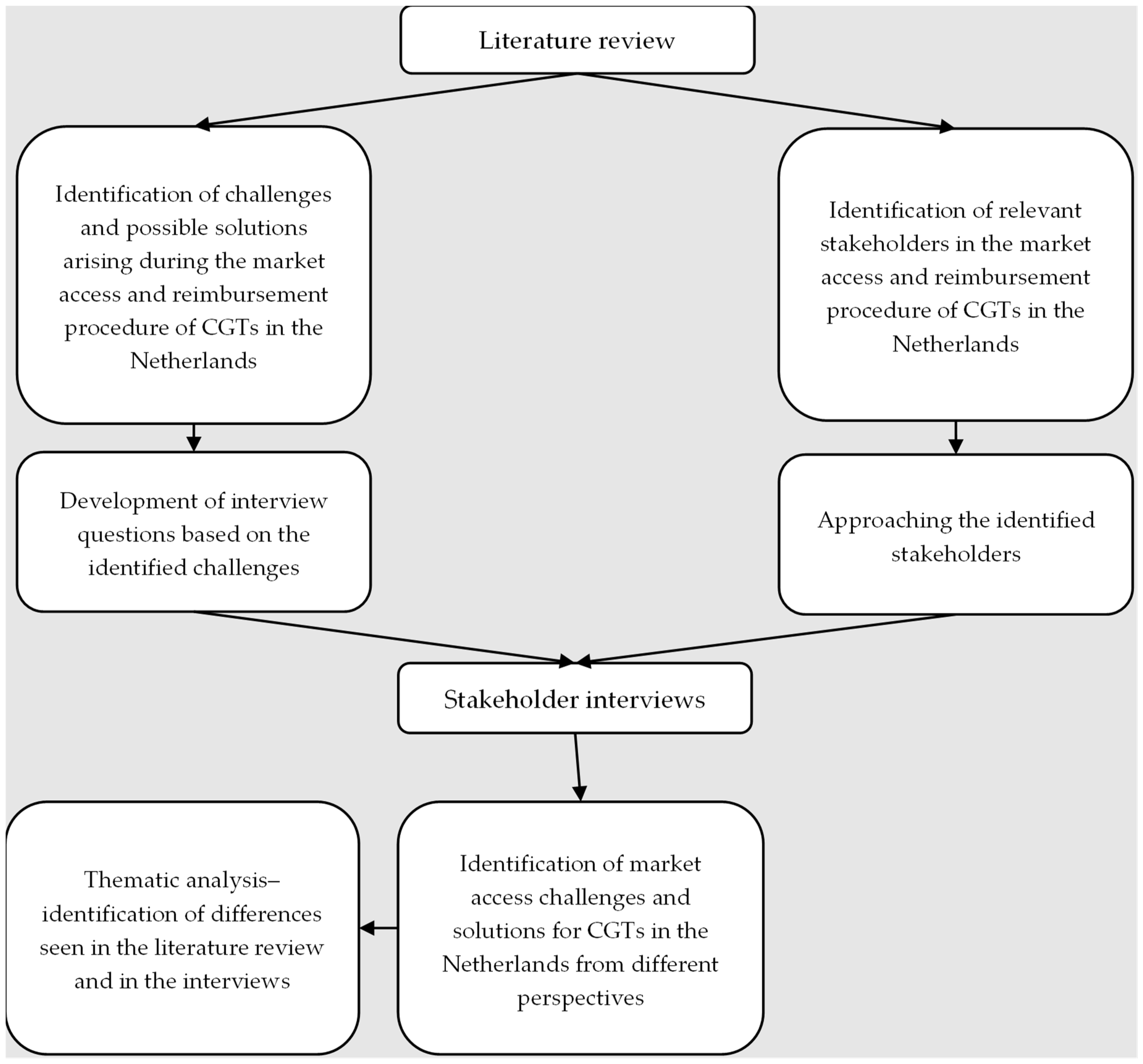
2. Materials and Methods
2.1. Literature Review
2.2. Study Sample
2.3. Developing the Interview Guide
2.4. Administering Semi-Structured Interviews
2.5. Analysing Data
3. Results
3.1. Literature Review
3.2. Study Sample
3.3. Interview Guide
3.4. Views on the Reimbursement Package Management Challenges
3.5. Views on the Clinical Trials, State-of-the-Art, and Science Challenges
3.6. Views on Health Economics Challenges
3.7. Views on Payment and Model Challenges
3.8. Views on Procedural and Organisational Challenges
3.9. Thematic Analysis of Interviews and the Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Category | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population (P) | Any patient population that is eligible for CGT | Patient population not eligible for CGT |
| Intervention (I) | CGTs | Not CGT |
| Comparators (Cs) | Any | None |
| Outcomes (Os) | Challenges and solutions in CGT market access | Not discussing CGT market access challenges and solutions |
| Study design (S) | Any | None |
| Language | English or Dutch language | Non-English or non-Dutch language |
| Time limit | Published from 2016 to July 2021 1 | Studies published before 2016 |
| Country | Any | None |

| Questions by Category |
| Introduction: We are conducting research on the market access challenges of CGTs in the Netherlands. The lead time for CGT medications is long due to additional challenges, and we hope this research will help streamline and accelerate the market access process. We aim to contribute to the structural access of patients to CGTs through these interviews. We have already identified a number of challenges in the literature, but we would like to identify the key challenges and potential solutions experienced by various parties involved in the Dutch practice through these interviews. We hope this will contribute to a future-proof package management as mentioned by ZIN to keep innovative care high quality, accessible, and affordable in the future. Finally, we would like to discuss possible solutions for the challenges, the transformations needed for this, and what the current state of affairs is. |
| Questions by Category |
| Open Questions |
|
|
|
|
| For the rest of the interview, we have divided the questions into the following topics: clinical CGT research, current state of science and practice, health economics, future-proof package management, funding, and procedures/organization. |
| Clinical Trial Challenges |
| Current clinical CGT studies have a number of shortcomings. |
|
|
|
|
|
| State of Science and Practice |
| CGTs obtain reimbursement through the same process as other therapies (conditional admission process or standard assessment from the sluice) |
|
|
|
|
| Health Economics |
|
|
|
|
|
|
|
| Future-Proof Package Management |
|
|
|
|
| Funding |
| CGTs are associated with high upfront costs. |
|
|
| Various innovative payment models can be used to reduce uncertainties/risk sharing or to spread payment over time. |
|
| What is the current state of affairs regarding the development of payment models that better fit CGT? (this is referred to in the July 2021 letter to parliament about future-oriented package management). |
|
|
|
| Procedural and Organizational Challenges |
|
|
| Closing |
|
|
| Challenges | Clinical Trial | Clinical Evidence—SvWP/Pakketbeheer | Health Economics | Payment Models | Value Assessment | Procedures & Organizational | |
|---|---|---|---|---|---|---|---|
| TLR/ Dutch Stakeholders | |||||||
| Overlapping challenges in TLR and Dutch stakeholders |
|
|
|
|
|
| |
| Additional Dutch challenges derived from interviews |
|
|
|
|
| ||
| Solutions | Clinical Trial | Clinical Evidence—SvWP/Pakketbeheer | Health Economics | Payment Models | Value Assessment | Procedures and Organisational | |
|---|---|---|---|---|---|---|---|
| TLR/ Dutch | |||||||
| Overlapping Proposed Solutions in TLR and Dutch stakeholders |
|
|
|
|
|
| |
| Proposed solution in TLR | - |
|
| ||||
| Additional Dutch proposed solutions |
|
|
|
|
|
| |
References
- ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 3 December 2023).
- Simon Alfano, A.G.; Alberto, L.; Pablo, S. Eight Imperatives for Launching Cell and Gene Therapies. Available online: https://www.mckinsey.com/industries/life-sciences/our-insights/eight-imperatives-for-launching-cell-and-gene-therapies (accessed on 20 January 2024).
- Aballéa, S.; Thokagevistk, K.; Velikanova, R.; Simoens, S.; Annemans, L.; Antonanzas, F.; Auquier, P.; François, C.; Fricke, F.-U.; Malone, D. Health economic evaluation of gene replacement therapies: Methodological issues and recommendations. J. Mark. Access Health Policy 2020, 8, 1822666. [Google Scholar] [CrossRef] [PubMed]
- Marsden, G.; Towse, A. Exploring the Assessment and Appraisal of Regenerative Medicines and Cell Therapy Products: Is the NICE Approach Fit for Purpose. Available online: https://www.ohe.org/publications/exploring-assessment-and-appraisal-regenerative-medicines-and-cell-therapy-products/ (accessed on 1 December 2023).
- Pochopień, M.; Paterak, E.; Clay, E.; Janik, J.; Aballea, S.; Biernikiewicz, M.; Toumi, M. An overview of health technology assessments of gene therapies with the focus on cost-effectiveness models. J. Mark. Access Health Policy 2021, 9, 2002006. [Google Scholar] [CrossRef] [PubMed]
- Pochopień, M.; Qiu, T.; Aballea, S.; Clay, E.; Toumi, M. Considering potential solutions for limitations and challenges in the health economic evaluation of gene therapies. Expert Rev. Pharmacoecon. Outcomes Res. 2021, 21, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- Hettle, R.; Corbett, M.; Hinde, S.; Hodgson, R.; Jones-Diette, J.; Woolacott, N.; Palmer, S. The assessment and appraisal of regenerative medicines and cell therapy products: An exploration of methods for review, economic evaluation and appraisal. Health Technol. Assess. 2017, 21, 1–204. [Google Scholar] [CrossRef] [PubMed]
- Hampson, G.; Towse, A.; Pearson, S.D.; Dreitlein, W.B.; Henshall, C. Gene therapy: Evidence, value and affordability in the US health care system. J. Comp. Eff. Res. 2018, 7, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, B.; Hampson, G.; Michaels, J.; Towse, A.; von der Schulenburg, J.-M.G.; Wong, O. Advanced therapy medicinal products and health technology assessment principles and practices for value-based and sustainable healthcare. Eur. J. Health Econ. 2019, 20, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Neumann, P.J.; Sullivan, S.D.; Fricke, F.-U.; Tunis, S.; Dabbous, O.; Toumi, M. Analytic considerations in applying a general economic evaluation reference case to gene therapy. Value Health 2019, 22, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Angelis, A.; Naci, H.; Hackshaw, A. Recalibrating health technology assessment methods for cell and gene therapies. Pharmacoeconomics 2020, 38, 1297–1308. [Google Scholar] [CrossRef] [PubMed]
- Coyle, D.; Durand-Zaleski, I.; Farrington, J.; Garrison, L.; Graf von der Schulenburg, J.-M.; Greiner, W.; Longworth, L.; Meunier, A.; Moutié, A.-S.; Palmer, S. HTA methodology and value frameworks for evaluation and policy making for cell and gene therapies. Eur. J. Health Econ. 2020, 21, 1421–1437. [Google Scholar] [CrossRef]
- Ten Ham, R.M.; Klungel, O.H.; Leufkens, H.G.; Frederix, G.W. A review of methodological considerations for economic evaluations of gene therapies and their application in literature. Value Health 2020, 23, 1268–1280. [Google Scholar] [CrossRef]
- Simoens, S.; De Groote, K.; Boersma, C. Critical reflections on reimbursement and access of advanced therapies. Front. Pharmacol. 2022, 13, 771966. [Google Scholar] [CrossRef] [PubMed]
- Svensson, M.; Nilsson, F.O.; Arnberg, K. Reimbursement decisions for pharmaceuticals in Sweden: The impact of disease severity and cost effectiveness. Pharmacoeconomics 2015, 33, 1229–1236. [Google Scholar] [CrossRef]
- Principles for Priority Setting in Health Care. Available online: https://www.regjeringen.no/contentassets/439a420e01914a18b21f351143ccc6af/en-gb/pdfs/stm201520160034000engpdfs.pdf (accessed on 23 January 2024).
- Changes We’re Making to Health Technology Evaluation. Available online: https://www.nice.org.uk/Media?Default/About/what-we-do/our-programmes/technology-appraisals/methods-processes-and-topic-selection-review-board-paper-appendix.docx (accessed on 23 January 2024).
- Adapted Value Assessment Methods for High-Impact “Single and Short-Term Therapies” (SSTs). Available online: https://icer.org/wp-content/uploads/2020/10/ICER_SST_FinalAdaptations_111219.pdf (accessed on 27 January 2024).
- Vergoeding Intramurale Geneesmiddelen: De Add-on Prestatie. Available online: http://www.hollandbio.nl/wp-content/uploads/2020/12/infographic-vergoeding-intramurale-geneesmiddelen_final.pdf (accessed on 11 June 2023).
- Vergoeding Intramurale Geneesmiddelen: Van EMA Registratie Tot Add-on. Available online: https://www.hollandbio.nl/wp-content/uploads/2023/02/infographic-vergoeding-intramurale-geneesmiddelen_versie-jan-2023.pdf (accessed on 10 June 2024).
- Ward, L.M.; Chambers, A.; Mechichi, E.; Wong-Rieger, D.; Campbell, C. An international comparative analysis of public reimbursement of orphan drugs in Canadian provinces compared to European countries. Orphanet J. Rare Dis. 2022, 17, 113. [Google Scholar] [CrossRef] [PubMed]
- Kuipers, E. Wijziging Beleidsregels voor de Toepassing van de Sluis voor dure Geneesmiddelen op Grond van Artikel 2.4a van het Besluit Zorgverzekering. 24 January 2023. Available online: https://open.overheid.nl/documenten/ronl-a04e9c698c6915588ffed5b381e5f2b7097c4bc6/pdf (accessed on 20 July 2023).
- Sluis Voor Dure Geneesmiddelen. Available online: https://www.zorginstituutnederland.nl/over-ons/programmas-en-samenwerkingsverbanden/horizonscan-geneesmiddelen/sluis-voor-dure-geneesmiddelen (accessed on 26 July 2023).
- Pakketadvies Sluisgeneesmiddel Ciltacabtagene Autoleucel (Carvykti®) Voor de Behandeling van Multipel Myeloom. Available online: https://www.zorginstituutnederland.nl/over-ons/publicaties/adviezen/2022/10/20/pakketadvies-sluisgeneesmiddel-ciltacabtagene-autoleucel-carvykti (accessed on 26 July 2023).
- Bluebird Bio Reports Second Quarter Financial Results and Provides Operational Update. Available online: https://investor.bluebirdbio.com/news-releases/news-release-details/bluebird-bio-reports-second-quarter-financial-results-and (accessed on 26 July 2023).
- Pakketadvies Sluisgeneesmiddel Atidarsagene Autotemcel (Libmeldy®) Voor de Behandeling van Metachromatische Leukodystrofie (MLD). Available online: https://www.zorginstituutnederland.nl/over-ons/publicaties/adviezen/2022/09/27/pakketadvies-sluisgeneesmiddel-atidarsagene-autotemcel-libmeldy (accessed on 26 May 2024).
- Paré, G.; Kitsiou, S. Methods for literature reviews. In Handbook of ehealth Evaluation: An Evidence-Based Approach; Lau, F., Kuziemsky, C., Eds.; University of Victoria: Victoria, BC, Canada, 2017. [Google Scholar]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef]
- Landfeldt, E. Gene therapy for neuromuscular diseases: Health economic challenges and future perspectives. J. Neuromuscul. Dis. 2022, 9, 675–688. [Google Scholar] [CrossRef] [PubMed]
- Qiu, T.; Pochopien, M.; Liang, S.; Saal, G.; Paterak, E.; Janik, J.; Toumi, M. Gene therapy evidence generation and economic analysis: Pragmatic considerations to facilitate fit-for-purpose health technology assessment. Front. Public Health 2022, 10, 773629. [Google Scholar] [CrossRef]
- Garrison, L.P.; Pezalla, E.; Towse, A.; Yang, H.; Faust, E.; Wu, E.Q.; Li, N.; Sawyer, E.K.; Recht, M. Hemophilia gene therapy value assessment: Methodological challenges and recommendations. Value Health 2021, 24, 1628–1633. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, J.; Neumann, P.J.; Council, I.H.A.S. Health technology assessment for gene therapies in haemophilia. Haemophilia 2022, 28, 19–26. [Google Scholar] [CrossRef]
- de Labry-Lima, A.O.; Ponce-Polo, A.; García-Mochón, L.; Ortega-Ortega, M.; Pérez-Troncoso, D.; Epstein, D. Challenges for economic evaluations of advanced therapy medicinal products: A systematic review. Value Health 2023, 26, 138–150. [Google Scholar] [CrossRef]
- Sabatini, M.T.; Xia, T.; Chalmers, M. Pricing and market access challenges in the era of one-time administration cell and gene therapies. Pharm. Med. 2022, 36, 265–274. [Google Scholar] [CrossRef]
- Fornaro, G.; Drummond, M.; Ciani, O.; Jommi, C. P48 Are Health Technology Assessment (HTA) Bodies Responding to the Assessment Challenges Posed By Cell and Gene Therapies? Value Health 2022, 25, S297. [Google Scholar] [CrossRef]
- Toumi, M.; Dabbous, O.; Aballéa, S.; Drummond, M.F.; von der Schulenburg, J.-M.G.; Malone, D.C.; Neumann, P.J.; Sullivan, S.D.; Tunis, S. Recommendations for economic evaluations of cell and gene therapies: A systematic literature review with critical appraisal. Expert Rev. Pharmacoecon. Outcomes Res. 2023, 23, 483–497. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velikanova, R.; Wolters, S.; Hofstra, H.S.; Postma, M.J.; Boersma, C. Market Access Challenges and Solutions in Cell and Gene Therapy in The Netherlands. J. Mark. Access Health Policy 2024, 12, 181-198. https://doi.org/10.3390/jmahp12030015
Velikanova R, Wolters S, Hofstra HS, Postma MJ, Boersma C. Market Access Challenges and Solutions in Cell and Gene Therapy in The Netherlands. Journal of Market Access & Health Policy. 2024; 12(3):181-198. https://doi.org/10.3390/jmahp12030015
Chicago/Turabian StyleVelikanova, Rimma, Sharon Wolters, Hinko S. Hofstra, Maarten J. Postma, and Cornelis Boersma. 2024. "Market Access Challenges and Solutions in Cell and Gene Therapy in The Netherlands" Journal of Market Access & Health Policy 12, no. 3: 181-198. https://doi.org/10.3390/jmahp12030015
APA StyleVelikanova, R., Wolters, S., Hofstra, H. S., Postma, M. J., & Boersma, C. (2024). Market Access Challenges and Solutions in Cell and Gene Therapy in The Netherlands. Journal of Market Access & Health Policy, 12(3), 181-198. https://doi.org/10.3390/jmahp12030015