Knowledge Representation for Prognosis of Health Status in Rehabilitation

Abstract
:1. Introduction
- • to present an application in the rehabilitation domain, in particular, a CDSS for the prognosis of health status of chronic patients who suffer from neurological diseases in the extra-hospital stage;
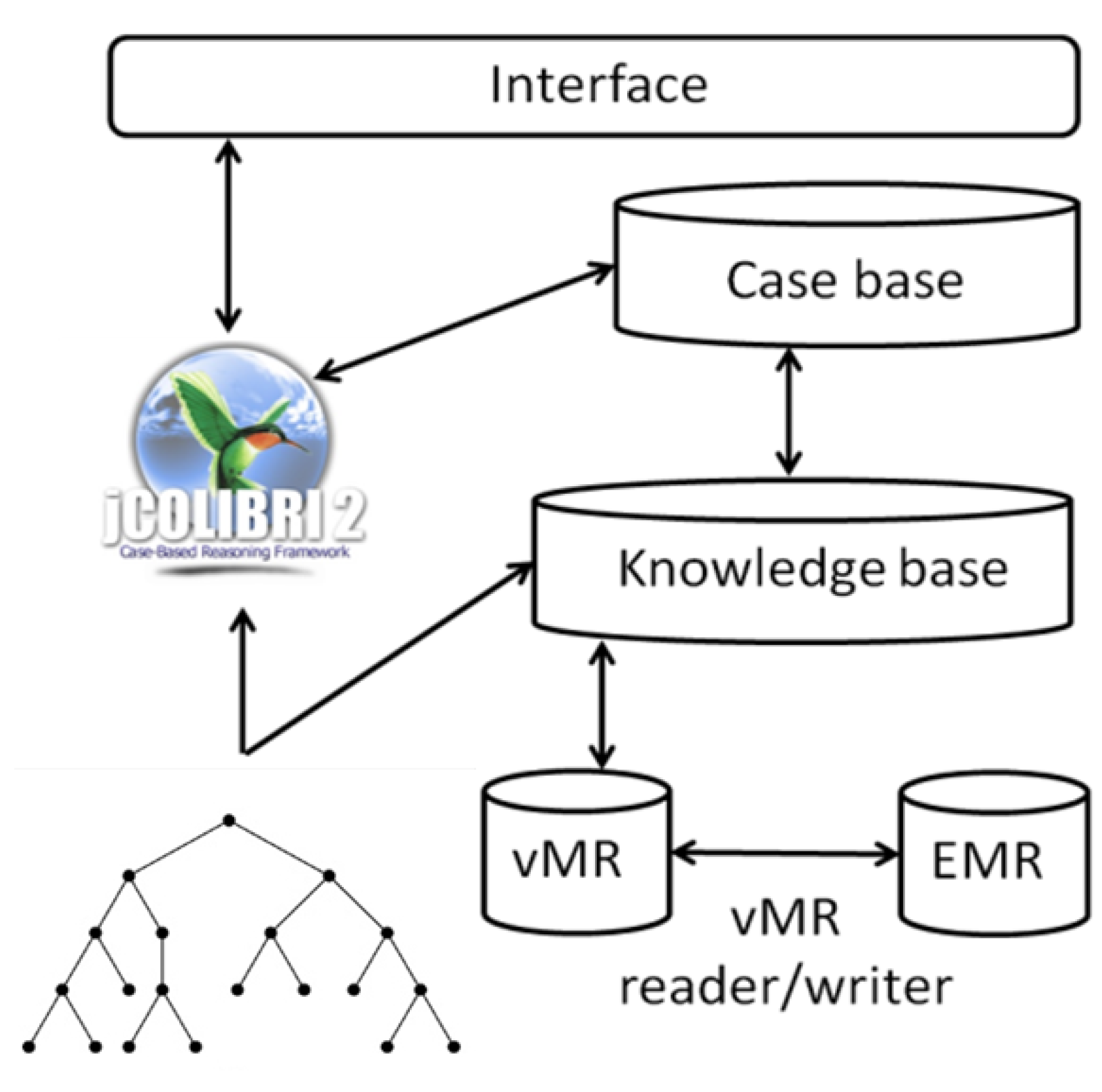
- • to describe how the ICF, ICD-10, SNOMED CT and vMR can be used to build interoperable CDSSs;
- • to show the pros and cons of representations methods of cases; and
- • to explain how the ICF and ICD-10 are used in similarity measures of functioning status and diversity.
2. Results and Discussion
2.1. Characterization of CDSS in Rehabilitation
2.2. Use of Information Models, Classifications and Terminologies in Rehabilitation
2.3. Representation of Cases
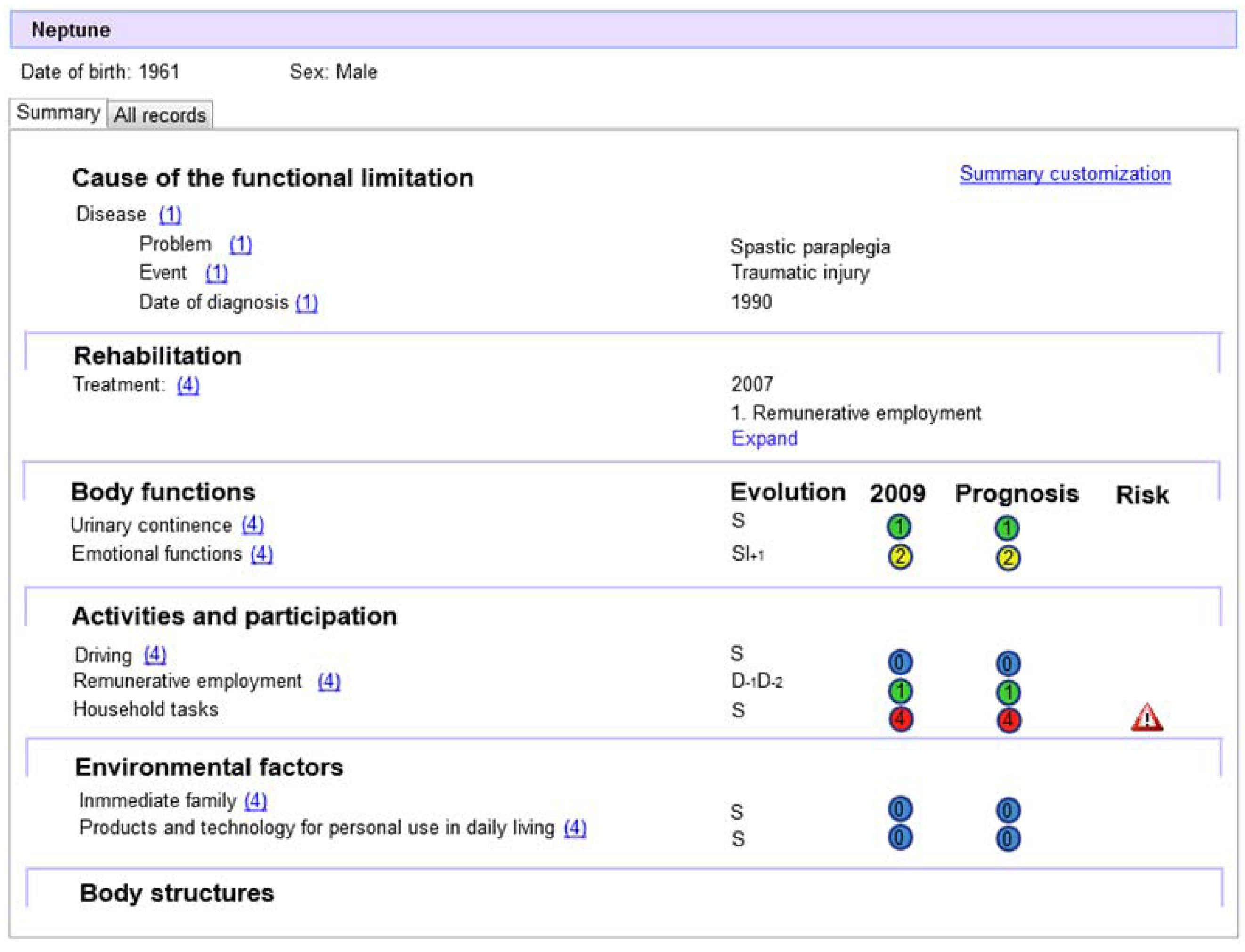
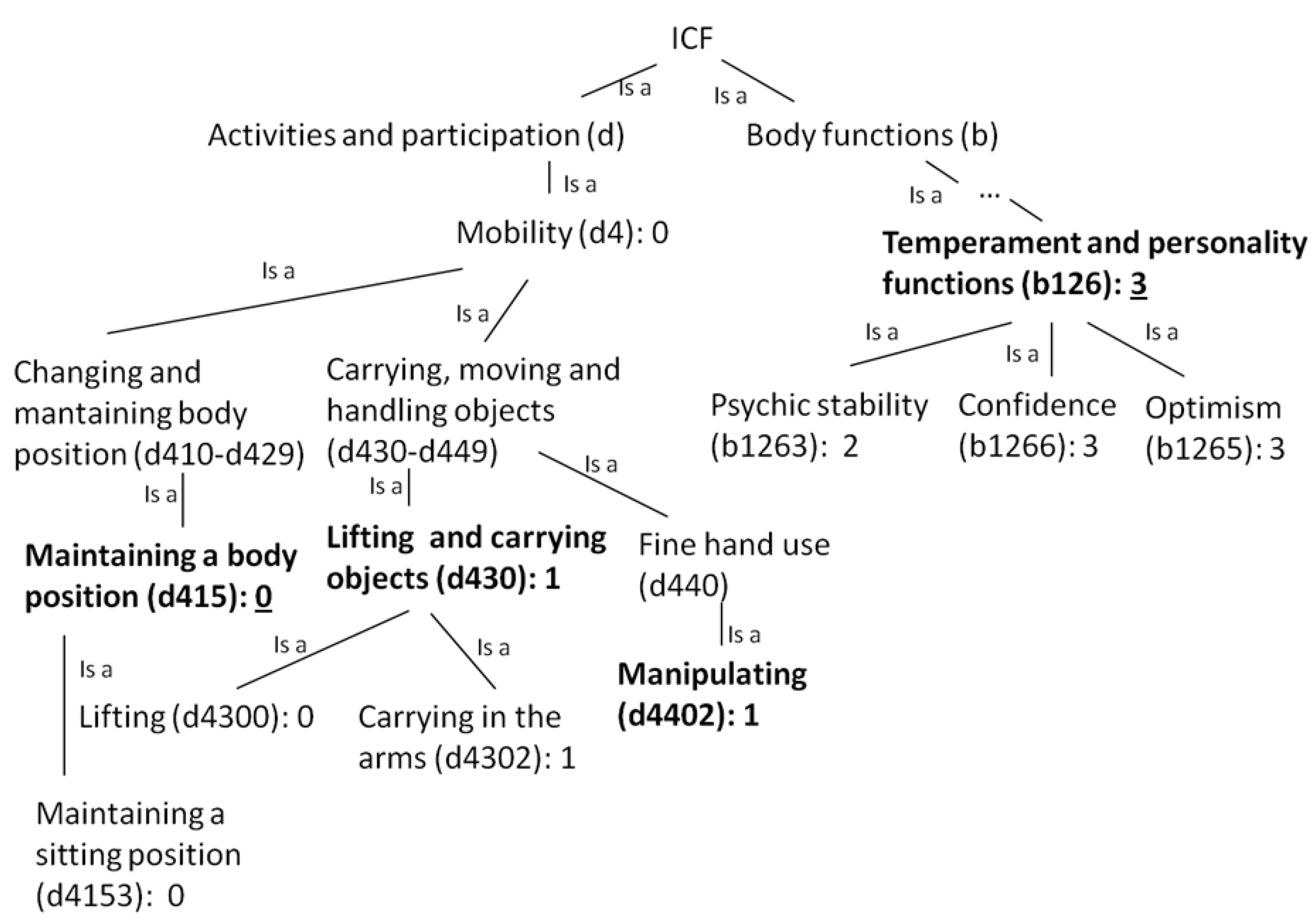
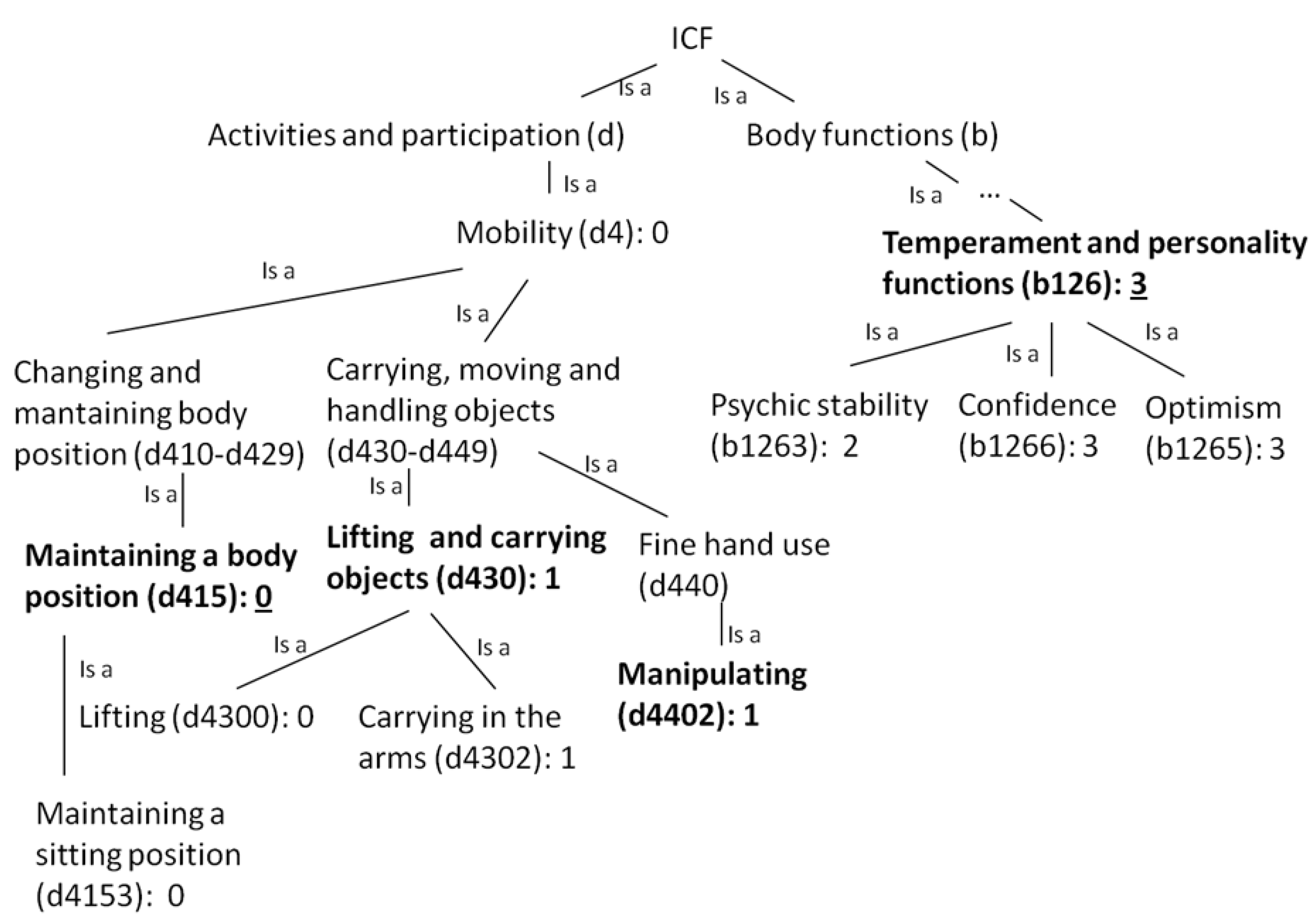
2.3.1. Point-based Representation

- • red/4: complete problem, difficulty, deficiency or environmental factors: 96%–100%;
- • orange/3: severe problem, difficulty, deficiency or environmental factors: 50%–95%;
- • yellow/2: moderate problem, difficulty, deficiency or environmental factors: 25%–49%;
- • green/1: mild problem, difficulty, deficiency or environmental factors: 5%–24%;
- • blue/0: no problem, difficulty, deficiency or environmental factors: 0%–4%.
2.3.2. Series-based Representation
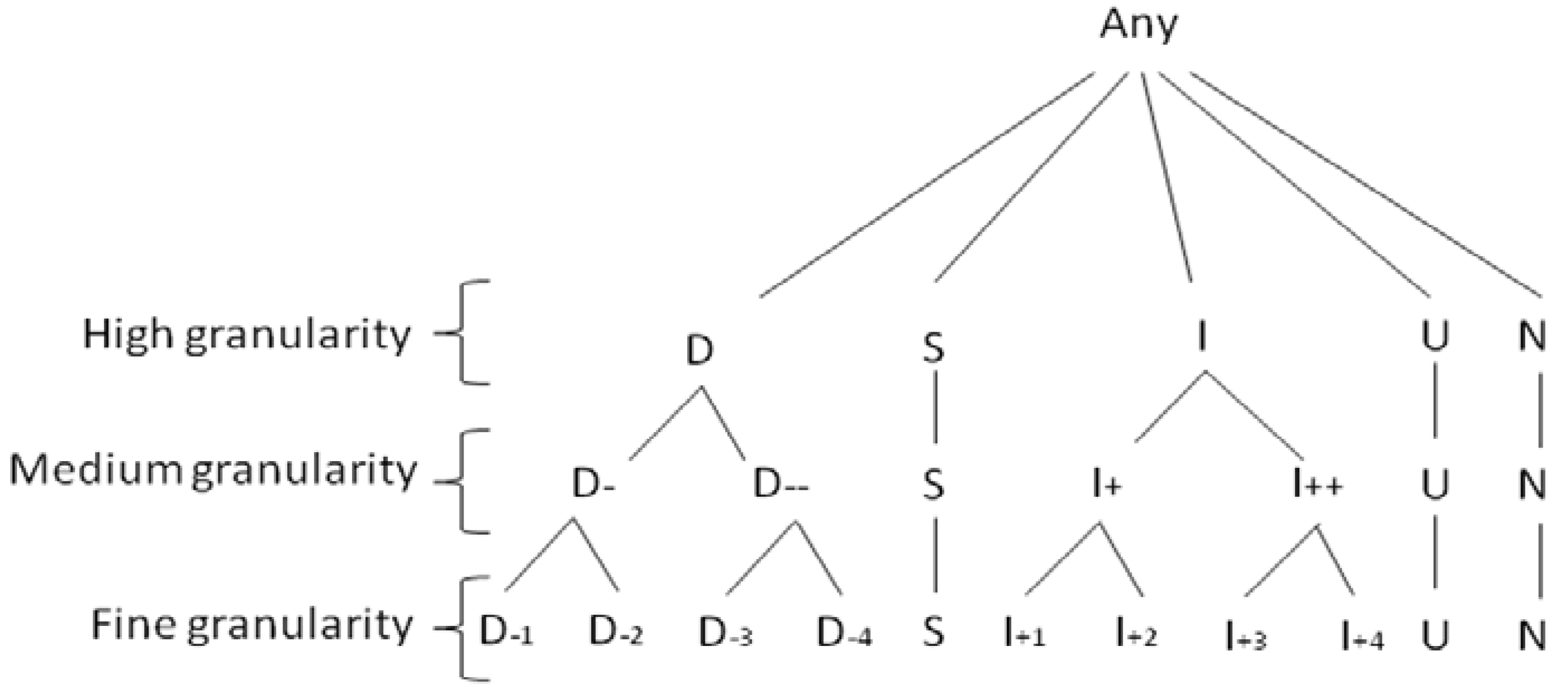
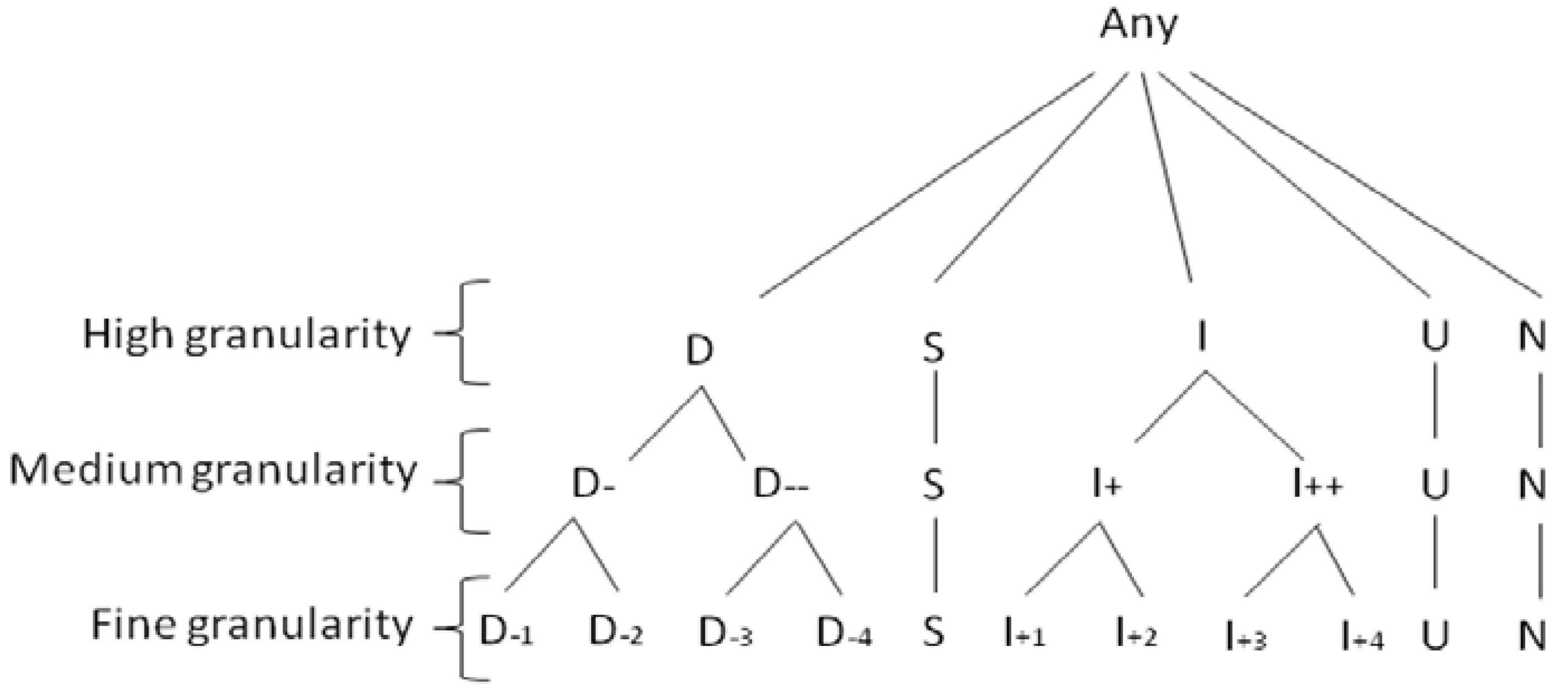
- • fine granularity, which contains all possible changes in ICF values: D−n means decreasing n levels; I+n means increasing n levels; and S means remaining stationary;
- • coarse granularity, which summarizes changes as decreasing (D), stationary (S) and increasing (I); and
- • medium granularity, which is an intermediate representation between coarse and fine granularity.
2.4. Patients’ Similarity Measure
 (2), in which X and Y are two patients, Sim(Xi,Yi) is the similarity on the ith attribute with weight wi. ICF core sets and ICF taxonomy are used for weight assignment. The weight given to level-4 and level-3 core set categories is 2 and 1, respectively. Therefore core set categories which are more specific in the ICF taxonomy (level 4 core set categories) carry more weight in the similarity calculation.
(2), in which X and Y are two patients, Sim(Xi,Yi) is the similarity on the ith attribute with weight wi. ICF core sets and ICF taxonomy are used for weight assignment. The weight given to level-4 and level-3 core set categories is 2 and 1, respectively. Therefore core set categories which are more specific in the ICF taxonomy (level 4 core set categories) carry more weight in the similarity calculation.- • Disease terms are not encoded to a single ICD-10 category. In this case, the most representative ICD-10 category is chosen.
- • Disease terms are encoded to the same ICD-10 category. In this case, both concepts cannot be distinguished if ICD-10 is not extended.
- • ICD-10 contains catch-all categories. In this case, only categories that cannot be encoded to an ICD-10 category are encoded to “Other disease of type X”.
- • ICD-10 contains scattered exclusions. In this case, the most representative ICD-10 category is chosen.
- • Diseases terms are complications of other diseases. In this case, the most representative ICD-10 category is chosen.

3. Experimental Section
3.1. Physical Rehabilitation Scenario
3.2. Use of Information Models, Classifications and Terminologies in Rehabilitation
- • functioning data, using the functional independence measure (FIM) and the spinal cord injury measure (SCIM);
- • emotional status and well-being, using the hospital anxiety and depression (HAD) questionnaire and the psychological well-being index (PWBI);
- • quality of life, using the short version of the world health organization quality of life assessment instrument (WHOQOL-BREF).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| vMR Class: attribute | Standard classification class | EMR reference |
|---|---|---|
| Person: name | Patient name | Patient’s static information |
| EvaluatedPerson (subclass of Person): birthTime, gender | Date of birth, gender | |
| Problem: problemCode | ICD-10 | |
| ProblemBase (subclass of Problem): diagnosticEventTime, severity | Date of diagnosis, severity score | |
| AdverseEventBase: adverseEventcode | Event | |
| GoalBase: goalFocus, goalAchievementTarget Time | Therapy, timing milestone | SDQ |
| ObservationBase: observationFocus | ICF | FIM, SCIM, HAD, PWBI, WHOQOL-BREF |
3.3. Use of Diseases to Measure Patients’ Similarity
- • Diseases not encoded to a single ICD-10 category. Myopathy is encoded as primary disorders of muscles (G71), other myopathies (G72) and disorders of muscles (M60-M63) and, if no additional information is available, the first option is chosen as it is the most representative according to an experts’ consensus.
- • Diseases encoded to the same ICD-10 category. Both complete paraplegia and incomplete paraplegia are encoded as spastic paraplegia (G82.1), therefore their similarity is considered equal to 1.
- • Diseases encoded to catch-all ICD-10 categories. Other ischemic stroke is encoded as other cerebral infarction (I63.8).
- • Diseases encoded to ICD-10 categories with scattered exclusions. In this case, if no additional information is available, the most representative ICD-10 category is chosen according to an experts’ consensus. For example, for paraplegia various categories exist which include the concept, such as hereditary spastic paraplegia (G11.4), but the spastic paraplegia (G82.1) category is chosen for being more representative.
- • Diseases that may occur as a complication in the course of some other disease. This problem has not been studied in the scenario.
3.4. Case Representation Methods
| Person, year\recommendations | Environmental factors | Activities and participation | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Immediate family | General social support services | Acquiring a place to live | Driving | Using transportation | Informal education | Pubic economic entitlement | Sports | Preparing meals | Crafts | Remunerative employment | |
| Neptune, 2006 | 0 | 8 | 0 | 0 | 8 | 2 | 0 | 4 | 4 | 4 | 4 |
| Neptune, 2007 | 0 | 8 | 0 | 0 | 8 | 2 | 0 | 4 | 4 | 4 | 3 |
| Neptune, 2009 | 0 | 8 | 0 | 0 | 8 | 2 | 0 | 4 | 4 | 4 | 1 |
| Neptune, 2010 | 0 | 8 | 0 | 0 | 8 | 3 | 0 | 4 | 4 | 4 | 1 |
| Symbol granularity | Recommendations\person | Neptune | Diana | Juno | Apollo | Venus | Minerva |
|---|---|---|---|---|---|---|---|
| Fine | Using transportation | M | M | SS | M | M | M |
| Driving | SSS | SSS | M | S | S | S | |
| Acquiring a place to live | SSS | SSS | SS | SSS | S | S | |
| Preparing meals | SS | SS | S | SS | I+4 | I+4 | |
| Informal education | SSI+1 | SSS | SS | I+1SS | S | S | |
| Remunerative employment | D−1D-2S | SSD−1 | I+1I+2 | I+1D−1S | S | S | |
| Public economic entitlement | SSS | SSS | SD-4 | SSS | S | S | |
| Sports | SSS | D−4SS | SS | I+4D−4S | S | S | |
| Crafts | SSS | SSS | SS | SD−4I+4 | S | S | |
| Immediate family | SSS | M | SS | SSS | S | S | |
| General social support services | M | M | SI+1 | M | M | M | |
| Medium | Preparing meals | S | S | S | S | I++ | I++ |
| Remunerative employment | D-S | SD- | I+ | I+D−S | S | S | |
| General social support services | M | M | SI+ | M | M | M | |
| Coarse | Preparing meals | S | S | S | S | I | I |
| Remunerative employment | DS | SD | I | IDS | S | S | |
| General social support services | M | M | SI | M | M | M |
| Recommendations/person | Neptune | Vesta | Diana | Ceres | Mars |
|---|---|---|---|---|---|
| Preparing meals | 4 > S | 0>S | 0 > S | 4 > S > D−4 | 4 > S |
| Remunerative employment | 4 > D−1 > D−2>S | 4 > S >D−1 | 4 > S > D−1 | 3 > S | 4 > S |
| General social support services | 8 | 8 | 0 | 1 > S > D−1 | 1 > S |
3.5. Limitations
4. Conclusions
Acknowledgments
References
- Carter, J.H. Design and Implementation Issues. In Clinical Decision Support Systems; Berner, E.S., Hannah, K.J., Ball, M., Eds.; Springer: New York, NY, USA, 2007; pp. 64–98, Section 1. [Google Scholar]
- College of American Pathologists and National Health Service. Systematized Nomenclature of Medicine—Clinical Terms (SNOMED CT). Available online: http://purl.bioontology.org/ontology/SNOMEDCT (accessed on 31 July 2012).
- World Health Organization. International Classification of Diseases (ICD-10). Available online: https://dkm.fbk.eu/index.php/ICD-10_Ontology (accessed on 30 July 2012).
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). Available online: http://purl.bioontology.org/ontology/ICF (accessed on 31 July 2012).
- Steiner, W.A.; Ryser, L.; Huber, E.; Uebelhart, D.; Aeschlimann, A.; Stucki, G. Use of the ICF model as a clinical problem-solving tool in physical therapy and rehabilitation medicine. J. Phys. Ther. 2002, 11, 1098–1107. [Google Scholar]
- Keravnou, E.; Shahar, Y. Temporal Reasoning in Medicine. In Handbook of Temporal Reasoning in Artificial Intelligence; Fisher, M.D., Gabbay, D.M., Vila, L., Eds.; Elsevier: Amsterdam, The Netherlands, 2005; pp. 587–653. [Google Scholar]
- Ding, H.; Trajcevski, G.; Scheuermann, P.; Wang, X.; Keogh, E. Querying and mining of time series data: Experimental comparison of representations and distance measures. Available online: http://www.vldb.org/pvldb/1/1454226.pdf (accessed on 14 August 2012).
- Romañach, J.; Lobato, M. Functional diversity, a new term in the struggle for dignity in the diversity of the human being. Available online: http://www.leeds.ac.uk/disability-studies/archiveuk/zavier/Functional%20Diversity%20%20%20%20%20%20%20%20%20%20_fv%20Roma%F1ach.pdf (accessed on 14 August 2012).
- Aamodt, A.; Plaza, E. Case-based reasoning: Foundational issues, methodological variations, and system approaches. J. AI Commun. 1994, 7, 39–59. [Google Scholar]
- VMR Project Team. Virtual Medical Record (vMR) for Clinical Decision Support—Domain Analysis Model 2011. Available online: http://wiki.hl7.org/index.php?title=Virtual_Medical_Record_(vMR) (accessed on 31 July 2012).
- Kashfi, H. The Intersection of Clinical Decision Support and Electronic Health Record: A Literature Review. In Proceedings of the Federated Conference on Computer Science and Information System, Szczecin, Poland, 18–21 September 2011; pp. 347–353.
- Martínez-Costa, C.; Menárguez-Tortosa, M.; Fernández-Breis, J.T. An approach for the semantic interoperability of ISO/EN 13606 and openEHR archetypes. J. Biomed. Informa. 2010, 43, 736–746. [Google Scholar] [CrossRef]
- Cieza, A.; Geyh, S.; Chatterji, S.; Konstanjsek, N. ICF linking rules: An update based on lessons learned. J. Rehabil. Med. 2005, 37, 212–218. [Google Scholar] [CrossRef]
- Ceccaroni, L.; Subirats, L. Interoperable knowledge representation in clinical decision support systems for rehabilitation. J. Appl. Comput. Math. 2012, 11, 303–316. [Google Scholar]
- Recio-Garcia, J.A.; Díaz-Agudo, B.; Gonález-Calero, P. jColibri2 Tutorial.; Universidad Complutense de Madrid: Madrid, Spain, 2008. [Google Scholar]
- Ceusters, W.; Steurs, F.; Zanstra, P.; van der Haring, E.; Rogers, J. From a time standard for medical informatics to a controlled language for health. J. Med. Inf. 1998, 48, 85–101. [Google Scholar]
- Coenen, M. Developing a method to validate the WHO ICF Core Sets from a patient perspective: Rheumatoid arthritis as a case point. Ph.D. Thesis, Ludwig-Maximilians-Universität, München, Germany, January 2008. [Google Scholar]
- Herrmann, K.H.; Kirchberger, I.; Stucki, G.; Cieza, A. The comprehensive ICF core sets for spinal cord injury from the perspective of occupational therapists: A worldwide validation study using the Delphi technique. J. Spinal Cord. 2011, 49, 600–613. [Google Scholar] [CrossRef]
- Centers for Medicare and Medicaid Services (CMS) and the National Center for Health and Statistics (NCHS). ICD-10-CM Official Guidelines for Coding and Reporting 2012. Available online: http://www.cdc.gov/nchs/data/icd10/10cmguidelines2012.pdf (accessed on 31 July 2012).
- Gibert, K.; García-Rudolph, A.; Curcoll, L.; Soler, D.; Pla, L.; Tormos, J.M. Knowledge Discovery about Quality of Life Changes of Spinal Cord Injury Patients: Clustering based on Rules by States. In Proceedings of the International Conference of the European Federation for Medical Informatics (MIE), Sarajevo, Bosnia and Herzegovina, 30 August–2 September 2009; pp. 579–583.
- Subirats, L.; Orte, S.; López, R.; Torrellas, S.; García-Rudolph, A.; Ceccaroni, L.; Gil, A.; Miralles, F.; Tormos, J.M. Use of Bio-psycho-social Standards and User Experience in a Social Network Which is Focused on People with Neurological Disability. In Proceedings of the International Congress on DesignResearch Networks and Technology for All (DRT4ALL), Madrid, Spain, 27–29 June 2011; pp. 314–330.
- Pesquita, C.; Faria, D.; Falcão, A.O.; Lord, P.; Couto, F.M. Semantic similarity in biomedical ontologies. PLoS Comput. Biol. 2009, 5. [Google Scholar] [CrossRef]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Subirats, L.; Ceccaroni, L.; Miralles, F. Knowledge Representation for Prognosis of Health Status in Rehabilitation. Future Internet 2012, 4, 762-775. https://doi.org/10.3390/fi4030762
Subirats L, Ceccaroni L, Miralles F. Knowledge Representation for Prognosis of Health Status in Rehabilitation. Future Internet. 2012; 4(3):762-775. https://doi.org/10.3390/fi4030762
Chicago/Turabian StyleSubirats, Laia, Luigi Ceccaroni, and Felip Miralles. 2012. "Knowledge Representation for Prognosis of Health Status in Rehabilitation" Future Internet 4, no. 3: 762-775. https://doi.org/10.3390/fi4030762
APA StyleSubirats, L., Ceccaroni, L., & Miralles, F. (2012). Knowledge Representation for Prognosis of Health Status in Rehabilitation. Future Internet, 4(3), 762-775. https://doi.org/10.3390/fi4030762