
68Ga Extemporaneous Preparations in Radiopharmacy

 ,
,  ,
,  and
and 
Abstract

1. Introduction
2. 68Ga in Nuclear Medicine
2.1. Chemical and Physical Properties of 68Ga
2.2. Production of 68Ga
2.3. 68Ga Chelators
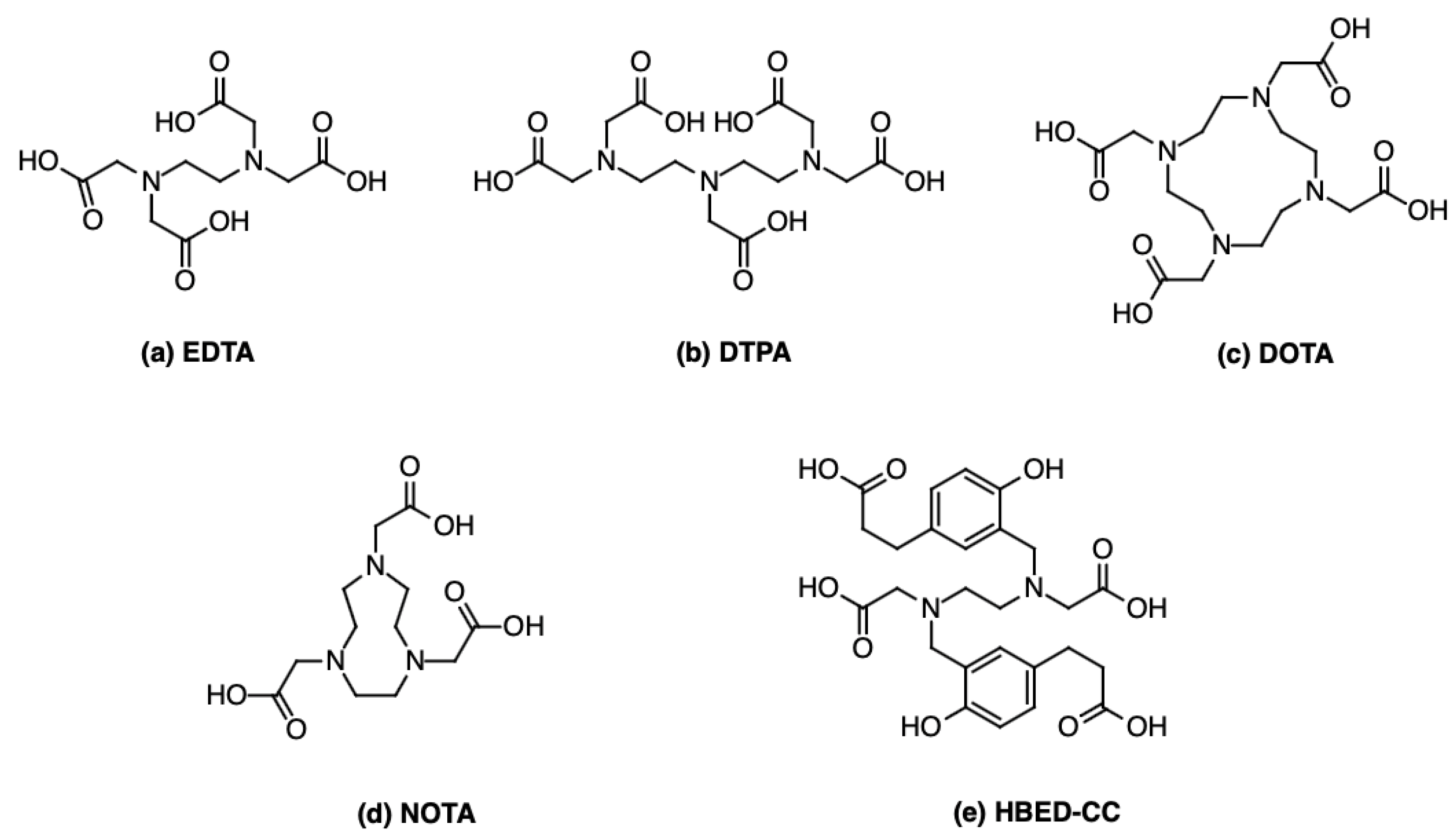
- DOTA (1,4,7,10-Tetraazacyclododecane-1,4,7,10-tetraacetic acid, Figure 4c), which forms exceptionally stable 68Ga complexes in vivo, preventing dissociation or transmetallation under physiological conditions [32]. For instance, the study performed by Oehlke and colleagues analysed the stability of [68Ga]Ga-DOTATATE towards transmetallation with Cu2+, Fe3+, Pb2+, and Zn2+, and found that only the addition of Cu2+ at 95 °C leads to noticeable transmetallation [33].DOTA radiolabelling requires high temperatures (~90 °C) for approximately 10 min. This heating step is crucial, due the rigidity of its macrocyclic structure, which must undergo conformational rearrangement to accommodate the Ga3+ ion within its coordination cavity [30]. The ideal pH range for DOTA chelation is 3.5–4.0. At lower pH, DOTA becomes overly protonated, while at higher pH, Ga3+ may form insoluble species [34]. Structurally, DOTA provides an octadentate N4O4 coordination environment and a relatively large macrocyclic cavity that may lead to slower complexation kinetics and reduced resistance to transchelation due to imperfect fitting with the ionic radius of Ga3+ [35].
- NOTA (1,4,7-Triazacyclononane-1,4,7-triacetic acid), which forms highly stable complexes at room temperature [30]. This property is attributed to the intrinsic structural features of NOTA (Figure 4d): its compact macrocyclic geometry, hexadentate N3O3 coordination, and smaller cavity size, which better matches the ionic radius of Ga3+, facilitating faster complex formation and superior kinetic stability [36]. Ga3+-NOTA complexes exhibit an exceptionally high stability constant (logK = 30.98), significantly higher than that of Ga³⁺-DOTA (logK = 21.33), highlighting NOTA’s stronger affinity for Ga3+ and more favourable thermodynamics [32]. Structurally, NOTA forms slightly distorted octahedral complexes with facially arranged donors, allowing the formation of multiple five-membered chelate rings with minimal strain, unlike DOTA. This lower energetic barrier enables efficient complexation even at mild conditions [37]. In terms of in vivo stability, although NOTA forms more inert complexes with Ga3+ than DOTA, the overall biological performance of the radiopharmaceutical also depends on the charge, hydrophilicity, and pharmacokinetics of the resulting bioconjugate. For example, DOTA-based vectors may display more favourable biodistribution in certain contexts, despite their lower thermodynamic stability [32]. Similarly to DOTA, NOTA has shown strong resistance to transmetallation, particularly against biologically relevant cations such as Zn2+ and Ca2+; additionally [33]. NOTA, provides enhanced kinetic inertness even under physiological conditions [32,38].
2.4. Conditions of 68Ga Complexation
3. Regulatory Guidelines of 68Ga Radiopharmaceuticals
3.1. Regulatory Guidelines and Radiation Protection Regulations
- Industrial-scale ready-to-use radiopharmaceuticals, produced under full GMP and subject to centralised marketing authorisation procedures;
- Radiopharmaceutical precursors, manufactured under GMP and intended for subsequent radiolabelling in healthcare facilities;
- Small-scale extemporaneous radiopharmaceutical preparations, compounded within hospital or academic radiopharmacy settings under national exemptions and pharmacopoeial standards [47].
3.2. European Pharmacopoeia
3.3. Good Manufacturing Practice Guidelines
- Part I, Basic Requirements for Medicinal Products, outlines the GMP standards applicable to the manufacture and control of finished pharmaceutical products for both human and veterinary use. It is organised into nine chapters: Chapter 1 defines the Pharmaceutical Quality System necessary to consistently produce medicines that meet regulatory and patient expectations; Chapter 2 specifies the responsibilities, qualifications, and training requirements for personnel involved in GMP activities; Chapter 3 outlines the design, maintenance, and control standards for premises and equipment; Chapter 4 addresses documentation management, including procedures, records, and batch documentation; Chapter 5 describes principles for production operations, contamination control, and process validation; Chapter 6 establishes the requirements for sampling, testing, release, and stability studies; Chapter 7 regulates the management of outsourced activities; Chapter 8 defines procedures for handling complaints, investigating quality defects, and executing product recalls; and Chapter 9 covers the requirements for self-inspections to ensure ongoing GMP compliance.
- Part II, Basic Requirements for Active Substances used as Starting Materials, defines the GMP framework for the production of active pharmaceutical ingredients (APIs), focusing on quality, purity, and traceability throughout the manufacturing process.
- Part III, GMP-related Documents, compiles complementary guidelines, such as ICH Q9 on Quality Risk Management and ICH Q10 on Pharmaceutical Quality Systems, which extend and reinforce the broader quality framework necessary for maintaining GMP compliance.
3.4. International Council for Harmonisation Guidelines
- Modifications in the radiopharmaceutical preparation process that may introduce new or different impurities not previously considered, such as a change in purification strategy or the use of an alternative precursor;
- Alterations in the final product composition, including increased radioactivity levels or the introduction of different excipients;
- Substantial adjustments to the analytical procedure itself, for instance, the replacement of the HPLC column with one featuring a different stationary phase, or major changes to the mobile phase composition [69].
4. Overview of Main 68Ga Tracers Extemporaneously Prepared
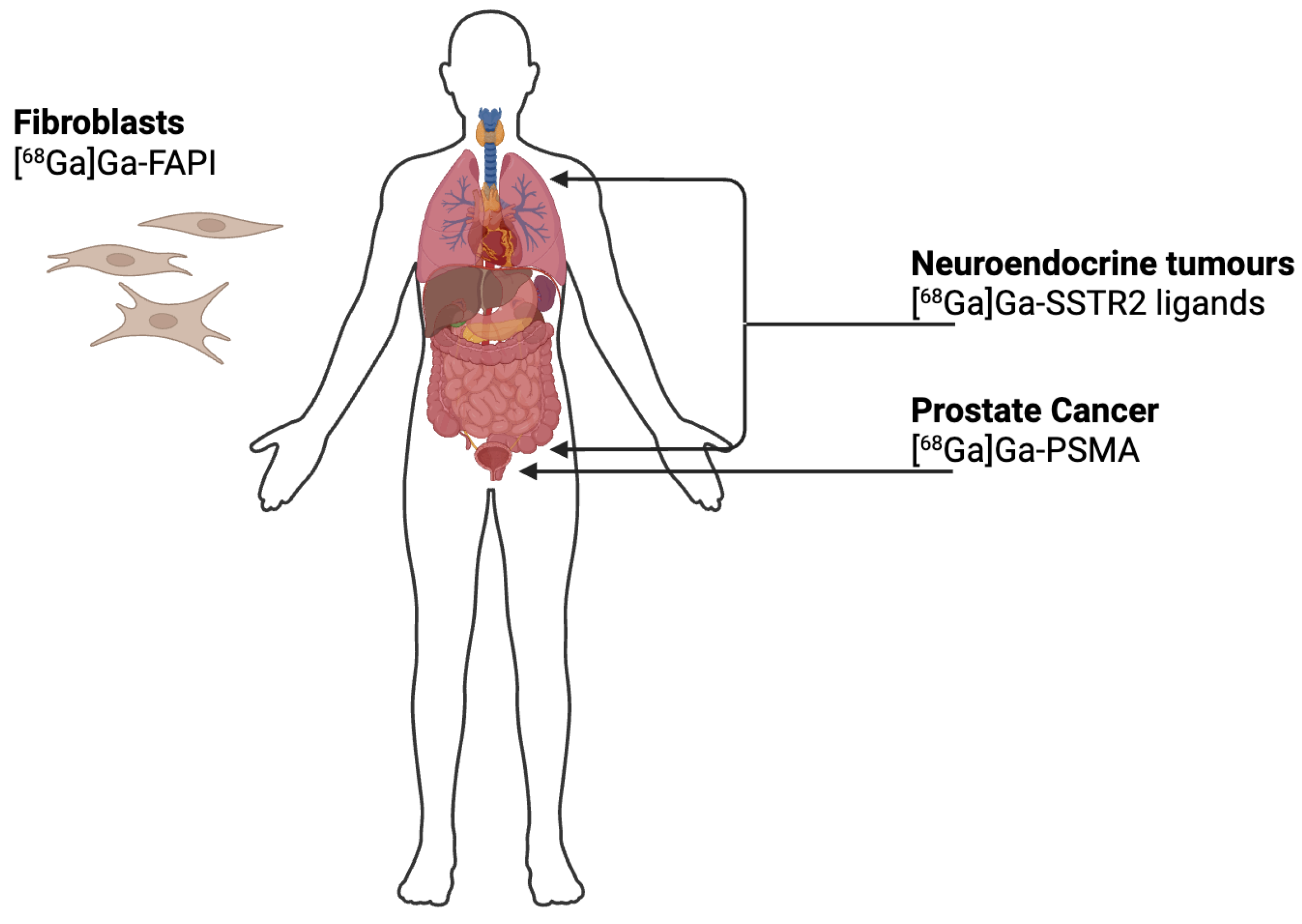
4.1. PSMA Tracers
4.2. DOTATOC and Somatostatin Receptor Tracers
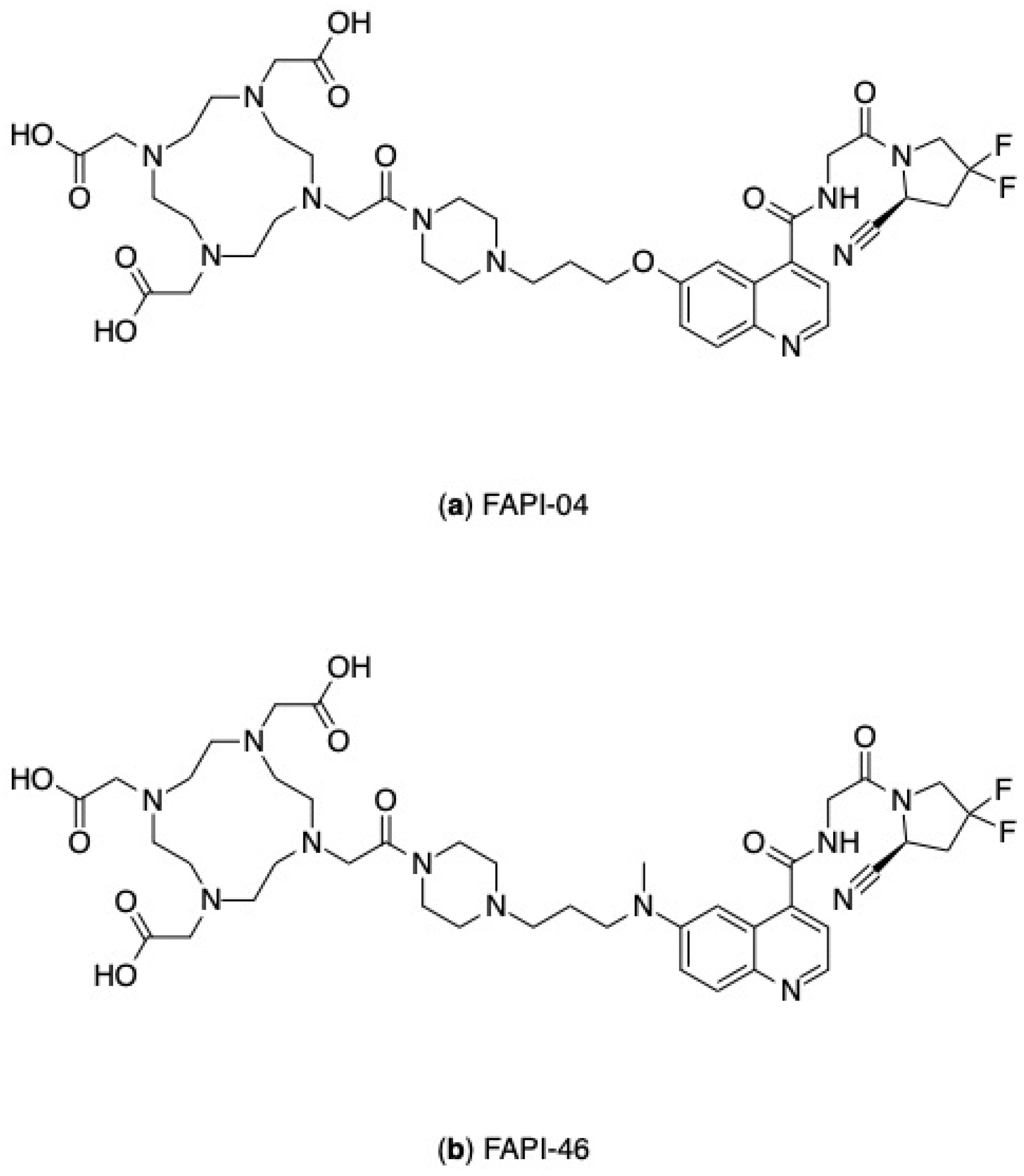
4.3. FAPI Tracers
5. Extemporaneous Formulations and Quality Control of 68Ga Radiopharmaceuticals
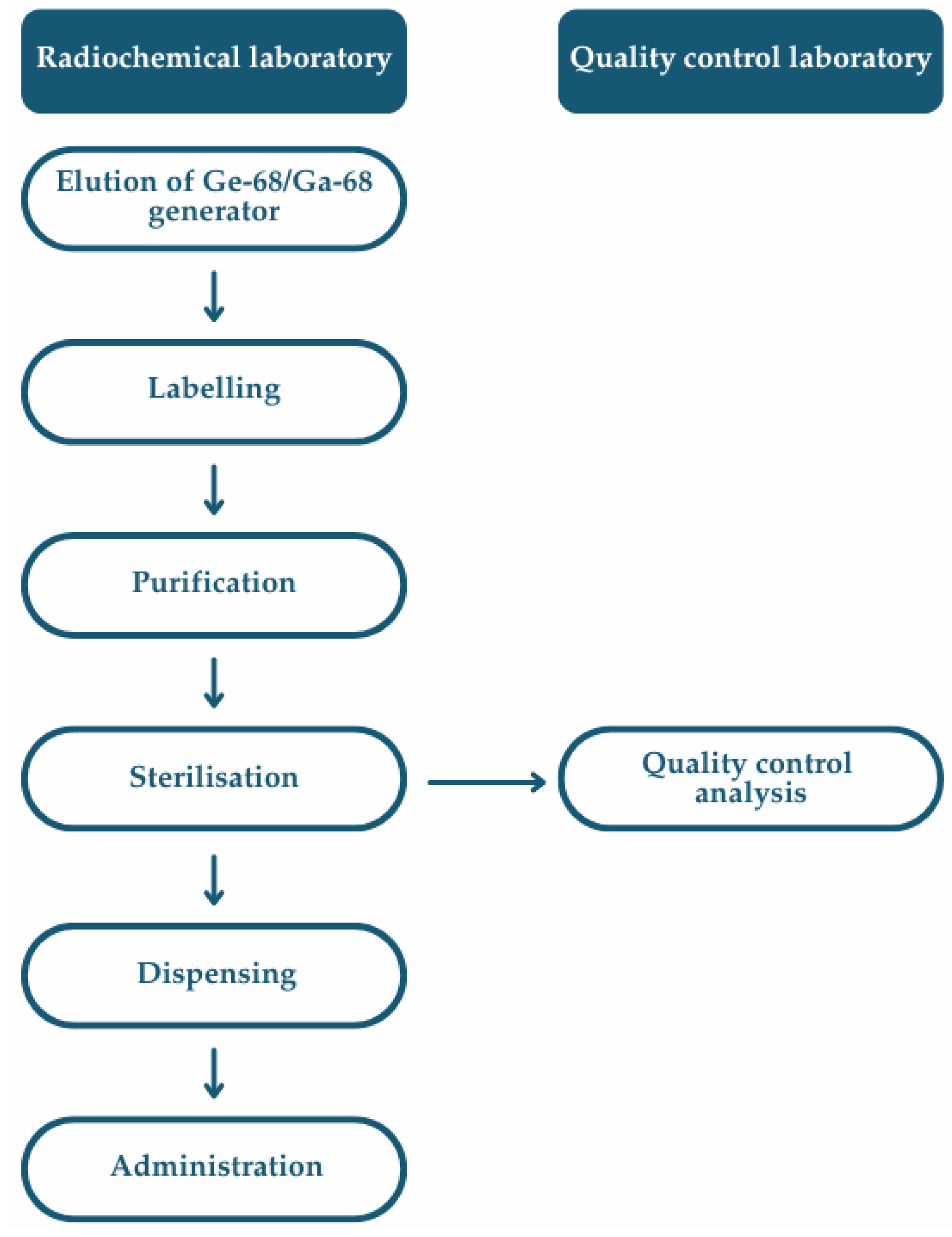
5.1. Production of Extemporaneous Formulations of 68Ga Radiopharmaceuticals for Clinical Uses
5.1.1. Manual Production
5.1.2. Automated Production
- Fractionation, which isolates the most active portion of the eluate, although this approach may lead to activity losses and requires higher precursor amounts [79];
- Anion-exchange chromatography, which traps the anionic [GaCl4]− complex formed at HCl concentrations > 5.5 M and releases Ga3+ upon elution with water [34];
- Cation-exchange chromatography, which retains Ga3+ while removing metal impurities (e.g., 68Ge, Zn2+, Fe3+) using acetone/HCl or alternative eluents such as HCl/NaCl. As acetone is not suitable for injection, its presence must be quantified by gas chromatography prior to clinical use [62].
- Fuscaldi et al. [92] described the synthesis of [68Ga]Ga-PSMA-11 using the Modular-Lab PharmTracer module. In this protocol, PSMA-11 (10–20 µg) is dissolved in 1.0 mL of 0.1 M sodium acetate buffer (pH 4.5). 68Ga is eluted from a 68Ge/68Ga generator with 0.1 M HCl, purified via cation exchange, and transferred into the reaction vial. Labelling occurs at 85 °C for 3–5 min, followed by C18 cartridge purification and sterile filtration, completing the process in approximately 25 min. The final product exhibits >99% radiochemical purity and is clinically suitable.
- Fouillet et al. [93] developed a method transposable to PSMA I&T and PSMA-617 using the GAIA® synthesis module (Elysia-Raytest, GmbH, Straubenhardt, Germany). Here, 10 µg of PSMA-11 is dissolved in 2.8 mL of 0.08 M ammonium acetate buffer (pH 4.6), with 68Ga eluted and concentrated via SCX cartridge, then labelled at 97 °C for 8 min. Purification through a C18 cartridge and sterile filtration yields a product meeting GMP clinical-grade standards with >91% radiochemical purity within 27 min.
- The Nuclear Medicine Department of Policlinico di Bari routinely synthesises [68Ga]Ga-DOTATOC using the GAIA® synthesis module. In this method, 5 mL of [68Ga]GaCl3 is labelled with 50 µg of DOTATOC at 90 °C for 10 min. The formulation uses a buffer system of acetic acid, ammonium acetate, and HCl, followed by C18 purification and sterile filtration to obtain the injectable product.
- Spreckelmeyer et al. [94] described the semi-automated production of [68Ga]Ga-FAPI-46 using the Modular Lab PharmTracer and Modular Lab eazy systems. After SCX purification and radiolabelling at 95–98 °C for 10 min, the product is purified with a CM cartridge and sterile-filtered. As the CM cartridge traps unreacted 68Ga species and flushes [68Ga]Ga-FAPI-46 directly in the product vial, this method avoids the use of ethanol, thereby eliminating the need for residual solvent testing.
5.1.3. Cold Kit
5.2. Quality Control Analysis
- Appearance: Radiopharmaceuticals must be clear, colourless solutions, free of visible particulate matter or turbidity. Visual inspection is typically performed under a calibrated light source using a clean glass inspection station or white background panel.
- pH: The final formulation, intended for intravenous administration, should exhibit a pH compatible with parenteral use, typically within the range of 3.5 to 8.5. For generator eluates, the pH is expected to be below 2 to prevent the precipitation of gallium hydroxide. Measurements are performed using benchtop pH meters with microelectrodes.
- Radionuclidic identity: established via half-life measurement (acceptable range: 62–74 min) and γ-emission spectrum, with characteristic peaks at 511 and 1077 keV. This requires a γ spectrometry system with energy-calibrated sodium iodide scintillation crystals or high-purity Germanium detectors.
- Radionuclidic purity: The level of long-lived impurities, particularly 68Ge breakthrough, must be below 0.001% of total radioactivity. Additional limits are set for any other unintended radionuclidic species. γ spectroscopy with shielding and spectral analysis software is used to quantify breakthrough and confirm compliance. Since 68Ge has a much longer half-life than 68Ga, this analysis must be performed after product release, once the sample has decayed sufficiently, in order to avoid interference from 68Ga and allow accurate quantification of long-lived contaminants.
- Radiochemical purity: Defined as the percentage of radioactivity bound to the intended compound, radiochemical purity must exceed 95%, as unbound 68Ga (e.g., free Ga3+ or colloidal species) could compromise diagnostic quality. Analytical procedures include thin-layer chromatography (iTLC) and high-performance liquid chromatography (HPLC), both equipped with radiometric detectors.
- Residual solvents: If organic solvents are used during synthesis (e.g., ethanol, acetic acid), their presence in the final formulation must be quantified by gas chromatography equipped at least with a flame ionisation detector (GC-FID), typically with headspace injection to comply with ICH guidelines.
- Bacterial endotoxins: evaluated using the Limulus Amebocyte Lysate (LAL) assay. Endotoxin quantification is commonly performed with portable or benchtop systems using kinetic chromogenic or turbidimetric methods (e.g., Endosafe® or similar), with an acceptance limit of ≤175 EU per total volume of the radiopharmaceutical.
- Sterility: While sterility testing is performed retrospectively in accordance to Ph. Eur. 2.6.1), integrity testing of the sterile filter (e.g., bubble point test) must be completed prior to batch release using validated integrity testers; sterility testing and sterile filtration are conducted in Grade A environments with Grade B background, typically inside shielded isolators or laminar flow hot cells.
- Radioactivity content and concentration: measured using ionisation chamber-based dose calibrators routinely cross-calibrated with secondary standards to ensure correct activity per administered volume.
- Specific or molar activity: Although not always required, the (apparent) specific activity (e.g., MBq/µg) or molar activity (e.g., MBq/nmol) can be reported, acknowledging the presence of excess unlabelled precursor or ligand in most preparations.
- Visual inspection for particulate matter and colour changes;
- pH determination using either a pH meter or indicator strips;
- Radiolabelling efficiency evaluation through iTLC;
- Radioactivity measurement using a dose calibrator.
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Martiniova, L.; Palatis, L.; Etchebehere, E.; Ravizzini, G. Gallium-68 in Medical Imaging. Curr. Radiopharm. 2016, 9, 187–207. [Google Scholar] [CrossRef] [PubMed]
- Kleynhans, J.; Ebenhan, T.; Sathekge, M.M. Expanding Role for Gallium-68 PET Imaging in Oncology. Semin. Nucl. Med. 2024, 54, 778–791. [Google Scholar] [CrossRef] [PubMed]
- Bois, F.; Noirot, C.; Dietemann, S.; Mainta, I.C.; Zilli, T.; Garibotto, V.; Walter, M.A. [(68)Ga]Ga-PSMA-11 in prostate cancer: A comprehensive review. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 349–374. [Google Scholar] [PubMed]
- Graham, M.M.; Gu, X.; Ginader, T.; Breheny, P.; Sunderland, J.J. (68)Ga-DOTATOC Imaging of Neuroendocrine Tumors: A Systematic Review and Metaanalysis. J. Nucl. Med. 2017, 58, 1452–1458. [Google Scholar] [CrossRef]
- Prive, B.M.; Boussihmad, M.A.; Timmermans, B.; van Gemert, W.A.; Peters, S.M.B.; Derks, Y.H.W.; van Lith, S.A.M.; Mehra, N.; Nagarajah, J.; Heskamp, S.; et al. Fibroblast activation protein-targeted radionuclide therapy: Background, opportunities, and challenges of first (pre)clinical studies. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 1906–1918. [Google Scholar] [CrossRef]
- Pretze, M.; Reffert, L.; Diehl, S.; Schonberg, S.O.; Wangler, C.; Hohenberger, P.; Wangler, B. GMP-compliant production of [(68)Ga]Ga-NeoB for positron emission tomography imaging of patients with gastrointestinal stromal tumor. EJNMMI Radiopharm. Chem. 2021, 6, 22. [Google Scholar] [CrossRef]
- Lindenberg, L.; Ahlman, M.; Lin, F.; Mena, E.; Choyke, P. Advances in PET Imaging of the CXCR4 Receptor: [(68)Ga]Ga-PentixaFor. Semin. Nucl. Med. 2024, 54, 163–170. [Google Scholar] [CrossRef]
- Urso, L.; Napolitano, R.; Speltri, G.; Tuncel, M.; Badrane, I.; Uccelli, L.; Porto, F.; Martini, P.; Niorettini, A.; Cittanti, C.; et al. (68)Ga-Trivehexin: Current Status of alphavbeta6-Integrin Imaging and Perspectives. Cancers 2025, 17, 1504. [Google Scholar] [CrossRef]
- Mirnezami, R.; Nicholson, J.; Darzi, A. Preparing for precision medicine. N. Engl. J. Med. 2012, 366, 489–491. [Google Scholar] [CrossRef]
- Holden, N.E. Table of the Isotopes. In Handbook of Chemistry and Physics, 85th ed.; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Amor-Coarasa, A.; Kelly, J.M.; Ponnala, S.; Nikolopoulou, A.; Williams, C., Jr.; Babich, J.W. (66)Ga: A Novelty or a Valuable Preclinical Screening Tool for the Design of Targeted Radiopharmaceuticals? Molecules 2018, 23, 2575. [Google Scholar] [CrossRef]
- Jalilian, A.R. An overview on Ga-68 radiopharmaceuticals for positron emission tomography applications. Iran. J. Nucl. Med. 2016, 24, 1–10. [Google Scholar]
- Greene, M.; Tucker, W. An Improved Gallium-68 cow. Radiat. Isot. 1961, 12, 62–63. [Google Scholar] [CrossRef]
- Velikyan, I. 68Ga-Based radiopharmaceuticals: Production and application relationship. Molecules 2015, 20, 12913–12943. [Google Scholar] [CrossRef] [PubMed]
- Eckert & Ziegler Radiopharma GmbH. GalliaPharm 68Ge/68Ga Generator—Summary of Product Characteristics; Eckert & Ziegler Radiopharma GmbH: Berlin, Germany, 2024. [Google Scholar]
- IRE ELiT, S.A. GalliAd® 68Ge/68Ga Generator—Riassunto delle Caratteristiche del Prodotto; IRE ELiT S.A.: Fleurus, Belgium, 2018. [Google Scholar]
- Cusnir, R.; Cakebread, A.; Cooper, M.S.; Young, J.D.; Blower, P.J.; Ma, M.T. The effects of trace metal impurities on Ga-68-radiolabelling with a tris(3-hydroxy-1,6-dimethylpyridin-4-one) (THP) chelator. RSC Adv. 2019, 9, 37214–37221. [Google Scholar] [CrossRef]
- Nelson, B.J.B.; Andersson, J.D.; Wuest, F.; Spreckelmeyer, S. Good practices for (68)Ga radiopharmaceutical production. EJNMMI Radiopharm. Chem. 2022, 7, 27. [Google Scholar] [CrossRef]
- Dash, A.; Chakravarty, R. Radionuclide generators: The prospect of availing PET radiotracers to meet current clinical needs and future research demands. Am. J. Nucl. Med. Mol. Imaging 2019, 9, 30–66. [Google Scholar]
- Eberl, S.; Eriksson, T.; Svedberg, O.; Norling, J.; Henderson, D.; Lam, P.; Fulham, M. High beam current operation of a PETtrace cyclotron for 18F- production. Appl. Radiat. Isot. 2012, 70, 922–930. [Google Scholar] [CrossRef]
- Lepareur, N. Cold Kit Labeling: The Future of (68)Ga Radiopharmaceuticals? Front. Med. 2022, 9, 812050. [Google Scholar] [CrossRef]
- Kumar, K. The Current Status of the Production and Supply of Gallium-68. Cancer Biother. Radiopharm. 2020, 35, 163–166. [Google Scholar] [CrossRef]
- Svedjehed, J.; Parnaste, M.; Gagnon, K. Demystifying solid targets: Simple and rapid distribution-scale production of [(68)Ga]GaCl(3) and [(68)Ga]Ga-PSMA-11. Nucl. Med. Biol. 2022, 104–105, 1–10. [Google Scholar] [CrossRef]
- Thisgaard, H.; Kumlin, J.; Langkjaer, N.; Chua, J.; Hook, B.; Jensen, M.; Kassaian, A.; Zeisler, S.; Borjian, S.; Cross, M.; et al. Multi-curie production of gallium-68 on a biomedical cyclotron and automated radiolabelling of PSMA-11 and DOTATATE. EJNMMI Radiopharm. Chem. 2021, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.J.B.; Wilson, J.; Richter, S.; Duke, M.J.M.; Wuest, M.; Wuest, F. Taking cyclotron (68)Ga production to the next level: Expeditious solid target production of (68)Ga for preparation of radiotracers. Nucl. Med. Biol. 2020, 80–81, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Riga, S.; Cicoria, G.; Pancaldi, D.; Zagni, F.; Vichi, S.; Dassenno, M.; Mora, L.; Lodi, F.; Morigi, M.P.; Marengo, M. Production of Ga-68 with a General Electric PETtrace cyclotron by liquid target. Phys. Med. 2018, 55, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Pandey, M.K.; Byrne, J.F.; Schlasner, K.N.; Schmit, N.R.; DeGrado, T.R. Cyclotron production of (68)Ga in a liquid target: Effects of solution composition and irradiation parameters. Nucl. Med. Biol. 2019, 74–75, 49–55. [Google Scholar] [CrossRef]
- Velikyan, I. Positron emitting [68Ga]Ga-based imaging agents: Chemistry and diversity. Med. Chem. 2011, 7, 345–379. [Google Scholar] [CrossRef]
- Martell, A.E.; Motekaitis, R.J.; Clarke, E.T.; Delgado, R.; Sun, Y.; Ma, R. Stability constants of metal complexes of macrocyclic ligands with pendant donor groups. Supramol. Chem. 1996, 6, 353–363. [Google Scholar] [CrossRef]
- Spang, P.; Herrmann, C.; Roesch, F. Bifunctional Gallium-68 Chelators: Past, Present, and Future. Semin. Nucl. Med. 2016, 46, 373–394. [Google Scholar] [CrossRef]
- Hofman, M.S.; Hicks, R.J. Gallium-68 EDTA PET/CT for Renal Imaging. Semin. Nucl. Med. 2016, 46, 448–461. [Google Scholar] [CrossRef]
- Price, E.W.; Orvig, C. Matching chelators to radiometals for radiopharmaceuticals. Chem. Soc. Rev. 2014, 43, 260–290. [Google Scholar] [CrossRef]
- Seemann, J.; Waldron, B.P.; Parker, D. Influence of metal ions on the 68Ga-labeling of DOTATATE. Appl. Radiat. Isot. 2013, 82, 63–68. [Google Scholar] [CrossRef]
- Meyer, G.J.; Macke, H.; Schuhmacher, J.; Knapp, W.H.; Hofmann, M. 68Ga-labelled DOTA-derivatised peptide ligands. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Ray Banerjee, S.; Chen, Z.; Pullambhatla, M.; Lisok, A.; Chen, J.; Mease, R.C.; Pomper, M.G. Preclinical Comparative Study of (68)Ga-Labeled DOTA, NOTA, and HBED-CC Chelated Radiotracers for Targeting PSMA. Bioconjug Chem. 2016, 27, 1447–1455. [Google Scholar] [CrossRef] [PubMed]
- Roesch, F.; Riss, P.J. The Renaissance of the 68Ge/68Ga Radionuclide Generator Initiates New Developments in 68Ga Radiopharmaceutical Chemistry. Curr. Top. Med. Chem. 2010, 10, 1633–1668. [Google Scholar] [CrossRef] [PubMed]
- Velikyan, I.; Maecke, H.; Langstrom, B. Convenient preparation of 68Ga-based PET-radiopharmaceuticals at room temperature. Bioconjug Chem. 2008, 19, 569–573. [Google Scholar] [CrossRef]
- Martell, A.E.; Smith, R.M. Critical Stability Constants. In Coordination Chemistry Reviews; Plenum Press: New York, NY, USA, 1977; Volume 1–4. [Google Scholar]
- Tsionou, M.I.; Knapp, C.E.; Foley, C.A.; Munteanu, C.R.; Cakebread, A.; Imberti, C.; Eykyn, T.R.; Young, J.D.; Paterson, B.M.; Blower, P.J.; et al. Comparison of macrocyclic and acyclic chelators for gallium-68 radiolabelling. RSC Adv. 2017, 7, 49586–49599. [Google Scholar] [CrossRef]
- Wood, S.; Samson, I. The aqueous geochemistry of gallium, germanium, indium and scandium. Ore Geol. Rev. 2006, 28, 57–102. [Google Scholar] [CrossRef]
- Blower, J.E.; Cooper, M.S.; Imberti, C.; Ma, M.T.; Marshall, C.; Young, J.D.; Blower, P.J. The Radiopharmaceutical Chemistry of the Radionuclides of Gallium and Indium. In Radiopharmaceutical Chemistry; Lewis, J.S., Windhorst, A.D., Zeglis, B.M., Eds.; Springer International Publishing: Cham, Switzerland, 2019; pp. 255–271. [Google Scholar]
- Bauwens, M.; Chekol, R.; Vanbilloen, H.; Bormans, G.; Verbruggen, A. Optimal buffer choice of the radiosynthesis of (68)Ga-Dotatoc for clinical application. Nucl. Med. Commun. 2010, 31, 753–758. [Google Scholar] [CrossRef]
- Weiner, R.E.; Thakur, M.L. Chemistry of gallium and indium radiopharmaceuticals. In Handbook of Radiopharmaceuticals: Radiochemistry and Applications; Welch, M.J., Redvanly, C.S., Eds.; John Wiley & Sons: New York, NY, USA, 2003; pp. 363–399. [Google Scholar]
- Council of Europe. European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023; Volume Supplement 11.3, pp. 2990–2991. [Google Scholar]
- Antunes, I.F.; Franssen, G.M.; Zijlma, R.; Laverman, P.; Boersma, H.H.; Elsinga, P.H. New sensitive method for HEPES quantification in (68)Ga-radiopharmaceuticals. EJNMMI Radiopharm. Chem. 2020, 5, 12. [Google Scholar] [CrossRef]
- le Roux, J.; Kleynhans, J.; Rubow, S. The use of HEPES-buffer in the production of gallium-68 radiopharmaceuticals—Time to reconsider strict pharmacopoeial limits? EJNMMI Radiopharm. Chem. 2021, 6, 15. [Google Scholar] [CrossRef]
- Gillings, N.; Hjelstuen, O.; Ballinger, J.; Behe, M.; Decristoforo, C.; Elsinga, P.; Ferrari, V.; Kolenc Peitl, P.; Koziorowski, J.; Laverman, P.; et al. Guidance on current good radiopharmacy practice (cGRPP) for the small-scale preparation of radiopharmaceuticals. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 82–84. [Google Scholar]
- European Union. Council Directive 89/343/EEC of 3 May 1989 amending Directive 65/65/EEC as regards medicinal products derived from human blood or human plasma. Off. J. Eur. Communities 1989, 142, 16–18. [Google Scholar]
- European Union. Directive 2001/83/EC of the European Parliament and of the Council of 6 November 2001 on the Community code relating to medicinal products for human use. Off. J. Eur. Communities 2001, 311, 67–128. [Google Scholar]
- Gillings, N.; Hjelstuen, O.; Behe, M.; Decristoforo, C.; Elsinga, P.H.; Ferrari, V.; Kiss, O.C.; Kolenc, P.; Koziorowski, J.; Laverman, P.; et al. EANM guideline on quality risk management for radiopharmaceuticals. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 3353–3364. [Google Scholar] [CrossRef] [PubMed]
- Hendrikse, H.; Kiss, O.; Kunikowska, J.; Wadsak, W.; Decristoforo, C.; Patt, M. EANM position on the in-house preparation of radiopharmaceuticals. Eur. J. Nucl. Med. Mol. Imaging 2022, 49, 1095–1098. [Google Scholar] [CrossRef]
- European Association of Nuclear Medicine (EANM Executive Office). Statement of the European Association of Nuclear Medicine (EANM) for a Better Inclusion of the Particularities of Radiopharmaceuticals Within the Review of Directive 2001/83/EC on Pharmaceutical Legislation; EANM Executive Office: Vienna, Austria, 2021. [Google Scholar]
- Republic of Italy. Legislative Decree No. 219 of 24 April 2006: Implementation of Directive 2001/83/EC and subsequent amendments, relating to medicinal products for human use. In Gazzetta Ufficiale della Repubblica Italiana, No. 142, 21 June 2006—Supplemento Ordinario No. 153; Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 2006. [Google Scholar]
- Ministero della Salute. Farmacopea Ufficiale Della Repubblica Italiana, XII Edizione—Supplemento: Norme di Buona Preparazione dei Radiofarmaci in Medicina Nucleare (NBP-MN); Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 2010. [Google Scholar]
- Republic of Italy. Legislative Decree No 101 of 31 July 2020: Implementation of Directive 2013/59/Euratom, establishing basic safety standards for protection against the dangers arising from exposure to ionising radiation. In Gazzetta Ufficiale Della Repubblica Italiana, No. 201, 12 August 2020—Supplemento Ordinario No. 29; Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 2020. [Google Scholar]
- European Union. Council Directive 2013/59/Euratom of 5 December 2013: Laying down basic safety standards for protection against the dangers arising from exposure to ionising radiation, and repealing Directives 89/618/Euratom, 90/641/Euratom, 96/29/Euratom, 97/43/Euratom and 2003/122/Euratom. Off. J. Eur. Union 2013, 13, 1–73. [Google Scholar]
- Republic of Italy. Legislative Decree No. 101 of 31 July 2020: Implementation of Directive 2013/59/Euratom, establishing basic safety standards for protection against the dangers arising from exposure to ionising radiation. Articles 130–131 (Radiation Protection Expert), Article 146, Annex XXIII. In Gazzetta Ufficiale Della Repubblica Italiana, No. 201, 12 August 2020—Supplemento Ordinario No. 29; Istituto Poligrafico e Zecca dello Stato: Rome, Italy, 2020. [Google Scholar]
- European Directorate for the Quality of Medicines and HealthCare. European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- European Directorate for the Quality of Medicines and HealthCare. Monograph 0125—Radiopharmaceutical Preparations. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- European Directorate for the Quality of Medicines and HealthCare. Monograph 3109—Gallium (68Ga) PSMA-11 Injection. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- European Directorate for the Quality of Medicines and HealthCare. Monograph 3098—Gallium (68Ga) Edotreotide Injection. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- Meisenheimer, M.; Saenko, Y.; Eppard, E. Gallium-68: Radiolabeling of Radiopharmaceuticals for PET Imaging—A Lot to Consider. Chapter 2. In Medical Isotopes; 2019; pp. 1–22. [Google Scholar]
- European Commission. EudraLex—Volume 4—Good Manufacturing Practice (GMP) Guidelines. 2022. Available online: https://health.ec.europa.eu/medicinal-products/eudralex/eudralex-volume-4_en (accessed on 21 March 2025).
- European Commission. EudraLex Volume 4, Annex 1: Manufacture of Sterile Medicinal Products. In The Rules Governing Medicinal Products in the European Union; European Commission: Brussels, Belgium, 2022. [Google Scholar]
- PIC/S Guide to Good Practices for the Preparation of Medicinal Products in Healthcare Establishments—Annex 3: Preparation of Radiopharmaceuticals. In Pharmaceutical Inspection Convention Pharmaceutical Inspection Co-Operation Scheme; PIC/S: Geneva, Switzerland, 2014.
- Moya, E.; Cerrato, C.; Bedoya, L.M.; Guerra, J.A. Radiopharmaceutical small-scale preparation in Europe: Will we be able to harmonize the situation? EJNMMI Radiopharm. Chem. 2024, 9, 64. [Google Scholar] [CrossRef]
- International Council for Harmonisation (ICH). ICH Harmonised Guideline: Validation of Analytical Procedures Q2(R2); ICH: Geneva, Switzerland, 2022. [Google Scholar]
- Velikyan, I. Prospective of 68Ga-Radiopharmaceutical Development. Theranostics 2014, 4, 47–80. [Google Scholar] [CrossRef]
- Gillings, N.; Todde, S.; Behe, M.; Decristoforo, C.; Elsinga, P.; Ferrari, V.; Hjelstuen, O.; Peitl, P.K.; Koziorowski, J.; Laverman, P.; et al. EANM guideline on the validation of analytical methods for radiopharmaceuticals. EJNMMI Radiopharm. Chem. 2020, 5, 7. [Google Scholar] [CrossRef]
- International Council for Harmonisation (ICH Secretariat). ICH Harmonised Guideline Q3C(R9): Impurities: Guideline for Residual Solvents; ICH Secretariat: Geneva, Switzerland, 2021. [Google Scholar]
- International Council for Harmonisation (ICH Secretariat). ICH Harmonised Guideline Q3D(R2): Guideline for Elemental Impurities; ICH Secretariat: Geneva, Switzerland, 2022. [Google Scholar]
- European Commission. Gallium (68Ga) chloride solution for radiolabelling. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023; p. 3051. [Google Scholar]
- European Commission. Gallium (68Ga) chloride solution produced by cyclotron. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023; p. 3052. [Google Scholar]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Mannweiler, S.; Amersdorfer, P.; Trajanoski, S.; Terrett, J.A.; King, D.; Mehes, G. Heterogeneity of prostate-specific membrane antigen (PSMA) expression in prostate carcinoma with distant metastasis. Pathol. Oncol. Res. 2009, 15, 167–172. [Google Scholar] [CrossRef]
- Hennrich, U.; Eder, M. [(68)Ga]Ga-PSMA-11: The First FDA-Approved (68)Ga-Radiopharmaceutical for PET Imaging of Prostate Cancer. Pharmaceuticals 2021, 14, 713. [Google Scholar] [CrossRef] [PubMed]
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Ceci, F.; Cho, S.; Giesel, F.; Haberkorn, U.; Hope, T.A.; Kopka, K.; et al. (68)Ga-PSMA PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Schuchardt, C.; Zhang, J.; Kulkarni, H.R.; Chen, X.; Muller, D.; Baum, R.P. Prostate-Specific Membrane Antigen Radioligand Therapy Using (177)Lu-PSMA I&T and (177)Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer: Comparison of Safety, Biodistribution, and Dosimetry. J. Nucl. Med. 2022, 63, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Breeman, W.A.; de Jong, M.; de Blois, E.; Bernard, B.F.; Konijnenberg, M.; Krenning, E.P. Radiolabelling DOTA-peptides with 68Ga. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 478–485. [Google Scholar] [CrossRef]
- Fani, M.; Nicolas, G.P.; Wild, D. Somatostatin Receptor Antagonists for Imaging and Therapy. J. Nucl. Med. 2017, 58, 61S–66S. [Google Scholar] [CrossRef]
- Reubi, J.C.; Waser, B. Concomitant expression of several peptide receptors in neuroendocrine tumours: Molecular basis for in vivo multireceptor tumour targeting. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 781–793. [Google Scholar] [CrossRef]
- Antunes, P.; Ginj, M.; Zhang, H.; Waser, B.; Baum, R.P.; Reubi, J.C.; Maecke, H. Are radiogallium-labelled DOTA-conjugated somatostatin analogues superior to those labelled with other radiometals? Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 982–993. [Google Scholar] [CrossRef]
- Garin-Chesa, P.; Old, L.J.; Rettig, W.J. Cell surface glycoprotein of reactive stromal fibroblasts as a potential antibody target in human epithelial cancers. Proc. Natl. Acad. Sci. USA 1990, 87, 7235–7239. [Google Scholar] [CrossRef]
- Calais, J. FAP: The Next Billion Dollar Nuclear Theranostics Target? J. Nucl. Med. 2020, 61, 163–165. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines and HealthCare. 5.19. Extemporaneous Preparation of Radiopharmaceuticals, 11th ed.; Council of Europe: Strasbourg, France, 2022. [Google Scholar]
- Council of Europe. Monograph: Gallium (68Ga) chloride (accelerator-produced). In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023; Volume Supplement 11.3. [Google Scholar]
- Lange, R.; ter Heine, R.; Decristoforo, C.; Penuelas, I.; Elsinga, P.H.; van der Westerlaken, M.M.; Hendrikse, N.H. Untangling the web of European regulations for the preparation of unlicensed radiopharmaceuticals: A concise overview and practical guidance for a risk-based approach. Nucl. Med. Commun. 2015, 36, 414–422. [Google Scholar] [CrossRef]
- Hasanain, F.; Guenther, K.; Mullett, W.M.; Craven, E. Gamma sterilization of pharmaceuticals--a review of the irradiation of excipients, active pharmaceutical ingredients, and final drug product formulations. PDA J. Pharm. Sci. Technol. 2014, 68, 113–137. [Google Scholar] [CrossRef] [PubMed]
- DeCollibus, D.P.; Searcy, J.; Tivesten, A.; Akhtar, N.; Lindenberg, C.; Abarrou, N.; Pradhan, S.; Fiandaca, M.; Franklin, J.; Govindan, G.; et al. Considerations for the Terminal Sterilization of Oligonucleotide Drug Products. Nucleic Acid. Ther. 2023, 33, 159–177. [Google Scholar] [CrossRef] [PubMed]
- International Atomic Energy Agency. Quality Control in the Production of Radiopharmaceuticals; International Atomic Energy Agency: Vienna, Austria, 2018. [Google Scholar]
- Decristoforo, C. Gallium-68—A new opportunity for PET available from a long shelf-life generator—Automation and applications. Curr. Radiopharm. 2012, 5, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Fuscaldi, L.L.; Sobral, D.V.; Durante, A.C.R.; Mendonca, F.F.; Miranda, A.C.C.; da Cunha, M.L.; Malavolta, L.; Mejia, J.; de Barboza, M.F. Standardization of the [(68)Ga]Ga-PSMA-11 Radiolabeling Protocol in an Automatic Synthesis Module: Assessments for PET Imaging of Prostate Cancer. Pharmaceuticals 2021, 14, 385. [Google Scholar] [CrossRef]
- Fouillet, J.; Donze, C.; Deshayes, E.; Santoro, L.; Rubira, L.; Fersing, C. “One Method to Label Them All”: A Single Fully Automated Protocol for GMP-Compliant (68)Ga Radiolabeling of PSMA-11, Transposable to PSMA-I&T and PSMA-617. Curr. Radiopharm. 2024, 17, 285–301. [Google Scholar] [CrossRef]
- Spreckelmeyer, S.; Balzer, M.; Poetzsch, S.; Brenner, W. Fully-automated production of [(68)Ga]Ga-FAPI-46 for clinical application. EJNMMI Radiopharm. Chem. 2020, 5, 31. [Google Scholar] [CrossRef]
- Satpati, D. Recent Breakthrough in (68)Ga-Radiopharmaceuticals Cold Kits for Convenient PET Radiopharmacy. Bioconjug Chem. 2021, 32, 430–447. [Google Scholar] [CrossRef]
- Derlin, T.; Schmuck, S.; Juhl, C.; Teichert, S.; Zorgiebel, J.; Wester, H.J.; Schneefeld, S.M.; Walte, A.C.A.; Thackeray, J.T.; Ross, T.L.; et al. Imaging Characteristics and First Experience of [(68)Ga]THP-PSMA, a Novel Probe for Rapid Kit-Based Ga-68 Labeling and PET Imaging: Comparative Analysis with [(68)Ga]PSMA I&T. Mol. Imaging Biol. 2018, 20, 650–658. [Google Scholar] [CrossRef]
- Decristoforo, C.; Patt, M. Are we “preparing” radiopharmaceuticals? EJNMMI Radiopharm. Chem. 2017, 1, 12. [Google Scholar] [CrossRef]
- Weber, W.A.; Barthel, H.; Bengel, F.; Eiber, M.; Herrmann, K.; Schafers, M. What Is Theranostics? J. Nucl. Med. 2023, 64, 669–670. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radionuclide | Half-Life | Emax (keV) | Radiation |
|---|---|---|---|
| 66Ga | 9.5 h | 4153 | β+ (56%) |
| 67Ga | 78.3 min | 91, 93, 185, 296, 388 | γ |
| 68Ga | 67.7 min | 1899, 770 | β+ (89%) |
| Method | Precursor | Reaction Buffer | Incubation | Purification | Final Processing | Time (min) |
|---|---|---|---|---|---|---|
| Manual [68Ga]Ga-PSMA-11 (Policlinico Bari) | 20 µg PSMA-11 | Sodium acetate buffer | 7.5 min, RT | None | NaCl addition + Filtration | ~15 |
| Automated [68Ga]Ga-PSMA-11 (Fuscaldi et al. [92]) | 10–20 µg PSMA-11 | 0.1 M Sodium acetate | 85 °C, 3–5 min | C18 Cartridge | Sterile Filtration | ~25 |
| Automated [68Ga]Ga-PSMA-11 (Fouillet et al. [93]) | 10 µg PSMA-11 | 0.08 M Ammonium acetate | 97 °C, 8 min | C18 Cartridge | Sterile Filtration | ~27 |
| Automated [68Ga]Ga-DOTATOC (Policlinico Bari) | 50 µg DOTATOC | Acetic acid, Ammonium acetate, HCl | 90 °C, 10 min | C18 Cartridge | Sterile Filtration | ~30 |
| Semi-Automated [68Ga]Ga-FAPI-46 (Spreckelmeyer et al. [94]) | 50 µg FAPI-46 | Acetate/Sodium ascorbate | 95–98 °C, 10 min | CM Cartridge | Sterile Filtration | ~30 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzello, M.; Pacelli, A.; De Bari, M.D.; Cutrignelli, A.; Iacobazzi, R.M.; Lopalco, A.; Denora, N. 68Ga Extemporaneous Preparations in Radiopharmacy. Pharmaceutics 2025, 17, 802. https://doi.org/10.3390/pharmaceutics17070802
Rizzello M, Pacelli A, De Bari MD, Cutrignelli A, Iacobazzi RM, Lopalco A, Denora N. 68Ga Extemporaneous Preparations in Radiopharmacy. Pharmaceutics. 2025; 17(7):802. https://doi.org/10.3390/pharmaceutics17070802
Chicago/Turabian StyleRizzello, Marzia, Anna Pacelli, Maria Domenica De Bari, Annalisa Cutrignelli, Rosa Maria Iacobazzi, Antonio Lopalco, and Nunzio Denora. 2025. "68Ga Extemporaneous Preparations in Radiopharmacy" Pharmaceutics 17, no. 7: 802. https://doi.org/10.3390/pharmaceutics17070802
APA StyleRizzello, M., Pacelli, A., De Bari, M. D., Cutrignelli, A., Iacobazzi, R. M., Lopalco, A., & Denora, N. (2025). 68Ga Extemporaneous Preparations in Radiopharmacy. Pharmaceutics, 17(7), 802. https://doi.org/10.3390/pharmaceutics17070802