
Ethosome-Based Transdermal Drug Delivery: Its Structural Components, Preparation Techniques, and Therapeutic Applications Across Metabolic, Chronic, and Oncological Conditions


Abstract

1. Introduction
2. Ethosomes
3. Advantages of Ethosomes
4. Types of Ethosomes
5. Mechanism of Action of Ethosomes
6. Preparation of Ethosomes
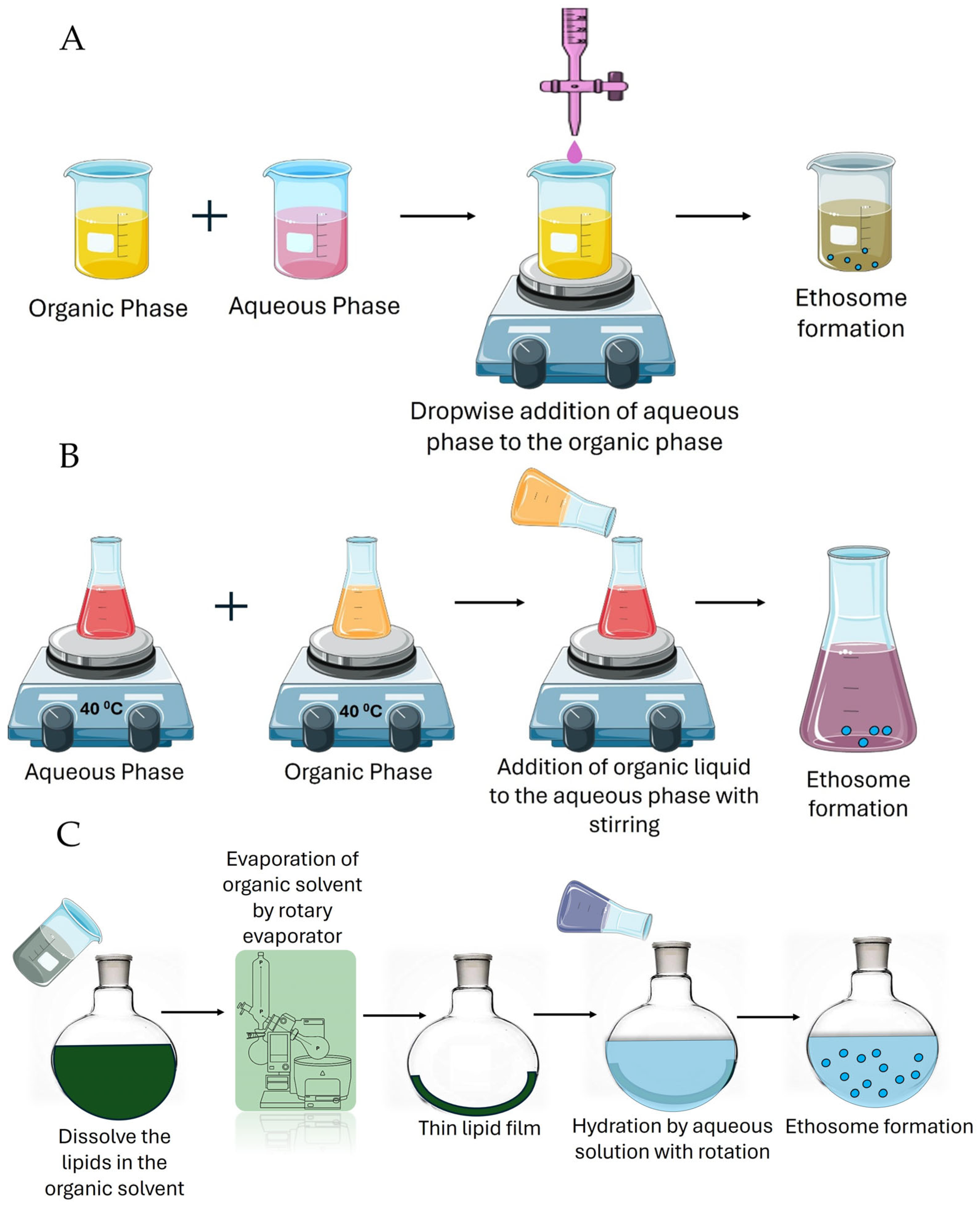
6.1. Cold Method
6.2. Hot Method
6.3. Thin Film Method
7. Application of Ethosomes in Disease Management
8. Therapeutic Applications in Selected Metabolic and Chronic Diseases
8.1. Management of Diabetic Mellitus
8.2. Management of Cardiovascular Diseases
8.3. Management of Neurodegenerative Diseases
8.4. Management of Arthritis
8.5. Management of Cancer
8.5.1. Skin Cancer
8.5.2. Breast Cancer
9. Safety Profile and Ethical Considerations of Ethosomes
10. Future Perspectives and Conclusions
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ramadon, D.; McCrudden, M.T.; Courtenay, A.J.; Donnelly, R.F. Enhancement strategies for transdermal drug delivery systems: Current trends and applications. Drug Deliv. Transl. Res. 2022, 12, 758–791. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.F.; Ang, K.P.; Sethi, G.; Looi, C.Y. Recent advancement of medical patch for transdermal drug delivery. Medicina 2023, 59, 778. [Google Scholar] [CrossRef] [PubMed]
- Kumar, C.A.; Ashwini, J.; Gl, A.; Laxmi, S.V.; Garige, A.K.; Chandupatla, V.; Haque, M.A.; Khan, S.L. Transdermal patches for the treatment of angina pectoris: An effective drug delivery system—A review. Int. J. Appl. Pharm. 2022, 14, 115–125. [Google Scholar] [CrossRef]
- Akhtar, N.; Singh, V.; Yusuf, M.; Khan, R.A. Non-invasive drug delivery technology: Development and current status of transdermal drug delivery devices, techniques and biomedical applications. Biomed. Technik. Biomed. Eng. 2020, 65, 243–272. [Google Scholar] [CrossRef]
- Peptu, C.; Rotaru, R.; Ignat, L.; Cristina Humelnicu, A.; Harabagiu, V.; Anisoara Peptu, C.; Leon, M.-M.; Mitu, F.; Cojocaru, E.; Boca, A. Nanotechnology approaches for pain therapy through transdermal drug delivery. Curr. Pharm. Des. 2015, 21, 6125–6139. [Google Scholar] [CrossRef]
- Liu, M.; Chen, S.; Zhang, Z.; Li, H.; Sun, G.; Yin, N.; Wen, J. Anti-ageing peptides and proteins for topical applications: A review. Pharm. Dev. Technol. 2022, 27, 108–125. [Google Scholar] [CrossRef]
- Alissa, I.; Nair, A.B.; Aldhubiab, B.; Shah, H.; Shah, J.; Mewada, V.; Almuqbil, R.M.; Jacob, S. Design, Development, and Evaluation of Treprostinil Embedded Adhesive Transdermal Patch. Pharmaceutics 2023, 15, 1226. [Google Scholar] [CrossRef]
- Jacob, S.; Kather, F.S.; Boddu, S.H.S.; Attimarad, M.; Nair, A.B. Nanosuspension Innovations: Expanding Horizons in Drug Delivery Techniques. Pharmaceutics 2025, 17, 136. [Google Scholar] [CrossRef]
- Sivadasan, D.; Madkhali, O.A. The Design Features, Quality by Design Approach, Characterization, Therapeutic Applications, and Clinical Considerations of Transdermal Drug Delivery Systems—A Comprehensive Review. Pharmaceuticals 2024, 17, 1346. [Google Scholar] [CrossRef]
- Bala, P.; Jathar, S.; Kale, S.; Pal, K. Transdermal drug delivery system (TDDS)—A multifaceted approach for drug delivery. J. Pharm. Res. 2014, 8, 1805–1835. [Google Scholar]
- Patel, H.J.; Trivedi, D.G.; Bhandari, A.K.; Shah, D.A. Penetration enhancers for transdermal drug delivery system: A review. J. Pharm. Cosmetol. 2011, 1, 67–80. [Google Scholar]
- Nair, A.; Reddy, C.; Jacob, S. Delivery of a classical antihypertensive agent through the skin by chemical enhancers and iontophoresis. Ski. Res. Technol. 2009, 15, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Herman, A.; Herman, A.P. Essential oils and their constituents as skin penetration enhancer for transdermal drug delivery: A review. J. Pharm. Pharmacol. 2015, 67, 473–485. [Google Scholar] [CrossRef]
- Javadzadeh, Y.; Bahari, L.A. Therapeutic nanostructures for dermal and transdermal drug delivery. In Nano- and Microscale Drug Delivery Systems; Elsevier: Amsterdam, The Netherlands, 2017; pp. 131–146. [Google Scholar]
- Kamboj, S.; Bala, S.; Nair, A.B. Solid lipid nanoparticles: An effective lipid based technology for poorly water soluble drugs. Int. J. Pharm. Sci. Rev. Res. 2010, 5, 78–90. [Google Scholar]
- Touitou, E.; Natsheh, H. Topical administration of drugs incorporated in carriers containing phospholipid soft vesicles for the treatment of skin medical conditions. Pharmaceutics 2021, 13, 2129. [Google Scholar] [CrossRef]
- Gorain, B.; Al-Dhubiab, B.E.; Nair, A.; Kesharwani, P.; Pandey, M.; Choudhury, H. Multivesicular liposome: A lipid-based drug delivery system for efficient drug delivery. Curr. Pharm. Des. 2021, 27, 4404–4415. [Google Scholar] [CrossRef]
- Chauhan, N.; Vasava, P.; Khan, S.L.; Siddiqui, F.A.; Islam, F.; Chopra, H.; Emran, T.B. Ethosomes: A novel drug carrier. Ann. Med. Surg. 2022, 82, 104595. [Google Scholar] [CrossRef]
- Soba, S.V.; Babu, M.; Panonnummal, R. Ethosomal gel formulation of alpha phellandrene for the transdermal delivery in gout. Adv. Pharm. Bull. 2020, 11, 137. [Google Scholar] [CrossRef]
- Patil, M.; Hussain, A.; Altamimi, M.A.; Ashique, S.; Haider, N.; Faruk, A.; Khuroo, T.; Sherikar, A.; Siddique, M.U.M.; Ansari, A. An insight of various vesicular systems, erythrosomes, and exosomes to control metastasis and cancer. Adv. Cancer Biol. Metastasis 2023, 7, 100103. [Google Scholar] [CrossRef]
- Alfehaid, F.S.; Nair, A.B.; Shah, H.; Aldhubiab, B.; Shah, J.; Mewada, V.; Jacob, S.; Attimarad, M. Enhanced transdermal delivery of apremilast loaded ethosomes: Optimization, characterization and in vivo evaluation. J. Drug Deliv. Sci. Technol. 2024, 91, 105211. [Google Scholar] [CrossRef]
- Nainwal, N.; Jawla, S.; Singh, R.; Saharan, V.A. Transdermal applications of ethosomes—A detailed review. J. Liposome Res. 2019, 29, 103–113. [Google Scholar] [CrossRef] [PubMed]
- Benson, H.A. Transfersomes for transdermal drug delivery. Expert Opin. Drug Deliv. 2006, 3, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Marianecci, C.; Di Marzio, L.; Rinaldi, F.; Celia, C.; Paolino, D.; Alhaique, F.; Esposito, S.; Carafa, M. Niosomes from 80s to present: The state of the art. Adv. Colloid Interface Sci. 2014, 205, 187–206. [Google Scholar] [CrossRef]
- Shehata, T.M.; Nair, A.B.; Al-Dhubiab, B.E.; Shah, J.; Jacob, S.; Alhaider, I.A.; Attimarad, M.; Elsewedy, H.S.; Ibrahim, M.M. Vesicular emulgel based system for transdermal delivery of insulin: Factorial design and in vivo evaluation. Appl. Sci. 2020, 10, 5341. [Google Scholar] [CrossRef]
- Verma, P.; Pathak, K. Therapeutic and cosmeceutical potential of ethosomes: An overview. J. Adv. Pharm. Technol. Res. 2010, 1, 274–282. [Google Scholar] [CrossRef]
- Jain, H.; Patel, J.; Joshi, K.; Patel, P.; Upadhyay, U. Ethosomes: A novel drug carrier. Int. J. Clin. Pract. 2011, 7, 1–4. [Google Scholar]
- Aute, P.P.; Kamble, M.S.; Chaudhari, P.D.; Bhosale, A.V. A comprehensive review on ethosomes. Int. J. Res. Dev. Pharm. Life Sci. 2012, 2, 218–224. [Google Scholar]
- Mohanty, D.; Mounika, A.; Bakshi, V.; Haque, M.A.; Sahoo, C.K. Ethosomes: A novel approach for transdermal drug delivery. Int. J. ChemTech Res. 2018, 11, 219–226. [Google Scholar] [CrossRef]
- Zhan, B.; Wang, J.; Li, H.; Xiao, K.; Fang, X.; Shi, Y.; Jia, Y. Ethosomes: A promising drug delivery platform for transdermal application. Chemistry 2024, 6, 993–1019. [Google Scholar] [CrossRef]
- Zhang, J.-P.; Wei, Y.-H.; Zhou, Y.; Li, Y.-Q.; Wu, X.-A. Ethosomes, binary ethosomes and transfersomes of terbinafine hydrochloride: A comparative study. Arch. Pharmacal Res. 2012, 35, 109–117. [Google Scholar] [CrossRef]
- Hamzah, M.L.; Kassab, H.J. Formulation and characterization of intranasal drug delivery of frovatriptan-loaded binary ethosomes gel for brain targeting. Nanotechnol. Sci. Appl. 2024, 17, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Song, C.K.; Balakrishnan, P.; Shim, C.-K.; Chung, S.-J.; Chong, S.; Kim, D.-D. A novel vesicular carrier, transethosome, for enhanced skin delivery of voriconazole: Characterization and in vitro/in vivo evaluation. Colloids Surf. B Biointerfaces 2012, 92, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Paiva-Santos, A.C.; Silva, A.L.; Guerra, C.; Peixoto, D.; Pereira-Silva, M.; Zeinali, M.; Mascarenhas-Melo, F.; Castro, R.; Veiga, F. Ethosomes as nanocarriers for the development of skin delivery formulations. Pharm. Res. 2021, 38, 947–970. [Google Scholar] [CrossRef] [PubMed]
- Rosmiati, M.; Sopyan, I.; Chaeruisaa, A.; Abdassah, M. Development of serum with 4-n-butylresorcinol in the transethosomes vesicular system. Int. J. Appl. Pharm. 2024, 16, 246–254. [Google Scholar] [CrossRef]
- Akhtar, N.; Pathak, K. Cavamax W7 composite ethosomal gel of clotrimazole for improved topical delivery: Development and comparison with ethosomal gel. AAPS PharmSciTech 2012, 13, 344–355. [Google Scholar] [CrossRef]
- Lu, J.; Guo, T.; Fan, Y.; Li, Z.; He, Z.; Yin, S.; Feng, N. Recent developments in the principles, modification and application prospects of functionalized ethosomes for topical delivery. Curr. Drug Deliv. 2021, 18, 570–582. [Google Scholar] [CrossRef]
- Guo, T.; Lu, J.; Fan, Y.; Zhang, Y.; Yin, S.; Sha, X.; Feng, N. TPGS assists the percutaneous administration of curcumin and glycyrrhetinic acid coloaded functionalized ethosomes for the synergistic treatment of psoriasis. Int. J. Pharm. 2021, 604, 120762. [Google Scholar] [CrossRef]
- Wang, P.; Hong, S.; Cao, C.; Guo, S.; Wang, C.; Chen, X.; Wang, X.; Song, P.; Li, N.; Xu, R. Ethosomes-mediated tryptanthrin delivery as efficient anti-psoriatic nanotherapy by enhancing topical drug absorption and lipid homeostasis. J. Nanobiotechnol. 2024, 22, 584. [Google Scholar] [CrossRef]
- Mehmood, Y.; Shahid, H.; Ahmed, S.; Khursheed, A.; Jamshaid, T.; Jamshaid, M.; Mengistie, A.A.; Dawoud, T.M.; Siddique, F. Synthesis of vitamin D3 loaded ethosomes gel to cure chronic immune-mediated inflammatory skin disease: Physical characterization, in vitro and ex vivo studies. Sci. Rep. 2024, 14, 23866. [Google Scholar] [CrossRef]
- Sangeetha, S. Ethosomes: A novel drug delivery system and their therapeutic applications—A review. Res. J. Pharm. Technol. 2020, 13, 1972–1980. [Google Scholar]
- Patrekar, P.V.; Inamdar, S.J.; Mali, S.S.; Mujib, M.T.; Ahir, A.A.; Hosmani, A.H. Ethosomes as novel drug delivery system: A review. Pharma Innov. 2015, 4, 10. [Google Scholar]
- Chandra, A.; Aggarwal, G.; Manchanda, S.; Narula, A. Development of topical gel of methotrexate incorporated ethosomes and salicylic acid for the treatment of psoriasis. Pharm. Nanotechnol. 2019, 7, 362–374. [Google Scholar] [CrossRef] [PubMed]
- El-Menshawe, S.F.; Sayed, O.M.; Abou-Taleb, H.A.; El Tellawy, N. Skin permeation enhancement of nicotinamide through using fluidization and deformability of positively charged ethosomal vesicles: A new approach for treatment of atopic eczema. J. Drug Deliv. Sci. Technol. 2019, 52, 687–701. [Google Scholar] [CrossRef]
- Kausar, H.; Mujeeb, M.; Ahad, A.; Moolakkadath, T.; Aqil, M.; Ahmad, A.; Akhter, M.H. Optimization of ethosomes for topical thymoquinone delivery for the treatment of skin acne. J. Drug Deliv. Sci. Technol. 2019, 49, 177–187. [Google Scholar] [CrossRef]
- Garg, B.J.; Garg, N.K.; Beg, S.; Singh, B.; Katare, O.P. Nanosized ethosomes-based hydrogel formulations of methoxsalen for enhanced topical delivery against vitiligo: Formulation optimization, in vitro evaluation and preclinical assessment. J. Drug Target. 2016, 24, 233–246. [Google Scholar] [CrossRef]
- Maheshwari, R.G.; Tekade, R.K.; Sharma, P.A.; Darwhekar, G.; Tyagi, A.; Patel, R.P.; Jain, D.K. Ethosomes and ultradeformable liposomes for transdermal delivery of clotrimazole: A comparative assessment. Saudi Pharm. J. 2012, 20, 161–170. [Google Scholar] [CrossRef]
- Godin, B.; Touitou, E. Erythromycin ethosomal systems: Physicochemical characterization and enhanced antibacterial activity. Curr. Drug Deliv. 2005, 2, 269–275. [Google Scholar] [CrossRef]
- Sharma, P.; Chawla, A.; Arora, S.; Pawar, P. Novel drug delivery approaches on antiviral and antiretroviral agents. J. Adv. Pharm. Technol. Res. 2012, 3, 147–159. [Google Scholar]
- Uner, B.; Ozdemir, S.; Pilevne, S.N.; Celebi, A.R.C. Timolol-loaded ethosomes for ophthalmic delivery: Reduction of high intraocular pressure in vivo. Int. J. Pharm. 2023, 640, 123021. [Google Scholar] [CrossRef]
- Sakran, W.; Abdel-Rashid, R.S.; Saleh, F.; Abdel-Monem, R. Ethosomal gel for rectal transmucosal delivery of domperidone: Design of experiment, in vitro, and in vivo evaluation. Drug Deliv. 2022, 29, 1477–1491. [Google Scholar] [CrossRef]
- Kumar, S.; Kumar, A.; Kumar, N.; Singh, P.; Singh, T.U.; Singh, B.R.; Gupta, P.K.; Thakur, V.K. In vivo therapeutic efficacy of Curcuma longa extract loaded ethosomes on wound healing. Vet. Res. Commun. 2022, 46, 1033–1049. [Google Scholar] [CrossRef] [PubMed]
- Raghuvanshi, A.; Shah, K.; Dewangan, H.K. Ethosome as antigen delivery carrier: Optimisation, evaluation and induction of immunological response via nasal route against hepatitis B. J. Microencapsul. 2022, 39, 352–363. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ng, W.; Hu, J.; Mussa, S.S.; Ge, Y.; Xu, H. Formulation and in vitro stability evaluation of ethosomal carbomer hydrogel for transdermal vaccine delivery. Colloids Surf. B Biointerfaces 2018, 163, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Milagro, F.I.; Riezu-Boj, J.I.; Martinez, J.A. Epigenetic signatures underlying inflammation: An interplay of nutrition, physical activity, metabolic diseases, and environmental factors for personalized nutrition. Inflamm. Res. 2021, 70, 29–49. [Google Scholar] [CrossRef]
- Barroso, I.; McCarthy, M.I. The genetic basis of metabolic disease. Cell 2019, 177, 146–161. [Google Scholar] [CrossRef]
- Duncan, L. Metabolic diseases-diabetes mellitus, obesity. In Textbook of Medical Treatment; Alstead, S., Macgregor, A.G., Eds.; Churchill Livingstone: Edinburgh, UK, 1971; Volume 12, p. 322. [Google Scholar]
- Munni, J.F. Impact of Chronic Diseases on Quality of Life; East West University: Dhaka, Bangladesh, 2016. [Google Scholar]
- Wilson, P.W.; D’Agostino, R.B.; Parise, H.; Sullivan, L.; Meigs, J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005, 112, 3066–3072. [Google Scholar] [CrossRef]
- Bagby, S.P. Obesity-initiated metabolic syndrome and the kidney: A recipe for chronic kidney disease? J. Am. Soc. Nephrol. 2004, 15, 2775–2791. [Google Scholar] [CrossRef]
- Shi, S.; Kong, N.; Feng, C.; Shajii, A.; Bejgrowicz, C.; Tao, W.; Farokhzad, O.C. Drug delivery strategies for the treatment of metabolic diseases. Adv. Healthc. Mater. 2019, 8, 1801655. [Google Scholar] [CrossRef]
- Yang, Y.; Zhou, R.; Wang, Y.; Zhang, Y.; Yu, J.; Gu, Z. Recent advances in oral and transdermal protein delivery systems. Angew. Chem. Int. Ed. 2023, 62, e202214795, Angew. Chem. 2023, 135, e202214795. [Google Scholar] [CrossRef]
- Adnan, M.; Akhter, M.H.; Afzal, O.; Altamimi, A.S.; Ahmad, I.; Alossaimi, M.A.; Jaremko, M.; Emwas, A.-H.; Haider, T.; Haider, M.F. Exploring nanocarriers as treatment modalities for skin cancer. Molecules 2023, 28, 5905. [Google Scholar] [CrossRef]
- Priya; Gaur, P.K.; Kumar, S. Nanocarrier-Mediated Dermal Drug Delivery System of Antimicrobial Agents for Targeting Skin and Soft Tissue Infections. ASSAY Drug Dev. Technol. 2025, 23, 2–28. [Google Scholar] [CrossRef]
- Jacob, S.; Kather, F.S.; Boddu, S.H.S.; Shah, J.; Nair, A.B. Innovations in Nanoemulsion Technology: Enhancing Drug Delivery for Oral, Parenteral, and Ophthalmic Applications. Pharmaceutics 2024, 16, 1333. [Google Scholar] [CrossRef] [PubMed]
- Bodade, S.S.; Shaikh, K.S.; Kamble, M.S.; Chaudhari, P.D. A study on ethosomes as mode for transdermal delivery of an antidiabetic drug. Drug Deliv. 2013, 20, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Khatarkar, M.; Dhote, V.K.; Pawar, R.S. Formulation & Evaluation of Linagliptin Loaded Ethosomes for Treatment of Diabetes. Asian J. Pharm. Educ. Res. 2023, 12, 1–6. [Google Scholar]
- Nabila, F.H.; Islam, R.; Yamin, L.; Yoshirou, K.; Wakabayashi, R.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Transdermal Insulin Delivery Using Ionic Liquid-Mediated Nanovesicles for Diabetes Treatment. ACS Biomater. Sci. Eng. 2024, 11, 402–414. [Google Scholar] [CrossRef]
- Bhulli, N.; Sharma, A. Preparation of novel vesicular carrier ethosomes with glimepiride and their invistigation of permeability. Int. J. Ther. Appl. 2012, 10, 1–10. [Google Scholar]
- Sundar, V.D.; Dhanaraju, M.D.; Anilkumar Vadaga, N. Dapagliflozin-Loaded Ethosomes as Transdermal Drug Delivery Carriers: Statistical Design, Formulation and Evaluation. Adv. Biores. 2023, 14, 289–300. [Google Scholar]
- Elbakry, A.M.; Marzouk, M.A.; Khalil, R.; Zahran, A.; ElArini, S. Design and Evaluation of Carvedilol Ethosomes using Box-Behnken Design. Int. J. Holist. Res. 2025, 2, 1–12. [Google Scholar] [CrossRef]
- Ammar, H.O.; Tadros, M.I.; Salama, N.M.; Ghoneim, A.M. Ethosome-derived invasomes as a potential transdermal delivery system for vardenafil hydrochloride: Development, optimization and application of physiologically based pharmacokinetic modeling in adults and geriatrics. Int. J. Nanomed. 2020, 15, 5671–5685. [Google Scholar] [CrossRef]
- Fouad, S.A.; Khatab, S.T.; Teaima, M.H.; El-Nabarawi, M.A.; Abdelmonem, R. Nanosized ethosomal dispersions for enhanced transdermal delivery of nebivolol using intradermal/transfollicular sustained reservoir: In vitro evaluation, confocal laser scanning microscopy, and in vivo pharmacokinetic studies. Pharm. Dev. Technol. 2024, 29, 40–51. [Google Scholar] [CrossRef]
- Ibrahim, T.M.; Abdallah, M.H.; El-Megrab, N.A.; El-Nahas, H.M. Transdermal ethosomal gel nanocarriers; a promising strategy for enhancement of anti-hypertensive effect of carvedilol. J. Liposome Res. 2019, 29, 215–228. [Google Scholar] [CrossRef] [PubMed]
- Salem, H.F.; El-Menshawe, S.F.; Khallaf, R.A.; Rabea, Y.K. A novel transdermal nanoethosomal gel of lercanidipine HCl for treatment of hypertension: Optimization using Box-Benkhen design, in vitro and in vivo characterization. Drug Deliv. Transl. Res. 2020, 10, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Moghaddam, A.A.; Aqil, M.; Ahmad, F.J.; Ali, M.M.; Sultana, Y.; Ali, A. Nanoethosomes mediated transdermal delivery of vinpocetine for management of Alzheimer’s disease. Drug Deliv. 2015, 22, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Lobo, C.L.; Priya, S. Design and Characterization of Transethosomes loaded with Rivastigmine for Enhanced Transdermal Delivery. J. Res. Pharm. 2024, 28, 1409–1422. [Google Scholar]
- Mishra, N.; Tiwari, D.K.; Mishra, K.; Gupta, A.; Suman, S.; Mishra, S. Development of intranasal deformable ethosomes of rasagiline mesylate for the effective management of parkinsonism. Int. J. Pharm. Biol. Sci. 2020, 10, 25–33. [Google Scholar]
- Sneh, P.; Jyothi, D.; James, J.P.; Maxwell, A. Formulation and optimization of ethosomes loaded with ropinirole hydrochloride: Application of quality by design approach. Res. J. Pharm. Technol. 2020, 13, 4339–4345. [Google Scholar] [CrossRef]
- ElShagea, H.N.; Makar, R.R.; Salama, A.H.; Elkasabgy, N.A.; Basalious, E.B. Investigating the targeting power to brain tissues of intranasal rasagiline mesylate-loaded transferosomal in situ gel for efficient treatment of Parkinson’s disease. Pharmaceutics 2023, 15, 533. [Google Scholar] [CrossRef]
- Babasahib, S.K.; Born, R.W.; Raghavendra, N.M. Trans ethosomal hybrid composites of naproxen-sulfapyridine in hydrogel carrier: Anti-inflammatory response in complete Freund’s adjuvant induced arthritis rats. Artif. Cells Nanomed. Biotechnol. 2022, 50, 59–70. [Google Scholar] [CrossRef]
- Barupal, A.; Gupta, V.; Ramteke, S. Preparation and characterization of ethosomes for topical delivery of aceclofenac. Indian J. Pharm. Sci. 2010, 72, 582. [Google Scholar]
- Kumar Sarwa, K.; Rudrapal, M.; Mazumder, B. Topical ethosomal capsaicin attenuates edema and nociception in arthritic rats. Drug Deliv. 2015, 22, 1043–1052. [Google Scholar] [CrossRef]
- Fang, Y.-P.; Tsai, Y.-H.; Wu, P.-C.; Huang, Y.-B. Comparison of 5-aminolevulinic acid-encapsulated liposome versus ethosome for skin delivery for photodynamic therapy. Int. J. Pharm. 2008, 356, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Ismail, T.A.; Shehata, T.M.; Mohamed, D.I.; Elsewedy, H.S.; Soliman, W.E. Quality by design for development, optimization and characterization of brucine ethosomal gel for skin cancer delivery. Molecules 2021, 26, 3454. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.S.; Billa, N.; Leong, C.-O.; Morris, A.P. An evaluation of tocotrienol ethosomes for transdermal delivery using Strat-M® membrane and excised human skin. Pharm. Dev. Technol. 2021, 26, 243–251. [Google Scholar] [CrossRef]
- Apolinário, A.C.; Naser, Y.A.; Volpe-Zanutto, F.; Vora, L.K.; Sabri, A.H.; Li, M.; Hutton, A.R.; McCarthy, H.O.; Lopes, L.B.; Donnelly, R.F. Novel lipid nanovesicle-loaded dissolving microarray patches for fenretinide in breast cancer chemoprevention. J. Control. Release 2024, 374, 76–88. [Google Scholar] [CrossRef]
- Mahmood, S.; Mandal, U.K.; Chatterjee, B. Transdermal delivery of raloxifene HCl via ethosomal system: Formulation, advanced characterizations and pharmacokinetic evaluation. Int. J. Pharm. 2018, 542, 36–46. [Google Scholar] [CrossRef]
- Lin, X.; Xu, Y.; Pan, X.; Xu, J.; Ding, Y.; Sun, X.; Song, X.; Ren, Y.; Shan, P.-F. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 2020, 10, 14790. [Google Scholar] [CrossRef]
- Chakraborty, T.; Gupta, S.; Nair, A.; Chauhan, S.; Saini, V. Wound healing potential of insulin-loaded nanoemulsion with Aloe vera gel in diabetic rats. J. Drug Deliv. Sci. Technol. 2021, 64, 102601. [Google Scholar] [CrossRef]
- Viana, A.L.M.; Doriguetto, A.C.; Viana, O.M.M.S.; Ruela, A.L.M.; Freitas, J.T.J.; Souto, B.E.M.; de Araujo, M.B.; de Araújo Paula, F.B. Pharmacokinetics and pharmacodynamics of glimepiride polymorphs. Int. J. Pharm. 2018, 553, 272–280. [Google Scholar] [CrossRef]
- Hussain, M.; Hafeez, A.; Kushwaha, S.P. Nanoformulation mediated transdermal delivery of anti-diabetic drugs: An updated review. Intell. Pharm. 2023, 1, 192–200. [Google Scholar] [CrossRef]
- Ahmed, T.A.; Khalid, M.; Aljaeid, B.M.; Fahmy, U.A.; Abd-Allah, F.I. Transdermal glimepiride delivery system based on optimized ethosomal nano-vesicles: Preparation, characterization, in vitro, ex vivo and clinical evaluation. Int. J. Pharm. 2016, 500, 245–254. [Google Scholar] [CrossRef]
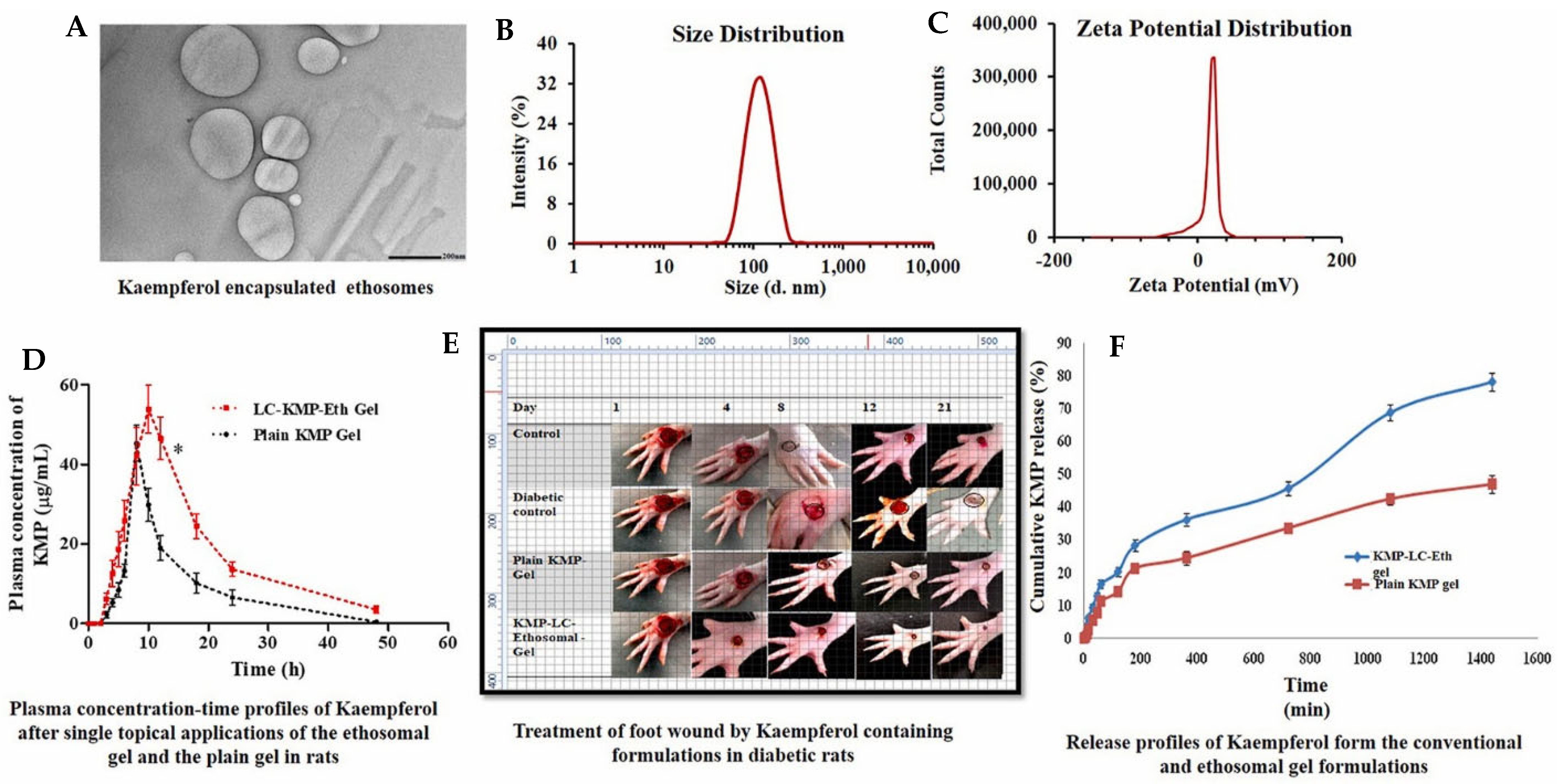
- Raghav, S.S.; Kumar, B.; Sethiya, N.K.; Singhal, M.; Alhowyan, A.; Kalam, M.A.; Malik, A. Potential of hybrid lecithin-chitosan kaempferol ethosomes for the treatment of diabetic foot ulcer: In vitro and In vivo investigation. J. Drug Deliv. Sci. Technol. 2024, 98, 105927. [Google Scholar] [CrossRef]
- Iribarren, C.; Sidney, S.; Sternfeld, B.; Browner, W.S. Calcification of the aortic arch: Risk factors and association with coronary heart disease, stroke, and peripheral vascular disease. JAMA 2000, 283, 2810–2815. [Google Scholar] [CrossRef] [PubMed]
- Morley, R.L.; Sharma, A.; Horsch, A.D.; Hinchliffe, R.J. Peripheral artery disease. BMJ 2018, 360, j5842. [Google Scholar] [CrossRef]
- Nair, A.; Vyas, H.; Shah, J.; Kumar, A. Effect of permeation enhancers on the iontophoretic transport of metoprolol tartrate and the drug retention in skin. Drug Deliv. 2011, 18, 19–25. [Google Scholar] [CrossRef]
- Timmis, A.; Aboyans, V.; Vardas, P.; Townsend, N.; Torbica, A.; Kavousi, M.; Boriani, G.; Huculeci, R.; Kazakiewicz, D.; Scherr, D.; et al. European society of cardiology: The 2023 atlas of cardiovascular disease statistics. Eur. Heart J. 2024, 45, 4019–4062. [Google Scholar] [CrossRef]
- Rana, J.; Nieuwdorp, M.; Jukema, J.; Kastelein, J. Cardiovascular metabolic syndrome—An interplay of, obesity, inflammation, diabetes and coronary heart disease. Diabetes Obes. Metab. 2007, 9, 218–232. [Google Scholar] [CrossRef]
- Hall, M.E.; do Carmo, J.M.; da Silva, A.A.; Juncos, L.A.; Wang, Z.; Hall, J.E. Obesity, hypertension, and chronic kidney disease. Int. J. Nephrol. Renov. Dis. 2014, 7, 75–88. [Google Scholar] [CrossRef]
- Anroop, B.; Ghosh, B.; Parcha, V.; Khanam, J. Transdermal delivery of atenolol: Effect of prodrugs and iontophoresis. Curr. Drug Deliv. 2009, 6, 280–290. [Google Scholar] [CrossRef]
- Turco, L.; Reiberger, T.; Vitale, G.; La Mura, V. Carvedilol as the new non-selective beta-blocker of choice in patients with cirrhosis and portal hypertension. Liver Int. 2023, 43, 1183–1194. [Google Scholar] [CrossRef]
- Carreira, R.; Monteiro, P.; Goncalves, L.; Providencia, L. Carvedilol: Just another Beta-blocker or a powerful cardioprotector? Cardiovasc. Hematol. Disord. Targets 2006, 6, 257–266. [Google Scholar] [CrossRef]
- Fernandes, G.J.; Kumar, L.; Sharma, K.; Tunge, R.; Rathnanand, M. A review on solubility enhancement of carvedilol—A BCS class II drug. J. Pharm. Innov. 2018, 13, 197–212. [Google Scholar] [CrossRef]
- Amarachinta, P.R.; Sharma, G.; Samed, N.; Chettupalli, A.K.; Alle, M.; Kim, J.-C. Central composite design for the development of carvedilol-loaded transdermal ethosomal hydrogel for extended and enhanced anti-hypertensive effect. J. Nanobiotechnol. 2021, 19, 100. [Google Scholar] [CrossRef] [PubMed]
- Jiang, D.; Jiang, Y.; Wang, K.; Wang, Z.; Pei, Y.; Wu, J.; He, C.; Mo, X.; Wang, H. Binary ethosomes-based transdermal patches assisted by metal microneedles significantly improve the bioavailability of carvedilol. J. Drug Deliv. Sci. Technol. 2022, 74, 103498. [Google Scholar] [CrossRef]
- Ahad, A.; Aqil, M.; Kohli, K.; Sultana, Y.; Mujeeb, M. Enhanced transdermal delivery of an anti-hypertensive agent via nanoethosomes: Statistical optimization, characterization and pharmacokinetic assessment. Int. J. Pharm. 2013, 443, 26–38. [Google Scholar] [CrossRef]
- Dave, V.; Sohgaura, A.; Tak, K.; Reddy, K.R.; Thylur, R.P.; Ramachandraiah, K.; Sadhu, V. Ethosomal polymeric patch containing losartan potassium for the treatment of hypertension: In-vitro and in-vivo evaluation. Biomed. Phys. Eng. Express 2019, 5, 065029. [Google Scholar] [CrossRef]
- Shang, H.; Zhao, X.; Zhang, X. Neurodegenerative diseases. In Pediatric Neuroimaging: Cases and Illustrations; Springer: Berlin/Heidelberg, Germany, 2022; pp. 211–214. [Google Scholar]
- Gonzales, M.M.; Garbarino, V.R.; Pollet, E.; Palavicini, J.P.; Kellogg, D.L.; Kraig, E.; Orr, M.E. Biological aging processes underlying cognitive decline and neurodegenerative disease. J. Clin. Investig. 2022, 132, e158453. [Google Scholar] [CrossRef]
- Newell, M.E.; Babbrah, A.; Aravindan, A.; Rathnam, R.; Kiernan, R.; Driver, E.M.; Bowes, D.A.; Halden, R.U. Prevalence rates of neurodegenerative diseases versus human exposures to heavy metals across the United States. Sci. Total Environ. 2024, 928, 172260. [Google Scholar] [CrossRef]
- Daneman, R.; Prat, A. The blood–brain barrier. Cold Spring Harb. Perspect. Biol. 2015, 7, a020412. [Google Scholar] [CrossRef]
- Tsuji, A. Small molecular drug transfer across the blood-brain barrier via carrier-mediated transport systems. NeuroRx 2005, 2, 54–62. [Google Scholar] [CrossRef]
- Jones, A.R.; Shusta, E.V. Blood–brain barrier transport of therapeutics via receptor-mediation. Pharm. Res. 2007, 24, 1759–1771. [Google Scholar] [CrossRef]
- Cascione, M.; De Matteis, V.; Leporatti, S.; Rinaldi, R. The new frontiers in neurodegenerative diseases treatment: Liposomal-based strategies. Front. Bioeng. Biotechnol. 2020, 8, 566767. [Google Scholar] [CrossRef]
- Pires, P.C.; Paiva-Santos, A.C.; Veiga, F. Liposome-derived nanosystems for the treatment of behavioral and neurodegenerative diseases: The promise of niosomes, transfersomes, and ethosomes for increased brain drug bioavailability. Pharmaceuticals 2023, 16, 1424. [Google Scholar] [CrossRef] [PubMed]
- Navaneethan, S.; Somashekhar, C.; Harshitha, V.Y. Formulation and design optimization of nano ethosomal gel for delivery of rasagiline mesylate: Improvement in brain localization and bioavailability. Eur. J. Pharm. Med. Res. 2022, 9, 536–551. [Google Scholar]
- Shi, J.; Wang, Y.; Luo, G. Ligustrazine phosphate ethosomes for treatment of Alzheimer’s disease, in vitro and in animal model studies. AAPS PharmSciTech 2012, 13, 485–492. [Google Scholar] [CrossRef]
- Ma, W.; Chen, H.; Yuan, Q.; Chen, X.; Li, H. Global, regional, and national epidemiology of osteoarthritis in working-age individuals: Insights from the global burden of disease study 1990–2021. Sci. Rep. 2025, 15, 7907. [Google Scholar] [CrossRef]
- Gravallese, E.M.; Harada, Y.; Wang, J.-T.; Gorn, A.H.; Thornhill, T.S.; Goldring, S. Identification of cell types responsible for bone resorption in rheumatoid arthritis and juvenile rheumatoid arthritis. Am. J. Pathol. 1998, 152, 943. [Google Scholar]
- Janssen, M.; Mihov, G.; Welting, T.; Thies, J.; Emans, P. Drugs and polymers for delivery systems in OA joints: Clinical needs and opportunities. Polymers 2014, 6, 799–819. [Google Scholar] [CrossRef]
- Mitchell, M.J.; Billingsley, M.M.; Haley, R.M.; Wechsler, M.E.; Peppas, N.A.; Langer, R. Engineering precision nanoparticles for drug delivery. Nat. Rev. Drug Discov. 2021, 20, 101–124. [Google Scholar] [CrossRef]
- Abdelbary, G.A.; Khowessah, O.M.; Bakr, A.-H.A.; Abu-Elyazid, S.K. Potential treatment of arthritis with an optimized Mometasone Furoate loaded-ethosomal gel in carrageenan-induced rat joint arthritis. J. Drug Deliv. Sci. Technol. 2020, 57, 101771. [Google Scholar] [CrossRef]
- Cui, Y.; Mo, Y.; Zhang, Q.; Tian, W.; Xue, Y.; Bai, J.; Du, S. Microneedle-assisted percutaneous delivery of paeoniflorin-loaded ethosomes. Molecules 2018, 23, 3371. [Google Scholar] [CrossRef]
- Roky, A.H.; Islam, M.M.; Ahasan, A.M.F.; Mostaq, M.S.; Mahmud, M.Z.; Amin, M.N.; Mahmud, M.A. Overview of skin cancer types and prevalence rates across continents. Cancer Pathog. Ther. 2024, 2, E01–E36. [Google Scholar] [CrossRef] [PubMed]
- Shinu, P.; Nair, A.B.; Kumari, B.; Jacob, S.; Kumar, M.; Tiwari, A.; Tiwari, V.; Venugopala, K.N.; Attimarad, M.; Nagaraja, S. Recent Advances and Appropriate use of Niosomes for the Treatment of Skin Cancer. Indian J. Pharm. Educ. Res. 2022, 56, 924–937. [Google Scholar] [CrossRef]
- Ma, L.; Wang, X.; Wu, J.; Zhang, D.; Zhang, L.; Song, X.; Hong, H.; He, C.; Mo, X.; Wu, S. Polyethylenimine and sodium cholate-modified ethosomes complex as multidrug carriers for the treatment of melanoma through transdermal delivery. Nanomedicine 2019, 14, 2395–2408. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Lin, L.; Choi, Y.; Michniak-Kohn, B. Development and in-vitro evaluation of co-loaded berberine chloride and evodiamine ethosomes for treatment of melanoma. Int. J. Pharm. 2020, 581, 119278. [Google Scholar] [CrossRef]
- Paolino, D.; Celia, C.; Trapasso, E.; Cilurzo, F.; Fresta, M. Paclitaxel-loaded ethosomes®: Potential treatment of squamous cell carcinoma, a malignant transformation of actinic keratoses. Eur. J. Pharm. Biopharm. 2012, 81, 102–112. [Google Scholar] [CrossRef]
- Kotta, S.; Aldawsari, H.M.; Badr-Eldin, S.M.; Nair, A.B.; Kaleem, M.; Dalhat, M.H. Thermosensitive Hydrogels Loaded with Resveratrol Nanoemulsion: Formulation Optimization by Central Composite Design and Evaluation in MCF-7 Human Breast Cancer Cell Lines. Gels 2022, 8, 450. [Google Scholar] [CrossRef]
- Xiong, X.; Zheng, L.-W.; Ding, Y.; Chen, Y.-F.; Cai, Y.-W.; Wang, L.-P.; Huang, L.; Liu, C.-C.; Shao, Z.-M.; Yu, K.-D.; et al. Breast cancer: Pathogenesis and treatments. Signal Transduct. Target. Ther. 2025, 10, 49. [Google Scholar] [CrossRef]
- Li, D.-M.; Feng, Y.-M. Signaling mechanism of cell adhesion molecules in breast cancer metastasis: Potential therapeutic targets. Breast Cancer Res. Treat. 2011, 128, 7–21. [Google Scholar] [CrossRef]
- Apolinário, A.C.; Hauschke, L.; Nunes, J.R.; Lourenço, F.R.; Lopes, L.B. Design of multifunctional ethosomes for topical fenretinide delivery and breast cancer chemoprevention. Colloids Surf. A Physicochem. Eng. Asp. 2021, 623, 126745. [Google Scholar] [CrossRef]
- Nasri, S.; Rahaie, M.; Ebrahimi-Hoseinzadeh, B.; Hatamian-Zarmi, A.; Sahraeian, R. A new ethosomal nanoparticle for controlled release of black cumin compounds against cancer cells. Nanomed. Res. J. 2021, 6, 158–169. [Google Scholar]
- Natsheh, H.; Touitou, E. Phospholipid vesicles for dermal/transdermal and nasal administration of active molecules: The effect of surfactants and alcohols on the fluidity of their lipid bilayers and penetration enhancement properties. Molecules 2020, 25, 2959. [Google Scholar] [CrossRef] [PubMed]
- Morsy, M.A.; Nair, A.B. Prevention of rat liver fibrosis by selective targeting of hepatic stellate cells using hesperidin carriers. Int. J. Pharm. 2018, 552, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Kather, F.S.; Boddu, S.H.S.; Rao, R.; Nair, A.B. Vesicular Carriers for Phytochemical Delivery: A Comprehensive Review of Techniques and Applications. Pharmaceutics 2025, 17, 464. [Google Scholar] [CrossRef] [PubMed]
- Ainbinder, D.; Paolino, D.; Fresia, M.; Touitou, E. Drug delivery applications with ethosomes. J. Biomed. Nanotechnol. 2010, 6, 558. [Google Scholar] [CrossRef]
- Paolino, D.; Lucania, G.; Mardente, D.; Alhaique, F.; Fresta, M. Ethosomes for skin delivery of ammonium glycyrrhizinate: In vitro percutaneous permeation through human skin and in vivo anti-inflammatory activity on human volunteers. J. Control. Release 2005, 106, 99–110. [Google Scholar] [CrossRef]
- Borysowski, J.; Wnukiewicz-Kozłowska, A.; Górski, A. Legal regulations, ethical guidelines and recent policies to increase transparency of clinical trials. Br. J. Clin. Pharmacol. 2020, 86, 679–686. [Google Scholar] [CrossRef]
- Krajnovic, D.; Dragicevic, N. Ethical Considerations in Research Involving Dermal and Transdermal Drug Delivery. In Percutaneous Penetration Enhancers Drug Penetration Into/Through the Skin; Springer: Berlin/Heidelberg, Germany, 2017; pp. 393–403. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Drug Delivered | Formulation | Vesicle Size | Entrapment Efficiency | In Vitro | In Vivo | Reference |
|---|---|---|---|---|---|---|---|
| Diabetes | Repaglinide | Dipalmitoyl phosphatidylcholine (DPPC), ethanol, and water | 0.171–1.727 μm | 56.75–92.28% | Permeation (63.64–96.96%). | An optimized ethosomal formulation, blended into a 1.5% Carbopol 940 gel, provided sustained antidiabetic activity in alloxan-induced diabetic rats compared to oral. | [66] |
| Diabetes | Linagliptin | Soya phospholipids, ethanol, and water | 105.65 ± 0.22 nm | 79.85 ± 0.41% | Drug release of 98.74% over 10 h. | - | [67] |
| Diabetes | Insulin | Lipid-based ionic liquid, ethanol, edge activators | 300 nm | - | - | A nanovesicle formulations effectively lowered blood glucose levels in an animal model. | [68] |
| Diabetes | Glimepiride | Phospholipids, ethanol (10–50%), propylene glycol, and water | 91–224 nm | 42–78% | Ethosomes showed a transdermal flux 3 times higher than liposomes and 25 times higher than a plain drug solution. | - | [69] |
| Diabetes | Dapagliflozin | Cholesterol and soy-lecithin and water | 103.46 ± 2.17 nm to 394.15 ± 1.06 nm | 45–88% | Steady-state flux was 1.93 μg/cm2/h. | - | [70] |
| Hypertension | Carvedilol | Phospholipid, ethanol, water | 46.75 ± 8.0 nm and 259.3 ± 8.02 nm | 86% and 97% | In vitro releases of 70.25 ± 4.26% after 24 h. | - | [71] |
| Pulmonary arterial hypertension | Vardenafil hydrochloride | Phosphatidylcholine and ethanol | 159.9 nm | 81.3% | - | It offered longer systemic exposure and greater bioavailability than oral administration. | [72] |
| Hypertension | Nebivolol | - | 73.50 ± 0.08 nm | 86.46 ± 0.15% | - | Pharmacokinetic studies revealed that OED-TP1 had 7.9 times higher bioavailability than oral Nevilob® tablets. | [73] |
| Hypertension | Carvedilol | Phospholipon 100 H, cholesterol, ethanol, and Transcutol P | 201.55–398.55 nm | 30.00–90.66% | - | A notable, gradual decrease (p < 0.01) in the mean arterial pressure of rats was observed. | [74] |
| Hypertension | Lercanidipine | Phospholipon 90G (PL90G), LER, and ethanol | 210.87 and 400.57 nm | 49.26 to 97.22% | - | The pharmacokinetics study showed a statistically significant (p < 0.05) threefold increase in LER bioavailability with transdermal nanoethosomal LER gel compared to oral LER suspension. | [75] |
| Alzheimer’s disease | Vinpocetine | - | 50.57 ± 26.11 nm | 97.51 ± 0.86% | - | The nanoethosomal formulation exhibited a significant increase in flux and entrapment efficiency compared to the control vinpocetine solution. | [76] |
| Alzheimer’s disease | Rivastigmine | Soya lecithin, ethanol | 140.94 + 22.38 nm | 62.87 ± 9.86% | The sustained effect was observed in this order: transethosomal suspension > ethosomal suspension > liposomal suspension > pure drug solution. | - | [77] |
| Parkinsonism | Rasagiline Mesylate | Ethanol, propylene glycol and phospholipids | 256 nm | 38% | The drug diffused through the nasal mucosa showed improved results, reaching 766 μg/cm2 within 6 h. | - | [78] |
| Parkinsonism | Ropinirole | Soya phosphatidyl choline and ethanol | 320.45 nm | 65.69 ± 3.5% | After 24 h, the optimized formulation showed a 64.8% release compared to the pure drug. | - | [79] |
| Parkinsonism | Rasagiline | Phosphatidylcholine and sodium deoxycholate | 198.63 ± 34.98 nm | 95.73 ± 0.09% | - | The optimal in situ gel demonstrated safety and biocompatibility on rats’ nasal mucosa, with improved brain bioavailability (131.17%). | [80] |
| Arthritis | Apremilast | Soy lecithin, ethanol, and apremilast | 93 nm (E4) to 158 nm | 93.56% | Higher drug level of 1.5% displayed a greater flux of 40.62 μg/cm2/h. | Cmax, plasma drug concentration 319.75 ± 35.28 ng/mL). | [21] |
| Arthritis | Naproxen | PL90G and cholesterol later crosslinked with Carbopol 934 | 251.1 ± 1.80 nm to 343.5 ± 3.23 nm | 66% | Ethosomes-hydrogel exhibited a sustained release effect (>8 h). | It significantly reduced inflammation (84.63%) and paw volume (0.1935 ± 0.08 mL) in Albino Wistar rats with induced arthritis. | [81] |
| Arthritis | Aceclofenac | Ethanol 10–50% (v/v), lecithin 1–4% (w/v), propylene glycol 5–20% (v/v) | 1.112 μm | 91.06 ± 0.79% | After 24 h, the cumulative amount permeated from the optimized ethosomal system (ETP2) was 0.49 ± 0.032 mg/cm2, compared to 0.31 ± 0.036 mg/cm2 from Movon gel. | - | [82] |
| Arthritis | Capsaicin | Phospholipid (2%) mixture was prepared in 30% ethanol | 295 and 271 nm | 61.31 ± 3.45% | Ethosomal capsaicin vesicles showed 72.98 ± 2.84% capsaicin permeation with a flux of 15.20 ± 1.7 cm/h × 10−3 in a modified diffusion cell over 24 h. | Capsaicin-loaded ethosomes significantly reduced carrageenan-induced acute rat paw edema. | [83] |
| Skin cancer | 5-aminolevulinic acid | - | <200 nm | 8–66% | All formulations showed enhancements ranging from 11- to 15-fold compared to the control. | - | [84] |
| Skin cancer | Brucine | Cholesterol, phospholipid, ethanol | 118 ± 1.5 nm to 218 ± 3.0 nm | 50.2 ± 1.8% and 77 ± 1.2% | Over 6 h, the percentage of BRU released was 68.87 ± 3.9% from BRU-loaded gel, 50.87 ± 4.5% from BRU-loaded ethosomes, and 33.67 ± 3.92% from BRU-loaded ethosomal gel. | - | [85] |
| Skin cancer | Tocotrienol | Phospholipid, cholesterol, polysorbate 80, ethanol | 64.9 ± 2.2 nm to 79.6 ± 3.9 nm | 66.8 ± 1.9% and 68.5 ± 1.2% | After 48 h, the cumulative amount was 1.03 ± 0.24 mg/cm2 with a flux of 0.03 ± 0.01 mg/cm2/h. HaCat cells exhibited significantly higher cell viability compared to the pure drug. | The flux of gamma-T3 across the Strat-M® and epidermal membrane was significantly greater than across full-thickness human skin. | [86] |
| Breast cancer | Retinoid fenretinide | Ethanol, propylene glycol, soya lecithin, water, and polysorbate 80 micelles | - | - | - | Oral administration kept plasma FENR levels below 10 ng/g in the first three hours, while MN administration delayed delivery, peaking at a maximum plasma concentration of 52 ng/g after 48 h. | [87] |
| Breast cancer | Raloxifene | - | 109.2 ± 1.52 nm to 150.73 ± 4.10 nm | 11.735 ± 0.19% to 62.65 ± 0.63 | The transdermal flux of the optimized ethosome formulation was 22.14 ± 0.83 µg/mL/cm2, 21 times higher than that of conventional liposomes. | Rats exhibited a 157% higher bioavailability of RXL with the ethosomal formulation compared to oral administration. | [88] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuqbil, R.M.; Aldhubiab, B. Ethosome-Based Transdermal Drug Delivery: Its Structural Components, Preparation Techniques, and Therapeutic Applications Across Metabolic, Chronic, and Oncological Conditions. Pharmaceutics 2025, 17, 583. https://doi.org/10.3390/pharmaceutics17050583
Almuqbil RM, Aldhubiab B. Ethosome-Based Transdermal Drug Delivery: Its Structural Components, Preparation Techniques, and Therapeutic Applications Across Metabolic, Chronic, and Oncological Conditions. Pharmaceutics. 2025; 17(5):583. https://doi.org/10.3390/pharmaceutics17050583
Chicago/Turabian StyleAlmuqbil, Rashed M., and Bandar Aldhubiab. 2025. "Ethosome-Based Transdermal Drug Delivery: Its Structural Components, Preparation Techniques, and Therapeutic Applications Across Metabolic, Chronic, and Oncological Conditions" Pharmaceutics 17, no. 5: 583. https://doi.org/10.3390/pharmaceutics17050583
APA StyleAlmuqbil, R. M., & Aldhubiab, B. (2025). Ethosome-Based Transdermal Drug Delivery: Its Structural Components, Preparation Techniques, and Therapeutic Applications Across Metabolic, Chronic, and Oncological Conditions. Pharmaceutics, 17(5), 583. https://doi.org/10.3390/pharmaceutics17050583