
Formulation and In Vitro Evaluation of Matrix Tablets Containing Ketoprofen–Beta Cyclodextrin Complex for Enhanced Rheumatoid Arthritis Therapy: Experimental and Computational Insights

 , ,
, ,  , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals and Reagents
2.2. Equipment
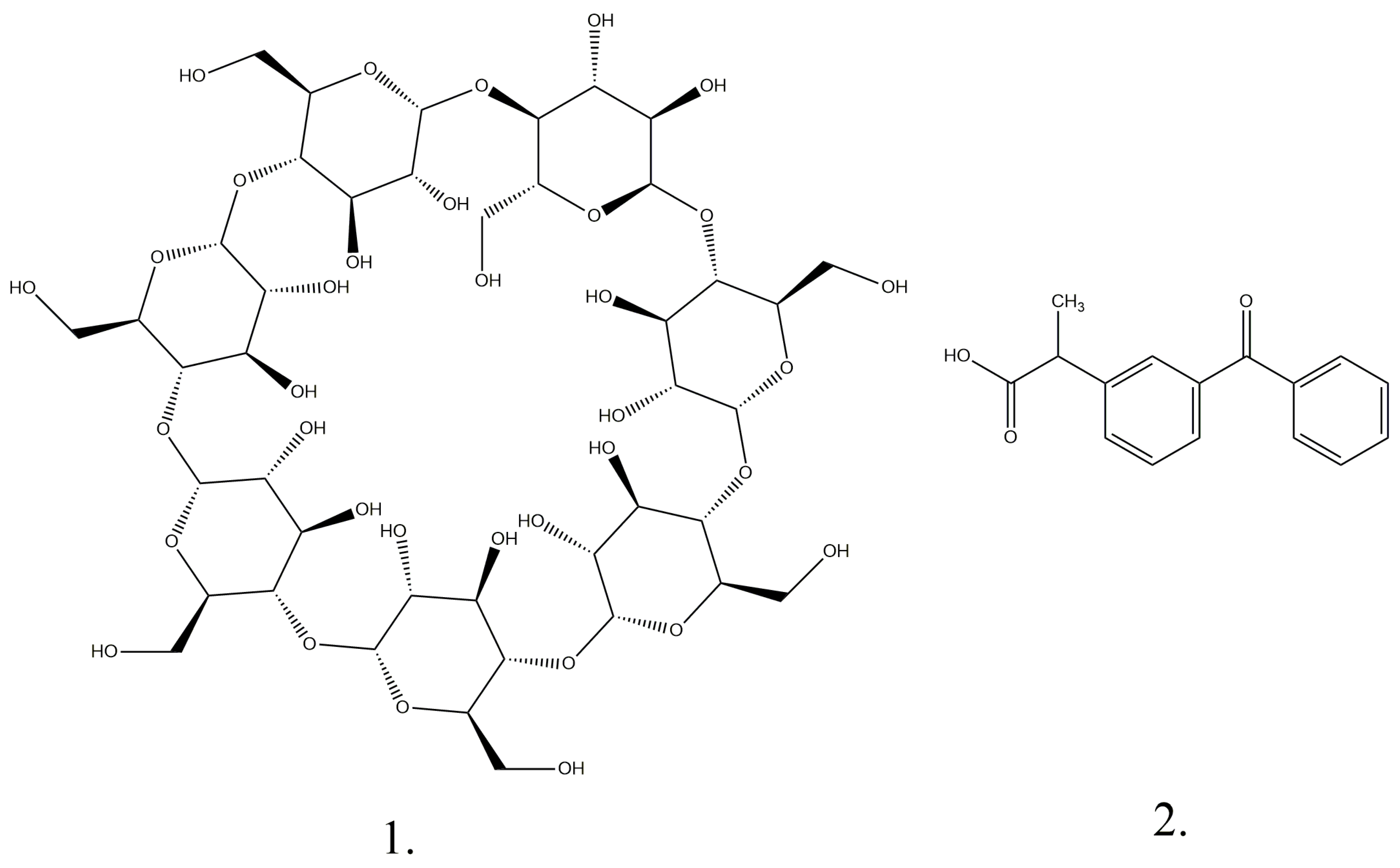
2.3. Preparation of Complexes with Ketoprofen and Beta Cyclodextrin
2.4. Characterization of Complexes with Ketoprofen and Beta Cyclodextrin
2.5. Development of Polymeric Matrix Tablets with Ketoprofen and Ketoprofen–Beta Cyclodextrin
2.6. Dissolution Studies
3. Results and Discussion
3.1. Analyses of the Solid K-β-CD Inclusion Complexes
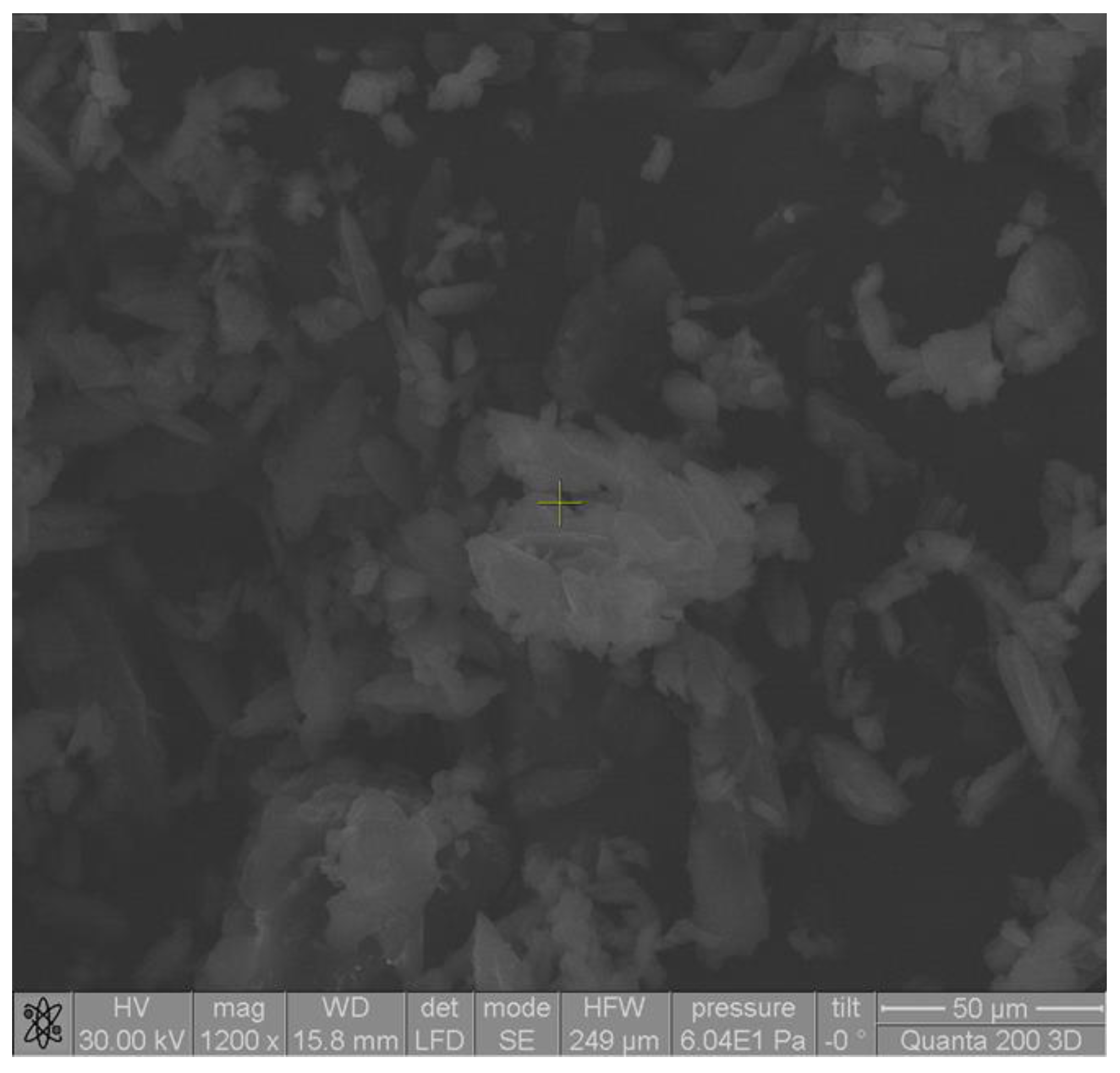
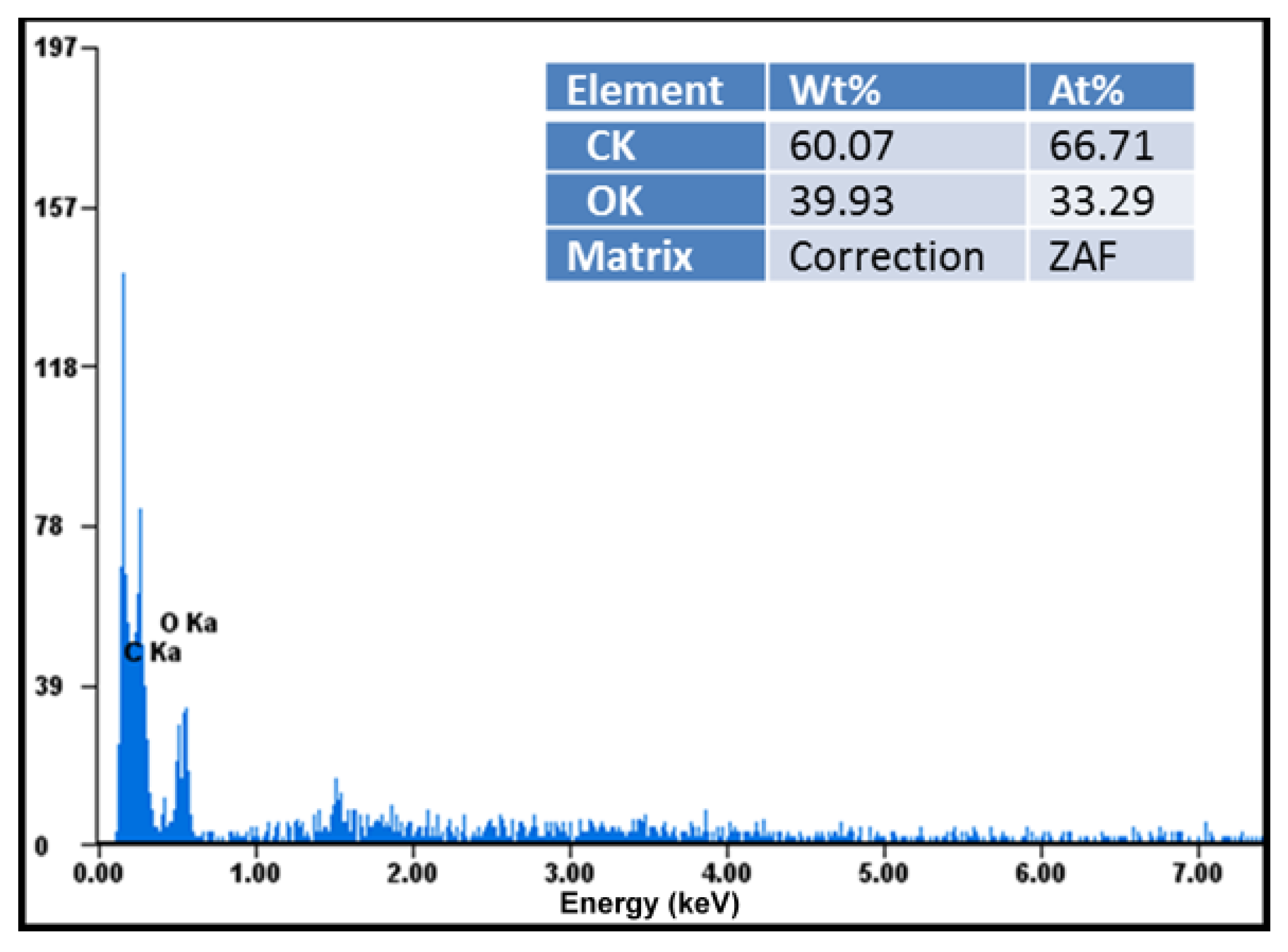
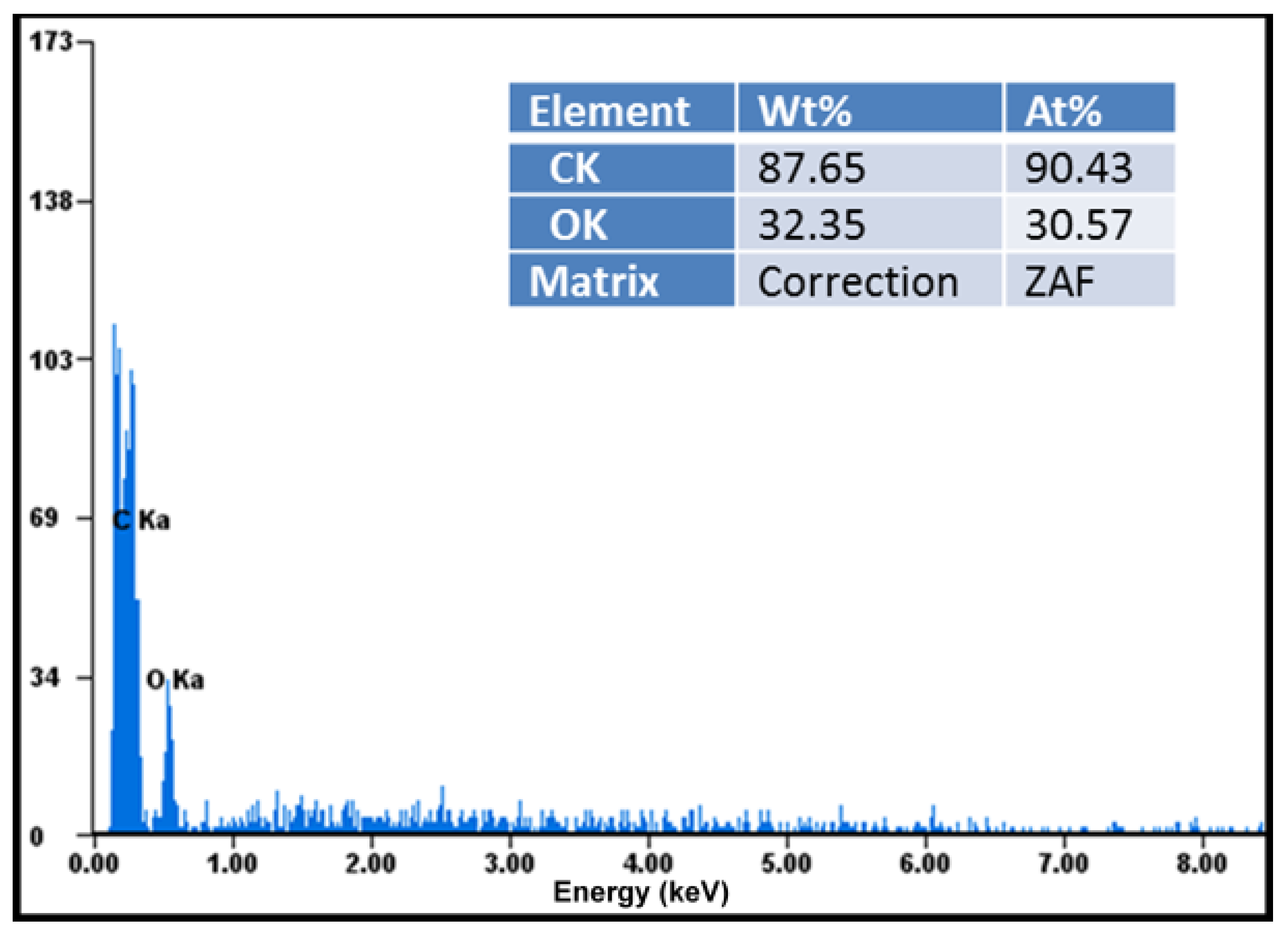
3.1.1. SEM Analysis
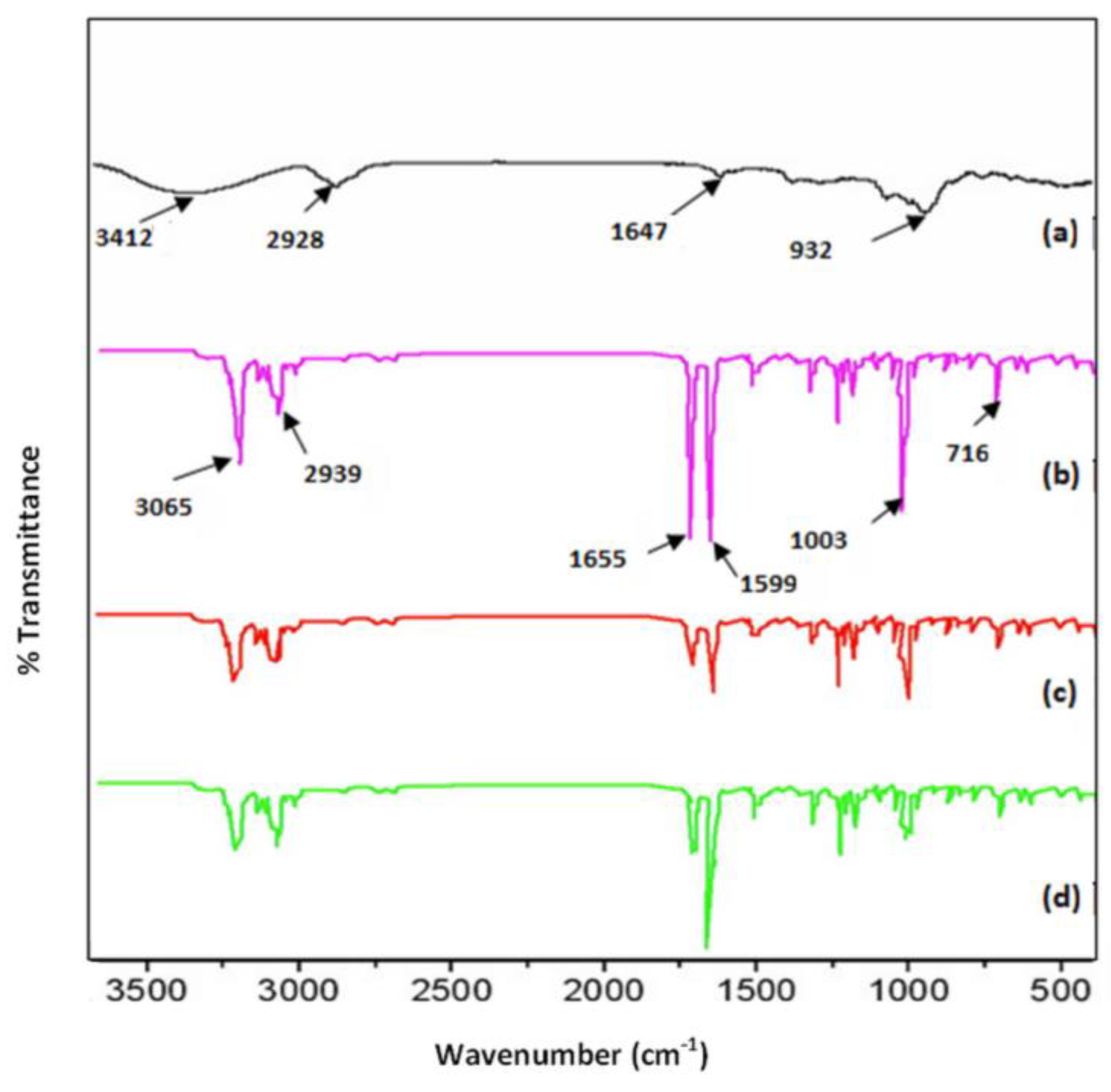
3.1.2. FTIR Analysis
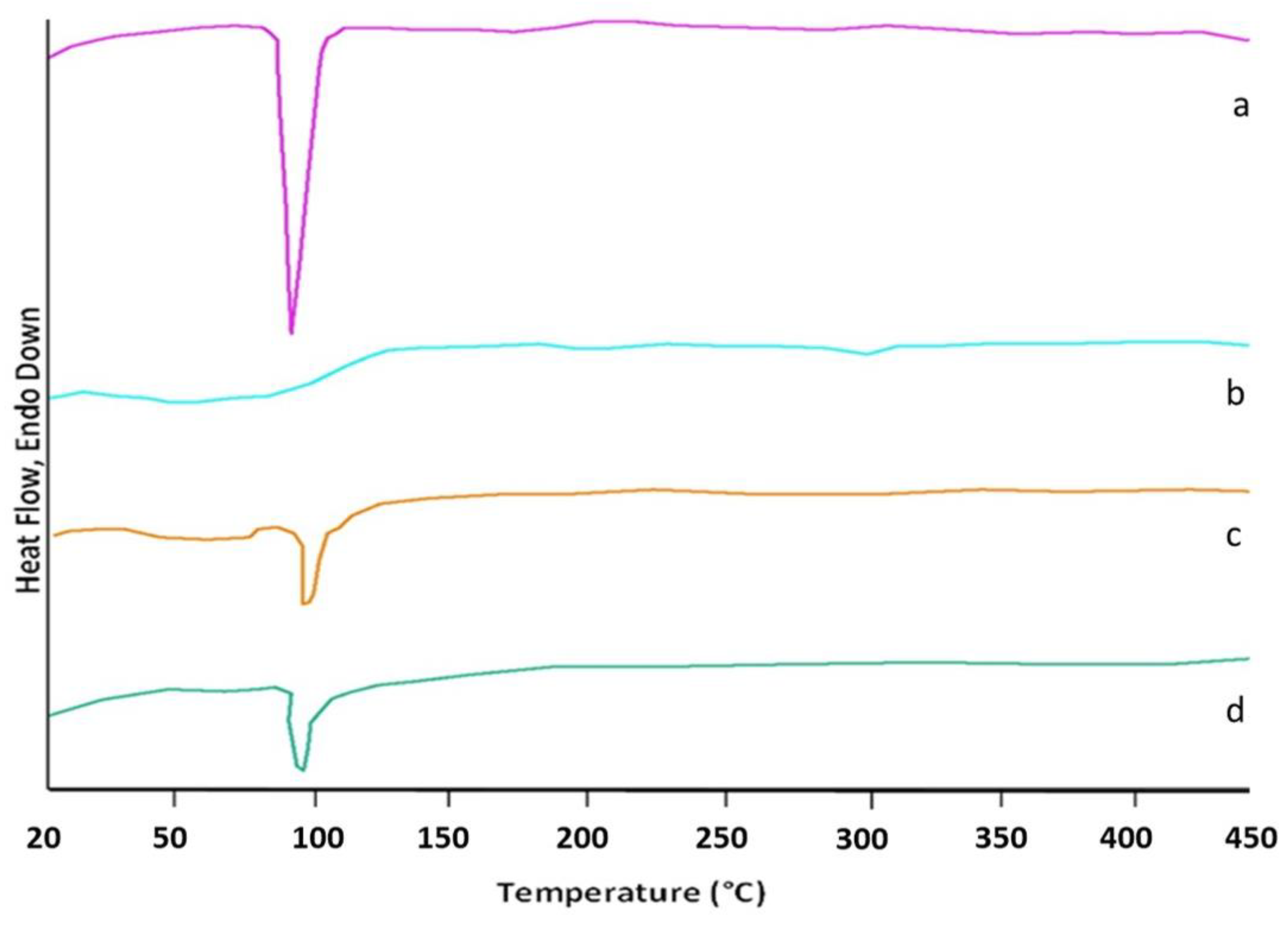
3.1.3. DSC Analysis
3.1.4. In Vitro Drug Dissolution Studies Using Complexes
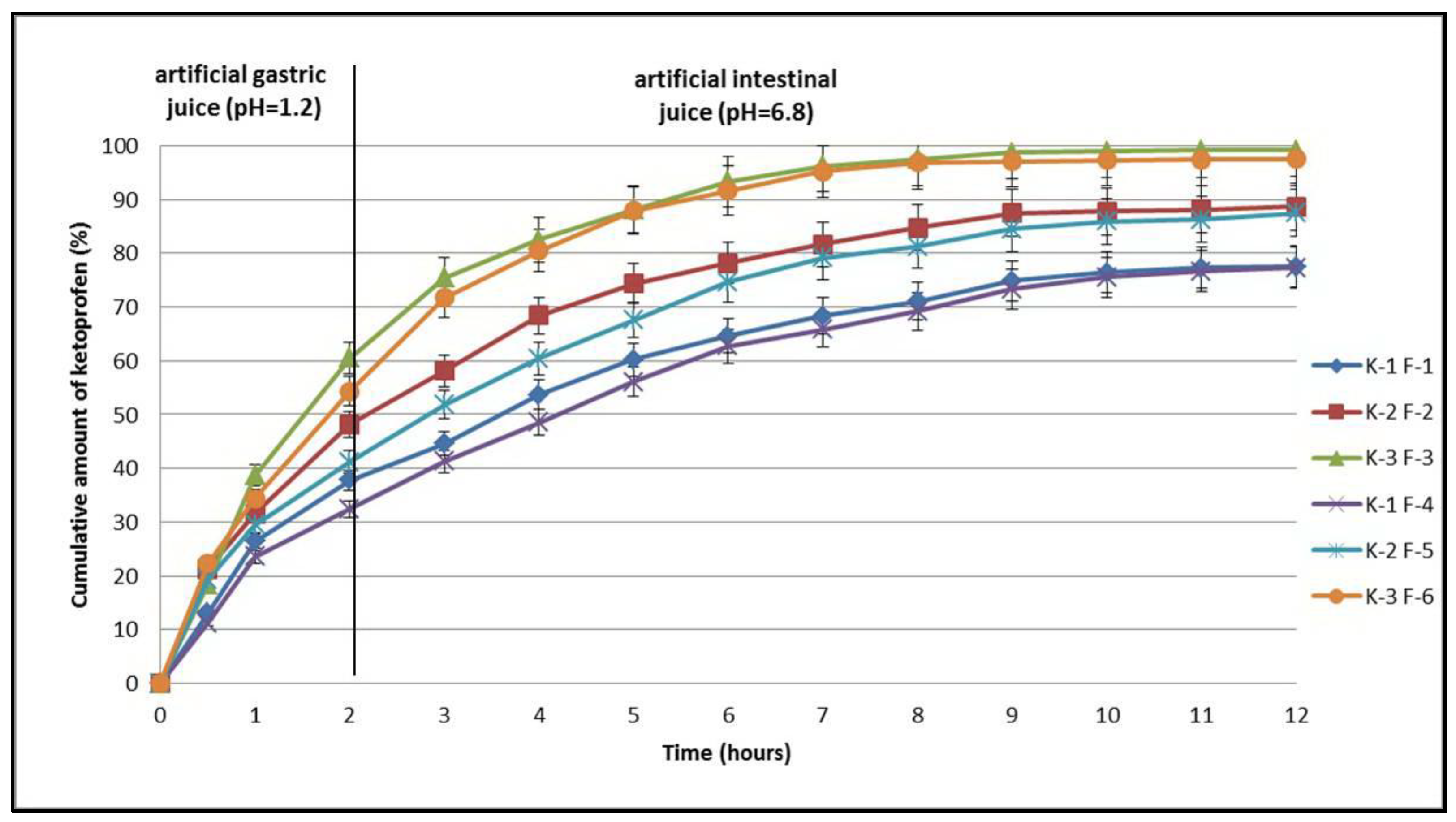
3.2. In Vitro Dissolution Studies Using Tablets
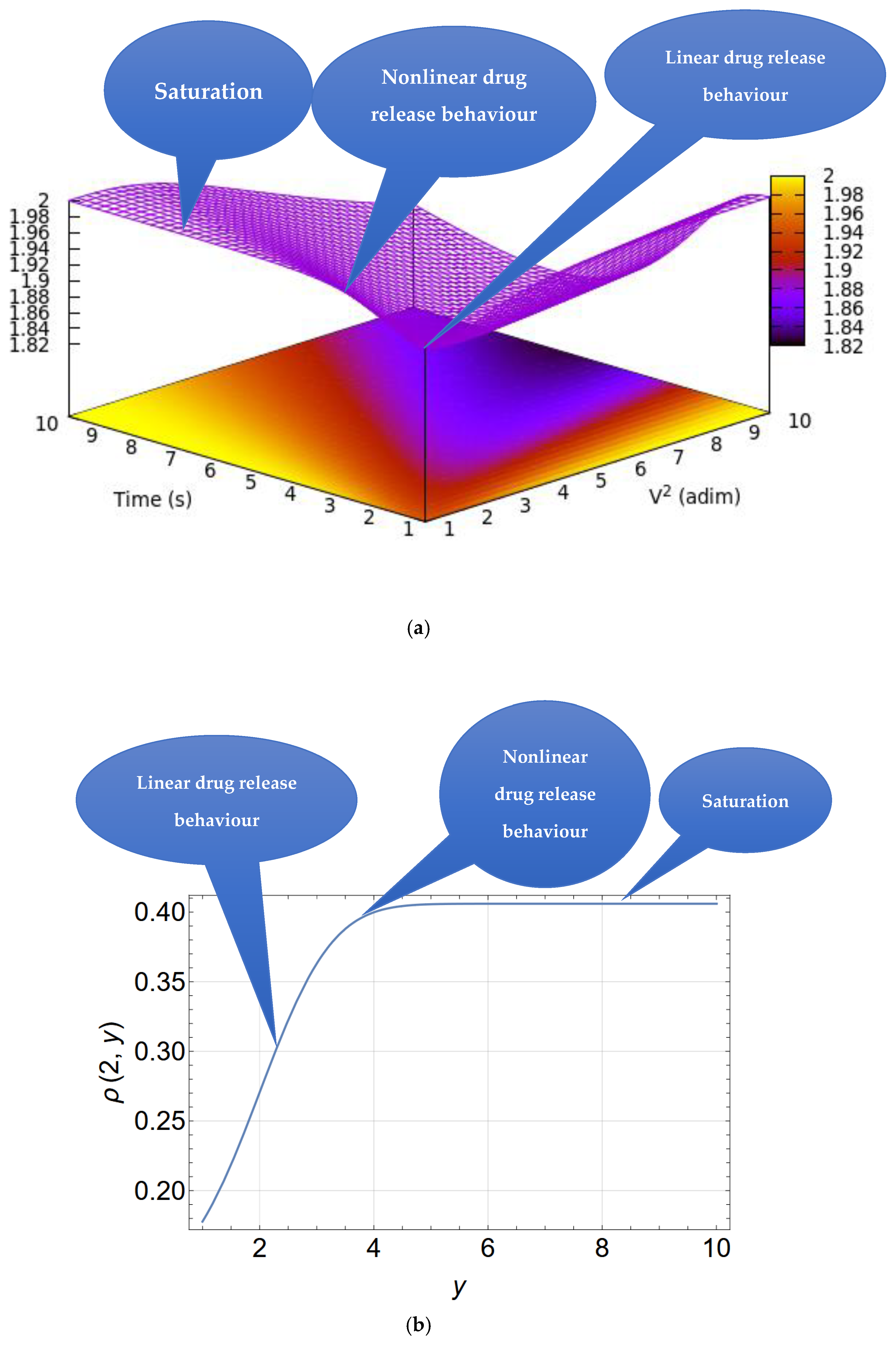
4. Theoretical Model
- (i)
- Nonlinear dynamics and self-similarity over several scales [31,32]: The drug release mechanism in a polymer–drug system is influenced by several elements, including the interaction between the polymer and drug molecules, the architecture of the polymer–drug network, and alterations at both microscopic and macroscopic sizes. This behavior is nonlinear but demonstrates self-similarity across many observational scales; for instance, analogous patterns may emerge when investigations are conducted at differing degrees of granularity. A multifractal, in mathematics, is an entity that demonstrates self-similarity across many scales and possesses nonlinear characteristics, meaning distinct locations may display varying fractal dimensions. Consequently, the behavior of the polymer–drug system may be regarded as self-similar and nonlinear, exhibiting characteristics of multifractality.
- (ii)
- Irregular drug distribution in polymers [32,33]: The polymer network structure is heterogeneous and can vary considerably, resulting in an irregular and non-uniform drug distribution. In a multifractal, the spatial distribution of points or components may be uneven and may display self-similarity across many levels of detail. The intricate architecture of polymers and the mechanisms of drug incorporation and release can be elucidated by mathematical principles related to multifractals.
- (iii)
- Fluctuating fractal dimensions [34]: A significant aspect of multifractals is the fluctuation in fractal dimensions over various sizes. In the polymer–drug system, the physicochemical characteristics, including the drug’s diffusion rate, can fluctuate considerably based on the local circumstances of the polymer network. This behavioral diversity can be likened to the fractal dimensions of a multifractal, which exhibit varying dimensions based on the observational details of the system’s structures.
- (iv)
- Intricate diffusion models [35]: Drug diffusion inside the polymer network may exhibit intricate patterns, where the movement of drug molecules is not only linear but is influenced by the network’s irregular structure. This phenomenon may be characterized using fractal mathematical models, which are employed to elucidate diffusion in irregular and complicated contexts. Fractality can characterize the variability in diffusion rates across several tiers of the polymer structure.
- (v)
- Reliance on local circumstances and scalability impacts [36]: In a polymer–drug system, localized interactions between drug molecules and the polymer network can significantly impact the overall release process, with these effects being applicable across many structural layers. Scalability and reliance on local circumstances are defining features of multifractals, which exhibit self-similarity and sensitivity to small-scale factors. Thus, a correlation can be discerned between these characteristics of the system and multifractals.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| K | ketoprofen |
| K-β-CD | ketoprofen complexed with beta cyclodextrin |
| β-CD | beta cyclodextrin |
| NSAIDs | Nonsteroidal anti-inflammatory drugs |
| SEM | Scanning electron microscopy |
| FTIR | Fourier transform infrared spectroscopy |
| DSC | Differential Scanning Calorimetry |
| EDAX | Energy-Dispersive X-Ray Analysis |
| K-1 F-1 | ketoprofen (tablet formula 1) |
| K-1 F-4 | ketoprofen (tablet formula 4) |
| K-2 F-2 | ketoprofen–beta cyclodextrin (2:1) (tablet formula 2) |
| K-2 F-5 | ketoprofen–beta cyclodextrin (2:1) (tablet formula 5) |
| K-3 F-3 | ketoprofen–beta cyclodextrin (1:1) (tablet formula 3) |
| K-3 F-6 | ketoprofen–beta cyclodextrin (1:1) (tablet formula 6) |
References
- Gao, Y.; Zhang, Y.; Liu, X. Rheumatoid arthritis: Pathogenesis and therapeutic advances. MedComm 2024, 5, e509. Available online: https://onlinelibrary.wiley.com/doi/epdf/10.1002/mco2.509 (accessed on 4 February 2025). [CrossRef] [PubMed]
- O’Neil, L.J.; Rodríguez, D.A.; Deane, K.D. Rheumatoid Arthritis: The Continuum of Disease and Strategies for Prediction, Early Intervention, and Prevention. J. Rheumatol. 2024, 51, 337–349. Available online: https://www.jrheum.org/content/51/4/337 (accessed on 4 February 2025). [CrossRef] [PubMed]
- Kumar, B.; Sahani, V.; Patil, S. Review on Ketoprofen (Anti-Inflammatory Drug). J. Res. Appl. Sci. Biotechnol. 2024, 3, 41–50. [Google Scholar] [CrossRef]
- Kuczynska, J.; Nieradko-Iwanicka, B. New uses of ketoprofen—A review of studies from 2015 to 2021. Curr. Issues Pharm. Med. Sci. 2022, 35, 16–20. [Google Scholar] [CrossRef]
- Shahiwala, A. Cyclodextrin conjugates for colon drug delivery. J. Drug Deliv. Sci. Technol. 2020, 55, 101448. [Google Scholar] [CrossRef]
- Cid-Samamed, A.; Rakamai, J.; Mejuto, J.C.; Simal-Gandara, J.; Astray, G. Cyclodextrins inclusion complex: Preparation methods, analytical techniques and food industry applications. Food Chem. 2022, 384, 132467. [Google Scholar] [CrossRef]
- Betlejewska-Kielak, K.; Bednarek, E.; Budzianowski, A.; Michalska, K.; Maurin, J.K. Comprehensive Characterisation of the Ketoprofen-β-Cyclodextrin Inclusion Complex Using X-ray Techniques and NMR Spectroscopy. Molecules 2021, 26, 4089. [Google Scholar] [CrossRef]
- Mura, P.; Bettinetti, G.P.; Manderioli, A.; Faucci, M.T.; Bramanti, M.; Sorrenti, G. Interactions of ketoprofen and ibuprofen with β-cyclodextrins in solution and in the solid state. Int. J. Pharm. 1998, 166, 189–203. [Google Scholar] [CrossRef]
- Samprasit, W.; Rojanarata, T.; Akkaramongkolporn, P.; Ngawhirunpat, T.; Opanasopit, P. The Influence of Cyclodextrin and pH on the Solubility of Ketoprofen. AMR 2012, 506, 433–436. [Google Scholar] [CrossRef]
- Vilar, G.; Puche, J.T.; Albericio, F. Polymers and drug delivery systems. Curr. Drug Deliv. 2012, 9, 367–394. [Google Scholar] [CrossRef]
- European Directorate for the Quality of Medicines and HealthCare. In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023.
- Stamate, M.I.; Ochiuz, L.; Timofte, D.; Ciuntu, B.; Ghiciuc, C.; Gherman, S.; Stefanache, A.; Stamate, C. Preparation and Pharmaco-Mechanical Characterization of Ketoprofen-Polyvinyl Alcohol Cryogel for Medical Applications. Rev. Chimie 2019, 70, 848–852. [Google Scholar] [CrossRef]
- Stamate, M.I.; Stamate, C.; Timofte, D.; Ciuntu, B.; Gafitanu, C.; Stefanache, A.; Ochiuz, L. Effect of Polymers on the Pharmaco-mechanical Properties of Direct Compressed Tablets with Ketoprofen. Mater. Plast. 2019, 56, 239–244. [Google Scholar] [CrossRef]
- Gafitanu, C.; Stamate, M.I.; Cojocaru, I.C. Formulation and preparation of omeprazol and ketoprofen bi-layer tablets by direct compression method. Farmacia 2015, 63, 672–678. Available online: https://farmaciajournal.com/wp-content/uploads/2015-04-art-17-Gafitanu_574-576.pdf (accessed on 25 January 2025).
- Wehbe, M.; Haslam, A.J.; Jackson, G.; Galindo, A. Phase behaviour and pH-solubility profile prediction of aqueous buffered solutions of ibuprofen and ketoprofen. Fluid Phase Equilibria 2022, 560, 113504. [Google Scholar] [CrossRef]
- Available online: https://www.pharmaexcipients.com/product/carbopol-971p-nf-polymer/ (accessed on 10 January 2025).
- Available online: https://www.chempoint.com/en-emea/products/iff/methocel-water-soluble-cellulose-ethers/methocel-water-soluble-cellulose-ethers/methocel-k4m (accessed on 10 January 2025).
- Available online: https://uk.vwr.com/store/product/25583315/croscarmellose-sodium-nf (accessed on 10 January 2025).
- Available online: https://sapharmachem.com/products/sorbitol-powder-c%E2%98%86pharm-sorbidex-p-16616/ (accessed on 10 January 2025).
- Available online: https://www.fao.org/fileadmin/user_upload/jecfa_additives/docs/monograph17/additive-538-m17.pdf (accessed on 10 January 2025).
- Sha’at, M.; Spac, A.F.; Stoleriu, I.; Bujor, A.; Cretan, M.S.; Hartan, M.; Ochiuz, L. Implementation of QbD Approach to the Analytical Method Development and Validation for the Estimation of Metformin Hydrochloride in Tablet Dosage Forms by HPLC. Pharmaceutics 2022, 14, 1187. [Google Scholar] [CrossRef]
- Romanian Pharmacopoeia Commission National Medicines Agency. Romanian Pharmacopoeia, 10th ed.; Medical Publishing House: Bucharest, Romania, 1993. [Google Scholar]
- Das, S.; Subuddhi, U. Studies on the complexation of diclofenac sodium with beta-cyclodextrin: Influence of method of preparation. J. Mol. Struct. 2015, 1099, 482–489. [Google Scholar] [CrossRef]
- Sarabia-Vallejo, Á.; Caja, M.d.M.; Olives, A.I.; Martín, M.A.; Menéndez, J.C. Cyclodextrin Inclusion Complexes for Improved Drug Bioavailability and Activity: Synthetic and Analytical Aspects. Pharmaceutics 2023, 15, 2345. [Google Scholar] [CrossRef]
- Kfoury, M.; Landy, D.; Fourmentin, S. Characterization of Cyclodextrin/Volatile Inclusion Complexes: A Review. Molecules 2018, 23, 1204. [Google Scholar] [CrossRef]
- Mazurek, A.H.; Szeleszczuk, L. Current status of quantum chemical studies of cyclodextrin host–guest complexes. Molecules 2022, 27, 3874. [Google Scholar] [CrossRef]
- Zhou, H.Y.; Jiang, L.J.; Zhang, Y.P.; LI, J.B. β-Cyclodextrin inclusion complex: Preparation, characterization, and its aspirin release in vitro. Front. Mater. Sci. 2012, 6, 259–267. [Google Scholar] [CrossRef]
- Gowtham, M.; Prachertha, K.; Kurra, V.G. Formulation & evaluation of cyclodextrin complexed tablets by enhancing the dissolution rate. J. Innov. Appl. Pharm. Sci. 2023, 8, 32–42. [Google Scholar] [CrossRef]
- Siepmann, J.; Peppas, N.A. Modeling of drug release from delivery systems based on hydroxypropyl methylcellulose (HPMC). Adv. Drug Deliv. Rev. 2001, 48, 139–157. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Singh, S.; Swain, S. Cyclodextrins: Concept to applications, regulatory issues and challenges. Nanomed. Res. J. 2020, 5, 202–214. [Google Scholar] [CrossRef]
- Iftime, M.M.; Dobreci, D.L.; Irimiciuc, S.A.; Agop, M.; Petrescu, T.; Doroftei, B. A theoretical mathematical model for assessing diclofenac release from chitosan-based formulations. Drug Deliv. 2020, 27, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Nyambura, C.W.; Sampath, J.; Nance, E.; Pfaendtner, J. Exploring structure and dynamics of the polylactic-co-glycolic acid–polyethylene glycol copolymer and its homopolymer constituents in various solvents using all-atom molecular dynamics. J. Appl. Polym. Sci. 2022, 139, e52732. [Google Scholar]
- Srivastava, A.; Yadav, T.; Sharma, S.; Nayak, A.; Kumari, A.A.; Mishra, N. Polymers in drug delivery. J. Biosci. Med. 2015, 4, 69–84. [Google Scholar]
- Pippa, N.; Dokoumetzidis, A.; Pispas, S.; Demetzos, C. The interplay between the rate of release from polymer grafted liposomes and their fractal morphology. Int. J. Pharm. 2014, 465, 63–69. [Google Scholar] [CrossRef]
- Kanjickal, D.G.; Lopina, S.T. Modeling of drug release from polymeric delivery systems—A review. Crit. Rev. Ther. Drug Carrier. Syst. 2004, 21, 345–386. [Google Scholar]
- Herdiana, Y.; Wathoni, N.; Shamsuddin, S.; Muchtaridi, M. Scale-up polymeric-based nanoparticles drug delivery systems: Development and challenges. OpenNano 2022, 7, 100048. [Google Scholar] [CrossRef]
- Agop, M.; Irimiciuc, S.A. Multifractal Theory of Motion: From Small to Large Scales; Springer Nature: Singapore, 2024. [Google Scholar]
- Sha’at, M.; Ignat, M.; Sacarescu, L.; Spac, A.F.; Barsan, A.; Ghizdovat, V.; Ochiuz, L. Multifractal Analysis and Experimental Evaluation of MCM-48 Mesoporous Silica as a Drug Delivery System for Metformin Hydrochloride. Biomedicines 2024, 12, 2838. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stamate Cretan, M.; Ochiuz, L.; Ghizdovat, V.; Molcalut, M.; Agop, M.; Gafițanu, C.A.; Barsan, A.; Sha’at, M.; Stamate, C. Formulation and In Vitro Evaluation of Matrix Tablets Containing Ketoprofen–Beta Cyclodextrin Complex for Enhanced Rheumatoid Arthritis Therapy: Experimental and Computational Insights. Pharmaceutics 2025, 17, 474. https://doi.org/10.3390/pharmaceutics17040474
Stamate Cretan M, Ochiuz L, Ghizdovat V, Molcalut M, Agop M, Gafițanu CA, Barsan A, Sha’at M, Stamate C. Formulation and In Vitro Evaluation of Matrix Tablets Containing Ketoprofen–Beta Cyclodextrin Complex for Enhanced Rheumatoid Arthritis Therapy: Experimental and Computational Insights. Pharmaceutics. 2025; 17(4):474. https://doi.org/10.3390/pharmaceutics17040474
Chicago/Turabian StyleStamate Cretan, Monica, Lacramioara Ochiuz, Vlad Ghizdovat, Monica Molcalut, Maricel Agop, Carmen Anatolia Gafițanu, Alexandra Barsan (Bujor), Mousa Sha’at, and Ciprian Stamate. 2025. "Formulation and In Vitro Evaluation of Matrix Tablets Containing Ketoprofen–Beta Cyclodextrin Complex for Enhanced Rheumatoid Arthritis Therapy: Experimental and Computational Insights" Pharmaceutics 17, no. 4: 474. https://doi.org/10.3390/pharmaceutics17040474
APA StyleStamate Cretan, M., Ochiuz, L., Ghizdovat, V., Molcalut, M., Agop, M., Gafițanu, C. A., Barsan, A., Sha’at, M., & Stamate, C. (2025). Formulation and In Vitro Evaluation of Matrix Tablets Containing Ketoprofen–Beta Cyclodextrin Complex for Enhanced Rheumatoid Arthritis Therapy: Experimental and Computational Insights. Pharmaceutics, 17(4), 474. https://doi.org/10.3390/pharmaceutics17040474