
Clinical Utility and Implementation of Pharmacogenomics for the Personalisation of Antipsychotic Treatments

 , , and
, , and
Abstract
1. Introduction
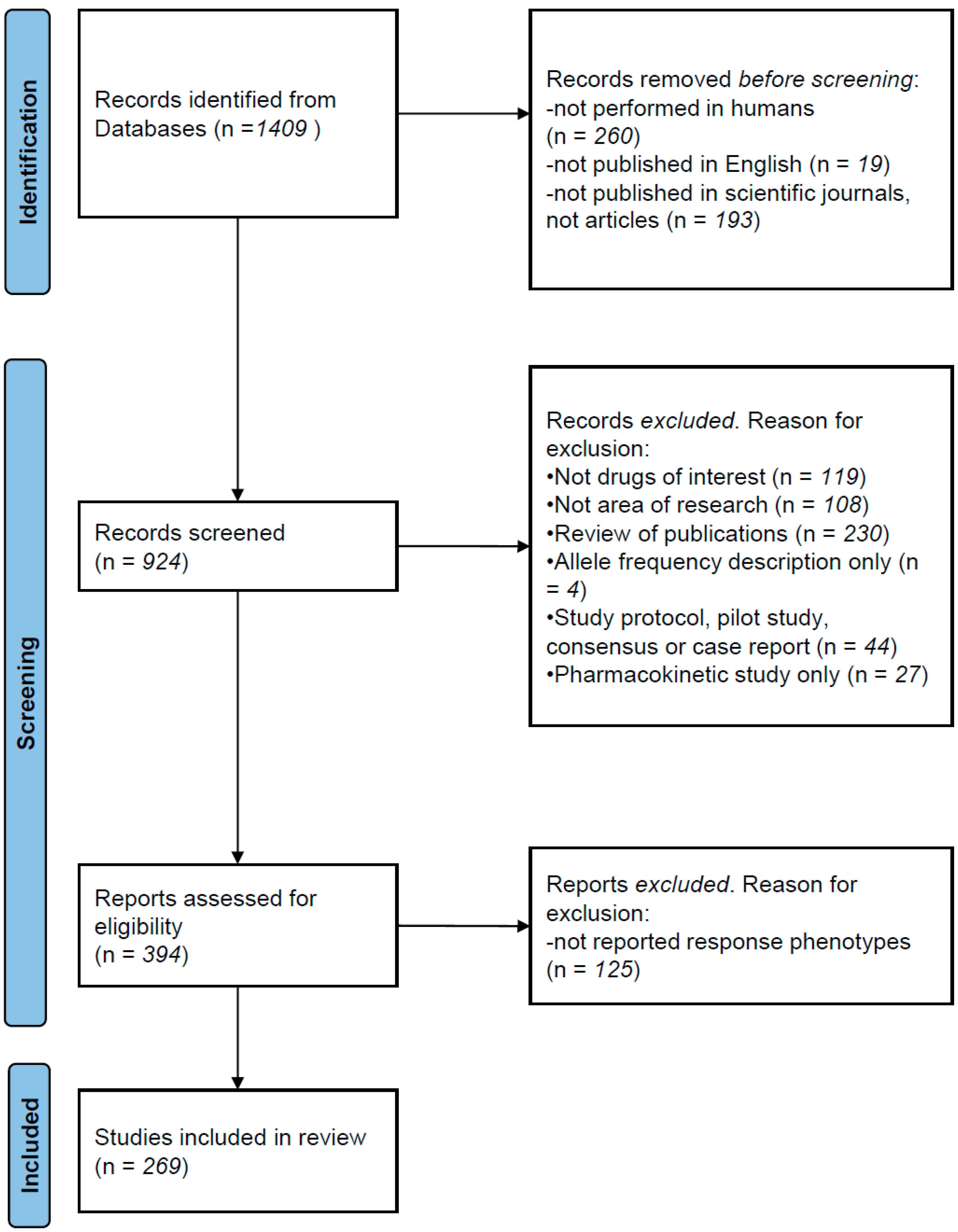
2. Methods
Literature Review
3. Pharmacogenetic Studies
3.1. Pharmacogenetic Associations with Treatment Response
3.2. Pharmacogenetic Associations with Antipsychotic-Induced Adverse Reactions
4. Pharmacogenomic Studies
5. Clinical Utility of Findings
6. Implementation of Pharmacogenetics for Antipsychotics
7. Discussion
8. Conclusions

{kind=link}
| Gene | Variant | Drug | n | Association | Ref. |
|---|---|---|---|---|---|
| 31 genes | 202 SNPs | SGA | 113 Caucasians | Four SNPs in DRD2, SLC18A2, HTR2A and GRIK3 contributed significantly to the risk of side effects (p = 1 × 10−4). | [99] |
| 38 genes | several | SGA | 300 Caucasian | Nominally significant association between antipsychotic dosage and GFRA1 variants. | [100] |
| 380 genes | several | SGA and FGA | 240 several ethnicities | NALCN rs2152324 had most significant association with response (p = 0.004). Not significant after FDR correction. | [101] |
| 74 genes | several | several | 279 Caucasians | BDNF significantly associated with treatment resistance: rs11030104 (OR = 2.57), rs10501087 (OR = 2.19) and rs6265 (OR = 2.08) | [23] |
| ADRB2, DRD3 and SLC6A4 | several | Risperidone | 111 Caucasians | Allele 16Gly of ADRB2 significantly associated with higher risk of sexual adverse events (p = 0.002) | [102] |
| BDNF | 4 SNPs | Clozapine | 257 Caucasians | rs11030104 and Val66Met associated with response (p = 0.04; 0.007, respectively). rs1519480 associated with WG (p = 0.04). | [22] |
| C4A and C4B | several | FGA | 87 Caucasians | Number of copies of C4BL nominally associated with TD severity (p = 0.020) | [103] |
| CNR1, FTO, MC4R, LEP and FAAH | several | Risperidone | 225 Caucasians | Variants in CNR1 (p = 1 × 10−5) and LEP (p = 1.4 × 10−4) associated with AIWG | [41] |
| COMT and DRD2 | several | Risperidone | 690 Chinese | COMT rs4680, DRD2 rs6275, rs1801028 and rs6277 associated with PANSS improvement (p = 0.05) | [19] |
| COMT | rs4680 and rs4818 | SGA | 521 Caucasians | rs4680 A allele and rs4680–rs4818 C-A haplotype associated with olanzapine response, but not with response to other antipsychotics | [20] |
| CYP1A2 and CYP2D6 | several | FGA or Risperidone | 475 Caucasians | CYP1A2*1F & CY2D6*4 associated with TD in patients on antipsychotics for a long time (p = 0.03) | [27] |
| CYP1A2 and CYP2B6 | several | Aripiprazol | 19 Caucasians | CYP1A2 UM & CYP2B6*1/*1 associated with aripiprazol- induced side effects | [104] |
| CYP2C19, LEPR, CYP1A2, HTR2C and ABCB1 | several | Clozapine | 60 Caucasians | Clozapine levels in patients with metabolic syndrome were significantly higher compared to those without (p < 0.01) and were associated with CYP2C19*2 (p = 0.04) | [25] |
| CYP2D6 | several | FGA and SGA | 198 Caucasians | Individuals with either increased or no CYP2D6 activity were at higher risk of having TD | [28] |
| CYP2D6 | several | Risperidone | 257 several ethnicities | Children and adolescents with PM variants showed poorer response to risperidone treatment | [29] |
| CYP2D6 | *4 | Haloperidol | 150 Caucasians | Carriers of *4 variant presented worse safety profile (p < 0.001) | [30] |
| CYP3A4 | several | Olanzapine | CATIE sample | rs472660 significantly predicted olanzapine clearance (p = 5.9 × 10−7). | [105] |
| DISC1 | several | FGA or SGA | 193 Caucasians | Two SNPs nominally associated with TD severity (p < 0.05). | [106] |
| DRD1 | rs4532 | several | 124 Brazilians | G-allele associated with treatment resistance (p = 0.001; adjusted OR = 2.71). GG had five-fold risk compared to A (p = 0.010; OR = 5.56). | [107] |
| DRD2, DRD3, HTR2A, HTR2C, COMT, NQO1, RGS2 and MnSOD | 13 SNPs | not specified | 402 Dutch | DRD2 TaqI associated with akathisia (OR = 2.3, p = 0.001), DRD2 −141C associated with TD (OR = 0.20, p = 0.001) | [32] |
| DRD2 | rs2514218 | Haloperidol and Risperidone | 100 Americans | In the aripiprazole group, C/C homozygotes had more akathisia; in the risperidone group, male T allele carriers had greater prolactin elevations | [37] |
| DRD2 and DRD3 | rs1800497, rs6277 and rs6280 | Cariprazine | 20 Caucasians | DRD2 rs1800497 and rs6277 associated with cariprazine response | [9] |
| DRD2 and DRD3 | several | SGA | 129 Caucasians | DRD2 rs1799732, DRD3 rs6280, and HTR2A rs7997012 associated with treatment resistance. | [10] |
| DRD3, DRD2, HTR2A, HTR2C, COMT and MTHFR | several | several | 329 Caucasians | DRD3 9Gly and MTHFR 677-T had better response (p = 0.034 and p = 0.019, respectively). | [7] |
| DRD4, HTR2A, TPH1, SLC18A1 and COMT | several | Haloperidol | 198 Tartars | Several associations of DRD4, HTR2A, TPH1 and SLC18A1 polymorphisms with antipsychotic response | [8] |
| EP300 | expression levels | several | 226 Caucasians | EP300 expression levels significantly associated with increases in BMIR, cholesterol levels and triglyceride concentrations | [108] |
| FKBP5, NR3C1, BDNF and NTRK2 | several | Clozapine | 591 Caucasians | Several associations between FKBP5 rs1360780, NTRK2 rs1778929 and rs10465180 with response | [109] |
| FTO | several | SGA | 259 + 91 Caucasians | In a subpopulation without additional weight-inducing comedication (n = 178), rs7185735-G carriers gained 3.4 times more weight (1.69 ± 3.1 kg, p = 0.019) | [110] |
| GLP1R | several | SGA | 464 Caucasians | Haplotypes associated with response to olanzapine (p = 0.002), perphenazine (p = 0.01), quetiapine (p = 0.008), risperidone (p = 0.02) and ziprasidone (p = 0.007) | [111] |
| GRIN2A, DRD3, HTR2C, DRD4 and GRIN2B | 42 SNPs | FGA or SGA | 431 + 168 Caucasians | Several significant associations with TD were identified, but only GRIN2A (rs1345423) was found in both patient populations | [112] |
| GRM3 | rs1468412 | Risperidone | 61 Caucasians | GRM3 rs1468412 associated with worsening spatial working | [113] |
| HLA | several | Clozapine | 180 neutropenia/ 1396 controls | HLA-DQB1 rs113332994 associated with clozapine-induced agranulocytosis (OR = 16.31) | [45] |
| HRH1 and CHRM3 | several | Several | 430 Caucasians | HRH1 haplotype rs346074–rs346070 associated with BMI (p = 0.025) and obesity (p = 0.005) in patients using high-H1 affinity antipsychotics | [15] |
| HRH3 | several | Risperidone | 129 Han Chinese | rs3787429 (p = 0.013–0.087) and rs3787430 (p = 0.024–0.010) associated with efficacy after 4–8 weeks, respectively | [16] |
| HRH4 | 5 SNPs | Risperidone | 113 Han Chinese | rs4483927 TT genotype predicts poor therapeutic response on the positive, negative, general and total scales of PANSS scores (p = 0.017, 0.019, 0.021 and 0.002, respectively) | [17] |
| HSD11B1 | several | SGA | 478 Caucasians | HSD11B1 rs846910-A, rs375319-A and rs4844488-G allele carriers associated with lower BMI in women | [114] |
| HTR2A | rs6313 | Olanzapine or Risperidone | 221 Caucasians | T allele carriers showed better response than non-carriers | [12] |
| HTR2C | −759T/C | SGA | 48 female Caucasians | T allele carriers gained less weight as compared to patients who did not have the allele | [36] |
| HTR2C | −759T/C | Risperidone | 108 Thai | 5-HT2C -759-T/C associated with hypertension but not with WG | [39] |
| HTR3A | rs1062613 and rs2276302 | several | 101 Indian patients | rs1062613-T and rs2276302-G alleles significantly associated with good clinical response to clozapine (p = 0.02) | [13] |
| HTR7 | several | Aripiprazol | 100 Japanese | rs12412496-rs7916403-rs1935349 A-T-A haplotype correlated with worse improvement in the cognition score (p = 0.046). | [115] |
| LEP and LEPR | several | FGA or SGA | 181 Caucasians | Significant association between a LEP haplotype (rs7799039G–rs10954173G–rs3828942G) and AIWG (p = 0.035) | [40] |
| MAOA, MAOB, DRD1, DRD2, DRD3, DRD4 and SLC6A3 | 41 SNPs | FGA or SGA | 446 Caucasians | Association between MAOB rs1799836 and HPRL in men. SLC6A3 rs40184 and rs3863145 associated with HPRL in risperidone/paliperidone subgroup | [116] |
| MC4R | rs489693 | SGA 4 weeks | 341 Caucasians | rs489693 A/A carriers showed 2.2 times higher weight increase than carriers of the C/C genotype (p = 0.039) | [43] |
| MC4R | rs17782313 | SGA 4 weeks | 51 Caucasians | rs17782313 C/C carriers higher risk of WG and BMI increase, with a dose effect of the C-allele (p = 0.002). | [117] |
| MC4R | rs489693 and rs17782313 | FGA or SGA | 1991 Chinese | Recessive effects of rs489693 on AIWG, WC and triglyceride change %, with A/A incurring more metabolic adverse effects | [44] |
| MC4R | rs17782313 | Amisulpride and Olanzapine | 212 Several | C carriers had higher WG than T homozygotes | [35] |
| NEUROD2 | several | SGA | 167 Caucasians | rs11078918 and rs12453682 associated with change in neuropsychological test results (p = 0.02–0.001). | [118] |
| NOS1AP | rs1214382 and rs10494366 | not specified | 347 Caucasian | rs12143842-CC and rs10494366-TT male carriers show positive correlation of QTc length with antipsychotic dosage | [119] |
| NPY5R | several | FGA and SGA | 99 Russians | rs11100494- C predisposes to AIWG (OR = 33.48, p< 0.001) | [120] |
| OXTR, CNR1, DDC and DRD2 | several | Clozapine or SGA | 196 Chileans | OXTR rs2228485, CNR1 rs806368 and rs1049353, and DDC rs10499696 associated with treatment resistance (p by genotype: 0.02, 0.001, 0.001 and 0.0003, respectively) | [121] |
| PLEKHA6 | rs7513240, rs4951353 | not specified | 263 Caucasians | rs7513240 and rs4951353 (A/G) associated with therapy response with different PANSS improvement after 4 weeks | [122] |
| PRKAR2B | 16 SNPs | Clozapine and Olanzapine | 99 Caucasians | rs9656135 minor allele carriers higher weight increase during treatment. | [123] |
| PTPRD | 4 SNPs | Clozapine or Olanzapine | 201 Caucasians and Africans | rs73398242 associated with AIWG in Europeans (p = 0.002) and with rs13294608 in African Americans (p = 0.003). | [124] |
| RELN | 15 SNPS | SGA | 260 Chinese | Two SNPs associated with antipsychotic treatment response (rs155333, p = 0.010 and rs6465938, p = 0.049) | [125] |
| RGS2 | several | Haloperidol | 258 Russians | RGS2*T/*T (rs2746073), *C/*C (rs4606) and *A/*A (rs2746071) associated with increased risk of antipsychotic-induced Parkinsonism | [126] |
| SLC18A2 | 9 SNPs | FGA long-term | 217 Caucasians | rs2015586 and rs363224 SNPs associated with TD and AIMS scores. | [127] |
| SLC6A5, GAD1, GRIA1, GRIA3, GRIA4, GRID2, GRIK1, GRIK2, GRIK3, GRIK4, GRIN2B, GRM1 and GRM4 | 62 SNPs | several | 101 + 71 + 118 Caucasian patients | SLC6A5 rs2298826 associated with a rapid rise of motor side effects at the beginning of the treatment (p = 0.0002) | [128] |
| SNAP25 | several | SGA and FGA | 3243 Chinese | rs6039769 significantly associated with AIWG (p < 0.001). | [129] |
| SULT4A1 | rs2285162 and rs2285167 | Olanzapine | 87 Caucasians | rs2285162 [A]-rs2285167 [G] haplotype superior olanzapine response (p = 0.004) and less AIWG per month (p = 0.04) | [130] |
| SV2C | 106 SNPs | SGA | 466 Caucasians | rs11960832-T/T significantly worse response to olanzapine treatment (p = 2.94 × 10−5; FDR = 2.18 × 10−2) | [131] |
| UGT1A4, UGT1A4 and ABCB1 | 7 SNPs | Olanzapine | 91 Japanese | Sympathetic nervous activity higher in individuals with the UGT1A4 rs2011425 G allele (p = 0.001). | [132] |
| Strategy | n | Treatment | Association | Ref. |
|---|---|---|---|---|
| GWAS | 122 + 174 Japanese | several | Association DPP6 rs6977820 with antipsychotic-induced TD (p = 0.008) | [55] |
| GWAS | 96 + 169 Caucasians | FGA or SGA | Two SNPs (rs7912580 and rs2412459) associated with response in both samples, located between ARID5B and RTKN2 genes | [48] |
| GWAS and WES | 163 Caucasians | Clozapine | HLA-DQB1 (126Q) (p = 4.7 × 10−14, OR = 0.19) and HLA-B (158T) (p = 6.4 × 10−10, OR = 3.3) associated with clozapine-induced agranulocytosis | [46] |
| Array 1995 genes | 89 Caucasians | Olanzapine or Risperidone | Significant associations between treatment response and SNPs in the chromosome 6, where the human leukocyte antigen (HLA) is located | [49] |
| GWAS | 189 + 86 Caucasians | SGA | OGFRL1 rs9346455 significantly associated with AIWG (p = 0.005) | [57] |
| WES | 11 + 103 + 87 several ethnicities | FGA or SGA | rs13025959 in MYO7B (E1647D) and rs10380 in MTRR (H622Y) associated with antipsychotic response | [51] |
| GWAS | 742 Indians | FGA or SGA | CCL2 rs4795893 (p = 7.62 × 10−4) and rs4586 (p = 1.13 × 10−3), GRIA4 rs2513265 (p = 1.44 × 10−3), ADCY2 rs1544938 (p = 7.68 × 10−4), and NRG1 rs13250975 (p = 6.81 × 10−3) and rs17716295 (p = 8.71 × 10−3) associated with response | [50] |
| GWAS | 534 + 547 Chinese | SGA | PTPRD rs10977144 (p = 9.26 × 10−9) and rs10977154 (p = 4.53 × 10−8), and GFPT2 rs12386481 (p = 1.98 × 10−7) associated with AIWG | [58] |
| GWAS | 50 + 380 Japanese | Clozapine | Variants in the human leukocyte antigen (HLA) region (rs1800625, p = 3.46 × 10−9, OR = 3.8) associated with agranulocytosis | [47] |
| WES | 316 + 1920 Chinese | FGA or SGA | Rare genetic variants in NMDA and AMPA enriched in the non-responder group | [52] |
| WES | 82 Jewish | not specified | RIMS2 showed significant enrichment of qualifying variants in TD patients (n = 39) (p = 5.32 × 10−8) | [56] |
| GWAS | 552 African ancestry | Clozapine | ACKR1 rs2814778-C/C carriers more likely to develop neutropenia and have to stop clozapine treatment (OR = 20.4, p = 3.44 × 10−7) | [60] |
| Sequencing 143 genes | 79 + 159 Han Chinese | Olanzapine | rs324026 (p = 0.023) and rs12610827 (p = 0.043) associated with response | [54] |
| GWAS | 339 several ethnicities | Amisulpride | Significant association in a locus not previously associated with AIWG (rs78310016; p = 3.66 × 10−8). Minor allale carriers had an OR of 3.98 (p = 1 × 10−3) for AIWG | [59] |
| GWAS | 2040 Chinese | FGA or SGA | ATAD3B rs20005072 and SKIL rs186507741 associated with antipsychotic-induced QTc interval change. | [61] |
| GWAS and WES | 189 + 222 Chinese | Risperidone | GWAS revealed a significant association between GRM7 SNPs (rs141134664, rs57521140 and rs73809055) and treatment response | [53] |
Summative Paragraph
- Genetic variants in genes coding for drug targets -dopamine and serotonin receptors in particular- may influence the efficacy and safety of antipsychotic medications.
- Functional variants in CYPs are associated with antipsychotic availability.
- Dose adjustment according to CYP functional variants present may help to improve adherence, efficacy and safety of antipsychotics.
- Clinical implementation of pharmacogenetic interventions for personalisation of antipsychotic treatment is limited.
- Improved clinical guidelines based on pharmacogenetic data, education and training in pharmacogenetics, reduced costs and shorter delivery times may increase implementation.
- Further research on the combined effect of pharmacogenetics, phenoconversion, and clinical and environmental factors is required.
Funding
Data Availability Statement
Conflicts of Interest
References
- Carbon, M.; Correll, C.U. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin. Neurosci. 2014, 16, 505–524. [Google Scholar] [CrossRef]
- Arranz, M.J.; Salazar, J.; Hernandez, M.H. Pharmacogenetics of antipsychotics: Clinical utility and implementation. Behav. Brain Res. 2021, 401, 113058. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Muller, D.J. Pharmacogenetics of Antipsychotic Drug Treatment: Update and Clinical Implications. Mol. Neuropsychiatry 2020, 5 (Suppl. S1), 1–26. [Google Scholar] [CrossRef] [PubMed]
- Arranz, M.J.; Gonzalez-Rodriguez, A.; Perez-Blanco, J.; Penades, R.; Gutierrez, B.; Ibanez, L.; Arias, B.; Brunet, M.; Cervilla, J.; Salazar, J.; et al. A pharmacogenetic intervention for the improvement of the safety profile of antipsychotic treatments. Transl. Psychiatry 2019, 9, 177. [Google Scholar] [CrossRef]
- Beunk, L.; Nijenhuis, M.; Soree, B.; de Boer-Veger, N.J.; Buunk, A.M.; Guchelaar, H.J.; Houwink, E.J.F.; Risselada, A.; Rongen, G.; van Schaik, R.H.N.; et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2D6, CYP3A4 and CYP1A2 and antipsychotics. Eur. J. Hum. Genet. 2023, 1–8. [Google Scholar] [CrossRef]
- Vasiliu, O. The pharmacogenetics of the new-generation antipsychotics—A scoping review focused on patients with severe psychiatric disorders. Front. Psychiatry 2023, 14, 1124796. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Burger, H.; Wilffert, B.; Al Hadithy, A.; Alizadeh, B.Z.; Snieder, H.; GROUP investigators. Clinical response to antipsychotic drug treatment: Association study of polymorphisms in six candidate genes. Eur. Neuropsychopharmacol. 2012, 22, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Gareeva, A.E.; Kinyasheva, K.O.; Galaktionova, D.Y.; Sabirov, E.T.; Valinourov, R.G.; Chudinov, A.V.; Zasedatelev, A.S.; Nasedkina, T.V.; Khusnutdinova, E.K. Brain neurotransmitter systems gene Polymorphism: The Search for pharmacogenetic markers of efficacy of haloperidol in Russians and Tatars. Mol. Biol. 2015, 49, 959–967. [Google Scholar] [CrossRef]
- De Pieri, M.; Ferrari, M.; Marino, F.; Traber, R.; Bolla, E.; Cosentino, M. Functional single nucleotide polymorphisms in dopaminergic receptors D2 predict clinical response to Cariprazine. Front. Pharmacol. 2023, 14, 1182393. [Google Scholar] [CrossRef]
- Del Casale, A.; Simmaco, M.; Modesti, M.N.; Zocchi, C.; Arena, J.F.; Bilotta, I.; Alcibiade, A.; Sarli, G.; Cutillo, L.; Antonelli, G.; et al. DRD2, DRD3, and HTR2A single-nucleotide polymorphisms involvement in high treatment resistance to atypical antipsychotic drugs. Biomedicines 2023, 11, 2088. [Google Scholar] [CrossRef]
- Liu, C.; Xu, X.; Liu, X.; Zhang, T.; Li, Y.; Yan, P. DRD3 Ser9Gly polymorphism and treatment response to antipsychotics in schizophrenia: A meta-analysis. Neurosci. Lett. 2022, 786, 136788. [Google Scholar] [CrossRef] [PubMed]
- Maffioletti, E.; Valsecchi, P.; Minelli, A.; Magri, C.; Bonvicini, C.; Barlati, S.; Sacchetti, E.; Vita, A.; Gennarelli, M. Association study between HTR2A rs6313 polymorphism and early response to risperidone and olanzapine in schizophrenia patients. Drug Dev. Res. 2020, 81, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, A.P.; Poonkuzhali, B.; Kuruvilla, A.; Jacob, M.; Jacob, K.S. Clinical predictors of serum clozapine levels in patients with treatment-resistant schizophrenia. Int. Clin. Psychopharmacol. 2013, 28, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Gressier, F.; Porcelli, S.; Calati, R.; Serretti, A. Pharmacogenetics of clozapine response and induced weight gain: A comprehensive review and meta-analysis. Eur. Neuropsychopharmacol. 2016, 26, 163–185. [Google Scholar] [CrossRef] [PubMed]
- Vehof, J.; Risselada, A.J.; Al Hadithy, A.F.; Burger, H.; Snieder, H.; Wilffert, B.; Arends, J.; Wunderink, L.; Knegtering, H.; Wiersma, D.; et al. Association of genetic variants of the histamine H1 and muscarinic M3 receptors with BMI and HbA1c values in patients on antipsychotic medication. Psychopharmacology 2011, 216, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Wang, L.; Zhang, M.; Xuan, J.; Wang, Y.; Liu, B.; Shao, L.; Li, J.; Zeng, Z.; Li, T.; et al. A pharmacogenetic study of risperidone on histamine H3 receptor gene (HRH3) in Chinese Han schizophrenia patients. J. Psychopharmacol. 2012, 26, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Wang, L.; Yu, T.; Wang, Y.; Sun, L.; Wang, T.; Huo, R.; Li, Y.; Wu, X.; Qin, S.; et al. Histamine H4 receptor polymorphism: A potential predictor of risperidone efficacy. J. Clin. Psychopharmacol. 2013, 33, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Schacht, J.P. COMT val158met moderation of dopaminergic drug effects on cognitive function: A critical review. Pharmacogenom. J. 2016, 16, 430–438. [Google Scholar] [CrossRef]
- Han, C.J.; Kohen, R.; Jun, S.; Jarrett, M.E.; Cain, K.C.; Burr, R.; Heitkemper, M.M. COMT Val158Met Polymorphism and Symptom Improvement Following a Cognitively Focused Intervention for Irritable Bowel Syndrome. Nurs. Res. 2017, 66, 75–84. [Google Scholar] [CrossRef][Green Version]
- Nikolac Perkovic, M.; Sagud, M.; Zivkovic, M.; Uzun, S.; Nedic Erjavec, G.; Kozumplik, O.; Svob Strac, D.; Mimica, N.; Mihaljevic Peles, A.; Pivac, N. Catechol-O-methyltransferase rs4680 and rs4818 haplotype association with treatment response to olanzapine in patients with schizophrenia. Sci. Rep. 2020, 10, 10049. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, M.; Zhou, W.; Li, M.; Huai, C.; Shen, L.; Wang, T.; Wu, H.; Zhang, N.; Zhang, Z.; et al. Association Between the COMT Val158Met Polymorphism and Antipsychotic Efficacy in Schizophrenia: An Updated Meta-Analysis. Curr. Neuropharmacol. 2021, 19, 1780–1790. [Google Scholar] [CrossRef]
- Zai, G.C.; Zai, C.C.; Chowdhury, N.I.; Tiwari, A.K.; Souza, R.P.; Lieberman, J.A.; Meltzer, H.Y.; Potkin, S.G.; Müller, D.J.; Kennedy, J.L. The role of brain-derived neurotrophic factor (BDNF) gene variants in antipsychotic response and antipsychotic-induced weight gain. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2012, 39, 96–101. [Google Scholar] [CrossRef]
- Zhang, J.P.; Lencz, T.; Geisler, S.; DeRosse, P.; Bromet, E.J.; Malhotra, A.K. Genetic variation in BDNF is associated with antipsychotic treatment resistance in patients with schizophrenia. Schizophr. Res. 2013, 146, 285–288. [Google Scholar] [CrossRef]
- Kneller, L.A.; Zubiaur, P.; Koller, D.; Abad-Santos, F.; Hempel, G. Influence of CYP2D6 Phenotypes on the Pharmacokinetics of Aripiprazole and Dehydro-Aripiprazole Using a Physiologically Based Pharmacokinetic Approach. Clin. Pharmacokinet. 2021, 60, 1569–1582. [Google Scholar] [CrossRef] [PubMed]
- Vasudev, K.; Choi, Y.H.; Norman, R.; Kim, R.B.; Schwarz, U.I. Genetic Determinants of Clozapine-Induced Metabolic Side Effects. Can. J. Psychiatry 2017, 62, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.R.; Schneiderhan, M.E.; Butler, T.; Carpentier, R.M.; Heins, K.R.; Formea, C.M. Pharmacogenomics to support mental health medication therapy management: Clinical practice considerations and a conceptual framework to enhance patient care. J. Am. Coll. Clin. Pharm. 2023. [Google Scholar] [CrossRef]
- Ivanova, S.A.; Toshchakova, V.A.; Filipenko, M.L.; Fedorenko, O.Y.; Boyarko, E.G.; Boiko, A.S.; Semke, A.V.; Bokhan, N.A.; Aftanas, L.I.; Loonen, A.J. Cytochrome P450 1A2 co-determines neuroleptic load and may diminish tardive dyskinesia by increased inducibility. World J. Biol. Psychiatry 2015, 16, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.Y.; Tiwari, A.K.; Freeman, N.; Zai, G.C.; de Luca, V.; Muller, D.J.; Tampakeras, M.; Herbert, D.; Emmerson, H.; Cheema, S.Y.; et al. Liver enzyme CYP2D6 gene and tardive dyskinesia. Pharmacogenomics 2020, 21, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Oshikoya, K.A.; Neely, K.M.; Carroll, R.J.; Aka, I.T.; Maxwell-Horn, A.C.; Roden, D.M.; Van Driest, S.L. CYP2D6 genotype and adverse events to risperidone in children and adolescents. Pediatr. Res. 2019, 85, 602–606. [Google Scholar] [CrossRef]
- Skryabin, V.Y.; Zastrozhin, M.S.; Parkhomenko, A.A.; Pankratenko, E.P.; Pozdnyakov, S.A.; Denisenko, N.P.; Akmalova, K.A.; Bryun, E.A.; Suychev, D.A. Investigating the use of pharmacogenetic and pharmacometabolic markers to predict haloperidol efficacy and safety rates. Hosp. Pharm. 2023, 58, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.H.; Lee, H.J. Oxidative stress and tardive dyskinesia: Pharmacogenetic evidence. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 46, 207–213. [Google Scholar] [CrossRef]
- Koning, J.P.; Vehof, J.; Burger, H.; Wilffert, B.; Al Hadithy, A.; Alizadeh, B.; van Harten, P.N.; Snieder, H.; Genetic Risk and Outcome in Psychosis (GROUP) investigators. Association of two DRD2 gene polymorphisms with acute and tardive antipsychotic-induced movement disorders in young Caucasian patients. Psychopharmacology 2012, 219, 727–736. [Google Scholar] [CrossRef]
- Zai, C.C.; Lee, F.H.; Tiwari, A.K.; Lu, J.Y.; de Luca, V.; Maes, M.S.; Herbert, D.; Shahmirian, A.; Cheema, S.Y.; Zai, G.C.; et al. Investigation of the HSPG2 Gene in Tardive Dyskinesia—New Data and Meta-Analysis. Front. Pharmacol. 2018, 9, 974. [Google Scholar] [CrossRef]
- Zhang, J.P.; Lencz, T.; Zhang, R.X.; Nitta, M.; Maayan, L.; John, M.; Robinson, D.G.; Fleischhacker, W.W.; Kahn, R.S.; Ophoff, R.A.; et al. Pharmacogenetic Associations of Antipsychotic Drug-Related Weight Gain: A Systematic Review and Meta-analysis. Schizophr. Bull. 2016, 42, 1418–1437. [Google Scholar] [CrossRef] [PubMed]
- Schreyer, K.F.; Leucht, S.; Heres, S.; Steimer, W. Genetic association of the rs17782313 polymorphism with antipsychotic-induced weight gain. Psychopharmacology 2023, 240, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Daray, F.M.; Rodante, D.; Carosella, L.G.; Silva, M.E.; Martinez, M.; Fernandez Busch, M.V.; Faccone, D.F.; Rothlin, R.P.; Maffia, P.C. -759C>T Polymorphism of the HTR2C Gene is Associated with Second Generation Antipsychotic-Induced Weight Gain in Female Patients with Schizophrenia. Pharmacopsychiatry 2017, 50, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.P.; Robinson, D.G.; Gallego, J.A.; John, M.; Yu, J.; Addington, J.; Tohen, M.; Kane, J.M.; Malhotra, A.K.; Lencz, T. Association of a Schizophrenia Risk Variant at the DRD2 Locus With Antipsychotic Treatment Response in First-Episode Psychosis. Schizophr. Bull. 2015, 41, 1248–1255. [Google Scholar] [CrossRef]
- Luo, C.; Liu, J.; Wang, X.; Mao, X.; Zhou, H.; Liu, Z. Pharmacogenetic Correlates of Antipsychotic-Induced Weight Gain in the Chinese Population. Neurosci. Bull. 2019, 35, 561–580. [Google Scholar] [CrossRef] [PubMed]
- Vanwong, N.; Ngamsamut, N.; Nuntamool, N.; Hongkaew, Y.; Sukprasong, R.; Puangpetch, A.; Limsila, P.; Sukasem, C. Risperidone-Induced Obesity in Children and Adolescents With Autism Spectrum Disorder: Genetic and Clinical Risk Factors. Front. Pharmacol. 2020, 11, 565074. [Google Scholar] [CrossRef] [PubMed]
- Brandl, E.J.; Frydrychowicz, C.; Tiwari, A.K.; Lett, T.A.; Kitzrow, W.; Büttner, S.; Ehrlich, S.; Meltzer, H.Y.; Lieberman, J.A.; Kennedy, J.L.; et al. Association study of polymorphisms in leptin and leptin receptor genes with antipsychotic-induced body weight gain. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2012, 38, 134–141. [Google Scholar] [CrossRef]
- Nurmi, E.L.; Spilman, S.L.; Whelan, F.; Scahill, L.L.; Aman, M.G.; McDougle, C.J.; Arnold, L.E.; Handen, B.; Johnson, C.; Sukhodolsky, D.G.; et al. Moderation of antipsychotic-induced weight gain by energy balance gene variants in the RUPP autism network risperidone studies. Transl. Psychiatry 2013, 3, e274. [Google Scholar] [CrossRef]
- Yoshida, K.; Maciukiewicz, M.; Zai, C.C.; Goncalves, V.F.; Brandl, E.J.; Lieberman, J.A.; Meltzer, H.Y.; Tiwari, A.K.; Kennedy, J.L.; Muller, D.J. Association between the -2548G/A polymorphism of the leptin gene and antipsychotic-induced weight gain: Analysis of the CATIE sample and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 102, 109952. [Google Scholar] [CrossRef]
- Czerwensky, F.; Leucht, S.; Steimer, W. Association of the common MC4R rs17782313 polymorphism with antipsychotic-related weight gain. J. Clin. Psychopharmacol. 2013, 33, 74–79. [Google Scholar] [CrossRef]
- Zhang, Y.; Ren, H.; Wang, Q.; Deng, W.; Yue, W.; Yan, H.; Tan, L.; Chen, Q.; Yang, G.; Lu, T.; et al. Testing the role of genetic variation of the MC4R gene in Chinese population in antipsychotic-induced metabolic disturbance. Sci. China Life Sci. 2019, 62, 535–543. [Google Scholar] [CrossRef]
- Konte, B.; Walters, J.T.R.; Rujescu, D.; Legge, S.E.; Pardinas, A.F.; Cohen, D.; Pirmohamed, M.; Tiihonen, J.; Hartmann, A.M.; Bogers, J.P.; et al. HLA-DQB1 6672G>C (rs113332494) is associated with clozapine-induced neutropenia and agranulocytosis in individuals of European ancestry. Transl. Psychiatry 2021, 11, 214. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.I.; Jarskog, L.F.; Hilliard, C.; Alfirevic, A.; Duncan, L.; Fourches, D.; Huang, H.; Lek, M.; Neale, B.M.; Ripke, S.; et al. Clozapine-induced agranulocytosis is associated with rare HLA-DQB1 and HLA-B alleles. Nat. Commun. 2014, 5, 4757. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Ikeda, M.; Mushiroda, T.; Ozeki, T.; Kondo, K.; Shimasaki, A.; Kawase, K.; Hashimoto, S.; Yamamori, H.; Yasuda, Y.; et al. Pharmacogenomic Study of Clozapine-Induced Agranulocytosis/Granulocytopenia in a Japanese Population. Biol. Psychiatry 2016, 80, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Drago, A.; Giegling, I.; Schafer, M.; Hartmann, A.M.; Konte, B.; Friedl, M.; Serretti, A.; Rujescu, D. Genome-wide association study supports the role of the immunological system and of the neurodevelopmental processes in response to haloperidol treatment. Pharmacogenet. Genom. 2014, 24, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Le Clerc, S.; Taing, L.; Fond, G.; Meary, A.; Llorca, P.M.; Blanc, O.; Beaune, P.; Rajagopal, K.; Jamain, S.; Tamouza, R.; et al. A double amino-acid change in the HLA-A peptide-binding groove is associated with response to psychotropic treatment in patients with schizophrenia. Transl. Psychiatry 2015, 5, e608. [Google Scholar] [CrossRef] [PubMed]
- Jajodia, A.; Kaur, H.; Kumari, K.; Kanojia, N.; Gupta, M.; Baghel, R.; Sood, M.; Jain, S.; Chadda, R.K.; Kukreti, R. Evaluation of genetic association of neurodevelopment and neuroimmunological genes with antipsychotic treatment response in schizophrenia in Indian populations. Mol. Genet. Genom. Med. 2016, 4, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Drogemoller, B.I.; Emsley, R.; Chiliza, B.; van der Merwe, L.; Wright, G.E.; Daya, M.; Hoal, E.; Malhotra, A.K.; Lencz, T.; Robinson, D.G.; et al. The identification of novel genetic variants associated with antipsychotic treatment response outcomes in first-episode schizophrenia patients. Pharmacogenet. Genom. 2016, 26, 235–242. [Google Scholar] [CrossRef]
- Wang, Q.; Man Wu, H.; Yue, W.; Yan, H.; Zhang, Y.; Tan, L.; Deng, W.; Chen, Q.; Yang, G.; Lu, T.; et al. Effect of Damaging Rare Mutations in Synapse-Related Gene Sets on Response to Short-term Antipsychotic Medication in Chinese Patients With Schizophrenia: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 1261–1269. [Google Scholar] [CrossRef]
- Zhao, M.; Ma, J.; Li, M.; Zhu, W.; Zhou, W.; Shen, L.; Wu, H.; Zhang, N.; Wu, S.; Fu, C.; et al. Different responses to risperidone treatment in Schizophrenia: A multicenter genome-wide association and whole exome sequencing joint study. Transl. Psychiatry 2022, 12, 173. [Google Scholar] [CrossRef]
- Zhou, W.; Xu, Y.; Lv, Q.; Sheng, Y.H.; Chen, L.; Li, M.; Shen, L.; Huai, C.; Yi, Z.; Cui, D.; et al. Genetic Association of Olanzapine Treatment Response in Han Chinese Schizophrenia Patients. Front. Pharmacol. 2019, 10, 177. [Google Scholar] [CrossRef]
- Tanaka, S.; Syu, A.; Ishiguro, H.; Inada, T.; Horiuchi, Y.; Ishikawa, M.; Koga, M.; Noguchi, E.; Ozaki, N.; Someya, T.; et al. DPP6 as a candidate gene for neuroleptic-induced tardive dyskinesia. Pharmacogenom. J. 2013, 13, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Alkelai, A.; Greenbaum, L.; Heinzen, E.L.; Baugh, E.H.; Teitelbaum, A.; Zhu, X.; Strous, R.D.; Tatarskyy, P.; Zai, C.C.; Tiwari, A.K.; et al. New insights into tardive dyskinesia genetics: Implementation of whole-exome sequencing approach. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 94, 109659. [Google Scholar] [CrossRef] [PubMed]
- Brandl, E.J.; Tiwari, A.K.; Zai, C.C.; Nurmi, E.L.; Chowdhury, N.I.; Arenovich, T.; Sanches, M.; Goncalves, V.F.; Shen, J.J.; Lieberman, J.A.; et al. Genome-wide association study on antipsychotic-induced weight gain in the CATIE sample. Pharmacogenom. J. 2016, 16, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Wang, L.; Lv, L.; Ma, C.; Du, B.; Lu, T.; Jin, C.; Yan, H.; Yang, Y.; Li, W.; et al. Genome-Wide Association Study Suggested the PTPRD Polymorphisms Were Associated With Weight Gain Effects of Atypical Antipsychotic Medications. Schizophr. Bull. 2016, 42, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Ter Hark, S.E.; Jamain, S.; Schijven, D.; Lin, B.D.; Bakker, M.K.; Boland-Auge, A.; Deleuze, J.F.; Troudet, R.; Malhotra, A.K.; Gülöksüz, S.; et al. A new genetic locus for antipsychotic-induced weight gain: A genome-wide study of first-episode psychosis patients using amisulpride (from the OPTiMiSE cohort). J. Psychopharmacol. 2020, 34, 524–531. [Google Scholar] [CrossRef]
- Legge, S.E.; Pardinas, A.F.; Helthuis, M.; Jansen, J.A.; Jollie, K.; Knapper, S.; MacCabe, J.H.; Rujescu, D.; Collier, D.A.; O’Donovan, M.C.; et al. A genome-wide association study in individuals of African ancestry reveals the importance of the Duffy-null genotype in the assessment of clozapine-related neutropenia. Mol. Psychiatry 2019, 24, 328–337. [Google Scholar] [CrossRef]
- Lu, Z.; Zhang, Y.; Yan, H.; Su, Y.; Guo, L.; Liao, Y.; Lu, T.; Yu, H.; Wang, L.; Li, J.; et al. ATAD3B and SKIL polymorphisms associated with antipsychotic-induced QTc interval change in patients with schizophrenia: A genome-wide association study. Transl. Psychiatry 2022, 12, 56. [Google Scholar] [CrossRef]
- Mas, S.; Gasso, P.; Boloc, D.; Rodriguez, N.; Marmol, F.; Sanchez, J.; Bernardo, M.; Lafuente, A. Network analysis of gene expression in mice provides new evidence of involvement of the mTOR pathway in antipsychotic-induced extrapyramidal symptoms. Pharmacogenom. J. 2016, 16, 293–300. [Google Scholar] [CrossRef]
- Sainz, J.; Prieto, C.; Ruso-Julve, F.; Crespo-Facorro, B. Blood Gene Expression Profile Predicts Response to Antipsychotics. Front. Mol. Neurosci. 2018, 11, 73. [Google Scholar] [CrossRef] [PubMed]
- Ovenden, E.S.; McGregor, N.W.; Emsley, R.A.; Warnich, L. DNA methylation and antipsychotic treatment mechanisms in schizophrenia: Progress and future directions. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 81, 38–49. [Google Scholar] [CrossRef]
- Lisoway, A.J.; Chen, C.C.; Zai, C.C.; Tiwari, A.K.; Kennedy, J.L. Toward personalized medicine in schizophrenia: Genetics and epigenetics of antipsychotic treatment. Schizophr. Res. 2021, 232, 112–124. [Google Scholar] [CrossRef]
- Zhou, J.; Li, M.; Wang, X.; He, Y.; Xia, Y.; Sweeney, J.A.; Kopp, R.F.; Liu, C.; Chen, C. Drug Response-Related DNA Methylation Changes in Schizophrenia, Bipolar Disorder, and Major Depressive Disorder. Front. Neurosci. 2021, 15, 674273. [Google Scholar] [CrossRef]
- Tang, H.; Dalton, C.F.; Srisawat, U.; Zhang, Z.J.; Reynolds, G.P. Methylation at a transcription factor-binding site on the 5-HT1A receptor gene correlates with negative symptom treatment response in first episode schizophrenia. Int. J. Neuropsychopharmacol. 2014, 17, 645–649. [Google Scholar] [CrossRef]
- Athanasiou, M.C.; Dettling, M.; Cascorbi, I.; Mosyagin, I.; Salisbury, B.A.; Pierz, K.A.; Zou, W.; Whalen, H.; Malhotra, A.K.; Lencz, T.; et al. Candidate gene analysis identifies a polymorphism in HLA-DQB1 associated with clozapine-induced agranulocytosis. J. Clin. Psychiatry 2011, 72, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Numata, S.; Umehara, H.; Ohmori, T.; Hashimoto, R. Clozapine Pharmacogenetic Studies in Schizophrenia: Efficacy and Agranulocytosis. Front. Pharmacol. 2018, 9, 1049. [Google Scholar] [CrossRef] [PubMed]
- Boloc, D.; Gortat, A.; Cheng-Zhang, J.Q.; Garcia-Cerro, S.; Rodriguez, N.; Parellada, M.; Saiz-Ruiz, J.; Cuesta, M.J.; Gasso, P.; Lafuente, A.; et al. Improving pharmacogenetic prediction of extrapyramidal symptoms induced by antipsychotics. Transl. Psychiatry 2018, 8, 276. [Google Scholar] [CrossRef]
- Tonozzi, T.R.; Braunstein, G.D.; Kammesheidt, A.; Curran, C.; Golshan, S.; Kelsoe, J. Pharmacogenetic profile and major depressive and/or bipolar disorder treatment: A retrospective, cross-sectional study. Pharmacogenomics 2018, 19, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.P.; Robinson, D.; Yu, J.; Gallego, J.; Fleischhacker, W.W.; Kahn, R.S.; Crespo-Facorro, B.; Vazquez-Bourgon, J.; Kane, J.M.; Malhotra, A.K.; et al. Schizophrenia Polygenic Risk Score as a Predictor of Antipsychotic Efficacy in First-Episode Psychosis. Am. J. Psychiatry 2019, 176, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Marshe, V.S.; Elsheikh, S.S.M.; Maciukiewicz, M.; Tiwari, A.; Brandl, E.J.; Lieberman, J.A.; Meltzer, H.Y.; Kennedy, J.L.; Muller, D.J. Polygenic risk scores analyses of psychiatric and metabolic traits with antipsychotic-induced weight gain in schizophrenia: An exploratory study. Pharmacogenom. J. 2023, 23, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Rodieux, F.; Daali, Y.; Rollason, V.; Samer, C.F.; Lorenzini, K.I. Practice of CYP450 genotyping and phenotyping in children in a real-life setting. Front. Pharmacol. 2023, 14, 1130100. [Google Scholar] [CrossRef] [PubMed]
- Toja-Camba, F.J.; Gesto-Antelo, N.; Maronas, O.; Echarri Arrieta, E.; Zarra-Ferro, I.; Gonzalez-Barcia, M.; Bandin-Vilar, E.; Mangas Sanjuan, V.; Facal, F.; Arrojo Romero, M.; et al. Review of Pharmacokinetics and Pharmacogenetics in Atypical Long-Acting Injectable Antipsychotics. Pharmaceutics 2021, 13, 935. [Google Scholar] [CrossRef] [PubMed]
- Bousman, C.A.; Stevenson, J.M.; Ramsey, L.B.; Sangkuhl, K.; Hicks, J.K.; Strawn, J.R.; Singh, A.B.; Ruano, G.; Mueller, D.J.; Tsermpini, E.E.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants. Clin. Pharmacol. Ther. 2023, 114, 51–68. [Google Scholar] [CrossRef]
- Hicks, J.K.; Sangkuhl, K.; Swen, J.J.; Ellingrod, V.L.; Müller, D.J.; Shimoda, K.; Bishop, J.R.; Kharasch, E.D.; Skaar, T.C.; Gaedigk, A.; et al. Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clin. Pharmacol. Ther. 2017, 102, 37–44. [Google Scholar] [CrossRef]
- Altar, C.A.; Carhart, J.; Allen, J.D.; Hall-Flavin, D.; Winner, J.; Dechairo, B. Clinical Utility of Combinatorial Pharmacogenomics-Guided Antidepressant Therapy: Evidence from Three Clinical Studies. Mol. Neuropsychiatry 2015, 1, 145–155. [Google Scholar] [CrossRef]
- Winner, J.G.; Carhart, J.M.; Altar, C.A.; Goldfarb, S.; Allen, J.D.; Lavezzari, G.; Parsons, K.K.; Marshak, A.G.; Garavaglia, S.; Dechairo, B.M. Combinatorial pharmacogenomic guidance for psychiatric medications reduces overall pharmacy costs in a 1 year prospective evaluation. Curr. Med. Res. Opin. 2015, 31, 1633–1643. [Google Scholar] [CrossRef]
- Arranz, M.J.; Salazar, J.; Bote, V.; Artigas-Baleri, A.; Serra-LLovich, A.; Triviño, E.; Roige, J.; Lombardia, C.; Cancino, M.; Hernandez, M.; et al. Pharmacogenetic Interventions Improve the Clinical Outcome of Treatment-Resistant Autistic Spectrum Disorder Sufferers. Pharmaceutics 2022, 14, 999. [Google Scholar] [CrossRef]
- Walden, L.M.; Brandl, E.J.; Tiwari, A.K.; Cheema, S.; Freeman, N.; Braganza, N.; Kennedy, J.L.; Müller, D.J. Genetic testing for CYP2D6 and CYP2C19 suggests improved outcome for antidepressant and antipsychotic medication. Psychiatry Res. 2019, 279, 111–115. [Google Scholar] [CrossRef]
- Scherf-Clavel, M.; Frantz, A.; Eckert, A.; Weber, H.; Unterecker, S.; Deckert, J.; Reif, A.; Hahn, M. Effect of CYP2D6 pharmacogenetic phenotype and phenoconversion on serum concentrations of antidepressants and antipsychotics: A retrospective cohort study. Int. J. Clin. Pharm. 2023, 45, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.T.; Campo-Soria, C.; Bishop, J.R. Current strategies for predicting side effects from second generation antipsychotics in youth. Expert Opin. Drug Metab. Toxicol. 2021, 17, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.I.; Schuette, P.; Burckart, G.J.; Green, D.J.; La, J.; Burnham, J.M.; Rakhmanina, N.; Robb, A.; Huang, S.M.; van den Anker, J.N. A Comparison of Pediatric and Adult Safety Studies for Antipsychotic and Antidepressant Drugs Submitted to the United States Food and Drug Administration. J. Pediatr. 2019, 208, 236–242.e3. [Google Scholar] [CrossRef] [PubMed]
- Jameson, A.; Fylan, B.; Bristow, G.C.; Sagoo, G.S.; Dalton, C.; Cardno, A.; Sohal, J.; McLean, S.L. What Are the Barriers and Enablers to the Implementation of Pharmacogenetic Testing in Mental Health Care Settings? Front. Genet. 2021, 12, 740216. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, P.; Martinez, J.; Shah, N.; Kenan, W.; Fowler, A.; Limdi, N.; Burns, L.; Cogan, E.S.; Gardiner, A.; Hain, D.; et al. Pharmacogenomic profiling of pediatric patients on psychotropic medications in an emergency department. Pediatr. Emerg. Care 2023, 39, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Eadon, M.T.; Rosenman, M.B.; Zhang, P.; Fulton, C.R.; Callaghan, J.T.; Holmes, A.M.; Levy, K.D.; Gupta, S.K.; Haas, D.M.; Vuppalanchi, R.; et al. The INGENIOUS trial: Impact of pharmacogenetic testing on adverse events in a pragmatic clinical trial. Pharmacogenom. J. 2023, 23, 169–177. [Google Scholar] [CrossRef]
- Carrascal-Laso, L.; Franco-Martin, M.A.; Garcia-Berrocal, M.B.; Marcos-Vadillo, E.; Sanchez-Iglesias, S.; Lorenzo, C.; Sanchez-Martin, A.; Ramos-Gallego, I.; Garcia-Salgado, M.J.; Isidoro-Garcia, M. Application of a Pharmacogenetics-Based Precision Medicine Model (5SPM) to Psychotic Patients That Presented Poor Response to Neuroleptic Therapy. J. Pers. Med. 2020, 10, 289. [Google Scholar] [CrossRef]
- Alshabeeb, M.A.; Deneer, V.H.M.; Khan, A.; Asselbergs, F.W. Use of Pharmacogenetic Drugs by the Dutch Population. Front. Genet. 2019, 10, 567. [Google Scholar] [CrossRef]
- Kang, Z.; Qin, Y.; Sun, Y.; Lu, Z.; Sun, Y.; Chen, H.; Feng, X.; Zhang, Y.; Guo, H.; Yan, H.; et al. Multigenetic pharmacogenomics-guided treatment vs treatment as usual among hospitalised men with schizophrenia. JAMA Netw. Open 2023, 6, e2335518. [Google Scholar] [CrossRef]
- Garcia-Perez, L.; Linertova, R.; Serrano-Perez, P.; Trujillo-Martin, M.; Rodriguez-Rodriguez, L.; Valcarcel-Nazco, C.; Del Pino-Sedeno, T. Interventions to improve medication adherence in mental health: The update of a systematic review of cost-effectiveness. Int. J. Psychiatry Clin. Pract. 2020, 24, 416–427. [Google Scholar] [CrossRef]
- Hall-Flavin, D.K.; Winner, J.G.; Allen, J.D.; Jordan, J.J.; Nesheim, R.S.; Snyder, K.A.; Drews, M.S.; Eisterhold, L.L.; Biernacka, J.M.; Mrazek, D.A. Using a pharmacogenomic algorithm to guide the treatment of depression. Transl. Psychiatry 2012, 2, e172. [Google Scholar] [CrossRef]
- Pérez, V.; Salavert, A.; Espadaler, J.; Tuson, M.; Saiz-Ruiz, J.; Sáez-Navarro, C.; Bobes, J.; Baca-García, E.; Vieta, E.; Olivares, J.M.; et al. Efficacy of prospective pharmacogenetic testing in the treatment of major depressive disorder: Results of a randomized, double-blind clinical trial. BMC Psychiatry 2017, 17, 250. [Google Scholar] [CrossRef]
- Laika, B.; Leucht, S.; Heres, S.; Steimer, W. Intermediate metabolizer: Increased side effects in psychoactive drug therapy. The key to cost-effectiveness of pretreatment CYP2D6 screening? Pharmacogenom. J. 2009, 9, 395–403. [Google Scholar] [CrossRef]
- Carrascal-Laso, L.; Franco-Martin, M.A.; Marcos-Vadillo, E.; Ramos-Gallego, I.; Garcia-Berrocal, B.; Mayor-Toranzo, E.; Sanchez-Iglesias, S.; Lorenzo, C.; Sevillano-Jimenez, A.; Sanchez-Martin, A.; et al. Economic Impact of the Application of a Precision Medicine Model (5SPM) on Psychotic Patients. Pharmacogenom. Pers. Med. 2021, 14, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Karamperis, K.; Koromina, M.; Papantoniou, P.; Skokou, M.; Kanellakis, F.; Mitropoulos, K.; Vozikis, A.; Muller, D.J.; Patrinos, G.P.; Mitropoulou, C. Economic evaluation in psychiatric pharmacogenomics: A systematic review. Pharmacogenom. J. 2021, 21, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Girardin, F.R.; Poncet, A.; Perrier, A.; Vernaz, N.; Pletscher, M.; Samer, C.F.; Lieberman, J.A.; Villard, J. Cost-effectiveness of HLA-DQB1/HLA-B pharmacogenetic-guided treatment and blood monitoring in US patients taking clozapine. Pharmacogenom. J. 2019, 19, 211–218. [Google Scholar] [CrossRef]
- Bousman, C.A.; Hopwood, M. Commercial pharmacogenetic-based decision-support tools in psychiatry. Lancet Psychiatry 2016, 3, 585–590. [Google Scholar] [CrossRef]
- Mas, S.; Gasso, P.; Lafuente, A.; Bioque, M.; Lobo, A.; Gonzalez-Pinto, A.; Olmeda, M.S.; Corripio, I.; Llerena, A.; Cabrera, B.; et al. Pharmacogenetic study of antipsychotic induced acute extrapyramidal symptoms in a first episode psychosis cohort: Role of dopamine, serotonin and glutamate candidate genes. Pharmacogenom. J. 2016, 16, 439–445. [Google Scholar] [CrossRef]
- Hettige, N.C.; Zai, C.; Hazra, M.; Borlido, C.; Kennedy, J.L.; Strauss, J.; Le Foll, B.; Wong, A.; Remington, G.; De Luca, V. Use of candidate gene markers to guide antipsychotic dosage adjustment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 54, 315–320. [Google Scholar] [CrossRef]
- Teo, C.; Zai, C.; Borlido, C.; Tomasetti, C.; Strauss, J.; Shinkai, T.; Le Foll, B.; Wong, A.; Kennedy, J.L.; De Luca, V. Analysis of treatment-resistant schizophrenia and 384 markers from candidate genes. Pharmacogenet. Genom. 2012, 22, 807–811. [Google Scholar] [CrossRef]
- Almoguera, B.; Riveiro-Alvarez, R.; Lopez-Castroman, J.; Dorado, P.; Vaquero-Lorenzo, C.; Fernandez-Piqueras, J.; Llerena, A.; Abad-Santos, F.; Baca-García, E.; Dal-Ré, R.; et al. Association of common genetic variants with risperidone adverse events in a Spanish schizophrenic population. Pharmacogenom. J. 2013, 13, 197–204. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zai, C.C.; Tiwari, A.K.; Zai, G.C.; Freeman, N.; Pouget, J.G.; Greco, J.; Tampakeras, M.; Shaikh, S.A.; Herbert, D.; Emmerson, H.; et al. Association Study of the Complement Component C4 Gene in Tardive Dyskinesia. Front. Pharmacol. 2019, 10, 1339. [Google Scholar] [CrossRef] [PubMed]
- Guzek, K.; Stelmach, A.; Roznowska, A.; Najbar, I.; Cichocki, L.; Sadakierska-Chudy, A. A preliminary study of genetic polymorphisms potentially related to the adverse effects of aripiprazole. Arch. Pharm. Pract. 2023, 14, 13–18. [Google Scholar] [CrossRef]
- Bigos, K.L.; Bies, R.R.; Pollock, B.G.; Lowy, J.J.; Zhang, F.; Weinberger, D.R. Genetic variation in CYP3A43 explains racial difference in olanzapine clearance. Mol. Psychiatry 2011, 16, 620–625. [Google Scholar] [CrossRef]
- Lu, J.Y.; Tiwari, A.K.; Zai, G.C.; Rastogi, A.; Shaikh, S.A.; Müller, D.J.; Voineskos, A.N.; Potkin, S.G.; Lieberman, J.A.; Meltzer, H.Y.; et al. Association study of Disrupted-In-Schizophrenia-1 gene variants and tardive dyskinesia. Neurosci. Lett. 2018, 686, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Ota, V.K.; Spíndola, L.N.; Gadelha, A.; dos Santos Filho, A.F.; Santoro, M.L.; Christofolini, D.M.; Bellucco, F.T.; Ribeiro-dos-Santos, Â.; Santos, S.; Mari, J.D.J.; et al. DRD1 rs4532 polymorphism: A potential pharmacogenomic marker for treatment response to antipsychotic drugs. Schizophr. Res. 2012, 142, 206–208. [Google Scholar] [CrossRef]
- Martinez-Pinteno, A.; Gasso, P.; Prohens, L.; Segura, A.G.; Parellada, M.; Saiz-Ruiz, J.; Cuesta, M.J.; Bernardo, M.; Lafuente, A.; Mas, S.; et al. Identification of EP300 as a Key Gene Involved in Antipsychotic-Induced Metabolic Dysregulation Based on Integrative Bioinformatics Analysis of Multi-Tissue Gene Expression Data. Front. Pharmacol. 2021, 12, 729474. [Google Scholar] [CrossRef] [PubMed]
- Mitjans, M.; Catalán, R.; Vázquez, M.; González-Rodríguez, A.; Penadés, R.; Pons, A.; Massana, G.; Munro, J.; Arranz, M.J.; Arias, B. Hypothalamic–pituitary–adrenal system, neurotrophic factors and clozapine response: Association with FKBP5 and NTRK2 genes. Pharmacogenet. Genom. 2015, 25, 274–277. [Google Scholar] [CrossRef]
- Schröder, C.; Czerwensky, F.; Leucht, S.; Steimer, W. Fat Mass and Obesity-Related Gene Variants rs9939609 and rs7185735 are Associated with Second-Generation Antipsychotic-Induced Weight Gain. Pharmacopsychiatry 2019, 52, 16–23. [Google Scholar] [CrossRef]
- Ramsey, T.L.; Brennan, M.D. Glucagon-like peptide 1 receptor (GLP1R) haplotypes correlate with altered response to multiple antipsychotics in the CATIE trial. Schizophr. Res. 2014, 160, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Bakker, P.R.; Al Hadithy, A.F.; Amin, N.; van Duijn, C.M.; van Os, J.; van Harten, P.N. Antipsychotic-induced movement disorders in long-stay psychiatric patients and 45 tag SNPs in 7 candidate genes: A prospective study. PLoS ONE 2012, 7, e50970. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.R.; Reilly, J.L.; Harris, M.S.; Patel, S.R.; Kittles, R.; Badner, J.A.; Prasad, K.M.; Nimgaonkar, V.L.; Keshavan, M.S.; Sweeney, J.A. Pharmacogenetic associations of the type-3 metabotropic glutamate receptor (GRM3) gene with working memory and clinical symptom response to antipsychotics in first-episode schizophrenia. Psychopharmacology 2015, 232, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Quteineh, L.; Vandenberghe, F.; Saigi Morgui, N.; Delacretaz, A.; Choong, E.; Gholam-Rezaee, M.; Magistretti, P.; Bondolfi, G.; Von Gunten, A.; Preisig, M.; et al. Impact of HSD11B1 polymorphisms on BMI and components of the metabolic syndrome in patients receiving psychotropic treatments. Pharmacogenet. Genom. 2015, 25, 246–258. [Google Scholar] [CrossRef] [PubMed]
- Takekita, Y.; Fabbri, C.; Kato, M.; Nonen, S.; Sakai, S.; Sunada, N.; Koshikawa, Y.; Wakeno, M.; Okugawa, G.; Kinoshita, T.; et al. Serotonin 7 Receptor Variants Are Not Associated with Response to Second-Generation Antipsychotics in Japanese Schizophrenia Patients. Neuropsychobiology 2015, 72, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Osmanova, D.Z.; Freidin, M.B.; Fedorenko, O.Y.; Pozhidaev, I.V.; Boiko, A.S.; Vyalova, N.M.; Tiguntsev, V.V.; Kornetova, E.G.; Loonen, A.J.M.; Semke, A.V.; et al. A pharmacogenetic study of patients with schizophrenia from West Siberia gets insight into dopaminergic mechanisms of antipsychotic-induced hyperprolactinemia. BMC Med. Genet. 2019, 20 (Suppl. S1), 47. [Google Scholar] [CrossRef]
- Czerwensky, F.; Leucht, S.; Steimer, W. MC4R rs489693: A clinical risk factor for second generation antipsychotic-related weight gain? Int. J. Neuropsychopharmacol. 2013, 16, 2103–2109. [Google Scholar] [CrossRef][Green Version]
- Spellmann, I.; Riedel, M.; Städtler, J.; Zill, P.; Obermeier, M.; Cerovecki, A.; Dehning, S.; Schennach, R.; Epple, M.; Opgen-Rhein, M.; et al. Associations of NEUROD2 polymorphisms and change of cognitive dysfunctions in schizophrenia and schizoaffective disorder after eight weeks of antipsychotic treatment. Cogn. Neuropsychiatry 2017, 22, 280–297. [Google Scholar] [CrossRef]
- Esen-Sehir, D.; Kopf, J.; Hagele, S.; Plichta, M.M.; Reif, A.; Freudenberg, F. Influence of NOS1AP Risk Variants on the Corrected QT (QTc) Interval in the Pharmacotherapy of Schizophrenia. Pharmacopsychiatry 2022, 55, 266–273. [Google Scholar] [CrossRef]
- Dobrodeeva, V.S.; Shnayder, N.A.; Novitsky, M.A.; Asadullin, A.R.; Vaiman, E.E.; Petrova, M.M.; Limankin, O.V.; Neznanov, N.G.; Garganeeva, N.P.; Nasyrova, R.F. Association of a Single-Nucleotide Variant rs11100494 of the NPY5R Gene with Antipsychotic-Induced Metabolic Disorders. Pharmaceutics 2022, 14, 222. [Google Scholar] [CrossRef]
- Zazueta, A.; Castillo, T.; Cavieres, A.; Gonzalez, R.; Abarca, M.; Nieto, R.R.; Deneken, J.; Araneda, C.; Moya, P.R.; Bustamante, M.L. Polymorphisms in Schizophrenia-Related Genes Are Potential Predictors of Antipsychotic Treatment Resistance and Refractoriness. Int. J. Neuropsychopharmacol. 2022, 25, 701–708. [Google Scholar] [CrossRef]
- Spellmann, I.; Rujescu, D.; Musil, R.; Meyerwas, S.; Giegling, I.; Genius, J.; Zill, P.; Dehning, S.; Cerovecki, A.; Seemuller, F.; et al. Pleckstrin homology domain containing 6 protein (PLEKHA6) polymorphisms are associated with psychopathology and response to treatment in schizophrenic patients. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 51, 190–195. [Google Scholar] [CrossRef]
- Gagliano, S.A.; Tiwari, A.K.; Freeman, N.; Lieberman, J.A.; Meltzer, H.Y.; Kennedy, J.L.; Knight, J.; Muller, D.J. Protein kinase cAMP-dependent regulatory type II beta (PRKAR2B) gene variants in antipsychotic-induced weight gain. Hum. Psychopharmacol. 2014, 29, 330–335. [Google Scholar] [CrossRef]
- Maciukiewicz, M.; Gorbovskaya, I.; Tiwari, A.K.; Zai, C.C.; Freeman, N.; Meltzer, H.Y.; Kennedy, J.L.; Müller, D.J. Genetic validation study of protein tyrosine phosphatase receptor type D (PTPRD) gene variants and risk for antipsychotic-induced weight gain. J. Neural Transm. 2019, 126, 27–33. [Google Scholar] [CrossRef]
- Xu, Q.; Li, M.; Qin, S.; Li, Y.; Ning, A.; Fu, Y.; Wang, D.; Zeng, D.; Li, H.; Yu, W.; et al. Two Novel Loci of RELN Associated With Antipsychotics Response in Chinese Han Population. Front. Pharmacol. 2020, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Gareeva, A.E.; Zakirov, D.F.; Valinurov, R.G.; Khusnutdinova, E.K. Polymorphism of RGS2 gene: Genetic markers of risk for schizophrenia and pharmacogenetic markers of typical neuroleptics efficiency. Mol. Biol. 2013, 47, 934–941. [Google Scholar] [CrossRef]
- Zai, C.C.; Tiwari, A.K.; Mazzoco, M.; de Luca, V.; Muller, D.J.; Shaikh, S.A.; Lohoff, F.W.; Freeman, N.; Voineskos, A.N.; Potkin, S.G.; et al. Association study of the vesicular monoamine transporter gene SLC18A2 with tardive dyskinesia. J. Psychiatr. Res. 2013, 47, 1760–1765. [Google Scholar] [CrossRef]
- Giegling, I.; Drago, A.; Dolzan, V.; Plesnicar, B.K.; Schafer, M.; Hartmann, A.M.; Sander, T.; Toliat, M.R.; Moller, H.J.; Stassen, H.H.; et al. Glutamatergic gene variants impact the clinical profile of efficacy and side effects of haloperidol. Pharmacogenet. Genom. 2011, 21, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Guan, F.; Zhang, T.; Han, W.; Zhu, L.; Ni, T.; Lin, H.; Liu, D.; Chen, G.; Xiao, J.; Li, T. Relationship of SNAP25 variants with schizophrenia and antipsychotic-induced weight change in large-scale schizophrenia patients. Schizophr. Res. 2020, 215, 250–255. [Google Scholar] [CrossRef]
- Ramsey, T.L.; Liu, Q.; Brennan, M.D. Replication of SULT4A1-1 as a pharmacogenetic marker of olanzapine response and evidence of lower weight gain in the high response group. Pharmacogenomics 2014, 15, 933–939. [Google Scholar] [CrossRef]
- Ramsey, T.L.; Liu, Q.; Massey, B.W.; Brennan, M.D. Genotypic variation in the SV2C gene impacts response to atypical antipsychotics the CATIE study. Schizophr. Res. 2013, 149, 21–25. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hattori, S.; Suda, A.; Miyauchi, M.; Shiraishi, Y.; Saeki, T.; Fukushima, T.; Fujibayashi, M.; Tsujita, N.; Ishii, C.; Ishii, N.; et al. The association of genetic polymorphisms in CYP1A2, UGT1A4, and ABCB1 with autonomic nervous system dysfunction in schizophrenia patients treated with olanzapine. BMC Psychiatry 2020, 20, 72. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernandez, M.; Cullell, N.; Cendros, M.; Serra-Llovich, A.; Arranz, M.J. Clinical Utility and Implementation of Pharmacogenomics for the Personalisation of Antipsychotic Treatments. Pharmaceutics 2024, 16, 244. https://doi.org/10.3390/pharmaceutics16020244
Hernandez M, Cullell N, Cendros M, Serra-Llovich A, Arranz MJ. Clinical Utility and Implementation of Pharmacogenomics for the Personalisation of Antipsychotic Treatments. Pharmaceutics. 2024; 16(2):244. https://doi.org/10.3390/pharmaceutics16020244
Chicago/Turabian StyleHernandez, Marta, Natalia Cullell, Marc Cendros, Alexandre Serra-Llovich, and Maria J. Arranz. 2024. "Clinical Utility and Implementation of Pharmacogenomics for the Personalisation of Antipsychotic Treatments" Pharmaceutics 16, no. 2: 244. https://doi.org/10.3390/pharmaceutics16020244
APA StyleHernandez, M., Cullell, N., Cendros, M., Serra-Llovich, A., & Arranz, M. J. (2024). Clinical Utility and Implementation of Pharmacogenomics for the Personalisation of Antipsychotic Treatments. Pharmaceutics, 16(2), 244. https://doi.org/10.3390/pharmaceutics16020244