

Development of a Carvedilol Oral Liquid Formulation for Paediatric Use


 ,
,  ,
,  ,
,  , ,
, , 

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Materials
2.1.1. Pharmaceutical Development Chemicals
2.1.2. Microbiological Test Materials
2.2. Solubility Studies
2.2.1. Determination of CARV Solubility at Different pH Levels
2.2.2. Determination of CARV Apparent Solubility at 1 mg/mL in Acid Media
2.3. Stability Studies
2.3.1. Preliminary Stability Study
- F1 and F2 formulations: 0.5 g/100 mL of sodium acetate trihydrate and 0.17 g/100 mL of acetic acid for F2 and additional acetic acid up to pH 4.0 for F1;
- F3 and F4 formulations: 0.8 g/100 mL of sodium hydroxide and 10.0 g/100 mL of citric acid monohydrate for F4 and additional citric acid up to pH 2.0 for F3;
- F5 and F6 formulations: 1.7 g/100 mL of malic acid for F5 and 0.8 g/100 mL of malic acid for F6.
- Appearance: clear solution, translucent, without undissolved particles;
- pH: initial pH ± 0.2;
- CARV assay (%): 95–105.
2.3.2. Final Stability Study
2.4. Design of Experiment (DoE)—Optimization of Preparation of CARV Solution
2.5. Efficacy of Antimicrobial Preservation (Challenge Test)
2.5.1. Preparation of CARV Solutions
2.5.2. Description of the Test
2.5.3. Test Conditions
3. Results
3.1. Solubility
3.2. Preliminary CARV Solutions
Stability
3.3. Malic Acid CARV Formulations
3.3.1. Saturation Study
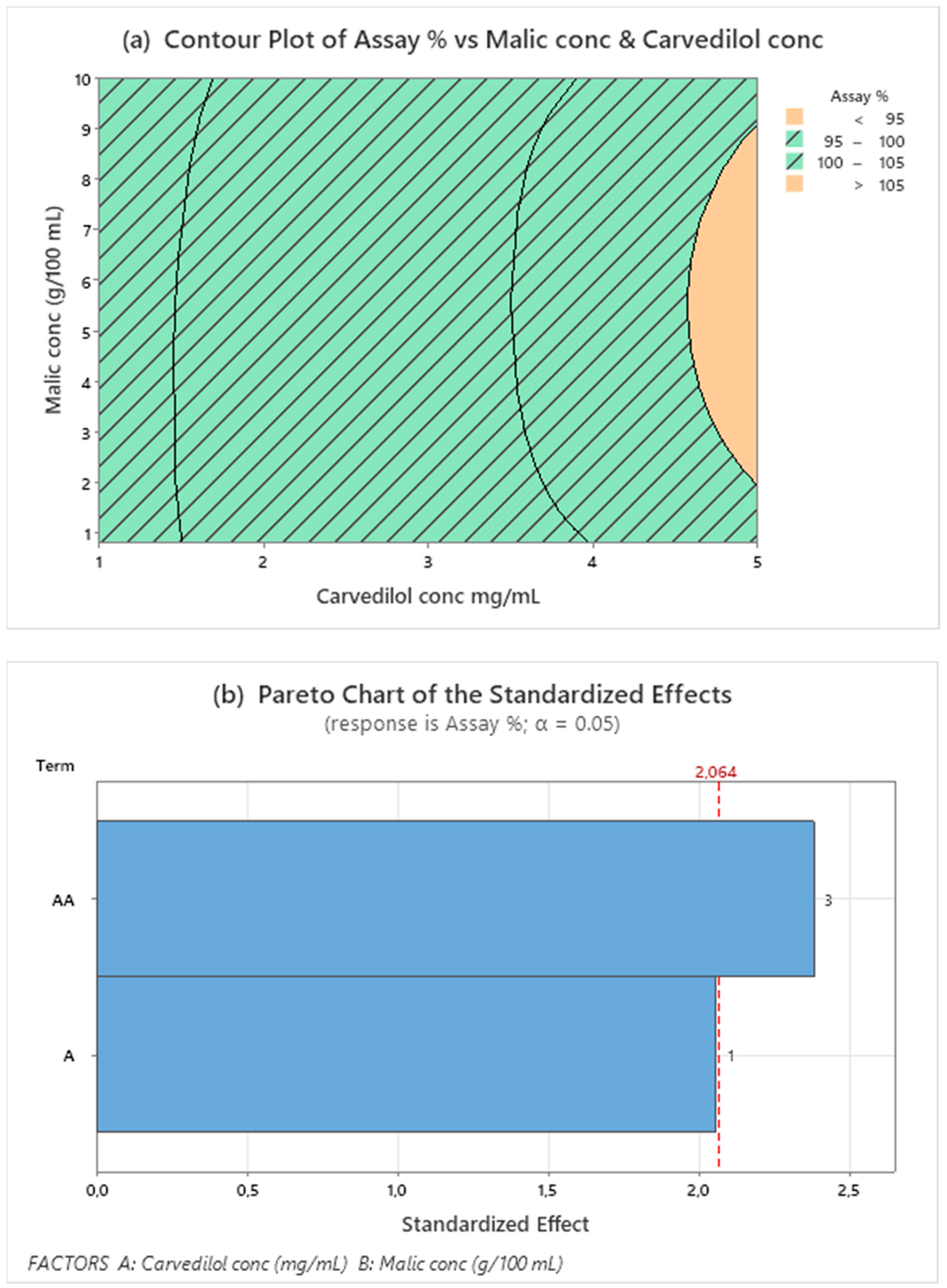
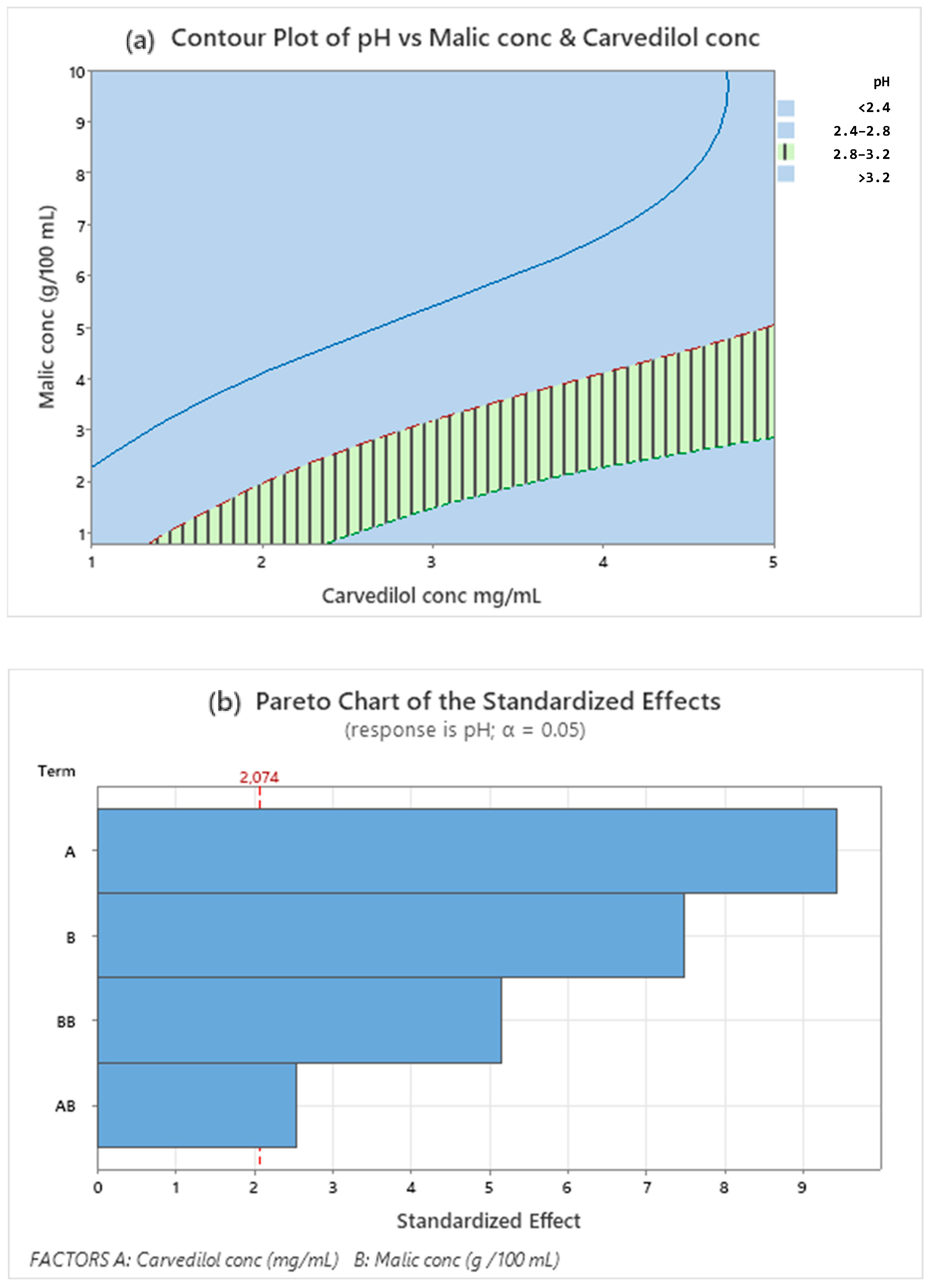
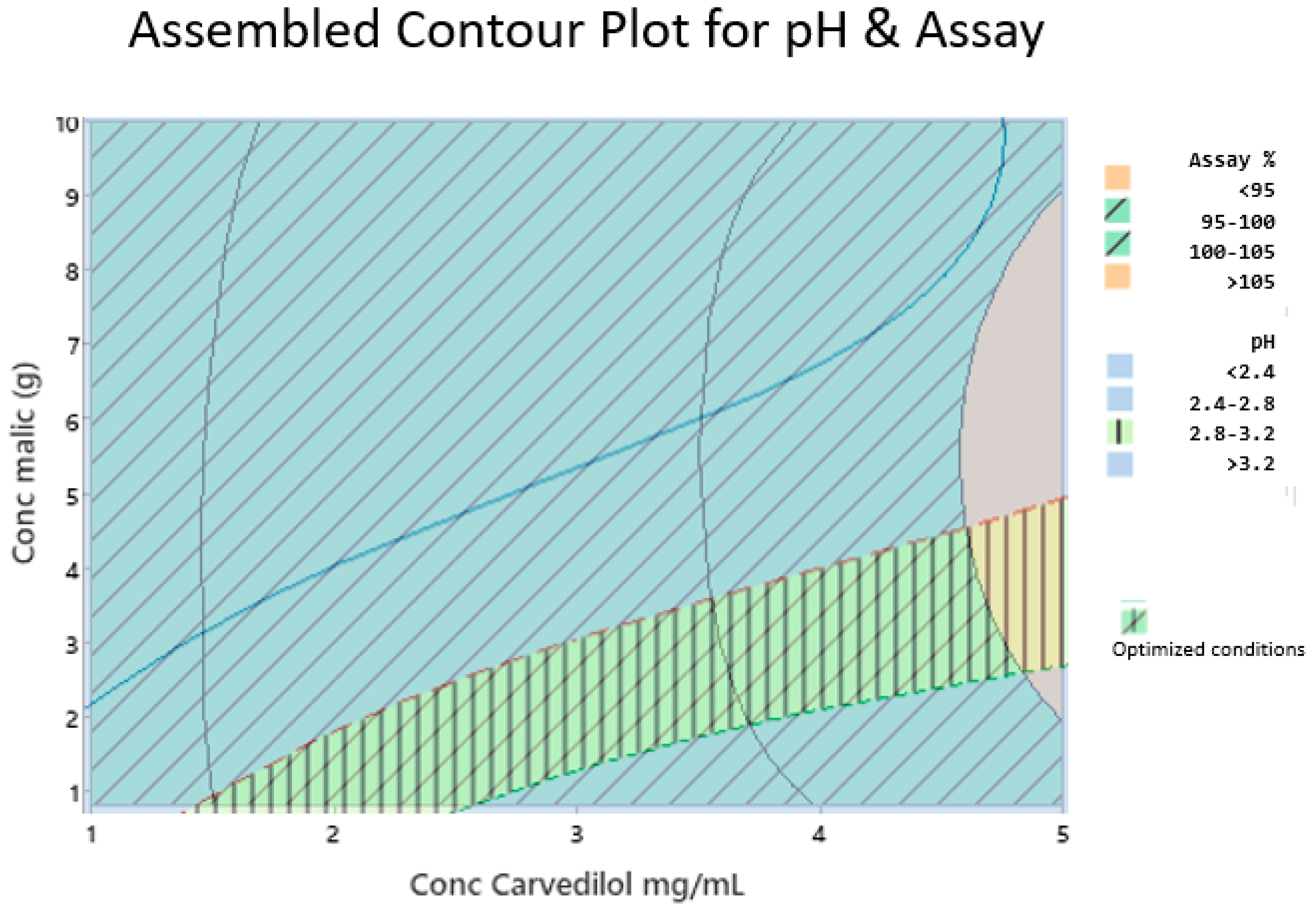
3.3.2. Design of Experiment (DoE)
3.3.3. Stability of Final CARV Formulations
3.3.4. Efficacy of Antimicrobial Preservation (Challenge Test)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Recla, S.; Schmidt, D.; Logeswaran, T.; Esmaeili, A.; Schranz, D. Pediatric Heart Failure Therapy: Why Β1-Receptor Blocker, Tissue ACE-I and Mineralocorticoid-Receptor-Blocker? Transl. Pediatr. 2019, 8, 127–132. [Google Scholar] [CrossRef]
- Vaidyanathan, B. Is There a Role for Carvedilol in the Management of Pediatric Heart Failure A Meta Analysis and E-Mail Survey of Expert Opinion. Ann. Pediatr. Cardiol. 2009, 2, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Bruns, L.A.; Chrisant, M.K.; Lamour, J.M.; Shaddy, R.E.; Pahl, E.; Blume, E.D.; Hallowell, S.; Addonizio, L.J.; Canter, C.E. Carvedilol as Therapy in Pediatric Heart Failure: An Initial Multicenter Experience. J. Pediatr. 2001, 138, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Starship Children’s Hospital. Clinical Guidelines. Carvedilol. 2020. Available online: https://starship.org.nz/guidelines/carvedilol (accessed on 30 May 2023).
- Bajcetic, M.; Samardzic, R. Effects of Carvedilol on Left Ventricular Function and Oxidative Stress in Infants and Children with Idiopathic Dilated Cardiomyopathy: A 12-Month, Two-Center, Open-Label Study. Clin. Ther. 2008, 30, 702–714. [Google Scholar] [CrossRef] [PubMed]
- Blume, E.D.; Canter, C.E.; Spicer, R.; Gauvreau, K.; Colan, S.; Jenkins, K.J. Prospective Single-Arm Protocol of Carvedilol in Children with Ventricular Dysfunction. Pediatr. Cardiol. 2006, 27, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Alabed, S.; Sabouni, A.; Al Dakhoul, S.; Bdaiwi, Y.; Frobel-Mercier, A.K. Beta-Blockers for Congestive Heart Failure in Children. Cochrane Database Syst. Rev. 2020, CD007037. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Human Medicines Development and Evaluation. Inventory of Paediatric Therapeutic Needs Cardiovascular Therapeutic Area. 2013. Available online: www.ema.europa.eu (accessed on 22 June 2023).
- Greenway, S.C.; Benson, L.N. The Use of Carvedilol in Pediatric Heart Failure. Cardiovasc. Hematol. Disord. Targets 2006, 6, 35–42. [Google Scholar] [CrossRef]
- Rouaz, K.; Chiclana-Rodríguez, B.; Nardi-Ricart, A.; Suñé-Pou, M.; Mercadé-Frutos, D.; Suñé-Negre, J.M.; Pérez-Lozano, P.; García-Montoya, E. Excipients in the Paediatric Population: A Review. Pharmaceutics 2021, 13, 387. [Google Scholar] [CrossRef]
- European Medicines Agency (EMA). Committee for Medicinal Products for Human Use (CHMP). Paediatric Committee (PDCO). Guideline on Pharmaceutical Development of Medicines for Paediatric Use. 2013. Available online: www.ema.europa.eu (accessed on 16 June 2023).
- Beattie, K.; Phadke, G.; Novakovic, J. Carvedilol. In Profiles of Drug Substances, Excipients and Related Methodology; Academic Press Inc.: Cambridge, MA, USA, 2013; Volume 38, pp. 113–157. [Google Scholar]
- Hamed, R.; Awadallah, A.; Sunoqrot, S.; Tarawneh, O.; Nazzal, S.; AlBaraghthi, T.; Al Sayyad, J.; Abbas, A. PH-Dependent Solubility and Dissolution Behavior of Carvedilol—Case Example of a Weakly Basic BCS Class II Drug. AAPS PharmSciTech 2016, 17, 418–426. [Google Scholar] [CrossRef]
- Nationwide Children’s Hospital. Specialties. Pharmacy Services. Compounding formulas. Carvedilol Oral. 2023. Available online: https://www.nationwidechildrens.org/specialties/pharmacy-services/compounding-formulas (accessed on 10 August 2023).
- Pharmaceutical Society of New Zealand. Services. Practice Support. Compounded Oral Liquid Formulaee. Carvedilol. 2021. Available online: https://www.psnz.org.nz/Folder?Action=View%20File&Folder_id=189&File=NZSOF%20Carvedilol%201mg-1mL.pdf (accessed on 15 June 2023).
- IWK Health Centre. IWK Compounding Formulas. Carvedilol Oral Suspension 1.25 mg/mL. 2010. Available online: https://www.iwk.nshealth.ca/sites/default/files/compounding-formulas/carvedilol_1.251.pdf?m=1 (accessed on 15 June 2023).
- Padagis. Products. Ora Sweet. Ora Blend. Available online: https://www.padagis.com/products/?letter=o (accessed on 26 June 2023).
- Watson, C.; Webb, E.A.; Kerr, S.; Davies, J.H.; Stirling, H.; Batchelor, H. How Close Is the Dose? Manipulation of 10 mg Hydrocortisone Tablets to Provide Appropriate Doses to Children. Int. J. Pharm. 2018, 545, 57–63. [Google Scholar] [CrossRef]
- Polonini, H.C.; Silva, S.L.; De Almeida, T.R.; Brandão, M.A.F.; Ferreira, A.O. Compatibility of Caffeine, Carvedilol, Clomipramine Hydrochloride, Folic Acid, Hydrochlorothiazide, Loperamide Hydrochloride, Methotrexate, Nadolol, Naltrexone Hydrochloride and Pentoxifylline in SyrSpend SF PH4 Oral Suspensions. Eur. J. Hosp. Pharm. 2016, 23, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Yamreudeewong, W.; Dolence, E.K.; Pahl, D. Stability of Two Extemporaneously Prepared Oral Metoprolol and Carvedilol Liquids; Wolters Kluwer Health, Inc.: Philadelphia, PA, USA, 2006; Volume 41. [Google Scholar]
- Buontempo, F.; Bernabeu, E.; Glisoni, R.J.; Quiroga, E.; Bregni, C.; Chiappetta, D.A. Carvedilol Stability in Paediatric Oral Liquid Formulations. Farm. Hosp. 2010, 34, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Allegaert, K.; Vanhaesebrouck, S.; Kulo, A.; Cosaert, K.; Verbesselt, R.; Debeer, A.; De Hoon, J. Prospective Assessment of Short-Term Propylene Glycol Tolerance in Neonates. Arch. Dis. Child. 2010, 95, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Operto, M.A.; Maggio, R.; Leonardi, D.; Vignaduzzo, S. Flexible New Dosage Forms Containing Carvedilol for the Treatment of Patients with Cardiovascular Disorders: Development, Stability, Palatability, and Microbiological Studies. AAPS PharmSciTech 2023, 24, 159. [Google Scholar] [CrossRef]
- Yochana, S.; Yu, M.; Alvi, M.; Varenya, S.; Chatterjee, P. Pharmaceutical Excipients and Pediatric Formulations. ChemToday 2012, 30, 56–61. [Google Scholar]
- Markeev, V.B.; Blynskaya, E.V.; Tishkov, S.V.; Alekseev, K.V.; Marakhova, A.I.; Vetcher, A.A.; Shishonin, A.Y. Composites of N-Butyl-N-Methyl-1-Phenylpyrrolo[1,2-a]Pyrazine-3-Carboxamide with Polymers: Effect of Crystallinity on Solubility and Stability. Int. J. Mol. Sci. 2023, 24, 12215. [Google Scholar] [CrossRef]
- Sun, J.; Du, J.; Liu, X.; An, J.; Li, Y.; Yu, Y.; Li, M.; Zheng, L.; Wu, C.; Hu, L. Preparation of Chitosan-Coated Hollow Tin Dioxide Nanoparticles and Their Application in Improving the Oral Bioavailability of Febuxostat. Int. J. Pharm. X 2023, 6, 100199. [Google Scholar] [CrossRef] [PubMed]
- Asad, M.; Rasul, A.; Abbas, G.; Shah, M.A.; Nazir, I. Self-Emulsifying Drug Delivery Systems: A Versatile Approach to Enhance the Oral Delivery of BCS Class III Drug via Hydrophobic Ion Pairing. PLoS ONE 2023, 18, e0286668. [Google Scholar] [CrossRef]
- Wegmann, M.; Parola, L.; Bertera, F.M.; Taira, C.A.; Cagel, M.; Buontempo, F.; Bernabeu, E.; Höcht, C.; Chiappetta, D.A.; Moretton, M.A. Novel Carvedilol Paediatric Nanomicelle Formulation: In-Vitro Characterization and in-Vivo Evaluation. J. Pharm. Pharmacol. 2017, 69, 544–553. [Google Scholar] [CrossRef]
- Choi, J.E.; Kim, J.S.; Choi, M.J.; Baek, K.; Woo, M.R.; Kim, J.O.; Choi, H.G.; Jin, S.G. Effects of Different Physicochemical Characteristics and Supersaturation Principle of Solidified SNEDDS and Surface-Modified Microspheres on the Bioavailability of Carvedilol. Int. J. Pharm. 2021, 597, 120377. [Google Scholar] [CrossRef]
- Sharma, M.; Sharma, R.; Jain, D.K.; Saraf, A. Enhancement of Oral Bioavailability of Poorly Water Soluble Carvedilol by Chitosan Nanoparticles: Optimization and Pharmacokinetic Study. Int. J. Biol. Macromol. 2019, 135, 246–260. [Google Scholar] [CrossRef] [PubMed]
- Ghassemi, S.; Haeri, A.; Shahhosseini, S.; Dadashzadeh, S. Labrasol-Enriched Nanoliposomal Formulation: Novel Approach to Improve Oral Absorption of Water-Insoluble Drug, Carvedilol. AAPS PharmSciTech 2018, 19, 2961–2970. [Google Scholar] [CrossRef]
- Khan, D.; Kirby, D.; Bryson, S.; Shah, M.; Mohammed, A.R. Development of an Age-Appropriate Mini Orally Disintegrating Carvedilol Tablet with Paediatric Biopharmaceutical Considerations. Pharmaceutics 2021, 13, 831. [Google Scholar] [CrossRef]
- European Medicines Agency. Human Regulatory. Research and Development. Paediatric Medicines. Paediatric Investigation Plans. Available online: https://www.ema.europa.eu/en/human-regulatory/research-development/paediatric-medicines/paediatric-investigation-plans (accessed on 31 May 2023).
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonised Guideline. Addendum to ICH E11: Guideline on Clinical Investigation of Medicinal Products in the Pediatric Population E11(R1). Final Version. 2017. Available online: https://database.ich.org/sites/default/files/E11_R1_Addendum.pdf (accessed on 12 August 2023).
- Committee for Medicinal Products for Human Use (CHMP). Reflection Paper: Formulations of Choice for the Paediatric Population Agreed by Paediatric Working Party & Quality Working Party Adoption by Chmp for Release for Consultation End of Consultation (Deadline for Comments). Available online: https://www.ema.europa.eu/en/formulations-choice-paediatric-population (accessed on 20 June 2023).
- Carvedilol: Pediatric Drug Information—UpToDate. Available online: www.uptodate.com (accessed on 3 June 2023).
- Colegio Oficial de Farmacéuticos de Bizkaia. Formulación Magistral de Medicamentos, 4th ed.; COF Bizkaia: Bilbao, Spain, 2004; pp. 409–410. [Google Scholar]
- International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. ICH Harmonised Guideline. Biopharmaceutics Classification System-Based Biowaivers M9. Final version. 2019. Available online: https://database.ich.org/sites/default/files/M9_Guideline_Step4_2019_1116.pdf (accessed on 20 June 2023).
- Council of Europe. Recommendations on Dissolution Testing (5.17.1.). In European Pharmacopoeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- Council of Europe. European Pharmacopoeia, 11th ed.; General Monographs; Carvedilol; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- International Conference of Harmonization (ICH). Stability Testing of New Drug Substances and Products Q2(R1). 2003. Available online: https://database.ich.org/sites/default/files/Q1A%28R2%29%20Guideline.pdf (accessed on 26 May 2023).
- Council of Europe. Efficacy of Antimicrobial Preservation (5.1.3). In European Pharmacopeia, 11th ed.; Council of Europe: Strasbourg, France, 2023. [Google Scholar]
- Attebäck, M.; Hedin, B.; Mattsson, S. Formulation Optimization of Extemporaneous Oral Liquids Containing Naloxone and Propranolol for Pediatric Use. Sci. Pharm. 2022, 90, 15. [Google Scholar] [CrossRef]
- Zhao, D.; Tsoi, J.K.H.; Wong, H.M.; Chu, C.H.; Matinlinna, J.P. Paediatric Over-the-Counter (OTC) Oral Liquids Can Soften and Erode Enamel. Dent. J. 2017, 5, 17. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, S.; Mathiron, D.; Moufawad, T.; Landy, D.; Djedaini-Pilard, F.; Marçon, F. Cyclodextrin Complexation as a Way of Increasing the Aqueous Solubility and Stability of Carvedilol. Pharmaceutics 2021, 13, 1746. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Development of Paediatric Medicines: Pharmaceutical Development; Points to Consider. Working Document QAS/08.257; World Health Organization: Geneva, Switzerland, 2008.
- Rowe, R.C.; Sheskey, P.J.; Owen, S.C. Handbook of Pharmaceutical Excipients, 6th ed.; Pharmaceutical Press: London, UK, 2006. [Google Scholar]
- European Paediatric Formulation Initiative (EuPFI). STEP Database. Available online: http://www.eupfi.org/step-database-info/ (accessed on 27 June 2023).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pH | Solubility (mg/mL) |
|---|---|
| 1.2 | 0.027 (±0.003) |
| 4.5 | 1.280 (±0.050) |
| 6.8 | 0.037 (±0.002) |
| pH | Acetic Media | Phosphoric Media | Citric Media | Malic Media |
|---|---|---|---|---|
| 2.0 | NS | S/not stable > 24 h | S/stable > 24 h | S/stable > 24 h |
| 2.5 | NS | S/not stable > 24 h | S/stable > 24 h | S/stable > 24 h |
| 3.0 | NS | NS | NS | S/stable > 24 h |
| 3.5 | S/difficult dissolution | NS | NS | NS |
| 4.0 | S/stable > 24 h | NS | NS | NS |
| 4.5 | S/stable > 24 h | NS | NS | NS |
| 5.0 | NS | NS | NS | NS |
| CARV Assay (%) | |||||
|---|---|---|---|---|---|
| Storage Temperature | 1 Week | 2 Weeks | 4 Weeks | 8 Weeks | 12 Weeks |
| F1 formulation (acetic media pH 4.0) | |||||
| 25 °C | 103.07 ± 1 | 102.70 ± 2 | 102.50 ± 1 | 101.80 ± 1 | 101.78 ± 2 |
| 40 °C | - | 102.20 ± 3 | 101.07 ± 1 | - | 101.90 ± 1 |
| F2 formulation (acetic media pH 4.5) | |||||
| 25 °C | 101.67 ± 1 | 101.37 ± 1 | 101.24 ± 1 | 101.16 ± 1 | 101.10 ± 1 |
| 30 °C | 101.26 ± 2 | 101.60 ± 1 | 101.45 ± 3 | 101.54 ± 2 | 101.50 ± 1 |
| 40 °C | 101.05 ± 1 | 100.50 ± 2 | 100.10 ± 2 | - | - |
| CARV Assay (%) | |||||
|---|---|---|---|---|---|
| Storage Temperature | 1 Week | 2 Weeks | 4 Weeks | 8 Weeks | 12 Weeks |
| F3 formulation (citric media pH 2.0) | |||||
| 25 °C | 98.13 ± 2 | 97.02 ± 1 | 96.38 ± 1 | 96.40 ± 2 | 95.02 ± 1 |
| F4 formulation (citric media pH 2.5) | |||||
| 25 °C | 100.46 ± 1 | 98.26 ± 3 | 97.02 ± 2 | 96.49 ± 1 | 95.78 ± 1 |
| CARV Assay (%) | |||||
|---|---|---|---|---|---|
| Storage Temperature | 1 Week | 2 Weeks | 4 Weeks | 8 Weeks | 12 Weeks |
| F5 formulation (malic media pH 2.0) | |||||
| 25 °C | 103.01 ± 1 | 102.26 ± 3 | 103.61 ± 2 | 101.50 ± 1 | 101.87 ± 2 |
| 40 °C | - | - | 102.50 ± 1 | 101.04 ± 1 | 101.10 ± 1 |
| F6 formulation (malic media pH 2.7) | |||||
| 25 °C | 102.40 ± 1 | 102.20 ± 1 | 102.50 ± 1 | 101.30 ± 2 | 101.20 ± 1 |
| 40 °C | - | - | 102.05 ± 1 | 101.70 ± 1 | 100.80 ± 1 |
| F7_1 | F7_2 | F7_3 | F7_4 | F7_5 | F7_6 | F7_7 | F7_8 | F7_9 | |
|---|---|---|---|---|---|---|---|---|---|
| CARV (mg/mL) | 1 | 3 | 5 | ||||||
| Malic acid (% m/v) | 0.8 | 5.4 | 10.0 | 0.8 | 5.4 | 10.0 | 0.8 | 5.4 | 10.0 |
| Malic Acid Concentration | |||||||
|---|---|---|---|---|---|---|---|
| 0.8% | 5.4% | 10.0% | |||||
| Batch | CARV Assay (%) | Batch | CARV Assay (%) | Batch | CARV Assay (%) | ||
| CARV concentration (mg/mL) | 1 | F7_1_1 | 102.14 | F7_2_1 | 100.73 | F7_3_1 | 102.67 |
| F7_1_2 | 101.31 | F7_2_2 | 102.66 | F7_3_2 | 103 | ||
| F7_1_3 | 100.12 | F7_2_3 | 101.78 | F7_3_3 | 99.76 | ||
| 3 | F7_4_1 | 99.07 | F7_5_1 | 99.53 | F7_6_1 | 97.86 | |
| F7_4_2 | 100.36 | F7_5_2 | 100.11 | F7_6_2 | 99.23 | ||
| F7_4_3 | 97.09 | F7_5_3 | 96.88 | F7_6_3 | 99.68 | ||
| 5 | F7_7_1 | 112.38 | F7_8_1 | 99.33 | F7_9_1 | 112.73 | |
| F7_7_2 | 98.44 | F7_8_2 | 112.65 | F7_9_2 | 100.35 | ||
| F7_7_3 | 97.66 | F7_8_3 | 111.93 | F7_9_3 | 96.78 | ||
| Malic Acid Concentration | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0.8% | 5.4% | 10.0% | ||||||||
| Batch | pH | Appearance after 24 h | Batch | pH | Appearance after 24 h | Batch | pH | Appearance after 24 h | ||
| CARV concentration (mg/mL) | 1 | F7_1_1 | 2.6 | Conform | F7_2_1 | 2.0 | Conform | F7_3_1 | 1.80 | Conform |
| F7_1_2 | 2.6 | F7_2_2 | 2.0 | F7_3_2 | 1.80 | |||||
| F7_1_3 | 2.75 | F7_2_3 | 2.05 | F7_3_3 | 1.85 | |||||
| 3 | F7_4_1 | 3.2 | Not conform | F7_5_1 | 2.35 | Conform | F7_6_1 | 1.85 | Conform | |
| F7_4_2 | 3.4 | F7_5_2 | 2.35 | F7_6_2 | 2.0 | |||||
| F7_4_3 | 3.55 | F7_5_3 | 2.50 | F7_6_3 | 2.15 | |||||
| 5 | F7_7_1 | 3.6 | Not conform | F7_8_1 | 2.75 | Conform | F7_9_1 | 2.40 | Conform | |
| F7_7_2 | 3.6 | F7_8_2 | 2.65 | F7_9_2 | 2.45 | |||||
| F7_7_3 | 3.95 | F7_8_3 | 2.85 | F7_9_3 | 2.6 | |||||
| F7_1_1 Formulation | ||||||
|---|---|---|---|---|---|---|
| Storage Temperature | T0 | 1 Month | 3 Months | 6 Months | 9 Months | 12 Months |
| % CARV Assay (mean of three batches ± SD) | ||||||
| 25 °C | 100.16 ± 1.48 | 101.60 ± 1.55 | 102.49 ± 0.05 | 100.71 ± 2.20 | 103.25 ± 0.63 | 100.50 ± 1.57 |
| 30 °C | 102.71 ± 0.84 | 102.02 ± 0.58 | 100.37 ± 1.16 | 103.56 ± 0.62 | 102.63 ± 1.62 | |
| 40 °C | 101.96 ± 1.46 | 102.03 ± 0.77 | 102.20 ± 1.10 | - | - | |
| P. aeruginosa (ATCC 9027) | S. aureus (ATCC 6538) | E. coli (ATCC 8739) | C. albicans (ATCC 10231) | A. brasiliensis (ATCC 16404) | ||
|---|---|---|---|---|---|---|
| Inoculum | 0 h | 8.00 | 9.11 | 9.04 | 8.88 | 5.73 |
| F8_1 | 0 h | <2 | <2 | <2 | 6.86 | <4 |
| 14 days | <2 | <2 | <2 | <2 | <2 | |
| 28 days | <1 | <1 | <1 | <1 | <1 | |
| F8_2 | 0 h | <2 | 3 | <2 | 6.81 | <4 |
| 14 days | <2 | <2 | <2 | <2 | <2 | |
| 28 days | <1 | <1 | <1 | <1 | 1 | |
| F8_3 | 0 h | <2 | 4.77 | <2 | 6.93 | <4 |
| 14 days | <2 | <2 | <2 | <2 | <2 | |
| 28 days | <1 | <1 | <1 | <1 | 1.69 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiclana-Rodríguez, B.; Garcia-Montoya, E.; Rouaz-El Hajoui, K.; Romero-Obon, M.; Nardi-Ricart, A.; Suñé-Pou, M.; Suñé-Negre, J.M.; Pérez-Lozano, P. Development of a Carvedilol Oral Liquid Formulation for Paediatric Use. Pharmaceutics 2023, 15, 2283. https://doi.org/10.3390/pharmaceutics15092283
Chiclana-Rodríguez B, Garcia-Montoya E, Rouaz-El Hajoui K, Romero-Obon M, Nardi-Ricart A, Suñé-Pou M, Suñé-Negre JM, Pérez-Lozano P. Development of a Carvedilol Oral Liquid Formulation for Paediatric Use. Pharmaceutics. 2023; 15(9):2283. https://doi.org/10.3390/pharmaceutics15092283
Chicago/Turabian StyleChiclana-Rodríguez, Blanca, Encarnacion Garcia-Montoya, Khadija Rouaz-El Hajoui, Miquel Romero-Obon, Anna Nardi-Ricart, Marc Suñé-Pou, Josep M. Suñé-Negre, and Pilar Pérez-Lozano. 2023. "Development of a Carvedilol Oral Liquid Formulation for Paediatric Use" Pharmaceutics 15, no. 9: 2283. https://doi.org/10.3390/pharmaceutics15092283
APA StyleChiclana-Rodríguez, B., Garcia-Montoya, E., Rouaz-El Hajoui, K., Romero-Obon, M., Nardi-Ricart, A., Suñé-Pou, M., Suñé-Negre, J. M., & Pérez-Lozano, P. (2023). Development of a Carvedilol Oral Liquid Formulation for Paediatric Use. Pharmaceutics, 15(9), 2283. https://doi.org/10.3390/pharmaceutics15092283