Author Contributions
T.X.: methodology, formal analysis, investigation, data curation, writing—original draft, writing—review and editing, funding acquisition. H.L.: conceptualization, methodology, formal analysis, data curation, writing—original draft. Y.X.: methodology, formal analysis, investigation, data curation. S.D.: formal analysis, investigation. Q.Y.: methodology, formal analysis, conceptualization, writing—review and editing, funding acquisition. G.Y.: conceptualization, writing—review and editing, funding acquisition. All authors have read and agreed to the published version of the manuscript.
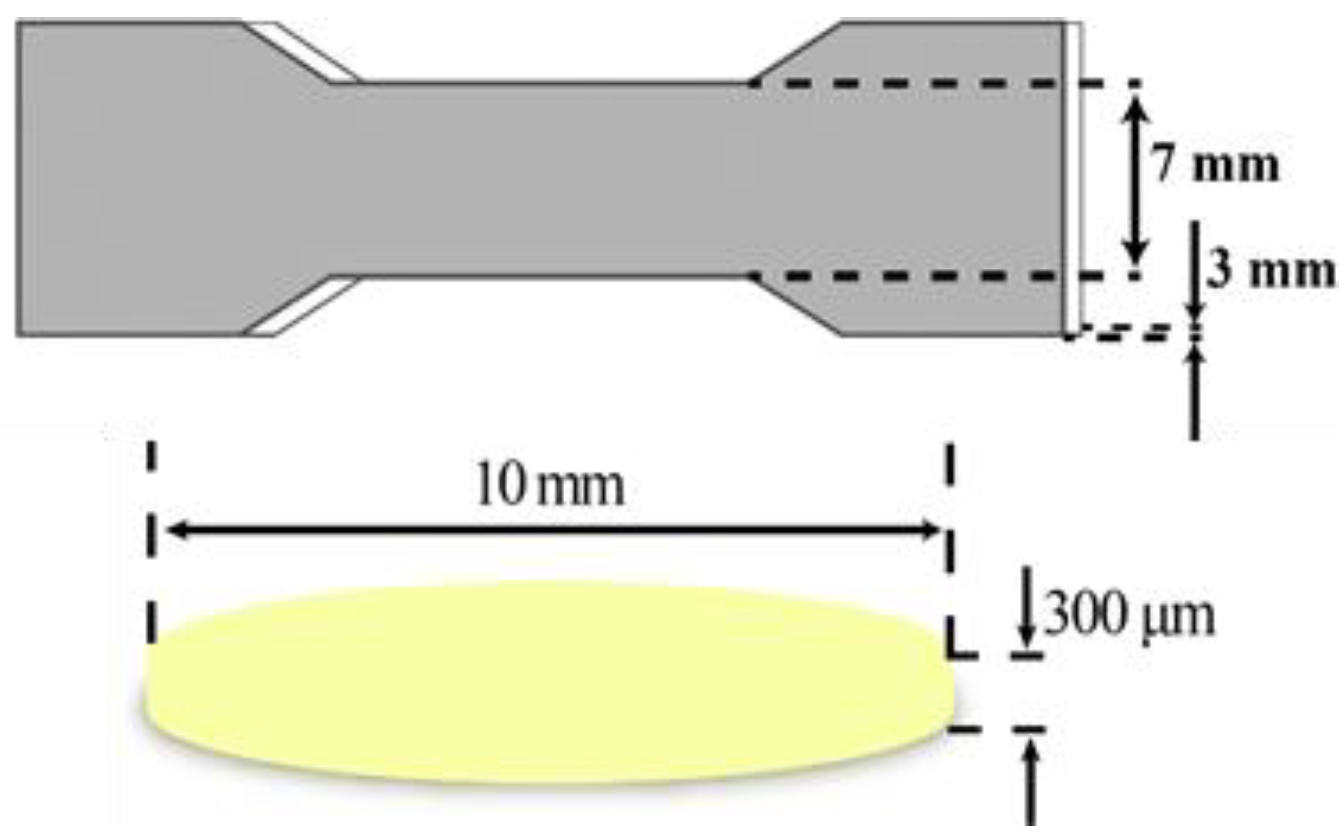
Figure 1.
The dimensions of specimen for mechanical tests and oral film samples.
Figure 1.
The dimensions of specimen for mechanical tests and oral film samples.
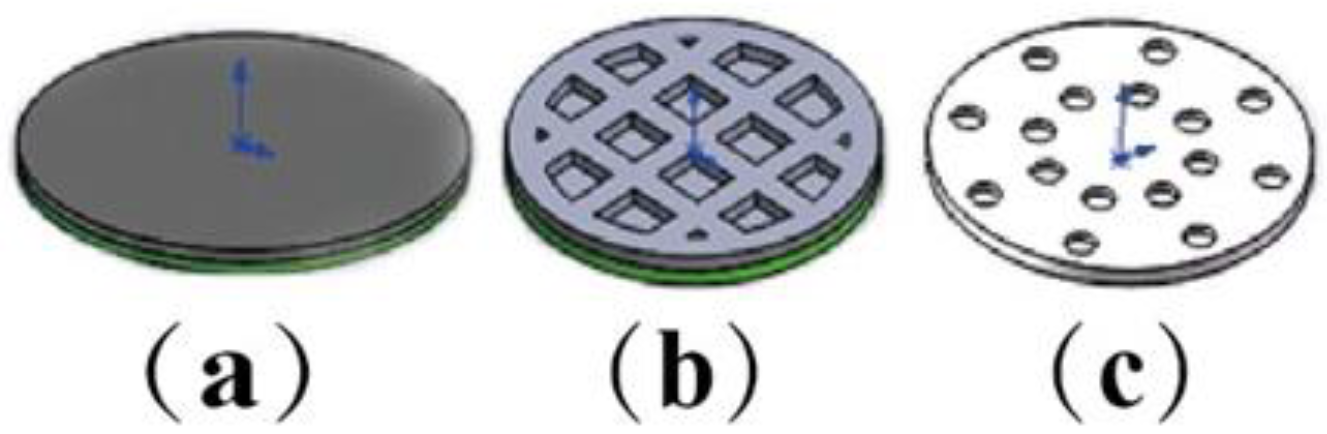
Figure 2.
The models of oral films: (a) solid sample, (b) hollow grid, (c) concentric holes.
Figure 2.
The models of oral films: (a) solid sample, (b) hollow grid, (c) concentric holes.
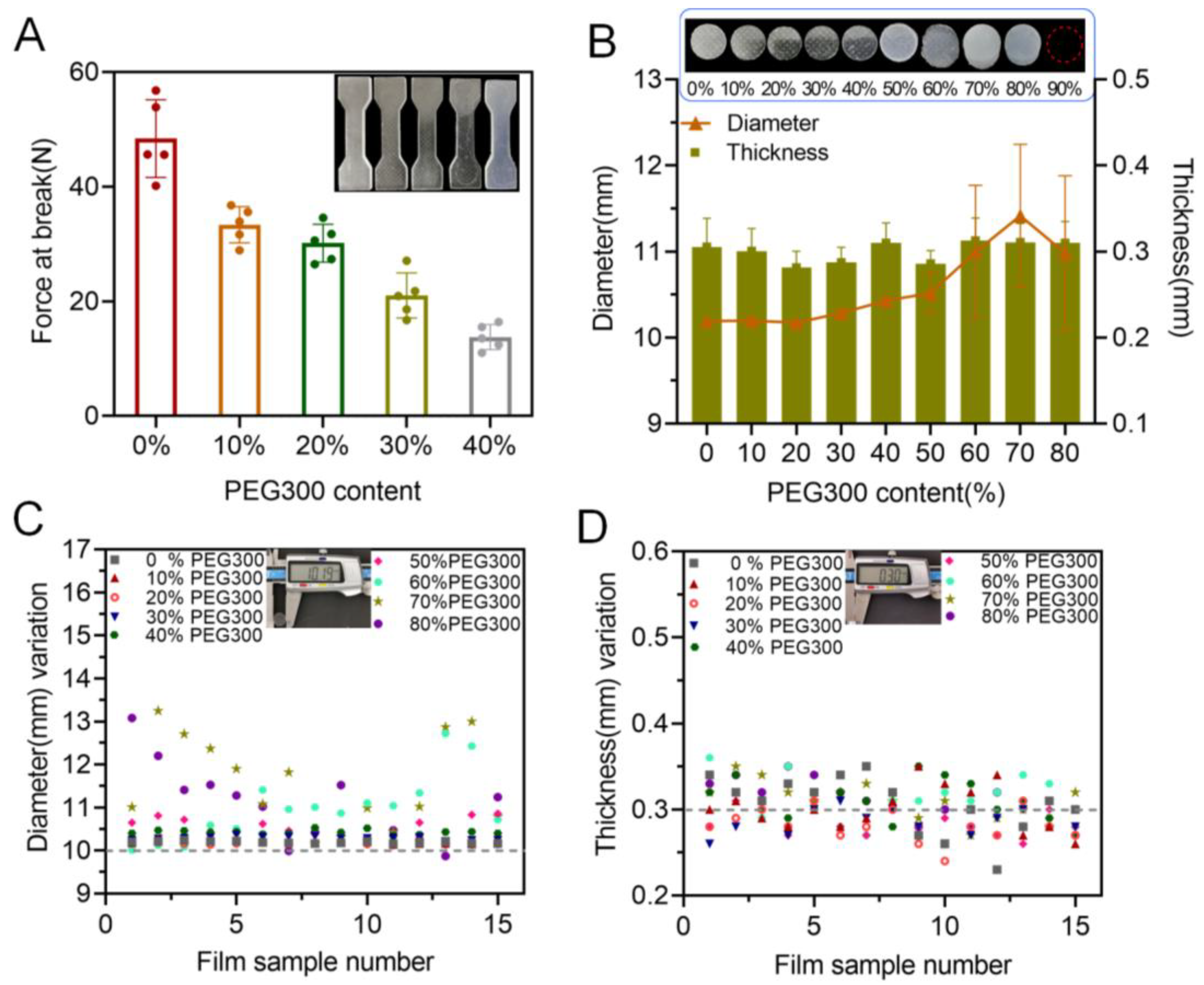
Figure 3.
Effect of PEG concentration on printability: (A) effect of PEG content on the tensile strength (n = 6); (B) effect of PEG content on the diameter and thickness of the produced oral films (n = 15); (C) diameter variations of the 3D-printed oral films; (D) thickness variations of the 3D-printed oral films.
Figure 3.
Effect of PEG concentration on printability: (A) effect of PEG content on the tensile strength (n = 6); (B) effect of PEG content on the diameter and thickness of the produced oral films (n = 15); (C) diameter variations of the 3D-printed oral films; (D) thickness variations of the 3D-printed oral films.
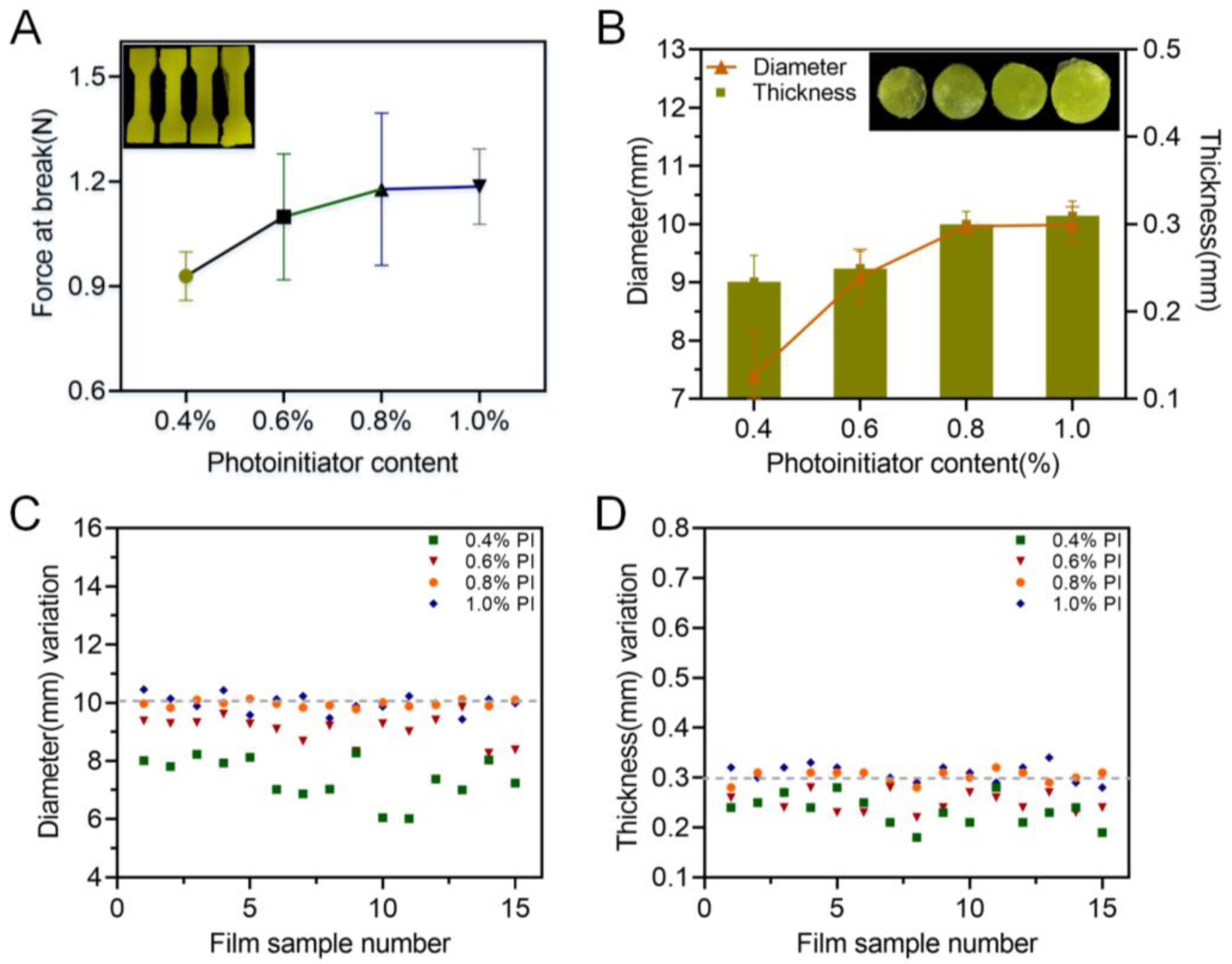
Figure 4.
Effect of the photoinitiator on the printability: (A) force at break of specimen samples (n = 6); (B) thickness and diameter of 3D-printed oral film samples (n = 15); (C) diameter variations and (D) thickness variations of 3D-printed oral film samples.
Figure 4.
Effect of the photoinitiator on the printability: (A) force at break of specimen samples (n = 6); (B) thickness and diameter of 3D-printed oral film samples (n = 15); (C) diameter variations and (D) thickness variations of 3D-printed oral film samples.
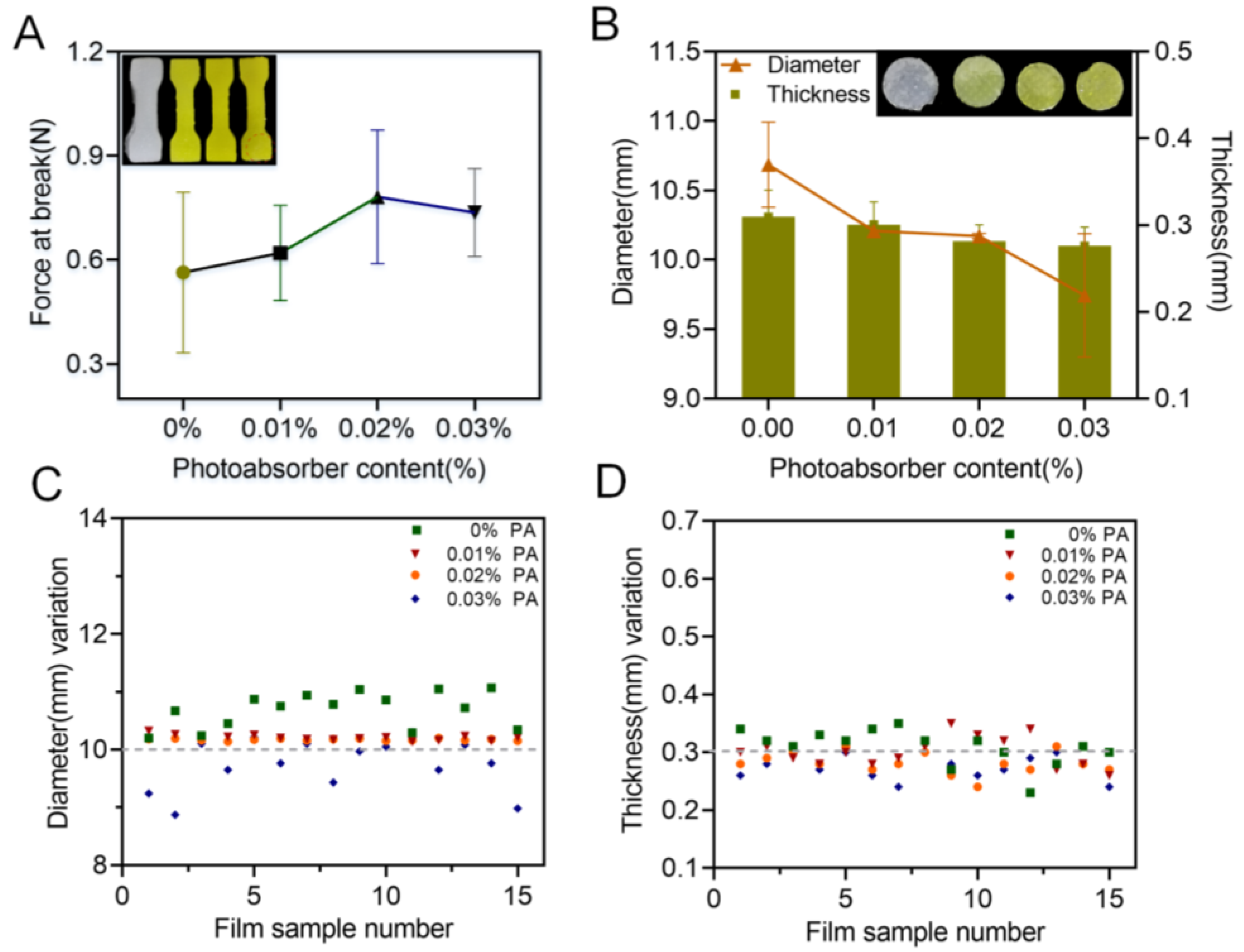
Figure 5.
Effect of the photoabsorber on the printability: (A) force at break of specimen samples (n = 6); (B) thickness and diameter of 3D-printed oral film samples (n = 15); (C) diameter variations and (D) thickness variations of 3D-printed oral film samples.
Figure 5.
Effect of the photoabsorber on the printability: (A) force at break of specimen samples (n = 6); (B) thickness and diameter of 3D-printed oral film samples (n = 15); (C) diameter variations and (D) thickness variations of 3D-printed oral film samples.
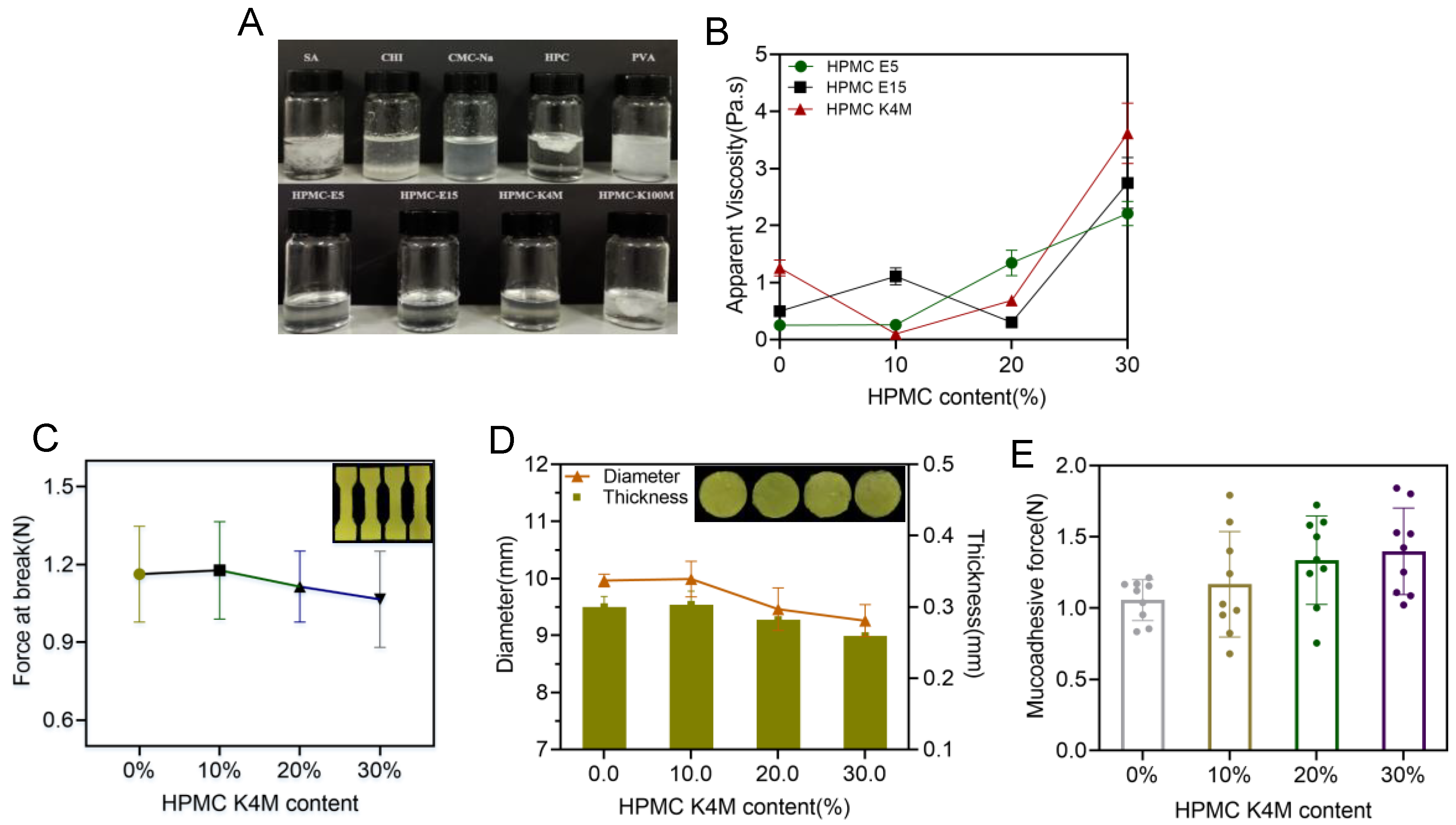
Figure 6.
(A) The physical state of adhesive materials mixture; (B) viscosity of the printing resin containing HPMC E5, E15, K4M at different concentrations (n = 6); (C) effect of HPMC K4M on the force at break of 3D-printed oral films (n = 6); (D) effect of HPMC K4M on the thickness and diameter of 3D-printed oral films(n = 15); (E) effect of HPMC K4M on the mucoadhesive force of 3D-printed oral films (n = 6).
Figure 6.
(A) The physical state of adhesive materials mixture; (B) viscosity of the printing resin containing HPMC E5, E15, K4M at different concentrations (n = 6); (C) effect of HPMC K4M on the force at break of 3D-printed oral films (n = 6); (D) effect of HPMC K4M on the thickness and diameter of 3D-printed oral films(n = 15); (E) effect of HPMC K4M on the mucoadhesive force of 3D-printed oral films (n = 6).
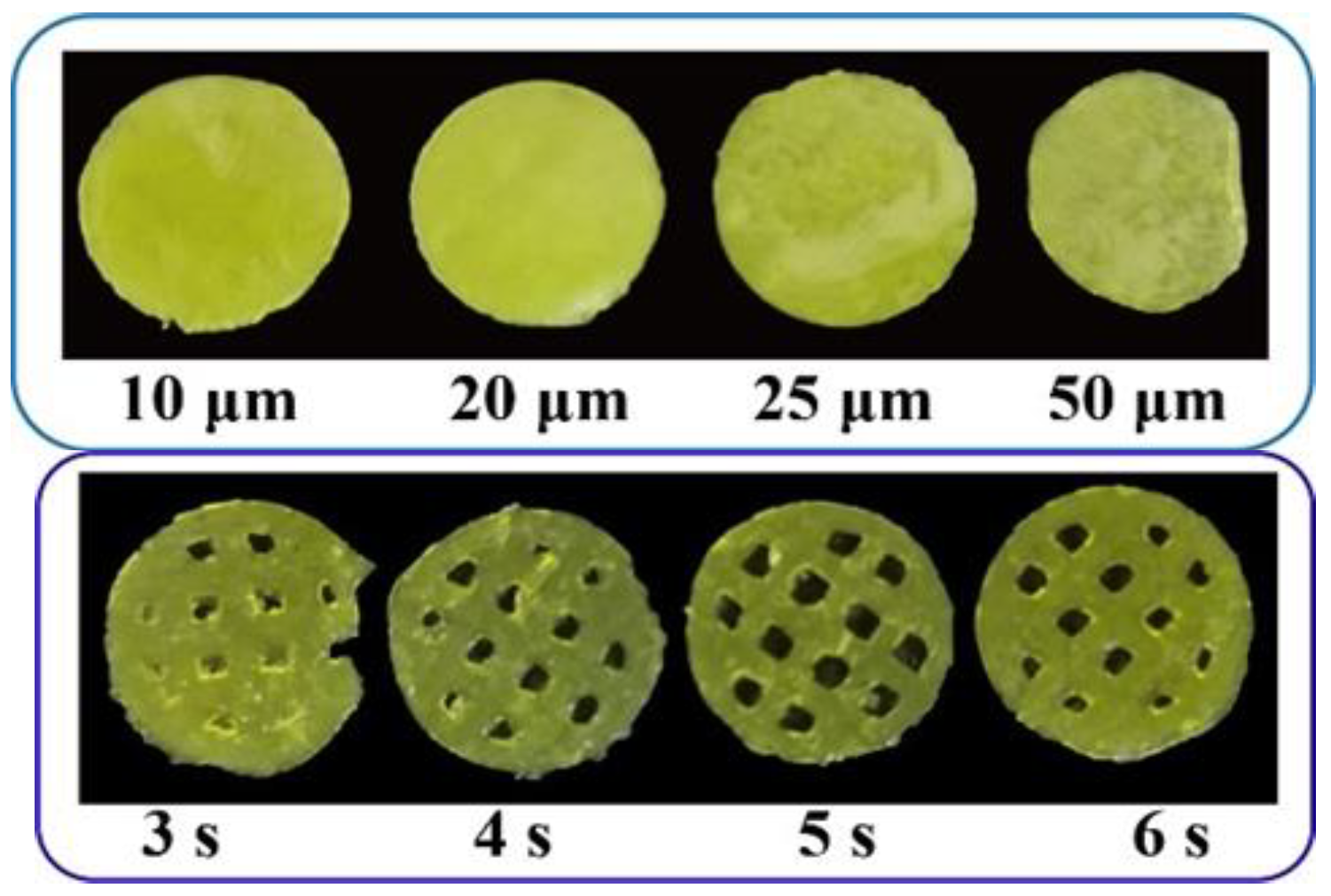
Figure 7.
Pictures of 3D-printed oral films with different printing parameters.
Figure 7.
Pictures of 3D-printed oral films with different printing parameters.
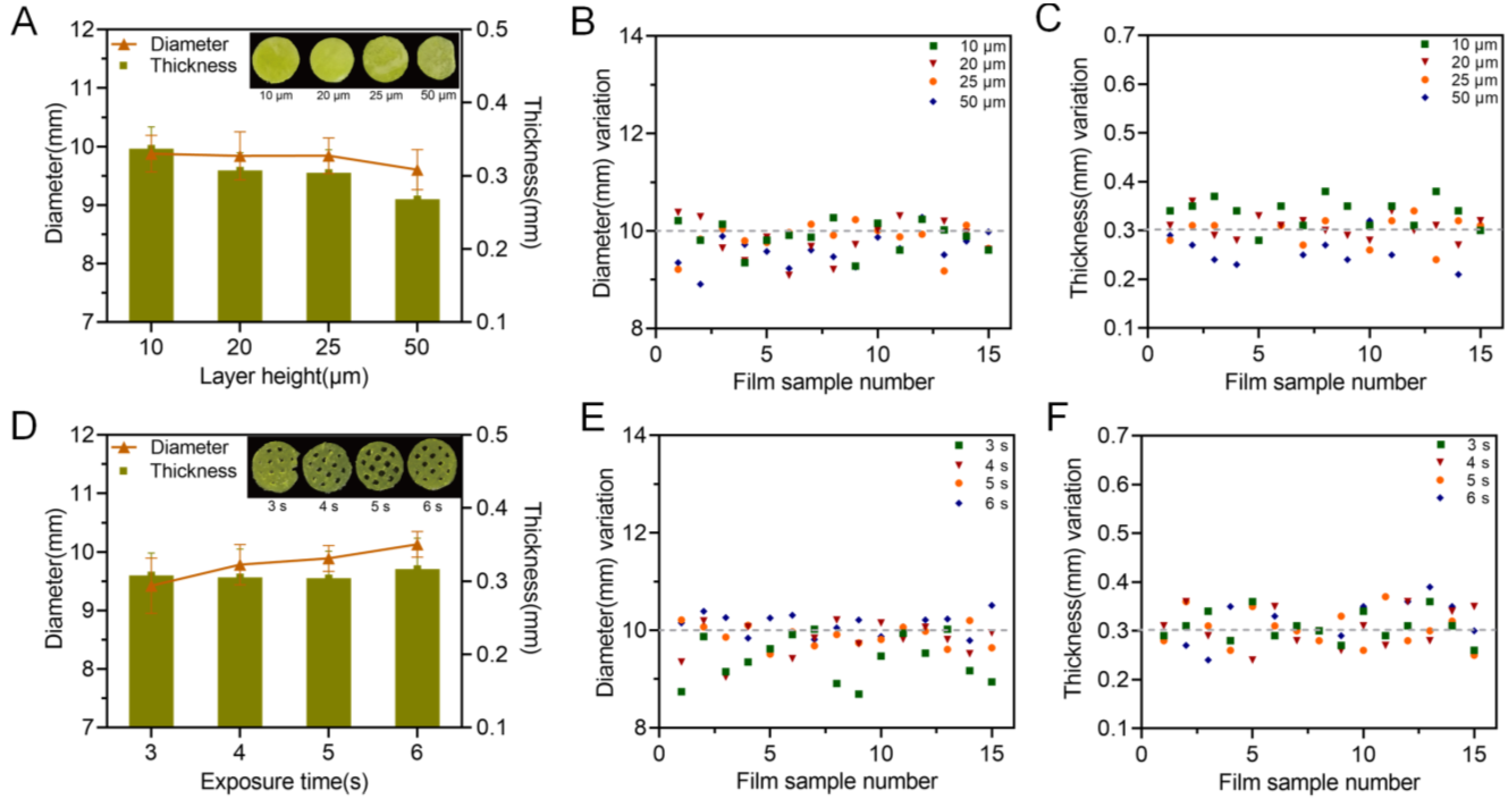
Figure 8.
Influence of printing parameters on the printability of the oral films. Exposure time and layer height; (A) effect of layer height on the diameter and thickness of 3D-printed oral films (n = 15); (B) diameter variations and (C) thickness variations of 3D-printed oral film samples from (A); (D) effect of exposure time on the diameter and thickness of 3D-printed oral films (n = 15); (E) diameter variations and (F) thickness variations of 3D-printed oral film samples from (D).
Figure 8.
Influence of printing parameters on the printability of the oral films. Exposure time and layer height; (A) effect of layer height on the diameter and thickness of 3D-printed oral films (n = 15); (B) diameter variations and (C) thickness variations of 3D-printed oral film samples from (A); (D) effect of exposure time on the diameter and thickness of 3D-printed oral films (n = 15); (E) diameter variations and (F) thickness variations of 3D-printed oral film samples from (D).
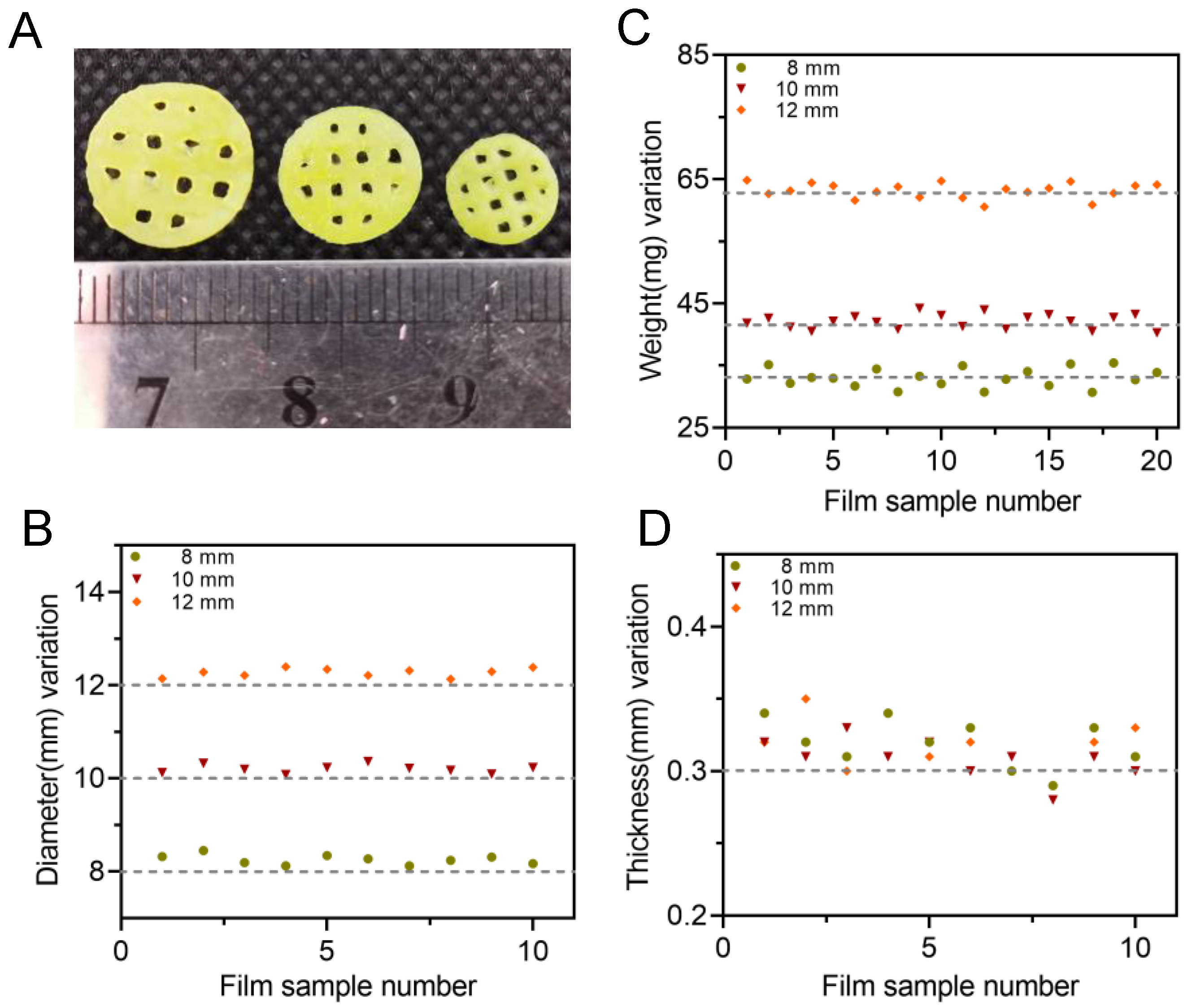
Figure 9.
(A) Appearances of 3D-printed oral films with three different diameters; (B) diameter variation of oral films (n = 10); (C) weight variation of oral film (n = 20) and (D) thickness of oral films (n = 10).
Figure 9.
(A) Appearances of 3D-printed oral films with three different diameters; (B) diameter variation of oral films (n = 10); (C) weight variation of oral film (n = 20) and (D) thickness of oral films (n = 10).
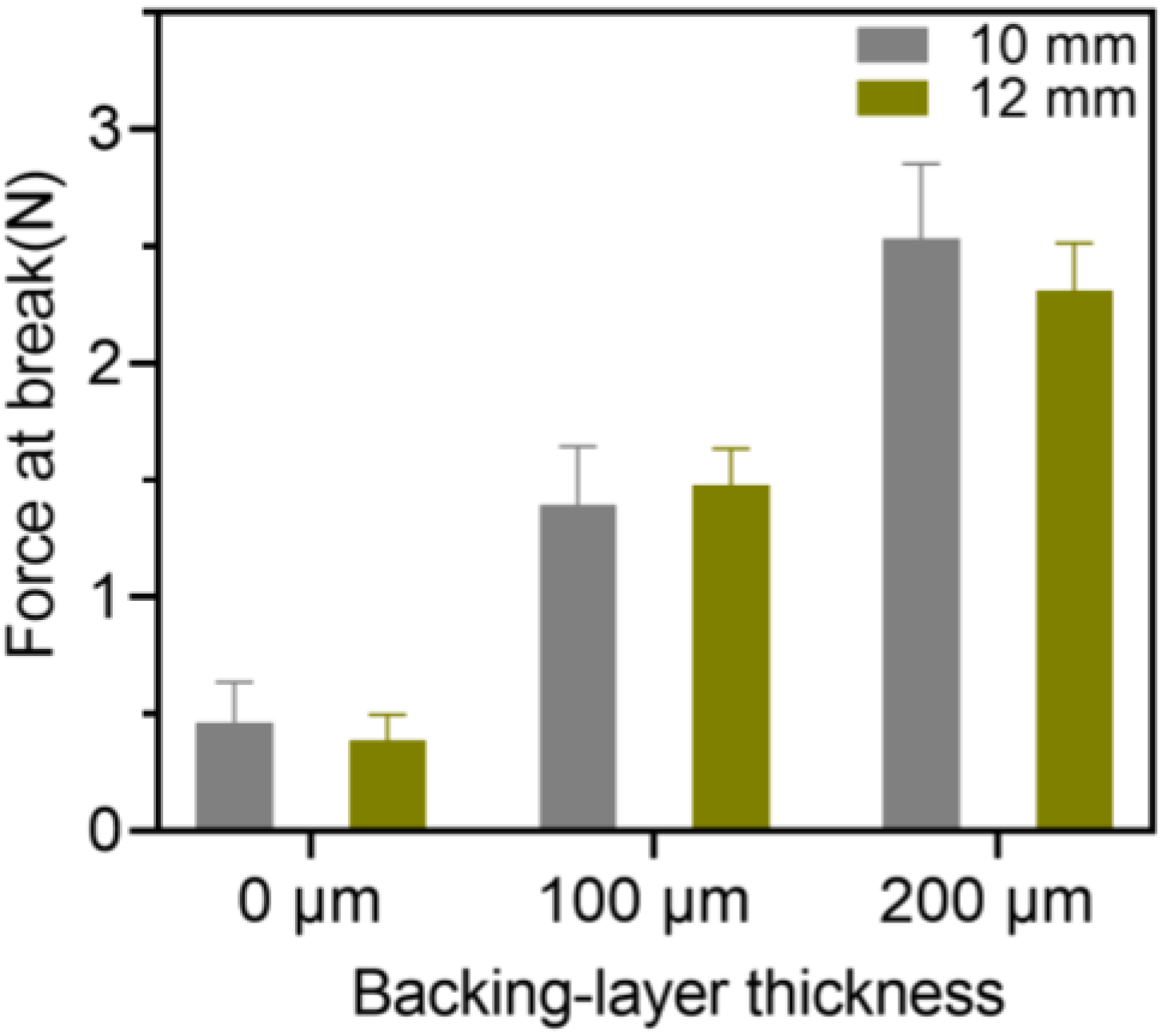
Figure 10.
Breaking force of the 3D-printed bilayer oral films (n = 6).
Figure 10.
Breaking force of the 3D-printed bilayer oral films (n = 6).
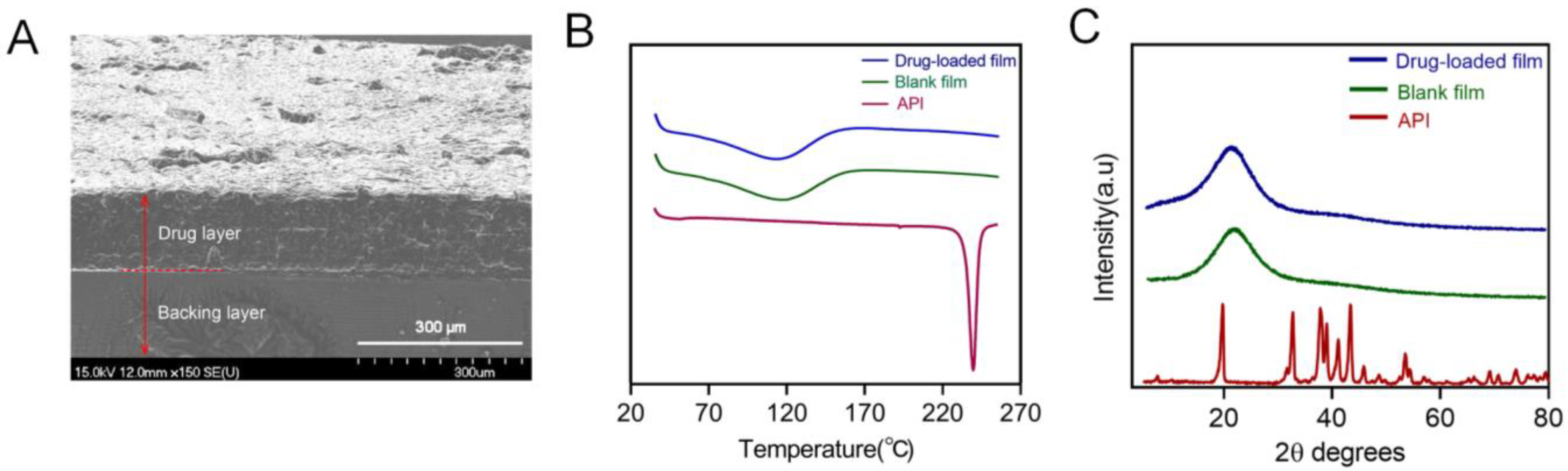
Figure 11.
(A) Cross-sectional morphology of the printed bilayer film; (B) DSC analysis pattern spectra of dexamethasone acetate, polymer film, drug-loaded bilayer film; (C) the X-ray Powder Diffraction spectra of dexamethasone acetate, polymer, drug-loaded bilayer film.
Figure 11.
(A) Cross-sectional morphology of the printed bilayer film; (B) DSC analysis pattern spectra of dexamethasone acetate, polymer film, drug-loaded bilayer film; (C) the X-ray Powder Diffraction spectra of dexamethasone acetate, polymer, drug-loaded bilayer film.
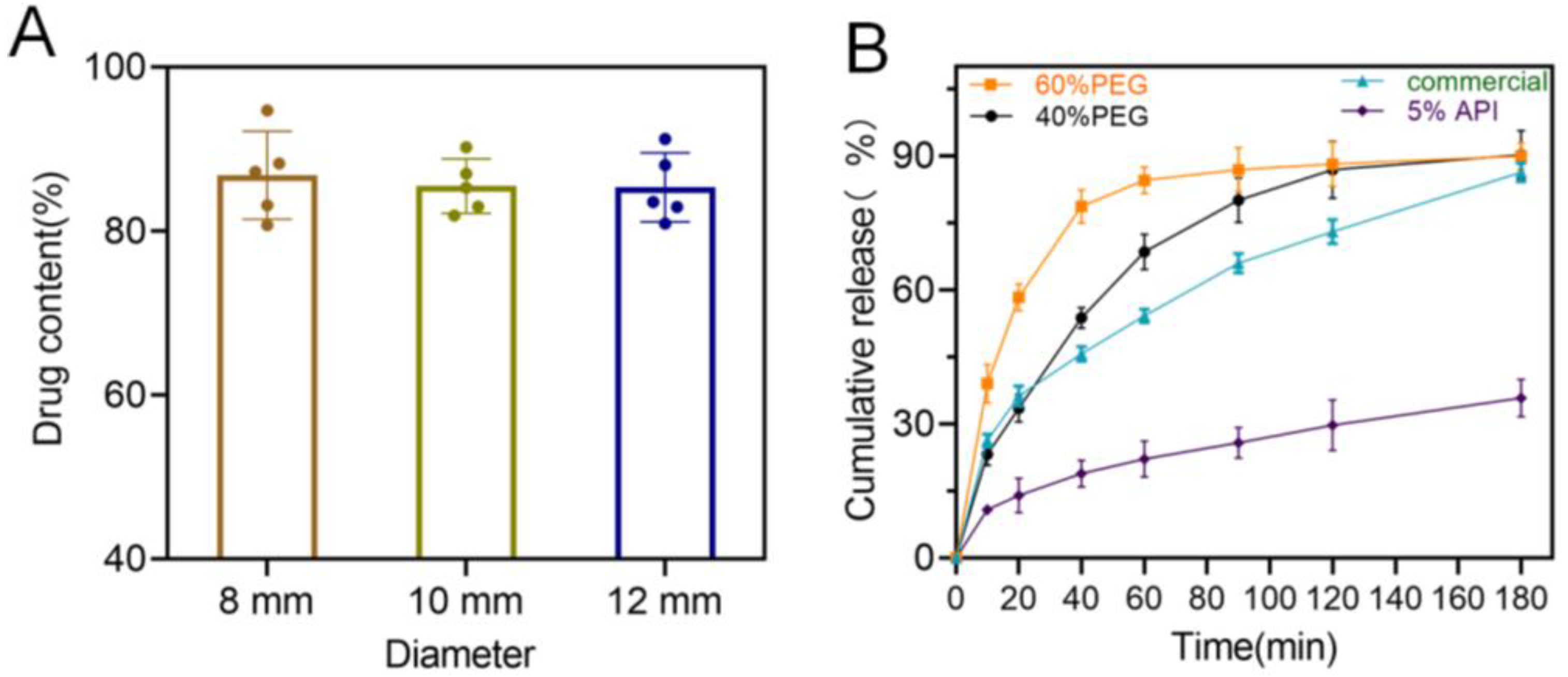
Figure 12.
(A) Drug content of the 3D-printed bilayer oral films (n = 6); (B) in vitro drug cumulative release from the 3D-printed bilayer oral films.
Figure 12.
(A) Drug content of the 3D-printed bilayer oral films (n = 6); (B) in vitro drug cumulative release from the 3D-printed bilayer oral films.
Figure 13.
(A) Ulcer area changes of the model, positive and DEX groups after treatments (n = 4, * p < 0.05, ** p < 0.01, ns: no significant difference); (B) HE staining results of different groups after treatments.
Figure 13.
(A) Ulcer area changes of the model, positive and DEX groups after treatments (n = 4, * p < 0.05, ** p < 0.01, ns: no significant difference); (B) HE staining results of different groups after treatments.
Table 1.
The printing formulations with different ratios of PEG 300 and PEGDA.
Table 1.
The printing formulations with different ratios of PEG 300 and PEGDA.
| PEG 300 (g) | PEGDA (g) | TPO (g) |
|---|
| 0 | 99.00 | 1.00 |
| 10.00 | 89.00 | 1.00 |
| 20.00 | 79.00 | 1.00 |
| 30.00 | 69.00 | 1.00 |
| 40.00 | 59.00 | 1.00 |
| 50.00 | 49.00 | 1.00 |
| 60.00 | 39.00 | 1.00 |
| 70.00 | 29.00 | 1.00 |
| 80.00 | 19.00 | 1.00 |
| 90.00 | 9.00 | 1.00 |
Table 2.
The printing formulations with different ratios of photoinitiator (TPO).
Table 2.
The printing formulations with different ratios of photoinitiator (TPO).
| PEG300 (g) | PEGDA (g) | Tartrazine (g) | TPO (g) |
|---|
| 80.00 | 19.58 | 0.02 | 0.40 |
| 80.00 | 19.38 | 0.02 | 0.60 |
| 80.00 | 19.18 | 0.02 | 0.80 |
| 80.00 | 18.98 | 0.02 | 1.00 |
Table 3.
The printing formulations with different ratios of photoabsorber (tartrazine).
Table 3.
The printing formulations with different ratios of photoabsorber (tartrazine).
| PEG300 (g) | PEGDA (g) | TPO (g) | Tartrazine (g) |
|---|
| 80.00 | 19.00 | 1.00 | 0 |
| 80.00 | 18.99 | 1.00 | 0.01 |
| 80.00 | 18.98 | 1.00 | 0.02 |
| 80.00 | 18.97 | 1.00 | 0.03 |
Table 4.
The printing formulations with different ratios of bioadhesive material.
Table 4.
The printing formulations with different ratios of bioadhesive material.
| HPMC E5/E15/K4M (g) | PEG300 (g) | PEGDA (g) | Tartrazine (g) | TPO (g) |
|---|
| 0 | 79.18 | 20.00 | 0.02 | 0.80 |
| 10.00 | 69.18 | 20.00 | 0.02 | 0.80 |
| 20.00 | 59.18 | 20.00 | 0.02 | 0.80 |
| 30.00 | 49.18 | 20.00 | 0.02 | 0.80 |
Table 5.
The parameters of 3D printing.
Table 5.
The parameters of 3D printing.
| Exposure Time of Each Layer (s) | Layer Height (μm) |
|---|
| 3 | 20 |
| 3 | 30 |
| 3 | 50 |
| 4 | 20 |
| 5 | 20 |
| 6 | 20 |
Table 6.
Printing formulation of the bilayer oral films.
Table 6.
Printing formulation of the bilayer oral films.
| | API | PEGDA | PEG300 | HPMC K4M | TPO | Tartrazine |
|---|
| Adhesion layer containing drug | 2.00 g | 20.00 g | 59.18 g | 20.00 g | 0.80 g | 0.02 g |
| Backing layer | | 69.2 g | 30.00 g | / | 0.80 g | / |
Table 7.
The thickness, diameter, weight of different batches of bilayer films.
Table 7.
The thickness, diameter, weight of different batches of bilayer films.
| Theoretical Diameter (mm) | Thickness (mm, n = 10) | Diameter (mm, n = 10) | Weight (mg, n = 20) |
|---|
| 8 | 0.32 ± 0.01 | 8.25 ± 0.11 | 33.03 ± 1.53 |
| 10 | 0.31 ± 0.02 | 10.20 ± 0.10 | 42.11 ± 1.17 |
| 12 | 0.32 ± 0.02 | 12.27 ± 0.09 | 64.14 ± 1.24 |
Table 8.
Bioadhesive ability of 3D-printed oral films with different diameters (n = 6).
Table 8.
Bioadhesive ability of 3D-printed oral films with different diameters (n = 6).
| Diameter (mm) | Adhesion Force (N) | Adhesion Time (h) |
|---|
| 8 | 1.23 ± 0.51 | 0.53 ± 0.19 |
| 10 | 0.98 ± 0.38 | 0.62 ± 0.23 |
| 12 | 1.27 ± 0.45 | 0.57 ± 0.14 |
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}