The Anti-ROR1 Monoclonal Antibody Zilovertamab Inhibits the Proliferation of Ovarian and Endometrial Cancer Cells

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methodologies
2.1. Cell Culture
2.2. Cell Viability Test
2.3. qRT-PCR and Western Blot Analysis
2.4. Statistical Analysis
3. Results
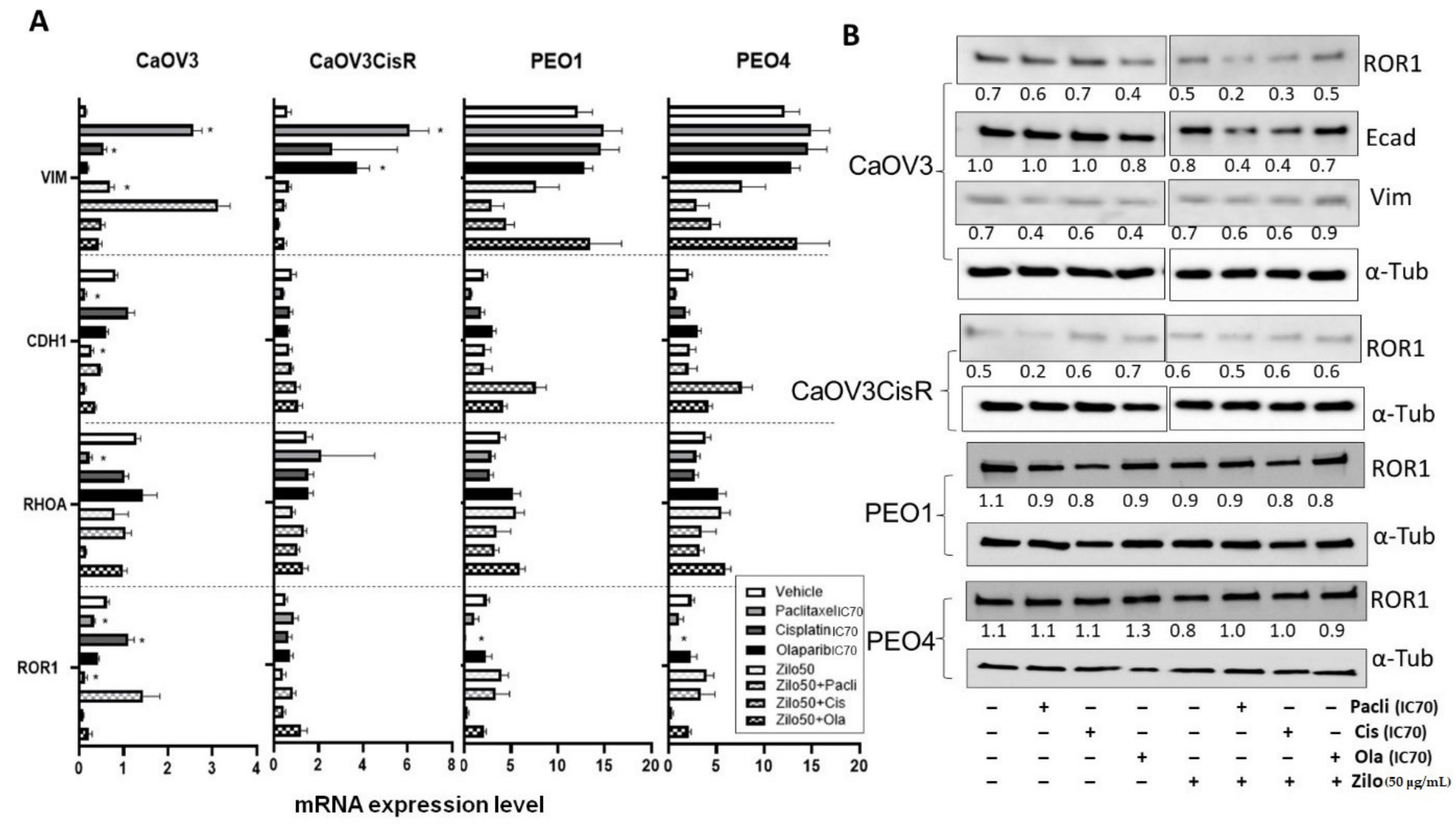
3.1. Single-Agent Zilovertamab Treatment Significantly Inhibits HGSOC Cell Proliferation
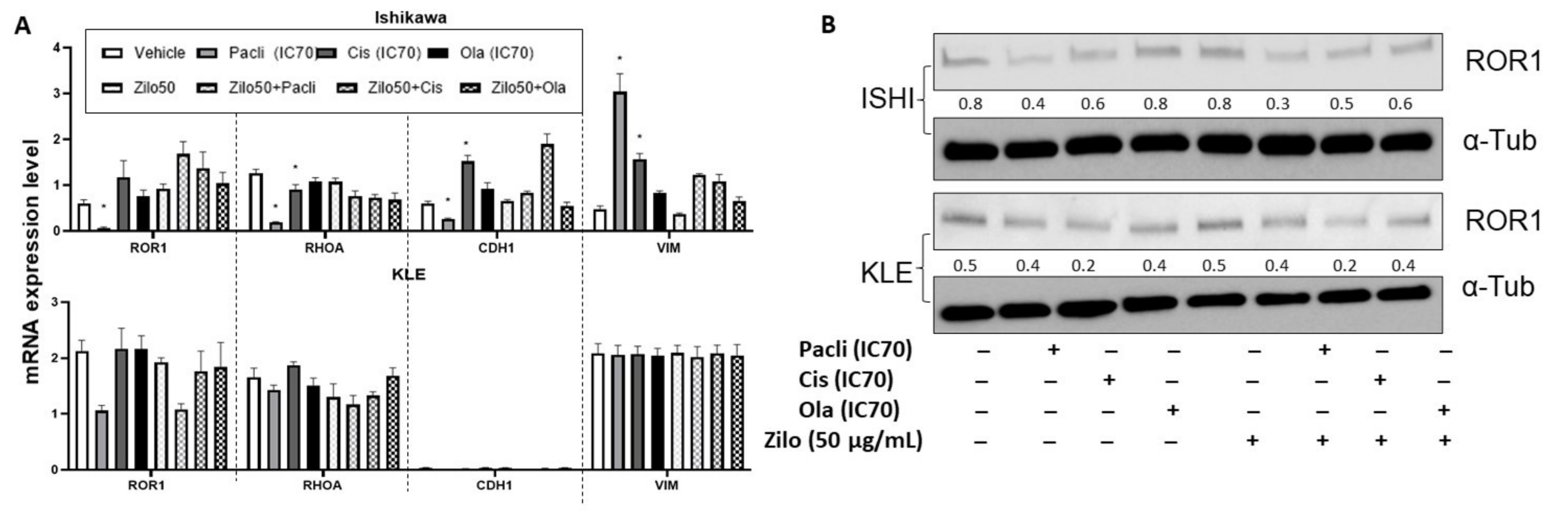
3.2. Single-Agent Zilovertamab Treatment Significantly Inhibited Endometrial Cancer Cell Proliferation
3.3. Synergistic Effect of Combined Zilovertamab and Paclitaxel in Platinum-Resistant HGSOC
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- DaneshManesh, A.H.; Mikaelsson, E.; Jeddi-Tehrani, M.; Bayat, A.A.; Ghods, R.; Ostadkarampour, M.; Akhondi, M.; Lagercrantz, S.; Larsson, C.; Österborg, A.; et al. Ror1, a cell surface receptor tyrosine kinase is expressed in chronic lymphocytic leukemia and may serve as a putative target for therapy. Int. J. Cancer 2008, 123, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chen, L.; Cui, B.; Chuang, H.-Y.; Yu, J.; Wang-Rodriguez, J.; Tang, L.; Chen, G.; Basak, G.W.; Kipps, T.J. ROR1 is expressed in human breast cancer and associated with enhanced tumor-cell growth. PLoS ONE 2012, 7, e31127. [Google Scholar]
- Zhang, S.; Chen, L.; Wang-Rodriguez, J.; Zhang, L.; Cui, B.; Frankel, W.; Wu, R.; Kipps, T.J. The onco-embryonic antigen ROR1 is expressed by a variety of human cancers. Am. J. Pathol. 2012, 181, 1903–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, J.-K.; Zheng, Y.-Z.; Liu, X.-S.; Gou, Q.; Ma, R.; Guo, C.-L.; Croce, C.M.; Liu, L.; Peng, Y. ROR1 expression as a biomarker for predicting prognosis in patients with colorectal cancer. Oncotarget 2017, 8, 32864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henry, C.; Hacker, N.; Ford, C. Silencing ROR1 and ROR2 inhibits invasion and adhesion in an organotypic model of ovarian cancer metastasis. Oncotarget 2017, 8, 112727. [Google Scholar] [CrossRef] [PubMed]
- Henry, C.; Emmanuel, C.; Lambie, N.; Loo, C.; Kan, B.; Kennedy, C.; de Fazio, A.; Hacker, N.; Ford, C. Distinct patterns of stromal and tumor expression of ROR1 and ROR2 in histological subtypes of epithelial ovarian cancer. Transl. Oncol. 2017, 10, 346–356. [Google Scholar] [CrossRef]
- Liu, D.; Gunther, K.; Enriquez, L.A.; Daniels, B.; O’Mara, T.A.; Tang, K.; Spurdle, A.B.; Ford, C.E. ROR1 is upregulated in endometrial cancer and represents a novel therapeutic target. Sci. Rep. 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Henry, C.; Llamosas, E.; Daniels, B.; Coopes, A.; Tang, K.; Ford, C. ROR1 and ROR2 play distinct and opposing roles in endometrial cancer. Gynecol. Oncol. 2018, 148, 576–584. [Google Scholar] [CrossRef]
- Henry, C.; Llamosas, E.; Djordjevic, A.; Hacker, N.; Ford, C. Migration and invasion is inhibited by silencing ROR1 and ROR2 in chemoresistant ovarian cancer. Oncogenesis 2016, 5, e226. [Google Scholar] [CrossRef]
- Choi, M.Y.; Widhopf, G.F., II; Wu, C.C.; Cui, B.; Lao, F.; Sadarangani, A.; Cavagnaro, J.; Prussak, C.; Carson, D.A.; Jamieson, C. Pre-clinical specificity and safety of UC-961, a first-in-class monoclonal antibody targeting ROR1. Clin. Lymphoma Myeloma Leuk. 2015, 15, S167–S169. [Google Scholar] [CrossRef] [Green Version]
- Choi, M.Y.; Wierda, W.G.; Lee, H.J.; Tzachanis, D.; Ianopulos, X.; Jezior, D.; Breitmeyer, J.B.; Jamieson, C.H.; Kipps, T.J.; Group, C.S. Phase 1/2 trial of cirmtuzumab and ibrutinib: Planned analysis of phase 1 CLL cohorts. Am. Soc. Clin. Oncol. 2019, 37, 7527. [Google Scholar] [CrossRef]
- Choi, M.Y.; Widhopf, G.F., II; Ghia, E.M.; Kidwell, R.L.; Hasan, M.K.; Yu, J.; Rassenti, L.Z.; Chen, L.; Chen, Y.; Pittman, E. Phase I trial: Cirmtuzumab inhibits ROR1 signaling and stemness signatures in patients with chronic lymphocytic leukemia. Cell Stem Cell 2018, 22, 951–959.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Choi, M.Y.; Siddiqi, T.; Wierda, W.G.; Barrientos, J.C.; Lamanna, N.; Goldenberg, A.; Isufi, I.; Tuscano, J.; Subbiah, S. Cirmtuzumab, an anti-ROR1 antibody, in combination with ibrutinib: Clinical activity in mantle cell lymphoma (MCL) or chronic lymphocytic leukemia (CLL) from a phase 1/2 study. Blood 2020, 136, 45–46. [Google Scholar] [CrossRef]
- Joshi, N.; Liu, D.; Dickson, K.-A.; Marsh, D.J.; Ford, C.E.; Stenzel, M.H. An organotypic model of high-grade serous ovarian cancer to test the anti-metastatic potential of ROR2 targeted Polyion complex nanoparticles. J. Mater. Chem. B 2021, 9, 9123–9135. [Google Scholar] [CrossRef]
- Jonsson, E.; Fridborg, H.; Nygren, P.; Larsson, R. Synergistic interactions of combinations of topotecan with standard drugs in primary cultures of human tumor cells from patients. Eur. J. Clin. Pharmacol. 1998, 54, 509–514. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Cole, A.J.; Dickson, K.-A.; Liddle, C.; Stirzaker, C.; Shah, J.S.; Clifton-Bligh, R.; Marsh, D.J. Ubiquitin chromatin remodelling after DNA damage is associated with the expression of key cancer genes and pathways. Cell. Mol. Life Sci. 2021, 78, 1011–1027. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, H.; Ghia, E.M.; Huang, J.; Wu, L.; Zhang, J.; Lam, S.; Lei, Y.; He, J.; Cui, B. Inhibition of chemotherapy resistant breast cancer stem cells by a ROR1 specific antibody. Proc. Natl. Acad. Sci. USA 2019, 116, 1370–1377. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Chen, L.; Cui, B.; Wu, C.; Choi, M.Y.; Chen, Y.; Zhang, L.; Rassenti, L.Z.; Widhopf Ii, G.; Kipps, T.J. Cirmtuzumab inhibits Wnt5a-induced Rac1 activation in chronic lymphocytic leukemia treated with ibrutinib. Leukemia 2017, 31, 1333–1339. [Google Scholar] [CrossRef]
- Cui, B.; Zhang, S.; Chen, L.; Yu, J.; Widhopf, G.F.; Fecteau, J.-F.; Rassenti, L.Z.; Kipps, T.J. Targeting ROR1 inhibits epithelial–mesenchymal transition and metastasis. Cancer Res. 2013, 73, 3649–3660. [Google Scholar] [CrossRef] [Green Version]
- Thiery, J.P.; Acloque, H.; Huang, R.Y.; Nieto, M.A. Epithelial-mesenchymal transitions in development and disease. Cell 2009, 139, 871–890. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Weinberg, R.A. Epithelial-mesenchymal transition: At the crossroads of development and tumor metastasis. Dev. Cell 2008, 14, 818–829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, I.H.; Kim, K.-R.; Lim, S.; Kim, S.-H.; Sung, C.O. Expression and prognostic significance of epithelial-mesenchymal transition-related markers and phenotype in serous ovarian cancer. Pathol. Res. Pract. 2018, 214, 1564–1571. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Wang, X.; Li, B. Expression profile of epithelial-mesenchymal transition-related genes as a prognostic biomarker for endometrial cancer. J. Cancer 2021, 12, 6484. [Google Scholar] [CrossRef] [PubMed]
- Liu, G. Receptor Tyrosine Kinase-Like Orphan Receptor-1 (ROR1) Expression in Breast Cancer Stem Cells Can Be Targeted for Anti-Cancer-Stem-Cell Therapy; University of California: San Diego, CA, USA, 2015. [Google Scholar]
- Zhang, S.; Cui, B.; Lai, H.; Liu, G.; Ghia, E.M.; Widhopf, G.F.; Zhang, Z.; Wu, C.C.; Chen, L.; Wu, R. Ovarian cancer stem cells express ROR1, which can be targeted for anti–cancer-stem-cell therapy. Proc. Natl. Acad. Sci. USA 2014, 111, 17266–17271. [Google Scholar] [CrossRef] [Green Version]
- Bitler, B.G.; Watson, Z.L.; Wheeler, L.J.; Behbakht, K. PARP inhibitors: Clinical utility and possibilities of overcoming resistance. Gynecol. Oncol. 2017, 147, 695–704. [Google Scholar] [CrossRef] [Green Version]
- Farmer, H.; McCabe, N.; Lord, C.J.; Tutt, A.N.; Johnson, D.A.; Richardson, T.B.; Santarosa, M.; Dillon, K.J.; Hickson, I.; Knights, C. Targeting the DNA repair defect in BRCA mutant cells as a therapeutic strategy. Nature 2005, 434, 917–921. [Google Scholar] [CrossRef]
- McCabe, N.; Turner, N.C.; Lord, C.J.; Kluzek, K.; Białkowska, A.; Swift, S.; Giavara, S.; O’Connor, M.J.; Tutt, A.N.; Zdzienicka, M.Z. Deficiency in the repair of DNA damage by homologous recombination and sensitivity to poly (ADP-ribose) polymerase inhibition. Cancer Res. 2006, 66, 8109–8115. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CaOV3 | CaOV3CisR | PEO1 | PEO4 | Ishikawa | KLE | |
|---|---|---|---|---|---|---|
| Paclitaxel (nM) | 0.788 | 0.649 | 3.620 | 3.038 | 6.852 | 12.680 |
| Cisplatin (µM) | 1.305 | 4.038 | 0.496 | 10.400 | 1.937 | 1.517 |
| Olaparib (µM) | 6.980 | 3.353 | 0.395 | 0.406 | 1.535 | 10.730 |
| Zilovertamab (25 µg/mL) | Zilovertamab (50 µg/mL) | |||||
|---|---|---|---|---|---|---|
| +Cisplatin | +Paclitaxel | +Olaparib | +Cisplatin | +Paclitaxel | +Olaparib | |
| CaOV3 | 1.37 (1.18, 1.56) | 1.47 (1.04, 1.90) | 1.27 (1.10, 1.44) | 1.51 (1.33, 1.69) | 1.37 (0.92, 1.82) | 1.41 (1.18, 1.64) |
| CaOV3CisR | 1.10 (0.74, 1.46) | 1.30 (0.74, 1.86) | 1.01 (0.80, 1.22) | 1.54 (0.00, 4.62) | 1.36 (0.87, 1.85) | 1.42 (0.08, 2.76) |
| PEO1 | 1.56 (0.95, 2.17) | 1.57 (1.00, 2.14) | 1.55 (0.81, 2.29) | 1.74 (1.14, 2.34) | 1.28 (0.84, 1.72) | 1.40 (0.91, 1.88) |
| PEO4 | 1.72 (0.48, 1.96) | 1.35 (0.90, 1.8) | 1.56 (0.82, 2.30) | 1.44 (0.47, 2.41) | 1.28 (0.69, 1.87) | 1.57 (0.26, 2.88) |
| Ishikawa | 1.54 (0.96, 2.12) | 1.63 (0.72, 2.54) | 3.77 (0.45, 7.09) | 2.02 (1.42, 2.62) | 1.84 (0.77, 2.9) | 3.73 (1.08, 6.38) |
| KLE | 1.03 (0.81, 1.25) | 0.99 (0.73, 1.25) | 1.04 (0.64, 1.44) | 1.40 (0.83, 1.97) | 1.15 (0.57, 1.73) | 1.29 (0.58, 2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, D.; Kaufmann, G.F.; Breitmeyer, J.B.; Dickson, K.-A.; Marsh, D.J.; Ford, C.E. The Anti-ROR1 Monoclonal Antibody Zilovertamab Inhibits the Proliferation of Ovarian and Endometrial Cancer Cells. Pharmaceutics 2022, 14, 837. https://doi.org/10.3390/pharmaceutics14040837
Liu D, Kaufmann GF, Breitmeyer JB, Dickson K-A, Marsh DJ, Ford CE. The Anti-ROR1 Monoclonal Antibody Zilovertamab Inhibits the Proliferation of Ovarian and Endometrial Cancer Cells. Pharmaceutics. 2022; 14(4):837. https://doi.org/10.3390/pharmaceutics14040837
Chicago/Turabian StyleLiu, Dongli, Gunnar F. Kaufmann, James B. Breitmeyer, Kristie-Ann Dickson, Deborah J. Marsh, and Caroline E. Ford. 2022. "The Anti-ROR1 Monoclonal Antibody Zilovertamab Inhibits the Proliferation of Ovarian and Endometrial Cancer Cells" Pharmaceutics 14, no. 4: 837. https://doi.org/10.3390/pharmaceutics14040837
APA StyleLiu, D., Kaufmann, G. F., Breitmeyer, J. B., Dickson, K.-A., Marsh, D. J., & Ford, C. E. (2022). The Anti-ROR1 Monoclonal Antibody Zilovertamab Inhibits the Proliferation of Ovarian and Endometrial Cancer Cells. Pharmaceutics, 14(4), 837. https://doi.org/10.3390/pharmaceutics14040837