
Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers


 ,
,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methodology
2.2.1. Formulation Design
2.2.2. Compression Technique
2.3. Solid-State Characterization
2.3.1. Fourier Transform Infrared Analysis (FTIR)
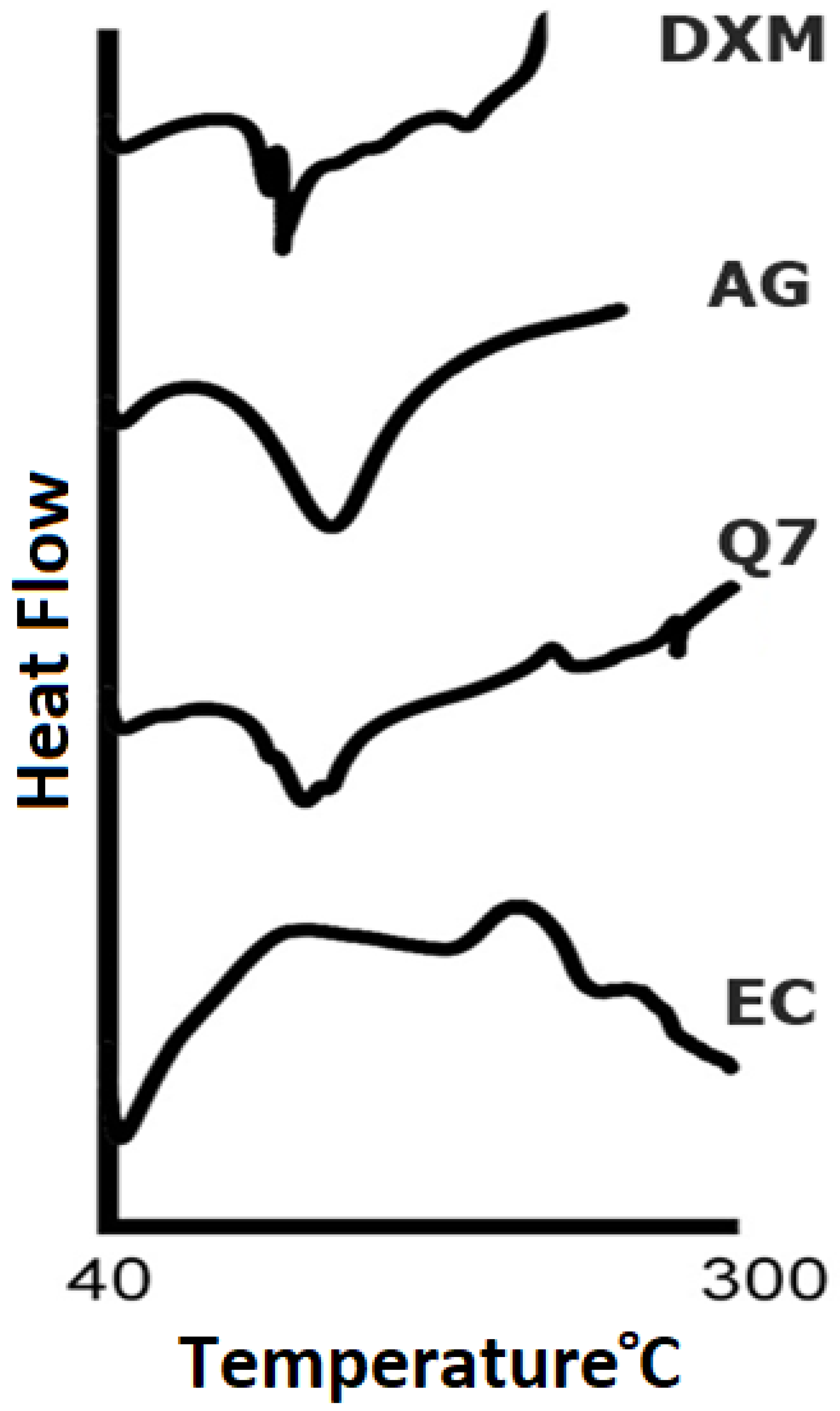
2.3.2. Differential Scanning Calorimetry (DSC)
2.4. Physicochemical Characterization
2.4.1. Weight Variation
2.4.2. Thickness and Diameter
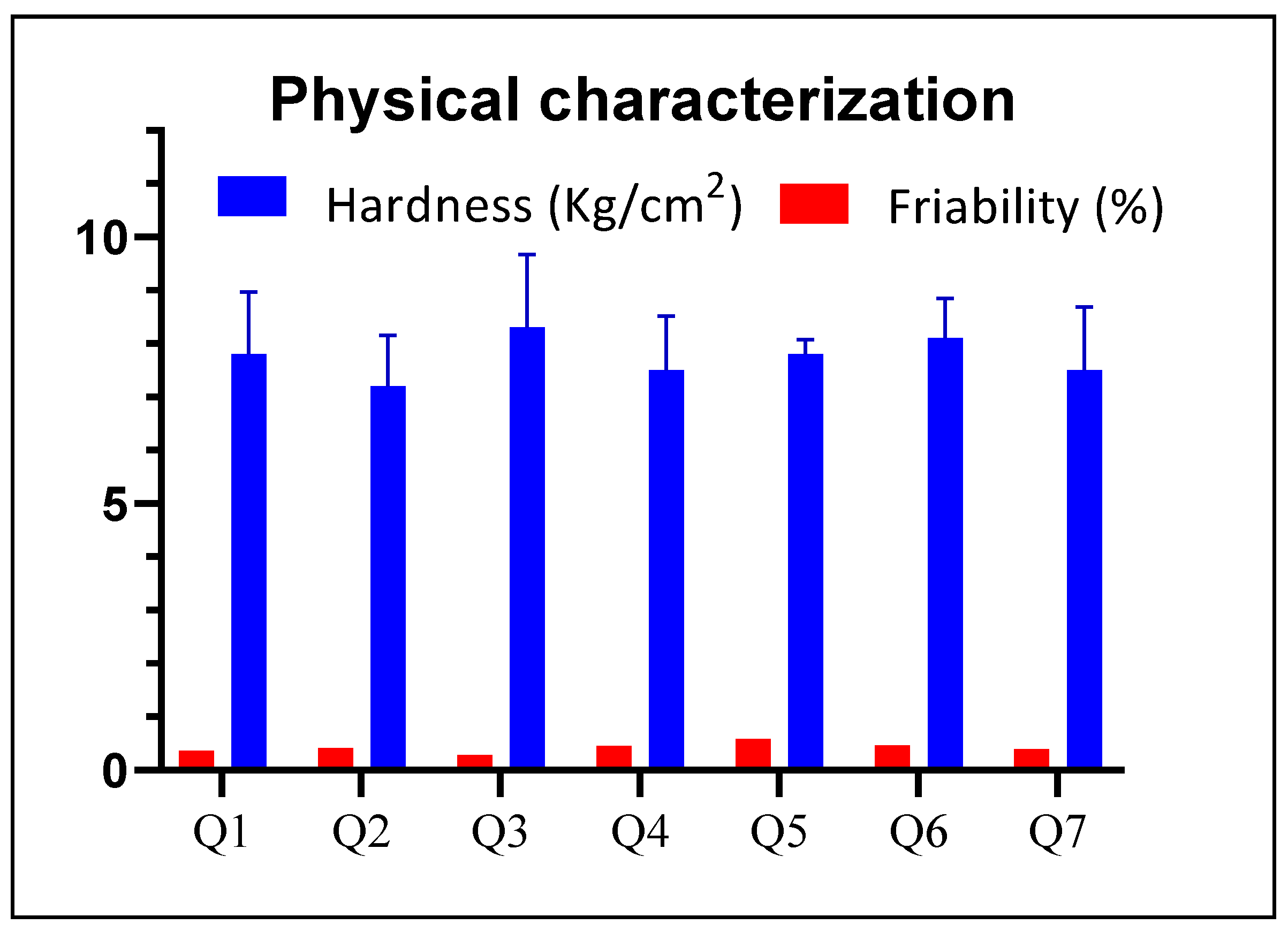
2.4.3. Hardness
2.4.4. Friability
2.4.5. Surface pH
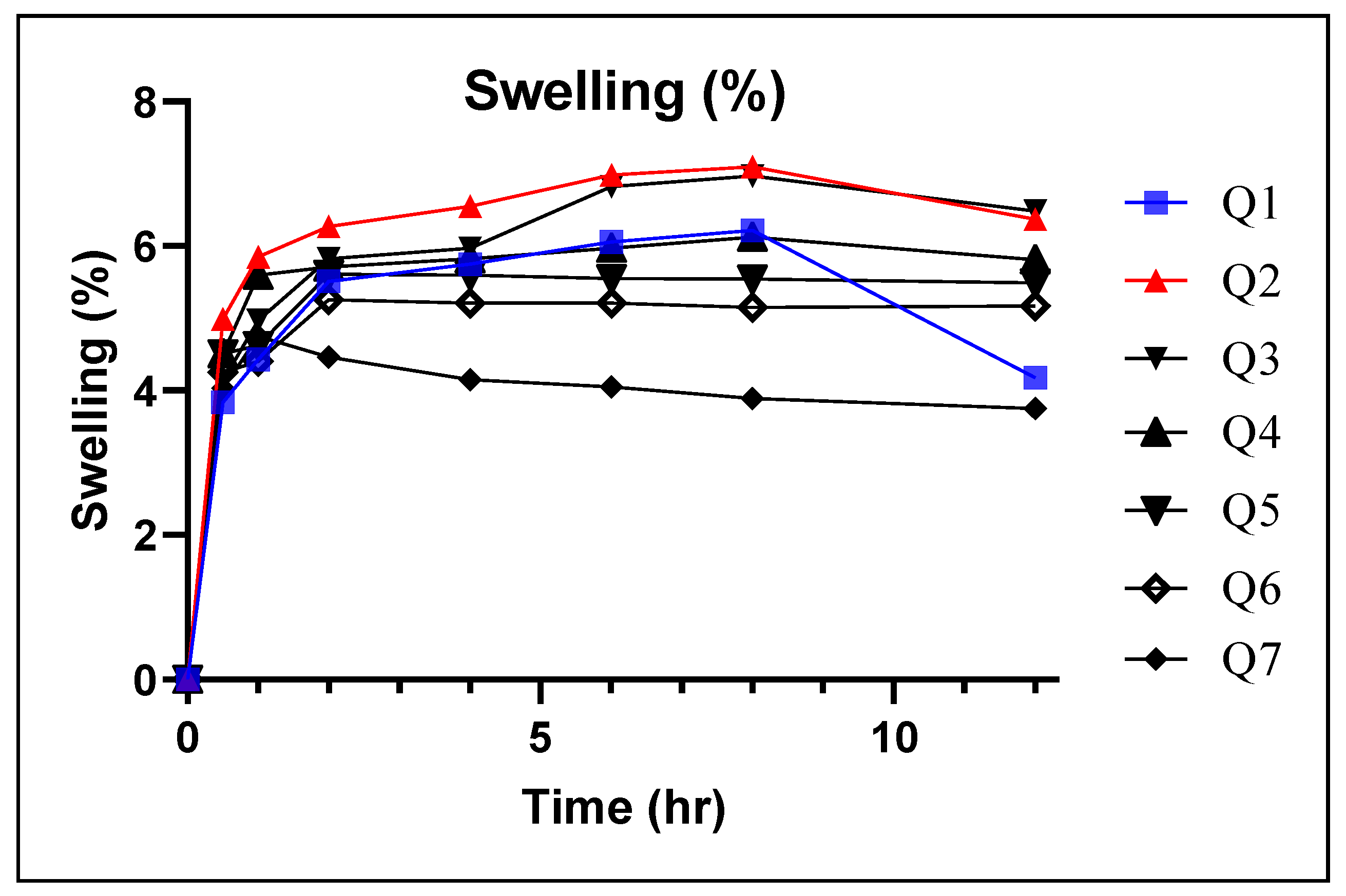
2.4.6. Swelling Index (SI)
2.4.7. Matrix Erosion (ME)
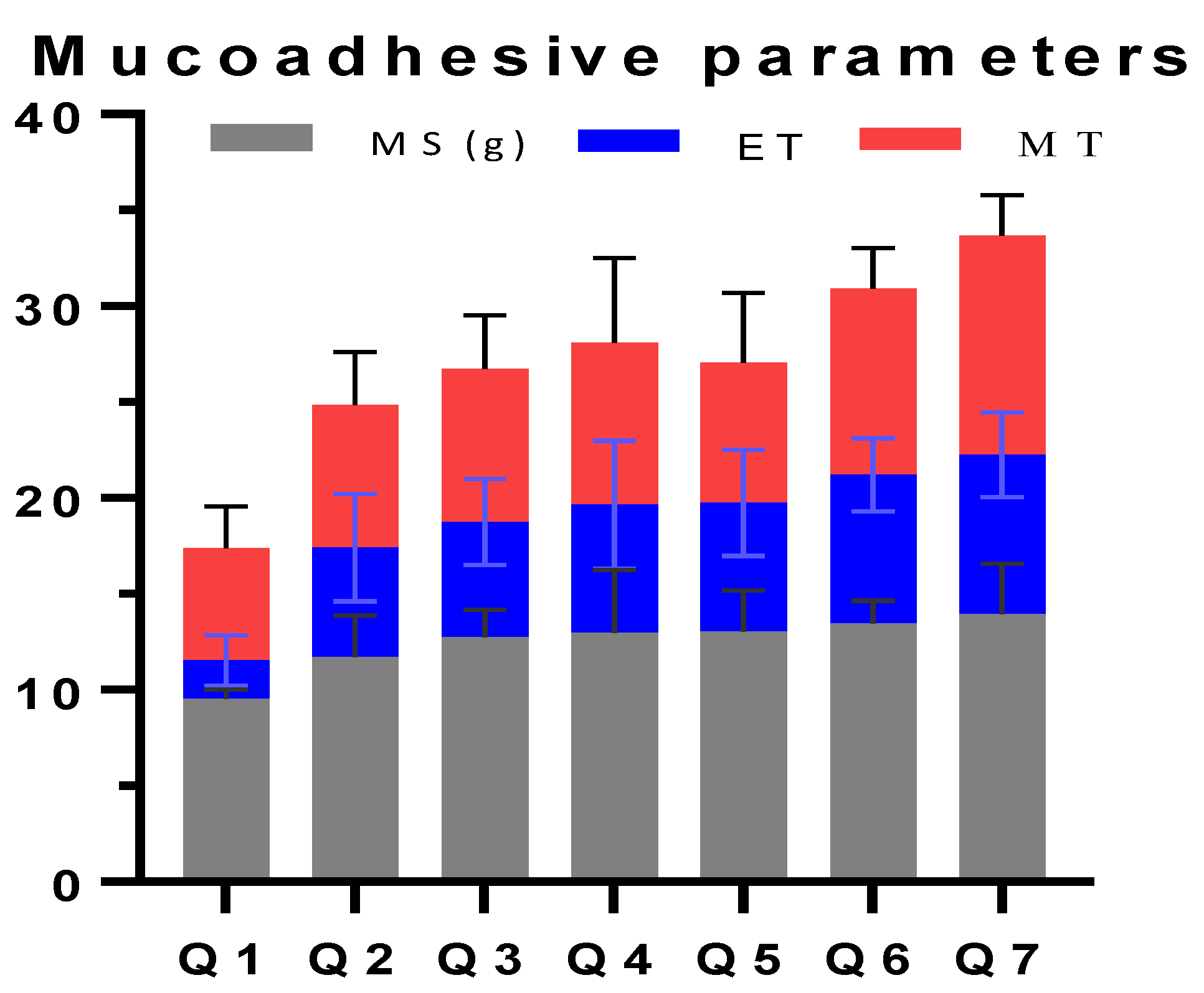
2.4.8. Ex Vivo Mucoadhesive Time (ET)
2.4.9. Ex Vivo Mucoadhesion Strength (MS)
Development of MS Apparatus
Evaluation of MS
2.4.10. Mucoadhesive Study in Volunteers (MT)
2.5. In Vitro Drug Release Study
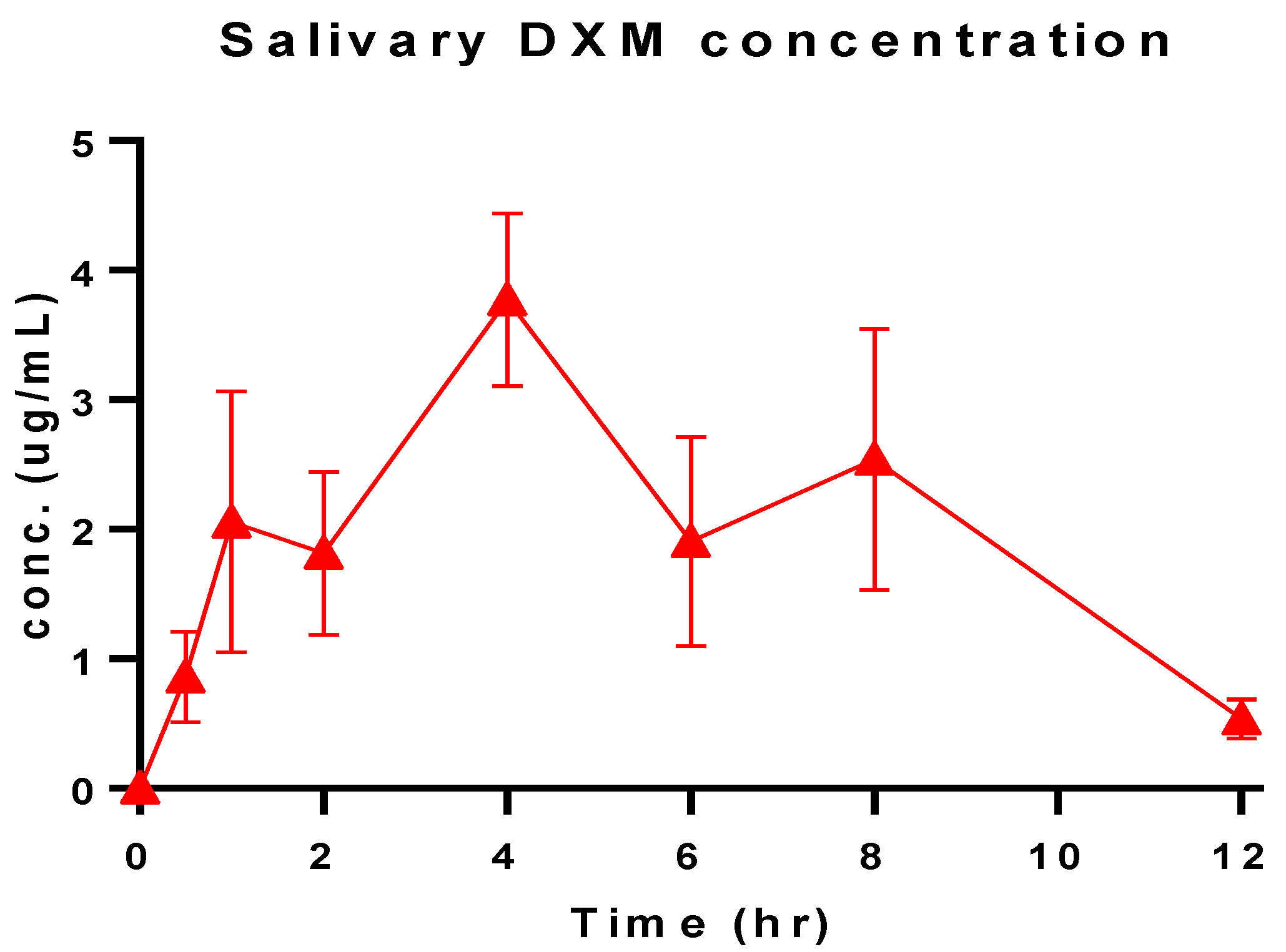
2.6. Salivary DXM Release in Volunteers
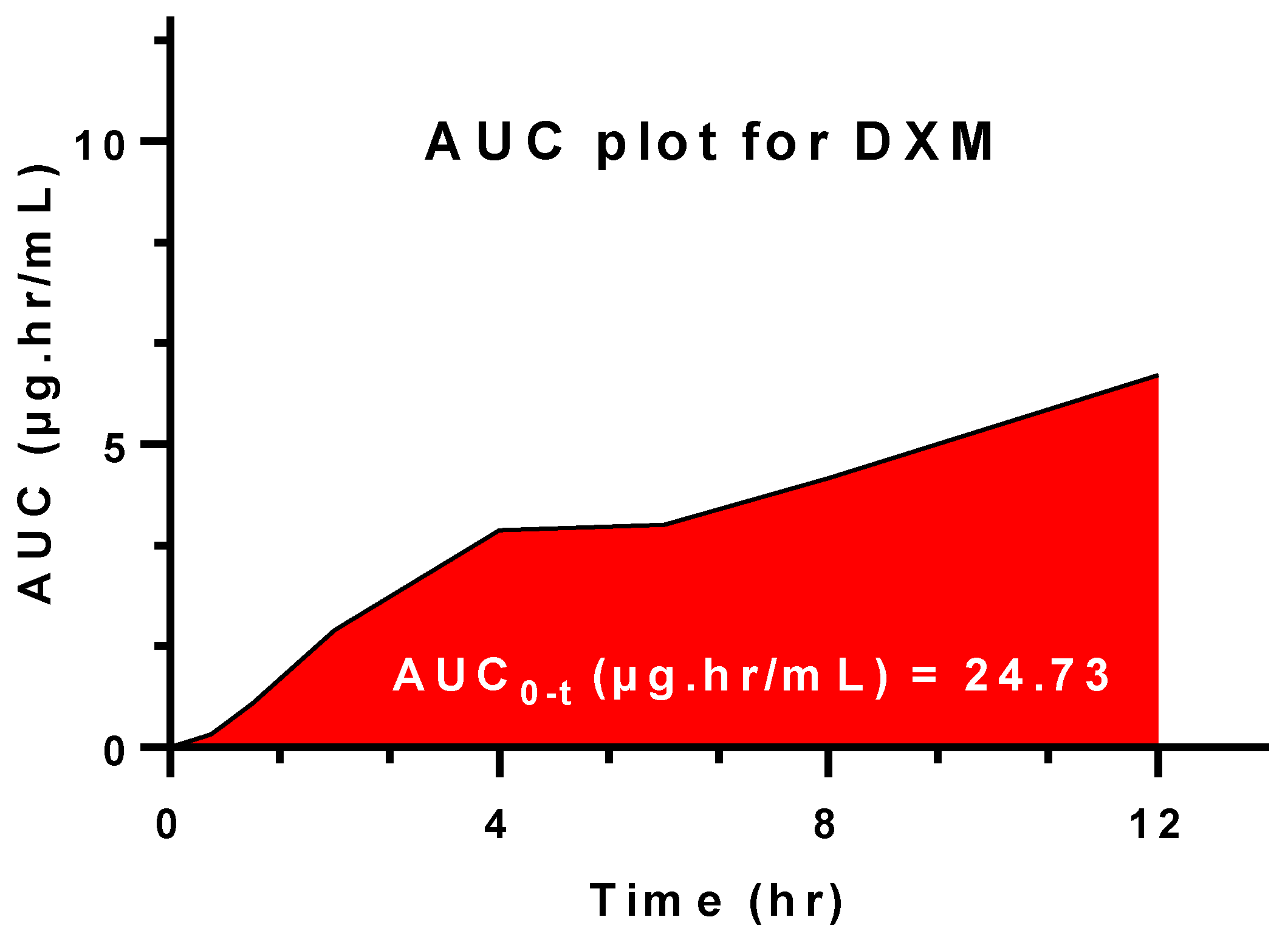
2.7. Salivary Pharmacokinetic Estimation
2.8. In Vitro Salivary Release Kinetics
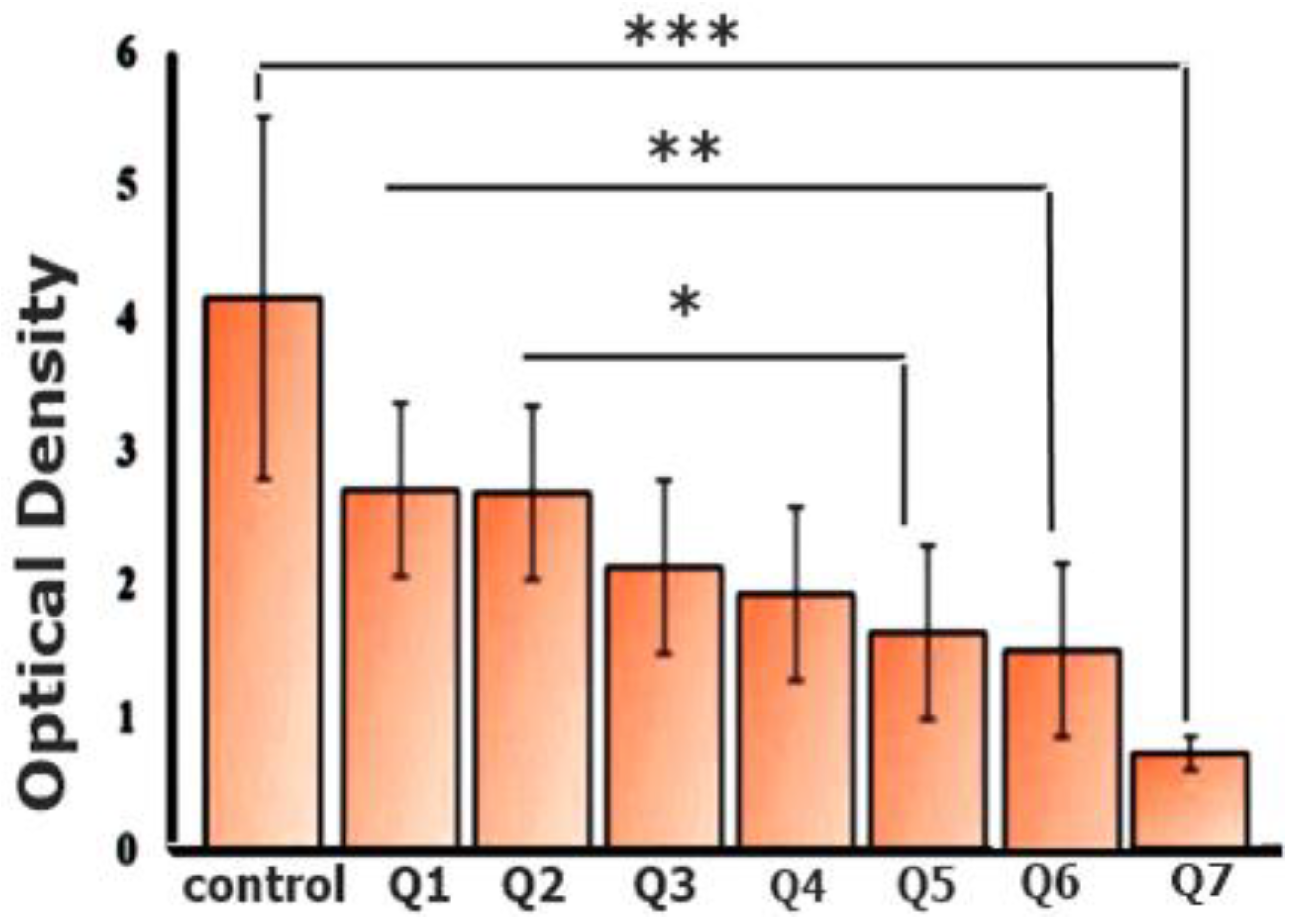
2.9. Coagulation Analysis via Optical Density
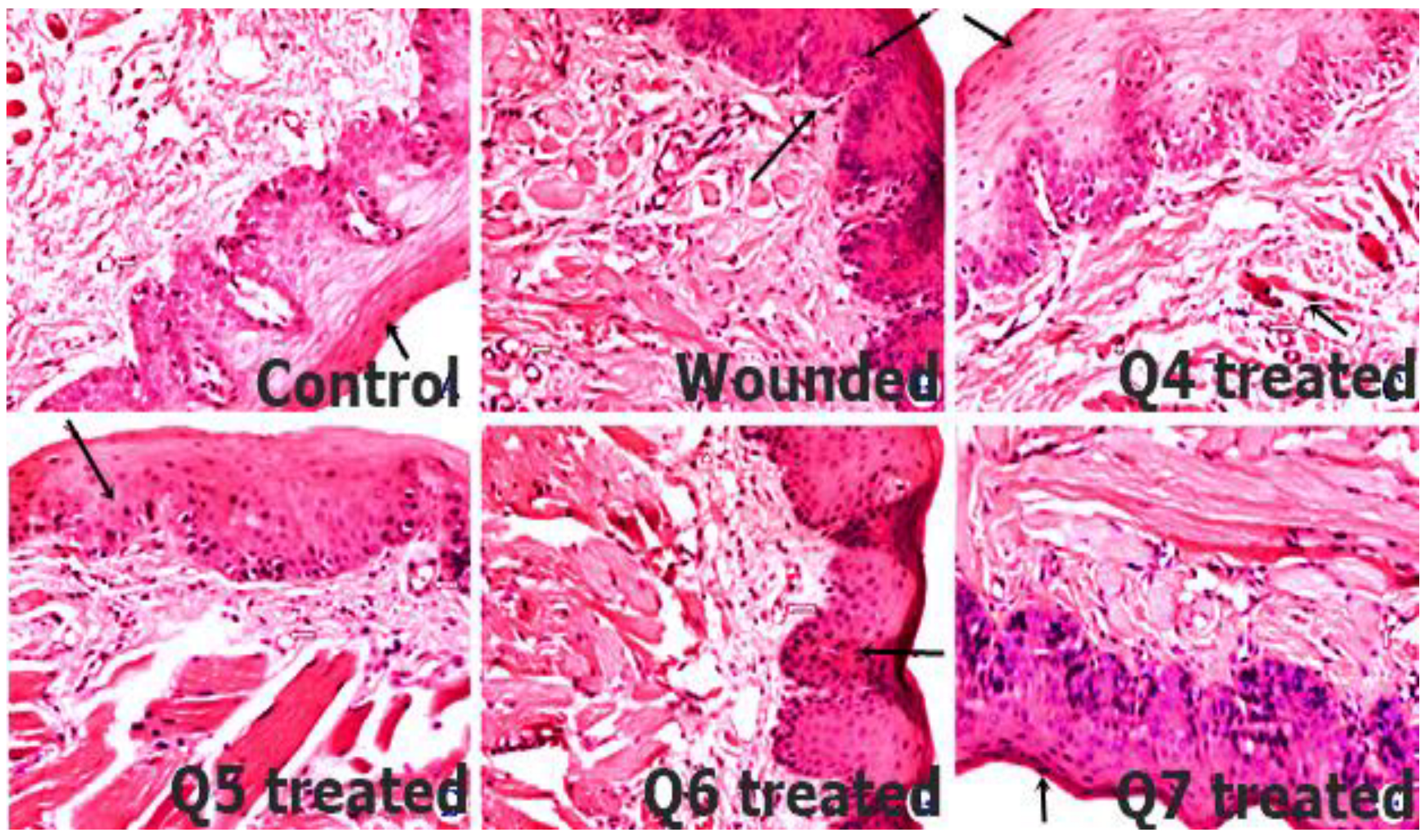
2.10. In Vivo Histopathological Analysis
2.11. Stability Study
2.12. Statistical Analysis
3. Results and Discussion
3.1. Solid-State Characterization
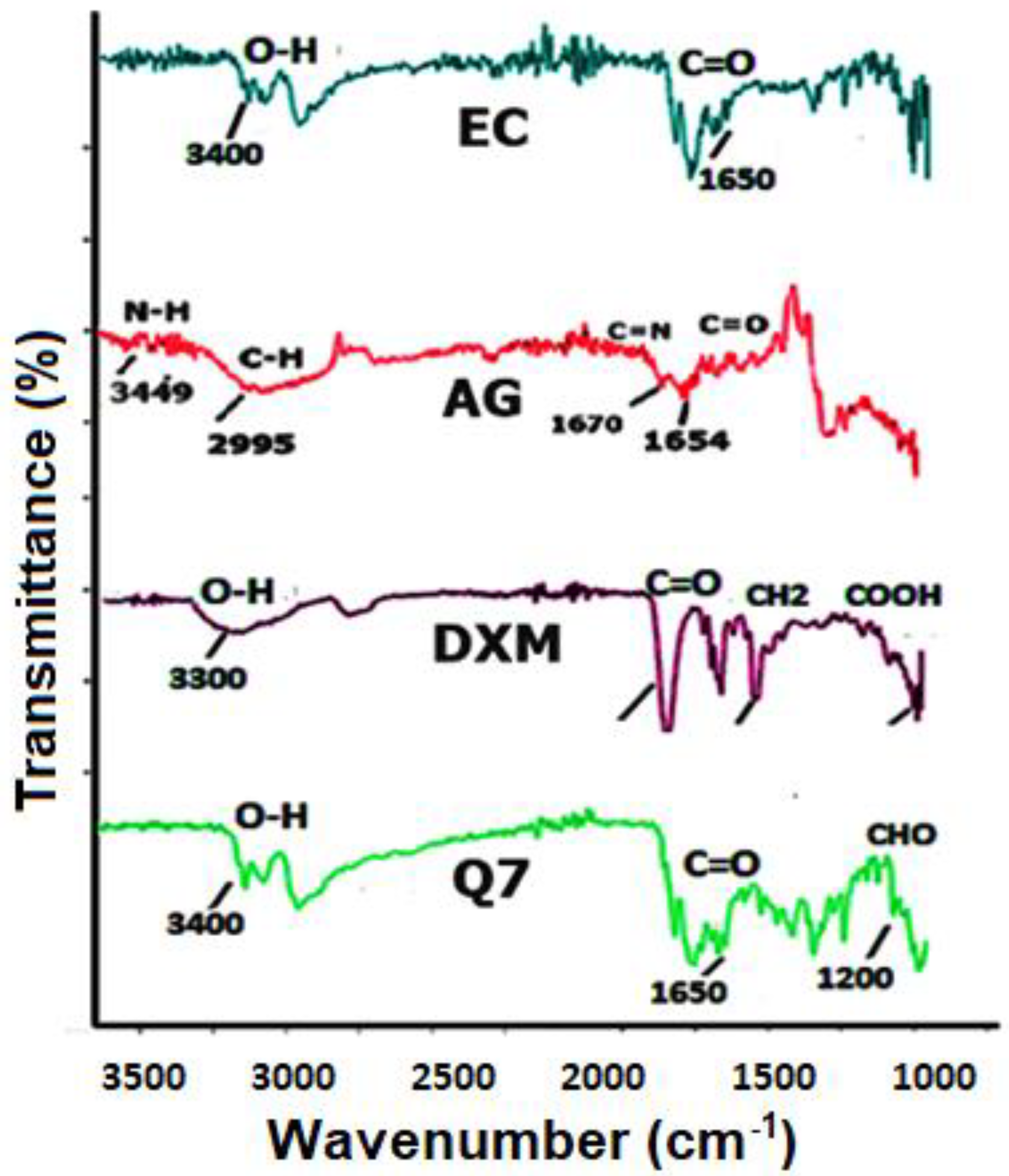
3.1.1. FTIR
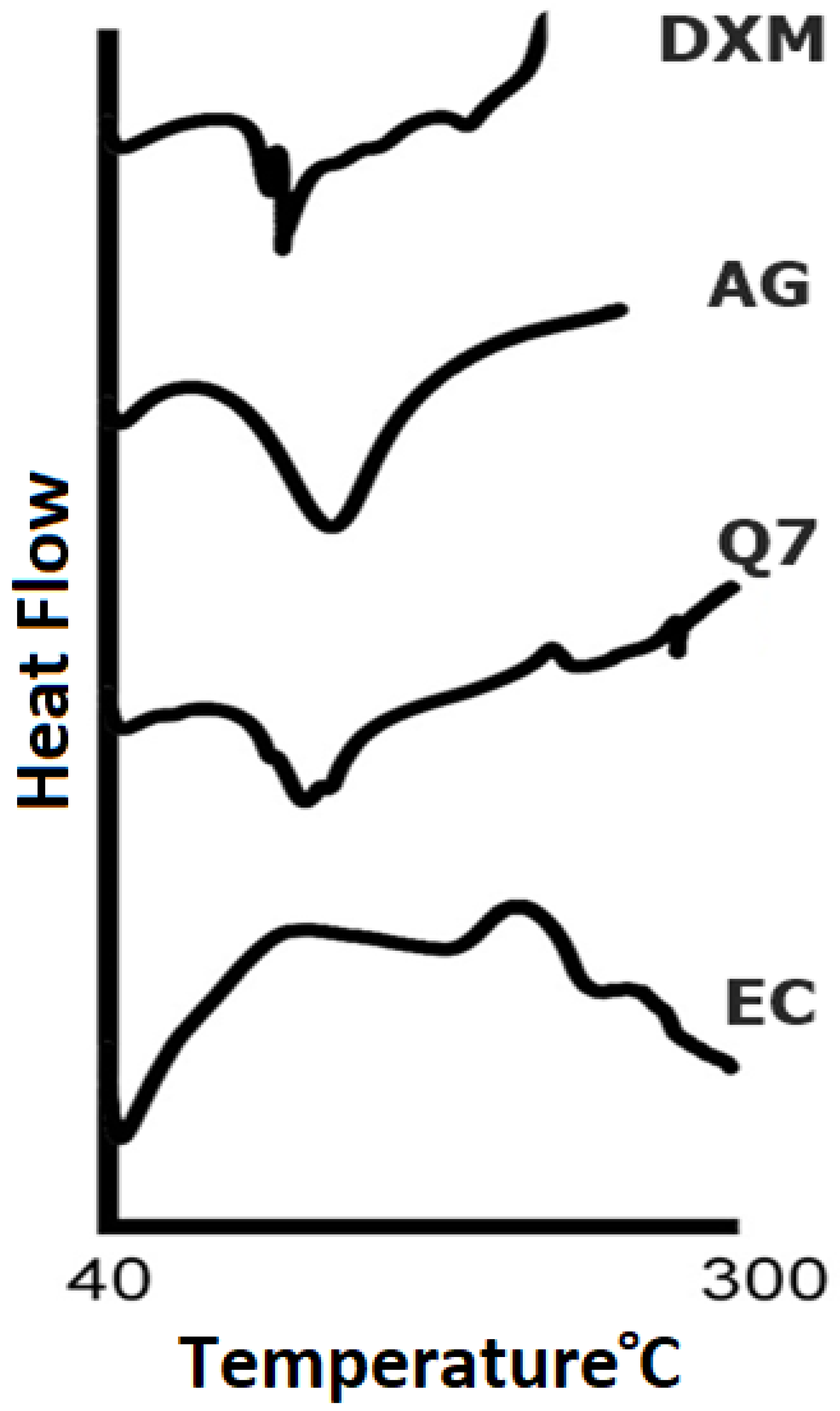
3.1.2. DSC
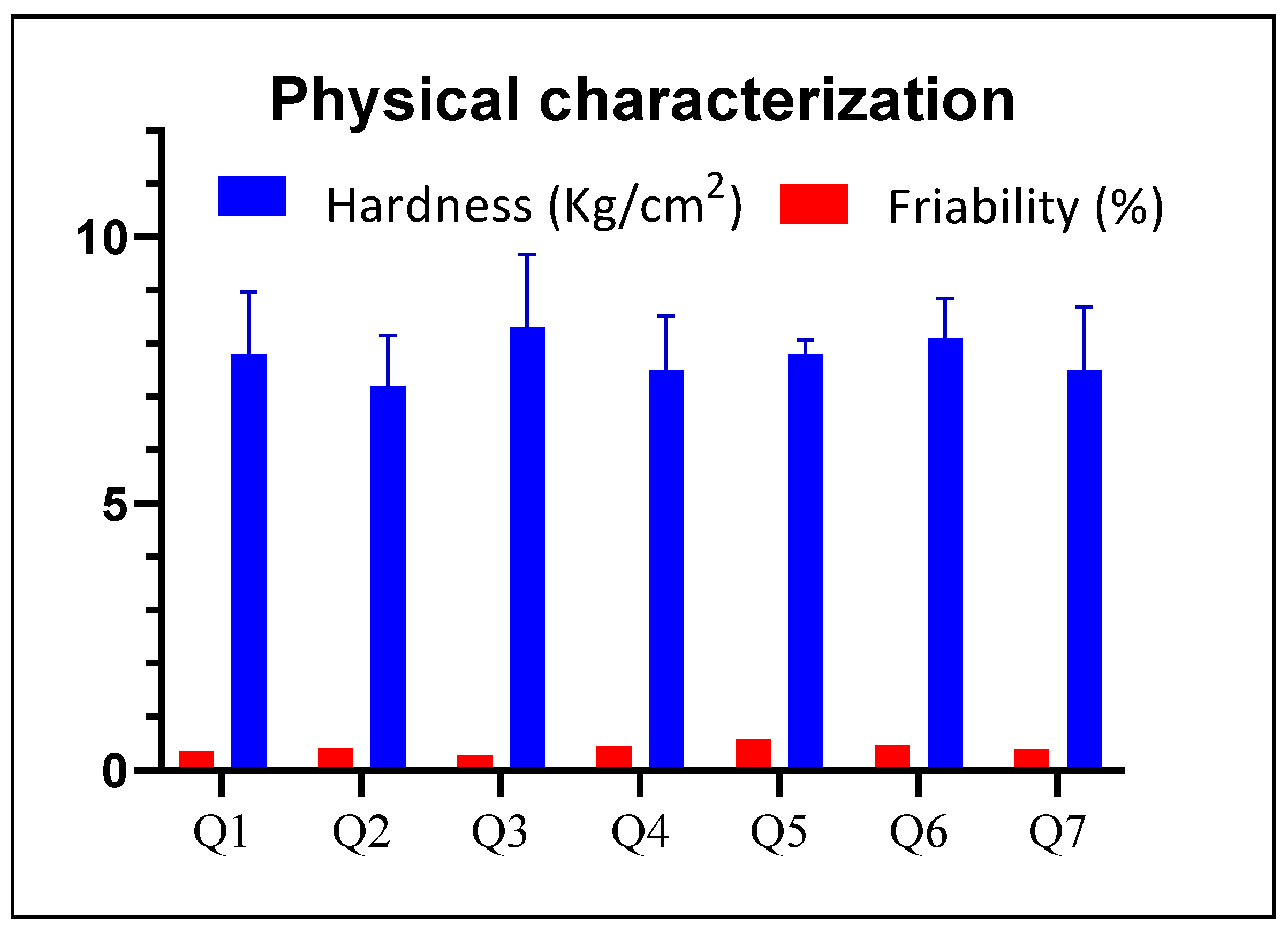
3.2. Physical Characterization
3.3. Surface pH
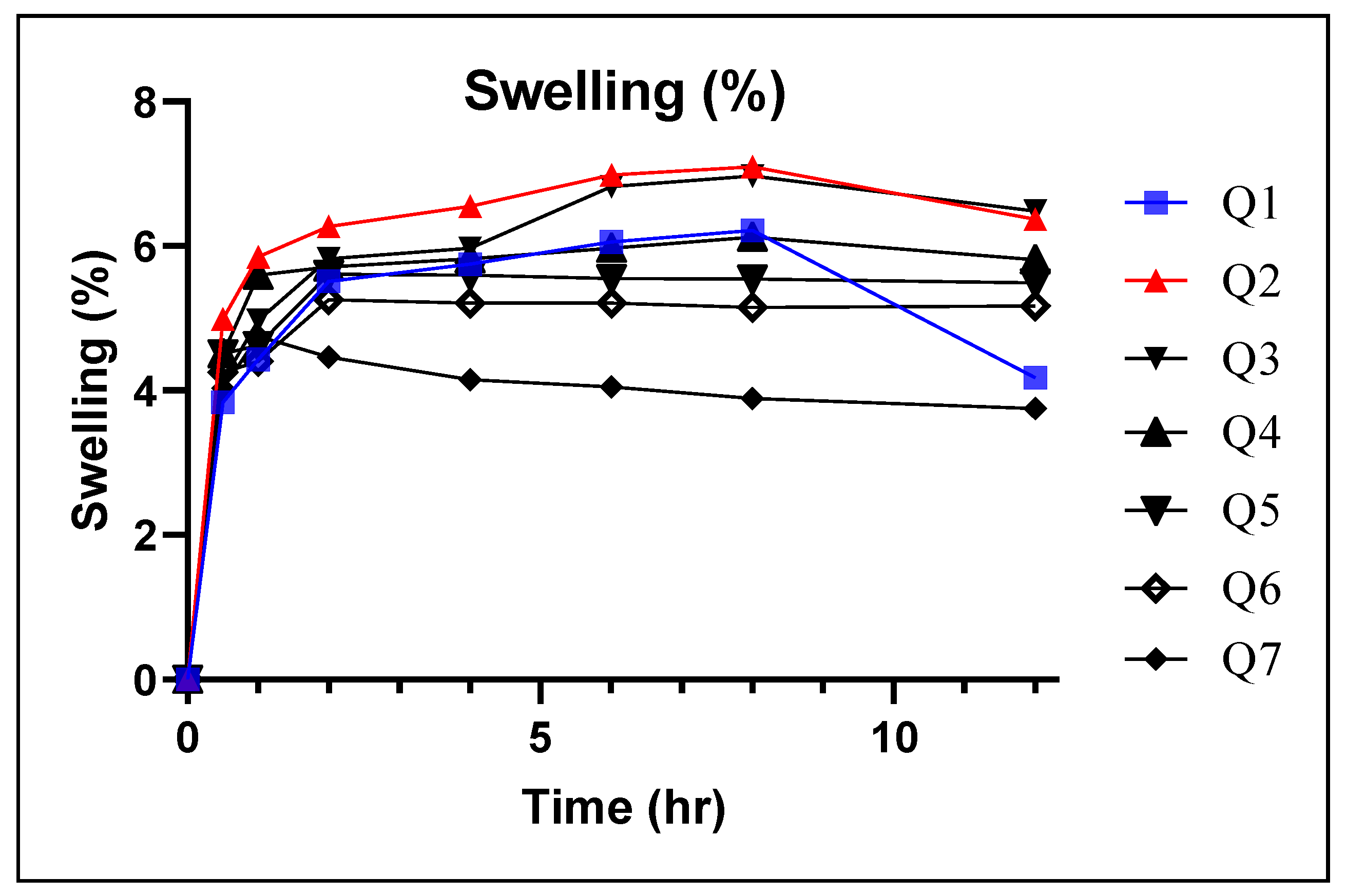
3.4. Swelling Index
3.5. Matrix Erosion (ME)
3.6. Ex Vivo Mucoadhesive Time (ET)
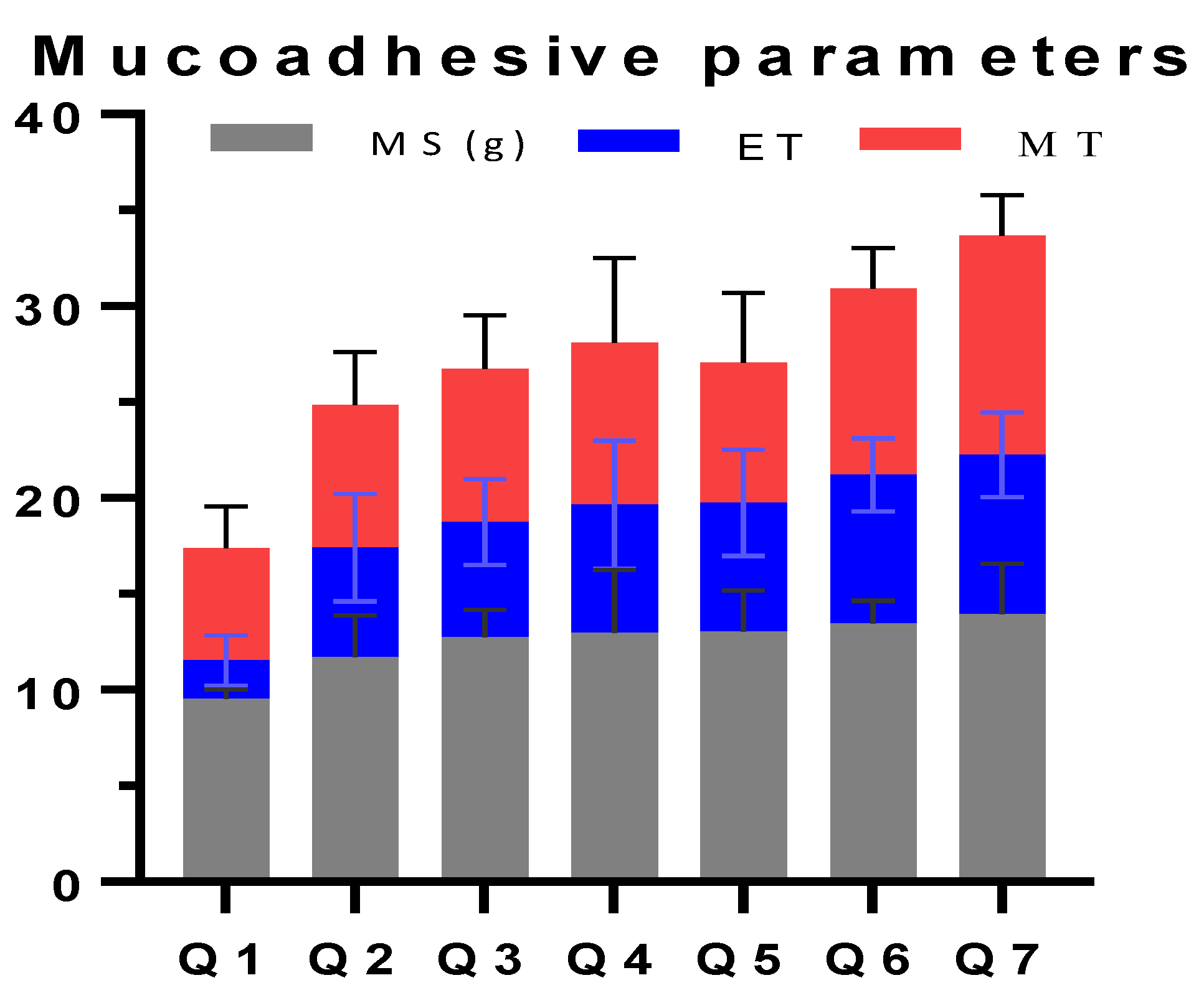
3.7. Ex Vivo Mucoadhesion Strength
3.8. Mucoadhesive Time in Volunteers (MT)
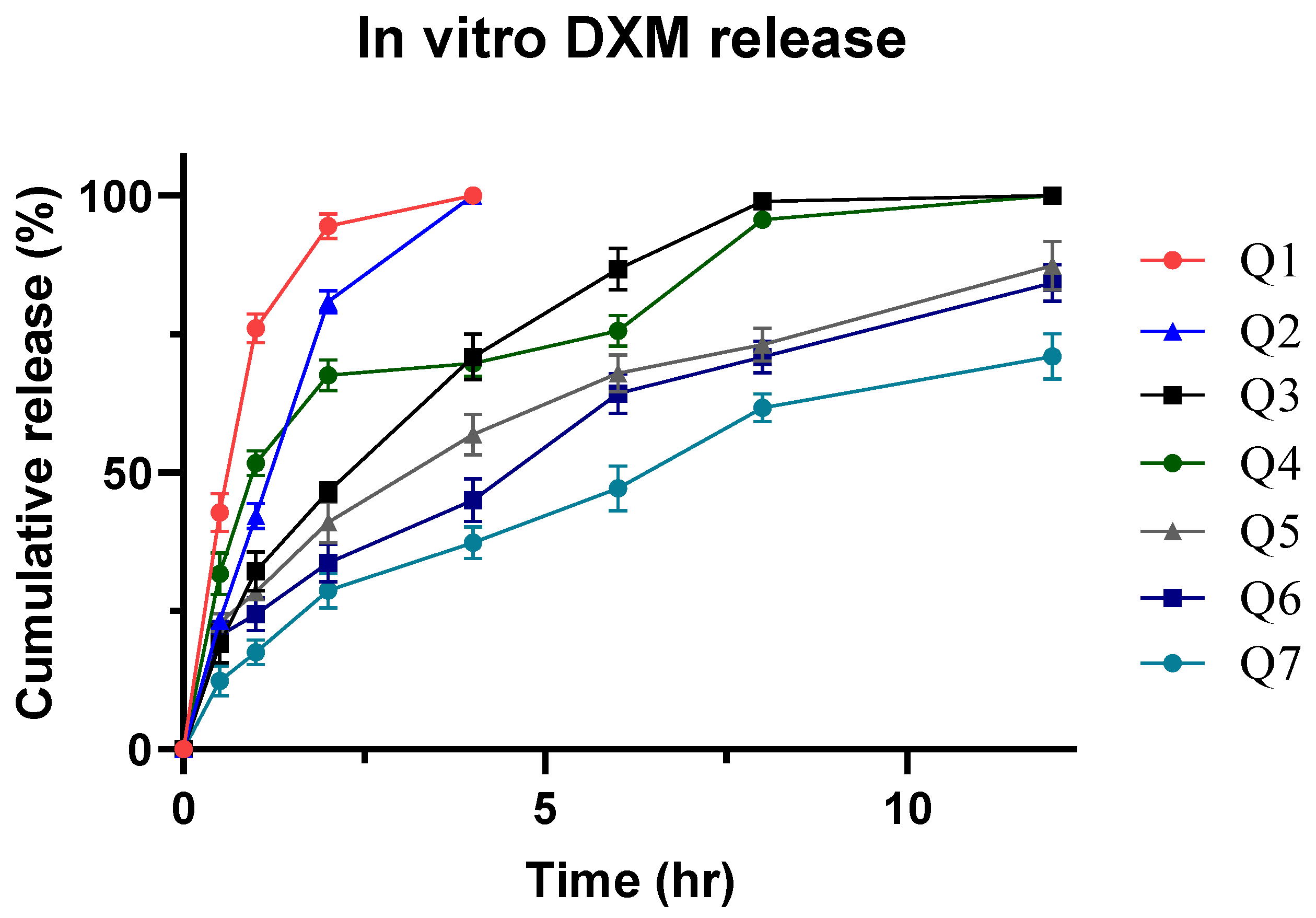
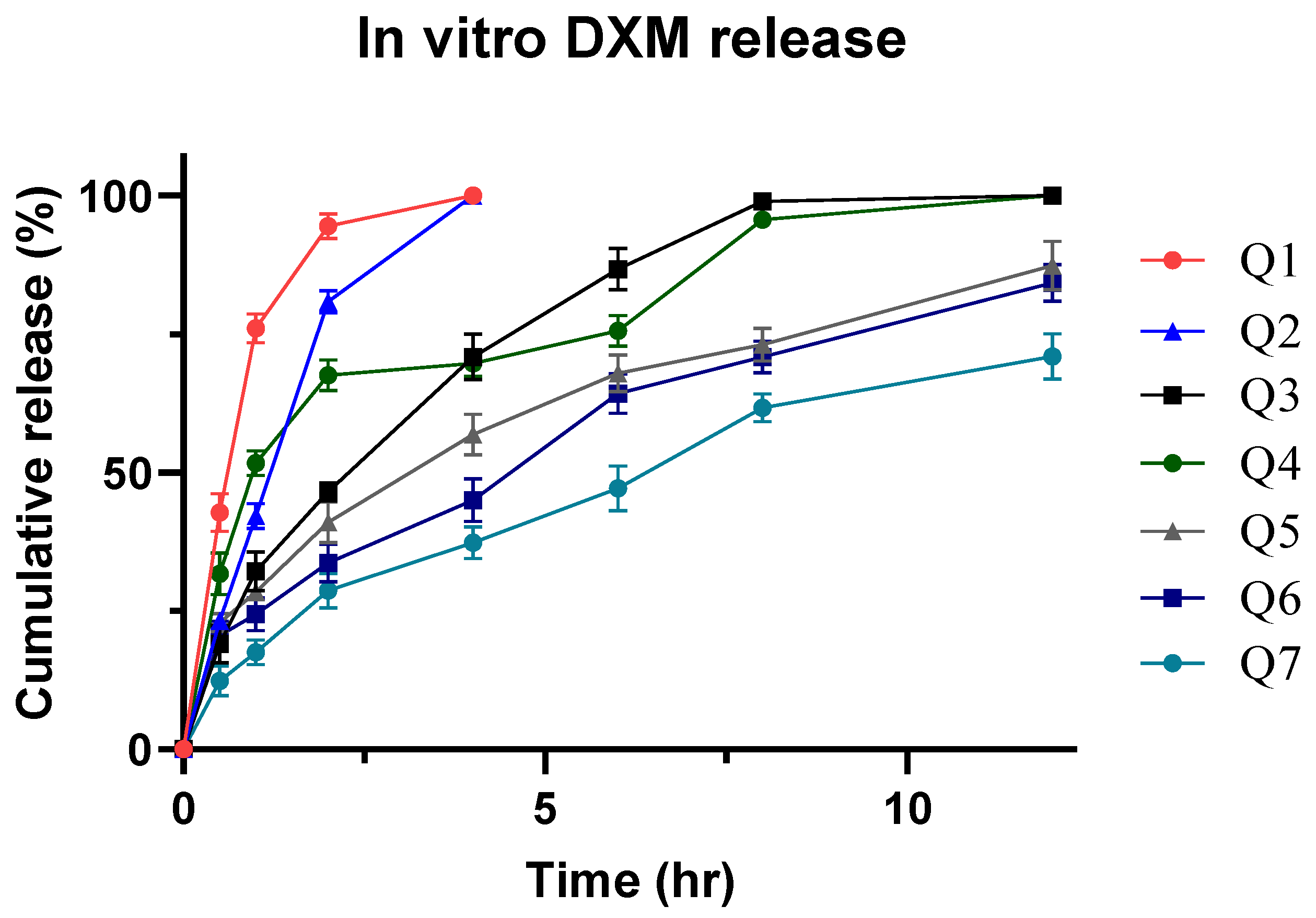
3.9. In Vitro Drug Release
3.10. Optimization of Formulation
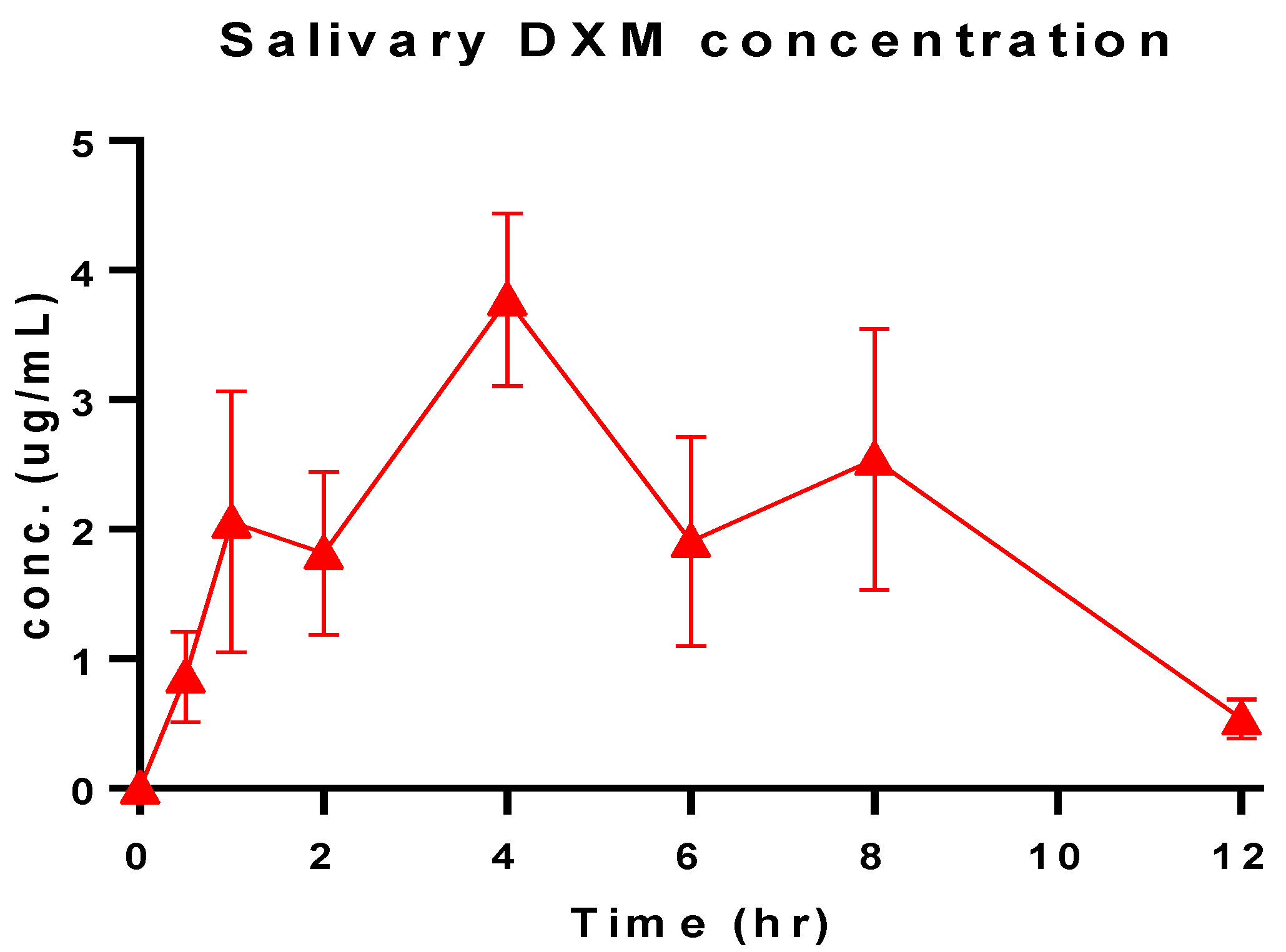
3.11. Salivary DXM Release in Volunteers
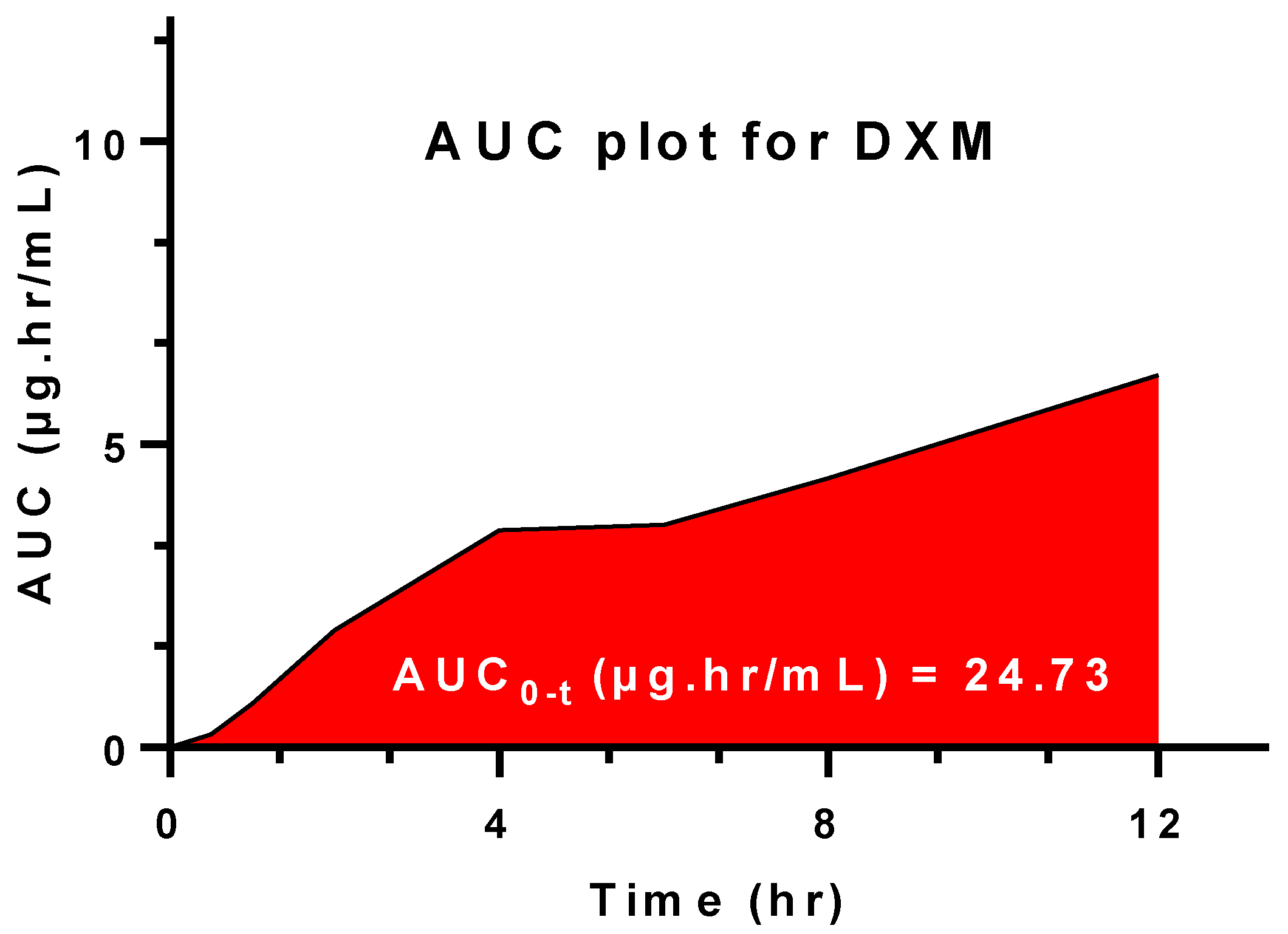
3.12. In Vitro-Salivary Release Kinetic
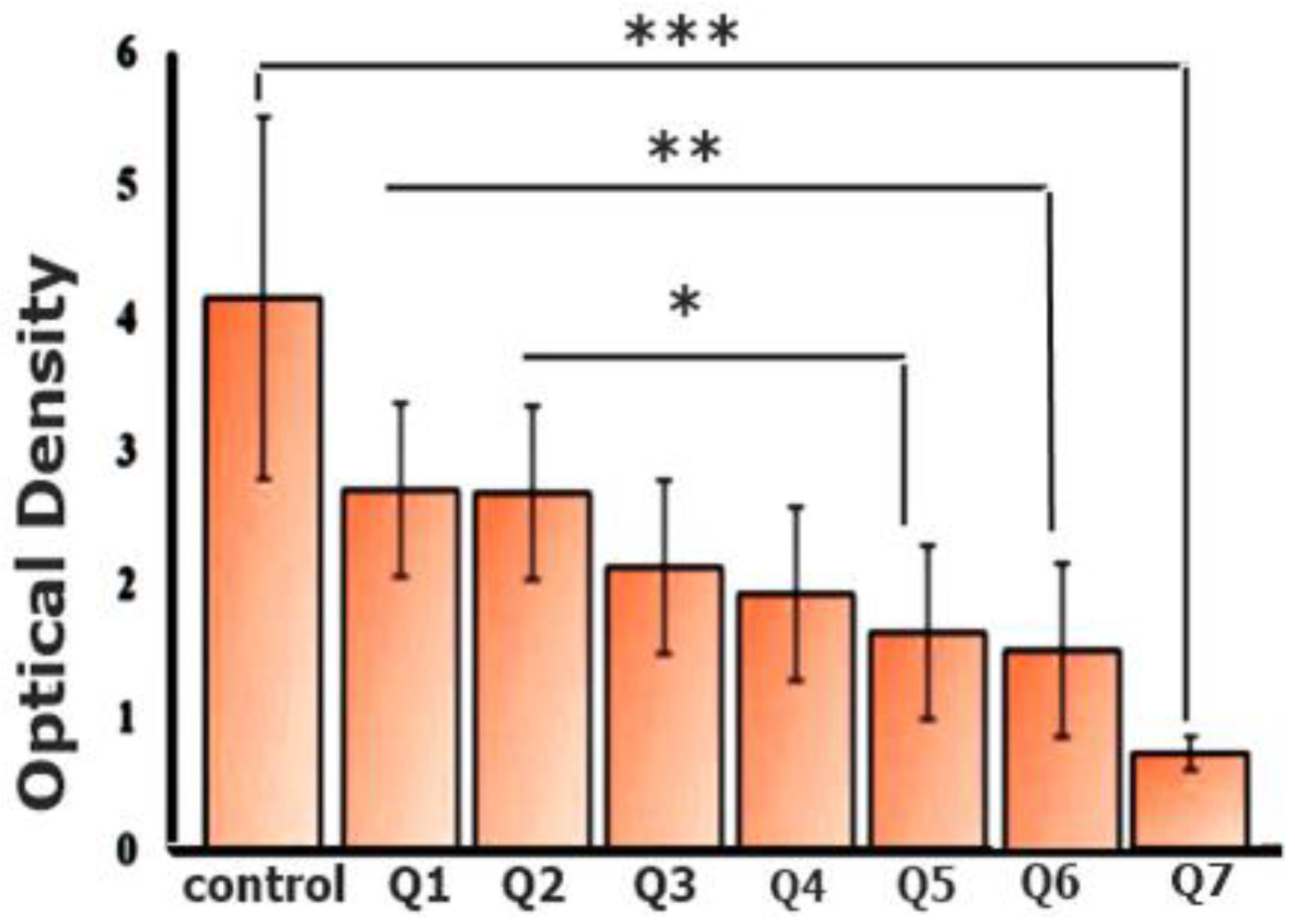
3.13. Coagulation Analysis via Optical Density
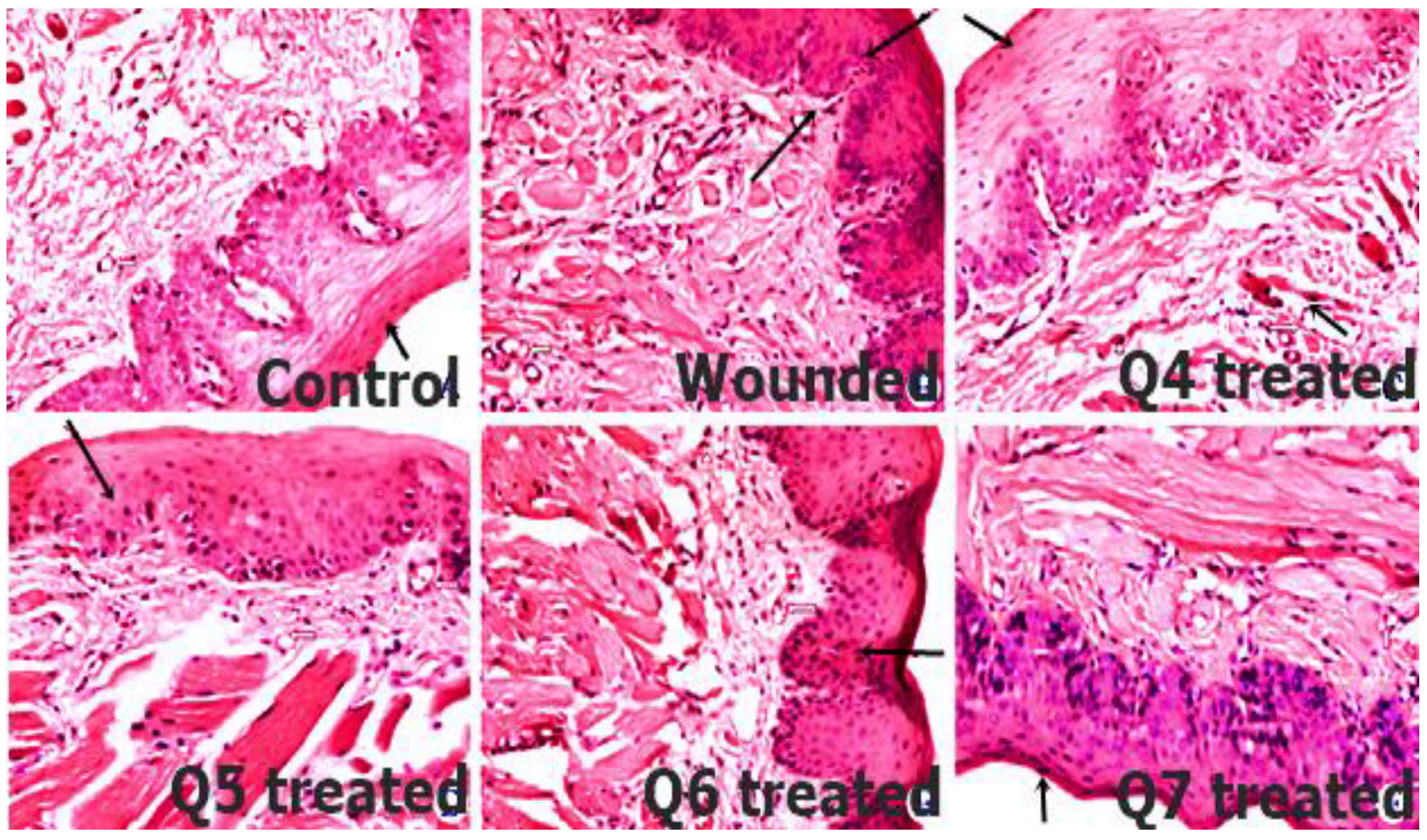
3.14. In Vivo Histopathological Evaluation
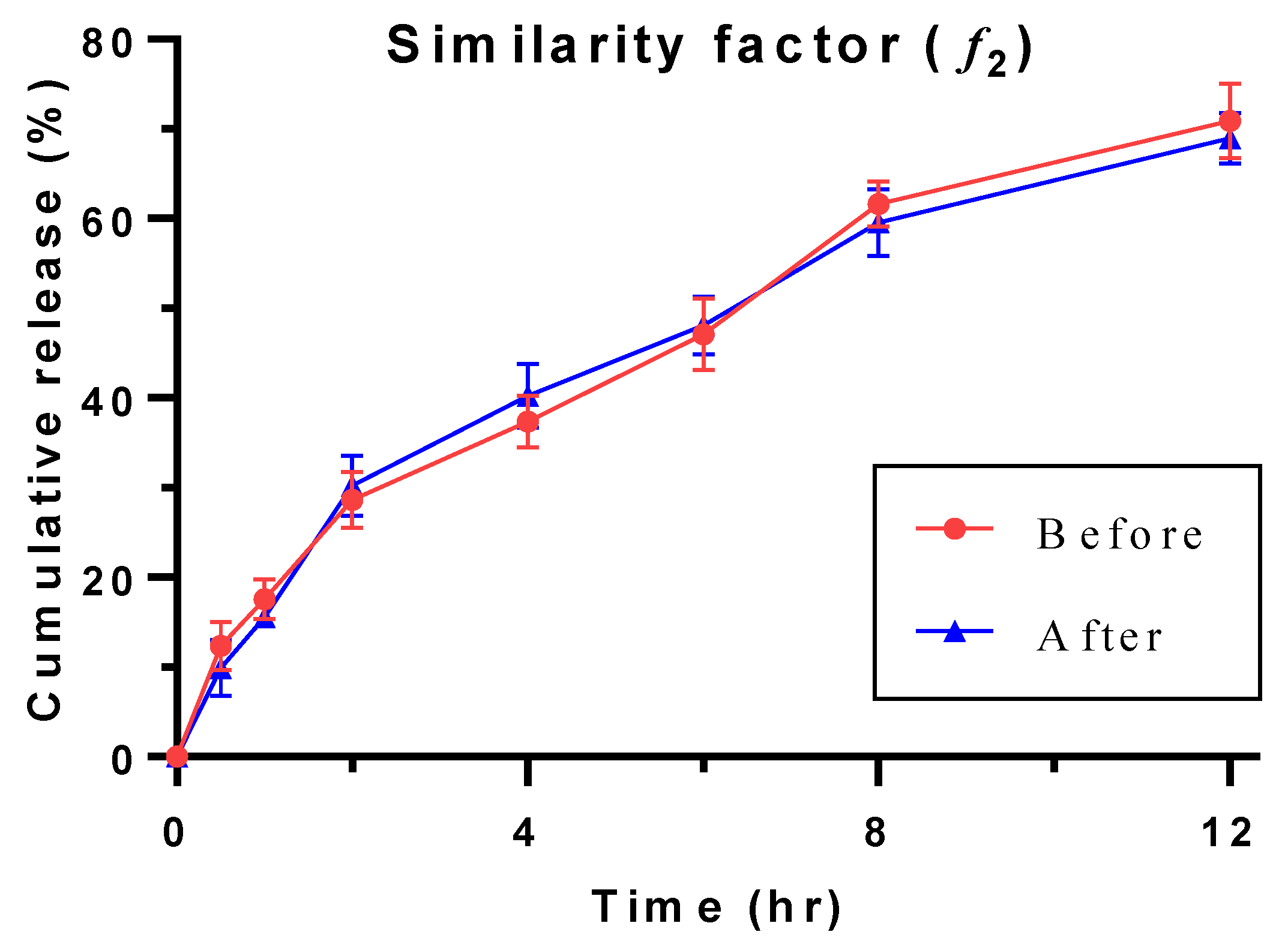
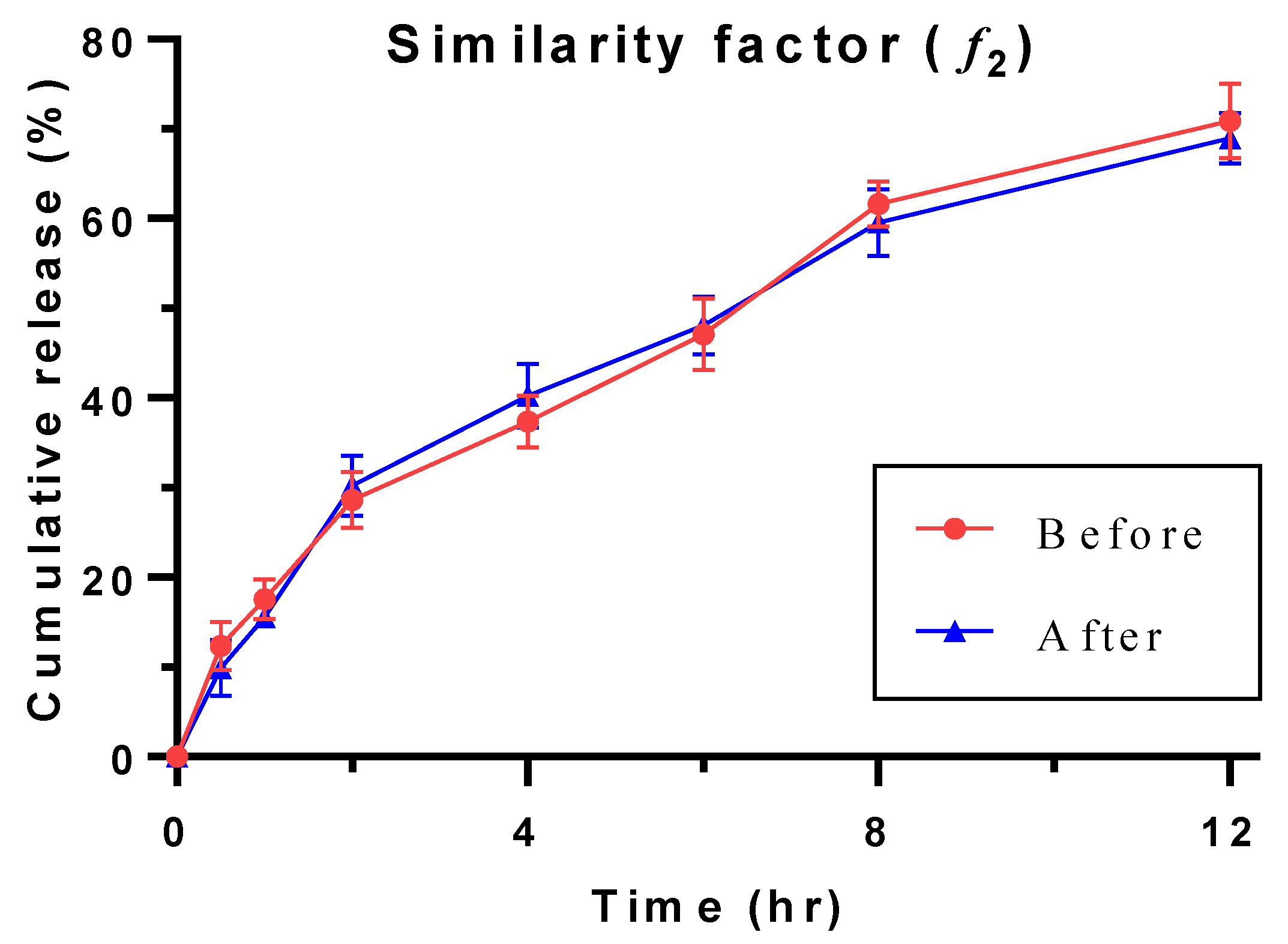
3.15. Stability Study
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Qing, C. The molecular biology in wound healing & non-healing wound. Chin. J. Traumatol. 2017, 20, 189–193. [Google Scholar] [PubMed]
- Oestem, H.; Tscheme, H. Pathophysiology and Classification of Soft Tissue Injuries Associated with Fractures; Fractures With Soft Tissue Injuries; Springer: Berlin, Germany, 1984; pp. 1–9. [Google Scholar]
- King, D.R.; Cohn, S.M.; Proctor, K.G.; Miami Clinical Trials Group. Modified rapid deployment hemostat bandage terminates bleeding in coagulopathic patients with severe visceral injuries. J. Trauma Acute Care Surg. 2004, 57, 756–759. [Google Scholar] [CrossRef] [PubMed]
- Hesketh, M.; Sahin, K.B.; West, Z.E.; Murray, R.Z. Macrophage phenotypes regulate scar formation and chronic wound healing. Int. J. Mol. Sci. 2017, 18, 1545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandavilli, S.; Nair, V.; Panchagnula, R. Polymers in transdermal drug delivery systems. Pharm. Technol. 2002, 26, 62–81. [Google Scholar]
- Malone-Povolny, M.J.; Maloney, S.E.; Schoenfisch, M.H. Nitric oxide therapy for diabetic wound healing. Adv. Healthc. Mater. 2019, 8, 1801210. [Google Scholar] [CrossRef]
- Price, N. Routine fluorescence imaging to detect wound bacteria reduces antibiotic use and antimicrobial dressing expenditure while improving healing rates: Retrospective analysis of 229 foot ulcers. Diagnostics 2020, 10, 927. [Google Scholar] [CrossRef]
- Narayanaswamy, R.; Torchilin, V. Hydrogels and their applications in targeted drug delivery. Molecules 2019, 24, 603. [Google Scholar] [CrossRef] [Green Version]
- Zhang, C.; Liu, Y.; Li, W.; Gao, P.; Xiang, D.; Ren, X.; Liu, D. Mucoadhesive buccal film containing ornidazole and dexamethasone for oral ulcers: In vitro and in vivo studies. Pharm. Dev. Technol. 2019, 24, 118–126. [Google Scholar] [CrossRef]
- Johnson, D.B.; Lopez, M.J.; Kelley, B. Dexamethasone; StatPearls: Treasure Island, FL, USA, 2018. [Google Scholar]
- Diaz-Salmeron, R.; Toussaint, B.; Huang, N.; Bourgeois Ducournau, E.; Alviset, G.; Goulay Dufaÿ, S.; Hillaireau, H.; Dufaÿ Wojcicki, A.; Boudy, V. Mucoadhesive poloxamer-based hydrogels for the release of HP-β-cd-complexed dexamethasone in the treatment of buccal diseases. Pharmaceutics 2021, 13, 117. [Google Scholar] [CrossRef]
- Karava, A.; Lazaridou, M.; Nanaki, S.; Michailidou, G.; Christodoulou, E.; Kostoglou, M.; Iatrou, H.; Bikiaris, D.N. Chitosan derivatives with mucoadhesive and antimicrobial properties for simultaneous nanoencapsulation and extended ocular release formulations of dexamethasone and chloramphenicol drugs. Pharmaceutics 2020, 12, 594. [Google Scholar] [CrossRef]
- Ansari, M.; Sadarani, B.; Majumdar, A. Optimization and evaluation of mucoadhesive buccal films loaded with resveratrol. J. Drug Deliv. Sci. Technol. 2018, 44, 278–288. [Google Scholar] [CrossRef]
- Ammar, H.O.; Ghorab, M.M.; Mahmoud, A.A.; Shahin, H.I. Design and in vitro/in vivo evaluation of ultra-thin mucoadhesive buccal film containing fluticasone propionate. AAPS PharmSciTech 2017, 18, 93–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De ACAlmeida, R.; Lemos, C.A.; De Moraes, S.L.; Pellizzer, E.P.; Vasconcelos, B.C. Efficacy of corticosteroids versus placebo in impacted third molar surgery: Systematic review and meta-analysis of randomized controlled trials. Int. J. Oral Maxillofac. Surg. 2019, 48, 118–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanif, S.; Sarfraz, R.M.; Syed, M.A.; Mahmood, A.; Minhas, M.U.; Irfan, M. Development and optimization of tibezonium iodide and lignocaine hydrochloride containing novel mucoadhesive buccal tablets: A pharmacokinetic investigation among healthy humans. Drug Dev. Ind. Pharm. 2021, 1–35. [Google Scholar] [CrossRef]
- Jovanović, M.; Petrović, M.; Cvijić, S.; Tomić, N.; Stojanović, D.; Ibrić, S.; Uskoković, P. 3D Printed Buccal Films for Prolonged-Release of Propranolol Hydrochloride: Development, Characterization and Bioavailability Prediction. Pharmaceutics 2021, 13, 2143. [Google Scholar] [CrossRef]
- Alves, T.F.; Rios, A.C.; da Silva Pontes, K.; Portella, D.L.; Aranha, N.; Severino, P.; Souto, E.B.; Gonsalves, J.K.; de Souza Nunes, R.; Chaud, M.V. Bilayer mucoadhesive buccal film for mucosal ulcers treatment: Development, characterization, and single study case. Pharmaceutics 2020, 12, 657. [Google Scholar] [CrossRef]
- Razzaq, S.; Syed, M.A.; Irfan, M.; Khan, I.; Sarfraz, R.M.; Shakir, R.; Ali, S.; Iqbal, Z.; Niaz, Y.; Mujtaba, S.H.; et al. Optimization of metronidazole SR buccal tablet for gingivitis using genetic algorithm. Pak. J. Pharm. Sci. 2021, 34, 2149–2158. [Google Scholar]
- Hanif, S.; Irfan, N.; Danish, Z.; Hussain, N.; Ali, M.; Nasir, B.; Iqbal, J.; Saeed, H.; Ali, R.; Saleem, Z. Computer aided formulation and characterization of propranolol hcl buccal tablet using polymeric blend. Open Conf. Proc. J. 2017, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hanif, S.; Sarfraz, R.M.; Syed, M.A.; Ali, S.; Iqbal, Z.; Shakir, R.; Iqbal, J. Formulation and evaluation of chitosan-based polymeric biodegradable mucoadhesive buccal delivery for locally acting drugs: In vitro, ex vivo and in vivo volunteers characterization. Lat. Am. J. Pharm. 2021, 40, 670–681. [Google Scholar]
- Razzaq, S.; Hanif, S.; Syed, M.A.; Iqbal, J.; Raza, S.A.; Riaz, H.; Abid, F. Development and evaluation of mucoadhesive buccal tablet containing metronidazole for the treatment of periodontitis and gingivitis. Pak. J. Pharm. Sci. 2018, 31, 1903–1910. [Google Scholar]
- Hussain, A.; Syed, M.A.; Abbas, N.; Hanif, S.; Arshad, M.S.; Bukhari, N.I.; Hussain, K.; Akhlaq, M.; Ahmad, Z. Development of ann optimized mucoadhesive buccal tablet containing flurbiprofen and lidocaine for dental pain. Acta Pharm. 2016, 66, 245–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrich, R.B.; Ravanello, A.; Cichota, L.C.; Rolim, C.M.; Beck, R.C. Validation of a simple and rapid UV spectrophotometric method for dexamethasone assay in tablets. Química Nova 2009, 32, 1052–1054. [Google Scholar] [CrossRef]
- Arshad, R.; Sohail, M.F.; Sarwar, H.S.; Saeed, H.; Ali, I.; Akhtar, S.; Hussain, S.Z.; Afzal, I.; Jahan, S.; Shahnaz, G. ZnO-NPs embedded biodegradable thiolated bandage for postoperative surgical site infection: In vitro and in vivo evaluation. PLoS ONE 2019, 14, e0217079. [Google Scholar] [CrossRef] [Green Version]
- Favero, R.; Apaza Alccayhuaman, K.A.; Botticelli, D.; Xavier, S.P.; Ferreira Balan, V.; Macchi, V.; De Caro, R. Sinus Mucosa Thinning and Perforations after Sinus Lifting Performed with Different Xenografts: A Histological Analysis in Rabbits. Dent. J. 2022, 10, 2. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.N.; Borkar, R.M.; Kalariya, P.D.; Gangwal, R.P.; Sangamwar, A.T.; Samanthula, G.; Ragampeta, S. Characterization of degradation products of Ivabradine by LC-HR-MS/MS: A typical case of exhibition of different degradation behaviour in HCl and H2SO4 acid hydrolysis. J. Mass Spectrom. 2015, 50, 344–353. [Google Scholar] [CrossRef]
- Suarez-Sharp, S.; Abend, A.; Hoffelder, T.; Leblond, D.; Delvadia, P.; Kovacs, E.; Diaz, D.A. In Vitro Dissolution Profiles Similarity Assessment in Support of Drug Product Quality: What, How, When—Workshop Summary Report. AAPS J. 2020, 22, 74. [Google Scholar] [CrossRef]
- Fahim, F.; Naseer, A.; Ahmed, S.; Sherazi, S.T.; Bhanger, M.I. A green approach for the determination of selected anti-diabetic drugs in pharmaceutical formulation by transmission FTIR spectroscopy. J. Braz. Chem. Soc. 2014, 25, 2032–2038. [Google Scholar] [CrossRef]
- Stofella, N.C.; Veiga, A.; Oliveira, L.J.; Montin, E.F.; Andreazza, I.F.; Carvalho Filho, M.A.; Bernardi, L.S.; Oliveira, P.R.; Murakami, F.S. Solid-state characterization of different crystalline forms of sitagliptin. Materials 2019, 12, 2351. [Google Scholar] [CrossRef] [Green Version]
- Ali, A.; Khalid, I.; Minhas, M.U.; Barkat, K.; Khan, I.U.; Syed, H.K.; Umar, A. Preparation and in vitro evaluation of Chondroitin sulfate and carbopol based mucoadhesive controlled release polymeric composites of Loxoprofen using factorial design. Eur. Polym. J. 2019, 121, 109312. [Google Scholar] [CrossRef]
- Punčochová, K.; Ewing, A.V.; Gajdošová, M.; Sarvašová, N.; Kazarian, S.G.; Beránek, J.; Štěpánek, F. Identifying the mechanisms of drug release from amorphous solid dispersions using MRI and ATR-FTIR spectroscopic imaging. Int. J. Pharm. 2015, 483, 256–267. [Google Scholar] [CrossRef]
- Rachid, O.; Rawas-Qalaji, M.; Simons, K.J. Epinephrine in anaphylaxis: Preclinical study of pharmacokinetics after sublingual administration of taste-masked tablets for potential pediatric use. Pharmaceutics 2018, 10, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baliga, S.; Muglikar, S.; Kale, R. Salivary pH: A diagnostic biomarker. J. Indian Soc. Periodontol. 2013, 17, 461. [Google Scholar] [CrossRef] [PubMed]
- Bahram, M.; Mohseni, N.; Moghtader, M. An introduction to hydrogels and some recent applications. In Emerging Concepts in Analysis and Applications of Hydrogels; IntechOpen: London, UK, 2016. [Google Scholar]
- Alshetaili, A.; Almutairy, B.K.; Alshehri, S.M.; Repka, M.A. Development and Characterization of Sustained-Released Donepezil Hydrochloride Solid Dispersions Using Hot Melt Extrusion Technology. Pharmaceutics 2021, 13, 213. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Liu, W.; Zhang, L.-j. The role of toll-like receptors in skin host defense, psoriasis, and atopic dermatitis. J. Immunol. Res. 2019, 2019, 1824624. [Google Scholar] [CrossRef]
- Weijtens, O.; Schoemaker, R.C.; Lentjes, E.G.; Romijn, F.P.; Cohen, A.F.; van Meurs, J.C. Dexamethasone concentration in the subretinal fluid after a subconjunctival injection, a peribulbar injection, or an oral dose. Ophthalmology 2000, 107, 1932–1938. [Google Scholar] [CrossRef]
- Chang-Lin, J.E.; Burke, J.A.; Peng, Q.; Lin, T.; Orilla, W.C.; Ghosn, C.R.; Zhang, K.M.; Kuppermann, B.D.; Robinson, M.R.; Whitcup, S.M.; et al. Pharmacokinetics of a sustained-release dexamethasone intravitreal implant in vitrectomized and nonvitrectomized eyes. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4605–4609. [Google Scholar] [CrossRef] [Green Version]
- Mircioiu, C.; Voicu, V.; Anuta, V.; Tudose, A.; Celia, C.; Paolino, D.; Fresta, M.; Sandulovici, R.; Mircioiu, I. Mathematical modeling of release kinetics from supramolecular drug delivery systems. Pharmaceutics 2019, 11, 140. [Google Scholar] [CrossRef] [Green Version]
- Lamoudi, L.; Chaumeil, J.C.; Daoud, K. Swelling, erosion and drug release characteristics of Sodium Diclofenac from heterogeneous matrix tablets. J. Drug Deliv. Sci. Technol. 2016, 31, 93–100. [Google Scholar] [CrossRef]
- Alam, N.; Beg, S.; Rizwan, M.; Ahmad, A.; Ahmad, F.J.; Ali, A.; Aqil, M. Mucoadhesive elementary osmotic pump tablets of trimetazidine for controlled drug delivery and reduced variability in oral bioavailability. Drug Dev. Ind. Pharm. 2015, 41, 692–702. [Google Scholar] [CrossRef]
- Boateng, J.; Okeke, O. Evaluation of clay-functionalized wafers and films for nicotine replacement therapy via buccal mucosa. Pharmaceutics 2019, 11, 104. [Google Scholar] [CrossRef] [Green Version]
- Szekalska, M.; Sosnowska, K.; Czajkowska-Kośnik, A.; Winnicka, K. Calcium chloride modified alginate microparticles formulated by the spray drying process: A strategy to prolong the release of freely soluble drugs. Materials 2018, 11, 1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ingredients | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 |
|---|---|---|---|---|---|---|---|
| DXM | 4 | 4 | 4 | 4 | 4 | 4 | 4 |
| Agar | 50 | 40 | 30 | 25 | 20 | 10 | 5 |
| EC | 5 | 10 | 20 | 25 | 30 | 40 | 50 |
| PVP | 5 | 5 | 5 | 5 | 5 | 5 | 5 |
| Poly. sucralose | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Mg. stearate | 3 | 3 | 3 | 3 | 3 | 3 | 3 |
| Lactose | 36 | 36 | 36 | 36 | 36 | 36 | 36 |
| Code | Weight Variation (mg ± SD) | Diameter (mm ± SD) | Thickness (mm ± SD) | ME (%) | Surface pH |
|---|---|---|---|---|---|
| Q1 | 200.4 ± 1.91 | 8.04 ± 0.07 | 3.77 ± 2.08 | 83.74 | 7.31 |
| Q2 | 198.9 ± 2.18 | 8.03 ± 0.04 | 3.76 ± 1.97 | 79.68 | 7.38 |
| Q3 | 201.6 ± 1.52 | 8.05 ± 0.09 | 3.77 ± 0.62 | 77.12 | 7.42 |
| Q4 | 200.4 ± 1.83 | 8.04 ± 0.16 | 3.76 ± 0.89 | 71.37 | 7.32 |
| Q5 | 203.5 ± 1.87 | 8.05 ± 0.08 | 3.77 ± 0.21 | 72.36 | 7.60 |
| Q6 | 200.1 ± 2.05 | 8.05 ± 0.11 | 3.76 ± 1.31 | 67.28 | 7.37 |
| Q7 | 198.2 ± 1.99 | 8.03 ± 0.09 | 3.75 ± 0.46 | 63.46 | 7.41 |
| Parameters | Findings |
|---|---|
| Dose (mg) | 8 |
| Cmax (µg/mL) | 3.77 |
| tmax (h) | 4 |
| kel (h−1) | 0.31 |
| AUC0–t (µg·hr/mL) | 24.73 |
| AUCt–∞ (µg·hr/mL) | 1.70 |
| AUC0–∞ (µg·hr/mL) | 26.44 |
| AUCt–∞ (%) | 6.43 |
| Contribution AUCt–∞ | insignificant |
| Model | Zero Order | 1st Order | Higuchi | Korsmeyer-Peppas | Hixson-Crowell | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| r2 | k0 | r2 | k1 | r2 | kH | r2 | kKP | n | r2 | kHC | |
| In vitro | 0.970 | 7.001 | 0.9507 | 0.117 | 0.989 | 20.204 | 0.9931 | 18.206 | 0.554 | 0.9333 | 0.033 |
| Salivary | 0.082 | 2.518 | 0.127 | 0.032 | 0.318 | 8.891 | 0.3301 | 20.484 | 0.05 | 0.112 | 0.01 |
| Interval (Months) | Contents (% ±SD) | ET | MS |
|---|---|---|---|
| 0 | 98.17 ± 1.44 | 8.29 ± 2.21 | 13.96 ± 2.63 |
| 0.5 | 99.42 ± 0.58 | 8.11 ± 1.42 | 13.73 ± 2.44 |
| 1 | 98.96 ± 1.36 | 8.19 ± 2.83 | 13.9 ± 1.09 |
| 3 | 98.01 ± 0.10 | 8.21 ± 2.65 | 13.95 ± 2.51 |
| 6 | 99.32 ± 0.25 | 8.1 ± 1.19 | 13.91 ± 2.18 |
| Release profile comparison after stability conditions | |||
| Dissimilarity factor (f1) [Specification 0–15] | 5.07 | ||
| Similarity factor (f2) [Specification 50–100] | 83.07 | ||
| Before-After Stability | Mean | Standard Deviation | Standard Error Mean | 95% Confidence Interval of the Difference | t Value | df | Sig. (2-Tailed) | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| DXM | 0.385 | 2.02 | 0.71 | −1.31 | 208 | 0.536 | 7 | 0.608 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javed, Q.u.A.; Syed, M.A.; Arshad, R.; Rahdar, A.; Irfan, M.; Raza, S.A.; Shahnaz, G.; Hanif, S.; Díez-Pascual, A.M. Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers. Pharmaceutics 2022, 14, 807. https://doi.org/10.3390/pharmaceutics14040807
Javed QuA, Syed MA, Arshad R, Rahdar A, Irfan M, Raza SA, Shahnaz G, Hanif S, Díez-Pascual AM. Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers. Pharmaceutics. 2022; 14(4):807. https://doi.org/10.3390/pharmaceutics14040807
Chicago/Turabian StyleJaved, Qurrat ul Ain, Muhammad Ali Syed, Rabia Arshad, Abbas Rahdar, Muhammad Irfan, Syed Atif Raza, Gul Shahnaz, Sana Hanif, and Ana M. Díez-Pascual. 2022. "Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers" Pharmaceutics 14, no. 4: 807. https://doi.org/10.3390/pharmaceutics14040807
APA StyleJaved, Q. u. A., Syed, M. A., Arshad, R., Rahdar, A., Irfan, M., Raza, S. A., Shahnaz, G., Hanif, S., & Díez-Pascual, A. M. (2022). Evaluation and Optimization of Prolonged Release Mucoadhesive Tablets of Dexamethasone for Wound Healing: In Vitro–In Vivo Profiling in Healthy Volunteers. Pharmaceutics, 14(4), 807. https://doi.org/10.3390/pharmaceutics14040807