
Packaging and Delivery of Asthma Therapeutics




Abstract
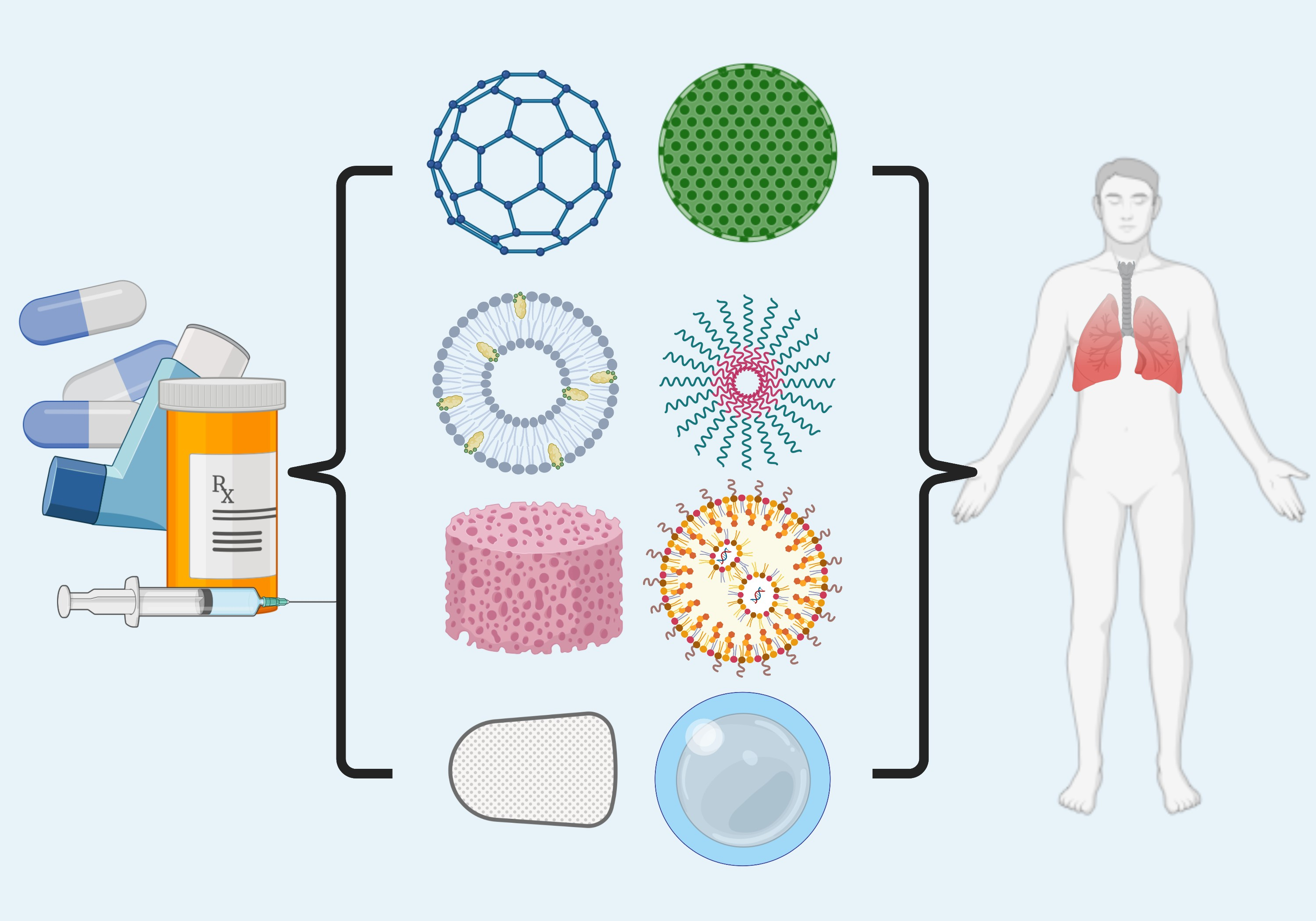
1. Introduction
Asthma Pathology
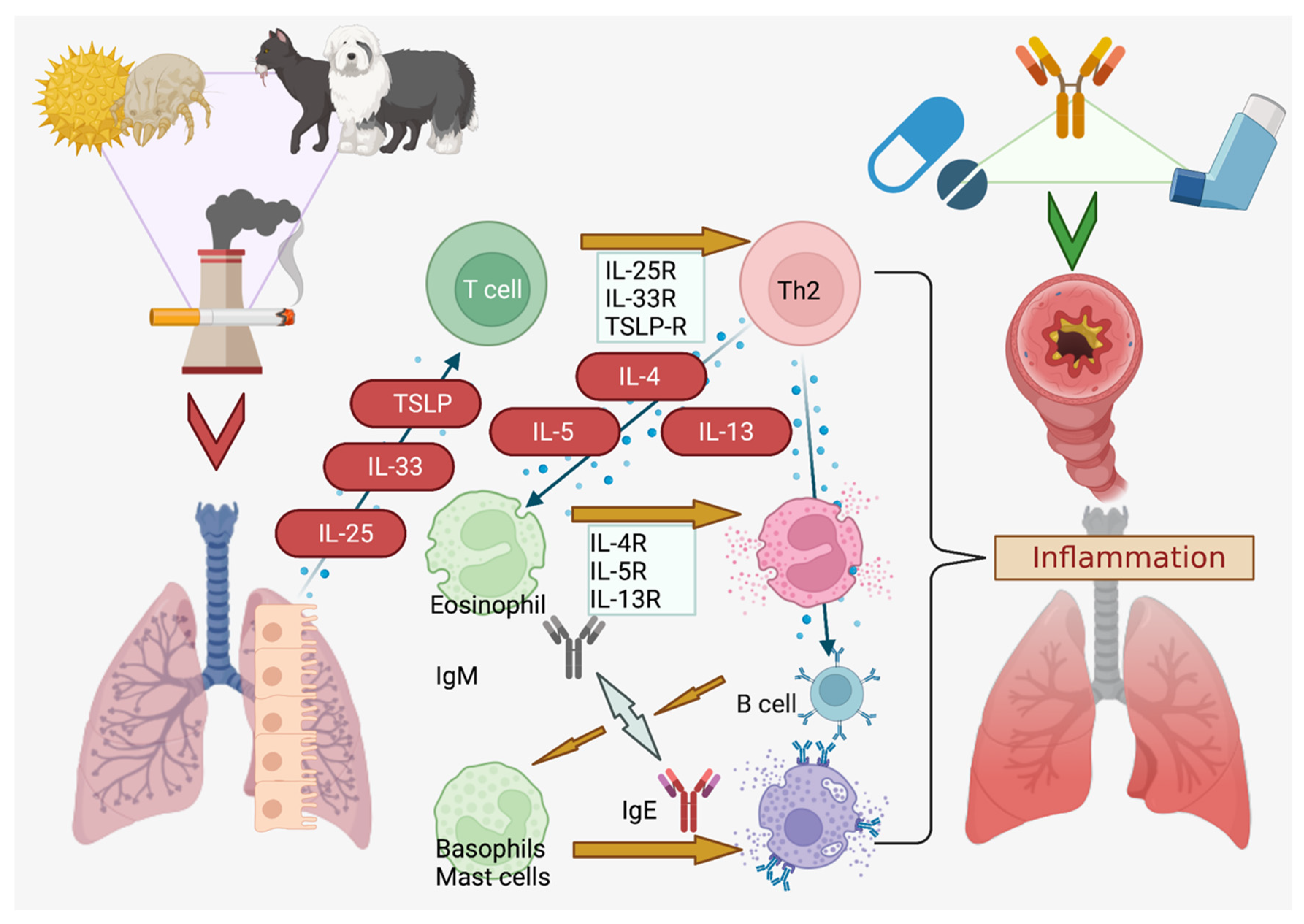
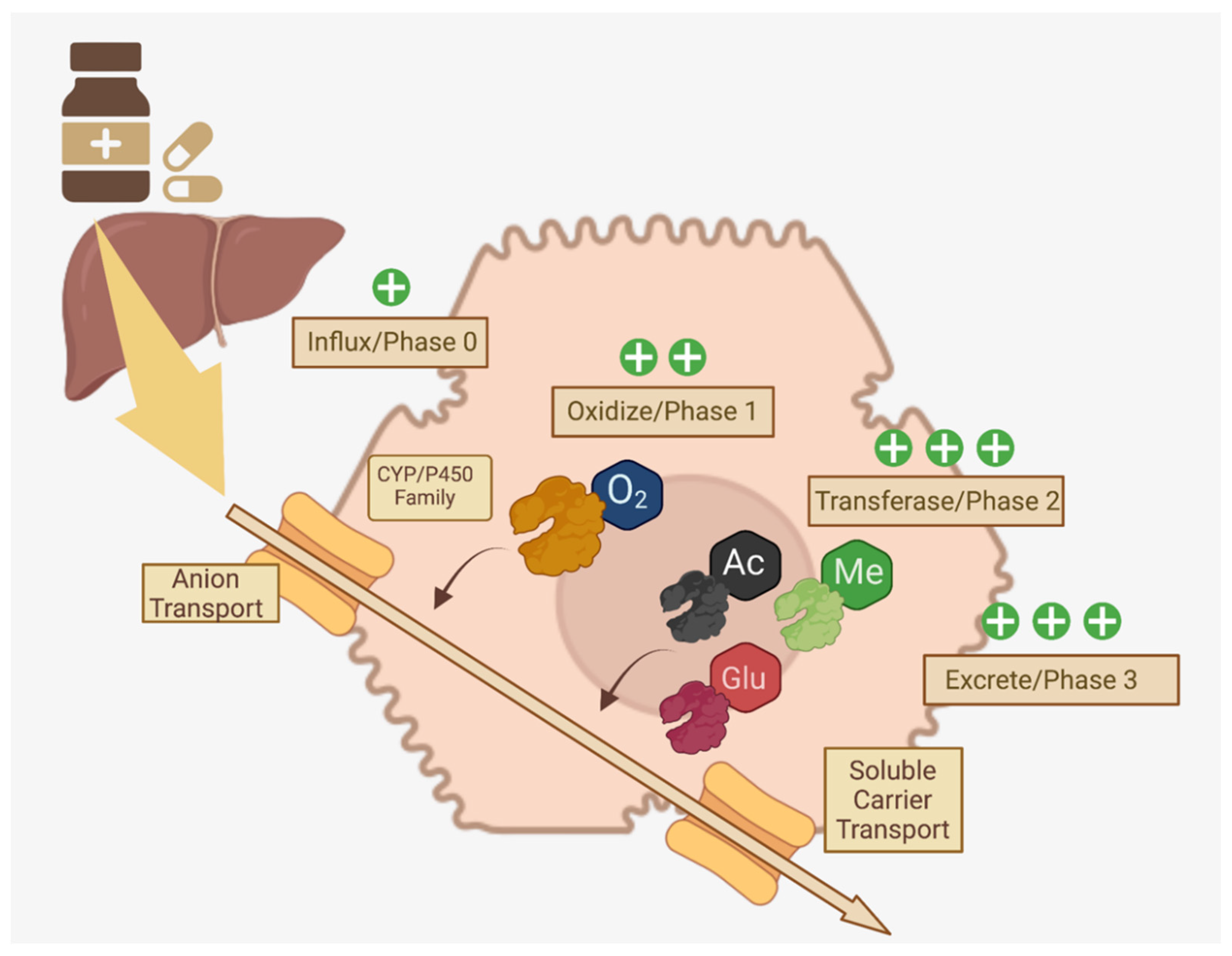
2. Asthma Drug Metabolism (General)
2.1. “First-Pass” Cytochrome Metabolic System
2.2. Drug Metabolism Phases
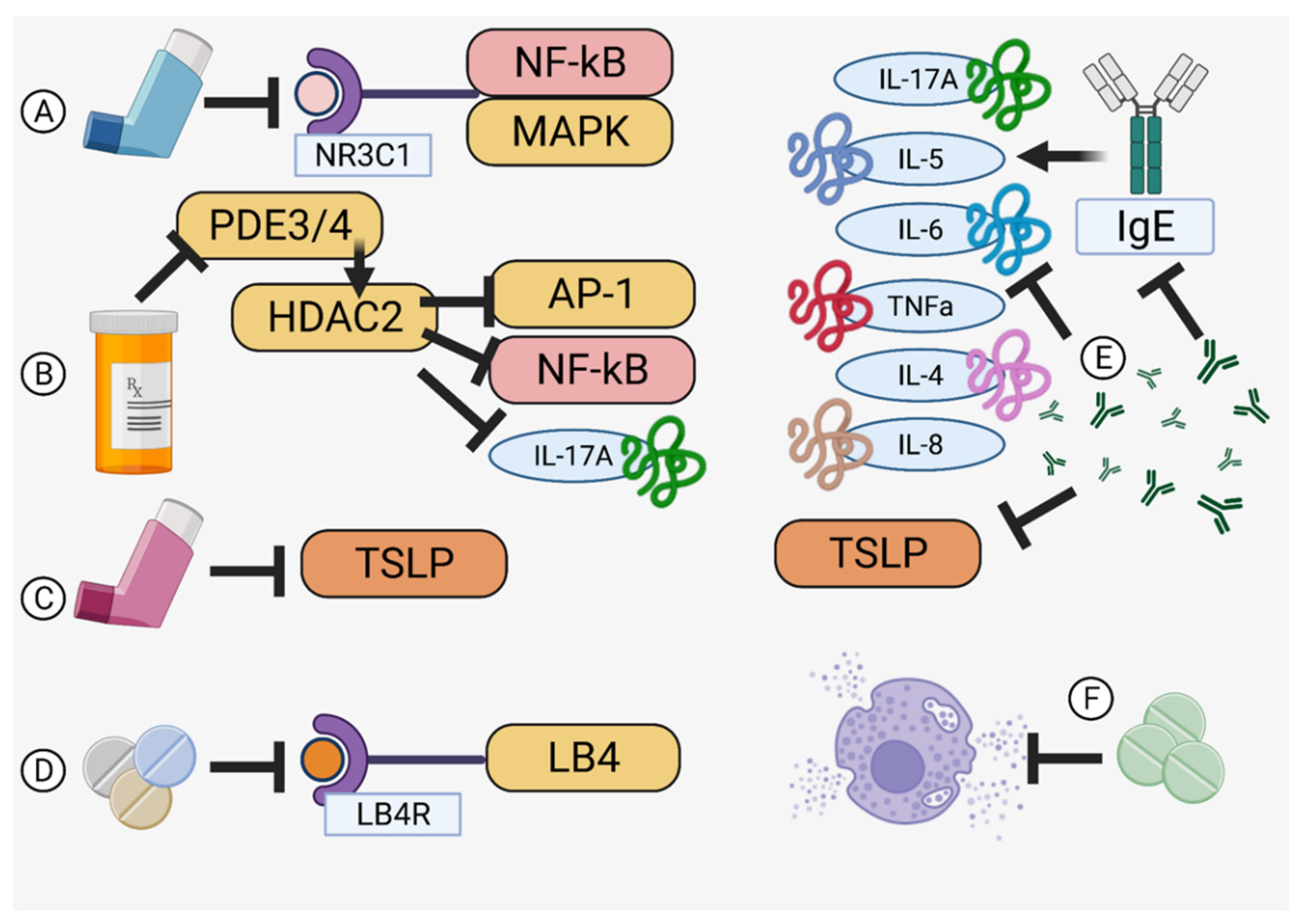
3. Asthma Treatments Currently Available
3.1. Steroids
3.2. Theophylline
3.3. Long-Acting Beta Agonists/Muscarinic Antagonists
3.4. Leukotriene Receptor Antagonists
3.5. Antibody-Derived Therapeutics
3.6. Anti-Histamines and Anti-Allergics

3.7. Comparisons and Efficacy between Traditional and Biologic Treatments
4. Lung-Focused, Mechanical Drug Delivery Systems
4.1. Propellant-Pressurized Metered Dose Inhalers
4.2. Dry Powder Inhalers
4.3. Nebulizers
4.4. Comparisons between Delivery Systems
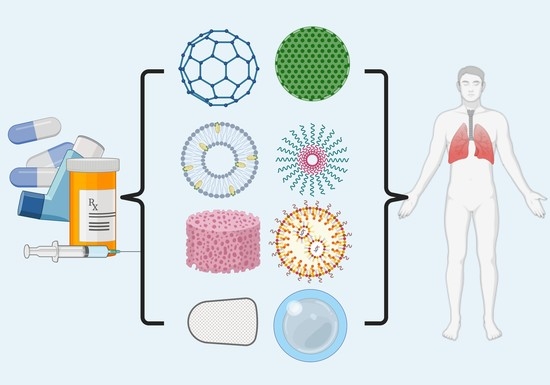
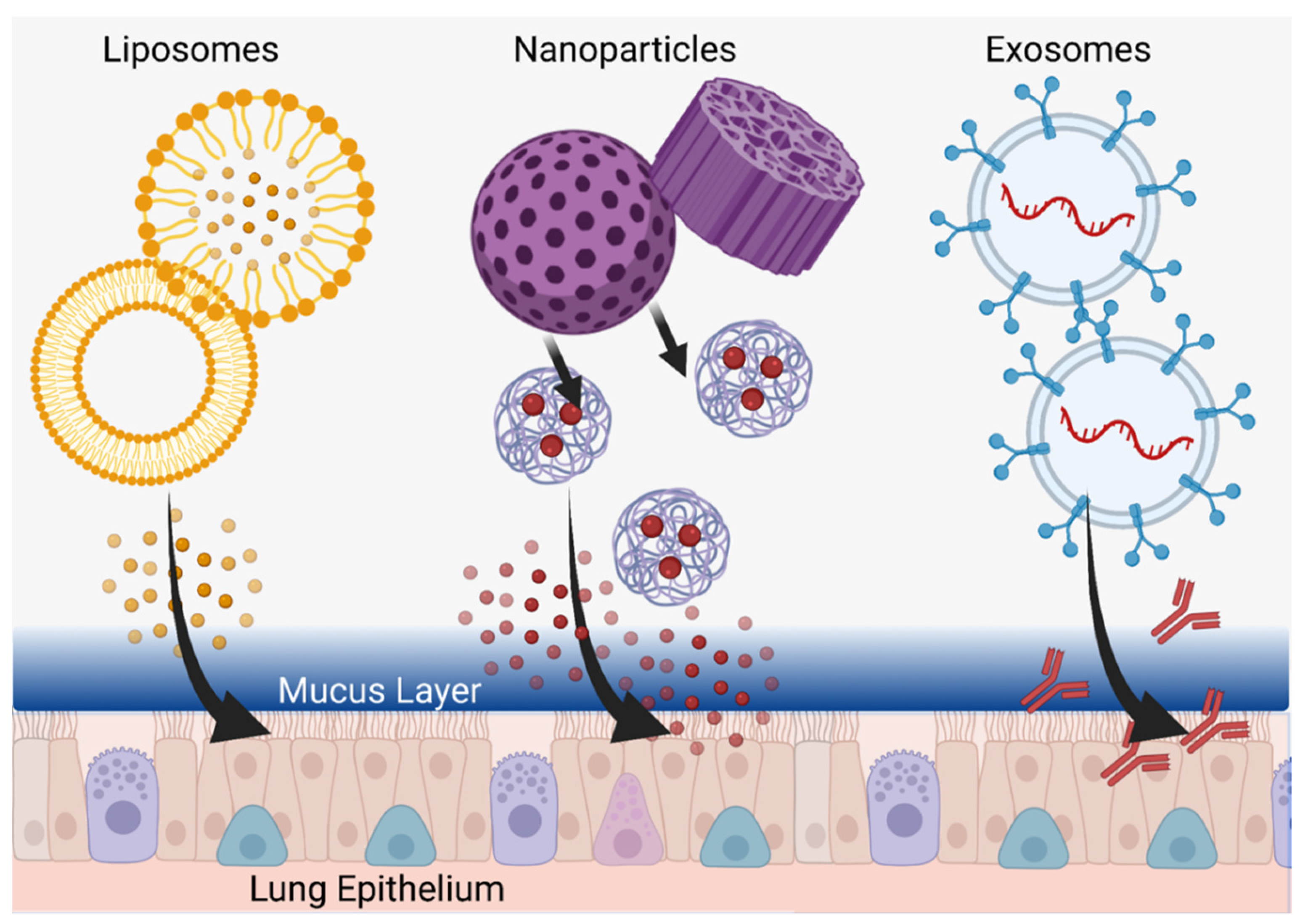
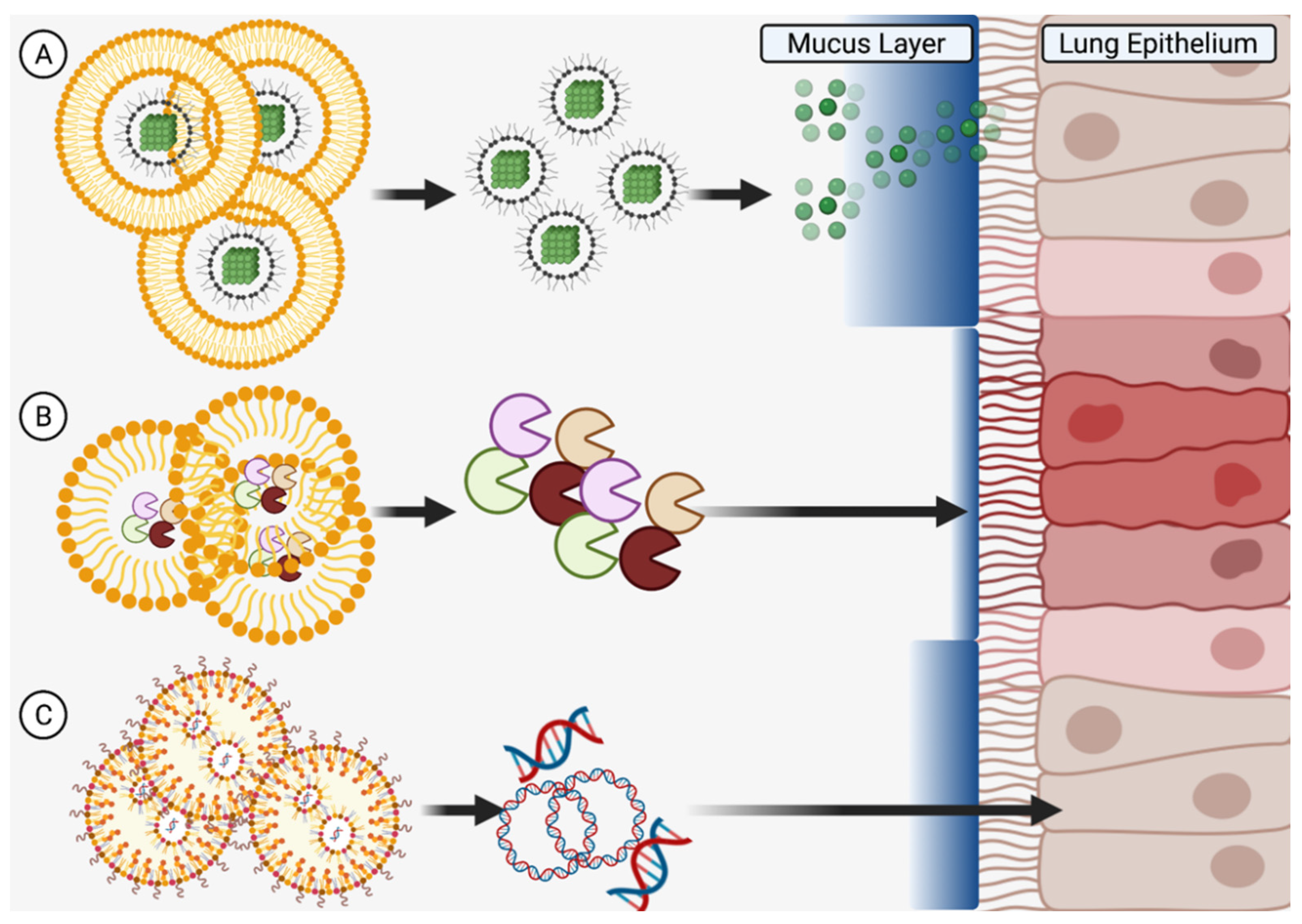
5. Drug Packaging
5.1. Use of Nanoparticles for Delivery of Therapeutic Agents in Asthma
5.2. Liposomes
5.3. Nanoparticles
5.4. Extracellular Vesicles
5.5. New Horizons of Delivery Potential
6. Requirements for Effectiveness in a Target Population
6.1. Nanoscale Delivery Parameters for Drug Delivery in Children
6.2. Nanoscale Delivery Parameters for Drug Delivery in Athletes
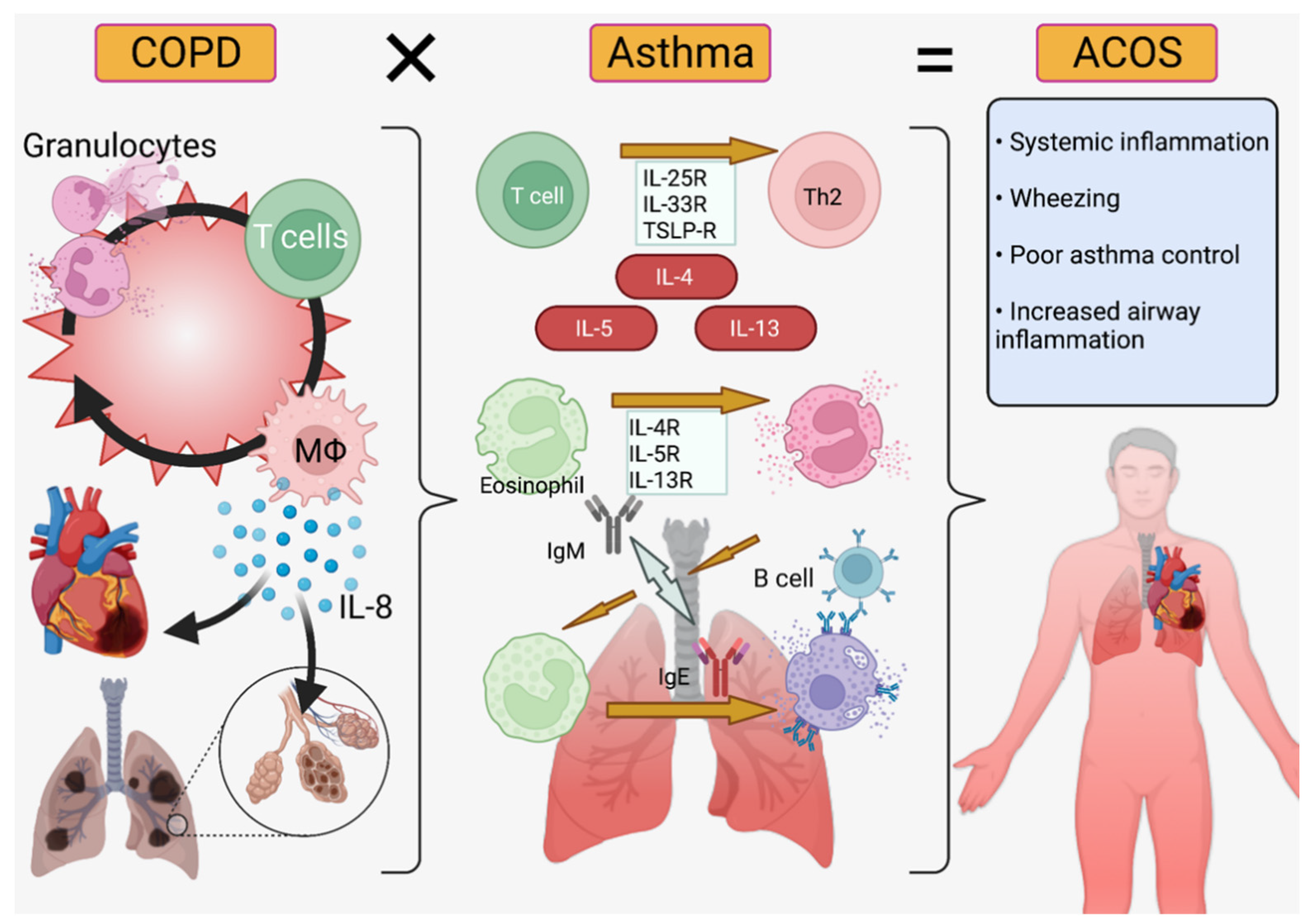
6.3. Nanoscale Delivery Parameters for Drug Delivery in Co-Morbid Conditions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| AERD | Aspirin-Exacerbated Respiratory Syndrome |
| ACOS | Asthma-COPD Overlap Syndrome |
| AG | Andrographolide |
| ATP | Adenosine Triphosphate |
| BALB/C | Bagg and Albino Mice (White Lab Mice) |
| COPD | Chronic Obstructive Pulmonary Disorder |
| DMPC | Dimyristoyl-sn-glycero-3-phosphocholine |
| DPI | Dry Powder Inhaler |
| FACET | Formoterol and Corticosteroids Establishing Therapy |
| FEV1 | Forced Expiratory Volume in the 1st Second |
| GERD | GastroEsophageal Reflux Disease |
| GOAL | Gaining Optimal Asthma controL |
| HSPC | Hydrogenated Soybean Phosphatidylcholine |
| hUCMSCs | Human Umbilical Cord MSCs |
| ICS | Inhaled Corticosteroids |
| IL | Interleukin |
| ILC2s | Group 2 Innate Lymphoid Cells |
| LABA/LAMA | Long-Acting Beta/Muscarinic Agonist |
| LRA | Leukotriene Receptor Antagonist |
| miR-1470 | Micro RNA 1470 |
| MSC | Mesenchymal Stem Cell |
| MSC-Exo | Exosomes Derived from Mesenchymal Stem Cells |
| PLGA | Polylactide-co-glycolide |
| pMDI | Pressurized Metered Dose Inhaler |
| poly(I:C) | Polyinosin-polycytidylic acid |
| sEV | MSC-small Extracellular Vesicles |
| SPIO | Superparamagnetic Nanoparticles of Iron Oxides |
References
- Yamauchi, Y.I. Epidemiology of Asthma: The Present and Near Future. Nihon Naika Gakkai Zasshi 2018, 107, 2059–2066. [Google Scholar] [CrossRef]
- Bush, A. Pathophysiological Mechanisms of Asthma. Front. Pediatr. 2019, 7, 68. [Google Scholar] [CrossRef] [PubMed]
- Alashkar Alhamwe, B.; Potaczek, D.P.; Miethe, S.; Alhamdan, F.; Hintz, L.; Magomedov, A.; Garn, H. Extracellular Vesicles and Asthma-More Than Just a Co-Existence. Int. J. Mol. Sci. 2021, 22, 4984. [Google Scholar] [CrossRef]
- Patel, M.; Shaw, D. A review of standard pharmacological therapy for adult asthma—Steps 1 to 5. Chron. Respir. Dis. 2015, 12, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Wenzel, S.E. Asthma phenotypes: The evolution from clinical to molecular approaches. Nat. Med. 2012, 18, 716–725. [Google Scholar] [CrossRef]
- Nomura, A.; Uchida, Y.; Sakamoto, T.; Ishii, Y.; Masuyama, K.; Morishima, Y.; Hirano, K.; Sekizawa, K. Increases in collagen type I synthesis in asthma: The role of eosinophils and transforming growth factor-beta. Clin. Exp. Allergy 2002, 32, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Olafsdottir, T.A.; Theodors, F.; Bjarnadottir, K.; Bjornsdottir, U.S.; Agustsdottir, A.B.; Stefansson, O.A.; Ivarsdottir, E.V.; Sigurdsson, J.K.; Benonisdottir, S.; Eyjolfsson, G.I.; et al. Eighty-eight variants highlight the role of T cell regulation and airway remodeling in asthma pathogenesis. Nat. Commun. 2020, 11, 393. [Google Scholar] [CrossRef] [PubMed]
- Gautier, C.; Charpin, D. Environmental triggers and avoidance in the management of asthma. J. Asthma Allergy 2017, 10, 47–56. [Google Scholar] [CrossRef]
- De Benedictis, F.M.; Attanasi, M. Asthma in childhood. Eur. Respir. Rev. 2016, 25, 41–47. [Google Scholar] [CrossRef]
- Fuseini, H.; Newcomb, D.C. Mechanisms Driving Gender Differences in Asthma. Curr. Allergy Asthma Rep. 2017, 17, 19. [Google Scholar] [CrossRef]
- Almqvist, C.; Worm, M.; Leynaert, B. Impact of gender on asthma in childhood and adolescence: A GA 2 LEN review. Allergy 2008, 63, 47–57. [Google Scholar]
- Scherzer, R.; Grayson, M.H. Heterogeneity and the origins of asthma. Ann. Allergy Asthma Immunol. 2018, 121, 400–405. [Google Scholar] [CrossRef]
- Pignataro, F.; Bonini, M.; Forgione, A.; Melandri, S.; Usmani, O. Asthma and gender: The female lung. Pharmacol. Res. 2017, 119, 384–390. [Google Scholar] [CrossRef]
- Matteis, M.; Polverino, F.; Spaziano, G.; Roviezzo, F.; Santoriello, C.; Sullo, N.; Bucci, M.R.; Rossi, F.; Polverino, M.; Owen, C.A.; et al. Effects of sex hormones on bronchial reactivity during the menstrual cycle. BMC Pulm. Med. 2014, 14, 108. [Google Scholar] [CrossRef]
- Kim, Y.I.; Schroeder, J.; Lynch, D.; Newell, J.; Make, B.; Friedlander, A.; Estépar, R.S.; Hanania, N.A.; Washko, G.; Murphy, J.R.; et al. Gender differences of airway dimensions in anatomically matched sites on CT in smokers. COPD 2011, 8, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, M.; Mathis, B. Biologic Treatments for Asthma and Chronic Obstructive Pulmonary Disorder. Allergies 2021, 1, 92–107. [Google Scholar] [CrossRef]
- Athari, S.S. Targeting cell signaling in allergic asthma. Signal Transduct. Target. Ther. 2019, 4, 45. [Google Scholar] [CrossRef]
- Froidure, A.; Mouthuy, J.; Durham, S.R.; Chanez, P.; Sibille, Y.; Pilette, C. Asthma phenotypes and IgE responses. Eur. Respir. J. 2016, 47, 304–319. [Google Scholar] [CrossRef] [PubMed]
- Kato, A.; Hulse, K.; Tan, B.K.; Schleimer, R.P. B-lymphocyte lineage cells and the respiratory system. J. Allergy Clin. Immunol. 2013, 131, 933–957. [Google Scholar] [CrossRef] [PubMed]
- Peebles, R.S. Prostaglandins in asthma and allergic diseases. Pharmacol. Ther. 2018, 193, 1–19. [Google Scholar] [CrossRef]
- Zhao, X.-Y.; Zhao, L.-Y.; Zheng, Q.-S.; Su, J.-L.; Guan, H.; Shang, F.-J. Chymase induces profibrotic response via transforming growth factor-beta 1/Smad activation in rat cardiac fibroblasts. Mol. Cell. Biochem. 2008, 310, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Bergeron, C.; Al-Ramli, W.; Hamid, Q. Remodeling in Asthma. Proc. Am. Thorac. Soc. 2009, 6, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Hough, K.P.; Curtiss, M.L.; Blain, T.J.; Liu, R.-M.; Trevor, J.; Deshane, J.S. Airway Remodeling in Asthma. Front. Med. 2020, 7, 191. [Google Scholar] [CrossRef] [PubMed]
- Guengerich, F.P. Cytochrome P450 research and The Journal of Biological Chemistry. J. Biol. Chem. 2019, 294, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Tyzack, J.D.; Kirchmair, J. Computational methods and tools to predict cytochrome P450 metabolism for drug discovery. Chem. Biol. Drug Des. 2018, 93, 377–386. [Google Scholar] [CrossRef] [PubMed]
- Shakunthala, N. New cytochrome P450 mechanisms: Implications for understanding molecular basis for drug toxicity at the level of the cytochrome. Expert Opin. Drug Metab. Toxicol. 2009, 6, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Gilardi, G.; Di Nardo, G. Heme iron centers in cytochrome P450: Structure and catalytic activity. Rend. Lince 2016, 28, 159–167. [Google Scholar] [CrossRef]
- Rajman, I.; Knapp, L.; Morgan, T.; Masimirembwa, C. African Genetic Diversity: Implications for Cytochrome P450-mediated Drug Metabolism and Drug Development. EBioMedicine 2017, 17, 67–74. [Google Scholar] [CrossRef]
- Esteves, F.; Rueff, J.; Kranendonk, M. The Central Role of Cytochrome P450 in Xenobiotic Metabolism—A Brief Review on a Fascinating Enzyme Family. J. Xenobiot. 2021, 11, 94–114. [Google Scholar] [CrossRef]
- Elfaki, I.; Mir, R.; Almutairi, F.M.; Abu Duhier, F.M. Cytochrome P450: Polymorphisms and Roles in Cancer, Diabetes and Atherosclerosis. Asian Pac. J. Cancer Prev. 2018, 19, 2057–2070. [Google Scholar]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Yiannakopoulou, E.C. Pharmacogenomics of phase II metabolizing enzymes and drug transporters: Clinical implications. Pharm. J. 2012, 13, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Chu, E.K.; Drazen, J.M. Asthma: One hundred years of treatment and onward. Am. J. Respir. Crit. Care Med. 2005, 171, 1202–1208. [Google Scholar] [CrossRef] [PubMed]
- Wiedmann, T.S.; Naqwi, A. Pharmaceutical salts: Theory, use in solid dosage forms and in situ preparation in an aerosol. Asian J. Pharm. Sci. 2016, 11, 722–734. [Google Scholar] [CrossRef]
- Falk, N.P.; Hughes, S.W.; Rodgers, B.C. Medications for Chronic Asthma. Am. Fam. Physician 2016, 94, 454–462. [Google Scholar]
- Müller, V.; Gálffy, G.; Eszes, N.; Losonczy, G.; Bizzi, A.; Nicolini, G.; Chrystyn, H.; Tamási, L. Asthma control in patients receiving inhaled corticosteroid and long-acting beta2-agonist fixed combinations. A real-life study comparing dry powder inhalers and a pressurized metered dose inhaler extrafine formulation. BMC Pulm. Med. 2011, 11, 40. [Google Scholar] [CrossRef]
- Aalbers, R.; Vogelmeier, C.; Kuna, P. Achieving asthma control with ICS/LABA: A review of strategies for asthma management and prevention. Respir. Med. 2015, 111, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.R.; Peters, S.P.; Busse, W.W. Asthma Exacerbations: Pathogenesis, Prevention, and Treatment. J. Allergy Clin. Immunol. Pract. 2017, 5, 918–927. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Theophylline. Am. J. Respir. Crit. Care Med. 2013, 188, 901–906. [Google Scholar] [CrossRef]
- Tamada, T.; Ichinose, M. Leukotriene Receptor Antagonists and Antiallergy Drugs. Handb. Exp. Pharmacol. 2016, 237, 153–169. [Google Scholar]
- Narendra, D.K.; Hanania, N.A. Targeting IL-5 in COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1045–1051. [Google Scholar] [CrossRef]
- Menzella, F.; Lusuardi, M.; Galeone, C.; Facciolongo, N.; Zucchi, L. The clinical profile of benralizumab in the management of severe eosinophilic asthma. Ther. Adv. Respir. Dis. 2016, 10, 534–548. [Google Scholar] [CrossRef]
- Caminati, M.; Menzella, F.; Guidolin, L.; Senna, G. Targeting eosinophils: Severe asthma and beyond. Drugs Context 2019, 8, 212587. [Google Scholar] [CrossRef]
- Okayama, Y.; Matsumoto, H.; Odajima, H.; Takahagi, S.; Hide, M.; Okubo, K. Roles of omalizumab in various allergic diseases. Allergol. Int. 2020, 69, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.M. Clinical Pharmacology of Corticosteroids. Respir. Care 2018, 63, 655–670. [Google Scholar] [CrossRef]
- Lin, S.-C.; Shi, L.-S.; Ye, Y.-L. Advanced Molecular Knowledge of Therapeutic Drugs and Natural Products Focusing on Inflammatory Cytokines in Asthma. Cells 2019, 8, 685. [Google Scholar] [CrossRef]
- Newton, R. Anti-inflammatory glucocorticoids: Changing concepts. Eur. J. Pharmacol. 2014, 724, 231–236. [Google Scholar] [CrossRef]
- Newton, R.; Giembycz, M.A. Understanding how long-acting β2-adrenoceptor agonists enhance the clinical efficacy of inhaled corticosteroids in asthma—An update. Br. J. Pharmacol. 2016, 173, 3405–3430. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.B.; White, A.G.; Scarpati, L.M.; Wan, G.; Nelson, W.W. Long-term Systemic Corticosteroid Exposure: A Systematic Literature Review. Clin. Ther. 2017, 39, 2216–2229. [Google Scholar] [CrossRef] [PubMed]
- Bhalla, R.; Taylor, W.; Jones, A.; Roland, N. The inflammation produced by corticosteroid inhalers in the pharynx in asthmatics. Clin. Otolaryngol. 2008, 33, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Xuan, L.; Cao, S.; Yu, G.; Hou, Q.; Wang, H. Decreased Histone Deacetylase 2 (HDAC2) in Peripheral Blood Monocytes (PBMCs) of COPD Patients. PLoS ONE 2016, 11, e0147380. [Google Scholar] [CrossRef]
- Lai, T.; Wu, M.; Zhang, C.; Che, L.; Xu, F.; Wang, Y.; Wu, Y.; Xuan, N.; Cao, C.; Du, X.; et al. HDAC2 attenuates airway inflammation by suppressing IL-17A production in HDM-challenged mice. Am. J. Physiol. Cell. Mol. Physiol. 2019, 316, L269–L279. [Google Scholar] [CrossRef]
- Barnes, P.J. Histone deacetylase-2 and airway disease. Ther. Adv. Respir. Dis. 2009, 3, 235–243. [Google Scholar] [CrossRef]
- Ito, K.; Yamamura, S.; Essilfie-Quaye, S.; Cosio, B.; Ito, M.; Barnes, P.J.; Adcock, I.M. Histone deacetylase 2-mediated deacetylation of the glucocorticoid receptor enables NF-κB suppression. J. Exp. Med. 2006, 203, 7–13. [Google Scholar] [CrossRef]
- Sevilla, L.M.; Jiménez-Panizo, A.; Alegre-Martí, A.; Estébanez-Perpiñá, E.; Caelles, C.; Pérez, P. Glucocorticoid Resistance: Interference between the Glucocorticoid Receptor and the MAPK Signalling Pathways. Int. J. Mol. Sci. 2021, 22, 10049. [Google Scholar] [CrossRef] [PubMed]
- Wendell, S.G.; Fan, H.; Zhang, C. G Protein–Coupled Receptors in Asthma Therapy: Pharmacology and Drug Action. Pharmacol. Rev. 2019, 72, 1–49. [Google Scholar] [CrossRef] [PubMed]
- Harada, M.; Hirota, T.; Jodo, A.I.; Hitomi, Y.; Sakashita, M.; Tsunoda, T.; Miyagawa, T.; Doi, S.; Kameda, M.; Fujita, K.; et al. Thymic Stromal Lymphopoietin Gene Promoter Polymorphisms Are Associated with Susceptibility to Bronchial Asthma. Am. J. Respir. Cell Mol. Biol. 2011, 44, 787–793. [Google Scholar] [CrossRef]
- Xia, Y.; Kelton, C.M.L.; Xue, L.; Guo, J.J.; Bian, B.; Wigle, P.R. Safety of long-acting beta agonists and inhaled corticosteroids in children and adolescents with asthma. Ther. Adv. Drug Saf. 2013, 4, 254–263. [Google Scholar] [CrossRef] [PubMed]
- Melani, A.S. Long-acting muscarinic antagonists. Expert. Rev. Clin. Pharmacol. 2015, 8, 479–501. [Google Scholar] [CrossRef] [PubMed]
- Yokomizo, T.; Nakamura, M.; Shimizu, T. Leukotriene receptors as potential therapeutic targets. J. Clin. Investig. 2018, 128, 2691–2701. [Google Scholar] [CrossRef] [PubMed]
- Jo-Watanabe, A.; Okuno, T.; Yokomizo, T. The Role of Leukotrienes as Potential Therapeutic Targets in Allergic Disorders. Int. J. Mol. Sci. 2019, 20, 3580. [Google Scholar] [CrossRef] [PubMed]
- Loutsios, C.; Farahi, N.; Porter, L.; Lok, L.S.; Peters, A.M.; Condliffe, A.; Chilvers, E.R. Biomarkers of eosinophilic inflammation in asthma. Expert Rev. Respir. Med. 2014, 8, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Scow, D.T.; Luttermoser, G.K.; Dickerson, K.S. Leukotriene inhibitors in the treatment of allergy and asthma. Am. Fam. Physician 2007, 75, 65–70. [Google Scholar] [PubMed]
- Liu, A.H.; Anderson, W.C.; Dutmer, C.M.; Searing, D.A.; Szefler, S.J. Advances in asthma 2015: Across the lifespan. J. Allergy Clin. Immunol. 2016, 138, 397–404. [Google Scholar] [CrossRef][Green Version]
- McGregor, M.C.; Krings, J.G.; Nair, P.; Castro, M. Role of Biologics in Asthma. Am. J. Respir. Crit. Care Med. 2019, 199, 433–445. [Google Scholar] [CrossRef]
- Hoshino, M.; Ohtawa, J. Effects of Adding Omalizumab, an Anti-Immunoglobulin E Antibody, on Airway Wall Thickening in Asthma. Respiration 2012, 83, 520–528. [Google Scholar] [CrossRef]
- Roth, M.; Tamm, M. The effects of omalizumab on IgE-induced cytokine synthesis by asthmatic airway smooth muscle cells. Ann. Allergy Asthma Immunol. 2010, 104, 152–160. [Google Scholar] [CrossRef]
- Lin, S.-C.; Chou, H.-C.; Chen, C.-M.; Chiang, B.-L. Anti-thymic stromal lymphopoietin antibody suppresses airway remodeling in asthma through reduction of MMP and CTGF. Pediatr. Res. 2019, 86, 181–187. [Google Scholar] [CrossRef]
- Lawrence, M.G.; Steinke, J.W.; Borish, L. Cytokine-targeting biologics for allergic diseases. Ann. Allergy, Asthma Immunol. 2018, 120, 376–381. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; Maspero, J.; Wenzel, S.; Rabe, K.F.; Busse, W.W.; Ford, L.; Sher, L.; Fitzgerald, J.M.; et al. Dupilumab Efficacy and Safety in Moderate-to-Severe Uncontrolled Asthma. N. Engl. J. Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef]
- Thangam, E.B.; Jemima, E.A.; Singh, H.; Baig, M.S.; Khan, M.; Mathias, C.B.; Church, M.K.; Saluja, R. The Role of Histamine and Histamine Receptors in Mast Cell-Mediated Allergy and Inflammation: The Hunt for New Therapeutic Targets. Front. Immunol. 2018, 9, 1873. [Google Scholar] [CrossRef]
- Yamauchi, K.; Ogasawara, M. The Role of Histamine in the Pathophysiology of Asthma and the Clinical Efficacy of Antihistamines in Asthma Therapy. Int. J. Mol. Sci. 2019, 20, 1733. [Google Scholar] [CrossRef]
- Hait, E.J.; McDonald, D.R. Impact of Gastroesophageal Reflux Disease on Mucosal Immunity and Atopic Disorders. Clin. Rev. Allergy Immunol. 2018, 57, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Ates, F.; Vaezi, M.F. Insight Into the Relationship Between Gastroesophageal Reflux Disease and Asthma. Gastroenterol. Hepatol. 2014, 10, 729–736. [Google Scholar]
- Menardo, J.-L.; Horak, F.; Danzig, M.R.; Czarlewski, W. A review of loratadine in the treatment of patients with allergic bronchial asthma. Clin. Ther. 1997, 19, 1278–1293. [Google Scholar] [CrossRef]
- Aaronson, D.W. Evaluation of Cetirizine in Patients with Allergic Rhinitis and Perennial Asthma. Ann. Allergy Asthma Immunol. 1996, 76, 440–446. [Google Scholar] [CrossRef]
- McTavish, D.; Goa, K.L.; Ferrill, M. Terfenadine. An updated review of its pharmacological properties and therapeutic efficacy. Drugs 1990, 39, 552–574. [Google Scholar] [CrossRef]
- Monahan, B.P. Torsades de Pointes Occurring in Association with Terfenadine Use. JAMA 1990, 264, 2788. [Google Scholar] [CrossRef]
- Josefson, D. Hay fever drug to be banned by the FDA. BMJ 1997, 314, 247. [Google Scholar] [CrossRef][Green Version]
- Fergeson, J.E.; Patel, S.S.; Lockey, R.F. Acute asthma, prognosis, and treatment. J. Allergy Clin. Immunol. 2016, 139, 438–447. [Google Scholar] [CrossRef]
- d’Ancona, G.; Kavanagh, J.; Roxas, C.; Green, L.; Fernandes, M.; Thomson, L.; Dhariwal, J.; Nanzer, A.M.; Jackson, D.J.; Kent, B.D. Adherence to corticosteroids and clinical outcomes in mepolizumab therapy for severe asthma. Eur. Respir. J. 2020, 55, 1902259. [Google Scholar] [CrossRef]
- Edris, A.; De Feyter, S.; Maes, T.; Joos, G.; LaHousse, L. Monoclonal antibodies in type 2 asthma: A systematic review and network meta-analysis. Respir. Res. 2019, 20, 179. [Google Scholar] [CrossRef]
- Beasley, R.; Harper, J.; Bird, G.; Dunphy, H.; Semprini, A.; Pavord, I.D.; Papi, A.; Weatherall, M. Dose-response relationship of ICS/fast-onset LABA as reliever therapy in asthma. BMC Pulm. Med. 2019, 19, 264. [Google Scholar] [CrossRef]
- Pauwels, R.A.; Löfdahl, C.G.; Postma, D.S.; Tattersfield, A.E.; O’Byrne, P.; Barnes, P.J.; Ullman, A. Effect of inhaled formoterol and budesonide on exacerbations of asthma. Formoterol and Corticosteroids Establishing Therapy (FACET) International Study Group. N. Engl. J. Med. 1997, 337, 1405–1411. [Google Scholar] [CrossRef]
- Charriot, J.; Maravic, M.; Huguet, M.; Vachier, I.; Suehs, C.; Bourdin, A. “Real-life” management of patients with severe asthma in the biologics era: Can we do better? World Allergy Organ. J. 2021, 14, 100528. [Google Scholar] [CrossRef]
- Boyman, O.; Comte, D.; Spertini, F. Adverse reactions to biologic agents and their medical management. Nat. Rev. Rheumatol. 2014, 10, 612–627. [Google Scholar] [CrossRef]
- Price, D.; Chrystyn, H.; Kaplan, A.; Haughney, J.; Román-Rodríguez, M.; Burden, A.; Chisholm, A.; Hillyer, E.; Von Ziegenweidt, J.; Ali, M.; et al. Effectiveness of Same Versus Mixed Asthma Inhaler Devices: A Retrospective Observational Study in Primary Care. Allergy Asthma Immunol. Res. 2012, 4, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, A.; van Boven, J.F.M. Switching Inhalers: A Practical Approach to Keep on UR RADAR. Pulm. Ther. 2020, 6, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Luczak-Wozniak, K.; Dabrowska, M.; Domagała, I.; Miszczuk, M.; Lubanski, W.; Leszczynski, A.; Krenke, R. Mishandling of pMDI and DPI inhalers in asthma and COPD—Repetitive and non-repetitive errors. Pulm. Pharmacol. Ther. 2018, 51, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Sanaullah, T.; Khan, S.; Masoom, A.; Mandokhail, Z.K.; Sadiqa, A.; Malik, M.I. Inhaler Use Technique in Chronic Obstructive Pulmonary Disease Patients: Errors, Practices and Barriers. Cureus 2020, 12, e10569. [Google Scholar] [CrossRef] [PubMed]
- Usmani, O.S.; Lavorini, F.; Marshall, J.; Dunlop, W.C.N.; Heron, L.; Farrington, E.; Dekhuijzen, R. Critical inhaler errors in asthma and COPD: A systematic review of impact on health outcomes. Respir. Res. 2018, 19, 10. [Google Scholar] [CrossRef]
- Williams, R.O.; Repka, M.; Liu, J. Influence of Propellant Composition on Drug Delivery from a Pressurized Metered-Dose Inhaler. Drug Dev. Ind. Pharm. 1998, 24, 763–770. [Google Scholar] [CrossRef]
- Myrdal, P.B.; Sheth, P.; Stein, S.W. Advances in Metered Dose Inhaler Technology: Formulation Development. AAPS PharmSciTech 2014, 15, 434–455. [Google Scholar] [CrossRef]
- Newman, S.P. Principles of metered-dose inhaler design. Respir. Care 2005, 50, 1177–1190. [Google Scholar]
- Woo, S.-D.; Ye, Y.-M.; Lee, Y.; Lee, S.-H.; Shin, Y.S.; Park, J.H.; Choi, H.; Lee, H.-Y.; Shin, H.-J.; Park, H.-S. Efficacy and Safety of a Pressurized Metered-Dose Inhaler in Older Asthmatics: Comparison to a Dry Powder Inhaler in a 12-Week Randomized Trial. Allergy Asthma Immunol. Res. 2020, 12, 454–466. [Google Scholar] [CrossRef]
- Morais-Almeida, M.; Pité, H.; Cardoso, J.; Costa, R.; Cordeiro, C.M.D.S.R.; Silva, E.; Todo-Bom, A.; Vicente, C.; Marques, J.A. Asthma management with breath-triggered inhalers: Innovation through design. Asthma Res. Pract. 2020, 6, 4. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.L.; Hardwell, A.; McKnight, E.; Holmes, J. Asthma patients’ inability to use a pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma control as defined by the global initiative for asthma (GINA) strategy: A retrospective analysis. Prim. Care Respir. J. 2013, 22, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, W.H.; Sarkis, A.; Aderian, S.S.; Milane, A. Asthma and COPD Patients’ Perception of Appropriate Metered-Dose Inhaler Technique. Dose-Response 2020, 18, 155932582091783. [Google Scholar] [CrossRef]
- Sellers, W.F.S. Asthma pressurised metered dose inhaler performance: Propellant effect studies in delivery systems. Allergy, Asthma Clin. Immunol. 2017, 13, 30. [Google Scholar] [CrossRef] [PubMed]
- Titosky, J.T.; Morin, C.M.; Suderman, J.D.; Olfert, J.S.; Finlay, W.H.; Vehring, R. The Effect of Altitude on Inhaler Performance. J. Pharm. Sci. 2014, 103, 2116–2124. [Google Scholar] [CrossRef] [PubMed]
- Seys, S.F.; Daenen, M.; Dilissen, E.; Van Thienen, R.; Bullens, D.M.A.; Hespel, P.; Dupont, L.J. Effects of high altitude and cold air exposure on airway inflammation in patients with asthma. Thorax 2013, 68, 906–913. [Google Scholar] [CrossRef]
- Berkenfeld, K.; Lamprecht, A.; McConville, J.T. Devices for Dry Powder Drug Delivery to the Lung. AAPS PharmSciTech 2015, 16, 479–490. [Google Scholar] [CrossRef]
- Richter, K. Successful use of DPI systems in asthmatic patients—Key parameters. Respir. Med. 2004, 98, S22–S27. [Google Scholar] [CrossRef] [PubMed]
- Scherließ, R.; Etschmann, C. DPI formulations for high dose applications—Challenges and opportunities. Int. J. Pharm. 2018, 548, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Park, H.-S.; Yoon, D.; Lee, H.Y.; Ban, G.; Ming, S.W.Y.; Jie, J.L.Z.; Carter, V.; Hardjojo, A.; Van Boven, J.F.; Price, D.B. Real-life effectiveness of inhaler device switch from dry powder inhalers to pressurized metered-dose inhalers in patients with asthma treated with ICS/LABA. Respirology 2019, 24, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Young, P.M.; Sung, A.; Traini, D.; Kwok, P.; Chiou, H.; Chan, H.-K. Influence of Humidity on the Electrostatic Charge and Aerosol Performance of Dry Powder Inhaler Carrier based Systems. Pharm. Res. 2007, 24, 963–970. [Google Scholar] [CrossRef]
- Lu, X.-Y.; Chen, L.; Wu, C.; Chan, H.-K.; Freeman, T. The Effects of Relative Humidity on the Flowability and Dispersion Performance of Lactose Mixtures. Materials 2017, 10, 592. [Google Scholar] [CrossRef]
- Ari, A. Jet, Ultrasonic, and Mesh Nebulizers: An Evaluation of Nebulizers for Better Clinical Outcomes. Eurasian J. Pulmonol. 2014, 16, 1–7. [Google Scholar] [CrossRef]
- Melani, A.S. Nebulized Corticosteroids in Asthma and COPD. An Italian Appraisal. Respir. Care 2012, 57, 1161–1174. [Google Scholar] [CrossRef]
- Talwar, D.; Bendre, S. Health-Related Effects of Home Nebulization with Glycopyrronium on Difficult-to-Treat Asthma: Post-Hoc Analyses of an Observational Study. Interact. J. Med. Res. 2020, 9, e17863. [Google Scholar] [CrossRef]
- Posa, D.; Pizzulli, A.; Wagner, P.; Perna, S.; Hofmaier, S.; Matricardi, P.M.; Lau, S. Efficacy and usability of a novel nebulizer targeting both upper and lower airways. Ital. J. Pediatr. 2017, 43, 89. [Google Scholar] [CrossRef] [PubMed]
- Kwok, P.C.L.; McDonnell, A.; Tang, P.; Knight, C.; McKay, E.; Butler, S.P.; Sivarajah, A.; Quinn, R.; Fincher, L.; Browne, E.; et al. In vivo deposition study of a new generation nebuliser utilising hybrid resonant acoustic (HYDRA) technology. Int. J. Pharm. 2020, 580, 119196. [Google Scholar] [CrossRef]
- Moore, R.H. The Use of Inhaler Devices in Children. UpToDate. 2021. Available online: https://www.uptodate.com/contents/the-use-of-inhaler-devices-in-children (accessed on 21 December 2021).
- Beeh, K.M.; Kuna, P.; Viaud, I.; Guasconi, A.; Corradi, M.; Georges, G. Comparison of a dry powder inhaler (DPI) to a pressurized metered-dose inhaler (pMDI) formulation of extra fine beclomethasone dipropionate/formoterol fumarate/glycopyrronium bromide (BDP/FF/GB) in patients with COPD: The TRI-D study. Airw. Pharmacol. Treat. Eur. Respir. Soc. 2020, 56, 3246. [Google Scholar]
- Price, D.; Roche, N.; Virchow, J.C.; Burden, A.; Ali, M.; Chisholm, A.; Lee, A.J.; Hillyer, E.V.; von Ziegenweidt, J. Device type and real-world effectiveness of asthma combination therapy: An observational study. Respir. Med. 2011, 105, 1457–1466. [Google Scholar] [CrossRef] [PubMed]
- Fanta, C.H. Acute Exacerbations of Asthma in Adults: Emergency Department and Inpatient Management. UpToDate. 2021. Available online: https://www.uptodate.com/contents/acute-exacerbations-of-asthma-in-adults-emergency-department-and-inpatient-management (accessed on 21 December 2021).
- Rodrigo, C.; Rodrigo, G. Salbutamol treatment of acute severe asthma in the ED: MDI versus hand-held nebulizer. Am. J. Emerg. Med. 1998, 16, 637–642. [Google Scholar] [CrossRef]
- Cates, C.J.; Welsh, E.J.; Rowe, B.H. Holding chambers (spacers) versus nebulisers for beta-agonist treatment of acute asthma. Cochrane Database Syst. Rev. 2013, 2013, CD000052. [Google Scholar]
- Wheless, J.W.; Phelps, S.J. A Clinician’s Guide to Oral Extended-Release Drug Delivery Systems in Epilepsy. J. Pediatr. Pharmacol. Ther. 2018, 23, 277–292. [Google Scholar] [CrossRef]
- Pierson, W.E.; LaForce, C.F.; Bell, T.D.; MacCosbe, P.E.; Sykes, R.; Tinkelman, D. Long-term, double-blind comparison of controlled-release albuterol versus sustained-release theophylline in adolescents and adults with asthma. J. Allergy Clin. Immunol. 1990, 85, 618–626. [Google Scholar] [CrossRef]
- Benfante, A.; Basile, M.; Battaglia, S.; Spatafora, M.; Scichilone, N. The use of ICS/LABA (extra-fine and non-extra-fine) in elderly asthmatics. Ther. Clin. Risk Manag. 2016, 12, 1553–1562. [Google Scholar] [CrossRef]
- McKeever, T.; Mortimer, K.; Wilson, A.; Walker, S.; Brightling, C.; Skeggs, A.; Pavord, I.; Price, D.; Duley, L.; Thomas, M.; et al. Quadrupling Inhaled Glucocorticoid Dose to Abort Asthma Exacerbations. N. Engl. J. Med. 2018, 378, 902–910. [Google Scholar] [CrossRef]
- Derendorf, H.; Nave, R.; Drollmann, A.; Cerasoli, F.; Wurst, W. Relevance of pharmacokinetics and pharmacodynamics of inhaled corticosteroids to asthma. Eur. Respir. J. 2006, 28, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal Formulations in Clinical Use: An Updated Review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Barenholz, Y. Doxil®—The first FDA-approved nano-drug: Lessons learned. J. Control Release 2012, 160, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Nakamura, H.; Maeda, H. The EPR effect: Unique features of tumor blood vessels for drug delivery, factors involved, and limitations and augmentation of the effect. Adv. Drug Deliv. Rev. 2011, 63, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Kan, S.; Hariyadi, D.M.; Grainge, C.; Knight, D.A.; Bartlett, N.W.; Liang, M. Airway epithelial-targeted nanoparticles for asthma therapy. Am. J. Physiol. Cell. Mol. Physiol. 2020, 318, L500–L509. [Google Scholar] [CrossRef]
- Yang, Z.; Chen, X.; Huang, W.; Wong, B.C.K.; Yin, L.; Wong, Y.F.; Xu, M. Liposomes prolong the therapeutic effect of anti-asthmatic medication via pulmonary delivery. Int. J. Nanomed. 2012, 7, 1139–1148. [Google Scholar] [CrossRef]
- Prishchepa, I.V.; Landyshev, I.S. The effect of the liposomal form of hydrocortisone on the status of cellular and humoral immunity in patients with steroid-dependent bronchial asthma. Ter. Arkh. 1997, 69, 39–42. [Google Scholar]
- Loureiro, J.A.; Andrade, S.; Ramalho, M.J.; Oliveira, N.; Pereira, M.C. The interaction of a β2 adrenoceptor agonist drug with biomimetic cell membrane models: The case of terbutaline sulphate. Life Sci. 2021, 285, 119992. [Google Scholar] [CrossRef]
- Myers, M.A.; Thomas, D.A.; Straub, L.; Soucy, D.W.; Niven, R.W.; Kaltenbach, M.; Hood, C.I.; Schreier, H.; Gonzalez-Rothi, R.J. Pulmonary Effects of Chronic Exposure to Liposome Aerosols in Mice. Exp. Lung Res. 1993, 19, 1–19. [Google Scholar] [CrossRef]
- Dauletbaev, N.; Cammisano, M.; Herscovitch, K.; Lands, L.C. Stimulation of the RIG-I/MAVS Pathway by Polyinosinic:Polycytidylic Acid Upregulates IFN-β in Airway Epithelial Cells with Minimal Costimulation of IL-8. J. Immunol. 2015, 195, 2829–2841. [Google Scholar] [CrossRef]
- Zaboronok, A.; Tsurushima, H.; Yamamoto, T.; Isobe, T.; Takada, K.; Sakae, T.; Yoshida, F.; Matsumura, A. Size-Dependent Radiosensitization Effects of Gold Nanoparticles on Human U251 Malignant Glioma Cells. Nanosci. Nanotechnol. Lett. 2013, 5, 990–994. [Google Scholar] [CrossRef]
- Zaboronok, A.; Taskaev, S.; Volkova, O.; Mechetina, L.; Kasatova, A.; Sycheva, T.; Nakai, K.; Kasatov, D.; Makarov, A.; Kolesnikov, I.; et al. Gold Nanoparticles Permit In Situ Absorbed Dose Evaluation in Boron Neutron Capture Therapy for Malignant Tumors. Pharmaceutics 2021, 13, 1490. [Google Scholar] [CrossRef]
- Omlor, A.J.; Le, D.D.; Schlicker, J.; Hannig, M.; Ewen, R.; Heck, S.; Herr, C.; Kraegeloh, A.; Hein, C.; Kautenburger, R.; et al. Local Effects on Airway Inflammation and Systemic Uptake of 5 nm PEGylated and Citrated Gold Nanoparticles in Asthmatic Mice. Small 2016, 13, 1603070. [Google Scholar] [CrossRef]
- Lee, H.; Jeong, S.W.; Jung, E.; Lee, D. Dexamethasone-loaded H2O2-activatable anti-inflammatory nanoparticles for on-demand therapy of inflammatory respiratory diseases. Nanomed. Nanotechnol. Biol. Med. 2020, 30, 102301. [Google Scholar] [CrossRef]
- Mohamed, S.; Nasr, M.; Salama, A.; Refai, H. Novel lipid–polymer hybrid nanoparticles incorporated in thermosensitive in situ gel for intranasal delivery of terbutaline sulphate. J. Microencapsul. 2020, 37, 577–594. [Google Scholar] [CrossRef]
- Chakraborty, S.; Ehsan, I.; Mukherjee, B.; Mondal, L.; Roy, S.; Das Saha, K.; Paul, B.; Debnath, M.C.; Bera, T. Therapeutic potential of andrographolide-loaded nanoparticles on a murine asthma model. Nanomed. Nanotechnol. Biol. Med. 2019, 20, 102006. [Google Scholar] [CrossRef]
- Morris, A.S.; Sebag, S.C.; Paschke, J.D.; Wongrakpanich, A.; Ebeid, K.; Anderson, M.E.; Grumbach, I.M.; Salem, A.K. Cationic CaMKII Inhibiting Nanoparticles Prevent Allergic Asthma. Mol. Pharm. 2017, 14, 2166–2175. [Google Scholar] [CrossRef]
- Lv, Y.; Zhang, J.; Wang, C. Self-assembled chitosan nanoparticles for intranasal delivery of recombinant protein interleukin-17 receptor C (IL-17RC): Preparation and evaluation in asthma mice. Bioengineered 2021, 12, 3029–3039. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Shi, W.; Wang, H.; Yue, J.; Mao, Y.; Zhou, W.; Kong, X.; Guo, Q.; Zhang, L.; Xu, P.; et al. Anti-ST2 Nanoparticle Alleviates Lung Inflammation by Targeting ILC2s-CD4+T Response. Int. J. Nanomed. 2020, 15, 9745–9758. [Google Scholar] [CrossRef] [PubMed]
- da Silva, A.L.; de Oliveira, G.P.; Kim, N.; Cruz, F.F.; Kitoko, J.Z.; Blanco, N.G. Nanoparticle-based thymulin gene therapy therapeutically reverses key pathology of experimental allergic asthma. Sci. Adv. 2020, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.-Q.; Zhong, J.-W.; Qiu, S.-Y.; Zhi, M.; Yang, L.-Q.; Zhou, Y.-L.; Zhou, F.-X.; Yang, P.-C.; Liu, D.-B.; Mo, L.-H. A20-OVA Nanoparticles Inhibit Allergic Asthma in a Murine Model. Inflammation 2020, 43, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Purghè, B.; Manfredi, M.; Ragnoli, B.; Baldanzi, G.; Malerba, M. Exosomes in chronic respiratory diseases. Biomed. Pharmacother. 2021, 144, 112270. [Google Scholar] [CrossRef] [PubMed]
- Sastre, B.; Cañas, J.A.; Muñoz, J.M.R.; Del Pozo, V. Novel Modulators of Asthma and Allergy: Exosomes and MicroRNAs. Front. Immunol. 2017, 8, 826. [Google Scholar] [CrossRef]
- Fujita, Y.; Yoshioka, Y.; Ito, S.; Araya, J.; Kuwano, K.; Ochiya, T. Intercellular Communication by Extracellular Vesicles and Their MicroRNAs in Asthma. Clin. Ther. 2014, 36, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Wagner, N.; Eberhardt, M.; Vera, J.; Cuomo, F.; Blume, K.; Galster, S.; Achenbach, S.; Laffert, B.; Kahlert, H.; Schuler, G.; et al. Plasma-derived extracellular vesicles discriminate type-1 allergy subjects from non-allergic controls. World Allergy Organ. J. 2021, 14, 100583. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Wang, Y.; Zheng, T.; Pu, Y.; Ma, Y.; Qi, X. Hypoxic hUCMSC-derived extracellular vesicles attenuate allergic airway inflammation and airway remodeling in chronic asthma mice. Stem. Cell. Res. Ther. 2021, 12, 4. [Google Scholar] [CrossRef]
- Ren, J.; Liu, Y.; Yao, Y.; Feng, L.; Zhao, X.; Li, Z.; Yang, L. Intranasal delivery of MSC-derived exosomes attenuates allergic asthma via expanding IL-10 producing lung interstitial macrophages in mice. Int. Immunopharmacol. 2020, 91, 107288. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.B.; Zhang, H.Y.; Wang, C.; He, B.X.; Liu, X.Q.; Meng, X.C.; Peng, Y.Q.; Xu, Z.B.; Fan, X.L.; Wu, Z.J.; et al. Small extracellular vesicles derived from human mesenchymal stromal cells prevent group 2 innate lymphoid cell-dominant allergic airway inflammation through delivery of mir-146a-5p. J. Extracell Vesicles 2020, 9, 1723260. [Google Scholar] [CrossRef]
- Tagalakis, A.D.; McAnulty, R.J.; Devaney, J.; Bottoms, S.E.; Wong, J.B.; Elbs, M.; Writer, M.J.; Hailes, H.; Tabor, A.B.; O’Callaghan, C.; et al. A Receptor-targeted Nanocomplex Vector System Optimized for Respiratory Gene Transfer. Mol. Ther. 2008, 16, 907–915. [Google Scholar] [CrossRef]
- Draijer, C.; Speth, J.; Penke, L.R.K.; Zaslona, Z.; Bazzill, J.D.; Lugogo, N.; Huang, Y.J.; Moon, J.J.; Peters-Golden, M. Resident alveolar macrophage-derived vesicular SOCS3 dampens allergic airway inflammation. FASEB J. 2020, 34, 4718–4731. [Google Scholar] [CrossRef]
- Shang, Y.; Sun, Y.; Xu, J.; Ge, X.; Hu, Z.; Xiao, J. Exosomes from mmu_circ_0001359-Modified ADSCs Attenuate Airway Remodeling by Enhancing FoxO1 Signaling-Mediated M2-like Macrophage Activation. Mol. Ther. Nucleic Acids 2020, 19, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yu, Q.; Zhang, M.; Zhou, Y.; Su, X.; Wu, M.; Lv, J.; Xia, Z. Hemin-primed dendritic cells suppress allergic airway inflammation through releasing extracellular vesicles. J. Leukoc. Biol. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zhuansun, Y.; Du, Y.; Huang, F.; Lin, L.; Chen, R.; Jiang, S.; Li, J. MSCs exosomal miR-1470 promotes the differentiation of CD4+CD25+FOXP3+ Tregs in asthmatic patients by inducing the expression of P27KIP1. Int. Immunopharmacol. 2019, 77, 105981. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, N.; Cheng, Q.; Zhang, H.; Liu, F.; Shang, Y. MiR-21-5p in Macrophage-Derived Exosomes Targets Smad7 to Promote Epithelial Mesenchymal Transition of Airway Epithelial Cells. J. Asthma Allergy 2021, 14, 513–524. [Google Scholar] [CrossRef] [PubMed]
- Carnino, J.M.; Ni, K.; Jin, Y. Extracellular Vesicle-Shuttling MicroRNAs Regulate the Development of Inflammatory Lung Responses. Ann. Pulm. Crit. Care Med. 2018, 1, 1–4. [Google Scholar] [PubMed]
- Cañas, J.A.; Sastre, B.; Rodrigo-Muñoz, J.M.; Fernández-Nieto, M.; Barranco, P.; Quirce, S.; Sastre, J.; del Pozo, V. Eosinophil-derived exosomes contribute to asthma remodelling by activating structural lung cells. Clin. Exp. Allergy 2018, 48, 1173–1185. [Google Scholar] [CrossRef]
- Esser, J.; Gehrmann, U.; D’Alexandri, F.L.; Hidalgo-Estévez, A.M.; Wheelock, C.E.; Scheynius, A.; Gabrielsson, S.; Rådmark, O. Exosomes from human macrophages and dendritic cells contain enzymes for leukotriene biosynthesis and promote granulocyte migration. J. Allergy Clin. Immunol. 2010, 126, 1032–1040.e4. [Google Scholar] [CrossRef]
- Jo, W.; Kim, J.; Yoon, J.; Jeong, D.; Cho, S.; Jeong, H.; Yoon, Y.J.; Kim, S.C.; Gho, Y.S.; Park, J. Large-scale generation of cell-derived nanovesicles. Nanoscale 2014, 6, 12056–12064. [Google Scholar] [CrossRef]
- Jo, W.; Jeong, D.; Kim, J.; Cho, S.; Jang, S.C.; Han, C.; Kang, J.Y.; Gho, Y.S.; Park, J. Microfluidic fabrication of cell-derived nanovesicles as endogenous RNA carriers. Lab Chip 2014, 14, 1261–1269. [Google Scholar] [CrossRef]
- Yoon, J.; Jo, W.; Jeong, D.; Kim, J.; Jeong, H.; Park, J. Generation of nanovesicles with sliced cellular membrane fragments for exogenous material delivery. Biomaterials 2015, 59, 12–20. [Google Scholar] [CrossRef]
- Wang, L.; Feng, M.; Li, Q.; Qiu, C.; Chen, R. Advances in nanotechnology and asthma. Ann. Transl. Med. 2019, 7, 180. [Google Scholar] [CrossRef]
- Yang, B.; Choi, H.; Kim, S.-H.; Yoon, H.J.; Lee, H. How will nanotechnology lead to better control of asthma? Ann. Transl. Med. 2019, 7, 515. [Google Scholar] [CrossRef]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Ferrante, G.; La Grutta, S. The Burden of Pediatric Asthma. Front. Pediatr. 2018, 6, 186. [Google Scholar] [CrossRef] [PubMed]
- Philip, J. The Effects of Inhaled Corticosteroids on Growth in Children. Open Respir. Med. J. 2014, 8, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Maglione, M.; Poeta, M.; Santamaria, F. New Drugs for Pediatric Asthma. Front. Pediatr. 2019, 6, 16. [Google Scholar] [CrossRef] [PubMed]
- Limb, S.L.; Starke, P.R.; Lee, C.E.; Chowdhury, B.A. Delayed onset and protracted progression of anaphylaxis after omalizumab administration in patients with asthma. J. Allergy Clin. Immunol. 2007, 120, 1378–1381. [Google Scholar] [CrossRef]
- Boutopoulou, B.; Koumpagioti, D.; Matziou, V.; Priftis, K.N.; Douros, K. Interventions on Adherence to Treatment in Children with Severe Asthma: A Systematic Review. Front. Pediatr. 2018, 6, 232. [Google Scholar] [CrossRef] [PubMed]
- Allen, H.; Backhouse, S.H.; Hull, J.H.; Price, O.J. Anti-doping Policy, Therapeutic Use Exemption and Medication Use in Athletes with Asthma: A Narrative Review and Critical Appraisal of Current Regulations. Sports Med. 2019, 49, 659–668. [Google Scholar] [CrossRef]
- Fragkaki, A.; Georgakopoulos, C.; Sterk, S.; Nielen, M. Sports doping: Emerging designer and therapeutic β2-agonists. Clin. Chim. Acta 2013, 425, 242–258. [Google Scholar] [CrossRef] [PubMed]
- Prausnitz, M.R.; Langer, R. Transdermal drug delivery. Nat. Biotechnol. 2008, 26, 1261–1268. [Google Scholar] [CrossRef]
- Gross, N.J.; Barnes, P.J. New Therapies for Asthma and Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2017, 195, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Onoue, S.; Matsui, T.; Aoki, Y.; Ishida, H.; Nukaya, H.; Kou, K.; Yamada, S. Self-assembled micellar formulation of chafuroside A with improved anti-inflammatory effects in experimental asthma/COPD-model rats. Eur. J. Pharm. Sci. 2012, 45, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Leung, J.M.; Sin, D.D. Asthma-COPD overlap syndrome: Pathogenesis, clinical features, and therapeutic targets. BMJ 2017, 358, j3772. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Name (Generic) | Drug Type | Benefits | Disadvantages | Representative Clinical Trials |
|---|---|---|---|---|
| Beclomethasone dipropionate [36] | Inhaled corticosteroid | Reduces airway swelling | Dry mouth, irritated throat, voice changes | NCT02040766 NCT03834012 NCT00497237 NCT02513160 |
| Fluticasone propionate [35] | Inhaled corticosteroid | Prevents allergic reactions | Nasal dryness, nausea, vomiting | NCT02175771 NCT02139644 NCT02301975 NCT02980133 |
| Budesonide [37] | Inhaled corticosteroid | Reduces airway swelling | Dysphonia, oropharyngeal candidiasis | NCT01676987 NCT05152355 NCT01070888 NCT00509028 |
| Ciclesonide [35] | Inhaled corticosteroid | Reduces airway swelling | Dysphonia, oropharyngeal candidiasis | NCT03839433 NCT00163293 NCT01455194 NCT00305461 |
| Fluticasone furoate [35] | Inhaled corticosteroid | Reduces airway swelling | Dysphonia, oropharyngeal candidiasis | NCT01159912 NCT02502734 NCT01165138 NCT00649025 |
| Mometasone [35] | Inhaled corticosteroid | Reduces airway swelling | Dysphonia, oropharyngeal candidiasis | NCT00556673 NCT02415179 NCT01555151 NCT01210170 |
| Tiotropium [38] | Long acting muscarinic antagonist | Bronchodilator | Dry mouth, constipation | NCT03964220 NCT00557700 NCT02676089 NCT01340209 NCT00776984 |
| Theophylline [39] | Xanthine Derivative | Relaxes airway muscles | Nausea, abdominal pain, headache, diarrhea | NCT01684683 NCT00119496 NCT00756418 NCT00000578 |
| Salmeterol xinafoate [36] | Long acting beta agonist | Prevents bronchoconstriction | Hives, headache, blurred vision | NCT02260492 NCT03461627 NCT04564456 NCT03535870 |
| Pranlukast hydrate [40] | Leukotriene receptor antagonist | Prevents bronchospasm | Headache, abdominal or stomach pain, cough, dental pain | NCT03826485 |
| Montelukast sodium [40] | Leukotriene receptor antagonist | Prevents bronchospasm | Numbness, pain in the arms or legs, sinus pain | NCT00140881 NCT00157937 NCT00092989 NCT00636207 |
| Mepolizumab [41] | Antibody derivative | Prevents airway swelling | Pain at injection site, headache, rash | NCT02281318 NCT01691521 NCT02555371 NCT02654145 |
| Reslizumab [42] | Antibody derivative | Anti-eosinophilic activity | Pain at injection site, headache | NCT03074942 NCT02452190 NCT00587288 NCT03052725 |
| Benralizumab [43] | Antibody derivative | Anti-eosinophilic activity | Pain at injection site, headache | NCT02322775 NCT02869438 NCT02075255 NCT02814643 |
| Omalizumab [44] | Anti-IgE antibody | Prevents allergic reaction | Itching, bruising, redness, pain, or swelling at the injection site | NCT00314574 NCT01922037 NCT02654145 NCT00046748 |
| Class of Delivery System | Delivery Method | Subtypes | Pros | Cons | Clinical Studies (Representative) |
|---|---|---|---|---|---|
| Propellant-Pressurized Metered Dose Inhalers (pMDI) | -Aerosolization via liquid propellant under pressure -Inhale deeply upon release | -Press-and-inhale -Velocity- modified -Breath-coordinated -Breath-actuated | -Precise and instant delivery -Waterproof -Pressure delivery | -Requires training -May be altitude sensitive -Tank can rupture -Spacer may be needed | NCT02091986 NCT01136382 NCT00746330 NCT01070524 NCT01803087 |
| Dry Powder Inhalers (DPI) | -Metered dispensing -Deep inhale -Breath hold | -Spring-loaded -Multi-dose | -Simple -Refillable -Rapid action -Easy to formulate | -Particle size is not ultrafine -Vulnerable to humidity and electrostatic influence | NCT03478657 NCT02794480 NCT02753712 NCT01191424 NCT02022761 |
| Nebulizers | -Aerosolization of liquid -Normal breathing | -Piezo-electric membrane -Bernoulli gas pressure differential -Ultrafine mesh | -Uses normal breathing pattern -Can mix drugs easily -Can fine tune particle size | -Bulky -Requires continuous pressure or electricity -Extended treatment time | NCT01951378 NCT01045174 NCT01649401 NCT03029156 NCT02774941 |
| Population | Condition | Requirements | Suitable Delivery Methods |
|---|---|---|---|
| Children |
|
|
|
| Athletes |
|
|
|
| Co-Morbid Ex: COPD |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mathis, B.J.; Kusumoto, M.; Zaboronok, A.; Hiramatsu, Y. Packaging and Delivery of Asthma Therapeutics. Pharmaceutics 2022, 14, 92. https://doi.org/10.3390/pharmaceutics14010092
Mathis BJ, Kusumoto M, Zaboronok A, Hiramatsu Y. Packaging and Delivery of Asthma Therapeutics. Pharmaceutics. 2022; 14(1):92. https://doi.org/10.3390/pharmaceutics14010092
Chicago/Turabian StyleMathis, Bryan J., Misa Kusumoto, Alexander Zaboronok, and Yuji Hiramatsu. 2022. "Packaging and Delivery of Asthma Therapeutics" Pharmaceutics 14, no. 1: 92. https://doi.org/10.3390/pharmaceutics14010092
APA StyleMathis, B. J., Kusumoto, M., Zaboronok, A., & Hiramatsu, Y. (2022). Packaging and Delivery of Asthma Therapeutics. Pharmaceutics, 14(1), 92. https://doi.org/10.3390/pharmaceutics14010092