
Optimization and Evaluation of the In Vitro Permeation Parameters of Topical Products with Non-Steroidal Anti-Inflammatory Drugs through Strat-M® Membrane

 ,
,  ,
,
Abstract
1. Introduction
- Develop and validate a single Ultra High Performance Liquid Chromatography (UHPLC) assay applicable to quantify all five NSAIDs (DNa/DEA, ETF, IBU, KTP, NPX) used in the study since we have no found such a method during an extensive literature search;
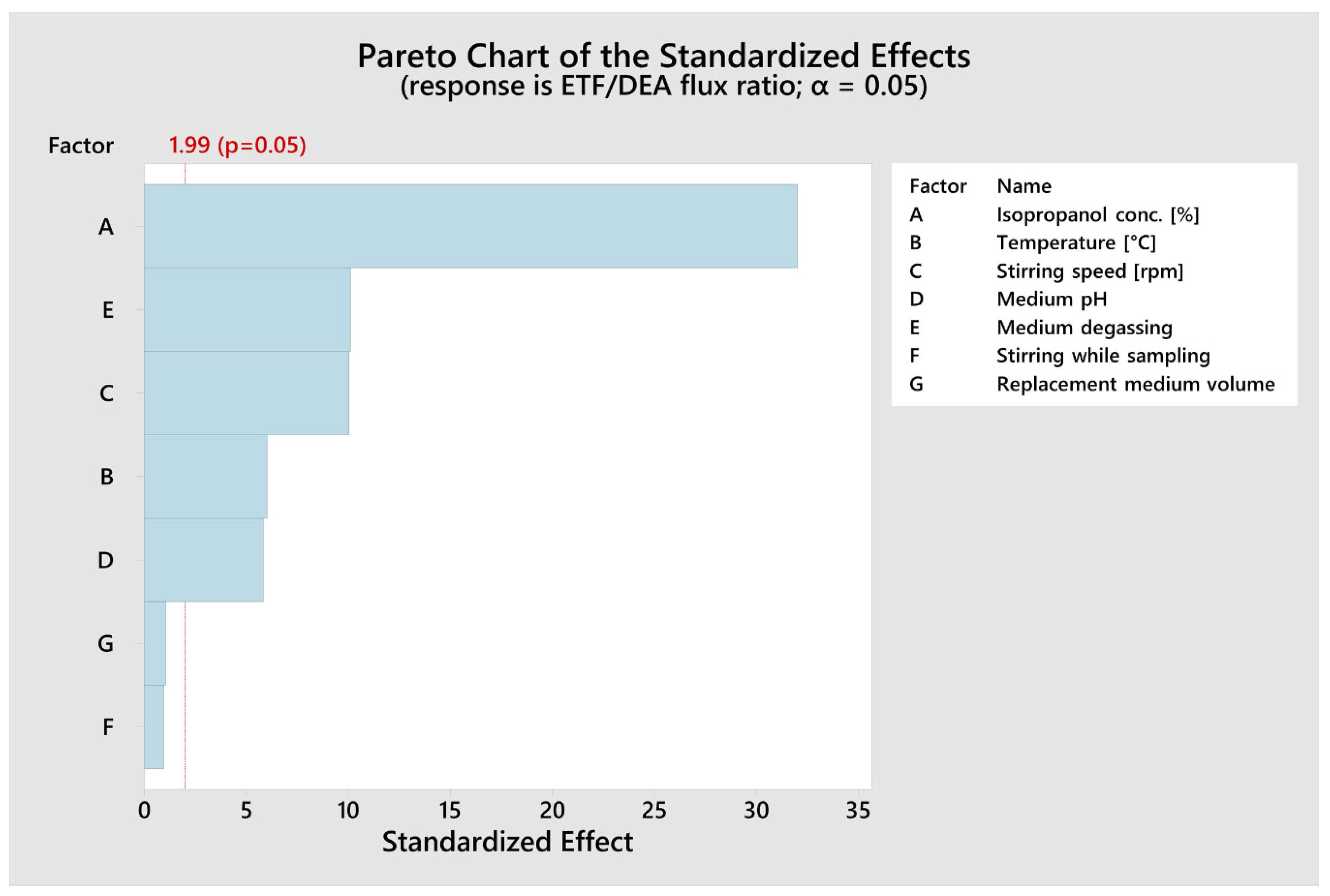
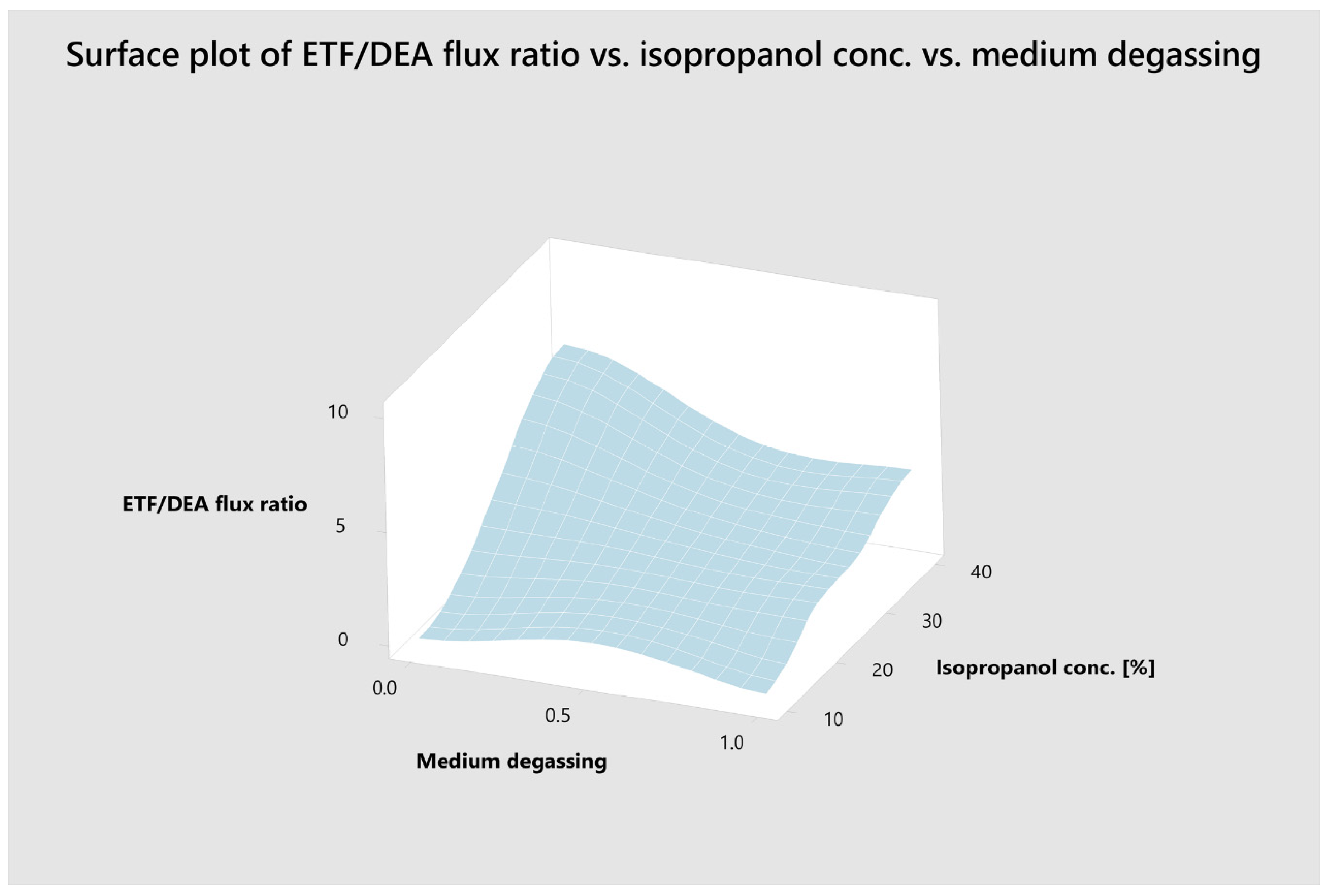
- Optimize the IVPT parameters using an automatic set of vertical Franz diffusion cells and Plackett–Burman factorial design to obtain bio-predictive IVPT based on ETF and DEA permeation across Strat-M® membrane;
- Evaluate NSAIDs’ in vitro permeation parameters (i.a. fluxes) from selected topical products obtained under optimized IVPT conditions.
2. Materials and Methods
2.1. Materials
2.2. PH, Conductivity, and Viscosity Measurements
2.3. In Vitro Permeation Test (IVPT)
2.4. UHPLC Analysis
2.5. Statistical Analysis
3. Results and Discussion
3.1. Characterisation of NSAIDs Formulations
3.2. Quantification of NSAIDs
3.3. Optimization of IVPT Conditions
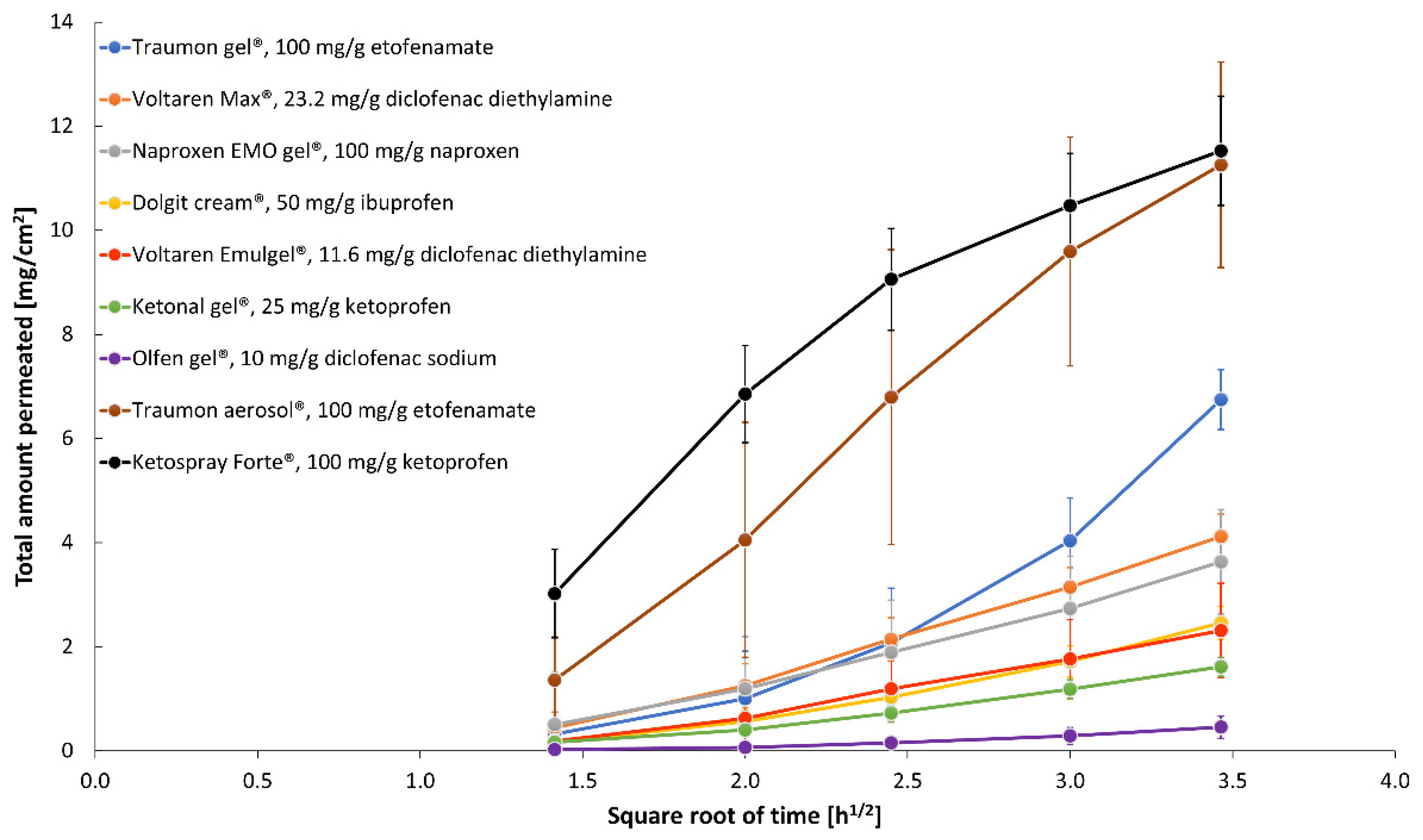
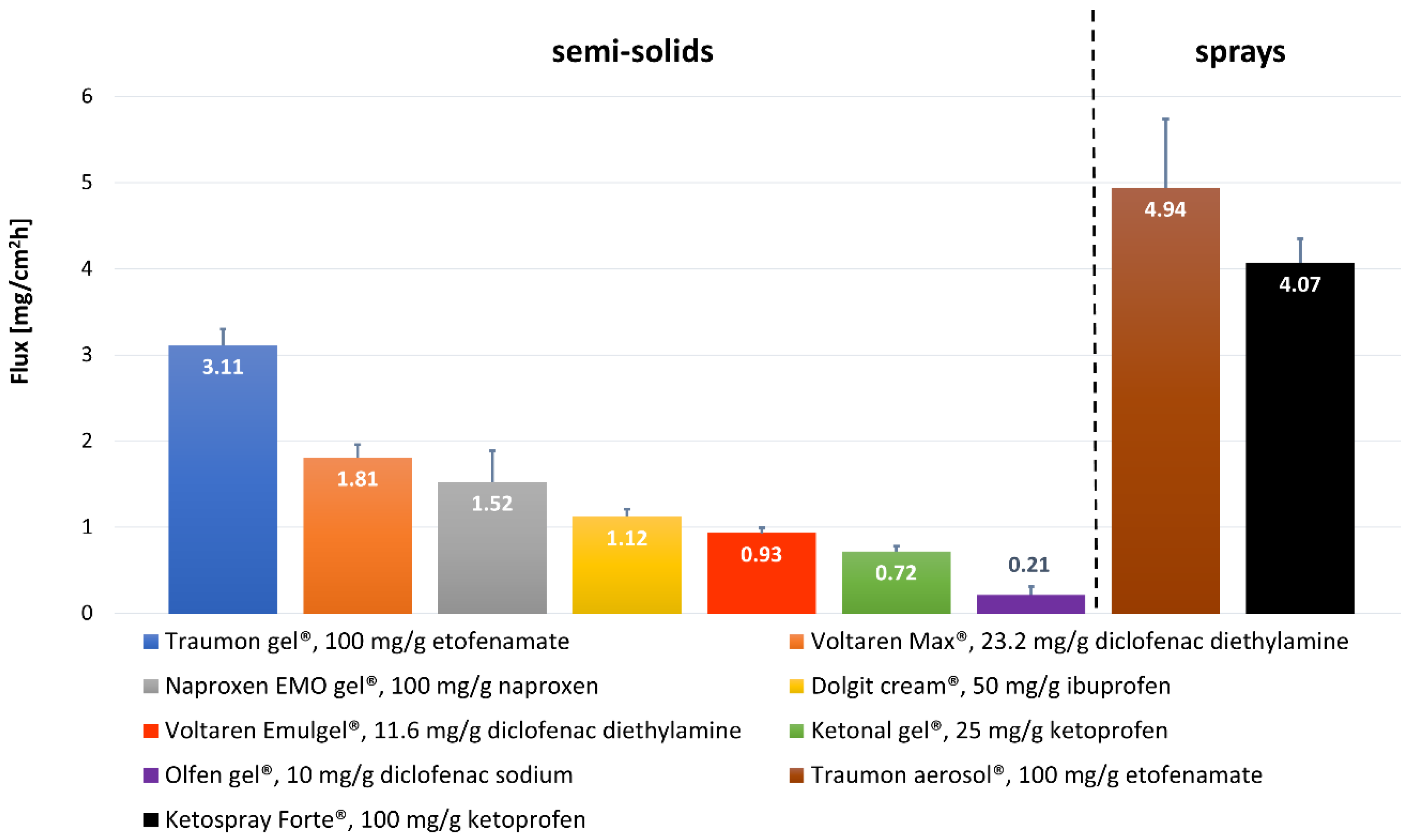
3.4. Comparative Analysis of NSAIDs Permeation under Optimized In Vitro Conditions
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rannou, F.; Pelletier, J.P.; Martel-Pelletier, J. Efficacy and safety of topical NSAIDs in the management of osteoarthritis: Evidence from real-life setting trials and surveys. Semin. Arthritis Rheum. 2016, 45, S18–S21. [Google Scholar] [CrossRef]
- FDA. Guidance for Industry: Nonsterile Semisolid Dosage Forms, Scale-Up and Postapproval Changes: Chemistry, Manufacturing, and Controls; In Vitro Release Testing and In Vivo Bioequivalence Documentation; U.S. Department of Health and Human Services Food and Drug Administration, Center for Drug Evaluation and Research (CDER), Office of Training and Communications Division of Communications Management, The Drug Information Branch: Rockville, MD, USA, 1997; pp. 1–37. [Google Scholar]
- USP43–NF38. General Chapter <1724>: Semisolid Drug Products—Performance Tests; United States Pharmacopoeial Convention, Inc.: Rockville, MD, USA, 2020. [Google Scholar]
- Schmook, F.P.; Meingassner, J.G.; Billich, A. Comparison of human skin or epidermis models with human and animal skin in in-vitro percutaneous absorption. Int. J. Pharm. 2001, 215, 51–56. [Google Scholar] [CrossRef]
- Trauer, S.; Richter, H.; Kuntsche, J.; Buttemeyer, R.; Liebsch, M.; Linscheid, M.; Fahr, A.; Schafer-Korting, M.; Lademann, J.; Patzelt, A. Influence of massage and occlusion on the ex vivo skin penetration of rigid liposomes and invasomes. Eur. J. Pharm. Biopharm. 2014, 86, 301–306. [Google Scholar] [CrossRef]
- Barbero, A.M.; Frasch, H.F. Pig and guinea pig skin as surrogates for human in vitro penetration studies: A quantitative review. Toxicol. In Vitro 2009, 23, 1–13. [Google Scholar] [CrossRef]
- Uchida, T.; Kadhum, W.R.; Kanai, S.; Todo, H.; Oshizaka, T.; Sugibayashi, K. Prediction of skin permeation by chemical compounds using the artificial membrane, Strat-M. Eur. J. Pharm. Sci. 2015, 67, 113–118. [Google Scholar] [CrossRef]
- Sterne, G.D.; Titley, O.G.; Christie, J.L. A qualitative histological assessment of various storage conditions on short term preservation of human split skin grafts. Br. J. Plast. Surg. 2000, 53, 331–336. [Google Scholar] [CrossRef]
- Dancik, Y.; Kichou, H.; Eklouh-Molinier, C.; Soucé, M.; Munnier, E.; Chourpa, I.; Bonnier, F. Freezing Weakens the Barrier Function of Reconstructed Human Epidermis as Evidenced by Raman Spectroscopy and Percutaneous Permeation. Pharmaceutics 2020, 12, 1041. [Google Scholar] [CrossRef] [PubMed]
- Joshi, V.; Brewster, D.; Colonero, P. In vitro diffusion studies in transdermal research: A synthetic membrane model in place of human skin. Drug Dev. Deliv. 2012, 12, 40–42. [Google Scholar]
- Neupane, R.; Boddu, S.H.S.; Renukuntla, J.; Babu, R.J.; Tiwari, A.K. Alternatives to Biological Skin in Permeation Studies: Current Trends and Possibilities. Pharmaceutics 2020, 12, 152. [Google Scholar] [CrossRef] [PubMed]
- Haq, A.; Goodyear, B.; Ameen, D.; Joshi, V.; Michniak-Kohn, B. Strat-M(R) synthetic membrane: Permeability comparison to human cadaver skin. Int. J. Pharm. 2018, 547, 432–437. [Google Scholar] [CrossRef]
- Haq, A.; Dorrani, M.; Goodyear, B.; Joshi, V.; Michniak-Kohn, B. Membrane properties for permeability testing: Skin versus synthetic membranes. Int. J. Pharm. 2018, 539, 58–64. [Google Scholar] [CrossRef]
- Kaur, L.; Singh, K.; Paul, S.; Singh, S.; Singh, S.; Jain, S.K. A Mechanistic Study to Determine the Structural Similarities Between Artificial Membrane Strat-M™ and Biological Membranes and Its Application to Carry Out Skin Permeation Study of Amphotericin B Nanoformulations. AAPS PharmSciTech 2018, 19, 1606–1624. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, L.A.; Kamal, N.; Elfakhri, K.H.; Ibrahim, S.; Ashraf, M.; Zidan, A.S. Application of synthetic membranes in establishing bio-predictive IVPT for testosterone transdermal gel. Int. J. Pharm. 2020, 586, 119572. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.F.; Rouse, J.J.; Sanderson, F.D.; Meidan, V.; Eccleston, G.M. Validation of a static Franz diffusion cell system for in vitro permeation studies. AAPS PharmSciTech 2010, 11, 1432–1441. [Google Scholar] [CrossRef] [PubMed]
- Plackett, R.L.; Burman, J.P. The design of optimum multifactorial experiments. Biometrika 1946, 33, 305–325. [Google Scholar] [CrossRef]
- Ebrahimi-Najafabadi, H.; Leardi, R.; Jalali-Heravi, M. Experimental design in analytical chemistry—Part I: Theory. J. Aoac. Int. 2014, 97, 3–11. [Google Scholar] [CrossRef]
- Hibbert, D.B. Experimental design in chromatography: A tutorial review. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2012, 910, 2–13. [Google Scholar] [CrossRef]
- Sahu, P.K.; Ramisetti, N.R.; Cecchi, T.; Swain, S.; Patro, C.S.; Panda, J. An overview of experimental designs in HPLC method development and validation. J. Pharmaceut. Biomed. 2018, 147, 590–611. [Google Scholar] [CrossRef]
- ICH Harmonised Tripartite Guideline. Validation of Analytical Procedures: Text and Methodology Q2(R1). In Proceedings of the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use, Geneva, Switzerland, 2 June 2014; pp. 1–13.
- Zhang, Y.; Huo, M.; Zhou, J.; Zou, A.; Li, W.; Yao, C.; Xie, S. DDSolver: An add-in program for modeling and comparison of drug dissolution profiles. AAPS J. 2010, 12, 263–271. [Google Scholar] [CrossRef]
- Pradal, J.; Vallet, C.M.; Frappin, G.; Bariguian, F.; Lombardi, M.S. Importance of the formulation in the skin delivery of topical diclofenac: Not all topical diclofenac formulations are the same. J. Pain Res. 2019, 12, 1149–1154. [Google Scholar] [CrossRef]
- Marto, J.; Baltazar, D.; Duarte, A.; Fernandes, A.; Gouveia, L.; Militao, M.; Salgado, A.; Simoes, S.; Oliveira, E.; Ribeiro, H.M. Topical gels of etofenamate: In vitro and in vivo evaluation. Pharm. Dev. Technol. 2015, 20, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Binder, L.; Mazál, J.; Petz, R.; Klang, V.; Valenta, C. The role of viscosity on skin penetration from cellulose ether-based hydrogels. Skin Res. Technol. 2019, 25, 725–734. [Google Scholar] [CrossRef]
- Sanna, V.; Peana, A.T.; Moretti, M.D. Effect of vehicle on diclofenac sodium permeation from new topical formulations: In vitro and in vivo studies. Curr. Drug Deliv. 2009, 6, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Peraman, R.; Nayakanti, D.; Dugga, H.H.; Kodikonda, S. Development and Validation of a Stability-Indicating Assay of Etofenamate by RP-HPLC and Characterization of Degradation Products. Sci. Pharm. 2013, 81, 1017–1028. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bhattacharya, S.S.; Banerjee, S.; Ghosh, A.K.; Chattopadhyay, P.; Verma, A.; Ghosh, A. A RP-HPLC method for quantification of diclofenac sodium released from biological macromolecules. Int. J. Biol. Macromol. 2013, 58, 354–359. [Google Scholar] [CrossRef]
- Hamed, R.; Basil, M.; AlBaraghthi, T.; Sunoqrot, S.; Tarawneh, O. Nanoemulsion-based gel formulation of diclofenac diethylamine: Design, optimization, rheological behavior and in vitro diffusion studies. Pharm. Dev. Technol. 2016, 21, 980–989. [Google Scholar] [CrossRef]
- Naik, P.; Shah, S.; Heaney, J.; Hanson, R.; Nagarsenker, M. Influence of Test Parameters on Release Rate of Hydrocortisone from Cream: Study Using Vertical Diffusion Cell. Dissolut. Technol. 2016, 23, 14–20. [Google Scholar] [CrossRef]
- Sheshala, R.; Anuar, N.K.; Abu Samah, N.H.; Wong, T.W. In Vitro Drug Dissolution/Permeation Testing of Nanocarriers for Skin Application: A Comprehensive Review. AAPS PharmSciTech 2019, 20, 164. [Google Scholar] [CrossRef]
- Marinho, O.D.S.; Pereira, A. Clinical Efficacy and Safety Profile of Topical Etofenamate in the Treatment of Patients with Musculoskeletal Disorders: A Systematic Review. Pain Ther. 2020, 9, 393–410. [Google Scholar] [CrossRef] [PubMed]
- Arce, F.J.; Asano, N.; See, G.L.; Itakura, S.; Todo, H.; Sugibayashi, K. Usefulness of Artificial Membrane, Strat-M®, in the Assessment of Drug Permeation from Complex Vehicles in Finite Dose Conditions. Pharmaceutics 2020, 12, 173. [Google Scholar] [CrossRef]
- Karadzovska, D.; Riviere, J.E. Assessing vehicle effects on skin absorption using artificial membrane assays. Eur. J. Pharm. Sci. 2013, 50, 569–576. [Google Scholar] [CrossRef]
- Walker, R.B.; Smith, E.W. The role of percutaneous penetration enhancers. Adv. Drug Deliv. Rev. 1996, 18, 295–301. [Google Scholar] [CrossRef]
- Hadgraft, J. Skin, the final frontier. Int. J. Pharm. 2001, 224, 1–18. [Google Scholar] [CrossRef]
- Klein, R.; Heckart, J.; Thakker, K. In Vitro Release Testing Methodology and Variability with the Vertical Diffusion Cell (VDC). Dissolut. Technol. 2018, 25, 52–61. [Google Scholar] [CrossRef]
- Klein, S. Influence of different test parameters on in vitro drug release from topical diclofenac formulations in a vertical diffusion cell setup. Pharmazie 2013, 68, 565–571. [Google Scholar]
- Thomas, S.; Shin, S.H.; Hammell, D.C.; Hassan, H.E.; Stinchcomb, A.L. Effect of Controlled Heat Application on Topical Diclofenac Formulations Evaluated by In Vitro Permeation Tests (IVPT) Using Porcine and Human Skin. Pharm. Res. 2020, 37, 49. [Google Scholar] [CrossRef] [PubMed]
- Haltner-Ukomadu, E.; Sacha, M.; Richter, A.; Hussein, K. Hydrogel increases diclofenac skin permeation and absorption. Biopharm. Drug Dispos. 2019, 40, 217–224. [Google Scholar] [CrossRef]
- Hadgraft, J.; Whitefield, M.; Rosher, P.H. Skin penetration of topical formulations of ibuprofen 5%: An in vitro comparative study. Skin Pharmacol. Appl. Skin Physiol. 2003, 16, 137–142. [Google Scholar] [CrossRef]
- Bolla, P.K.; Clark, B.A.; Juluri, A.; Cheruvu, H.S.; Renukuntla, J. Evaluation of Formulation Parameters on Permeation of Ibuprofen from Topical Formulations Using Strat-M® Membrane. Pharmaceutics 2020, 12, 151. [Google Scholar] [CrossRef]
- Sacha, M.; Faucon, L.; Hamon, E.; Ly, I.; Haltner-Ukomadu, E. Ex vivo transdermal absorption of a liposome formulation of diclofenac. Biomed. Pharmacother. 2019, 111, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Minghetti, P.; Cilurzo, F.; Casiraghi, A.; Montanari, L.; Fini, A. Ex Vivo Study of Transdermal Permeation of Four Diclofenac Salts from Different Vehicles. J. Pharm. Sci. 2007, 96, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Benbow, T.; Campbell, J. Microemulsions as transdermal drug delivery systems for nonsteroidal anti-inflammatory drugs (NSAIDs): A literature review. Drug Dev. Ind. Pharm. 2019, 45, 1849–1855. [Google Scholar] [CrossRef]
- Andega, S.; Kanikkannan, N.; Singh, M. Comparison of the effect of fatty alcohols on the permeation of melatonin between porcine and human skin. J. Control. Release 2001, 77, 17–25. [Google Scholar] [CrossRef]
- Pradal, J. Comparison of Skin Permeation and Putative Anti-Inflammatory Activity of Commercially Available Topical Products Containing Ibuprofen and Diclofenac. J. Pain Res. 2020, 13, 2805–2814. [Google Scholar] [CrossRef] [PubMed]
- Kopečná, M.; Kováčik, A.; Novák, P.; Boncheva Bettex, M.; Vávrová, K. Transdermal Permeation and Skin Retention of Diclofenac and Etofenamate/Flufenamic Acid From Over-the-Counter Pain Relief Products. J. Pharm. Sci. 2021, 110, 2517–2523. [Google Scholar] [CrossRef] [PubMed]
- Osmalek, T.; Milanowski, B.; Froelich, A.; Gorska, S.; Bialas, W.; Szybowicz, M.; Kapela, M. Novel organogels for topical delivery of naproxen: Design, physicochemical characteristics and in vitro drug permeation. Pharm. Dev. Technol. 2017, 22, 521–536. [Google Scholar] [CrossRef]
- Brain, K.R.; Green, D.M.; Dykes, P.J.; Marks, R.; Bola, T.S. The role of menthol in skin penetration from topical formulations of ibuprofen 5% in vivo. Skin Pharmacol. Physiol. 2006, 19, 17–21. [Google Scholar] [CrossRef]
- Salamanca, C.H.; Barrera-Ocampo, A.; Lasso, J.C.; Camacho, N.; Yarce, C.J. Franz Diffusion Cell Approach for Pre-Formulation Characterisation of Ketoprofen Semi-Solid Dosage Forms. Pharmaceutics 2018, 10, 148. [Google Scholar] [CrossRef]
- Chantasart, D.; Chootanasoontorn, S.; Suksiriworapong, J.; Kevin Li, S. Investigation of pH Influence on Skin Permeation Behavior of Weak Acids Using Nonsteroidal Anti-Inflammatory Drugs. J. Pharm. Sci. 2015, 104, 3459–3470. [Google Scholar] [CrossRef]
- Baert, B.; Annavarapu, S.; Burvenich, C.; De Spiegeleer, B. Analytical, biopharmaceutical and regulatory evaluation of topical testosterone preparations. Eur. J. Pharm. Biopharm. 2009, 72, 275–281. [Google Scholar] [CrossRef]
- Takahashi, K.; Sakano, H.; Numata, N.; Kuroda, S.; Mizuno, N. Effect of Fatty Acid Diesters on Permeation of Anti-Inflammatory Drugs Through Rat Skin. Drug Dev. Ind. Pharm. 2002, 28, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Haroutiunian, S.; Drennan, D.A.; Lipman, A.G. Topical NSAID Therapy for Musculoskeletal Pain. Pain Med. 2010, 11, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Graham, G.G. Fenamates. In Compendium of Inflammatory Diseases; Parnham, M.J., Ed.; Springer: Basel, Switzerland, 2016; pp. 477–482. [Google Scholar] [CrossRef]
- Drago, S.; Imboden, R.; Schlatter, P.; Buylaert, M.; Krahenbuhl, S.; Drewe, J. Pharmacokinetics of Transdermal Etofenamate and Diclofenac in Healthy Volunteers. Basic Clin. Pharmacol. Toxicol. 2017, 121, 423–429. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Commercial Name and Batch Number (Type of Formulation) | Drug and Its Concentration (mg/g) | Excipients (from Manufacturer’s Label) | pH Mean ± SD (n = 4) | Conductivity (mS/m) Mean ± SD (n = 4) | Viscosity (mPa·s) Mean ± SD (n = 4) | |
|---|---|---|---|---|---|---|
| 10 rpm | 75 rpm | |||||
| Dolgit®, Lot: 811007, (cream) | Ibuprofen (IBU), 50 | Methyl 4-hydroxybenzoate sodium, medium-chain triglycerides, glycerol monostearate, polyoxyethylene 30 stearate, polyoxyethylene 100 stearate, propylene glycol, xanthan gum, lavender oil, orange oil, purified water | 5.99 ± 0.05 | 15.57 ± 0.18 | 32,567 ± 1097 | 7397 ± 55 |
| Ketonal®, Lot: JE4531, (gel) | Ketoprofen (KTP), 25 | Carbomer, triethanolamine, lavender essential oil, ethanol 96%, purified water | 6.31 ± 0.08 | 210.45 ± 2.90 | 54,367 ± 1801 | 11,311 ± 328 |
| Naproxen EMO, Lot: 81671, (gel) | Naproxen (NPX), 100 | Chloralhydrate, levomenthol, ethanol 96%, ethyl p-hydroxybenzoate, sodium hydroxide, carbomer, purified water | 7.48 ± 0.08 | 1049.50 ± 4.95 | 62,233 ± 1290 | 12,851 ± 311 |
| Olfen®, Lot: T26318A, (gel) | Diclofenac sodium (DNa), 10 | Isopropyl adipinate, lactic acid, isopropyl alcohol, sodium pyrosulphite, hydroxypropylcellulose, hydroxyethylcellulose, purified water | 6.13 ± 0.02 | 63.28 ± 0.62 | 26,733 ± 2003 | 6933 ± 127 |
| Traumon®, Lot: 3832641, (gel) | Etofenamate (ETF), 100 | Carbomer, fatty alcohol-polyglycol-ether, sodium hydroxide, isopropyl alcohol, macrogol 400, propylene glycol, purified water | 5.15 ± 0.05 | 10.90 ± 0.02 | 62,567 ± 1060 | 13,005 ± 100 |
| Voltaren® Emulgel®, Lot: 2G3R, (emulsion gel) | Diclofenac diethylamine (DEA), 11.6 (equivalent to 10 mg/g diclofenac sodium) | Carbomer, cocoyl caprylocaprate, diethylamine, isopropyl alcohol, liquid paraffin, macrogol cetostearyl ether, perfume, propylene glycol, purified water | 7.41 ± 0.04 | 140.10 ± 0.57 | 30,633 ± 513 | 7623 ± 110 |
| Voltaren® Max, Lot: 876D, (emulsion gel) | Diclofenac diethylamine (DEA), 23.2 (equivalent to 20 mg/g diclofenac sodium) | Butylhydroxytoluene, carbomer, cocoyl caprylocaprate, diethylamine, isopropyl alcohol, liquid paraffin, macrogol cetostearyl ether, oleyl alcohol, perfume, propylene glycol, purified water | 7.45 ± 0.02 | 195.40 ± 1.56 | 30,167 ± 153 | 6670 ± 437 |
| Ketospray® forte, Lot: 216554-21, (topical spray, solution) | Ketoprofen (KTP), 100 | Propylene glycol, isopropyl alcohol, soya lecithin, ethanol, sodium dihydrogen phosphate dihydrate, disodium phosphate dodecahydrate, sodium hydroxide, peppermint oil, purified water | 7.22 ± 0.02 | 806.15 ± 1.77 | n/a | n/a |
| Traumon® aerosol, Lot: 3823121, (topical spray, solution) | Etofenamate (ETF), 100 | Diisopropyl adipate, fatty alcohol-polyglycol-ether, macrogol 400, isopropyl alcohol, propylene glycol, purified water | 6.45 ± 0.13 | 1.66 ± 0.01 | n/a | n/a |
| Exp. No. | Factors with Levels | Responses Mean ± SD (n = 3) | Fluxes Comparison | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Isopropanol Conc. (%) | Temp. (°C) | Stirring Speed (rpm) | Medium pH | Medium Degassing | Stirring While Sampling | Replacement Medium Volume (mL) | ETF Flux (µg/cm2h) | DEA Flux (µg/cm2h) | ETF/DEA Flux Ratio Value | |
| 1 | 10 | 32 | 600 | 7.4 | yes | yes | 1 | 30 ± 5 | 416 ± 40 | 0.07 ± 0.01 |
| 2 | 10 | 32 | 1000 | 7.4 | no | no | 2 | 53 ± 7 | 518 ± 43 | 0.10 ± 0.01 |
| 3 | 10 | 37 | 600 | 5.8 | yes | no | 2 | 50 ± 4 | 436 ± 72 | 0.12 ± 0.02 |
| 4 | 10 | 37 | 1000 | 5.8 | no | yes | 1 | 59 ± 3 | 518 ± 12 | 0.11 ± 0.01 |
| 5 (C) | 25 | 34.5 | 800 | 6.6 | no/yes a | no/yes b | 1.5 | 1014 ± 164 | 528 ± 32 | 1.92 ± 0.29 |
| 6 | 40 | 32 | 600 | 5.8 | no | yes | 2 | 3976 ± 256 | 690 ± 76 | 5.82 ± 0.64 |
| 7 | 40 | 32 | 1000 | 5.8 | yes | no | 1 | 1614 ± 56 | 674 ± 63 | 2.41 ± 0.21 |
| 8 | 40 | 37 | 600 | 7.4 | no | no | 1 | 3015 ± 688 | 414 ± 42 | 7.32 ± 1.58 |
| 9 | 40 | 37 | 1000 | 7.4 | yes | yes | 2 | 2824 ± 630 | 623 ± 18 | 4.54 ± 0.88 |
| Source | DF | Adj. SS | Adj. MS | F-Value | p-Value Prob > F |
|---|---|---|---|---|---|
| Model | 8 | 555.532 | 69.441 | 163.44 | <0.001 |
| Linear | 7 | 552.311 | 78.902 | 185.70 | <0.001 |
| Isopropanol Conc. (%) | 1 | 435.510 | 435.510 | 1025.01 | <0.001 |
| Temperature (°C) | 1 | 15.368 | 15.368 | 36.17 | <0.001 |
| Stirring Speed (rpm) | 1 | 42.711 | 42.711 | 100.52 | <0.001 |
| Medium pH | 1 | 14.470 | 14.470 | 34.06 | <0.001 |
| Medium Degassing | 1 | 43.394 | 43.394 | 102.13 | <0.001 |
| Stirring While Sampling | 1 | 0.384 | 0.384 | 0.90 | 0.345 |
| Replacement Medium Volume (mL) | 1 | 0.474 | 0.474 | 1.12 | 0.294 |
| Curvature | 1 | 0.031 | 0.031 | 0.07 | 0.788 |
| Error | 72 | 30.592 | 0.425 | ||
| Total | 80 | 586.123 |
| Commercial Formulation (API) | Drug Flux (Jss) (mg/cm2h) | Determination Coefficient (R2) | Permeability Coefficient (KP) (cm/h) | Total Amount Permeated at 12 h (AQ12 h) (mg/cm2) |
|---|---|---|---|---|
| Dolgit® cream 5% (IBU) | 1.12 ± 0.09 | 0.9735 ± 0.0095 | (2.24± 0.18) × 10−2 | 2.45 ± 0.31 |
| Ketonal® gel 2.5% (KTP) | 0.72 ± 0.06 | 0.9767 ± 0.0093 | (2.88 ± 0.25) × 10−2 | 1.61 ± 0.18 |
| Naproxen EMO gel 10% (NPX) | 1.52 ± 0.36 | 0.9878 ± 0.0070 | (1.52 ± 0.36) × 10−2 | 3.63 ± 0.85 |
| Olfen® gel 1% (DNa) | 0.21 ± 0.10 | 0.9272 ± 0.0309 | (2.11 ± 0.98) × 10−2 | 0.45 ± 0.22 |
| Traumon® gel 10% (ETF) | 3.11 ± 0.19 | 0.9110 ± 0.0532 | (3.11 ± 0.19) × 10−2 | 6.75 ± 0.58 |
| Voltaren® Emulgel® 1.16% (DEA) | 0.93 ± 0.06 | 0.9887 ± 0.0053 | (9.32 ± 0.61) × 10−2 | 2.31 ± 0.91 |
| Voltaren® Max 2.32% (DEA) | 1.81 ± 0.15 | 0.9921 ± 0.0079 | (9.05 ± 0.75) × 10−2 | 4.12 ± 0.43 |
| Ketospray ® 10% (KTP) | 4.07 ± 0.28 | 0.9378 ± 0.0343 | (4.07 ± 0.28) × 10−2 | 11.53 ± 1.05 |
| Traumon® aerosol 10% (ETF) | 4.94 ± 0.80 | 0.9463 ± 0.0428 | (4.94 ± 0.80) × 10−2 | 11.26 ± 1.97 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milanowski, B.; Wosicka-Frąckowiak, H.; Główka, E.; Sosnowska, M.; Woźny, S.; Stachowiak, F.; Suchenek, A.; Wilkowski, D. Optimization and Evaluation of the In Vitro Permeation Parameters of Topical Products with Non-Steroidal Anti-Inflammatory Drugs through Strat-M® Membrane. Pharmaceutics 2021, 13, 1305. https://doi.org/10.3390/pharmaceutics13081305
Milanowski B, Wosicka-Frąckowiak H, Główka E, Sosnowska M, Woźny S, Stachowiak F, Suchenek A, Wilkowski D. Optimization and Evaluation of the In Vitro Permeation Parameters of Topical Products with Non-Steroidal Anti-Inflammatory Drugs through Strat-M® Membrane. Pharmaceutics. 2021; 13(8):1305. https://doi.org/10.3390/pharmaceutics13081305
Chicago/Turabian StyleMilanowski, Bartłomiej, Hanna Wosicka-Frąckowiak, Eliza Główka, Małgorzata Sosnowska, Stanisław Woźny, Filip Stachowiak, Angelika Suchenek, and Dariusz Wilkowski. 2021. "Optimization and Evaluation of the In Vitro Permeation Parameters of Topical Products with Non-Steroidal Anti-Inflammatory Drugs through Strat-M® Membrane" Pharmaceutics 13, no. 8: 1305. https://doi.org/10.3390/pharmaceutics13081305
APA StyleMilanowski, B., Wosicka-Frąckowiak, H., Główka, E., Sosnowska, M., Woźny, S., Stachowiak, F., Suchenek, A., & Wilkowski, D. (2021). Optimization and Evaluation of the In Vitro Permeation Parameters of Topical Products with Non-Steroidal Anti-Inflammatory Drugs through Strat-M® Membrane. Pharmaceutics, 13(8), 1305. https://doi.org/10.3390/pharmaceutics13081305