
Development of a Biphasic-Release Multiple-Unit Pellet System with Diclofenac Sodium Using Novel Calcium Phosphate-Based Starter Pellets

 ,
, 

 , , , , , and
, , , , , and
Abstract

1. Introduction
2. Materials and Methods
2.1. Preparation of Multiple-Unit Diclofenac Sodium Capsules
2.2. Characterization of Starter and Drug-Layered Pellets
2.3. Scanning Electron Microscopy and Raman Imaging
2.4. Dissolution Tests (Modified Compendial Methods)
2.5. Dissolution under Conditions Simulating pH Changes in Fasted and Fed States
- (A)
- Simulation of fasted state:
- 120 min in 0.1 M hydrochloric acid pH 1.0 at 15 dpm;
- 20 min in 0.05 M phosphate buffer solution pH 5.6 at 15 dpm;
- 100 min in 0.05 M phosphate buffer solution pH 6.8 at 15 dpm;
- 1080 min in 0.05 M phosphate buffer solution pH 6.8 at 10 dpm;
- (B)
- Simulation of fed state:
- 30 min in 0.05 M phosphate buffer solution pH 4.5 at 8 dpm;
- 60 min in 0.05 M phosphate buffer solution pH 3.5 at 8 dpm;
- 150 min in 0.01 M hydrochloric acid pH 2.0 at 15 dpm;
- 30 min in 0.05 M phosphate buffer solution pH 5.6 at 15 dpm;
- 330 min in 0.05 M phosphate buffer solution pH 6.8 at 15 dpm;
- 840 min in 0.05 M phosphate buffer solution pH 6.8 at 10 dpm.
3. Results
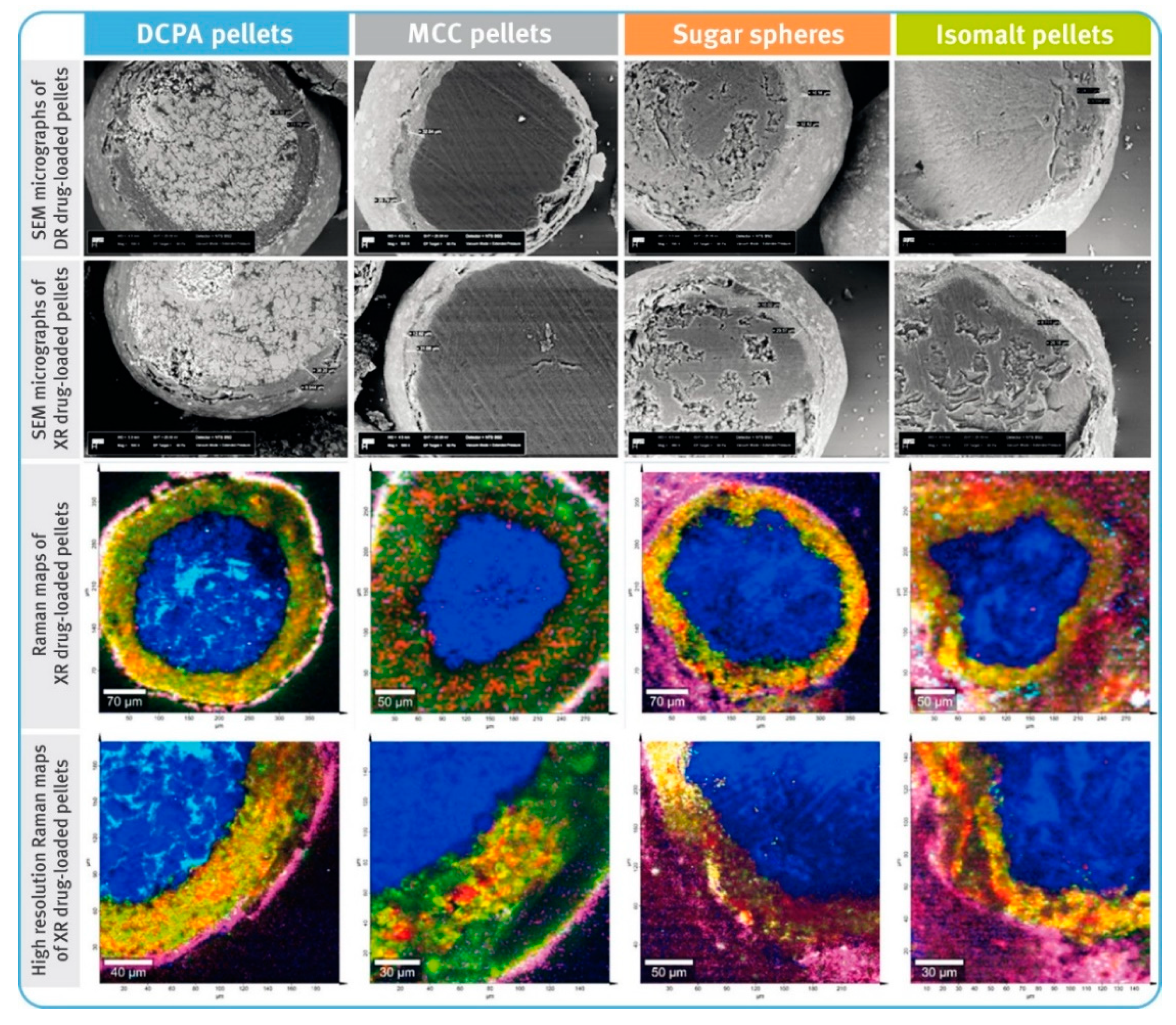
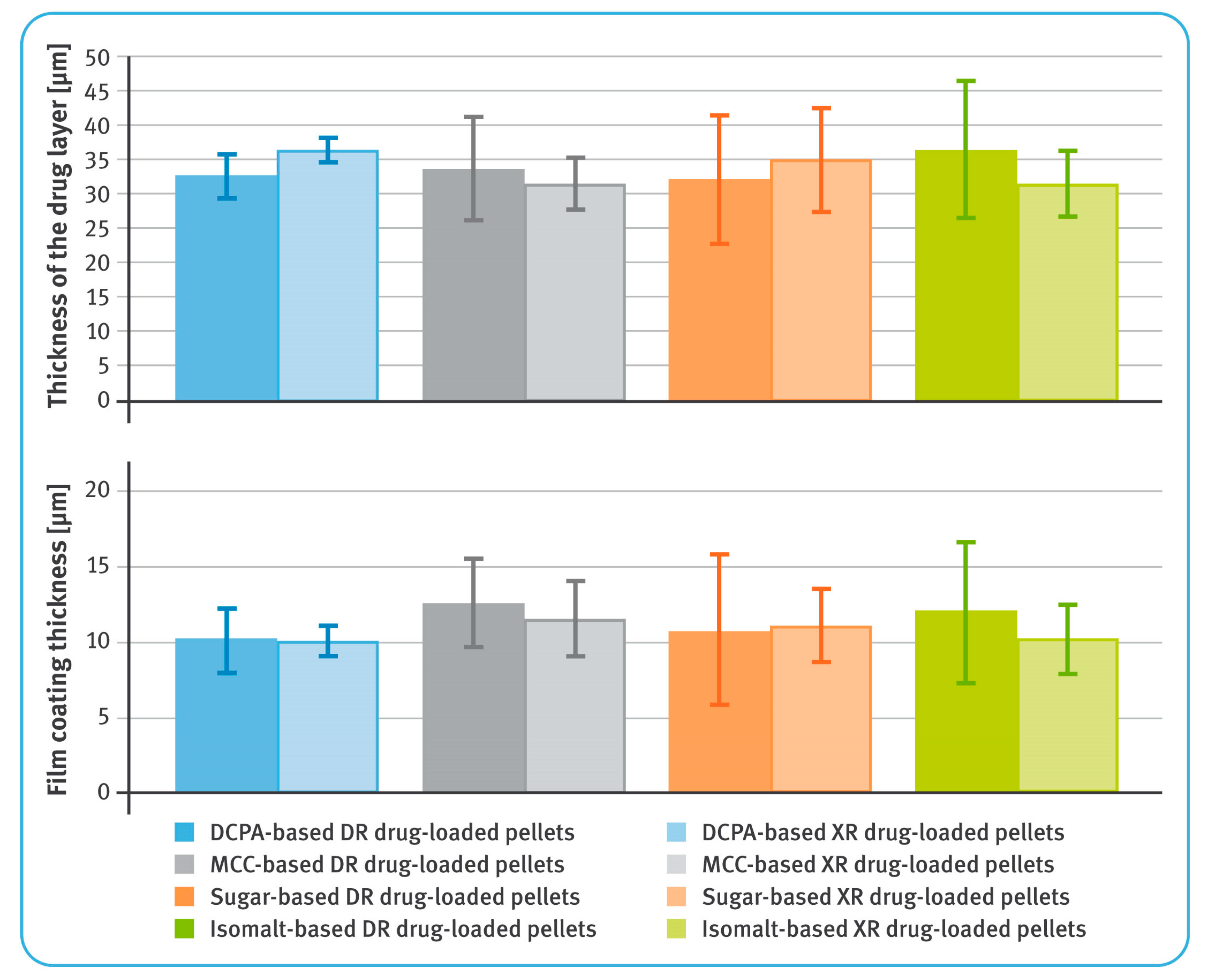
3.1. Characterization of Starter and Drug-Layered Pellets
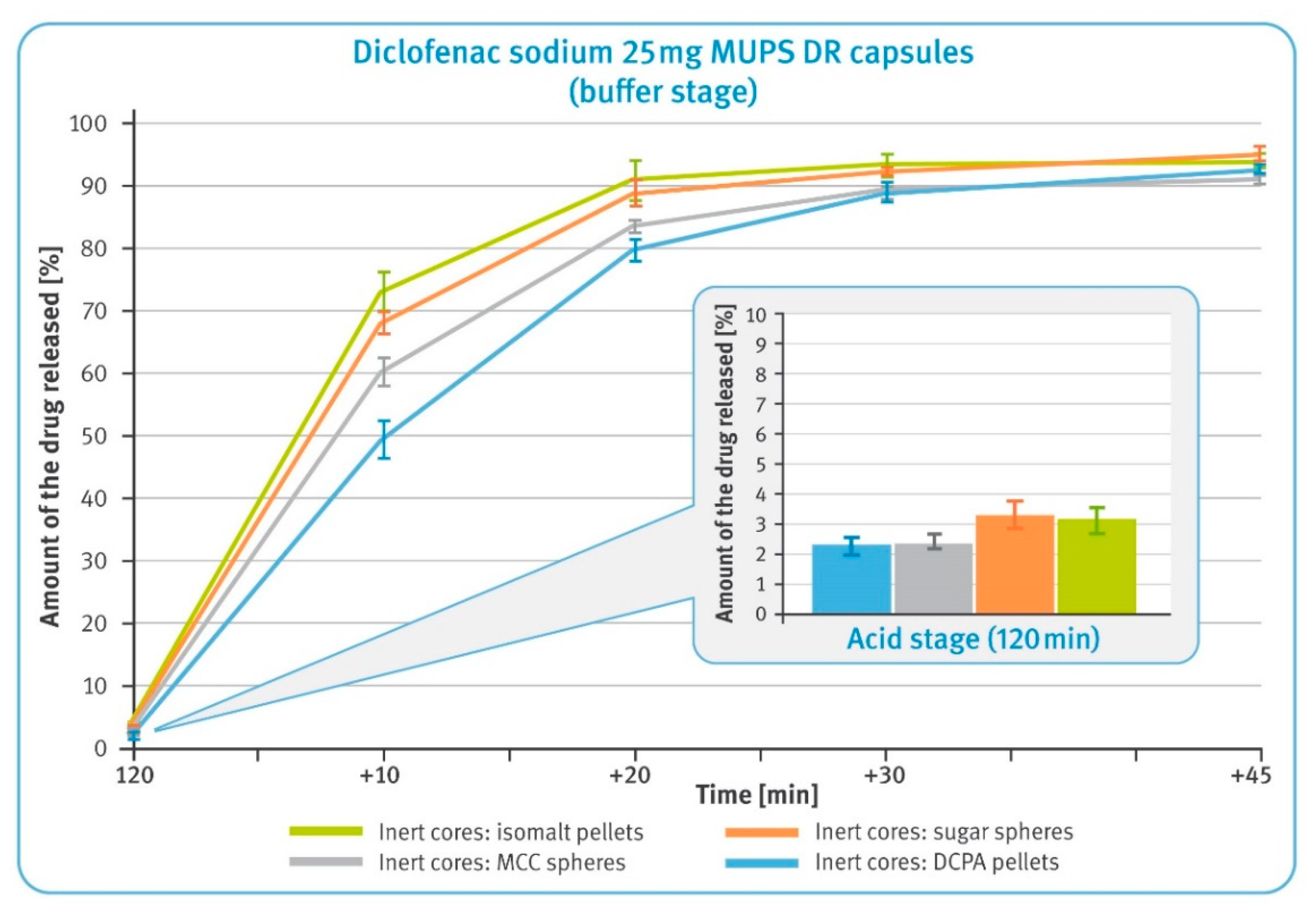
3.2. Dissolution Testing of Diclofenac Sodium DR Pellets
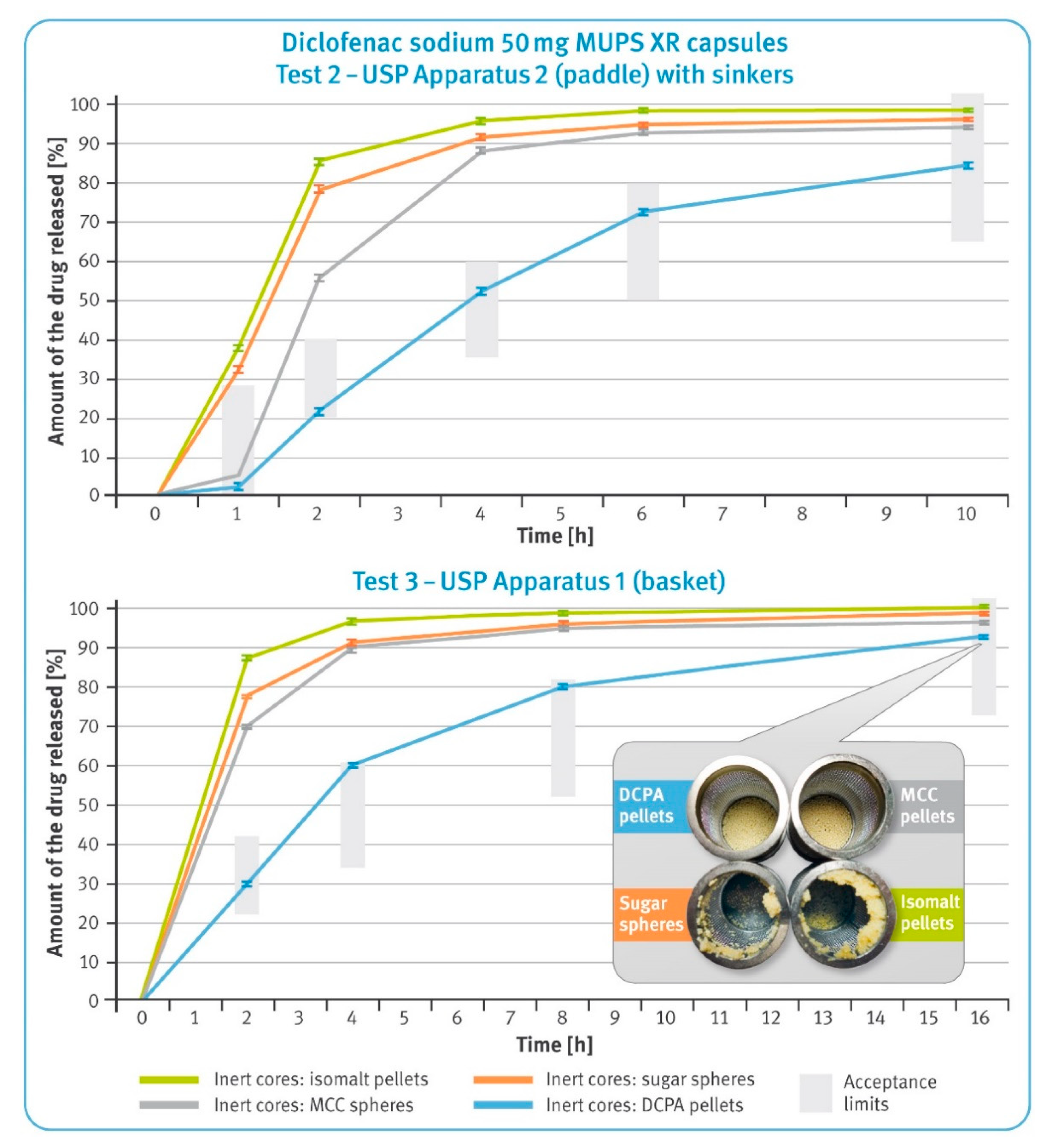
3.3. Dissolution Test of Diclofenac Sodium XR Pellets
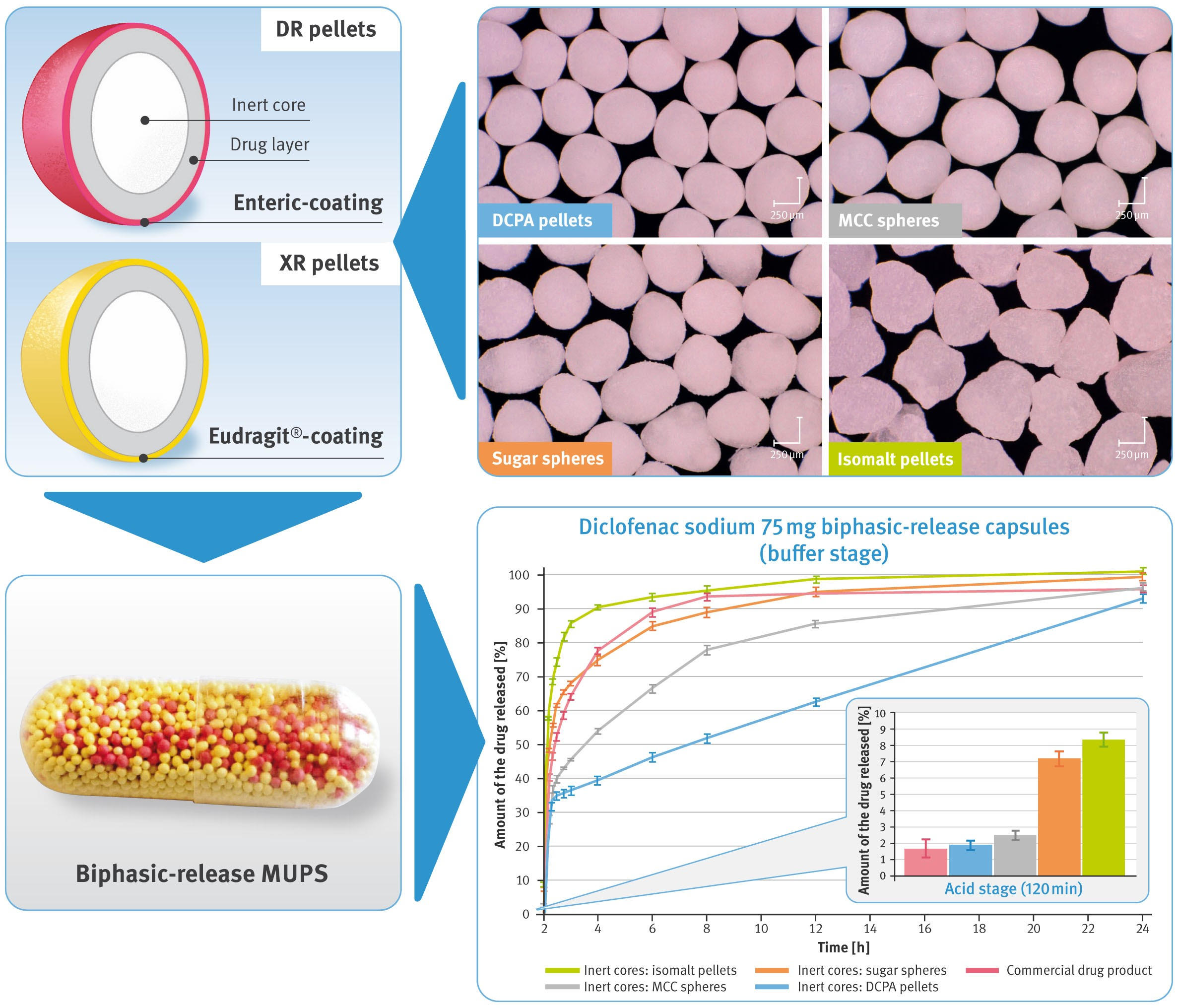
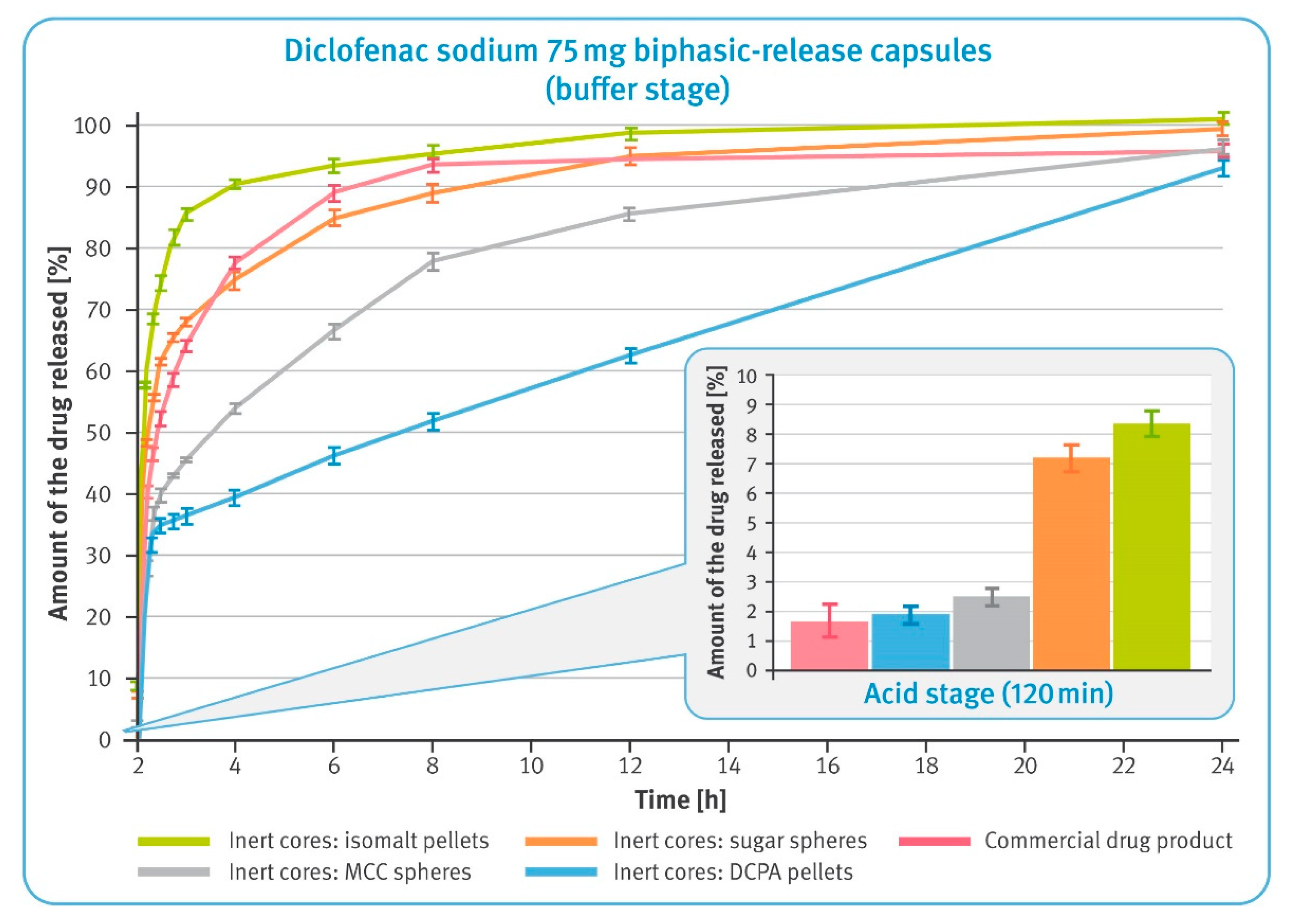
3.4. Dissolution Test of Diclofenac Sodium 75 mg BPR Hard Gelatin Capsules (Modified Compendial Methods)
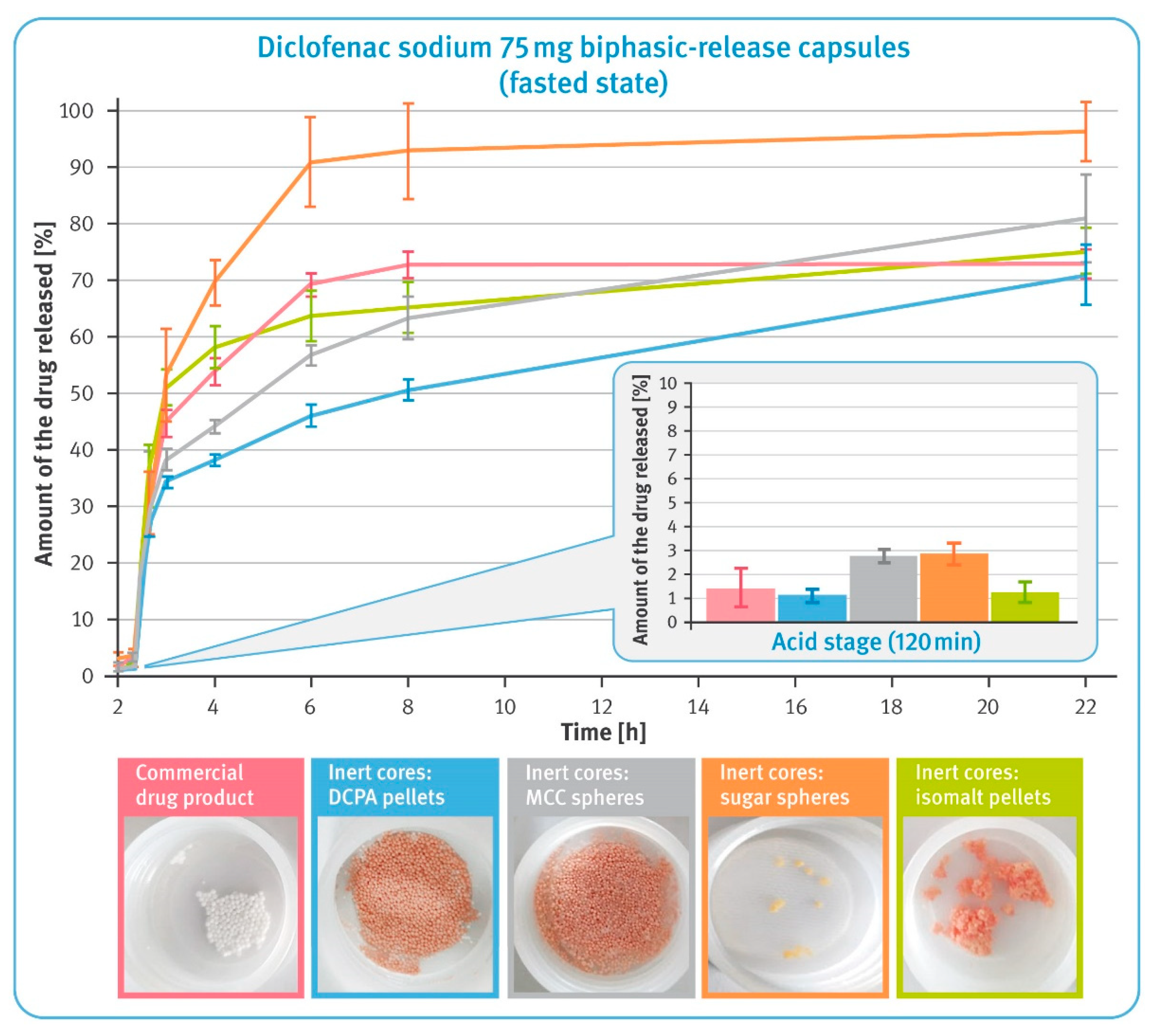
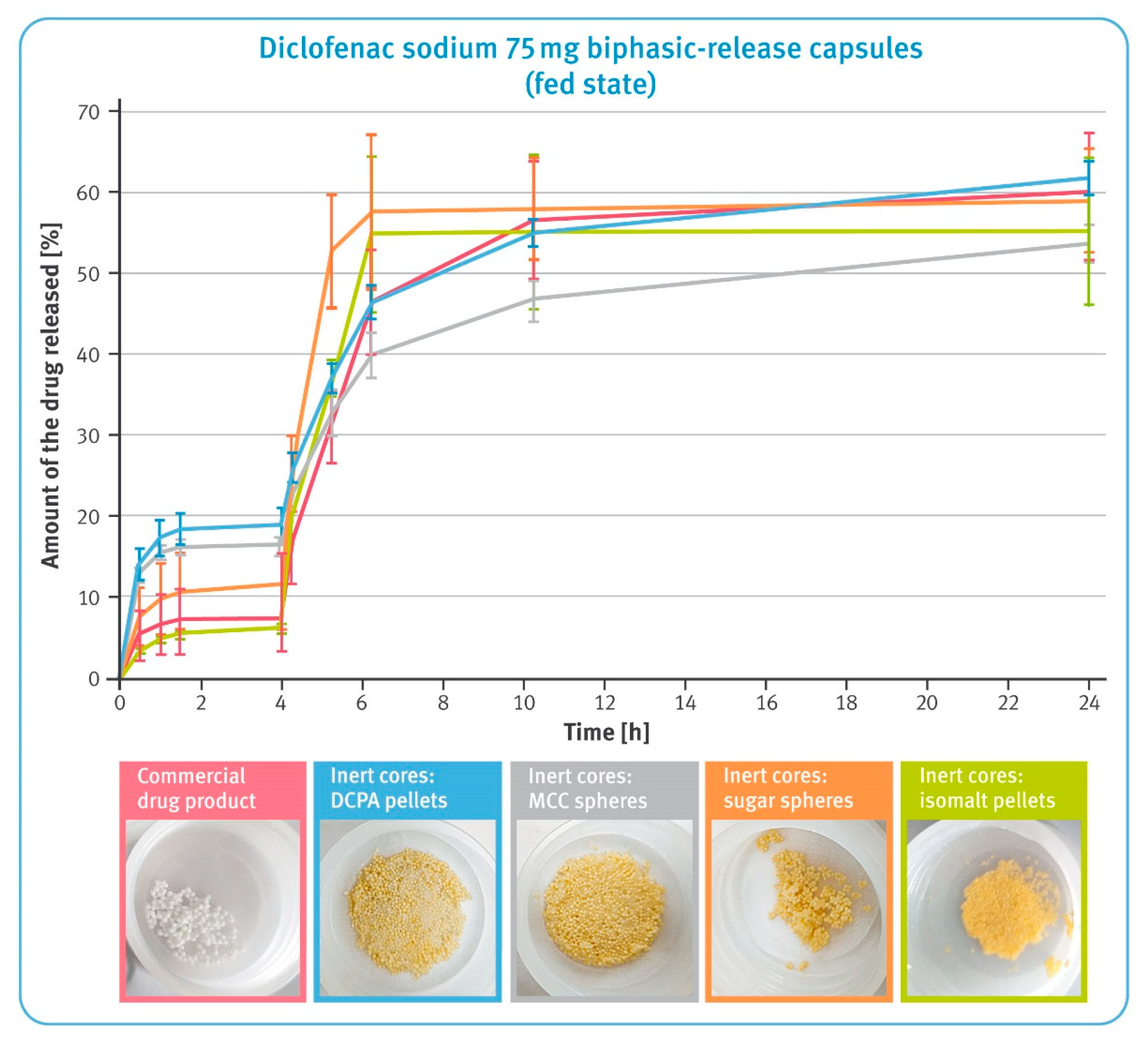
3.5. Dissolution under Conditions Simulating pH Changes in Fasted and Fed States
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pöllinger, N. Drug product development for older adults-multiparticulate formulations. In Developing Drug Products in an Aging Society-From Concept to Prescribing, 1st ed.; Stegemann, S., Ed.; Springer International Publishing: New York, NY, USA, 2016; Volume 26, pp. 247–278. [Google Scholar]
- Sidwell, R.; Hansell, J.; Rane, M.; Rajabi-Siahboomi, A.R. Characterization of inert cores for multiparticulate dosage. In Multiparticulate Drug Delivery; Rajabi-Siahboomi, A.R., Ed.; Springer: New York, NY, USA, 2017; pp. 5–36. [Google Scholar]
- Ghebre-Sellassie, I. Pellets: A general overview. In Pharmaceutical Pelletization Technology, 1st ed.; Ghebre-Sellassie, I., Ed.; MarcelDekker Inc.: New York, NY, USA, 1989; pp. 1–14. [Google Scholar]
- US Food and Drugs Administration Guidance for Industry. Size of Beads in Drug Products Labeled for Sprinkle. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/size-beads-drug-products-labeled-sprinkle-rev1 (accessed on 30 April 2021).
- Hamman, H.; Hamman, J.; Wessels, A.; Scholtz, J.; Steenekamp, J. Development of multiple-unit pellet system tablets by employing the SeDeM expert diagram system II: Pellets containing different active pharmaceutical ingredients. Pharm. Dev. Technol. 2019, 24, 145–156. [Google Scholar] [CrossRef]
- Politis, S.N.; Rekkas, D.M. Pelletization processes for pharmaceutical applications: A patent review. Recent Pat. Drug. Deliv. Formul. 2011, 5, 61–78. [Google Scholar] [CrossRef] [PubMed]
- Laicher, A.; Fuchs, W.S. Pellet technology. Sustained-release pellets in hard gelatin capsules—A suitable dosage form for theophylline. Arzneimittel-forschung 1998, 48, 540–547. [Google Scholar] [PubMed]
- Chen, T.; Li, J.; Chen, T.; Sun, C.C.; Zheng, Y. Tablets of multi-unit pellet system for controlled drug delivery. J. Control Release 2017, 262, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Abdul, S.; Chandewar, A.V.; Jaiswal, S.B. A flexible technology for modified-release drugs: Multiple-unit pellet system (MUPS). J. Control Release 2010, 147, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Lopez, F.L.; Ernest, T.B.; Tuleu, C.; Gul, M.O. Formulation approaches to pediatric oral drug delivery: Benefits and limitations of current platforms. Expert Opin. Drug Deliv. 2015, 12, 1727–1740. [Google Scholar] [CrossRef] [PubMed]
- Dukić-Ott, A.; Remon, J.P.; Foreman, P.; Vervaet, C. Immediate release of poorly soluble drugs from starch-based pellets pre-pared via extrusion/spheronisation. Eur. J. Pharm. Biopharm. 2007, 67, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Patel, H.; Gohel, M.; Tiwari, S. Dissolution rate improvement of telmisartan through modified MCC pellets using 32 full factorial design. Saudi Pharm. J. 2016, 24, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Kilor, V.A.; Sapkal, N.P.; Awari, J.G.; Shewale, B.D. Development and characterization of enteric-coated immediate-release pellets of aceclofenac by extrusion/spheronization technique using kappa-carrageenan as a pelletizing agent. AAPS PharmSciTech 2010, 11, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhang, Y.; Cai, P.; Yuan, S.; Ma, Q.; Song, Y.; Wei, H.; Wu, Z.; Wu, Z.; Qi, X. Highly specific colon-targeted transformable capsules containing indomethacin immediate-release pellets for colon cancers therapy. J. Drug Target. 2020, 28, 102–110. [Google Scholar] [CrossRef]
- Sántha, K.; Kállai-Szabó, N.; Fülöp, V.; Jakab, G.; Gordon, P.; Kállai-Szabó, B.; Balogh, E.; Antal, I. Comparative Evaluation of Pellet Cushioning Agents by Various Imaging Techniques and Dissolution Studies. AAPS PharmSciTech 2021, 22, 14. [Google Scholar] [CrossRef]
- Trofimiuk, M.; Wasilewska, K.; Winnicka, K. How to Modify Drug Release in Paediatric Dosage Forms? Novel Technologies and Modern Approaches with Regard to Children’s Population. Int. J. Mol. Sci. 2019, 20, 3200. [Google Scholar] [CrossRef]
- Desai, D.; Wang, J.; Wen, H.; Li, X.; Timmins, P. Formulation design, challenges, and development considerations for fixed dose combination (FDC) of oral solid dosage forms. Pharm. Dev. Technol. 2012, 18, 1265–1276. [Google Scholar] [CrossRef]
- Varum, F.J.; Merchant, H.A.; Basit, A.W. Oral modified-release formulations in motion: The relationship between gastrointes-tinal transit and drug absorption. Int. J. Pharm. 2010, 395, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, H.; Khalifeh, I.; Alkhalidi, B.; Aiedeh, K.; Alkhatib, H.S. Application of active layering and coating techniques in the development of a multiparticulate, controlled release dosage form of a high-dose, highly soluble drug. Pharm. Dev. Technol. 2013, 19, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Zaman, M.; Saeed-Ul-Hassan, S.; Sarfraz, R.M.; Batool, N.; Qureshi, M.J.; Akram, M.A.; Muneer, S.; Danish, Z. Pellets and pelletization: Emerging trends in the pharma industry. Acta Pol. Pharm. Drug Res. 2016, 73, 1415–1425. [Google Scholar]
- Al-Hashimi, N.; Begg, N.; Alany, R.G.; Hassanin, H.; Elshaer, A. Oral Modified Release Multiple-Unit Particulate Systems: Compressed Pellets, Microparticles and Nanoparticles. Pharmaceutics 2018, 10, 176. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, N.R.; Rajan, M.G.; Johnson, J.R.; Shukla, A.J. Pharmaceutical approaches to preparing pelletized dosage forms using the extrusion-spheronization process. Crit. Rev. Ther. Drug Carr. Syst. 2007, 24, 1–40. [Google Scholar] [CrossRef]
- Podczeck, F.; Knight, P. The evaluation of formulations for the preparation of pellets with high drug loading by extrusion/spheronization. Pharm. Dev. Technol. 2006, 11, 263–274. [Google Scholar] [CrossRef]
- Gryczová, E.; Rabisková, M.; Vetchý, D.; Krejcová, K. Pellet starters in layering technique using concentrated drug solution. Drug Dev. Ind. Pharm. 2008, 34, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Young, C.R.; Koleng, J.J.; McGinity, J.W. Properties of drug-containing spherical pellets produced by a hot-melt extrusion and spheronization process. J. Microencapsul. 2003, 20, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Zakowiecki, D.; Szczepanska, M.; Hess, T.; Cal, K.; Mikolaszek, B.; Paszkowska, J.; Wiater, M.; Hoc, D.; Garbacz, G. Preparation of delayed-release multiparticulate formulations of diclofenac sodium and evaluation of their dissolution characteristics using biorelevant dissolution methods. J. Drug Deliv. Sci. Technol. 2020, 60, 101986. [Google Scholar] [CrossRef]
- Small, R.E. Diclofenac sodium. Clin. Pharm. 1989, 8, 545–558. [Google Scholar]
- Todd, P.A.; Sorkin, E.M. Diclofenac sodium. A reappraisal of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy. Drugs 1988, 35, 244–285. [Google Scholar] [CrossRef]
- Brogden, R.N.; Heel, R.C.; Pakes, G.E.; Speight, T.M.; Avery, G.S. Diclofenac sodium: A review of its pharmacological properties and therapeutic use in rheumatic diseases and pain of varying origin. Drugs 1980, 20, 24–48. [Google Scholar] [CrossRef]
- Chuasuwan, B.; Binjesoh, V.; Polli, J.E.; Zhang, H.; Amidon, G.L.; Junginger, H.E.; Midha, K.K.; Shah, V.P.; Stavchansky, S.; Dressman, J.B.; et al. Biowaiver monographs for immediate release solid oral dosage forms: Diclofenac sodium and diclofenac potassium. J. Pharm. Sci. 2009, 98, 1206–1219. [Google Scholar] [CrossRef]
- Davies, N.M.; Anderson, K.E. Clinical pharmacokinetics of diclofenac. Therapeutic insights and pitfalls. Clin. Pharmacokinet. 1997, 33, 184–213. [Google Scholar] [CrossRef]
- Riess, W.; Stierlin, H.; Degen, P.; Faigle, J.W.; Gérardin, A.; Moppert, J.; Sallmann, A.; Schmid, K.; Schweizer, A.; Sulc, M.; et al. Pharmacokinetics and metabolism of the anti-inflammatory agent Voltaren. Scand. J. Rheumatol. Suppl. 1978, 22, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Willis, J.V.; Kendall, M.J.; Flinn, R.M.; Thornhill, D.P.; Welling, P.G. The pharmacokinetics of diclofenac sodium following intravenous and oral administration. Eur. J. Clin. Pharmacol. 1979, 16, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Derry, P.; Derry, S.; Moore, R.A.; McQuay, H.J. Single dose oral diclofenac for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2009, 2, CD004768. [Google Scholar]
- Altman, R.; Bosch, B.; Brune, K.; Patrignani, P.; Young, C. Advances in NSAID development: Evolution of diclofenac products using pharmaceutical technology. Drugs 2015, 75, 59–77. [Google Scholar] [CrossRef]
- Rosen, H.; Abribat, T. The rise and rise of drug delivery. Nat. Rev. Drug Discov. 2005, 4, 381–385. [Google Scholar] [CrossRef]
- Bravo, S.A.; Lamas, M.C.; Salamón, C.J. In-vitro studies of diclofenac sodium controlled- release from biopolymeric hydrophilic matrices. J. Pharm. Pharm. Sci. 2002, 5, 213–219. [Google Scholar]
- Tschopp, P. Starting pellets: Materials, manufacturing methods, and applications. Tablets Capsul. 2015, 13, 10–13. [Google Scholar]
- Werner, D. Sugar spheres: A versatile excipient for oral pellet medications with modified release kinetics. Pharmaceut. Technol. Eur. 2006, 18, 35–41. [Google Scholar]
- Luhn, O.; Kállai, N.; Nagy, Z.K.; Kovács, K.; Fritzsching, B.; Klebovich, I.; Antal, I. Dissolution profile of novel composite pellet cores based on different ratios of microcrystalline cellulose and isomalt. J. Pharm. Sci. 2012, 101, 2675–2680. [Google Scholar] [CrossRef]
- Kállai, N.; Luhn, O.; Dredán, J.; Kovács, K.; Lengyel, M.; Antal, I. Evaluation of drug release from coated pellets based on isomalt, sugar, and microcrystalline cellulose inert cores. AAPS PharmSciTech 2010, 11, 383–391. [Google Scholar] [CrossRef]
- Zakowiecki, D.; Lachmann, M.; Schaum, V.; Hess, T. Novel starter pellets based on dibasic calcium phosphate anhydrous: Properties and application. Express Pharma 2019, 15, 34–36. [Google Scholar]
- Perlovich, G.L.; Surov, A.O.; Hansen, L.K.; Bauer-Brandl, A. Energetic aspects of diclofenac acid in crystal modifications and in solutions--mechanism of solvation, partitioning and distribution. J. Pharm. Sci. 2007, 96, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Panchagnula, R. Design of controlled release delivery systems using a modified pharmacokinetic approach: A case study for drugs having a short elimination half-life and a narrow therapeutic index. Int. J. Pharm. 2003, 261, 27–41. [Google Scholar] [CrossRef]
- Elzayat, E.M.; Abdel-Rahman, A.A.; Ahmed, S.M.; Alanazi, F.K.; Habib, W.A.; Abou-Auda, H.S.; Sakr, A. Formulation and pharmacokinetics of multi-layered matrix tablets: Biphasic delivery of diclofenac. Saudi Pharm. J. 2017, 25, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Marucci, M.; Ragnarsson, G.; Axelsson, A. Evaluation of osmotic effects on coated pellets using a mechanistic model. Int. J. Pharm. 2007, 336, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, A.G.; Ozturk, S.S.; Palsson, B.O.; Wheatley, T.A.; Dressman, J.B. Mechanism of release from pellets coated with an ethylcellulose-based film. J. Control Release 1990, 14, 203–213. [Google Scholar] [CrossRef]
- Kleinebudde, P. Shrinking and swelling properties of pellets containing microcrystalline cellulose and low substituted hydroxypropylcellulose: II. Swelling properties. Int. J. Pharm. 1994, 109, 221–227. [Google Scholar] [CrossRef]
- Manohar, P.; Venkatesh, M.; Saurabh, J.S.; Vinayak, S.; Girish, D.K.; Jain, K. Extended Release Dosage Forms of Metoprolol. U.S. Patent US8962016B2, 24 February 2015. Available online: https://patentimages.storage.googleapis.com/27/6c/db/66f0f9df7423ad/US8962016.pdf (accessed on 30 April 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Process Parameter | Drug Loading | Enteric Release Coating | Functional Film Coating |
|---|---|---|---|
| Inlet airflow rate | 0.31 ± 0.1 m3/min | 0.32 ± 0.1 m3/min | 0.30 ± 0.1 m3/min |
| Inlet air temperature | 57 ± 2 °C | 56 ± 2 °C | 31 ± 2 °C |
| Product temperature | 40 ± 2 °C | 41 ± 2 °C | 26 ± 2 °C |
| Spraying pressure | 1.1 ± 0.2 bar | 1.1 ± 0.2 bar | 1.0 ± 0.2 bar |
| Coating mixture flow rate | 1.3 g/min | 1.0 g/min | 1.0 g/min |
| Drying time | 10 min | 30 min | 30 min |
| Curing time and temperature | - | - | 24 h at 42 ± 2 °C |
| Inert Cores | DCPA Pellets | MCC Spheres | Sugar Spheres | Isomalt Pellets |
|---|---|---|---|---|
| Starter pellets | 1.06 ± 0.02 g/mL | 0.89 ± 0.01 g/mL | 0.87 ± 0.01 g/mL | 0.81 ± 0.02 g/mL |
| DR drug-loaded pellets | 1.02 ± 0.01 g/mL | 0.85 ± 0.02 g/mL | 0.88 ± 0.01 g/mL | 0.86 ± 0.02 g/mL |
| XR drug-loaded pellets | 1.05 ± 0.02 g/mL | 0.92 ± 0.02 g/mL | 0.89 ± 0.02 g/mL | 0.90 ± 0.02 g/mL |
| Inert Cores | DCPA Pellets | MCC Spheres | Sugar Spheres | Isomalt Pellets | ||||
|---|---|---|---|---|---|---|---|---|
| Parameter | Roundness | Convexity | Roundness | Convexity | Roundness | Convexity | Roundness | Convexity |
| Starter pellets | 0.891 ± 0.015 | 0.995 ± 0.004 | 0.874 ± 0.023 | 0.993 ± 0.007 | 0.845 ± 0.030 | 0.981 ± 0.011 | 0.787 ± 0.042 | 0.968 ± 0.013 |
| DR drug-loaded pellets | 0.892 ± 0.017 | 0.998 ± 0.005 | 0.869 ± 0.028 | 0.994 ± 0.008 | 0.845 ± 0.057 | 0.978 ± 0.027 | 0.785 ± 0.082 | 0.956 ± 0.047 |
| XR drug-loaded pellets | 0.890 ± 0.022 | 0.993 ± 0.010 | 0.873 ± 0.026 | 0.991 ± 0.012 | 0.867 ± 0.034 | 0.991 ± 0.014 | 0.828 ± 0.034 | 0.985 ± 0.010 |
| Inert Cores | DCPA Pellets | MCC Spheres | Sugar Spheres | Isomalt Pellets |
|---|---|---|---|---|
| DR drug-loaded pellets | 7.37 ± 0.01% | 7.62 ± 0.04% | 7.31 ± 0.07% | 7.24 ± 0.05% |
| XR drug-loaded pellets | 8.02 ± 0.06% | 8.04 ± 0.08% | 7.93 ± 0.01% | 8.18 ± 0.09% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zakowiecki, D.; Frankiewicz, M.; Hess, T.; Cal, K.; Gajda, M.; Dabrowska, J.; Kubiak, B.; Paszkowska, J.; Wiater, M.; Hoc, D.; et al. Development of a Biphasic-Release Multiple-Unit Pellet System with Diclofenac Sodium Using Novel Calcium Phosphate-Based Starter Pellets. Pharmaceutics 2021, 13, 805. https://doi.org/10.3390/pharmaceutics13060805
Zakowiecki D, Frankiewicz M, Hess T, Cal K, Gajda M, Dabrowska J, Kubiak B, Paszkowska J, Wiater M, Hoc D, et al. Development of a Biphasic-Release Multiple-Unit Pellet System with Diclofenac Sodium Using Novel Calcium Phosphate-Based Starter Pellets. Pharmaceutics. 2021; 13(6):805. https://doi.org/10.3390/pharmaceutics13060805
Chicago/Turabian StyleZakowiecki, Daniel, Maja Frankiewicz, Tobias Hess, Krzysztof Cal, Maciej Gajda, Justyna Dabrowska, Bartlomiej Kubiak, Jadwiga Paszkowska, Marcela Wiater, Dagmara Hoc, and et al. 2021. "Development of a Biphasic-Release Multiple-Unit Pellet System with Diclofenac Sodium Using Novel Calcium Phosphate-Based Starter Pellets" Pharmaceutics 13, no. 6: 805. https://doi.org/10.3390/pharmaceutics13060805
APA StyleZakowiecki, D., Frankiewicz, M., Hess, T., Cal, K., Gajda, M., Dabrowska, J., Kubiak, B., Paszkowska, J., Wiater, M., Hoc, D., Garbacz, G., & Haznar-Garbacz, D. (2021). Development of a Biphasic-Release Multiple-Unit Pellet System with Diclofenac Sodium Using Novel Calcium Phosphate-Based Starter Pellets. Pharmaceutics, 13(6), 805. https://doi.org/10.3390/pharmaceutics13060805