
Intrapericardial Delivery of APA-Microcapsules as Promising Stem Cell Therapy Carriers in an Experimental Acute Myocardial Infarction Model

 , ,
, ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
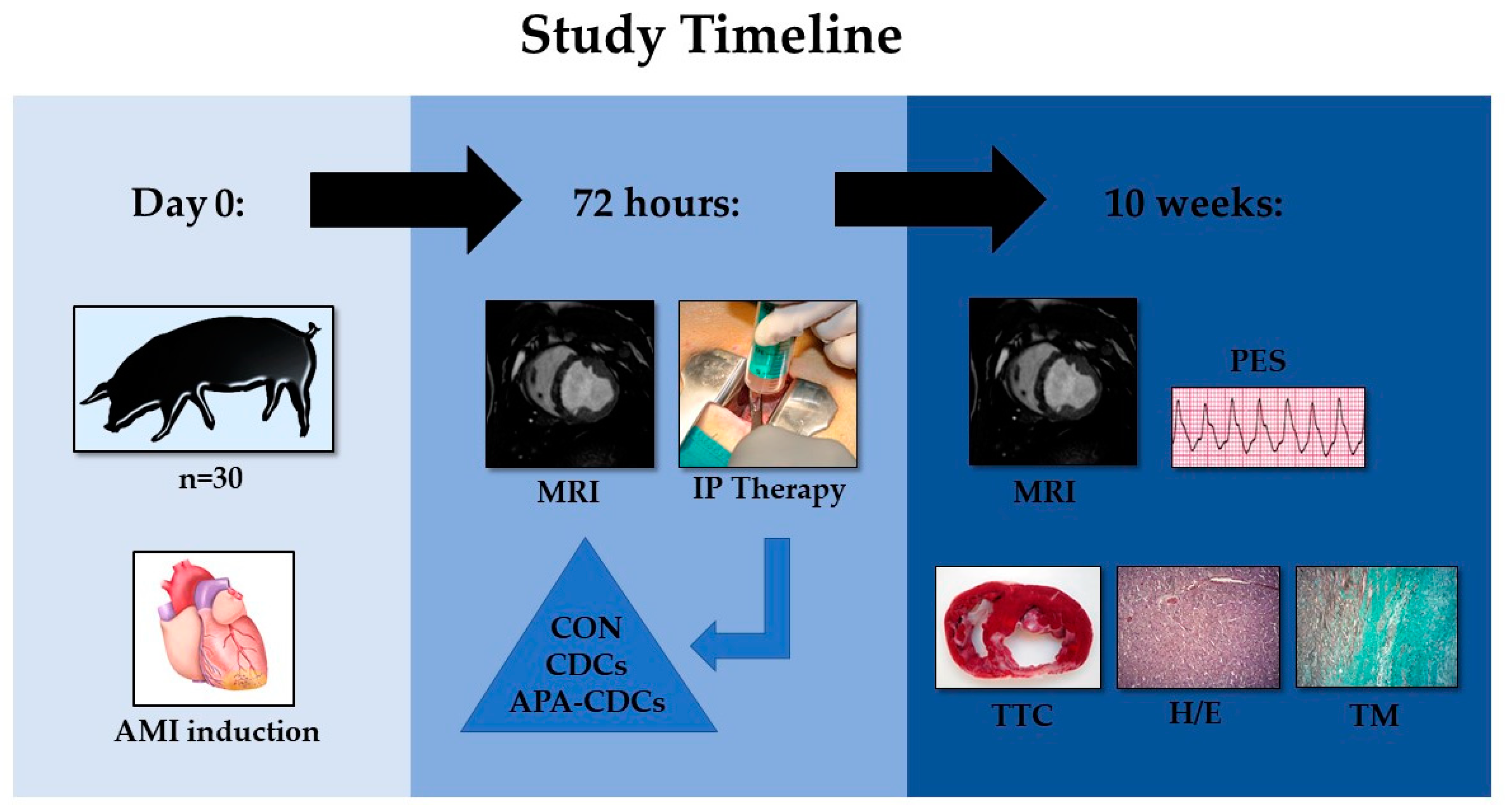
2.1. Experimental Protocol
2.2. Anaesthesia and Analgesia
2.3. Infarct Induction
2.4. CDCs Isolation and Culture
2.5. Cell Encapsulation
2.6. Group Allocation and IP Administration
2.7. MRI Studies
2.8. End of Study and Post-Mortem Examinations
2.9. Statistical Analysis
3. Results
3.1. Infarct Induction
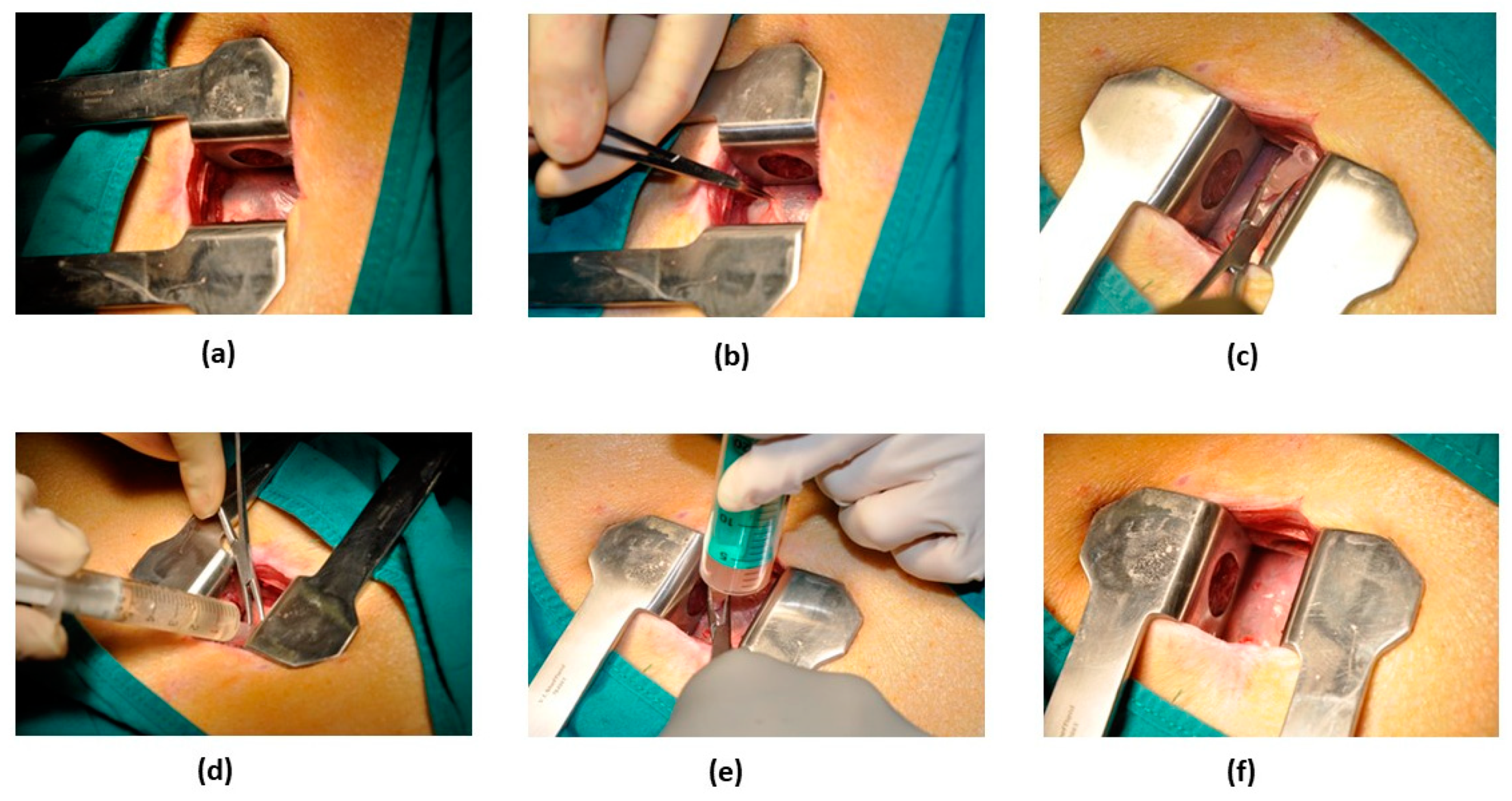
3.2. IP Therapy Administration
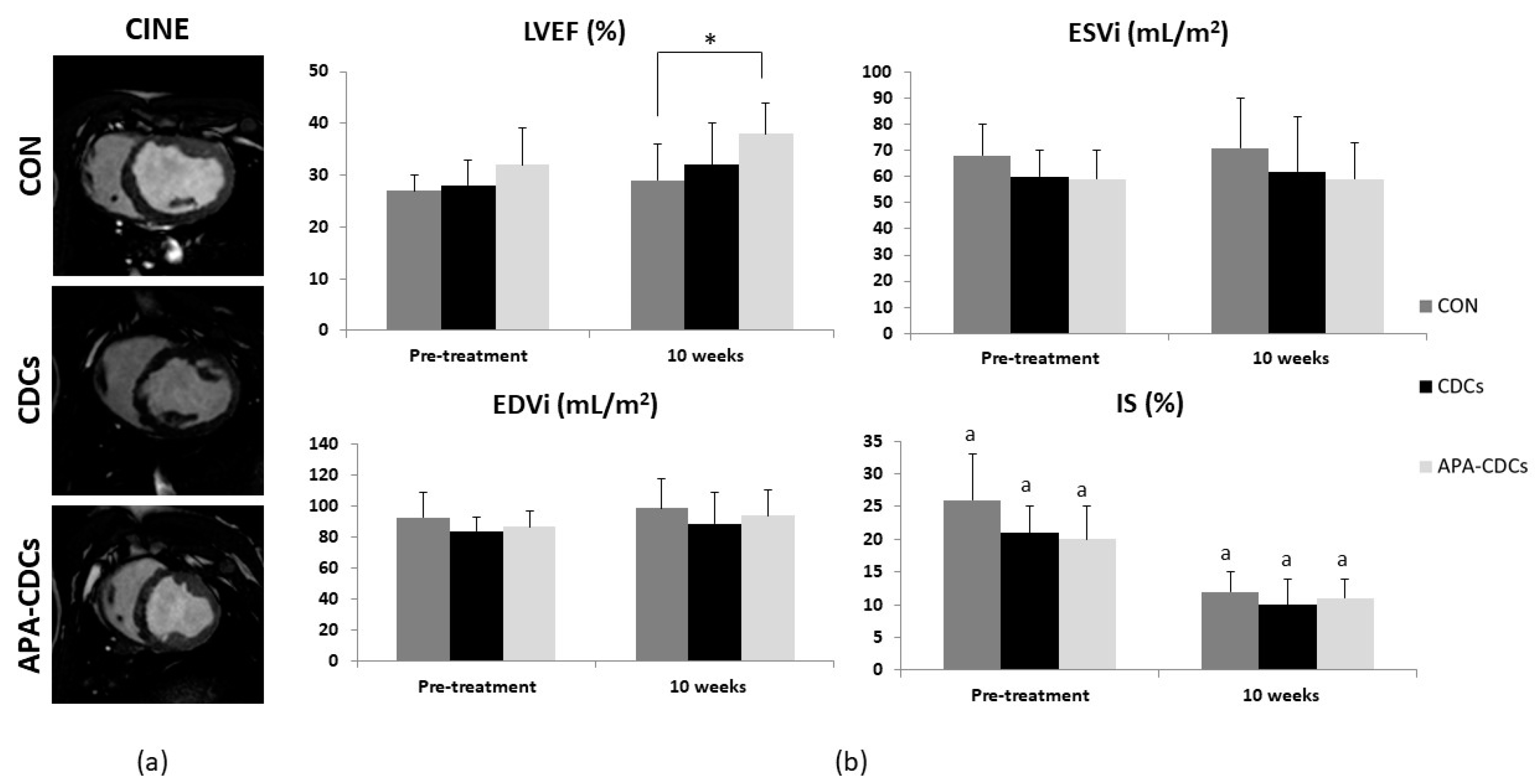
3.3. MRI Studies
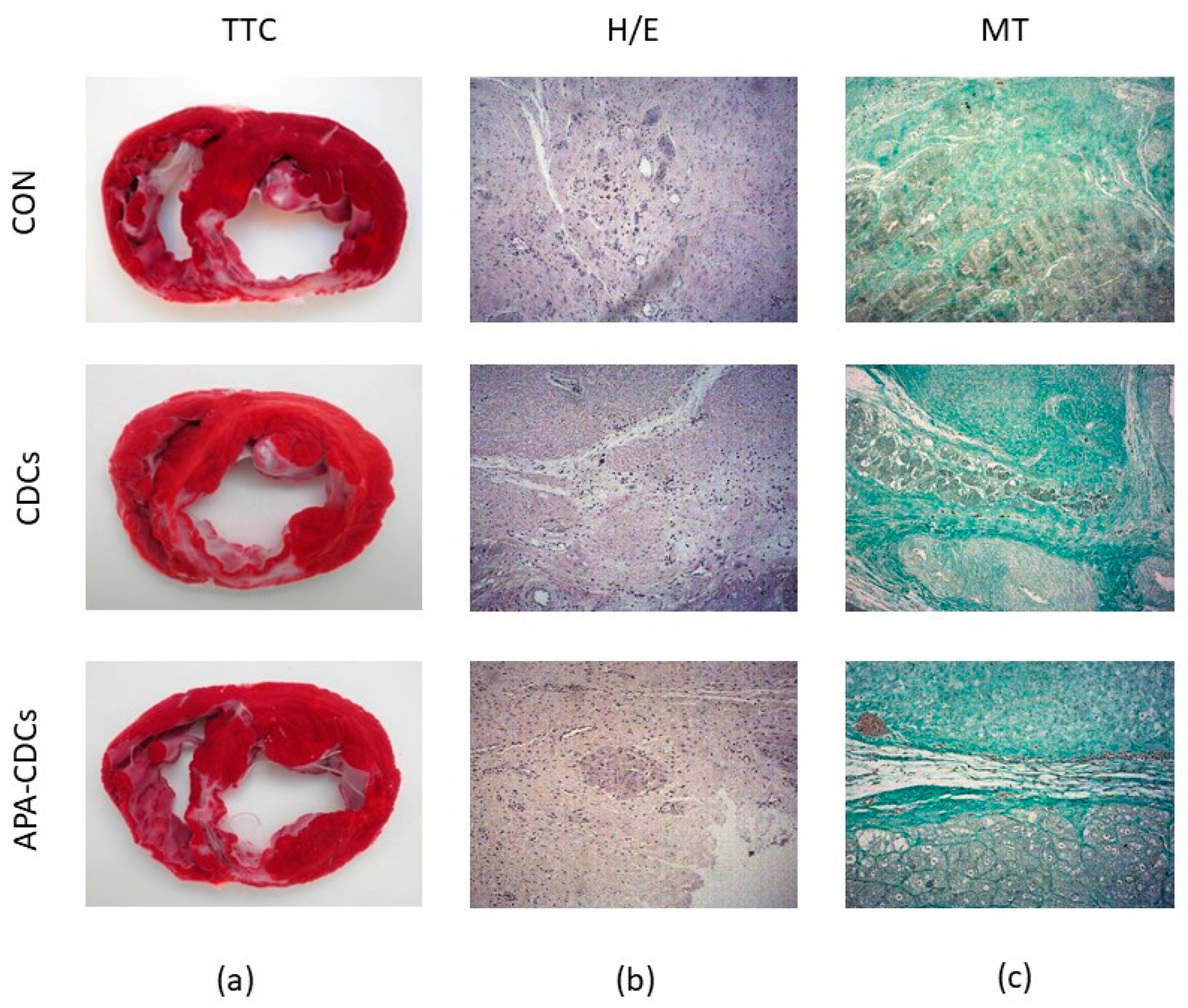
3.4. End of Study and Post-Mortem Examinations
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; E Petersen, S.; A Mossialos, E.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef]
- Townsend, N.; Nichols, M.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe — epidemiological update 2015. Eur. Heart J. 2015, 36, 2696–2705. [Google Scholar] [CrossRef]
- Ponikowski, P.; Anker, S.D.; Alhabib, K.; Cowie, M.R.; Force, T.L.; Hu, S.; Jaarsma, T.; Krum, H.; Rastogi, V.; Rohde, L.E.; et al. Heart failure: Preventing disease and death worldwide. ESC Hear. Fail. 2014, 1, 4–25. [Google Scholar] [CrossRef]
- Dimmeler, S.; Burchfield, J.; Zeiher, A.M. Cell-Based Therapy of Myocardial Infarction. Arter. Thromb. Vasc. Biol. 2008, 28, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Van Der Spoel, T.I.; Lorkeers, S.J.J.O.; Agostoni, P.; VAN Belle, E.; Gyöngyösi, M.; Sluijter, J.; Cramer, M.J.; Doevendans, P.A.; Chamuleau, S.A. Human relevance of pre-clinical studies in stem cell therapy: Systematic review and meta-analysis of large animal models of ischaemic heart disease. Cardiovasc. Res. 2011, 91, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.V.; Sasano, T.; Mills, K.; Evers, R.; Lee, S.-T.; Smith, R.R.; Lardo, A.C.; Lai, S.; Steenbergen, C.; Gerstenblith, G.; et al. Engraftment, Differentiation, and Functional Benefits of Autologous Cardiosphere-Derived Cells in Porcine Ischemic Cardiomyopathy. Circ. 2009, 120, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Malliaras, K.; Li, T.-S.; Luthringer, D.; Terrovitis, J.; Cheng, K.; Chakravarty, T.; Galang, G.; Zhang, Y.; Schoenhoff, F.; Van Eyk, J.; et al. Safety and Efficacy of Allogeneic Cell Therapy in Infarcted Rats Transplanted With Mismatched Cardiosphere-Derived Cells. Circ. 2012, 125, 100–112. [Google Scholar] [CrossRef]
- Kapelios, C.J.; Nanas, J.N.; Malliaras, K. Allogeneic cardiosphere-derived cells for myocardial regeneration: Current progress and recent results. Future Cardiol. 2016, 12, 87–100. [Google Scholar] [CrossRef]
- Malliaras, K.; Zhang, Y.; Seinfeld, J.; Galang, G.; Tseliou, E.; Cheng, K.; Sun, B.; Aminzadeh, M.; Marbán, E. Cardiomyocyte proliferation and progenitor cell recruitment underlie therapeutic regeneration after myocardial infarction in the adult mouse heart. EMBO Mol. Med. 2013, 5, 191–209. [Google Scholar] [CrossRef]
- Malliaras, K.; Makkar, R.R.; Smith, R.R.; Cheng, K.; Wu, E.; Bonow, R.O.; Marbán, L.; Mendizabal, A.; Cingolani, E.; Johnston, P.V.; et al. Intracoronary Cardiosphere-Derived Cells After Myocardial Infarction. J. Am. Coll. Cardiol. 2014, 63, 110–122. [Google Scholar] [CrossRef]
- Macia, E.; Boyden, P.A. Stem Cell Therapy Is Proarrhythmic. Circ. 2009, 119, 1814–1823. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.; Rieger, A.C.; Balkan, W.; Hare, J.M. Clinical-based Cell Therapies for Heart Disease-Current and Future State. Rambam Maimonides Med J. 2020, 11, e0015. [Google Scholar] [CrossRef]
- Li, T.-S.; Cheng, K.; Malliaras, K.; Smith, R.R.; Zhang, Y.; Sun, B.; Matsushita, N.; Blusztajn, A.; Terrovitis, J.; Kusuoka, H.; et al. Direct Comparison of Different Stem Cell Types and Subpopulations Reveals Superior Paracrine Potency and Myocardial Repair Efficacy With Cardiosphere-Derived Cells. J. Am. Coll. Cardiol. 2012, 59, 942–953. [Google Scholar] [CrossRef]
- Ellison, G.; Torella, D.; Dellegrottaglie, S.; Pérez-Martínez, C.; de Prado, A.P.; Vicinanza, C.; Purushothaman, S.; Galuppo, V.; Iaconetti, C.; Waring, C.D.; et al. Endogenous Cardiac Stem Cell Activation by Insulin-Like Growth Factor-1/Hepatocyte Growth Factor Intracoronary Injection Fosters Survival and Regeneration of the Infarcted Pig Heart. J. Am. Coll. Cardiol. 2011, 58, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.D.; Bertaso, A.G.; Psaltis, P.J.; Frost, L.; Carbone, A.; Paton, S.; Nelson, A.; Wong, D.T.; Worthley, M.I.; Gronthos, S.; et al. Impact of Timing and Dose of Mesenchymal Stromal Cell Therapy in a Preclinical Model of Acute Myocardial Infarction. J. Card. Fail. 2013, 19, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Gnecchi, M.; He, H.; Melo, L.G.; Noiseaux, N.; Morello, F.; De Boer, R.A.; Zhang, L.; Pratt, R.E.; Dzau, V.J.; Ingwall, J.S. Early Beneficial Effects of Bone Marrow-Derived Mesenchymal Stem Cells Overexpressing Akt on Cardiac Metabolism after Myocardial Infarction. STEM CELLS 2009, 27, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Mauricio, R.G.; Acarregui, A.; Margallo, F.M.S.; Crisóstomo, V.; Gallo, I.; Hernández, R.M.; Pedraz, J.L.; Orive, G.; Martín-Cancho, M.F. A preliminary approach to the repair of myocardial infarction using adipose tissue-derived stem cells encapsulated in magnetic resonance-labelled alginate microspheres in a porcine model. Eur. J. Pharm. Biopharm. 2013, 84, 29–39. [Google Scholar] [CrossRef]
- Blázquez, R.; Sánchez-Margallo, F.M.; Crisóstomo, V.; Báez, C.; Maestre, J.; García-Lindo, M.; Usón, A.; Álvarez, V.; Casado, J.G. Intrapericardial Administration of Mesenchymal Stem Cells in a Large Animal Model: A Bio-Distribution Analysis. PLoS ONE 2015, 10, e0122377. [Google Scholar] [CrossRef]
- Sun, F.; Sánchez, F.M.; Crisóstomo, V.; Luis, L.; Usón, J.; Maynar, M. Subxiphoid Access to Normal Pericardium with Micropuncture Set: Technical Feasibility Study in Pigs. Radiology 2006, 238, 719–724. [Google Scholar] [CrossRef]
- Zhu, D.; Li, Z.; Huang, K.; Caranasos, T.G.; Rossi, J.S.; Cheng, K. Minimally invasive delivery of therapeutic agents by hydrogel injection into the pericardial cavity for cardiac repair. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Fernandez-Jimenez, R.; Sánchez-González, J.; Aguero, J.; García-Prieto, J.; López-Martín, G.J.; García-Ruiz, J.M.; Iracheta, A.D.M.; Rossello, X.; Friera, L.F.; Pizarro, G.; et al. Myocardial Edema After Ischemia/Reperfusion Is Not Stable and Follows a Bimodal Pattern. J. Am. Coll. Cardiol. 2015, 65, 315–323. [Google Scholar] [CrossRef]
- Crisostomo, V.; Díaz, C.B.; Maestre, J.; Garcia-Lindo, M.; Sun, F.; Casado, J.G.; Blazquez, R.; Abad, J.L.; Palacios, I.; Rodriguez-Borlado, L.; et al. Delayed administration of allogeneic cardiac stem cell therapy for acute myocardial infarction could ameliorate adverse remodeling: Experimental study in swine. J. Transl. Med. 2015, 13, 1–16. [Google Scholar] [CrossRef]
- Blázquez, R.; Margallo, F.M.S.; Crisostomo, V.; Báez, C.; Maestre, J.; Álvarez, V.; Casado, J.G. Intrapericardial Delivery of Cardiosphere-Derived Cells: An Immunological Study in a Clinically Relevant Large Animal Model. PLoS ONE 2016, 11, e0149001. [Google Scholar] [CrossRef] [PubMed]
- Báez-Díaz, C.; Blanco-Blázquez, V.; Sánchez-Margallo, F.-M.; Bayes-Genis, A.; González, I.; Abad, A.; Steendam, R.; Franssen, O.; Palacios, I.; Sánchez, B.; et al. Microencapsulated Insulin-Like Growth Factor-1 therapy improves cardiac function and reduces fibrosis in a porcine acute myocardial infarction model. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Levit, R.D.; Landázuri, N.; Phelps, E.A.; Brown, M.E.; García, A.J.; Davis, M.E.; Joseph, G.; Long, R.; Safley, S.A.; Suever, J.D.; et al. Cellular Encapsulation Enhances Cardiac Repair. J. Am. Hear. Assoc. 2013, 2, e000367. [Google Scholar] [CrossRef] [PubMed]
- Choe, G.; Park, J.; Park, H.; Lee, J.Y. Hydrogel Biomaterials for Stem Cell Microencapsulation. Polymer 2018, 10, 997. [Google Scholar] [CrossRef] [PubMed]
- Bartunek, J.; Wijns, W.; Heyndrickx, G.R.; Vanderheyden, M. Timing of intracoronary bone-marrow-derived stem cell transplantation after ST-elevation myocardial infarction. Nat. Clin. Pr. Neurol. 2006, 3, S52–S56. [Google Scholar] [CrossRef]
- Huang, R.; Yao, K.; Sun, A.; Qian, J.; Ge, L.; Zhang, Y.; Niu, Y.; Wang, K.; Zou, Y.; Ge, J. Timing for intracoronary administration of bone marrow mononuclear cells after acute ST-elevation myocardial infarction: A pilot study. Stem Cell Res. Ther. 2015, 6, 1–11. [Google Scholar] [CrossRef]
- Wilson, J.L.; McDevitt, T.C. Stem cell microencapsulation for phenotypic control, bioprocessing, and transplantation. Biotechnol. Bioeng. 2013, 110, 667–682. [Google Scholar] [CrossRef]
- Ziani, K.; Espona-Noguera, A.; Crisóstomo, V.; Casado, J.G.; Sanchez-Margallo, F.M.; Saenz-Del-Burgo, L.; Ciriza, J.; Pedraz, J.L. Characterization of encapsulated porcine cardiosphere-derived cells embedded in 3D alginate matrices. Int. J. Pharm. 2021, 599, 120454. [Google Scholar] [CrossRef]
- Hajifathaliha, F.; Mahboubi, A.; Nematollahi, L.; Mohit, E.; Bolourchian, N. Comparison of different cationic polymers efficacy in fabrication of alginate multilayer microcapsules. Asian J. Pharm. Sci. 2020, 15, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Crisostomo, V.; Baez, C.; Abad, J.L.; Sanchez, B.; Alvarez, V.; Rosado, R.; Gómez-Mauricio, G.; Gheysens, O.; Blanco-Blázquez, V.; Blazquez, R.; et al. Dose-dependent improvement of cardiac function in a swine model of acute myocardial infarction after intracoronary administration of allogeneic heart-derived cells. Stem Cell Res. Ther. 2019, 10, 1–17. [Google Scholar] [CrossRef]
- Palomares, J.F.R.; Gavara, J.; Ferreira-González, I.; Valente, F.; Rios-Navarro, C.; Rodríguez-García, J.; Bonanad, C.; del Blanco, B.G.; Miñana, G.; Mutuberria, M.; et al. Prognostic Value of Initial Left Ventricular Remodeling in Patients with Reperfused STEMI. JACC Cardiovasc. Imaging 2019, 12, 2445–2456. [Google Scholar] [CrossRef]
- Solomon, S.D.; Glynn, R.J.; Greaves, S.; Ajani, U.; Rouleau, J.-L.; Menapace, F.; Arnold, J.M.O.; Hennekens, C.; Pfeffer, M.A. Recovery of ventricular function after myocardial infarction in the reperfusion era: The healing and early afterload reducing therapy study. Ann. Intern. Med. 2001, 134, 451–458. [Google Scholar] [CrossRef]
- Román, J.A.S.; Candell-Riera, J.; Arnold, R.; Sanchez, P.L.; Aguadé-Bruix, S.; Bermejo, J.; Revilla, A.; Villa, A.; Cuéllar, H.; Hernandez, C.; et al. Análisis cuantitativo de la función ventricular izquierda como herramienta para la investigación clínica. Fundamentos y metodología. Rev. Española Cardiol. 2009, 62, 535–551. [Google Scholar] [CrossRef]
- Sanz, J.; LaRocca, G.; Mirelis, J.G. Mapeo miocárdico con resonancia magnética cardiaca: Valor diagnóstico de las nuevas secuencias. Revista Española de Cardiología 2016, 69, 849–861. [Google Scholar] [CrossRef]
- Desch, S.; Eitel, I.; De Waha, S.; Fuernau, G.; Lurz, P.; Gutberlet, M.; Schuler, G.; Thiele, H. Cardiac magnetic resonance imaging parameters as surrogate endpoints in clinical trials of acute myocardial infarction. Trials 2011, 12, 204. [Google Scholar] [CrossRef]
- Khan, J.N.; McCann, G.P. Cardiovascular magnetic resonance imaging assessment of outcomes in acute myocardial infarction. World J. Cardiol. 2017, 9, 109–133. [Google Scholar] [CrossRef]
- Crisostomo, V.; Maestre, J.; Maynar, M.; Sun, F.; Báez-Díaz, C.; Usón, J.; Margallo, F.M.S. Development of a Closed Chest Model of Chronic Myocardial Infarction in Swine: Magnetic Resonance Imaging and Pathological Evaluation. ISRN Cardiol. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bulluck, H.; Hammond-Haley, M.; Weinmann, S.; Martinez-Macias, R.; Hausenloy, D.J. Myocardial Infarct Size by CMR in Clinical Cardioprotection Studies. JACC Cardiovasc. Imaging 2017, 10, 230–240. [Google Scholar] [CrossRef]
- Jablonowski, R.; Engblom, H.; Kanski, M.; Nordlund, D.; Koul, S.; van der Pals, J.; Englund, E.; Heiberg, E.; Erlinge, D.; Carlsson, M.; et al. Contrast-Enhanced CMR Overestimates Early Myocardial Infarct Size. JACC Cardiovasc. Imaging 2015, 8, 1379–1389. [Google Scholar] [CrossRef]
- Makkar, R.R.; Smith, R.R.; Cheng, K.; Malliaras, K.; Thomson, L.E.; Berman, D.; Czer, L.S.; Marbán, L.; Mendizabal, A.; Johnston, P.V.; et al. Intracoronary cardiosphere-derived cells for heart regeneration after myocardial infarction (CADUCEUS): A prospective, randomised phase 1 trial. Lancet 2012, 379, 895–904. [Google Scholar] [CrossRef]
- Hirsch, A.; Nijveldt, R.; Van Der Vleuten, P.A.; Tijssen, J.G.; Van Der Giessen, W.J.; Tio, R.A.; Waltenberger, J.; Berg, J.M.T.; Doevendans, P.A.; Aengevaeren, W.R.; et al. Intracoronary infusion of mononuclear cells from bone marrow or peripheral blood compared with standard therapy in patients after acute myocardial infarction treated by primary percutaneous coronary intervention: Results of the randomized controlled HEBE trial. Eur. Hear. J. 2010, 32, 1736–1747. [Google Scholar] [CrossRef]
- Liu, Y.; Tse, H.-F. The proarrhythmic risk of cell therapy for cardiovascular diseases. Expert Rev. Cardiovasc. Ther. 2011, 9, 1593–1601. [Google Scholar] [CrossRef]
- Menasché, P. Stem Cell Therapy for Heart Failure. Circulation 2009, 119, 2735–2740. [Google Scholar] [CrossRef] [PubMed]
- Ramireddy, A.; Brodt, C.R.; Mendizabal, A.M.; Difede, D.L.; Healy, C.; Goyal, V.; Alansari, Y.; Coffey, J.O.; Viles-Gonzalez, J.F.; Heldman, A.W.; et al. Effects of Transendocardial Stem Cell Injection on Ventricular Proarrhythmia in Patients with Ischemic Cardiomyopathy: Results from the POSEIDON and TAC-HFT Trials. STEM CELLS Transl. Med. 2017, 6, 1366–1372. [Google Scholar] [CrossRef]
- Gómez-Cid, L.; Moro-López, M.; De La Nava, A.S.; Hernández-Romero, I.; Fernández, A.I.; Suárez-Sancho, S.; Atienza, F.; Grigorian-Shamagian, L.; Fernández-Avilés, F. Electrophysiological Effects of Extracellular Vesicles Secreted by Cardiosphere-Derived Cells: Unraveling the Antiarrhythmic Properties of Cell Therapies. Processes 2020, 8, 924. [Google Scholar] [CrossRef]
- Almeida, S.O.; Skelton, R.J.; Adigopula, S.; Ardehali, R. Arrhythmia in Stem Cell Transplantation. Card. Electrophysiol. Clin. 2015, 7, 357–370. [Google Scholar] [CrossRef]
- Azene, N.M.; Ehtiati, T.; Fu, Y.; Flammang, A.; Guehring, J.; Gilson, W.D.; Kedziorek, D.D.; Cook, J.; Johnston, P.V.; Kraitchman, D.L. Intrapericardial delivery of visible microcapsules containing stem cells using xfm (x-ray fused with magnetic resonance imaging). J. Cardiovasc. Magn. Reson. 2011, 13, P26. [Google Scholar] [CrossRef]
- López, E.; Blázquez, R.; Marinaro, F.; Álvarez, V.; Blanco, V.; Báez, C.; González, I.; Abad, A.; Moreno, B.; Sánchez-Margallo, F.M.; et al. The Intrapericardial Delivery of Extracellular Vesicles from Cardiosphere-Derived Cells Stimulates M2 Polarization during the Acute Phase of Porcine Myocardial Infarction. Stem Cell Rev. Rep. 2020, 16, 612–625. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Baseline | Pre-Treatment | Post-Treatment |
|---|---|---|---|
| CON | 0.02 ± 0.01 a | 5.61 ± 2.56 a,b | 2.65 ± 1.69 b |
| CDCs | 0.02 ± 0.01 a | 4.83 ± 2.26 a,b | 3.04 ± 2.06 b |
| APA-CDCs | 0.02 ± 0.02 a | 3.49 ± 2.24 a,b | 2.11 ± 0.93 b |
| Groups | CON | CDCs | APA-CDCs | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | 10 Weeks | Treatment Effect | Pre | 10 Weeks | Treatment Effect | Pre | 10 Weeks | Treatment Effect | |
| LVEF (%) | 27 ± 3 | 29 ± 7 * | 2 ± 7 | 28 ± 5 | 32 ± 8 | 3 ± 9 | 32 ± 7 | 38 ± 6 * | 5 ± 5 |
| IS (%) | 26 ± 7 a | 12 ± 3 a | −13 ± 6 | 21 ± 4 a | 10 ± 4 a | −11 ± 6 | 20 ± 5 a | 11 ± 3 a | −9 ± 4 |
| EDVi (mL/m2) | 93 ± 16 | 99 ± 19 | 6 ± 24 | 84 ± 9 | 89 ± 20 | 5 ± 21 | 87 ± 10 | 94 ± 17 | 8 ± 10 |
| ESVi (mL/m2) | 68 ± 12 | 71 ± 19 | 3 ± 21 | 60 ± 8 | 62 ± 21 | 2 ± 21 | 59 ± 11 | 59 ± 14 | 2 ± 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Báez-Díaz, C.; Blanco-Blázquez, V.; Sánchez-Margallo, F.M.; López, E.; Martín, H.; Espona-Noguera, A.; Casado, J.G.; Ciriza, J.; Pedraz, J.L.; Crisóstomo, V. Intrapericardial Delivery of APA-Microcapsules as Promising Stem Cell Therapy Carriers in an Experimental Acute Myocardial Infarction Model. Pharmaceutics 2021, 13, 1824. https://doi.org/10.3390/pharmaceutics13111824
Báez-Díaz C, Blanco-Blázquez V, Sánchez-Margallo FM, López E, Martín H, Espona-Noguera A, Casado JG, Ciriza J, Pedraz JL, Crisóstomo V. Intrapericardial Delivery of APA-Microcapsules as Promising Stem Cell Therapy Carriers in an Experimental Acute Myocardial Infarction Model. Pharmaceutics. 2021; 13(11):1824. https://doi.org/10.3390/pharmaceutics13111824
Chicago/Turabian StyleBáez-Díaz, Claudia, Virginia Blanco-Blázquez, Francisco Miguel Sánchez-Margallo, Esther López, Helena Martín, Albert Espona-Noguera, Javier G. Casado, Jesús Ciriza, José Luis Pedraz, and Verónica Crisóstomo. 2021. "Intrapericardial Delivery of APA-Microcapsules as Promising Stem Cell Therapy Carriers in an Experimental Acute Myocardial Infarction Model" Pharmaceutics 13, no. 11: 1824. https://doi.org/10.3390/pharmaceutics13111824
APA StyleBáez-Díaz, C., Blanco-Blázquez, V., Sánchez-Margallo, F. M., López, E., Martín, H., Espona-Noguera, A., Casado, J. G., Ciriza, J., Pedraz, J. L., & Crisóstomo, V. (2021). Intrapericardial Delivery of APA-Microcapsules as Promising Stem Cell Therapy Carriers in an Experimental Acute Myocardial Infarction Model. Pharmaceutics, 13(11), 1824. https://doi.org/10.3390/pharmaceutics13111824