Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer




Abstract
1. Introduction
2. Treatment Strategies for Breast Cancer
2.1. Current Treatment Approaches
2.1.1. Therapeutic Options for Luminal Breast Cancer
2.1.2. Treatment Options for HER2-Positive BC
2.1.3. Management of Triple-Negative Breast Cancer (TNBC)
2.2. Novel Treatment Approaches for Breast Cancer by Targeted Therapy
2.2.1. Therapy of Luminal Breast Cancer (LBC)
CDK4/6 Inhibitors
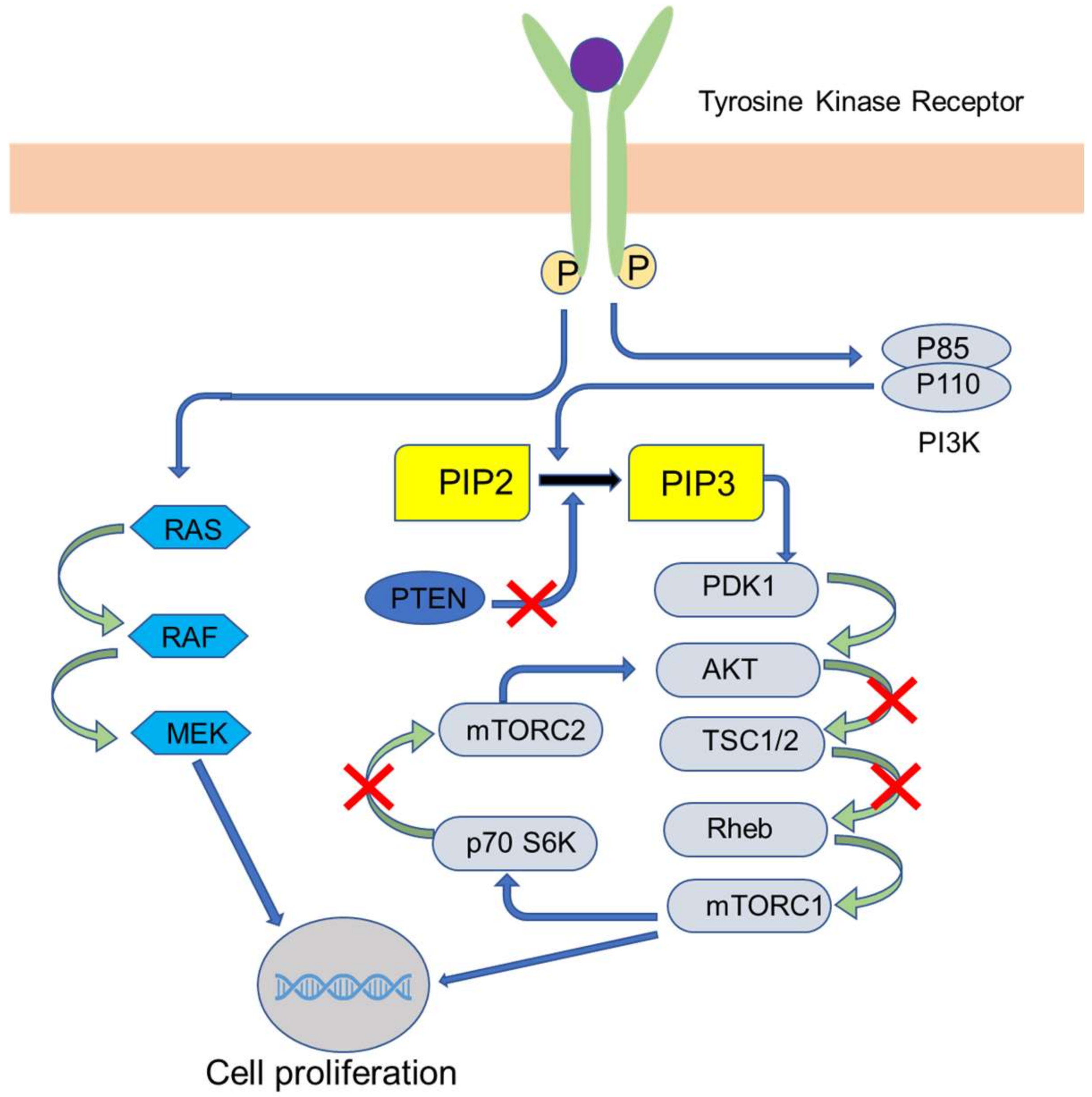
PI3K/AKT/mTOR Pathway Inhibitors
Steroid Sulfatase Inhibitors
2.2.2. Therapy for HER2 Positive Breast Cancers
PI3K/AKT/mTOR Inhibitors
Monoclonal Antibodies (MAbs)
Tyrosine Kinase (TK) Inhibitors
Antibody-Drug Conjugates (ADCs)
Immunotherapy
2.2.3. Therapy of TNBC
Poly (ADP-ribose) Polymerase (PARP) Inhibitors
Anti-Angiogenic Agents
Immunotherapy
Monoclonal Antibody
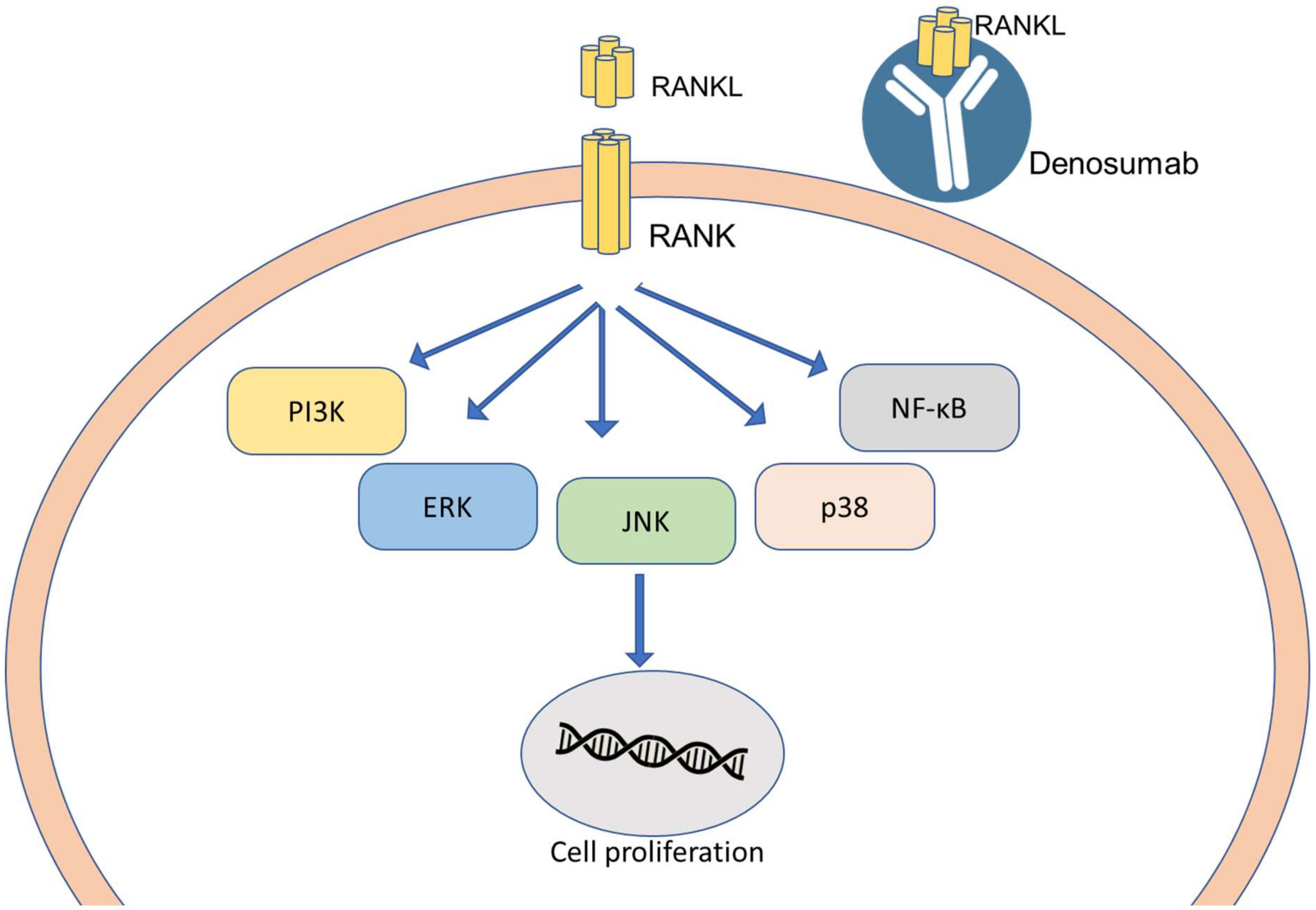
RANKL and RANK System
3. Multidrug-Resistant (MDR) BC
4. Nanomedicine Used in the Management of Breast Cancer
4.1. Polymer-Based Nanoparticles (PBNP)
4.2. Lipid-Based Drug Carriers
4.3. Dendrimers (DM)
4.4. Aptamer
4.5. Inorganic Nanoparticles
4.6. Carbon Nanotubes (CNTs)
4.7. Nanoshells (NSs)
4.8. Viral Nanoparticles
5. Artificial Intelligence in Personalized BC Therapy
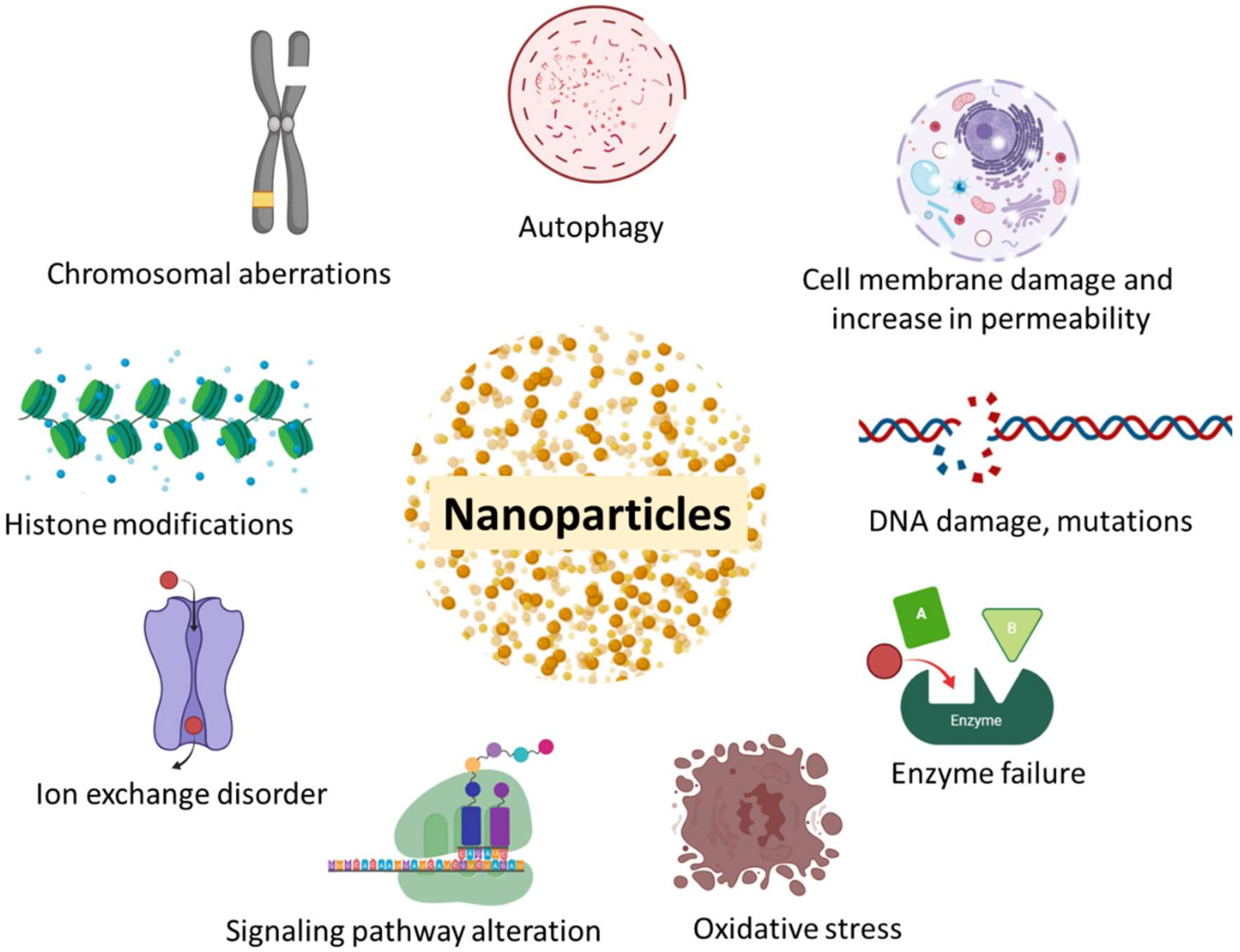
6. Toxicity Associated with Advanced Nano-Based Therapy of BC
7. Summary and Future Perspective
8. Conclusions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019 (US statistics). CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Study Forecasts New Breast Cancer Cases by 2030-National Cancer Institute. Available online: https://www.cancer.gov/news-events/cancer-currents-blog/2015/breast-forecast (accessed on 17 March 2020).
- Polyak, K. Heterogeneity in breast cancer Find the latest version: Review series introduction Heterogeneity in breast cancer. J. Clin. Investig. 2011, 121, 3786–3788. [Google Scholar] [CrossRef] [PubMed]
- Tong, C.W.S.; Wu, M.; Cho, W.C.S.; To, K.K.W. Recent Advances in the Treatment of Breast Cancer. Front. Oncol. 2018, 8, 227. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; Ahmed, S.A.; Inzhakova, G.; Shi, J.; Avila, C.; Polikoff, J.; Bernstein, L.; Enger, S.M.; Press, M.F. Impact of breast cancer subtypes and treatment on survival: An analysis spanning two decades. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Breast Cancer|Breast Cancer Information & Overview. Available online: https://www.cancer.org/cancer/breast-cancer.html (accessed on 17 March 2020).
- Day, C.M.; Hickey, S.M.; Song, Y.; Plush, S.E.; Garg, S. Novel tamoxifen nanoformulations for improving breast cancer treatment: Old wine in new bottles. Molecules 2020, 25, 1182. [Google Scholar] [CrossRef]
- Reinert, T.; Barrios, C.H. Optimal management of hormone receptor positive metastatic breast cancer in 2016. Ther. Adv. Med. Oncol. 2015, 7, 304–320. [Google Scholar] [CrossRef]
- Haque, M.M.; Desai, K.V. Pathways to Endocrine Therapy Resistance in Breast Cancer. Front. Endocrinol. (Lausanne) 2019, 10, 573. [Google Scholar] [CrossRef]
- Szostakowska, M.; Trębińska-Stryjewska, A.; Grzybowska, E.A.; Fabisiewicz, A. Resistance to endocrine therapy in breast cancer: Molecular mechanisms and future goals. Breast Cancer Res. Treat. 2019, 173, 489–497. [Google Scholar] [CrossRef]
- Liedtke, C.; Mazouni, C.; Hess, K.R.; André, F.; Tordai, A.; Mejia, J.A.; Symmans, W.F.; Gonzalez-Angulo, A.M.; Hennessy, B.; Green, M.; et al. Response to neoadjuvant therapy and long-term survival in patients with triple-negative breast cancer. J. Clin. Oncol. 2008, 26, 1275–1281. [Google Scholar] [CrossRef]
- Berrada, N.; Delaloge, S.; André, F. Treatment of triple-negative metastatic breast cancer: Toward individualized targeted treatments or chemosensitization? Ann. Oncol. 2010, 21, vii30–vii35. [Google Scholar] [CrossRef]
- Shah, A.N.; Cristofanilli, M. The Growing Role of CDK4/6 Inhibitors in Treating Hormone Receptor-Positive Advanced Breast Cancer. Curr. Treat. Options Oncol. 2017, 18, 6. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Yu, S.; Liu, Q.; Yuan, X.; Mani, S.; Pestell, R.G.; Wu, K. Recent advances of highly selective CDK4/6 inhibitors in breast cancer. J. Hematol. Oncol. 2017, 10, 97. [Google Scholar] [CrossRef] [PubMed]
- Gelbert, L.M.; Cai, S.; Lin, X.; Sanchez-Martinez, C.; del Prado, M.; Lallena, M.J.; Torres, R.; Ajamie, R.T.; Wishart, G.N.; Flack, R.S.; et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: In-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Investig. New Drugs 2014, 32, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Kwapisz, D. Cyclin-dependent kinase 4/6 inhibitors in breast cancer: Palbociclib, ribociclib, and abemaciclib. Breast Cancer Res. Treat. 2017, 166, 41–54. [Google Scholar] [CrossRef]
- FDA Expands Ribociclib Indication in HR-Positive, HER2-Negative Advanced or Metastatic Breast Cancer|FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-ribociclib-indication-hr-positive-her2-negative-advanced-or-metastatic-breast-cancer (accessed on 6 October 2019).
- FDA Approves Abemaciclib as Initial Therapy for HR-Positive, HER2-Negative Metastatic Breast Cancer|FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-abemaciclib-initial-therapy-hr-positive-her2-negative-metastatic-breast-cancer (accessed on 6 October 2019).
- Palbociclib (IBRANCE)|FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/palbociclib-ibrance (accessed on 6 October 2019).
- Engelman, J.A.; Luo, J.; Cantley, L.C. The evolution of phosphatidylinositol 3-kinases as regulators of growth and metabolism. Nat. Rev. Genet. 2006, 7, 606–619. [Google Scholar] [CrossRef]
- Martini, M.; De Santis, M.C.; Braccini, L.; Gulluni, F.; Hirsch, E. PI3K/AKT signaling pathway and cancer: An updated review. Ann. Med. 2014, 46, 372–383. [Google Scholar] [CrossRef]
- Fruman, D.A.; Chiu, H.; Hopkins, B.D.; Bagrodia, S.; Cantley, L.C.; Abraham, R.T. The PI3K Pathway in Human Disease. Cell 2017, 170, 605–635. [Google Scholar] [CrossRef]
- Slomovitz, B.M.; Coleman, R.L. The PI3K/AKT/mTOR Pathway as a Therapeutic Target in Endometrial Cancer. Clin. Cancer Res. 2012, 18, 5856–5864. [Google Scholar] [CrossRef]
- DiNitto, J.P.; Cronin, T.C.; Lambright, D.G. Membrane recognition and targeting by lipid-binding domains. Sci. STKE 2003, 2003, re16. [Google Scholar] [CrossRef]
- Sarbassov, D.D.; Guertin, D.A.; Ali, S.M.; Sabatini, D.M. Phosphorylation and regulation of Akt/PKB by the rictor-mTOR complex. Science 2005, 307, 1098–1101. [Google Scholar] [CrossRef]
- Polivka, J.; Janku, F. Molecular targets for cancer therapy in the PI3K/AKT/mTOR pathway. Pharmacol. Ther. 2014, 142, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Dowling, R.J.O.; Zakikhani, M.; Fantus, I.G.; Pollak, M.; Sonenberg, N. Metformin inhibits mammalian target of rapamycin-dependent translation initiation in breast cancer cells. Cancer Res. 2007, 67, 10804–10812. [Google Scholar] [CrossRef] [PubMed]
- Barra, F.; Evangelisti, G.; Ferro Desideri, L.; Di Domenico, S.; Ferraioli, D.; Vellone, V.G.; De Cian, F.; Ferrero, S. Investigational PI3K/AKT/mTOR inhibitors in development for endometrial cancer. Expert Opin. Investig. Drugs 2019, 28, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.M.; Dickler, M.N. Estrogen Receptor-Positive Breast Cancer: Exploiting Signaling Pathways Implicated in Endocrine Resistance. Oncologist 2018, 23, 528–539. [Google Scholar] [CrossRef] [PubMed]
- Brufsky, A.M. Long-term management of patients with hormone receptor-positive metastatic breast cancer: Concepts for sequential and combination endocrine-based therapies. Cancer Treat. Rev. 2017, 59, 22–32. [Google Scholar] [CrossRef]
- Tolaney, S.; Burris, H.; Gartner, E.; Mayer, I.A.; Saura, C.; Maurer, M.; Ciruelos, E.; Garcia, A.A.; Campana, F.; Wu, B.; et al. Phase I/II study of pilaralisib (SAR245408) in combination with trastuzumab or trastuzumab plus paclitaxel in trastuzumab-refractory HER2-positive metastatic breast cancer. Breast Cancer Res. Treat. 2015, 149, 151–161. [Google Scholar] [CrossRef]
- Saura, C.; Bendell, J.; Jerusalem, G.; Su, S.; Ru, Q.; De Buck, S.; Mills, D.; Ruquet, S.; Bosch, A.; Urruticoechea, A.; et al. Phase Ib Study of Buparlisib plus Trastuzumab in Patients with HER2-Positive Advanced or Metastatic Breast Cancer That Has Progressed on Trastuzumab-Based Therapy. Clin. Cancer Res. 2014, 20, 1935–1945. [Google Scholar] [CrossRef]
- Guerin, M.; Rezai, K.; Isambert, N.; Campone, M.; Autret, A.; Pakradouni, J.; Provansal, M.; Camerlo, J.; Sabatier, R.; Bertucci, F.; et al. PIKHER2: A phase IB study evaluating buparlisib in combination with lapatinib in trastuzumab-resistant HER2-positive advanced breast cancer. Eur. J. Cancer 2017, 86, 28–36. [Google Scholar] [CrossRef]
- Palmieri, C.; Stein, R.C.; Liu, X.; Hudson, E.; Nicholas, H.; Sasano, H.; Guestini, F.; Holcombe, C. CLINICAL TRIAL IRIS study: A phase II study of the steroid sulfatase inhibitor Irosustat when added to an aromatase inhibitor in ER-positive breast cancer patients. Breast Cancer Res. Treat. 2017, 165, 343–353. [Google Scholar] [CrossRef] [PubMed]
- Morozkina, S.N.; Shavva, G.A. Estrone Sulfatase Inhibitors as New Anticancer Agents. In Chemistry and Biological Activity of Steroids; IntechOpen: London, UK, 2019. [Google Scholar]
- Wisinski, K.B.; Tevaarwerk, A.J.; Burkard, M.E.; Rampurwala, M.; Eickhoff, J.; Bell, M.C.; Kolesar, J.M.; Flynn, C.; Liu, G. Phase I study of an AKT inhibitor (MK-2206) combined with lapatinib in adult solid tumors followed by dose expansion in advanced HER2 + breast cancer. Clin. Cancer Res. 2016, 22, 2659–2667. [Google Scholar] [CrossRef]
- Acevedo-Gadea, C.; Hatzis, C.; Chung, G.; Fishbach, N.; Lezon-Geyda, K.; Zelterman, D.; DiGiovanna, M.P.; Harris, L.; Abu-Khalaf, M.M. Sirolimus and trastuzumab combination therapy for HER2-positive metastatic breast cancer after progression on prior trastuzumab therapy. Breast Cancer Res. Treat. 2015, 150, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Her, W.; Metastatic, T.; Seiler, M.; Ray-coquard, I.; Melichar, B.; Yardley, D.A.; Wang, R.X.; Dodion, P.F.; Lee, M.A. Oral Ridaforolimus Plus Trastuzumab for Patients Breast Cancer. Clin. Breast Cancer 2015, 15, 60–65. [Google Scholar]
- Mukai, H.; Saeki, T.; Aogi, K.; Naito, Y.; Matsubara, N.; Shigekawa, T.; Ueda, S.; Takashima, S.; Hara, F.; Yamashita, T.; et al. Patritumab plus trastuzumab and paclitaxel in human epidermal growth factor receptor 2-overexpressing metastatic breast cancer. Cancer Sci. 2016, 107, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Bahrami, A.; Khazaei, M.; Shahidsales, S.; Hassanian, S.M.; Hasanzadeh, M.; Maftouh, M.; Ferns, G.A.; Avan, A. The Therapeutic Potential of PI3K/Akt/mTOR Inhibitors in Breast Cancer: Rational and Progress. J. Cell. Biochem. 2018, 119, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Hudis, C.A. Trastuzumab—Mechanism of Action and Use in Clinical Practice. N. Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Mitri, Z.; Constantine, T.; O’Regan, R. The HER2 Receptor in Breast Cancer: Pathophysiology, Clinical Use, and New Advances in Therapy. Chemother. Res. Pract. 2012, 2012, 743193. [Google Scholar] [CrossRef]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S.; Li, H.; Ciccarone, V.; Zhang, T.; Stavenhagen, J.; et al. Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. [Google Scholar] [CrossRef]
- Bang, Y.J.; Giaccone, G.; Im, S.A.; Oh, D.Y.; Bauer, T.M.; Nordstrom, J.L.; Li, H.; Chichili, G.R.; Moore, P.A.; Hong, S.; et al. First-in-human Phase 1 study of margetuximab (MGAH22), an Fc-modified chimeric monoclonal antibody, in patients with HER2-positive advanced solid tumors. Ann. Oncol. 2017, 28, mdx002. [Google Scholar] [CrossRef]
- Pento, J.T. Monoclonal Antibodies for the Treatment of Cancer. Anticancer Res. 2017, 37, 5935–5939. [Google Scholar]
- Chan, A.; Delaloge, S.; Holmes, F.A.; Moy, B.; Iwata, H.; Harvey, V.J.; Robert, N.J.; Silovski, T.; Gokmen, E.; von Minckwitz, G.; et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): A multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016, 17, 367–377. [Google Scholar] [CrossRef]
- Dhillon, S. Neratinib in Early-Stage Breast Cancer: A Profile of Its Use in the EU. Clin. Drug Investig. 2019, 39, 221–229. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves Neratinib for Metastatic HER2-Positive Breast Cancer|FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-neratinib-metastatic-her2-positive-breast-cancer (accessed on 17 March 2020).
- Ma, F.; Li, Q.; Chen, S.; Zhu, W.; Fan, Y.; Wang, J.; Luo, Y.; Xing, P.; Lan, B.; Li, M.; et al. Phase I study and biomarker analysis of pyrotinib, a novel irreversible Pan-ERBB receptor tyrosine kinase inhibitor, in patients with human epidermal growth factor receptor 2–positive metastatic breast cancer. J. Clin. Oncol. 2017, 35, 3105–3112. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.H.; Lee, K.-H.; Sohn, J.H.; Lee, K.S.; Jung, K.H.; Kim, J.-H.; Lee, K.H.; Ahn, J.S.; Kim, T.-Y.; Kim, G.M.; et al. A phase II trial of the pan-HER inhibitor poziotinib, in patients with HER2-positive metastatic breast cancer who had received at least two prior HER2-directed regimens: Results of the NOV120101-203 trial. Int. J. Cancer 2018, 143, 3240–3247. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Ma, F.; Ouyang, Q.; Li, W.; Jiang, Z.; Tong, Z.; Liu, Y.; Li, H.; Yu, S.; Feng, J.; et al. Abstract PD3-08: A randomized phase II trial of pyrotinib plus capecitabine versus lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer previously treated with taxanes, anthracyclines and/or trastuzumab. Proc. Poster Discuss. Abstr. Am. Assoc. Cancer Res. 2018, 78, PD3-08. [Google Scholar]
- Moulder, S.L.; Borges, V.F.; Baetz, T.; Mcspadden, T.; Fernetich, G.; Murthy, R.K.; Chavira, R.; Guthrie, K.; Barrett, E.; Chia, S.K. Phase I Study of ONT-380, a HER2 Inhibitor, in Patients with HER2 +—Advanced Solid Tumors, with an Expansion Cohort in HER2+ Metastatic Breast Cancer (MBC). Clin. Cancer Res. 2017, 23, 3529–3536. [Google Scholar] [CrossRef]
- Anders, C.; Murthy, R.; Hamilton, E.; Borges, V.; Cameron, D.; Carey, L.; Müller, V.; Curigliano, G.; Gelmon, K.; Hortobagyi, G.; et al. Abstract CT055: A randomized, double-blinded, controlled study of tucatinib (ONT-380) vs. placebo in combination with capecitabine (C) and trastuzumab (Tz) in patients with pretreated HER2+ unresectable locally advanced or metastatic breast carcinoma (MBC) (HER2CLIMB). Proc. Clin. Trials Am. Assoc. Cancer Res. 2017, 77, CT055. [Google Scholar]
- Tolcher, A.W. Antibody drug conjugates: Lessons from 20 years of clinical experience. Ann. Oncol. 2016, 27, 2168–2172. [Google Scholar] [CrossRef]
- McCombs, J.R.; Owen, S.C. Antibody Drug Conjugates: Design and Selection of Linker, Payload and Conjugation Chemistry. AAPS J. 2015, 17, 339–351. [Google Scholar] [CrossRef]
- Iwata, H.; Tamura, K.; Doi, T.; Tsurutani, J.; Modi, S.; Park, H.; Krop, I.E.; Sagara, Y.; Redfern, C.H.; Murthy, R.K.; et al. Trastuzumab deruxtecan (DS-8201a) in subjects with HER2-expressing solid tumors: Long-term results of a large phase 1 study with multiple expansion cohorts. J. Clin. Oncol. 2018, 36, 2501. [Google Scholar] [CrossRef]
- Tamura, K.; Tsurutani, J.; Takahashi, S.; Iwata, H.; Krop, I.E.; Redfern, C.; Sagara, Y.; Doi, T.; Park, H.; Murthy, R.K.; et al. Trastuzumab deruxtecan (DS-8201a)in patients with advanced HER2-positive breast cancer previously treated with trastuzumab emtansine: A dose-expansion, phase 1 study. Lancet Oncol. 2019, 20, 816–826. [Google Scholar] [CrossRef]
- Van der Lee, M.M.C.; Groothuis, P.G.; Ubink, R.; van der Vleuten, M.A.J.; van Achterberg, T.A.; Loosveld, E.M.; Damming, D.; Jacobs, D.C.H.; Rouwette, M.; Egging, D.F.; et al. The Preclinical Profile of the Duocarmycin-Based HER2-Targeting ADC SYD985 Predicts for Clinical Benefit in Low HER2-Expressing Breast Cancers. Mol. Cancer Ther. 2015, 14, 692–703. [Google Scholar] [CrossRef] [PubMed]
- Menderes, G.; Bonazzoli, E.; Bellone, S.; Black, J.; Altwerger, G.; Masserdotti, A.; Pettinella, F.; Zammataro, L.; Buza, N.; Hui, P.; et al. SYD985, a novel duocarmycin-based HER2-targeting antibody-drug conjugate, shows promising antitumor activity in epithelial ovarian carcinoma with HER2/Neu expression. Gynecol. Oncol. 2017, 146, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, E.P.; Barve, M.A.; Bardia, A.; Beeram, M.; Bendell, J.C.; Mosher, R.; Hailman, E.; Bergstrom, D.A.; Burris, H.A.; Soliman, H.H. Phase 1 dose escalation of XMT-1522, a novel HER2-targeting antibody-drug conjugate (ADC), in patients (pts) with HER2-expressing breast, lung and gastric tumors. J. Clin. Oncol. 2018, 36, 2546. [Google Scholar] [CrossRef]
- Wang, J.; Xu, B.; Wang, W.; Fang, J. An open-label, dose-escalation phase I study to evaluate RC48-ADC, a novel antibody-drug conjugate, in patients with HER2-positive metastatic breast cancer. J. Clin. Oncol. 2018, 36, 1030. [Google Scholar] [CrossRef]
- Pegram, M.; Hamilton, E.; Tan, A.R.; Storniolo, A.M.; Elgeioushi, N.; Marshall, S.; Abdullah, S.; Patel, M. 47OPhase 1 study of bispecific HER2 antibody-drug conjugate MEDI4276 in patients with advanced HER2-positive breast or gastric cancer. Ann. Oncol. 2018, 29. [Google Scholar] [CrossRef]
- Zizzari, I.G.; Veglia, F.; Taurino, F.; Rahimi, H.; Quaglino, E.; Belleudi, F.; Riccardo, F.; Antonilli, M.; Napoletano, C.; Bellati, F.; et al. HER2-based recombinant immunogen to target DCs through FcγRs for cancer immunotherapy. J. Mol. Med. 2011, 89, 1231–1240. [Google Scholar] [CrossRef]
- Liu, L.; Wang, Y.; Miao, L.; Liu, Q.; Musetti, S.; Li, J.; Huang, L. Combination Immunotherapy of MUC1 mRNA Nano-vaccine and CTLA-4 Blockade Effectively Inhibits Growth of Triple Negative Breast Cancer. Mol. Ther. 2018, 26, 45–55. [Google Scholar] [CrossRef]
- Narod, S.A.; Salmena, L. BRCA1 and BRCA2 mutations and breast cancer. Discov. Med. 2011, 12, 445–453. [Google Scholar]
- BRCA: The Breast Cancer Gene-National Breast Cancer Foundation. Available online: https://www.nationalbreastcancer.org/what-is-brca (accessed on 7 October 2019).
- Paul, A.; Paul, S. The breast cancer susceptibility genes (BRCA) in breast and ovarian cancers. Front. Biosci. (Landmark Ed.) 2014, 19, 605–618. [Google Scholar] [CrossRef]
- Chen, H.; Wu, J.; Zhang, Z.; Tang, Y.; Li, X.; Liu, S.; Cao, S.; Li, X. Association between BRCA status and triple-negative breast cancer: A meta-analysis. Front. Pharmacol. 2018, 9, 909. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-Negative Breast Cancer. N. Engl. J. Med. 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [PubMed]
- Nolan, E.; Savas, P.; Policheni, A.N.; Darcy, P.K.; Vaillant, F.; Mintoff, C.P.; Dushyanthen, S.; Mansour, M.; Pang, J.-M.B.; Fox, S.B.; et al. Combined immune checkpoint blockade as a therapeutic strategy for BRCA1 -mutated breast cancer. Sci. Transl. Med. 2017, 9, eaal4922. [Google Scholar] [CrossRef] [PubMed]
- Triple-Negative Breast Cancer Responds to New Dual-Target Therapy. Available online: https://www.medicalnewstoday.com/articles/324107#Triple-negative-breast-cancer (accessed on 31 May 2020).
- Triple-Negative Breast Cancer: Overview, Treatment, and More. Available online: https://www.breastcancer.org/symptoms/diagnosis/trip_neg (accessed on 31 May 2020).
- Mouw, K.W.; Goldberg, M.S.; Konstantinopoulos, P.A.; D’Andrea, A.D. DNA damage and repair biomarkers of immunotherapy response. Cancer Discov. 2017, 7, 675–693. [Google Scholar] [CrossRef] [PubMed]
- Vinayak, S.; Tolaney, S.M.; Schwartzberg, L.S.; Mita, M.M.; McCann, G.A.-L.; Tan, A.R.; Wahner Hendrickson, A.E.; Forero-Torres, A.; Anders, C.K.; Wulf, G.M.; et al. TOPACIO/Keynote-162: Niraparib + pembrolizumab in patients (pts) with metastatic triple-negative breast cancer (TNBC), a phase 2 trial. J. Clin. Oncol. 2018, 36, 1011. [Google Scholar] [CrossRef]
- Galluzzi, L.; Buqué, A.; Kepp, O.; Zitvogel, L.; Kroemer, G. Immunogenic cell death in cancer and infectious disease. Nat. Rev. Immunol. 2017, 17, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Demaria, S.; Volm, M.D.; Shapiro, R.L.; Yee, H.T.; Oratz, R.; Formenti, S.C.; Muggia, F.; Symmans, W.F. Development of tumor-infiltrating lymphocytes in breast cancer after neoadjuvant paclitaxel chemotherapy. Clin. Cancer Res. 2001, 7, 3025–3030. [Google Scholar]
- Li, J.Y.; Duan, X.F.; Wang, L.P.; Xu, Y.J.; Huang, L.; Zhang, T.F.; Liu, J.Y.; Li, F.; Zhang, Z.; Yue, D.L.; et al. Selective depletion of regulatory t cell subsets by docetaxel treatment in patients with nonsmall cell lung cancer. J. Immunol. Res. 2014, 2014, 286170. [Google Scholar] [CrossRef]
- Roselli, M.; Cereda, V.; di Bari, M.G.; Formica, V.; Spila, A.; Jochems, C.; Farsaci, B.; Donahue, R.; Gulley, J.L.; Schlom, J.; et al. Effects of conventional therapeutic interventions on the number and function of regulatory T cells. Oncoimmunology 2013, 2, e27025. [Google Scholar] [CrossRef]
- Kodumudi, K.N.; Woan, K.; Gilvary, D.L.; Sahakian, E.; Wei, S.; Djeu, J.Y. A novel chemoimmunomodulating property of docetaxel: Suppression of myeloid-derived suppressor cells in tumor bearers. Clin. Cancer Res. 2010, 16, 4583–4594. [Google Scholar] [CrossRef]
- Ghiringhelli, F.; Menard, C.; Puig, P.E.; Ladoire, S.; Roux, S.; Martin, F.; Solary, E.; Le Cesne, A.; Zitvogel, L.; Chauffert, B. Metronomic cyclophosphamide regimen selectively depletes CD4+CD25+ regulatory T cells and restores T and NK effector functions in end stage cancer patients. Cancer Immunol. Immunother. 2007, 56, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Kwa, M.; Li, X.; Novik, Y.; Oratz, R.; Jhaveri, K.; Wu, J.; Gu, P.; Meyers, M.; Muggia, F.; Speyer, J.; et al. Serial immunological parameters in a phase II trial of exemestane and low-dose oral cyclophosphamide in advanced hormone receptor-positive breast cancer. Breast Cancer Res. Treat. 2018, 168, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.; Mignot, G.; Chalmin, F.; Ladoire, S.; Bruchard, M.; Chevriaux, A.; Martin, F.; Apetoh, L.; Rebe, C.; Ghiringhelli, F. 5-Fluorouracil Selectively Kills Tumor-Associated Myeloid-Derived Suppressor Cells Resulting in Enhanced T Cell-Dependent Antitumor Immunity. Cancer Res. 2010, 70, 3052–3061. [Google Scholar] [CrossRef] [PubMed]
- Homma, Y.; Taniguchi, K.; Nakazawa, M.; Matsuyama, R.; Mori, R.; Takeda, K.; Ichikawa, Y.; Tanaka, K.; Endo, I. Changes in the immune cell population and cell proliferation in peripheral blood after gemcitabine-based chemotherapy for pancreatic cancer. Clin. Transl. Oncol. 2014, 16, 330–335. [Google Scholar] [CrossRef]
- Huang, X.; Cui, S.; Shu, Y. Cisplatin selectively downregulated the frequency and immunoinhibitory function of myeloid-derived suppressor cells in a murine B16 melanoma model. Immunol. Res. 2016, 64, 160–170. [Google Scholar] [CrossRef]
- Nio, Y.; Hirahara, N.; Minari, Y.; Iguchi, C.; Yamasawa, K.; Toga, T.; Tamura, K. Induction of tumor-specific antitumor immunity after chemotherapy with cisplatin in mice bearing MOPC-104E plasmacytoma by modulation of MHC expression on tumor surface. Anticancer Res. 2000, 20, 3293–3299. [Google Scholar]
- Jackaman, C.; Majewski, D.; Fox, S.A.; Nowak, A.K.; Nelson, D.J. Chemotherapy broadens the range of tumor antigens seen by cytotoxic CD8+ T cells in vivo. Cancer Immunol. Immunother. 2012, 61, 2343–2356. [Google Scholar] [CrossRef]
- Ray Chaudhuri, A.; Nussenzweig, A. The multifaceted roles of PARP1 in DNA repair and chromatin remodelling. Nat. Rev. Mol. Cell Biol. 2017, 18, 610–621. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Timms, K.M.; Abkevich, V.; Hughes, E.; Neff, C.; Reid, J.; Morris, B.; Kalva, S.; Potter, J.; Tran, T.V.; Chen, J.; et al. Association of BRCA1/2 defects with genomic scores predictive of DNA damage repair deficiency among breast cancer subtypes. Breast Cancer Res. 2014, 16, 475. [Google Scholar] [CrossRef]
- Miles, D.W.; Chan, A.; Dirix, L.Y.; Cortés, J.; Pivot, X.; Tomczak, P.; Delozier, T.; Sohn, J.H.; Provencher, L.; Puglisi, F.; et al. Phase III study of bevacizumab plus docetaxel compared with placebo plus docetaxel for the first-line treatment of human epidermal growth factor receptor 2-negative metastatic breast cancer. J. Clin. Oncol. 2010, 28, 3239–3247. [Google Scholar] [CrossRef] [PubMed]
- Nanda, R.; Chow, L.Q.M.; Dees, E.C.; Berger, R.; Gupta, S.; Geva, R.; Pusztai, L.; Pathiraja, K.; Aktan, G.; Cheng, J.D.; et al. Pembrolizumab in Patients With Advanced Triple-Negative Breast Cancer: Phase Ib KEYNOTE-012 Study. J. Clin. Oncol. 2016, 34, 2460. [Google Scholar] [CrossRef] [PubMed]
- Motta, L.L.; Ledaki, I.; Purshouse, K.; Haider, S.; De Bastiani, M.A.; Baban, D.; Morotti, M.; Steers, G.; Wig, S.; Bridges, E.; et al. The BET inhibitor JQ1 selectively impairs tumour response to hypoxia and downregulates CA9 and angiogenesis in triple negative breast cancer. Oncogene 2017, 36, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Gu, Z.; Chen, Y.; Chen, B.; Chen, W.; Weng, L.; Liu, X. Application of PD-1 Blockade in Cancer Immunotherapy. Comput. Struct. Biotechnol. J. 2019, 17, 661–674. [Google Scholar] [CrossRef]
- FDA Approves Atezolizumab for PD-L1 Positive Unresectable Locally Advanced or Metastatic Triple-Negative Breast Cancer|FDA. Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-approves-atezolizumab-pd-l1-positive-unresectable-locally-advanced-or-metastatic-triple-negative (accessed on 7 October 2019).
- Rugo, H.S.; Delord, J.P.; Im, S.A.; Ott, P.A.; Piha-Paul, S.A.; Bedard, P.L.; Sachdev, J.; Le Tourneau, C.; van Brummelen, E.M.J.; Varga, A.; et al. Safety and antitumor activity of pembrolizumab in patients with estrogen receptor–positive/human epidermal growth factor receptor 2–negative advanced breast cancer. Clin. Cancer Res. 2018, 24, 2804–2811. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.; Schmid, P.; Rugo, H.S.; Winer, E.P.; Loirat, D.; Awada, A.; Cescon, D.W.; Iwata, H.; Campone, M.; Nanda, R.; et al. Phase 2 study of pembrolizumab (pembro) monotherapy for previously treated metastatic triple-negative breast cancer (mTNBC): KEYNOTE-086 cohort A. J. Clin. Oncol. 2017, 35, 1008. [Google Scholar] [CrossRef]
- Rose, A.A.N.; Grosset, A.A.; Dong, Z.; Russo, C.; MacDonald, P.A.; Bertos, N.R.; St-Pierre, Y.; Simantov, R.; Hallett, M.; Park, M.; et al. Glycoprotein nonmetastatic B is an independent prognostic indicator of recurrence and a novel therapeutic target in breast cancer. Clin. Cancer Res. 2010, 16, 2147–2156. [Google Scholar] [CrossRef]
- Dirix, L.Y.; Takacs, I.; Jerusalem, G.; Nikolinakos, P.; Arkenau, H.T.; Forero-Torres, A.; Boccia, R.; Lippman, M.E.; Somer, R.; Smakal, M.; et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: A phase 1b JAVELIN solid tumor study. Breast Cancer Res. Treat. 2018, 167, 671–686. [Google Scholar] [CrossRef]
- Wang, X.; Lin, Y. Tumor necrosis factor and cancer, buddies or foes? Acta Pharmacol. Sin. 2008, 29, 1275–1288. [Google Scholar] [CrossRef]
- Gonzalez-Suarez, E.; Branstetter, D.; Armstrong, A.; Dinh, H.; Blumberg, H.; Dougall, W.C. RANK Overexpression in Transgenic Mice with Mouse Mammary Tumor Virus Promoter-Controlled RANK Increases Proliferation and Impairs Alveolar Differentiation in the Mammary Epithelia and Disrupts Lumen Formation in Cultured Epithelial Acini. Mol. Cell. Biol. 2007, 27, 1442. [Google Scholar] [CrossRef]
- Renema, N.; Navet, B.; Heymann, M.-F.; Lezot, F.; Heymann, D. RANK-RANKL signalling in cancer. Biosci. Rep. 2016, 36, e00366. [Google Scholar] [CrossRef]
- Diédhiou, D.; Cuny, T.; Sarr, A.; Norou Diop, S.; Klein, M.; Weryha, G. Efficacy and safety of denosumab for the treatment of osteoporosis: A systematic review. Ann. Endocrinol. (Paris) 2015, 76, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Lochter, A. Plasticity of mammary epithelia during normal development and neoplastic progression. Biochem. Cell Biol. 1998, 76, 997–1008. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zhang, H.; Assaraf, Y.G.; Zhao, K.; Xu, X.; Xie, J.; Yang, D.-H.; Chen, Z.-S. Overcoming ABC transporter-mediated multidrug resistance: Molecular mechanisms and novel therapeutic drug strategies. Drug Resist. Updates 2016, 27, 14–29. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, H.; Chen, X. Drug resistance and combating drug resistance in cancer. Cancer Drug Resist. 2019, 2, 141–160. [Google Scholar] [CrossRef]
- Shen, F.; Bailey, B.J.; Chu, S.; Bence, A.K.; Xue, X.; Erickson, P.; Safa, A.R.; Beck, W.T.; Erickson, L.C. Dynamic assessment of mitoxantrone resistance and modulation of multidrug resistance by valspodar (PSC833) in multidrug resistance human cancer cells. J. Pharmacol. Exp. Ther. 2009, 330, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Aniogo, E.C.; Plackal Adimuriyil George, B.; Abrahamse, H. The role of photodynamic therapy on multidrug resistant breast cancer. Cancer Cell Int. 2019, 19, 91. [Google Scholar] [CrossRef]
- Yang, L.; Li, Y.; Bhattacharya, A.; Zhang, Y. A recombinant human protein targeting HER2 overcomes drug resistance in HER2-positive breast cancer. Sci. Transl. Med. 2019, 11, eaav1620. [Google Scholar] [CrossRef]
- Vadlapatla, R.K.; Pal, D.; Vadlapudi, A.D.; Mitra, A.K. Ritonavir: A Powerful Boosting Agent for Overcoming Drug Resistance in Cancer Chemotherapy. J. Cancer Sci. Ther. 2014, 6, 446–454. [Google Scholar] [CrossRef]
- Allahverdiyev, A.M.; Parlar, E.; Dinparvar, S.; Bagirova, M.; Abamor, E.Ş. Current aspects in treatment of breast cancer based of nanodrug delivery systems and future prospects. Artif. Cells Nanomed. Biotechnol. 2018, 46, S755–S762. [Google Scholar] [CrossRef]
- Dadwal, A.; Baldi, A.; Kumar Narang, R. Nanoparticles as carriers for drug delivery in cancer. Artif. Cells Nanomed. Biotechnol. 2018, 46, 295–305. [Google Scholar] [CrossRef]
- Zhao, L.; Gu, C.; Gan, Y.; Shao, L.; Chen, H.; Zhu, H. Exosome-mediated siRNA delivery to suppress postoperative breast cancer metastasis. J. Control. Release 2020, 318, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Werner, M.E.; Cummings, N.D.; Sethi, M.; Wang, E.C.; Sukumar, R.; Moore, D.T.; Wang, A.Z. Preclinical evaluation of genexol-pm, a nanoparticle formulation of paclitaxel, as a novel radiosensitizer for the treatment of non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C.L. Progress in nanomedicine: Approved and investigational nanodrugs. Pharm. Ther. 2017, 42, 742–755. [Google Scholar]
- Genexol® PM.-Pharmaceuticals-Product Samyang Biopharmaceuticals. Available online: https://www.samyangbiopharm.com/eng/ProductIntroduce/injection01 (accessed on 31 May 2020).
- FDA. ABRAXANE® for Injectable Suspension (Paclitaxel Protein-Bound Particles for Injectable Suspension) (Albumin-Bound). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021660s031lbl.pdf (accessed on 4 June 2020).
- FDA. ABRAXANE ® for Injectable Suspension (Paclitaxel Protein-Bound Particles for Injectable Suspension) (Albumin-Bound) (Patient Information Enclosed) ABRAXANE for Injectable Suspension (Paclitaxel Protein-Bound Particles for. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/021660Orig1s031.pdf (accessed on 4 June 2020).
- Doxoves™—Liposome Doxorubicin Compared to Doxil®. Available online: http://www.liposomeexpert.com/content/FSI%20files/FSI%20products/Doxoves%20-%20Liposome%20Doxorubicin%20Compared%20to%20Doxil.pdf (accessed on 4 June 2020).
- FDA. DOXIL® (Doxorubicin HCl Liposome Injection) for Intravenous Infusion. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2007/050718s029lbl.pdf (accessed on 4 June 2020).
- FDA. DEPOCYT (Cytarabine Liposome Injection). Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/021041s031lbl.pdf (accessed on 4 June 2020).
- DEPOCYT—Cytarabine Injection, Lipid Complex. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021041s023lbl.pdf (accessed on 4 June 2020).
- Panel Recommends FDA Approval of DepoCyt. Available online: https://www.cancernetwork.com/articles/panel-recommends-fda-approval-depocyt (accessed on 4 June 2020).
- Lipodox-FDA. Prescribing Information, Side Effects and Uses. Available online: https://www.drugs.com/pro/lipodox.html (accessed on 31 May 2020).
- Yu, D.S.; Yan, H.Y.; Wu, C.L.; Hung, S.H. Comparison of therapeutic efficacy of lipo-doxorubicin and doxorubicin in treating bladder cancer. Urol. Sci. 2017, 28, 200–205. [Google Scholar] [CrossRef]
- DaunoXome-FDA. Prescribing Information, Side Effects and Uses. Available online: https://www.drugs.com/pro/daunoxome.html (accessed on 31 May 2020).
- DaunoXome® (Daunorubicin Citrate Liposome Injection). Available online: https://hemonc.org/w/images/d/d2/Daunorubicinliposomal.pdf (accessed on 4 June 2020).
- Guo, C.; Chen, Y.; Gao, W.; Chang, A.; Ye, Y.; Shen, W.; Luo, Y.; Yang, S.; Sun, P.; Xiang, R.; et al. Liposomal nanoparticles carrying anti-IL6R antibody to the tumour microenvironment inhibit metastasis in two molecular subtypes of breast cancer mouse models. Theranostics 2017, 7, 775–788. [Google Scholar] [CrossRef]
- Salkho, N.M.; Paul, V.; Kawak, P.; Vitor, R.F.; Martins, A.M.; Al Sayah, M.; Husseini, G.A. Ultrasonically controlled estrone-modified liposomes for estrogen-positive breast cancer therapy. Artif. Cells Nanomed. Biotechnol. 2018, 46, 462–472. [Google Scholar] [CrossRef]
- Zhang, N.; Zhang, J.; Wang, P.; Liu, X.; Huo, P.; Xu, Y.; Chen, W.; Xu, H.; Tian, Q. Investigation of an antitumor drug-delivery system based on anti-HER2 antibody-conjugated BSA nanoparticles. Anticancer Drugs 2018, 29, 307–322. [Google Scholar] [CrossRef]
- Viravaidya-Pasuwat, K.; Naruphontjirakul, P. Development of anti-her2-targeted doxorubicin–core-shell chitosan nanoparticles for the treatment of human breast cancer. Int. J. Nanomed. 2019, 14, 4105–4121. [Google Scholar]
- Kim, B.; Shin, J.; Wu, J.; Omstead, D.T.; Kiziltepe, T.; Littlepage, L.E.; Bilgicer, B. Engineering peptide-targeted liposomal nanoparticles optimized for improved selectivity for HER2-positive breast cancer cells to achieve enhanced in vivo efficacy. J. Control. Release 2020, 322, 530–541. [Google Scholar] [CrossRef]
- Cristofolini, T.; Dalmina, M.; Sierra, J.A.; Silva, A.H.; Pasa, A.A.; Pittella, F.; Creczynski-Pasa, T.B. Multifunctional hybrid nanoparticles as magnetic delivery systems for siRNA targeting the HER2 gene in breast cancer cells. Mater. Sci. Eng. C 2020, 109, 110555. [Google Scholar] [CrossRef] [PubMed]
- Rong, L.; Zhou, S.; Liu, X.; Li, A.; Jing, T.; Liu, X.; Zhang, Y.; Cai, S.; Tang, X. Trastuzumab-modified DM1-loaded nanoparticles for HER2 + breast cancer treatment: An in vitro and in vivo study. Artif. Cells Nanomed. Biotechnol. 2018, 46, 1708–1718. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, B.B.S.; Lasham, A.; Shelling, A.N.; Al-Kassas, R. Development of biodegradable PLGA nanoparticles surface engineered with hyaluronic acid for targeted delivery of paclitaxel to triple negative breast cancer cells. Mater. Sci. Eng. C 2017, 76, 593–600. [Google Scholar] [CrossRef]
- Siddhartha, V.T.; Pindiprolu, S.K.S.S.; Chintamaneni, P.K.; Tummala, S.; Nandha Kumar, S. RAGE receptor targeted bioconjuguate lipid nanoparticles of diallyl disulfide for improved apoptotic activity in triple negative breast cancer: In vitro studies. Artif. Cells Nanomed. Biotechnol. 2018, 46, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Kamalabadi-Farahani, M.; Vasei, M.; Ahmadbeigi, N.; Ebrahimi-Barough, S.; Soleimani, M.; Roozafzoon, R. Anti-tumour effects of TRAIL-expressing human placental derived mesenchymal stem cells with curcumin-loaded chitosan nanoparticles in a mice model of triple negative breast cancer. Artif. Cells Nanomed. Biotechnol. 2018, 46, S1011–S1021. [Google Scholar] [CrossRef] [PubMed]
- Kavithaa, K.; Paulpandi, M.; Padma, P.R.; Sumathi, S. Induction of intrinsic apoptotic pathway and cell cycle arrest: Via baicalein loaded iron oxide nanoparticles as a competent nano-mediated system for triple negative breast cancer therapy. RSC Adv. 2016, 6, 64531–64543. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Ghosh, A.; Maiti, S.; Ahir, M.; Debnath, G.H.; Gupta, P.; Bhattacharjee, M.; Ghosh, S.; Chattopadhyay, S.; Mukherjee, P.; et al. Delivery of thymoquinone through hyaluronic acid-decorated mixed Pluronic® nanoparticles to attenuate angiogenesis and metastasis of triple-negative breast cancer. J. Control. Release 2020, 322, 357–374. [Google Scholar] [CrossRef]
- Ngamcherdtrakul, W.; Morry, J.; Gu, S.; Castro, D.J.; Goodyear, S.M.; Sangvanich, T.; Reda, M.M.; Lee, R.; Mihelic, S.A.; Beckman, B.L.; et al. Cationic Polymer Modified Mesoporous Silica Nanoparticles for Targeted siRNA Delivery to HER2 + Breast Cancer. Adv. Funct. Mater. 2015, 25, 2646–2659. [Google Scholar] [CrossRef]
- Shavi, G.V.; Nayak, U.Y.; Maliyakkal, N.; Deshpande, P.B.; Raghavendra, R.; Kumar, A.R.; Reddya, M.S.; Udupa, N.; Shrawan, B. Nanomedicine of anastrozole for breast cancer: Physicochemical evaluation, in vitro cytotoxicity on BT-549 and MCF-7 cell lines and preclinical study on rat model. Life Sci. 2015, 141, 143–155. [Google Scholar] [CrossRef]
- DeVeaux, S.D.; Gomillion, C.T. Assessing the Potential of Chitosan/Polylactide Nanoparticles for Delivery of Therapeutics for Triple-Negative Breast Cancer Treatment. Regen. Eng. Transl. Med. 2019, 5, 61–73. [Google Scholar] [CrossRef]
- Jin, G.; He, R.; Liu, Q.; Dong, Y.; Lin, M.; Li, W.; Xu, F. Theranostics of Triple-Negative Breast Cancer Based on Conjugated Polymer Nanoparticles. ACS Appl. Mater. Interfaces 2018, 10, 10634–10646. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zhang, P.; Huang, C.; Song, Y.; Garg, S.; Luan, Y. Co-delivery of doxorubicin hydrochloride and verapamil hydrochloride by pH-sensitive polymersomes for the reversal of multidrug resistance. RSC Adv. 2015, 5, 77986–77995. [Google Scholar] [CrossRef]
- Yao, Y.; Saw, P.E.; Nie, Y.; Wong, P.P.; Jiang, L.; Ye, X.; Chen, J.; Ding, T.; Xu, L.; Yao, H.; et al. Multifunctional sharp pH-responsive nanoparticles for targeted drug delivery and effective breast cancer therapy. J. Mater. Chem. B 2019, 7, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Yin, T.; Wang, L.; Yin, L.; Zhou, J.; Huo, M. Biomaterials Co-delivery of hydrophobic paclitaxel and hydrophilic AURKA speci fi c siRNA by redox-sensitive micelles for effective treatment of breast cancer. Biomaterials 2015, 61, 10–25. [Google Scholar] [CrossRef]
- Nima, Z.A.; Watanabe, F.; Jamshidi-Parsian, A.; Sarimollaoglu, M.; Nedosekin, D.A.; Han, M.; Watts, J.A.; Biris, A.S.; Zharov, V.P.; Galanzha, E.I. Bioinspired magnetic nanoparticles as multimodal photoacoustic, photothermal and photomechanical contrast agents. Sci. Rep. 2019, 9, 887. [Google Scholar] [CrossRef]
- Xie, X.; Chen, Y.; Chen, Z.; Feng, Y.; Wang, J.; Li, T.; Li, S.; Qin, X.; Wu, C.; Zheng, C.; et al. Polymeric Hybrid Nanomicelles for Cancer Theranostics: An Efficient and Precise Anticancer Strategy for the Codelivery of Doxorubicin/miR-34a and Magnetic Resonance Imaging. ACS Appl. Mater. Interfaces 2019, 11, 43865–43878. [Google Scholar] [CrossRef]
- Meng, J.; Guo, F.; Xu, H.; Liang, W.; Wang, C.; Yang, X. Combination Therapy using Co-encapsulated Resveratrol and Paclitaxel in Liposomes for Drug Resistance Reversal in Breast Cancer Cells in vivo. Sci. Rep. 2016, 6, 22390. [Google Scholar] [CrossRef]
- Shavi, G.V.; Reddy, M.S.; Raghavendra, R.; Nayak, U.Y.; Kumar, A.R.; Deshpande, P.B.; Udupa, N.; Behl, G.; Dave, V.; Kushwaha, K. PEGylated liposomes of anastrozole for long-term treatment of breast cancer: In vitro and in vivo evaluation. J. Liposome Res. 2016, 26, 28–46. [Google Scholar] [CrossRef]
- Piccolo, M.; Misso, G.; Ferraro, M.G.; Riccardi, C.; Capuozzo, A.; Zarone, M.R.; Maione, F.; Trifuoggi, M.; Stiuso, P.; D’Errico, G.; et al. Exploring cellular uptake, accumulation and mechanism of action of a cationic Ru-based nanosystem in human preclinical models of breast cancer. Sci. Rep. 2019, 9, 7006. [Google Scholar] [CrossRef]
- Kamoun, W.S.; Kirpotin, D.B.; Huang, Z.R.; Tipparaju, S.K.; Noble, C.O.; Hayes, M.E.; Luus, L.; Koshkaryev, A.; Kim, J.; Olivier, K.; et al. Antitumour activity and tolerability of an EphA2-targeted nanotherapeutic in multiple mouse models. Nat. Biomed. Eng. 2019, 3, 264–280. [Google Scholar] [CrossRef]
- Yue, W.; Chen, L.; Yu, L.; Zhou, B.; Yin, H.; Ren, W.; Liu, C.; Guo, L.; Zhang, Y.; Sun, L.; et al. Checkpoint blockade and nanosonosensitizer-augmented noninvasive sonodynamic therapy combination reduces tumour growth and metastases in mice. Nat. Commun. 2019, 10, 2025. [Google Scholar] [CrossRef] [PubMed]
- Yassemi, A.; Kashanian, S.; Zhaleh, H. Folic acid receptor-targeted solid lipid nanoparticles to enhance cytotoxicity of letrozole through induction of caspase-3 dependent-apoptosis for breast cancer treatment. Pharm. Dev. Technol. 2020, 25, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Abd-Ellatef, G.E.F.; Gazzano, E.; Chirio, D.; Hamed, A.R.; Belisario, D.C.; Zuddas, C.; Peira, E.; Rolando, B.; Kopecka, J.; Marie, M.A.S.; et al. Curcumin-loaded solid lipid nanoparticles bypass p-glycoprotein mediated doxorubicin resistance in triple negative breast cancer cells. Pharmaceutics 2020, 12, 96. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Jia, X.; Niu, H. Nanostructured lipid carriers co-delivering lapachone and doxorubicin for overcoming multidrug resistance in breast cancer therapy. Int. J. Nanomed. 2018, 13, 4107–4119. [Google Scholar] [CrossRef]
- Poonia, N.; Kaur Narang, J.; Lather, V.; Beg, S.; Sharma, T.; Singh, B.; Pandita, D. Resveratrol loaded functionalized nanostructured lipid carriers for breast cancer targeting: Systematic development, characterization and pharmacokinetic evaluation. Colloids Surfaces B Biointerfaces 2019, 181, 756–766. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhao, J.; Hu, H.; Yan, Y.; Hu, X.; Zhou, K.; Xiao, S.; Zhang, Y.; Feng, N. Construction and in vitro and in vivo evaluation of folic acid-modified nanostructured lipid carriers loaded with paclitaxel and chlorin e6. Int. J. Pharm. 2019, 569, 118595. [Google Scholar] [CrossRef]
- Liang, T.; Yao, Z.; Ding, J.; Min, Q.; Jiang, L.; Zhu, J.J. Cascaded Aptamers-Governed Multistage Drug-Delivery System Based on Biodegradable Envelope-Type Nanovehicle for Targeted Therapy of HER2-Overexpressing Breast Cancer. ACS Appl. Mater. Interfaces 2018, 10, 34050–34059. [Google Scholar] [CrossRef]
- Ray, S.; Li, Z.; Hsu, C.H.; Hwang, L.P.; Lin, Y.C.; Chou, P.T.; Lin, Y.Y. Dendrimer-and copolymer-based nanoparticles for magnetic resonance cancer theranostics. Theranostics 2018, 8, 6322–6349. [Google Scholar] [CrossRef]
- Nosrati, H.; Adibtabar, M.; Sharafi, A.; Danafar, H. PAMAM-modified citric acid-coated magnetic nanoparticles as pH sensitive biocompatible carrier against human breast cancer cells. Drug Dev. Ind. Pharm. 2018, 44, 1377–1384. [Google Scholar] [CrossRef]
- Kulhari, H.; Pooja, D.; Shrivastava, S.; Kuncha, M.; Naidu, V.G.M.; Bansal, V.; Sistla, R.; Adams, D.J. Trastuzumab-grafted PAMAM dendrimers for the selective delivery of anticancer drugs to HER2-positive breast cancer. Sci. Rep. 2016, 6, 23179. [Google Scholar] [CrossRef]
- Liu, C.; Gao, H.; Zhao, Z.; Rostami, I.; Wang, C.; Zhu, L.; Yang, Y. Improved tumor targeting and penetration by a dual-functional poly(amidoamine) dendrimer for the therapy of triple-negative breast cancer. J. Mater. Chem. B 2019, 7, 3724–3736. [Google Scholar] [CrossRef]
- Torres-Pérez, S.A.; del Ramos-Godínez, M.P.; Ramón-Gallegos, E. Effect of methotrexate conjugated PAMAM dendrimers on the viability of breast cancer cells. AIP Conf. Proc. 2019, 2090, 050014. [Google Scholar]
- Li, N.; Guo, C.; Duan, Z.; Yu, L.; Luo, K.; Lu, J.; Gu, Z. A stimuli-responsive Janus peptide dendron-drug conjugate as a safe and nanoscale drug delivery vehicle for breast cancer therapy. J. Mater. Chem. B 2016, 4, 3760–3769. [Google Scholar] [CrossRef]
- Wang, Y.M.; Wu, Z.; Liu, S.J.; Chu, X. Structure-Switching Aptamer Triggering Hybridization Chain Reaction on the Cell Surface for Activatable Theranostics. Anal. Chem. 2015, 87, 6470–6474. [Google Scholar] [CrossRef]
- Hasanzadeh, M.; Razmi, N.; Mokhtarzadeh, A.; Shadjou, N.; Mahboob, S. Aptamer based assay of plated-derived grow factor in unprocessed human plasma sample and MCF-7 breast cancer cell lysates using gold nanoparticle supported α-cyclodextrin. Int. J. Biol. Macromol. 2018, 108, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Wu, X.; Yang, H.; Li, L.; Ye, Z.; Rao, Y. A nuclear targeted Dox-aptamer loaded liposome delivery platform for the circumvention of drug resistance in breast cancer. Biomed. Pharmacother. 2019, 117, 109072. [Google Scholar] [CrossRef] [PubMed]
- Duan, T.; Xu, Z.; Sun, F.; Wang, Y.; Zhang, J.; Luo, C.; Wang, M. HPA aptamer functionalized paclitaxel-loaded PLGA nanoparticles for enhanced anticancer therapy through targeted effects and microenvironment modulation. Biomed. Pharmacother. 2019, 117, 109121. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Wu, J.; Gao, H.; Hu, X.; Liu, L.; Midgley, A.C.; Liu, Q.; Sun, Z.; Liu, Y.; Ding, D.; et al. Hypoxia-tropic nanozymes as oxygen generators for tumor-favoring theranostics. Biomaterials 2020, 230, 119635. [Google Scholar] [CrossRef]
- Siminzar, P.; Omidi, Y.; Golchin, A.; Aghanejad, A.; Barar, J. Targeted delivery of doxorubicin by magnetic mesoporous silica nanoparticles armed with mucin-1 aptamer. J. Drug Target. 2020, 28, 92–101. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.; Lim, S.C.; Lim, K.; Lee, E.S.; Oh, K.T.; Choi, H.G.; Youn, Y.S. Gold nanocluster-loaded hybrid albumin nanoparticles with fluorescence-based optical visualization and photothermal conversion for tumor detection/ablation. J. Control. Release 2019, 304, 7–18. [Google Scholar] [CrossRef]
- Choi, G.; Kwon, O.; Oh, Y.; Yun, C.; Choy, J. Inorganic Nanovehicle Targets Tumor in an Orthotopic Breast Cancer Model. Sci. Rep. 2014, 4, 4430. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Qian, J.; Hou, G.; Wang, Y.; Wang, J.; Sun, T.; Ji, L.; Suo, A.; Yao, Y. A dual-targeted hyaluronic acid-gold nanorod platform with triple-stimuli responsiveness for photodynamic/photothermal therapy of breast cancer. Acta Biomater. 2019, 83, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Xu, Q.; Li, X.; Zhang, P.; Zhao, X.; Wang, Y. Redox-responsive hyaluronic acid nanogels for hyperthermia- assisted chemotherapy to overcome multidrug resistance. Carbohydr. Polym. 2019, 203, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Crawford, L.J.; Walker, B.; Irvine, A.E. Proteasome inhibitors in cancer therapy. J. Cell Commun. Signal. 2011, 5, 101–110. [Google Scholar] [CrossRef]
- Gu, Y.; Bouwman, P.; Greco, D.; Saarela, J.; Yadav, B.; Jonkers, J.; Kuznetsov, S.G. Suppression of BRCA1 sensitizes cells to proteasome inhibitors. Cell Death Dis. 2014, 5, e1580. [Google Scholar] [CrossRef]
- Gu, S.; Hu, Z.; Ngamcherdtrakul, W.; Castro, D.J.; Morry, J.; Reda, M.M.; Gray, J.W.; Yantasee, W. Therapeutic siRNA for drug-resistant HER2-positive breast cancer. Oncotarget 2016, 7, 14727–14741. [Google Scholar] [CrossRef]
- Parmar, M.B.; Bahadur K.C., R.; Löbenberg, R.; Uludağ, H. Additive Polyplexes to Undertake siRNA Therapy against CDC20 and Survivin in Breast Cancer Cells. Biomacromolecules 2018, 19, 4193–4206. [Google Scholar] [CrossRef]
- Gao, Y.; Zhang, L.; Liu, Y.; Sun, S.; Yin, Z.; Zhang, L.; Li, A.; Lu, G.; Wu, A.; Zeng, L. Ce6/Mn2+-chelated polydopamine@black-TiO2 nanoprobes for enhanced synergistic phototherapy and magnetic resonance imaging in 4T1 breast cancer. Nanoscale 2020, 12, 1801–1810. [Google Scholar] [CrossRef]
- Li, L.; Lu, Y.; Jiang, C.; Zhu, Y.; Yang, X.; Hu, X.; Lin, Z. Actively Targeted Deep Tissue Imaging and Photothermal-Chemo Therapy of Breast Cancer by Antibody-Functionalized Drug-Loaded X-Ray-Responsive Bismuth Sulfide @ Mesoporous Silica Core–Shell Nanoparticles. Adv. Funct. Mater. 2018, 28, 1704623. [Google Scholar] [CrossRef]
- Sayed, A.; Halwani, R. Specific targeting and noninvasive imaging of breast cancer stem cells using single-walled carbon nanotubes as novel multimodality nanoprobes. Nanomedicine 2016, 11, 31–46. [Google Scholar]
- Yu, S.; Zhang, Y.; Chen, L.; Li, Q.; Du, J.; Gao, Y.; Zhang, L.; Yang, Y. Antitumor effects of carbon nanotube-drug complex against human breast cancer cells. Exp. Ther. Med. 2018, 16, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Mehra, N.K.; Jain, N.K. Development and Characterization of the Paclitaxel loaded Riboflavin and Thiamine Conjugated Carbon Nanotubes for Cancer Treatment. Pharm. Res. 2016, 33, 1769–1781. [Google Scholar] [CrossRef] [PubMed]
- Morton, J.G.; Day, E.S.; Halas, N.J.; West, J.L. Nanoshells for photothermal cancer therapy. Methods Mol. Biol. 2010, 624, 101–117. [Google Scholar] [PubMed]
- Ramasamy, T.; Ruttala, H.B.; Sundaramoorthy, P.; Poudel, B.K.; Youn, Y.S.; Ku, S.K.; Choi, H.; Yong, C.S.; Kim, J.O. Multimodal selenium nanoshell-capped Au@mSi 2 nanoplatform for NIR-responsive chemo-photothermal therapy against metastatic breast cancer. NPG Asia Mater. 2018, 10, 197–216. [Google Scholar] [CrossRef]
- Nunes, T.; Pons, T.; Hou, X.; Van Do, K.; Caron, B.; Rigal, M.; Di Benedetto, M.; Palpant, B.; Leboeuf, C.; Janin, A.; et al. Pulsed-laser irradiation of multifunctional gold nanoshells to overcome trastuzumab resistance in HER2-overexpressing breast cancer. J. Exp. Clin. Cancer Res. 2019, 38, 306. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, D.S.; Reddy, B.P.K.; Mishra, S.K.; Prasad, R.; Dhanka, M.; Vats, M.; Ravichandran, G.; Poojari, D.; Mhatre, O.; De, A.; et al. Comprehensive Evaluation of Degradable and Cost-Effective Plasmonic Nanoshells for Localized Photothermolysis of Cancer Cells. Langmuir 2019, 35, 7805–7815. [Google Scholar] [CrossRef]
- Esfandiari, N. Targeting Breast Cancer With Bio-inspired Virus Nanoparticles. Arch. Breast Cancer 2018, 5, 90–95. [Google Scholar]
- Esfandiari, N.; Arzanani, M.K.; Soleimani, M. A new application of plant virus nanoparticles as drug delivery in breast cancer. Tumor Biol. 2016, 37, 1229–1236. [Google Scholar] [CrossRef]
- Bruckman, M.A.; Czapar, A.E.; VanMeter, A.; Randolph, L.N.; Steinmetz, N.F. Tobacco mosaic virus-based protein nanoparticles and nanorods for chemotherapy delivery targeting breast cancer. J. Control. Release 2016, 231, 103–113. [Google Scholar] [CrossRef]
- AI Reveals New Breast Cancer Types That Respond Differently to Treatment. Available online: https://www.sciencedaily.com/releases/2019/08/190802131354.htm (accessed on 4 June 2020).
- Ho, D.; Wang, P.; Kee, T. Artificial intelligence in nanomedicine. Nanoscale Horiz. 2019, 4, 365–377. [Google Scholar] [CrossRef]
- Adir, O.; Poley, M.; Chen, G.; Froim, S.; Krinsky, N.; Shklover, J.; Shainsky-Roitman, J.; Lammers, T.; Schroeder, A. Integrating Artificial Intelligence and Nanotechnology for Precision Cancer Medicine. Adv. Mater. 2020, 32, 1901989. [Google Scholar] [CrossRef] [PubMed]
- Marcu, L.G.; Boyd, C.; Bezak, E. Current issues regarding artificial intelligence in cancer and health care. Implications for medical physicists and biomedical engineers. Health Technol. (Berl.) 2019, 9, 375–381. [Google Scholar] [CrossRef]
- Crisponi, G.; Nurchi, V.M.; Lachowicz, J.I.; Peana, M.; Medici, S.; Zoroddu, M.A. Toxicity of Nanoparticles: Etiology and Mechanisms. In Antimicrobial Nanoarchitectonics: From Synthesis to Applications; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 511–546. ISBN 9780323527347. [Google Scholar]
- Khan, I.; Saeed, K.; Khan, I. Nanoparticles: Properties, applications and toxicities. Arab. J. Chem. 2019, 12, 908–931. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-related adverse events associated with immune checkpoint blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Gambichler, T.; Strutzmann, S.; Tannapfel, A.; Susok, L. Paraneoplastic acral vascular syndrome in a patient with metastatic melanoma under immune checkpoint blockade. BMC Cancer 2017, 17, 327. [Google Scholar] [CrossRef]
- What Is Gene Therapy?|OncoLink. Available online: https://www.oncolink.org/cancer-treatment/immunotherapy/what-is-gene-therapy (accessed on 14 February 2020).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Agent | Cyclin-Dependent Kinase IC50 (in nM) | |
|---|---|---|
| CDK6 | CDK4 | |
| Ribociclib | 39 | 10 |
| Palbociclib | 15 | 11 |
| Abemaciclib | 9.9 | 2 |
| Drug | Combination With | Description | ClinicalTrials.Gov Identifier NCT Number | Phase |
|---|---|---|---|---|
| Palbociclib | Endocrine therapy (exemestane, fulvestrant, letrozole, tamoxifen) Chemotherapy (capecitabine, epirubicin, paclitaxel, vinorelbine) | To evaluate/compare palbociclib in combination with endocrine therapeutic agents and with chemotherapeutic agents in HER2-positive or HER2-negative metastatic BC patients | NCT03355157 | IV |
| Palbociclib | Fulvestrant, exemestane, letrozole, anastrozole | To evaluate eHealth-support in locally advanced or metastatic BC patient’s life quality when treated with palbociclib with endocrine therapy | NCT03220178 | IV |
| Ribociclib | Endocrine therapy | To study the effectiveness of ribociclib with endocrine therapy in the ER-positive BC patients | NCT03285412 | II |
| Ribociclib | Letrozole/anastrozole, goserelin | To evaluate the safety and efficacy of 400 mg of ribociclib when given in combination with aromatase inhibitors in the post- and pre-menopausal women with HR-positive/HR-negative patients with advanced BC | NCT03822468 | II |
| Ribociclib | Letrozole 2.5 mg, doxorubicin, cyclophosphamide, paclitaxel | To evaluate the efficacy and safety of ribociclib (LEE011) with multi-agent chemotherapy or letrozole in postmenopausal patients with luminal B/HER2 negative BC | NCT03248427 | II |
| Ribociclib | Non-steroidal aromatase inhibitors- letrozole 2.5 mg/day or anastrozole 1 mg/day orally, LHRH agonist-triptorelin 3.75 mg or leuprolide 3.75 mg or goserelin 3.6 mg, as injectable | Ribociclib in combination with a non-steroidal aromatase inhibitor/LHRH agonist in HR-Positive/HER2-negative patients with advanced BC | NCT03944434 | II |
| Ribociclib | PDR001, fulvestrant | Ribociclib (LEE011), in combination with PDR001 an immunotherapeutic drug and fulvestrant in HR-positive, HER2-negative patient for metastatic hormone-receptor-positive (HR+), HER2-negative BC. | NCT03294694 | I |
| Ribociclib (LEE011) | Paclitaxel | To assess the safety and dose escalation of paclitaxel with ribociclib in retinoblastoma (Rb)-positive patients with advanced BC. | NCT02599363 | I |
| Abemaciclib | Fulvestrant | To compare the effectiveness of combination therapy of abemaciclib with fulvestrant and chemotherapy in HR-positive, HER2-negative patients with metastatic BC (visceral Metastases) | NCT04031885 | IV |
| Abemaciclib | Fulvestrant | To compare fulvestrant alone with a combination of fulvestrant and abemaciclib in progression-free survival in HR-positive and HER2-negative patients. | NCT02107703 | III |
| Abemaciclib | Atezolizumab (MPDL3280A), bevacizumab, entinostat, exemestane, fulvestrant, ipatasertib, tamoxifen | To evaluate the safety, efficacy, and pharmacokinetics of immunotherapy-based combination with CDK 4/6 inhibitor and anti-estrogen agents in advanced or metastatic HR-positive and HER2-negative patients. | NCT03280563 | I |
| Receptor | Drugs | Mechanism of Action |
|---|---|---|
| PI3K | Taselisib (GDC0032), pilaralisib (XL147), alpelisib (BYL719), buparlisib (BKM120), pictilisib (GDC0941), MLN1117 | PI3K inhibition |
| AKT | Capivasertib (AZD5363), uprosertib (GSK2141795), miransertib (ARQ092), MK2206 | Inhibition of AKT 1,2,3 isoforms |
| mTORC1 | Sirolimus, ridaforolimus, everolimus, temsirolimus | Allosteric inhibition of mTORC1 |
| PI3K and mTOR | Dactolisib (NVP-BEZ235), gedatolisib (PF05212384), LY3023414 | Dual inactivation of PI3K and mTOR |
| mTORC1 and mTORC2 | Vistusertib (AZD2014), sapanisertib (TAK-228), CC-223, AZD8055, MLN0138, | Allosteric inhibition of mTORC1 and mTORC2 |
| Drug | Combination With | Study Arm | Description | ClinicalTrials.Gov Identifier: NCT Number | Phase |
|---|---|---|---|---|---|
| Taselisib | Taselisib, trastuzumab emtansine, pertuzumab, trastuzumab paclitaxel | Arm A: Taselisib with trastuzumab emtansine Arm B: Taselisib with trastuzumab emtansine and pertuzumab Arm C: Taselisib with pertuzumab and trastuzumab Arm D: Taselisib with pertuzumab, trastuzumab, and paclitaxel | Combination of taselisib (GDC-0032) with anti-HER2 therapies in participants with advanced HER2+ breast cancer—a Phase Ib dose-escalation trial | NCT02390427 | Ib |
| Pilaralisib (XL147) | Letrozole (Femara) | Arm A: Pilaralisib with letrozole | A Phase 1/2 dose-escalation study of XL147 (SAR245408), or XL765 (SAR245409) in combination with letrozole performed on subjects with hormone receptor-positive and HER2-negative breast cancer refractory to a nonsteroidal aromatase inhibitor | NCT01082068 | Completed |
| Pilaralisib (XL147) | Trastuzumab, Paclitaxel | Arm A: Pilaralisib with trastuzumab Arm B: Pilaralisib with trastuzumab and paclitaxel | To study the efficacy of a combination of pilaralisib with trastuzumab or paclitaxel and trastuzumab in patients with metastatic -BC | NCT01042925 | Completed |
| Alpelisib (BYL719) | Fulvestrant | Arm A: Alpelisib (300 mg; oral; once daily with fulvestrant (500 mg; IM-injection) | To assess the safety and efficacy in men and postmenopausal women patients with advanced-BC | NCT02437318 | III |
| Alpelisib | Fulvestrant | Arm A: Alpelisib 300 mg oral daily with fulvestrant 500 mg intramuscular on in first cycle 1st day and 15th day, and thereafter every 28-day cycle. | To study the molecular features in HR-positive and HER2-negative postmenopausal women with a PIK3CA mutation | NCT03439046 | III |
| MK2206 | Arm A: MK-2206 mg orally once a week | To study the efficacy of MK2206, an AKT inhibitor in patients with advanced BC and having AKT mutation and/or PTEN Loss/PTEN mutation and/or PIK3CA mutation | NCT01277757 | Completed | |
| Everolimus, | Letrozole, everolimus, TRC105 | Arm A: Letrozole 2.5 mg + everolimus 5 mg + TRC105 15 mg/kg i.v Arm B: Letrozole 2.5 mg + everolimus 10 mg + TRC105 15 mg/kg i.v Arm C: Letrozole 2.5 mg + everolimus 5 mg + 10 mg/kg i.v Arm D: Letrozole 2.5 mg + 5 or 10 mg + TRC105 15 or 10 mg/kg i.v. | To study how well a combination of letrozole, TRC105 everolimus works in patients with stage 2 and 3 BC, and how well it is tolerated | NCT02520063 | I/II |
| Everolimus | Palbociclib, exemestane | Palbociclib, everolimus, exemestane are administered in a cycle of 28 days | To study the efficacy of a combination of palbociclib, everolimus, exemestane in HR-positive and HER2-negative patients with metastatic-BC | NCT02871791 | I/II |
| Temsirolimus | Bevacizumab, cetuximab valproic acid | Arm A: Temsirolimus, bevacizumab, cetuximab Arm B: Temsirolimus, bevacizumab, valproic acid Arm C: temsirolimus, bevacizumab | To study the efficacy of bevacizumab and temsirolimus alone or combination with valproic acid or cetuximab in patients with advanced or metastatic- BC | NCT01552434 | I |
| Gedatolisib (PF05212384) | Trastuzumab biosimilar (herzuma) | Arm A: Herzuma + Gedatolisib | To evaluate the safety and antitumor activity of Herzuma® with gedatolisib in HER-2 positive patients with metastatic-BC | NCT03698383 | II |
| Vistusertib (AZD2014) | Palbociclib, fulvestrant | Arm A: A triple combination of AZD2014 + palbociclib +fulvestrant | To study the efficacy of a combination of AZD2014, palbociclib, fulvestrant, in ER-positive patients with metastatic-BC | NCT02599714 | I |
| Drug | Combination With | Study Arm | Description | ClinicalTrials.Gov Identifier: NCT Number | Phase |
|---|---|---|---|---|---|
| Cisplatin | Romidepsin, nivolumab | Arm A: cisplatin (75 mg/m2) + romidepsin (8 mg/m2) Arm B: romidepsin (10 mg/m2) + cisplatin (75 mg/m2) Arm C: romidepsin (12 mg/m2) + cisplatin (75 mg/m2) Arm D: romidepsin MTD (maximum tolerable dose) + cisplatin (75 mg/m2) + nivolumab 360 mg | To study the efficacy of cisplatin in combination with romidepsin and nivolumab in patients with TNBC or BRCA mutation or metastatic-BC | NCT02393794 | I/II |
| MM-310 | Arm A: MM-310 i.v., 21-day cycle. | MM-310 is a docetaxel loaded liposomal formulation with targeting ability of EphA2 receptor. In this study, safety and efficacy of MM-310 in patients with TNBC was studied | NCT03076372 | I | |
| Carboplatin | Everolimus | Arm A: Carboplatin alone Arm B: Carboplatin + everolimus | To study the safety and efficacy of carboplatin alone and carboplatin in combination with everolimus in patients with advanced TNBC | NCT02531932 | II |
| Leronlimab | Carboplatin | Arm A: leronlimab (350 mg) + AUC 5 carboplatin Arm B: leronlimab (525 mg) + AUC 5 carboplatin Arm C: leronlimab (700 mg) + AUC 5 carboplatin Arm D: leronlimab (MTD) + AUC 5 carboplatin | To study the safety and efficacy of leronlimab when given in combination carboplatin in the patients with advanced TNBC | NCT03838367 | Ib/II |
| Nab-Paclitaxel | Mifepristone | Arm A: nab-paclitaxel 100 mg + mifepristone 300 mg Arm B: nab-paclitaxel 100 mg + placebo | To study the efficacy of Nab-paclitaxel alone and in combination with mifepristone in the glucocorticoid receptor-positive and TNBC patients | NCT02788981 | II |
| L-NMMA | Docetaxel amlodipine pegfilgrastim Enteric-coated aspirin | Arm A: L-NMMA + docetaxel + amlodipine + pegfilgrastim + Enteric-coated aspirin | To study the L-NMMA’s MTD, dose-limiting toxicities and to find out the efficacy in combination with docetaxel in patients with advanced TNBC | NCT02834403 | Ib/II |
| Mirvetuximab soravtansine | Gemcitabine hydrochloride | Arm A: mirvetuximab soravtansine + gemcitabine hydrochloride | To study the dose-escalation, tolerability safety and efficacy of mirvetuximab soravtansine in combination with gemcitabine hydrochloride in patients with folate receptor-positive ovarian and TNBC | NCT02996825 | I |
| Atezolizumab | Paclitaxel | Arm A: atezolizumab (840 mg) and paclitaxel (90 mg/m2) Arm B: placebo and paclitaxel (90 mg/m2) | To study the efficacy of a combination of a PD-L1-antibody, atezolizumab, and paclitaxel in advanced TNBC patients | NCT03125902 | III |
| Tak-228 | Tak-117 Cisplatin Nab-Paclitaxel | Arm A: Tak-228 and Tak-117 followed by cisplatin and nab-paclitaxel | To study the efficacy of TAK- 228 and TAK- 117 treatment followed by cisplatin and nab-paclitaxel treatment in patients with metastatic TNBC | NCT03193853 | II |
| Onalespib | paclitaxel | Arm A: onalespib (i.v.) on day 7 + paclitaxel (i.v.) days 1, 8, and 15; 28-day cycle | To study the best dose and side effects of onalespib when given in combination with paclitaxel in advanced TNBC patients | NCT02474173 | I |
| Product | Drug | Company | Nanoparticle | Composition | Particle Size | Indication | Approval by US FDA and others | Reference |
|---|---|---|---|---|---|---|---|---|
| Genexol-PM | Paclitaxel | Samyang/Biopharm | PEG-PLA polymeric micelle | Paclitaxel, monomethoxy poly (ethylene glycol)-block-poly (D,L- lactide) | 23.91 nm | Breast, lung, ovarian cancer | 2007 (South Korea) | [114,115,116] |
| Abraxane | Paclitaxel | Abraxis/Celgene | Nanoparticle-bound albumin | Paclitaxel, human albumin | 130 nm | In breast, pancreatic and non-small cell lung cancer | 2005 | [117,118] |
| Doxil | Doxorubicin | Johnson and Johnson | Liposome | N-(carbonyl-methoxypolyethylene glycol 2000)-1,2-distearoyl-sn-glycero-3-phosphoethanolamine sodium salt (DSPE-PEG 2000), hydrogenated soy phosphatidylcholine, and cholesterol | 85 nm | Kaposi’s sarcoma Ovarian cancer Breast cancer Multiple myeloma | 1995 1999 2003 2007 (Europe, Canada) | [119,120] |
| Myocet | Doxorubicin | Cephalon | Liposome | Egg phosphatidylcholine and cholesterol with Doxorubicin citric acid aqueous core | 190 nm | Breast cancer | 2000 (EU) | [119,120] |
| Depocyt | Cytarabine | Pacira | Liposome | Cholesterol, glycerol trioleate, triglyceride, phospholipids (dipalmitoyl phosphatidylglycerol), and dioleoyl phosphatidylcholine | 20 µm | Neoplastic meningitis | 1999 | [121,122,123] |
| Lipo-Dox | Doxorubicin | Taiwan Liposome | Liposome | Cholesterol, N-(carbonyl-ethoxypolyethylene glycol 2000)-1,2-distearoyl-sn-glycero-3-phosphoethanolamine, hydrogenated soybean lecithin | 104.2 nm | Breast, ovarian cancer | 1998 (Taiwan) | [124,125] |
| DaunoXome | Daunorubicin | Galen | Liposome | Cholesterol, distearoylphosphatidylcholine | 45 nm | Kaposi’s sarcoma | 1996 | [126,127] |
| Nanoparticle Type | Type of Breast Cancer | Therapeutic Agent | Materials Used | Entrapment Efficiency (EE) and Particle Size | Key Outcome | Reference |
|---|---|---|---|---|---|---|
| Liposomes | luminal breast cancer | Anti-IL6R antibody, Doxorubicin | Cholesterol, 1,2-dioleoyl-sn-glycero-3-phosphoethanolamine 1,2-dioleoyl-sn-glycero-3-phosphocholine In (1:1:1 molar ratio) | 85.81% ± 0.4799% to 89.03% ± 0.143%, ∼100 nm | Formulation showed an enhanced tumor targeting efficacy with anti-tumor metastasis effects in BALB/c mice bearing 4T1 cells | [128] |
| Liposomes | Luminal breast cancer- Estrogen positive BC | Doxorubicin | Estrone conjugated DPPC and DSPE-PEG2000-NH2 liposomes | EE not reported, 194 nm | Formulations showed significant uptake in ER-positive (MCF-7) and non- significant uptake in ER-negative (MDA-MB-231) cell lines | [129] |
| Albumin nanoparticles | HER2 positive BC | 2-methoxy-estradiol | Bovine serum albumin | 89.85% ± 3.80% to 88.70% ± 2.95%, ∼238.8 ± 5.1 nm | Formulated NPs showed enhanced cytotoxicity and cellular uptake when compared with the free drug when assessed in SK-BR-3 and MCF-7 cell line and SK-BR-3, MCF-7 tumor-bearing mice | [130] |
| chitosan nanoparticles | HER2 positive BC | doxorubicin | O-succinyl chitosan graft Pluronic® F127 and 5% to 10% anti-HER2 peptide | 73.69% ± 0.53% to 74.65% ± 0.44%, 34.92 to 50.79 nm | In vitro cytotoxicity and cellular-uptake study were performed on MCF-7 cell line which showed that the NP conjugated with anti-HER2 showed higher cytotoxicity when compared with free drug | [131] |
| liposomal | HER2 positive BC | doxorubicin | HER2pep-K3-palmitic acid conjugate, DSPC, mPEG2000-DSPE | >98%, ~80 nm | In vitro cytotoxicity and cellular-uptake studies were performed on BT-474, SK-BR-3 and MCF-7. The formulation showed higher cytotoxicity and cellular uptake with lower systemic toxicity when compared with free drug | [132] |
| Iron oxide | HER2 positive BC | siRNA | Iron oxide, caffeic acid, calcium phosphate and PEG-polyanion block copolymer | EE not reported, 130 nm | In vitro cytotoxicity and cellular-uptake studies were performed on HCC1954. After treating with NP, HER2 mRNA expression was decreased by 38% when compared with naked siRNA | [133] |
| Polymeric nanoparticles | HER2 positive BC | Emtansine | D-α-tocopheryl polyethylene glycol 1000 succinate-poly (D, L-lactide) | 84–94%, 102–125 nm | In vitro cytotoxicity and cellular-uptake studies were performed on MDA-MB-453 cell lines and in vivo cytotoxicity study in MDA-MB-453 xenograft mice model. The nanoparticle showed superior antitumor effect when compared with the free drug | [134] |
| Polymeric nanoparticles | TNBC | Paclitaxel | Poly(lactic-co-glycolic acid) NP coated with hyaluronic acid | 84–98.34%, 225.1±0.43 nm | In vitro cell viability and cellular-uptake studies were performed on MDA-MB-231. The prepared NP showed an improved cellular uptake and thereby higher cytotoxicity in cancer cells when compared with free drug | [135] |
| SLN | TNBC | Di-allyl-disulfide | SLN prepared with palmitic acid, soya lecithin and pluronic F-68 and surface modified with glycation end products antibody | 79.23%, 116.20 nm | Formulated NP demonstrated a high cellular uptake by MDA-MB231 cell line and thereby reduction in systemic side effect of the drug and increased activity at tumor site | [136] |
| Polymer nanoparticles | TNBC | Curcumin, | Chitosan NPs with apoptosis-inducing ligand (TRAIL) | 51.67%, 652 ± 10 nm, | The NPs showed a reduced tumor volume when compared to control when tested in BALB/c mice | [137] |
| Iron oxide NPs | TNBC | Baicalein | PEG-coated iron oxide magnetic nanoparticles | 95.3%, 100 nm | Significantly inhibited the MDA-MB-231 cell growth when tested in vitro and showed significant anti-apoptotic activity | [138] |
| Polymeric NPs | TNBC | Thymoquinone | Hyaluronic acid conjugated Pluronic® P123 and Pluronic® F127 NPs | EE not reported, 22.0 ± 3.1 nm | Formulations retarded cell growth and migration of MDA-MB-231. Studies in Balb/c mice showed significant reduction in tumor load when treated with formulations | [139] |
| Product | Drug | Manufacturer | Indications | US FDA Approved Date/Clinical Trial Status |
|---|---|---|---|---|
| Doxil (Caelyx) | Pegylated doxorubicin | Orthobiotech, Schering-Plough | Ovarian/breast cancer | November 1995 |
| Myocet | Liposome-encapsulated Doxorubicin | Elan/Sopherion Therapeutics | Breast cancer | 2000, Approved in Europe and Canada |
| LEP-ETU | Liposomal Paclitaxel | Neopharma | Ovarian/breast/lung cancers | Phase I/II |
| EndoTAG-I | Paclitaxel | Medigene/SynCore Biotechnology | Breast cancer/pancreatic cancer | Phase II |
| Genexal-PM | Paclitaxel-loaded polymeric micelle | Samyang | Breast cancer/small cell lung cancer | Marketed in Europe, Korea |
| Nektar -102 | Irinotecan, PEGylated liposome | Nektar therapeutics | Breast/colorectal cancer | Phase III |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gadag, S.; Sinha, S.; Nayak, Y.; Garg, S.; Nayak, U.Y. Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer. Pharmaceutics 2020, 12, 524. https://doi.org/10.3390/pharmaceutics12060524
Gadag S, Sinha S, Nayak Y, Garg S, Nayak UY. Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer. Pharmaceutics. 2020; 12(6):524. https://doi.org/10.3390/pharmaceutics12060524
Chicago/Turabian StyleGadag, Shivaprasad, Shristi Sinha, Yogendra Nayak, Sanjay Garg, and Usha Y. Nayak. 2020. "Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer" Pharmaceutics 12, no. 6: 524. https://doi.org/10.3390/pharmaceutics12060524
APA StyleGadag, S., Sinha, S., Nayak, Y., Garg, S., & Nayak, U. Y. (2020). Combination Therapy and Nanoparticulate Systems: Smart Approaches for the Effective Treatment of Breast Cancer. Pharmaceutics, 12(6), 524. https://doi.org/10.3390/pharmaceutics12060524