
Establishment of the First National Standard for Neutralizing Antibodies against SARS-CoV-2 XBB Variants

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials and Ethics Statement
2.2. Production and Evaluation of the Candidates
2.3. Collaborative Calibration Study
2.3.1. Samples and Virus
2.3.2. Participating Laboratories
2.3.3. Collaborative Calibration Study
2.4. Statistical Methods
3. Results
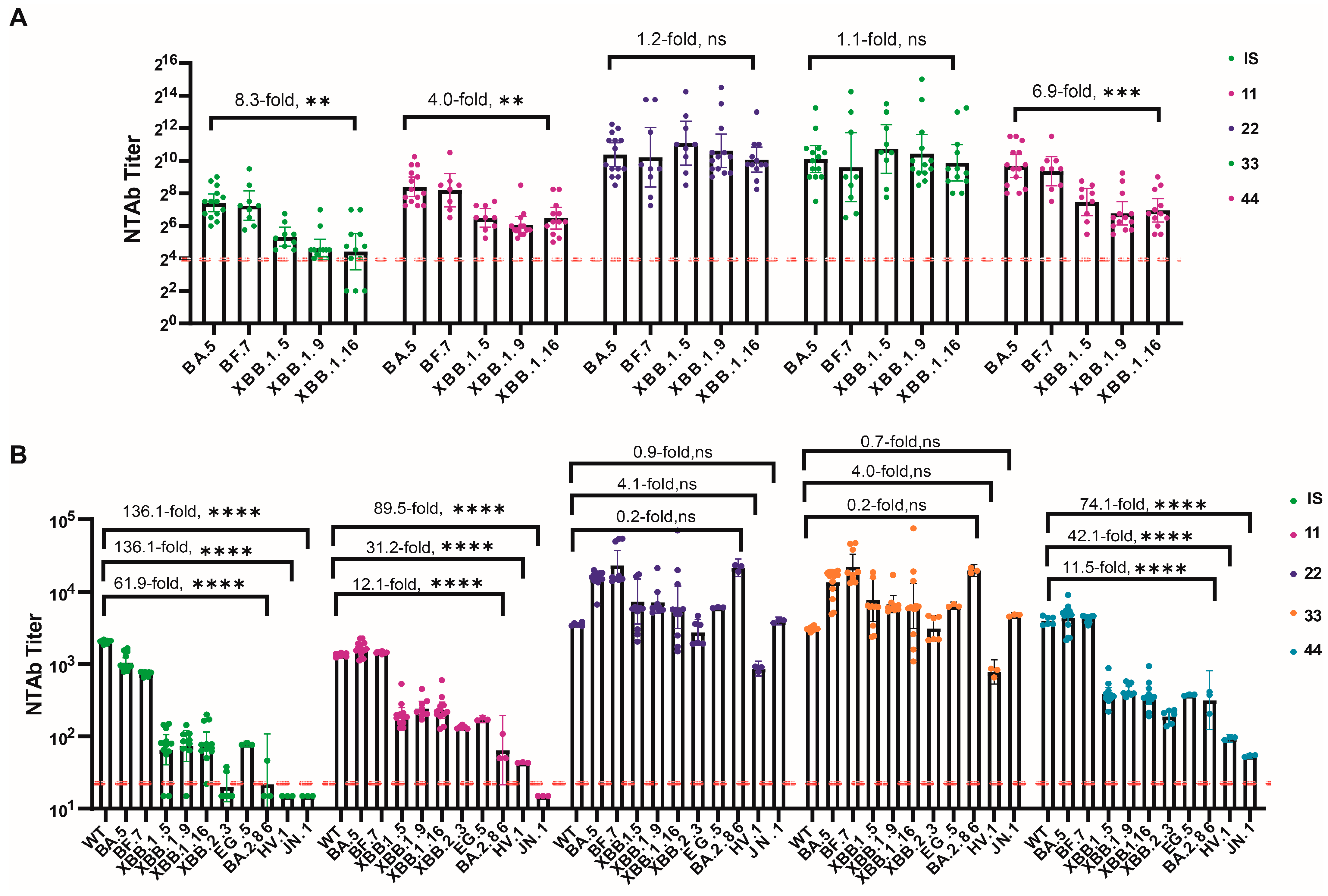
3.1. Neutralizing Activity of the Candidate Standards
3.2. Inter-Laboratory Variability
3.2.1. Variability among Laboratories for Candidate Standards
3.2.2. Inter-Laboratory Variability after Normalization
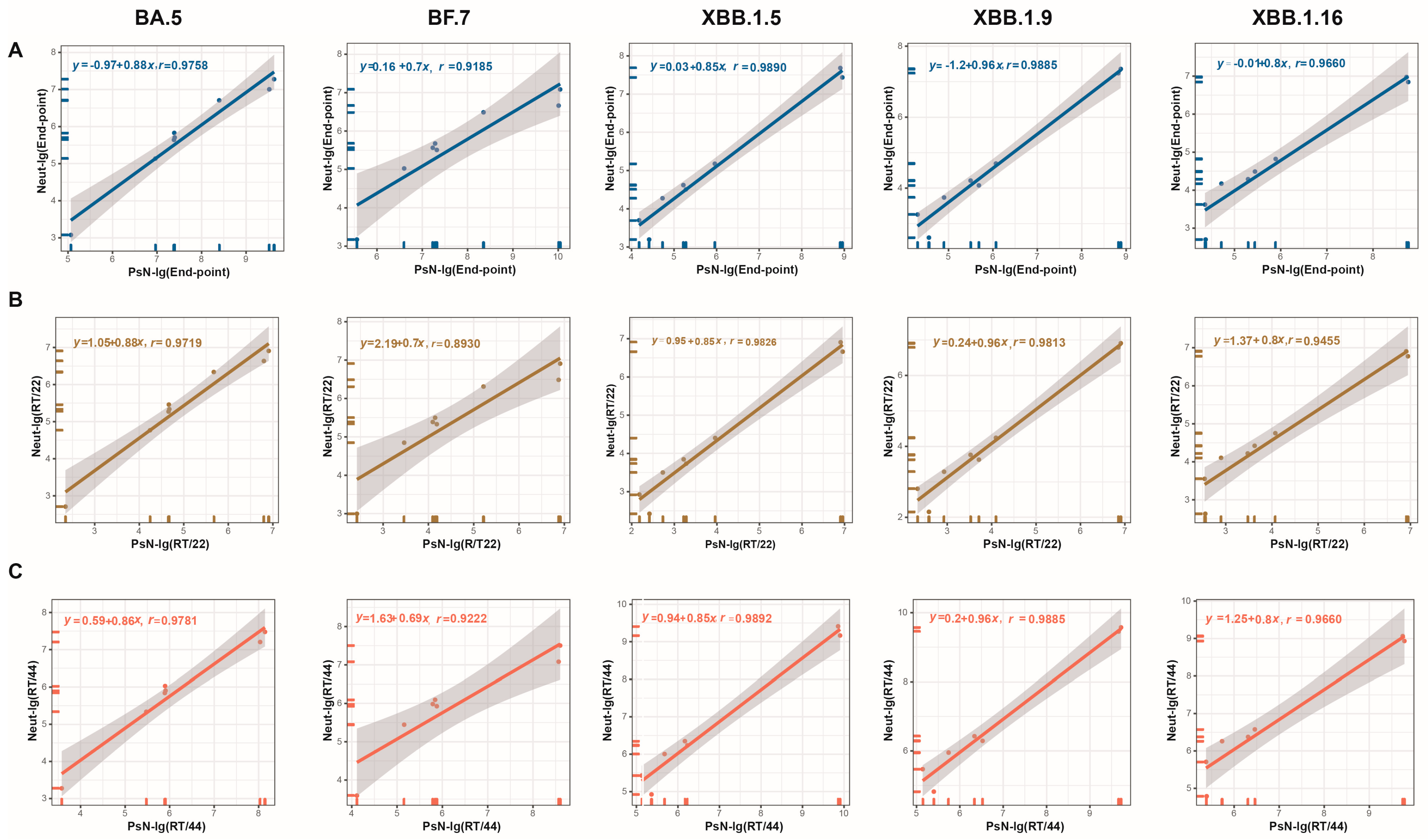
3.3. Inter-Assay Variability
3.3.1. Correlation between Neut and PsN Methods
3.3.2. Differences in GMT between Detection Methods before and after Normalization
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Director-General’s Opening Remarks at Themedia Briefing on COVID-19. 2020. Available online: https://vietnam.un.org/en/38806-who-director-generals-opening-remarksmedia-briefing-covid-19 (accessed on 14 December 2023).
- WHO. WHO Coronavirus (COVID-19) Dashboard. Available online: https://data.who.int/dashboards/covid19/cases?n=c (accessed on 14 December 2023).
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Callaway, E. The next generation of coronavirus vaccines: A graphical guide. Nature 2023, 614, 22–25. [Google Scholar] [CrossRef] [PubMed]
- WHO. COVID-19 Vaccine Tracker and Landscape. Available online: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines (accessed on 30 December 2023).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Mao, Q.; Wu, X.; He, Q.; Bian, L.; Bai, Y.; Wang, Z.; Wang, Q.; Zhang, J.; Liang, Z.; et al. Considerations for the Feasibility of Neutralizing Antibodies as a Surrogate Endpoint for COVID-19 Vaccines. Front. Immunol. 2022, 13, 814365. [Google Scholar] [CrossRef] [PubMed]
- WHO. Establishment of the 2nd WHO International Standard for Anti-SARS-CoV-2 Immunoglobulin and Reference Panel for Antibodies to SARS-CoV-2 Variants of Concern (WHO/BS/2022.2427). Available online: https://www.who.int/publications/m/item/who-bs-2022.2427 (accessed on 12 December 2023).
- WHO. Establishment of the WHO International Standard and Reference Panel for Anti-SARS-CoV-2 Antibody (WHO/BS.2020.2403). Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 8 November 2023).
- Guan, L.; Mao, Q.; Tan, D.; Liu, J.; Zhang, X.; Li, L.; Liu, M.; Wang, Z.; Cheng, F.; Cui, B.; et al. Establishment of national standard for anti-SARS-CoV-2 neutralizing antibody in China: The first National Standard calibration traceability to the WHO International Standard. Front. Immunol. 2023, 14, 1107639. [Google Scholar] [CrossRef] [PubMed]
- Guan, L.; Yu, Y.; Wu, X.; Nie, J.; Zhang, J.; Wang, Z.; Li, N.; Shi, R.; Zhao, H.; Chen, H.; et al. The first Chinese national standards for SARS-CoV-2 neutralizing antibody. Vaccine 2021, 39, 3724–3730. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, I.; Mattiuzzo, G.; Page, M.; Minor, P.; Griffiths, E.; Nuebling, M.; Moorthy, V. WHO International Standard for evaluation of the antibody response to COVID-19 vaccines: Call for urgent action by the scientific community. Lancet Microbe 2022, 3, e235–e240. [Google Scholar] [CrossRef] [PubMed]
- Channabasappa, N.K.; Niranjan, A.K.; Emran, T.B. SARS-CoV-2 variant omicron XBB.1.5: Challenges and prospects-correspondence. Int. J. Surg. 2023, 109, 1054–1055. [Google Scholar] [CrossRef] [PubMed]
- WHO. XBB.1.5 Updated Risk Assessment. Available online: https://www.who.int/docs/default-source/coronaviruse/20230620xbb.1.5.pdf?sfvrsn=fff6f686_3 (accessed on 21 December 2023).
- WHO. Statement on the Antigen Composition of COVID-19 Vaccines. Available online: https://www.who.int/news/item/18-05-2023-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 18 December 2023).
- WHO. Statement on the Antigen Composition of COVID-19 Vaccines [EB/OL]. Available online: https://www.who.int/news/item/13-12-2023-statement-on-the-antigen-composition-of-covid-19-vaccines (accessed on 2 January 2023).
- FDA. Spikevax. Available online: https://www.fda.gov/vaccines-blood-biologics/spikevax (accessed on 21 September 2023).
- Novavax. Novavax’s Updated COVID-19 Vaccine Now Authorized in Canada. Available online: https://ir.novavax.com/press-releases/2023-12-05-Novavaxs-Updated-COVID-19-Vaccine-Now-Authorized-in-Canada#:~:text=The%20expanded%20authorization%20was%20based,antibody%20responses%20to%20subvariants%20BA (accessed on 2 January 2024).
- NIFDC. Summary of the Publicity of the Batch Issuance of Biological Products. Available online: https://bio.nifdc.org.cn/pqf/search.do?formAction=pqfGs (accessed on 15 October 2016).
- FDA. COMIRNATY. Available online: https://www.fda.gov/vaccines-blood-biologics/comirnaty (accessed on 7 December 2023).
- Cao, Y.; Jian, F.; Zhang, Z.; Yisimayi, A.; Hao, X.; Bao, L.; Yuan, F.; Yu, Y.; Du, S.; Wang, J.; et al. Rational identification of potent and broad sarbecovirus-neutralizing antibody cocktails from SARS convalescents. Cell Rep. 2022, 41, 111845. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Manual for the Preparation of Reference Materials for Use as Secondary Standards in Antibody Testing, TRS 1043, Annex 2. Available online: https://www.who.int/publications/m/item/who-manual-for-reference-material-for-antibody-testing-annex-2 (accessed on 21 December 2023).
- Bewley, K.R.; Coombes, N.S.; Gagnon, L.; McInroy, L.; Baker, N.; Shaik, I.; St-Jean, J.R.; St-Amant, N.; Buttigieg, K.R.; Humphries, H.E.; et al. Quantification of SARS-CoV-2 neutralizing antibody by wild-type plaque reduction neutralization, microneutralization and pseudotyped virus neutralization assays. Nat. Protoc. 2021, 16, 3114–3140. [Google Scholar] [CrossRef] [PubMed]
- Nie, J.; Li, Q.; Wu, J.; Zhao, C.; Hao, H.; Liu, H.; Zhang, L.; Nie, L.; Qin, H.; Wang, M.; et al. Quantification of SARS-CoV-2 neutralizing antibody by a pseudotyped virus-based assay. Nat. Protoc. 2020, 15, 3699–3715. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Bai, Y.; Liu, M.; Tan, D.; Li, J.; Wang, Z.; Liang, Z.; Xu, M.; Wang, J.; Mao, Q. Standardized neutralization antibody analytical procedure for clinical samples based on the AQbD concept. Signal Transduct. Target. Ther. 2023, 8, 165. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wei, M.; Wu, Y.; Wang, J.; Hong, Y.; Huang, Y.; Yuan, L.; Ma, J.; Wang, K.; Wang, S.; et al. Cross-species tropism and antigenic landscapes of circulating SARS-CoV-2 variants. Cell Rep. 2022, 38, 110558. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Z.; Zhuang, X.; Zhang, S.; Chen, Z.; Zou, Y.; Sheng, J.; Li, T.; Tai, W.; Yu, J.; et al. Inactivated vaccine-elicited potent antibodies can broadly neutralize SARS-CoV-2 circulating variants. Nat. Commun. 2023, 14, 2179. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Faraone, J.N.; Evans, J.P.; Zheng, Y.M.; Carlin, C.; Anghelina, M.; Stevens, P.; Fernandez, S.; Jones, D.; Panchal, A.R.; et al. Enhanced evasion of neutralizing antibody response by Omicron XBB.1.5, CH.1.1, and CA.3.1 variants. Cell Rep. 2023, 42, 112443. [Google Scholar] [CrossRef] [PubMed]
- Kirkeby, L.; Rasmussen, T.T.; Reinholdt, J.; Kilian, M. Immunoglobulins in nasal secretions of healthy humans: Structural integrity of secretory immunoglobulin A1 (IgA1) and occurrence of neutralizing antibodies to IgA1 proteases of nasal bacteria. Clin. Diagn. Lab. Immunol. 2000, 7, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Marcotte, H.; Cao, Y.; Zuo, F.; Simonelli, L.; Sammartino, J.C.; Pedotti, M.; Sun, R.; Cassaniti, I.; Hagbom, M.; Piralla, A.; et al. Conversion of monoclonal IgG to dimeric and secretory IgA restores neutralizing ability and prevents infection of Omicron lineages. Proc. Natl. Acad. Sci. USA 2024, 121, e2315354120. [Google Scholar] [CrossRef] [PubMed]
- WHO. Recommendations for the Preparation, Characterization and Establishment of International and Other Biological Reference Standards. Available online: https://iris.who.int/bitstream/handle/10665/43278/WHO_TRS_932_eng.pdf?sequence=1 (accessed on 21 December 2023).

{kind=link}
{kind=link}
| Sample Code | Description | Formulation |
|---|---|---|
| 10 | 1st International Standard 2022 Antibodies to SARS-CoV-2 variants of concern, 21/338 | freeze-dry |
| 11 | Candidate 1, convalescent plasma, positive | liquid |
| 22 | Candidate 2, positive plasma with SA55 | liquid |
| 33 | Candidate 3, negative plasma with SA55 | liquid |
| 44 | Candidate 4, human anti-SARS-CoV-2 immunoglobulin | liquid |
| 55 | Concentrated nasal wash | liquid |
| 66 | Convalescent plasma from one donor, medium neutralizing capacity against XBB | liquid |
| 77 | Convalescent plasma from one donor with high NtAb titers against XBB | liquid |
| 88 | Convalescent plasma from one donor with low NtAb titers against XBB | liquid |
| 99 | Negative plasma | liquid |
| Detection Methods | Lab | Challenge Virus | Summary | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ancestral | BA.5 Sublineages | XBB Sublineages | BA.2.86 Sublineages | ||||||||||
| WT | BA.5 | BF.7 | XBB.1.5 | XBB.1.9 | XBB.1.16 | XBB.2.3 | EG.5 | HV.1 | BA2.86 | JN.1 | |||
| Neut assay | LB1 | / | √ | √ | / | √ | / | / | / | / | / | 4 | |
| LB2 | / | √ | / | / | √ | / | / | / | / | / | / | 2 | |
| LB3 | / | / | / | / | √ | √ | / | / | / | / | / | 2 | |
| LB4 | / | √ | √ | √ | √ | √ | / | / | / | / | / | 5 | |
| LB5 | / | √ | √ | √ | √ | √ | / | / | / | / | / | 5 | |
| PsN assay | LB2 | / | √ | / | / | √ | / | / | / | / | / | / | 2 |
| LB6 | / | √ | / | √ | / | √ | / | / | / | / | / | 3 | |
| LB7 | √ | √ | √ | √ | √ | √ | √ | √ | / | / | / | 8 | |
| LB8 | √ | √ | √ | √ | √ | √ | √ | / | √ | √ | √ | 10 | |
| LB9 | / | √ | √ | √ | / | √ | / | / | / | / | / | 4 | |
| Challenge Virus | GCV, % | Sample Code | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 11 | 22 | 33 | 44 | 55 | 66 | 77 | 88 | ||
| BA5 | Endpoint | 95.4 | 112.4 | 152.1 | 141.5 | 149.2 | 94.6 | 115.6 | 84.1 | 103.0 |
| RT/10 | / | 10.7 | 71.1 | 113.1 | 33.0 | 25.5 | 14.0 | 13.0 | 4.5 | |
| RT/11 | 10.7 | / | 61.1 | 108.6 | 20.7 | 31.9 | 3.7 | 22.1 | 7.4 | |
| RT/22 | 136.9 | 313.9 | / | 146.3 | 92.9 | 189.2 | 118.0 | 134.8 | 127.2 | |
| RT/33 | 113.1 | 108.6 | 42.1 | / | 101.5 | 154.7 | 103.3 | 104.7 | 111.4 | |
| RT/44 | 33.0 | 20.7 | 46.9 | 101.5 | / | 56.6 | 17.2 | 42.3 | 28.0 | |
| BF.7 | Endpoint | 131.4 | 148.6 | 506.8 | 742.5 | 132.0 | 51.7 | 132.0 | 96.8 | 107.8 |
| RT/10 | / | 27.8 | 167.1 | 270.6 | 14.3 | 58.2 | 33.0 | 41.6 | 37.5 | |
| RT/11 | 27.8 | 126.8 | 179.4 | 32.8 | 88.4 | 44.6 | 79.4 | 40.3 | ||
| RT/22 | 167.1 | 126.8 | 38.9 | 181.6 | 322.5 | 211.2 | 261.2 | 243.5 | ||
| RT/33 | 270.6 | 179.4 | 38.9 | / | 289.0 | 486.2 | 326.7 | 397.7 | 372.6 | |
| RT/44 | 14.3 | 32.8 | 181.6 | 289.0 | / | 54.3 | 16.5 | 28.6 | 23.2 | |
| XBB.1.5 | Endpoint | 73.5 | 69.8 | 257.8 | 322.2 | 128.3 | 51.9 | 73.5 | 73.5 | 84.3 |
| RT/10 | / | 5.9 | 106.2 | 143.8 | 40.3 | 41.6 | 10.5 | 35.7 | 16.5 | |
| RT/11 | 5.9 | / | 111.9 | 151.6 | 48.2 | 45.6 | 16.5 | 42.1 | 12.2 | |
| RT/22 | 106.2 | 111.9 | / | 20.0 | 70.5 | 167.1 | 109.1 | 135.1 | 101.4 | |
| RT/33 | 143.8 | 151.6 | 20.0 | / | 93.9 | 208.1 | 144.7 | 169.2 | 140.7 | |
| RT/44 | 40.3 | 48.2 | 70.5 | 93.9 | / | 59.5 | 33.0 | 38.9 | 54.3 | |
| XBB.1.9 | Endpoint | 93.6 | 70.9 | 245.8 | 299.0 | 141.1 | 68.0 | 65.1 | 37.2 | 66.7 |
| RT/10 | / | 27.4 | 99.5 | 117.0 | 39.7 | 30.2 | 34.7 | 45.5 | 23.3 | |
| RT/11 | 27.4 | / | 102.8 | 135.8 | 41.6 | 30.1 | 9.0 | 26.2 | 7.7 | |
| RT/22 | 99.5 | 102.8 | / | 33.0 | 46.5 | 132.8 | 110.9 | 154.5 | 110.5 | |
| RT/33 | 117.0 | 128.0 | 29.7 | / | 81.7 | 173.1 | 156.7 | 176.9 | 137.8 | |
| RT/44 | 39.7 | 41.6 | 46.5 | 73.2 | / | 59.2 | 50.3 | 78.3 | 47.1 | |
| XBB.1.16 | Endpoint | 209.2 | 106.8 | 123.1 | 224.8 | 131.5 | 80.7 | 97.6 | 77.3 | 230.7 |
| RT/10 | / | 95.2 | 93.9 | 128.3 | 101.4 | 81.0 | 95.8 | 88.1 | 133.5 | |
| RT/11 | 95.2 | / | 21.5 | 98.4 | 21.0 | 26.3 | 12.8 | 24.4 | 69.7 | |
| RT/22 | 93.9 | 21.5 | / | 63.6 | 7.8 | 36.7 | 14.6 | 33.7 | 77.9 | |
| RT/33 | 128.3 | 98.4 | 63.6 | / | 66.7 | 111.2 | 84.9 | 107.7 | 106.4 | |
| RT/44 | 101.4 | 21.0 | 7.8 | 66.7 | / | 43.3 | 18.8 | 40.1 | 56.2 | |
| Challenge Virus | GCV, % | Sample Code | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 11 | 22 | 33 | 44 | 55 | 66 | 77 | 88 | ||
| BA5 | Endpoint | 27.1 | 24.3 | 20.2 | 61.9 | 46.6 | 26.9 | 46.1 | 33.2 | 28.9 |
| RT/10 | / | 19.4 | 40.0 | 88.4 | 41.8 | 25.4 | 36.9 | 30.3 | 31.4 | |
| RT/11 | 19.4 | / | 39.6 | 76.6 | 24.6 | 7.4 | 19.3 | 9.7 | 15.8 | |
| RT/22 | 40.0 | 39.6 | / | 40.1 | 69.1 | 43.4 | 65.2 | 48.2 | 33.5 | |
| RT/33 | 88.4 | 76.6 | 40.1 | / | 105.7 | 78.1 | 99.4 | 78.9 | 56.6 | |
| RT/44 | 41.8 | 24.6 | 69.1 | 105.7 | / | 18.6 | 12.1 | 18.8 | 36.5 | |
| BF.7 | Endpoint | 8.6 | 1.5 | 104.4 | 81.4 | 13.2 | 45.5 | 2.6 | 21.2 | 8.4 |
| RT/10 | / | 10.2 | 94.7 | 71.1 | 19.4 | 55.5 | 11.0 | 30.3 | 12.1 | |
| RT/11 | 10.2 | / | 106.0 | 83.1 | 12.8 | 44.1 | 1.8 | 19.9 | 8.3 | |
| RT/22 | 94.7 | 106.0 | / | 17.2 | 130.9 | 195.9 | 109.5 | 146.2 | 92.1 | |
| RT/33 | 71.1 | 83.1 | 17.2 | / | 104.0 | 163.8 | 86.0 | 119.6 | 72.1 | |
| RT/44 | 19.4 | 12.8 | 130.9 | 104.0 | / | 30.4 | 10.8 | 10.7 | 22.1 | |
| XBB.1.5 | Endpoint | 110.0 | 37.1 | 200.8 | 186.6 | 35.2 | 50.2 | 9.7 | 19.8 | 36.7 |
| RT/10 | / | 73.4 | 148.2 | 142.5 | 80.3 | 72.1 | 109.3 | 126.6 | 53.8 | |
| RT/11 | 73.4 | / | 122.9 | 112.7 | 4.9 | 15.9 | 29.1 | 38.4 | 23.9 | |
| RT/22 | 148.2 | 122.9 | / | 5.4 | 123.1 | 104.4 | 177.9 | 190.5 | 157.9 | |
| RT/33 | 142.5 | 112.7 | 5.4 | / | 112.7 | 95.4 | 164.5 | 176.1 | 147.4 | |
| RT/44 | 80.3 | 4.9 | 123.1 | 112.7 | / | 18.2 | 28.2 | 45.9 | 23.3 | |
| XBB.1.9 | Endpoint | 73.9 | 33.0 | 48.3 | 26.1 | 23.6 | 17.3 | 20.9 | 23.0 | 15.0 |
| RT/10 | / | 49.0 | 37.3 | 44.0 | 50.9 | 80.8 | 57.8 | 73.2 | 62.3 | |
| RT/11 | 49.0 | / | 13.0 | 9.3 | 7.8 | 25.5 | 10.4 | 17.8 | 16.1 | |
| RT/22 | 37.3 | 13.0 | / | 18.1 | 20.2 | 41.8 | 24.4 | 32.8 | 30.6 | |
| RT/33 | 44.0 | 9.3 | 18.1 | / | 5.0 | 25.6 | 9.7 | 20.6 | 13.0 | |
| RT/44 | 50.9 | 7.8 | 20.2 | 5.0 | / | 20.1 | 4.6 | 14.9 | 8.8 | |
| XBB.1.16 | Endpoint | 84.2 | 45.7 | 196.6 | 214.4 | 49.9 | 44.4 | 29.5 | 42.7 | 26.3 |
| RT/10 | / | 30.6 | 61.2 | 72.5 | 23.2 | 44.3 | 57.7 | 43.0 | 51.2 | |
| RT/11 | 30.6 | / | 107.3 | 119.5 | 14.2 | 18.2 | 28.3 | 18.4 | 20.4 | |
| RT/22 | 61.2 | 107.3 | / | 12.3 | 98.4 | 125.2 | 147.6 | 121.5 | 140.7 | |
| RT/33 | 72.5 | 119.5 | 12.3 | / | 111.5 | 141.6 | 157.7 | 130.1 | 152.7 | |
| RT/44 | 23.2 | 14.2 | 98.4 | 111.5 | / | 27.6 | 32.4 | 24.8 | 25.3 | |
| Variants | Sample Number | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 10 | 11 | 22 | 33 | 44 | 55 | 66 | 77 | 88 | ||
| BA5 | Endpoint | 5.92 | 4.53 | 11.45 | 12.85 | 5.16 | 6.88 | 5.19 | 5.43 | 4.58 |
| RT/10 | / | 1.31 | 1.93 | 2.17 | 1.15 | 1.16 | 1.14 | 1.09 | 1.29 | |
| RT/11 | 1.31 | / | 2.53 | 2.84 | 1.14 | 1.52 | 1.15 | 1.20 | 1.01 | |
| RT/22 | 2.74 | 5.06 | / | 1.26 | 3.14 | 2.36 | 3.12 | 2.98 | 3.53 | |
| RT/33 | 2.17 | 2.84 | 1.12 | / | 2.49 | 1.87 | 2.48 | 2.37 | 2.80 | |
| RT/44 | 1.15 | 1.14 | 2.22 | 2.49 | / | 1.33 | 1.01 | 1.05 | 1.13 | |
| BF.7 | Endpoint | 4.83 | 4.47 | 19.24 | 28.40 | 6.44 | 10.80 | 6.13 | 5.29 | 4.19 |
| RT/10 | / | 1.21 | 3.99 | 5.89 | 1.33 | 2.24 | 1.27 | 1.10 | 1.15 | |
| RT/11 | 1.21 | / | 4.65 | 7.35 | 1.62 | 2.61 | 1.51 | 1.37 | 1.03 | |
| RT/22 | 3.99 | 4.65 | / | 1.48 | 2.99 | 1.78 | 3.14 | 3.64 | 4.59 | |
| RT/33 | 5.89 | 7.35 | 1.48 | / | 4.41 | 2.63 | 4.63 | 5.37 | 6.77 | |
| RT/44 | 1.33 | 1.62 | 2.99 | 4.41 | / | 1.68 | 1.05 | 1.22 | 1.54 | |
| XBB.1.5 | Endpoint | 1.62 | 2.17 | 3.40 | 4.56 | 2.18 | 5.06 | 1.58 | 1.82 | 1.49 |
| RT/10 | / | 1.34 | 2.10 | 2.82 | 1.35 | 3.13 | 1.03 | 1.12 | 1.09 | |
| RT/11 | 1.34 | / | 1.57 | 2.11 | 1.01 | 2.34 | 1.37 | 1.19 | 1.46 | |
| RT/22 | 2.10 | 1.57 | / | 1.34 | 1.56 | 1.49 | 2.16 | 1.87 | 2.29 | |
| RT/33 | 2.82 | 2.11 | 1.34 | / | 2.09 | 1.11 | 2.89 | 2.51 | 3.07 | |
| RT/44 | 1.35 | 1.01 | 1.56 | 2.09 | / | 2.31 | 1.46 | 1.22 | 1.60 | |
| XBB.1.9 | Endpoint | 3.29 | 3.54 | 4.31 | 4.66 | 3.83 | 8.42 | 3.13 | 4.93 | 3.03 |
| RT/10 | / | 1.07 | 1.31 | 1.41 | 1.16 | 2.55 | 1.05 | 1.50 | 1.09 | |
| RT/11 | 1.07 | / | 1.22 | 1.32 | 1.08 | 2.38 | 1.13 | 1.39 | 1.17 | |
| RT/22 | 1.31 | 1.22 | / | 1.08 | 1.13 | 1.95 | 1.38 | 1.14 | 1.42 | |
| RT/33 | 1.41 | 1.23 | 1.14 | / | 1.20 | 1.76 | 1.45 | 1.18 | 1.51 | |
| RT/44 | 1.16 | 1.08 | 1.13 | 1.22 | / | 2.20 | 1.22 | 1.29 | 1.26 | |
| XBB.1.16 | Endpoint | 3.67 | 2.59 | 5.75 | 6.79 | 2.91 | 7.31 | 1.72 | 2.73 | 1.91 |
| RT/10 | / | 1.41 | 1.57 | 1.85 | 1.26 | 2.00 | 2.13 | 1.34 | 1.92 | |
| RT/11 | 1.41 | / | 2.22 | 2.62 | 1.12 | 2.82 | 1.51 | 1.05 | 1.40 | |
| RT/22 | 1.57 | 2.22 | / | 1.18 | 1.97 | 1.27 | 3.34 | 2.11 | 3.25 | |
| RT/33 | 1.85 | 2.62 | 1.18 | / | 2.33 | 1.08 | 3.95 | 2.49 | 3.77 | |
| RT/44 | 1.26 | 1.12 | 1.97 | 2.33 | / | 2.51 | 1.69 | 1.07 | 1.53 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Guan, L.; Li, N.; Wang, Y.; Li, L.; Liu, M.; He, Q.; Lu, J.; Zeng, H.; Yu, S.; et al. Establishment of the First National Standard for Neutralizing Antibodies against SARS-CoV-2 XBB Variants. Viruses 2024, 16, 554. https://doi.org/10.3390/v16040554
Zhang X, Guan L, Li N, Wang Y, Li L, Liu M, He Q, Lu J, Zeng H, Yu S, et al. Establishment of the First National Standard for Neutralizing Antibodies against SARS-CoV-2 XBB Variants. Viruses. 2024; 16(4):554. https://doi.org/10.3390/v16040554
Chicago/Turabian StyleZhang, Xuanxuan, Lidong Guan, Na Li, Ying Wang, Lu Li, Mingchen Liu, Qian He, Jiansheng Lu, Haiyuan Zeng, Shan Yu, and et al. 2024. "Establishment of the First National Standard for Neutralizing Antibodies against SARS-CoV-2 XBB Variants" Viruses 16, no. 4: 554. https://doi.org/10.3390/v16040554
APA StyleZhang, X., Guan, L., Li, N., Wang, Y., Li, L., Liu, M., He, Q., Lu, J., Zeng, H., Yu, S., Guo, X., Gong, J., Li, J., Gao, F., Wu, X., Chen, S., Wang, Q., Wang, Z., Huang, W., ... Xu, M. (2024). Establishment of the First National Standard for Neutralizing Antibodies against SARS-CoV-2 XBB Variants. Viruses, 16(4), 554. https://doi.org/10.3390/v16040554