
Impact of Tuberculosis on Disease Severity and Viral Shedding Duration in COVID-19 Patients


Abstract
1. Introduction
2. Methods
2.1. Study Patients
2.2. Data Collection
2.3. Related Definitions
- Symptoms/signs suggestive of tuberculosis;
- Chest radiograph consistent with tuberculosis;
- Close tuberculosis exposure or immunologic evidence of mycobacterium tuberculosis infection;
- Positive response to tuberculosis treatment.
2.4. RT-PCR Assay for SARS-CoV-2 RNA
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of COVID-19 Patients with and without Tuberculosis
3.2. Treatments and Outcomes of COVID-19 Patients with and without Tuberculosis
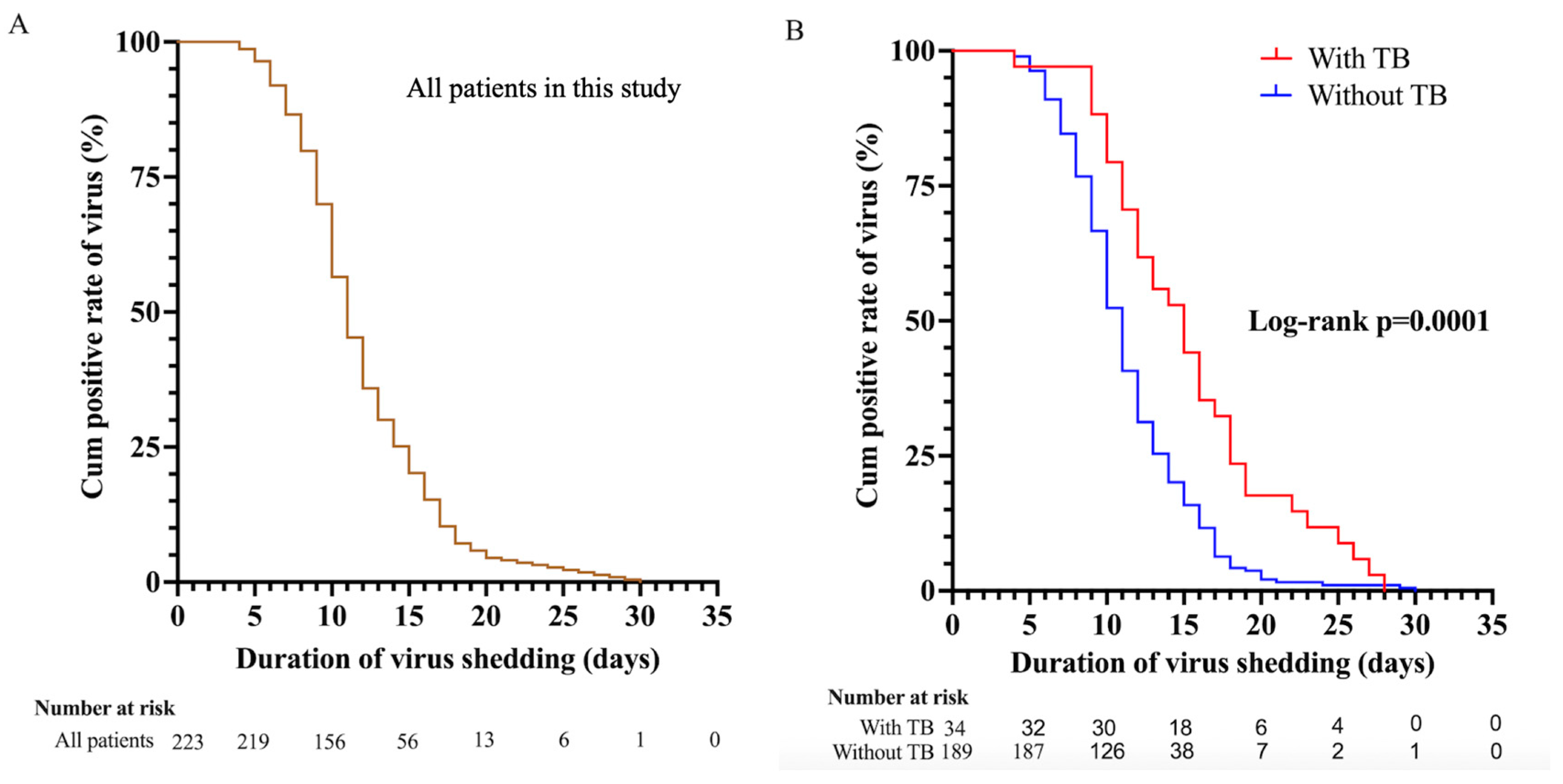
3.3. Risk Factors for SARS-CoV-2 Shedding
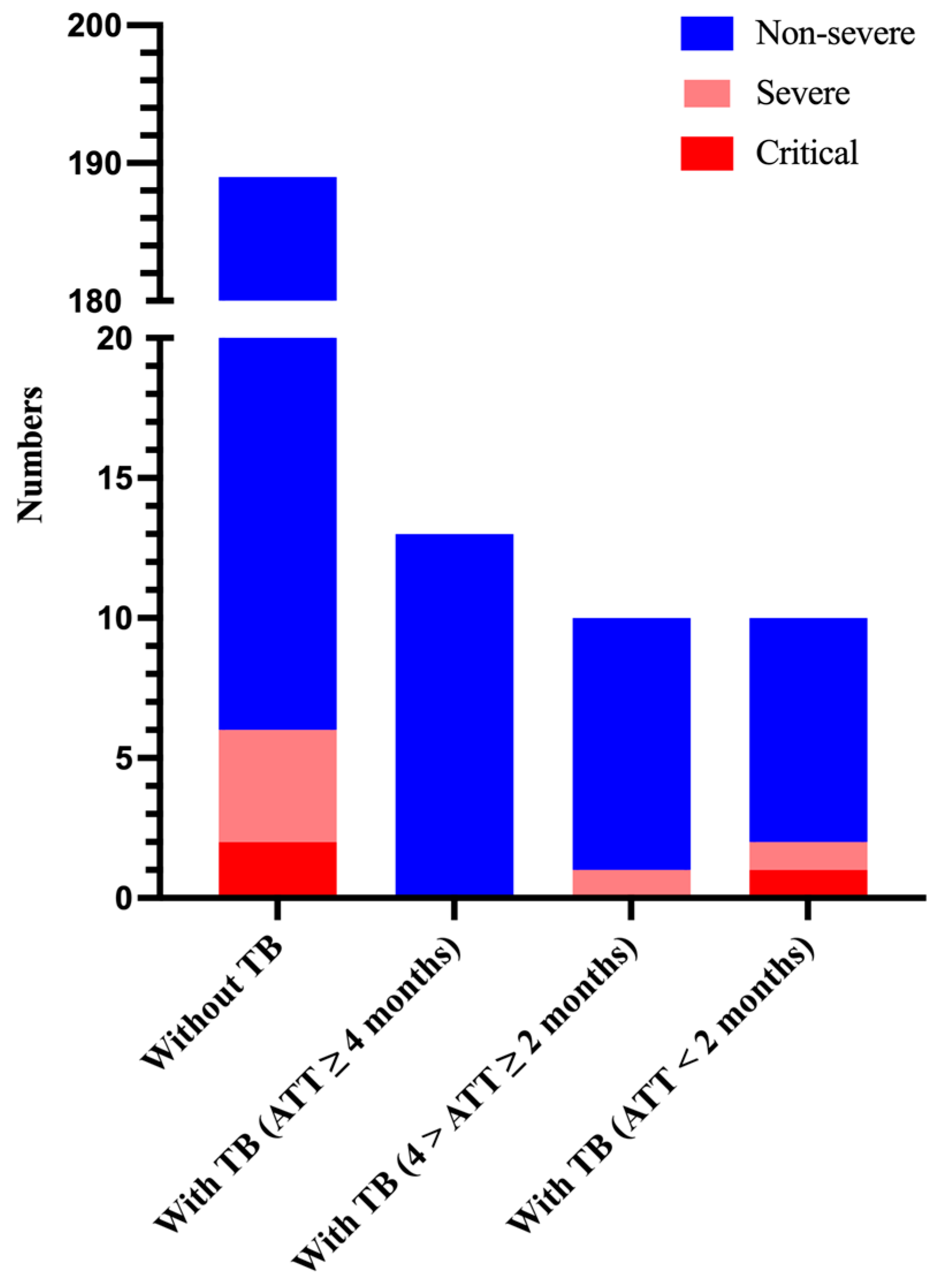
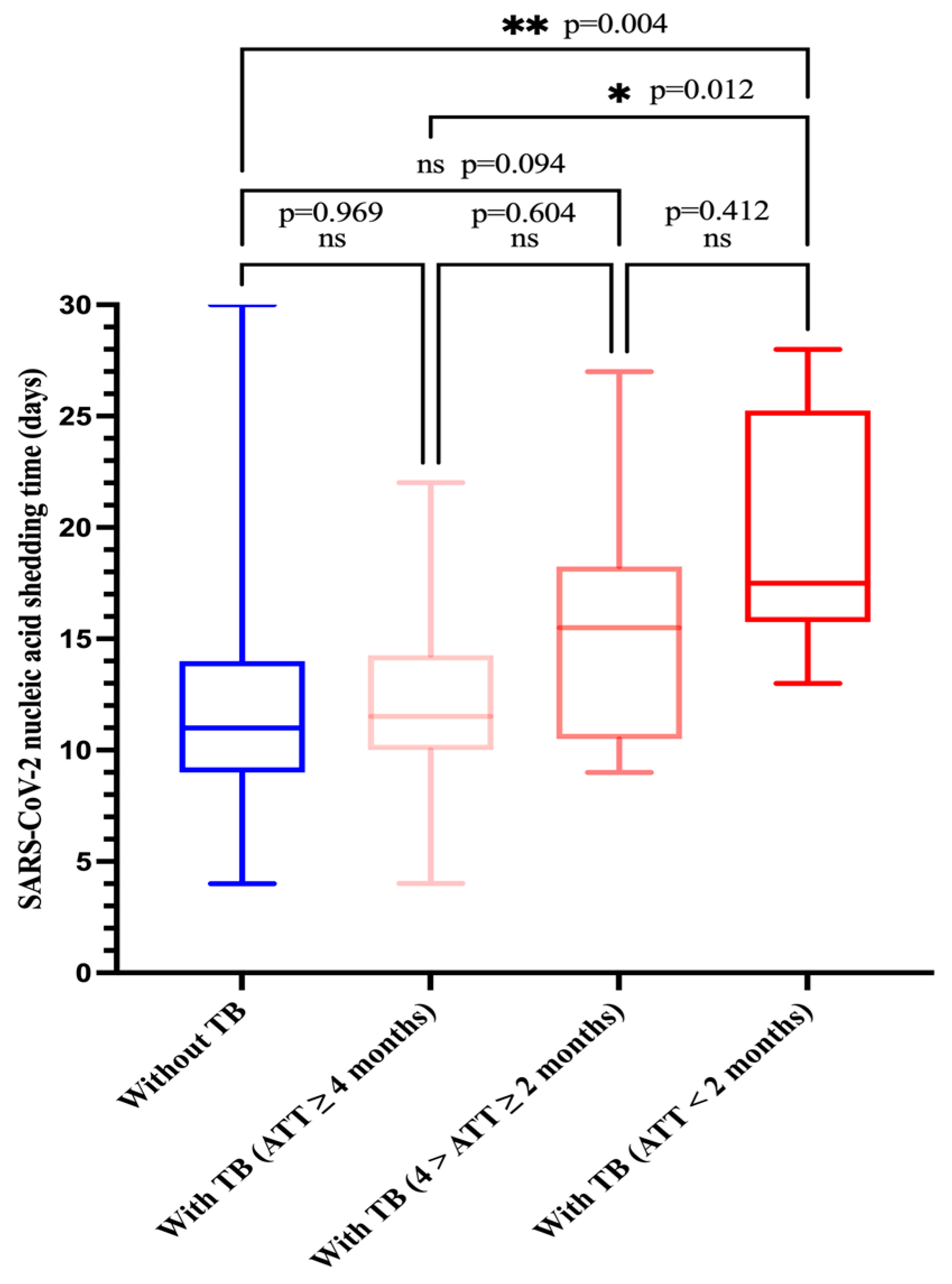
3.4. Subgroup Analysis of Severity of Hospitalization and SARS-CoV-2 Shedding Duration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Available online: https://covid19.who.int (accessed on 7 August 2023).
- Zhang, J.J.; Dong, X.; Liu, G.H.; Gao, Y.D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef]
- Varshney, K.; Pillay, P.; Mustafa, A.D.; Shen, D.; Adalbert, J.R.; Mahmood, M.Q. A systematic review of the clinical characteristics of influenza-COVID-19 co-infection. Clin. Exp. Med. 2023, 23, 3265–3275. [Google Scholar] [CrossRef]
- Spinelli, M.A.; Jones, B.L.H.; Gandhi, M. COVID-19 Outcomes and Risk Factors Among People Living with HIV. Curr. HIV/AIDS Rep. 2022, 19, 425–432. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Tuberculosis Report 2022; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2022 (accessed on 18 October 2023).
- Tadolini, M.; Codecasa, L.R.; García-García, J.M.; Blanc, F.X.; Borisov, S.; Alffenaar, J.W.; Andréjak, C.; Bachez, P.; Bart, P.A.; Belilovski, E.; et al. Active tuberculosis, sequelae and COVID-19 co-infection: First cohort of 49 cases. Eur. Respir. J. 2020, 56, 2001398. [Google Scholar] [CrossRef] [PubMed]
- Stochino, C.; Villa, S.; Zucchi, P.; Parravicini, P.; Gori, A.; Raviglione, M.C. Clinical characteristics of COVID-19 and active tuberculosis co-infection in an Italian reference hospital. Eur. Respir. J. 2020, 56, 2001708. [Google Scholar] [CrossRef]
- Zaini, J.; Fadhillah, M.R.; Reisa, T.; Isbaniyah, F.; Handayani, R.R.D. The Tuberculosis and COVID-19 coinfection: A report of two cases at a tertiary referral in Indonesia. J. Infect. Dev. Ctries. 2022, 16, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Guo, S.; Wei, X.; Dong, Q.; Xu, N.; Li, H.; Zhao, J.; Sun, Q. Global prevalence, treatment and outcome of tuberculosis and COVID-19 coinfection: A systematic review and meta-analysis (from November 2019 to March 2021). BMJ Open 2022, 12, e059396. [Google Scholar] [CrossRef] [PubMed]
- Song, W.M.; Zhao, J.Y.; Zhang, Q.Y.; Liu, S.Q.; Zhu, X.H.; An, Q.Q.; Xu, T.T.; Li, S.J.; Liu, J.Y.; Tao, N.N.; et al. COVID-19 and Tuberculosis Coinfection: An Overview of Case Reports/Case Series and Meta-Analysis. Front. Med. 2021, 8, 657006. [Google Scholar] [CrossRef]
- Sarkar, S.; Khanna, P.; Singh, A.K. Impact of COVID-19 in patients with concurrent co-infections: A systematic review and meta-analyses. J. Med. Virol. 2021, 93, 2385–2395. [Google Scholar] [CrossRef]
- Tamuzi, J.L.; Ayele, B.T.; Shumba, C.S.; Adetokunboh, O.O.; Uwimana-Nicol, J.; Haile, Z.T.; Inugu, J.; Nyasulu, P.S. Implications of COVID-19 in high burden countries for HIV/TB: A systematic review of evidence. BMC Infect. Dis. 2020, 20, 744. [Google Scholar] [CrossRef]
- Zhang, W.; Wu, H.; Guo, Q.; Xu, X.; Pu, Y.; Chen, C.; Cao, M.; Sun, D.; Lu, W.; Yi, H.; et al. Association of clinical characteristics and vaccines with risk of persistently viral clearance in patients infected with SARS-CoV-2 Omicron variant in Shanghai, China. Heliyon 2023, 10, e23256. [Google Scholar] [CrossRef]
- Kang, S.W.; Kim, J.W.; Kim, J.Y.; Lim, S.Y.; Jang, C.Y.; Chang, E.; Yang, J.S.; Kim, K.C.; Jang, H.C.; Kim, D.; et al. Characteristics and risk factors of prolonged viable virus shedding in immunocompromised patients with COVID-19: A prospective cohort study. J. Infect. 2023, 86, 412–414. [Google Scholar] [CrossRef]
- Chinese Clinical Guidance for COVID-19 Pneumonia Diagnosis and Treatment (7th edition). Available online: http://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989.shtml (accessed on 4 March 2020).
- Wang, Y.; Feng, R.; Xu, J.; Hou, H.; Feng, H.; Yang, H. An updated meta-analysis on the association between tuberculosis and COVID-19 severity and mortality. J. Med. Virol. 2021, 93, 5682–5686. [Google Scholar] [CrossRef]
- Sy, K.T.L.; Haw, N.J.L.; Uy, J. Previous and active tuberculosis increases risk of death and prolongs recovery in patients with COVID-19. Infect. Dis. 2020, 52, 902–907. [Google Scholar] [CrossRef] [PubMed]
- TB/COVID-19 Global Study Group. Tuberculosis and COVID-19 co-infection: Description of the global cohort. Eur. Respir. J. 2022, 59, 2102538. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, Y.; Fleming, J.; Yu, Y.; Gu, Y.; Liu, C.; Fan, L.; Wang, X.; Cheng, M.; Bi, L.; et al. Active or latent tuberculosis increases susceptibility to COVID-19 and disease severity. medRxiv 2020, 2020, 3. [Google Scholar]
- Jassat, W.; Cohen, C.; Tempia, S.; Masha, M.; Goldstein, S.; Kufa, T.; Murangandi, P.; Savulescu, D.; Walaza, S.; Bam, J.L.; et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV 2021, 8, e554–e567. [Google Scholar] [CrossRef] [PubMed]
- Western Cape Department of Health in Collaboration with the National Institute for Communicable Diseases SA. Risk factors for coronavirus disease 2019 (COVID-19) death in a population cohort study from the western cape province, South Africa. Clin. Infect. Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef] [PubMed]
- du Bruyn, E.; Stek, C.; Daroowala, R.; Said-Hartley, Q.; Hsiao, M.; Schafer, G.; Goliath, R.T.; Abrahams, F.; Jackson, A.; Wasserman, S.; et al. Effects of tuberculosis and/or HIV-1 infection on COVID-19 presentation and immune response in Africa. Nat. Commun. 2023, 14, 188. [Google Scholar] [CrossRef] [PubMed]
- Global Tuberculosis Network and TB/COVID-19 Global Study Group. Long-term outcomes of the global tuberculosis and COVID-19 co-infection cohort. Eur. Respir. J. 2023, 62, 2300925. [Google Scholar] [CrossRef] [PubMed]
- Flores-Lovon, K.; Ortiz-Saavedra, B.; Cueva-Chicaña, L.A.; Aperrigue-Lira, S.; Montes-Madariaga, E.S.; Soriano-Moreno, D.R.; Bell, B.; Macedo, R. Immune responses in COVID-19 and tuberculosis coinfection: A scoping review. Front. Immunol. 2022, 13, 992743. [Google Scholar] [CrossRef]
- Wang, K.; Zhang, X.; Sun, J.; Ye, J.; Wang, F.; Hua, J.; Zhang, H.; Shi, T.; Li, Q.; Wu, X. Differences of Severe Acute Respiratory Syndrome Coronavirus 2 Shedding Duration in Sputum and Nasopharyngeal Swab Specimens Among Adult Inpatients with Coronavirus Disease 2019. Chest 2020, 158, 1876–1884. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Liu, X.Y.; Zhu, Y.N.; Huang, L.; Dan, B.T.; Zhang, G.J.; Gao, Y.H. Factors associated with prolonged viral shedding and impact of lopinavir/ritonavir treatment in hospitalised non-critically ill patients with SARS-CoV-2 infection. Eur. Respir. J. 2020, 56, 2000799. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Hill, H.R. Role of Host Immune and Inflammatory Responses in COVID-19 Cases with Underlying Primary Immunodeficiency: A Review. J. Interferon Cytokine Res. 2020, 40, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Martins, T.B.; Peterson, L.K.; Hill, H.R. Clinical significance of measuring serum cytokine levels as inflammatory biomarkers in adult and pediatric COVID-19 cases: A review. Cytokine 2021, 142, 155478. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.M.; Beck, E.M.; Fisher, M.A. The Brief Case: Ventilator-Associated Corynebacterium accolens Pneumonia in a Patient with Respiratory Failure Due to COVID-19. J. Clin. Microbiol. 2021, 59, e0013721. [Google Scholar]
- Park, W.B.; Poon, L.L.M.; Choi, S.J.; Choe, P.G.; Song, K.H.; Bang, J.H.; Kim, E.S.; Kim, H.B.; Park, S.W.; Kim, N.J.; et al. Replicative virus shedding in the respiratory tract of patients with Middle East respiratory syndrome coronavirus infection. Int. J. Infect. Dis. 2018, 72, 8–10. [Google Scholar] [CrossRef]
- de Jong, M.D.; Simmons, C.P.; Thanh, T.T.; Hien, V.M.; Smith, G.J.; Chau, T.N.; Hoang, D.M.; Chau, N.V.; Khanh, T.H.; Dong, V.C.; et al. Fatal outcome of human influenza A (H5N1) is associated with high viral load and hypercytokinemia. Nat. Med. 2006, 12, 1203–1207. [Google Scholar] [CrossRef]
- van Riel, D.; Munster, V.J.; de Wit, E.; Rimmelzwaan, G.F.; Fouchier, R.A.; Osterhaus, A.D.; Kuiken, T. H5N1 Virus Attachment to Lower Respiratory Tract. Science 2006, 312, 399. [Google Scholar] [CrossRef]
- Min, C.K.; Cheon, S.; Ha, N.Y.; Sohn, K.M.; Kim, Y.; Aigerim, A.; Shin, H.M.; Choi, J.Y.; Inn, K.S.; Kim, J.H.; et al. Comparative and kinetic analysis of viral shedding and immunological responses in MERS patients representing a broad spectrum of disease severity. Sci. Rep. 2016, 6, 25359. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Chen, L.L.; Zhang, R.R.; Tsang, O.T.; Chan, J.M.; Tam, A.R.; Leung, W.S.; Chik, T.S.; Lau, D.P.; Choi, C.Y.; et al. Boosting of serum neutralizing activity against the Omicron variant among recovered COVID-19 patients by BNT162b2 and CoronaVac vaccines. EBioMedicine 2022, 79, 103986. [Google Scholar] [CrossRef] [PubMed]
- Lim, W.W.; Mak, L.; Leung, G.M.; Cowling, B.J.; Peiris, M. Comparative immunogenicity of mRNA and inactivated vaccines against COVID-19. Lancet Microbe 2021, 2, e423. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.K.P.; Cohen, C.A.; Cheng, S.M.S.; Chen, C.; Kwok, K.O.; Yiu, K.; Chan, T.O.; Bull, M.; Ling, K.C.; Dai, Z.; et al. Comparison of the immunogenicity of BNT162b2 and CoronaVac COVID-19 vaccines in Hong Kong. Respirology 2022, 27, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Sun, F.; Lin, Y.; Wang, X.; Gao, Y.; Ye, S. Paxlovid in patients who are immunocompromised and hospitalised with SARS-CoV-2 infection. Lancet Infect. Dis. 2022, 22, 1279. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef]
- Hu, X.; Xing, Y.; Jia, J.; Ni, W.; Liang, J.; Zhao, D.; Song, X.; Gao, R.; Jiang, F. Factors associated with negative conversion of viral RNA in patients hospitalized with COVID-19. Sci. Total Environ. 2020, 728, 138812. [Google Scholar] [CrossRef]
- Bennasrallah, C.; Zemni, I.; Dhouib, W.; Sriha, H.; Mezhoud, N.; Bouslama, S.; Taboubi, W.; Beji, M.O.; Kacem, M.; Abroug, H.; et al. Factors associated with a prolonged negative conversion of viral RNA in patients with COVID-19. Int. J. Infect. Dis. 2021, 105, 463–469. [Google Scholar] [CrossRef]
- Liu, B.; Totten, M.; Nematollahi, S.; Datta, K.; Memon, W.; Marimuthu, S.; Wolf, L.A.; Carroll, K.C.; Zhang, S.X. Development and Evaluation of a Fully Automated Molecular Assay Targeting the Mitochondrial Small Subunit rRNA Gene for the Detection of Pneumocystis jirovecii in Bronchoalveolar Lavage Fluid Specimens. J. Mol. Diagn. 2020, 22, 1482–1493. [Google Scholar] [CrossRef]
- Li, G.; Yang, F.; He, X.; Liu, Z.; Pi, J.; Zhu, Y.; Ke, X.; Liu, S.; Ou, M.; Guo, H.; et al. Anti-tuberculosis (TB) chemotherapy dynamically rescues Th1 and CD8+ T effector levels in Han Chinese pulmonary TB patients. Microbes Infect. 2020, 22, 119–126. [Google Scholar] [CrossRef]
- Da Silva, M.V.; Figueiredo, A.A.; Machado, J.R.; Castellano, L.C.; Alexandre, P.B.; Oliveira, R.F.; Faria, G.E.; Pereira, S.A.; Rodrigues, D.B.; Rodrigues, V., Jr. T Cell Activation and Proinflammatory Cytokine Production in Clinically Cured Tuberculosis Are Time-Dependent and Accompanied by Upregulation of IL-10. PLoS ONE 2013, 8, e65492. [Google Scholar] [CrossRef] [PubMed]
- DeWolf, S.; Laracy, J.C.; Perales, M.A.; Kamboj, M.; van den Brink, M.R.M.; Vardhana, S. SARS-CoV-2 in immunocompromised individuals. Immunity 2022, 55, 1779–1798. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Kim, J.W.; Kim, J.Y.; Kang, S.W.; Jang, C.Y.; Chang, E.; Yang, J.S.; Kim, K.C.; Jang, H.C.; Kim, D.S.; et al. The association between antibody responses and prolonged viable SARS-CoV-2 shedding in immunocompromised patients: A prospective cohort study. J. Infect. Dis. 2023, jiad579. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Overall (n = 223) | With TB (n = 34) | Without TB (n = 189) | p Value | |
|---|---|---|---|---|
| Age (years) | 47.0 (32.0–65.0) | 49.0 (31.8–59.8) | 47.0 (32.0–65.0) | 0.479 |
| Male (n, %) | 144 (64.6%) | 26 (76.5%) | 118 (62.4%) | 0.115 |
| BMI | 22.2 (20.6–24.5) | 21.8 (21.0–23.4) | 22.3 (20.6–24.6) | 0.428 |
| Comorbidities (%) | 71 (31.8%) | 13 (38.2%) | 58 (30.7%) | 0.384 |
| Diabetes | 35 (15.7%) | 8 (23.5%) | 27 (14.3%) | |
| Hypertension | 21 (9.4%) | 3 (8.8%) | 18 (9.5%) | |
| COPD | 12 (5.4%) | 2 (5.9%) | 10 (5.3%) | |
| Cardio-cerebrovascular disease | 13 (5.8%) | 2 (5.9%) | 11 (5.8%) | |
| Chronic kidney disease | 9 (4.0%) | 2 (5.9%) | 7 (3.7%) | |
| Cancer | 3 (1.3%) | 0 (0) | 3 (1.6%) | |
| Autoimmune disease | 2 (0.9%) | 0 (0) | 2 (1.1%) | |
| Vaccination booster | ||||
| Yes | 98 (43.9%) | 18 (52.9%) | 80 (42.3%) | 0.251 |
| TB location a | ||||
| PTB | / | 31 (91.2%) | / | / |
| EPTB | / | 7 (20.6%) | / | / |
| Clinical presentation on admission | 0.597 | |||
| Asymptomatic | 45 (20.2%) | 8 (23.5%) | 37 (19.6%) | |
| Symptomatic | 178 (79.8%) | 26 (76.5%) | 152 (80.4%) | |
| Laboratory findings on admission | ||||
| Blood leukocyte count (3.5–9.5 × 109/L) | 5.5 (4.3–7.2) | 5.4 (4.2–7.1) | 5.6 (4.3–7.2) | 0.724 |
| Lymphopenia b (%) | 69 (30.9%) | 15 (44.1%) | 54 (28.6%) | 0.071 |
| C-reactive protein ≥ 10 mg/L (%) | 46 (20.6%) | 10 (29.4%) | 36 (19.0%) | 0.169 |
| Overall (n = 223) | With TB (n = 34) | Without TB (n = 189) | p Value | |
|---|---|---|---|---|
| O2 supply (%) | 17 (7.6%) | 3 (8.8%) | 14 (7.4%) | 0.729  |
| Nirmatrelvir/ritonavir (%) | 15 (6.7%) | 3 (8.8%) | 12 (6.3%) | 0.707  |
| Required high-flow ventilation | 6 (2.7%) | 2 (5.8%) | 4 (2.1%) | 0.228  |
| Required IMV (%) | 3 (1.3%) | 1 (2.9%) | 2 (1.1%) | 0.393  |
| COVID-19 diagnosis | 0.142  | |||
| Severe or critical | 9 (4.0%) | 3 (8.8%) | 6 (3.2%) | |
Non-severe  | 214 (96.0%) | 31 (91.2%) | 183 (96.8%) | |
| Die (%) | 3 (1.3%) | 1 (2.9%) | 2 (1.1%) | 0.393  |
 Fisher’s exact test;
Fisher’s exact test;  non-severe include mild and moderate.
non-severe include mild and moderate.| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| With TB vs. without TB | 1.927 (1.325–2.803) | 0.001 | 2.207 (1.370–2.999) | 0.000 |
| Age (years) | 1.017 (1.009–1.025) | 0.000 | 1.018 (1.007–1.030) | 0.001 |
| Gender | ||||
| Male vs. female | 1.543 (1.165–2.044) | 0.003 | 1.083 (0.799–1.468) | 0.608 |
| BMI | 1.006 (0.960–1.053) | 0.806 | ||
| Comorbidities | ||||
| One or more vs. none | 1.481(1.114–1.967) | 0.007 | 1.166 (0.790–1.720) | 0.439 |
| Vaccination booster | ||||
| Yes vs. no | 0.927 (0.710–1.209) | 0.575 | 0.922 (0.703–1.210) | 0.558 |
| Treatment | ||||
| Paxlovid (required vs. not required) | 0.473 (0.271–0.827) | 0.009 | 0.823 (0.432–1.571) | 0.555 |
| Disease severity | ||||
Severe or critical vs. non-severe  | 5.667 (2.424–13.249) | 0.000 | 5.625 (2.103–15.046) | 0.001 |
 non-severe includes mild and moderate.
non-severe includes mild and moderate.Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, W.; Liu, P.; Yan, B.; Zheng, F.; Yang, Y.; Xi, X.; Xia, L.; Shen, Y. Impact of Tuberculosis on Disease Severity and Viral Shedding Duration in COVID-19 Patients. Viruses 2024, 16, 260. https://doi.org/10.3390/v16020260
Huang W, Liu P, Yan B, Zheng F, Yang Y, Xi X, Xia L, Shen Y. Impact of Tuberculosis on Disease Severity and Viral Shedding Duration in COVID-19 Patients. Viruses. 2024; 16(2):260. https://doi.org/10.3390/v16020260
Chicago/Turabian StyleHuang, Wei, Ping Liu, Bo Yan, Fang Zheng, Yang Yang, Xiuhong Xi, Lu Xia, and Yinzhong Shen. 2024. "Impact of Tuberculosis on Disease Severity and Viral Shedding Duration in COVID-19 Patients" Viruses 16, no. 2: 260. https://doi.org/10.3390/v16020260
APA StyleHuang, W., Liu, P., Yan, B., Zheng, F., Yang, Y., Xi, X., Xia, L., & Shen, Y. (2024). Impact of Tuberculosis on Disease Severity and Viral Shedding Duration in COVID-19 Patients. Viruses, 16(2), 260. https://doi.org/10.3390/v16020260