


Clinical Significance of Elevated KSHV Viral Load in HIV-Related Kaposi’s Sarcoma Patients in South Africa

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. KSHV Serology and Quantification and hIL-6 Assays
2.3. Statistical Analysis
2.4. Ethics
3. Results
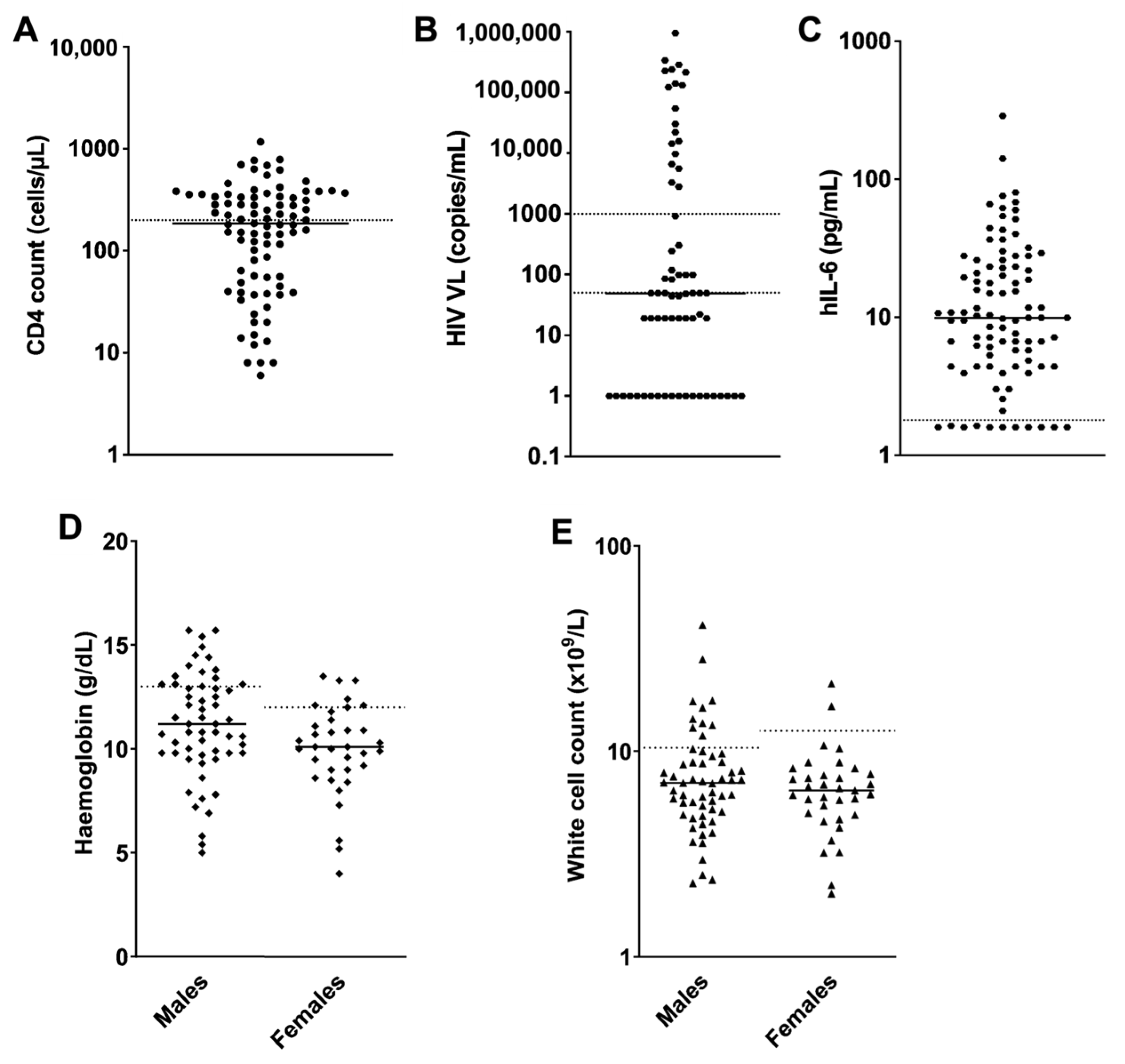
3.1. Patient Characteristics
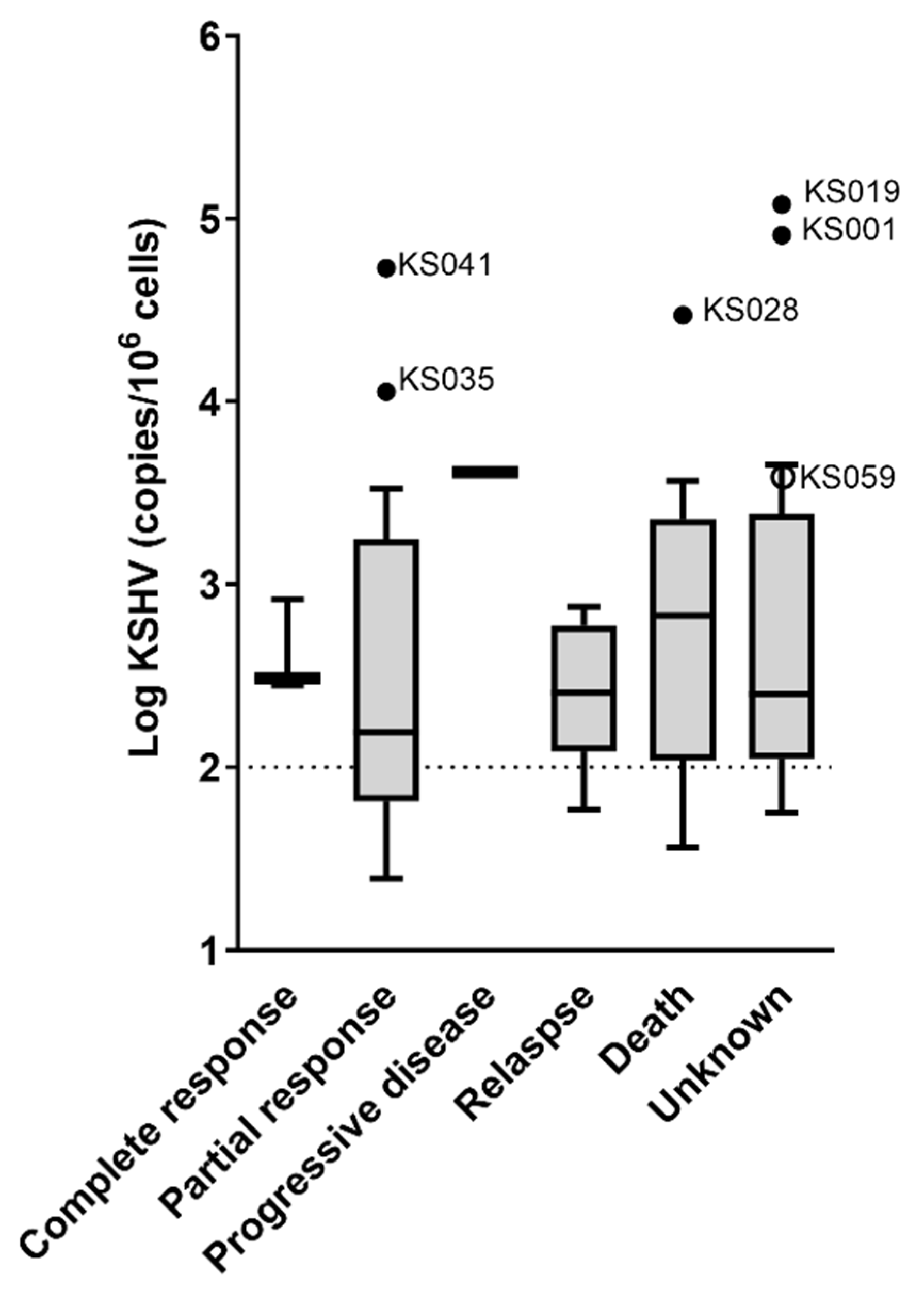
3.2. Association of KSHV VL with KS Severity, Response to Treatment and Outcome
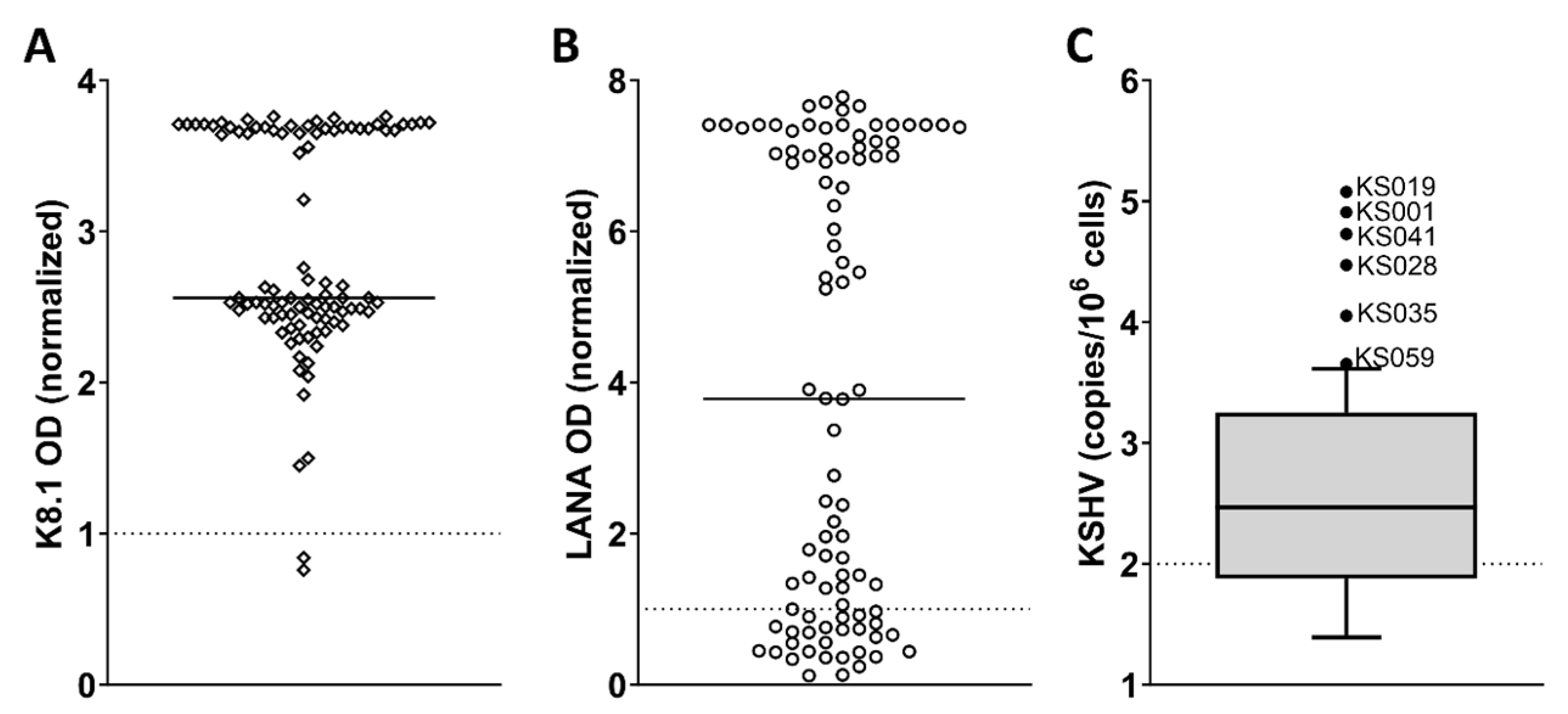
3.3. Severe Clinical Features of Patients with Extremely Elevated KSHV VL
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Newton, R.; Labo, N.; Wakeham, K.; Miley, W.; Asiki, G.; Johnston, W.T.; Whitby, D. Kaposi Sarcoma-Associated Herpesvirus in a Rural Ugandan Cohort, 1992–2008. J. Infect. Dis. 2018, 217, 263–269. [Google Scholar] [CrossRef]
- Jaffe, H.W.; Bregman, D.J.; Selik, R.M. Acquired Immune Deficiency Syndrome in the United States: The First 1000 Cases. J. Infect. Dis. 2017, 148, 339–345. [Google Scholar] [CrossRef]
- Mbulaiteye, S.M.; Biggar, R.J.; Pfeiffer, R.M.; Bakaki, P.M.; Gamache, C.; Owor, A.M.; Katongole-Mbidde, E.; Ndugwa, C.M.; Goedert, J.J.; Whitby, D.; et al. Water, Socioeconomic Factors, and Human Herpesvirus 8 Infection in Ugandan Children and Their Mothers. J. Acquir. Immune Defic. Syndr. 2005, 38, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Orenstein, J.M. Ultrastructure of Kaposi Sarcoma. Ultrastruct. Pathol. 2008, 32, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Gramolelli, S.; Schulz, T.F. The Role of Kaposi Sarcoma-Associated Herpesvirus in the Pathogenesis of Kaposi Sarcoma. J. Pathol. 2015, 235, 368–380. [Google Scholar] [CrossRef] [PubMed]
- Hengge, U.R.; Ruzicka, T.; Tyring, S.K.; Stuschke, M.; Roggendorf, M.; Schwartz, R.A.; Seeber, S. Update on Kaposi’s Sarcoma and Other HHV8 Associated Diseases. Part 1: Epidemiology, Environmental Predispositions, Clinical Manifestations, and Therapy. Lancet Infect. Dis. 2002, 2, 281–292. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Abrahamian, F.; Stroger, J.H. Gastrointestinal Kaposi’s Sarcoma. Am. J. Gastroenterol. 2012, 107, 2012. [Google Scholar] [CrossRef]
- Polizzotto, M.N.; Uldrick, T.S.; Hu, D.; Yarchoan, R. Clinical Manifestations of Kaposi Sarcoma Herpesvirus Lytic Activation: Multicentric Castleman Disease (KSHV-MCD) and the KSHV Inflammatory Cytokine Syndrome. Front. Microbiol. 2012, 3, 73. [Google Scholar] [CrossRef] [PubMed]
- Polizzotto, M.N.; Uldrick, T.S.; Wyvill, K.M.; Aleman, K.; Marshall, V.; Wang, V.; Whitby, D.; Pittaluga, S.; Jaffe, E.S.; Millo, C.; et al. Clinical Features and Outcomes of Patients with Symptomatic Kaposi Sarcoma Herpesvirus (KSHV)-Associated Inflammation: Prospective Characterization of KSHV Inflammatory Cytokine Syndrome (KICS). Clin. Infect. Dis. 2015, 62, 730–738. [Google Scholar] [CrossRef]
- Uldrick, T.S.; Wang, V.; O’Mahony, D.; Aleman, K.; Wyvill, K.M.; Marshall, V.; Steinberg, S.M.; Pittaluga, S.; Maric, I.; Whitby, D.; et al. An Interleukin-6-Related Systemic Inflammatory Syndrome in Patients Co-Infected with Kaposi Sarcoma-Associated Herpesvirus and HIV but without Multicentric Castleman Disease. Clin. Infect. Dis. 2010, 51, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Lurain, K.; Polizzotto, M.N.; Aleman, K.; Bhutani, M.; Wyvill, K.M.; Gonçalves, P.H.; Ramaswami, R.; Marshall, V.A.; Miley, W.; Steinberg, S.M.; et al. Viral, Immunologic, and Clinical Features of Primary Effusion Lymphoma. Blood 2019, 133, 1753–1761. [Google Scholar] [CrossRef]
- Oksenhendler, E.; Duarte, M.; Soulier, J.; Cacoub, P.; Welker, Y.; Cadranel, J.; Cazals-Hatem, D.; Autran, B.; Clauvel, J.; Raphael, M. Multicentric Castleman’s Disease in HIV Infection: A Clinical and Pathological Study of 20 Patients. AIDS 1996, 10, 61–67. [Google Scholar] [CrossRef]
- Goncalves, P.H.; Uldrick, T.S.; Yarchoan, Y. HIV-Associated Kaposi Sarcoma and Related Diseases. AIDS 2017, 31, 1903–1916. [Google Scholar] [CrossRef]
- Grulich, A.E.; Van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of Cancers in People with HIV/AIDS Compared with Immunosuppressed Transplant Recipients: A Meta-Analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Reid, E.; Suneja, G.; Ambinder, R.F.; Ard, K.; Baiocchi, R.; Barta, S.K.; Carchman, E.; Cohen, A.; Crysler, O.V.; Gupta, N.; et al. AIDS-Related Kaposi Sarcoma, Version 2.2019. JNCCN J. Natl. Compr. Cancer Netw. 2019, 17, 171–189. [Google Scholar] [CrossRef] [PubMed]
- Krown, S.E.; Metroka, C.; Wernz, J.C. Kaposi’s Sarcoma in the Acquired Immune Deficiency Syndrome: A Proposal for Uniform Evaluation, Response, and Staging Criteria. J. Clin. Oncol. 1989, 7, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Krown, S.E.; Testa, M.A.; Huang, J. AIDS-Related Kaposi’s Sarcoma: Prospective Validation of the AIDS Clinical Trials Group Staging Classification. AIDS Clinical Trials Group Oncology Committee. J. Clin. Oncol. 1997, 15, 3085–3092. [Google Scholar] [CrossRef]
- Okuku, F.; Krantz, E.M.; Kafeero, J.; Kamya, M.R.; Orem, J.; Casper, C.; Phipps, W. Evaluation of a Predictive Staging Model for HIV-Associated Kaposi Sarcoma in Uganda. J. Acquir. Immune Defic. Syndr. 2017, 74, 548–554. [Google Scholar] [CrossRef]
- Nasti, G.; Talamini, R.; Antinori, A.; Martellotta, F.; Jacchetti, G.; Chiodo, F.; Ballardini, G.; Stoppini, L.; Di Perri, G.; Mena, M.; et al. AIDS-Related Kaposi’s Sarcoma: Evaluation of Potential New Prognostic Factors and Assessment of the AIDS Clinical Trial Group Staging System in the Haart Era—The Italian Cooperative Group on AIDS and Tumors and the Italian Cohort of Patients Naïve from Antiretrovirals. J. Clin. Oncol. 2003, 21, 2876–2882. [Google Scholar] [CrossRef]
- Boffi, E.; Amari, E.; Toutous-Trellu, L.; Le Gayet-Ageron, A.; Baumann, M.; Cathomas, G.; Steffen, I.; Erb, P.; Mueller, N.J.; Furrer, H.; et al. Predicting the Evolution of Kaposi Sarcoma, in the Highly Active Antiretroviral Therapy Era. AIDS 2008, 22, 1019–1028. [Google Scholar] [CrossRef]
- Maurer, T.; Ponte, M.; Leslie, K. HIV-Associated Kaposi’s Sarcoma with a High CD4 Count and a Low Viral Load. N. Engl. J. Med. 2007, 357, 1352–1353. [Google Scholar] [CrossRef] [PubMed]
- Krown, S.E.; Moser, C.B.; MacPhail, P.; Matining, R.M.; Godfrey, C.; Caruso, S.R.; Hosseinipour, M.C.; Samaneka, W.; Nyirenda, M.; Busakhala, N.W.; et al. Treatment of Advanced AIDS-Associated Kaposi Sarcoma in Resource-Limited Settings: A Three-Arm, Open-Label, Randomised, Non-Inferiority Trial. Lancet 2020, 395, 1195–1207. [Google Scholar] [CrossRef]
- Freeman, E.E.; Busakhala, N.; Regan, S.; Asirwa, F.C.; Wenger, M.; Seth, D.; Moon, K.C.; Semeere, A.; Maurer, T.; Wools-Kaloustian, K.; et al. Real-World Use of Chemotherapy for Kaposi’s Sarcoma in a Large Community-Based HIV Primary Care System in Kenya. BMC Cancer 2020, 20, 71. [Google Scholar] [CrossRef]
- Whitby, D.; Howard, M.R.; Tenant-Flowers, M.; Brink, N.S.; Copas, A.; Boshoff, C.; Hatzioannou, T.; Suggett, F.E.; Aldam, D.M.; Denton, A.S. Detection of Kaposi Sarcoma Associated Herpesvirus in Peripheral Blood of HIV-Infected Individuals and Progression to Kaposi’s Sarcoma. Lancet 1995, 346, 799–802. [Google Scholar] [CrossRef] [PubMed]
- Jary, A.; Leducq, V.; Palich, R.; Gothland, A.; Descamps, D.; Joly, V.; Lambert-Niclot, S.; Amiel, C.; Canestri, A.; Mirand, A.; et al. Usefulness of Kaposi’s Sarcoma-Associated Herpesvirus (KSHV) DNA Viral Load in Whole Blood for Diagnosis and Monitoring of KSHV-Associated Diseases. J. Clin. Microbiol. 2018, 56, e00569-18. [Google Scholar] [CrossRef]
- Marcelin, A.; Motol, J.; Guihot, A.; Caumes, E.; Viard, J.; Dussaix, E.; Cadranel, J.; Francès, C.; Carcelain, G.; Calvez, V.; et al. Relationship between the Quantity of Kaposi Sarcoma–Associated Herpesvirus (KSHV) in Peripheral Blood and Effusion Fluid Samples and KSHV—Associated Disease. J. Infect. Dis. 2007, 196, 1163–1166. [Google Scholar] [CrossRef]
- Broccolo, F.; Din, C.T.; Viganò, M.G.; Rutigliano, T.; Esposito, S.; Lusso, P.; Tambussi, G.; Malnati, M.S. HHV-8 DNA Replication Correlates with the Clinical Status in AIDS-Related Kaposi’s Sarcoma. J. Clin. Virol. 2016, 78, 47–52. [Google Scholar] [CrossRef]
- Laney, A.S.; Cannon, M.J.; Jaffe, H.W.; Offermann, M.K.; Ou, C.Y.; Radford, K.W.; Patel, M.M.; Spira, T.J.; Gunthel, C.J.; Pellett, P.E.; et al. Human Herpesvirus 8 Presence and Viral Load Are Associated with the Progression of AIDS-Associated Kaposi’s Sarcoma. AIDS 2007, 21, 1541–1545. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.; Enbom, M.; Bidoli, E.; Linde, A.; De Paoli, P.; Dillner, J. Viral Load of Human Herpesvirus 8 in Peripheral Blood of Human Immunodeficiency Virus-Infected Patients with Kaposi’s Sarcoma. J. Clin. Microbiol. 2001, 39, 4269–4273. [Google Scholar] [CrossRef] [PubMed]
- Uldrick, T.S.; Polizzotto, M.N.; Aleman, K.; O’Mahony, D.; Wyvill, K.M.; Wang, V.; Marshall, V.; Pittaluga, S.; Steinberg, S.M.; Tosato, G.; et al. High-Dose Zidovudine plus Valganciclovir for Kaposi Sarcoma Herpesvirus-Associated Multicentric Castleman Disease: A Pilot Study of Virus-Activated Cytotoxic Therapy. Blood 2011, 117, 6977–6986. [Google Scholar] [CrossRef] [PubMed]
- Marcelin, A.; Aaron, L.; Mateus, C.; Gyan, E.; Gorin, I.; Viard, J.-P.; Calvez, V.; Dupin, N. Rituximab Therapy for HIV-Associated Castleman Disease. Blood 2003, 102, 2786–2788. [Google Scholar] [CrossRef]
- Blumenthal, M.J.; Schutz, C.; Barr, D.; Locketz, M.; Marshall, V.; Whitby, D.; Katz, A.A.; Uldrick, T.; Meintjes, G.; Schäfer, G. The Contribution of Kaposi’s Sarcoma-Associated Herpesvirus to Mortality in Hospitalized Human Immunodeficiency Virus-Infected Patients Being Investigated for Tuberculosis in South Africa. J. Infect. Dis. 2019, 220, 841–851. [Google Scholar] [CrossRef]
- Blumenthal, M.J.; Lambarey, H.; Chetram, A.; Riou, C.; Wilkinson, R.J.; Schäfer, G. Kaposi’s Sarcoma-Associated Herpesvirus, but Not Epstein-Barr Virus, Co-Infection Associates with Coronavirus Disease 2019 Severity and Outcome in South African Patients. Front. Microbiol. 2022, 12, 795555. [Google Scholar] [CrossRef] [PubMed]
- Borok, M.; Fiorillo, S.; Gudza, I.; Putnam, B.; Ndemera, B.; White, I.E.; Gwanzura, L.; Schooley, R.T.; Campbell, T.B. Evaluation of Plasma Human Herpesvirus 8 DNA as a Marker of Clinical Outcomes during Antiretroviral Therapy for AIDS-Related Kaposi Sarcoma in Zimbabwe. Clin. Infect. Dis. 2010, 51, 342–349. [Google Scholar] [CrossRef]
- Blumenthal, M.J.; Schutz, C.; Meintjes, G.; Mohamed, Z.; Mendelson, M.; Ambler, J.M.; Whitby, D.; Mackelprang, R.D.; Carse, S.; Katz, A.A.; et al. EPHA2 Sequence Variants Are Associated with Susceptibility to Kaposi’s Sarcoma-Associated Herpesvirus Infection and Kaposi’s Sarcoma Prevalence in HIV-Infected Patients. Cancer Epidemiol. 2018, 56, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Mwafongo, A.A.; Rosenberg, N.E.; Ng’ambi, W.; Werner, A.B.; Garneau, W.M.; Gumulira, J.; Phiri, S.; Hosseinipour, M.C. Treatment Outcomes of AIDS-Associated Kaposi’s Sarcoma under a Routine Antiretroviral Therapy Program in Lilongwe, Malawi: Bleomycin/Vincristine Compared to Vincristine Monotherapy. PLoS ONE 2014, 9, e91020. [Google Scholar] [CrossRef]
- Kranzer, K.; Bs, M.B.; Uk, M.; Lewis, J.J. Treatment Interruption in a Primary Care Antiretroviral Therapy Programme in South Africa: Cohort Analysis of Trends and Risk Factors. J. Acquir. Immune Defic. Syndr. 2010, 55, e17. [Google Scholar] [CrossRef]
- Mbisa, G.L.; Miley, W.; Gamache, C.J.; Gillette, W.K.; Esposito, D.; Hopkins, R.; Busch, M.P.; Schreiber, G.B.; Little, R.F.; Yarchoan, R.; et al. Detection of Antibodies to Kaposi’s Sarcoma-Associated Herpesvirus: A New Approach Using K8.1 ELISA and a Newly Developed Recombinant LANA ELISA. J. Immunol. Methods 2010, 356, 39–46. [Google Scholar] [CrossRef]
- De Sanjosé, S.; Marshall, V.; Solà, J.; Palacio, V.; Almirall, R.; Goedert, J.J.; Bosch, F.X.; Whitby, D. Prevalence of Kaposi’s Sarcoma-Associated Herpesvirus Infection in Sex Workers and Women from the General Population in Spain. Int. J. Cancer 2002, 98, 155–158. [Google Scholar] [CrossRef]
- Blumenthal, M.; Schutz, C.; Barr, D.; Marshall, V.; Locketz, M.; Whitby, D.; Katz, A.; Uldrick, T.; Meintjes, G.; Schäfer, G. The Contribution of KSHV to Mortality in Hospitalized HIV-Infected Patients Being Investigated for Tuberculosis in South Africa. In Proceedings of the Conference on Retroviruses and Opportunistic Infection, Seattle, WA, USA, 4–9 March 2019. [Google Scholar]
- Whitby, D.; Marshall, V.A.; Bagni, R.K.; Miley, W.J.; McCloud, T.G.; Hines-boykin, R.; Goedert, J.J.; Conde, B.A.; Mikovits, J.; Dittmer, D.P.; et al. Reactivation of Kaposi’s Sarcoma-Associated Herpesvirus by Natural Products from Kaposi’s Sarcoma Endemic Regions. Int. J. Cancer 2007, 120, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Borges, Á.H.; Connor, J.L.O.; Phillips, A.N.; Rönsholt, F.F.; Pett, S.; Vjecha, M.J. Factors Associated with Plasma IL-6 Levels during HIV Infection. J. Infect. Dis. 2015, 212, 585–595. [Google Scholar] [CrossRef] [PubMed]
- Box, A.G.E.P.; Tidwell, P.W. Transformation of the Independent Variables. Technometrics 1962, 4, 531–550. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) or Median (IQR) | |
|---|---|---|
| Sex | Male | 59 (63%) |
| Female | 35 (37%) | |
| Age (years) | 37 (32–42) | |
| On ART | Yes | 91 (97%) |
| No | 1 (1%) | |
| Unknown | 2 (2%) | |
| On ART for >1 year | Yes | 8 (9%) |
| No | 30 (32%) | |
| Unknown | 56 (59%) | |
| Defaulted on ART | Yes | 15 (16%) |
| No | 2 (2%) | |
| Unknown | 77 (82%) | |
| KS staging | T0 | 3 (3%) |
| T1 | 91 (97%) | |
| Lymphedema | 54 (59%) | |
| Extensive cutaneous disease | 20 (22%) | |
| Pulmonary KS | 12 (13%) | |
| GIT/another visceral site | 6 (6%) | |
| I0 | 48 (51%) | |
| I1 | 46 (49%) | |
| S0 | 85 (90%) | |
| S1 | 9 (10%) | |
| Response to treatment | Responded | 40 (43%) |
| Complete response | 3 (3%) | |
| Partial response | 37 (39%) | |
| Did not respond/progressed | 12 (13%) | |
| Progressive disease | 2 (2%) | |
| Relapse | 10 (11%) | |
| Died | 20 (21%) | |
| Unknown | 22 (23%) | |
| Survival at long-term follow-up | Survived | 36 (38%) |
| Died | 36 (38%) | |
| LTFU | 22 (24%) | |
| CD4 count at diagnosis (cells/µL) | 186 (55–341) | |
| Haemoglobin (g/dL) | Females | 10.1 (9.0–11.4) |
| Males | 11.2 (9.8–13.1) | |
| White cell count (×109 cells/L) | 6.7 (5.0–8.8) | |
| Platelets (×109 cells/L) | 320.5 (232.0–413.0) | |
| Albumin (g/L) | 34 (26–40) | |
| hIL-6 (pg/mL) | 9.9 (4.4–23.3) | |
| HIV VL (copies/mL) | 49 (1–5553) | |
| KSHV VL | Not detectable | 30 (32%) |
| Detectable | 64 (68%) | |
| Elevated >100 copies/106 cells | 46 (49%) | |
| KSHV VL (copies/106 cells) | 280.5 (69.7–1727.3) | |
| Characteristic | Unadjusted Odds Ratio | 95% CI for Unadjusted Odds Ratio | Adjusted Odds Ratio | 95% CI for Adjusted Odds Ratio | p Value | ||
|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | ||||
| KSHV viral load 1 | 1.79 | 0.78 | 4.14 | 5.55 | 1.28 | 24.14 | 0.022 * |
| Treatment stage: 2 | |||||||
| Mid-chemotherapy | 0.31 | 0.06 | 1.70 | 0.62 | 0.05 | 7.90 | 0.71 |
| Post-chemotherapy | 0.75 | 013 | 4.31 | 7.70 | 0.28 | 211.04 | 0.23 |
| Sex 3 | 0.45 | 0.09 | 2.30 | 0.00 | 0.00 | 0.00 | 0.99 |
| Age | 0.96 | 0.88 | 1.05 | 0.95 | 0.81 | 1.11 | 0.50 |
| CD4 count 4 | 1.00 | 1.00 | 1.00 | 1.01 | 1.00 | 1.01 | 0.070 |
| Host interleukin 6 (IL-6) | 1.01 | 0.99 | 1.02 | 1.00 | 0.98 | 1.02 | 0.94 |
| KSHV VL Outliers (n = 6) | Remainder of Cohort (n = 88) | p Value | |
|---|---|---|---|
| Male sex | 4 (67%) | 55 (63%) | 0.838 |
| Age (years) | 38.5 (35.7–44.5) | 35.5 (31.3–41.0) | 0.258 |
| K8.1 OD | 3.7 (2.6–3.7) | 2.6 (2.4–3.7) | 0.210 |
| LANA OD | 1.5 (0.6–2.7) | 3.9 (0.9–7.2) | 0.137 |
| KS staging | |||
| T1 | 6 (100%) | 85 (97%) | 0.646 |
| Lymphedema | 0 (0%) | 54 (63%) | - |
| Extensive cutaneous disease | 0 (0%) | 20 (23%) | - |
| Pulmonary KS | 4 (67%) | 7 (8%) | <0.001 * |
| GIT/another visceral site | 2 (33%) | 5 (6%) | 0.014 * |
| I1 | 6 (83%) | 41 (47%) | 0.107 |
| S1 | 2 (33%) | 7 (8%) | 0.100 |
| Response to treatment | |||
| Complete response | 0 (0%) | 3 (3%) | |
| Partial response | 2 (33%) | 35 (40%) | |
| Progressive disease | 0 (0%) | 2 (2%) | 0.687 |
| Relapse | 0 (0%) | 10 (11%) | |
| Died | 1 (17%) | 19 (22%) | |
| Unknown | 3 (50%) | 19 (22%) | |
| Survival at long-term follow-up | |||
| Survived | 1 (17%) | 35 (40%) | |
| Died | 4 (66%) | 32 (36%) | 0.324 |
| LTFU | 1 (17%) | 21 (24%) | |
| CD4 count at diagnosis (cells/µL) | 57.0 (42.5–317) | 202.5 (55.8–345.0) | 0.484 |
| HIV VL (copies/mL) | 44.0 (1.0–3236.5) | 49.0 (1.0–7348.3) | 0.668 |
| Anaemic | 6 (100%) | 65 (75.6%) | 0.168 |
| White cell count (×109 cells/L) | 7.7 (6.7–10.0) | 6.4 (4.9–8.7) | 0.209 |
| Platelets (×109 cells/L) | 392 (252–518) | 300 (229–403) | 0.243 |
| hIL-6 (pg/mL) | 22.36 (11.77–66.10) | 9.86 (4.40–23.05) | 0.040 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tibenderana, R.M.; Blumenthal, M.J.; Bukajumbe, E.; Schäfer, G.; Mohamed, Z. Clinical Significance of Elevated KSHV Viral Load in HIV-Related Kaposi’s Sarcoma Patients in South Africa. Viruses 2024, 16, 189. https://doi.org/10.3390/v16020189
Tibenderana RM, Blumenthal MJ, Bukajumbe E, Schäfer G, Mohamed Z. Clinical Significance of Elevated KSHV Viral Load in HIV-Related Kaposi’s Sarcoma Patients in South Africa. Viruses. 2024; 16(2):189. https://doi.org/10.3390/v16020189
Chicago/Turabian StyleTibenderana, Rebecca Monica, Melissa Jayne Blumenthal, Emmanuel Bukajumbe, Georgia Schäfer, and Zainab Mohamed. 2024. "Clinical Significance of Elevated KSHV Viral Load in HIV-Related Kaposi’s Sarcoma Patients in South Africa" Viruses 16, no. 2: 189. https://doi.org/10.3390/v16020189
APA StyleTibenderana, R. M., Blumenthal, M. J., Bukajumbe, E., Schäfer, G., & Mohamed, Z. (2024). Clinical Significance of Elevated KSHV Viral Load in HIV-Related Kaposi’s Sarcoma Patients in South Africa. Viruses, 16(2), 189. https://doi.org/10.3390/v16020189