
In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants

 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Cells and Viral Stocks
2.2. Drugs and Cytotoxicity Assay
2.3. Antiviral Activity Assay
2.4. Dose-Effect Relationships with Compound Combinations
2.5. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Semenzato, L.; Botton, J.; Drouin, J.; Baricault, B.; Bertrand, M.; Jabagi, M.-J.; Cuenot, F.; Le Vu, S.; Dray-Spira, R.; Weill, A.; et al. Characteristics Associated with the Residual Risk of Severe COVID-19 after a Complete Vaccination Schedule: A Cohort Study of 28 Million People in France. Lancet Reg. Health. Eur. 2022, 19, 100441. [Google Scholar] [CrossRef] [PubMed]
- Turtle, L.; Thorpe, M.; Drake, T.M.; Swets, M.; Palmieri, C.; Russell, C.D.; Ho, A.; Aston, S.; Wootton, D.G.; Richter, A.; et al. Outcome of COVID-19 in Hospitalised Immunocompromised Patients: An Analysis of the WHO ISARIC CCP-UK Prospective Cohort Study. PLoS Med. 2023, 20, e1004086. [Google Scholar] [CrossRef] [PubMed]
- Qu, P.; Faraone, J.N.; Evans, J.P.; Zheng, Y.-M.; Carlin, C.; Anghelina, M.; Stevens, P.; Fernandez, S.; Jones, D.; Panchal, A.R.; et al. Enhanced Evasion of Neutralizing Antibody Response by Omicron XBB.1.5, CH.1.1, and CA.3.1 Variants. Cell Rep. 2023, 42, 112443. [Google Scholar] [CrossRef] [PubMed]
- Menegale, F.; Manica, M.; Zardini, A.; Guzzetta, G.; Marziano, V.; d’Andrea, V.; Trentini, F.; Ajelli, M.; Poletti, P.; Merler, S. Evaluation of Waning of SARS-CoV-2 Vaccine-Induced Immunity: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2023, 6, e2310650. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, S.S.; Stern, R.A.; Patel, P.C.; Chu, D.K. COVID-19 Treatments: Then and Now. J. Allergy Clin. Immunol. Pract. 2023, 11, 3321–3333. [Google Scholar] [CrossRef] [PubMed]
- Touret, F.; Giraud, E.; Bourret, J.; Donati, F.; Tran-Rajau, J.; Chiaravalli, J.; Lemoine, F.; Agou, F.; Simon-Lorière, E.; van der Werf, S.; et al. Enhanced Neutralization Escape to Therapeutic Monoclonal Antibodies by SARS-CoV-2 Omicron Sub-Lineages. iScience 2023, 26, 106413. [Google Scholar] [CrossRef]
- Cho, J.; Shin, Y.; Yang, J.-S.; Kim, J.W.; Kim, K.-C.; Lee, J.-Y. Evaluation of Antiviral Drugs against Newly Emerged SARS-CoV-2 Omicron Subvariants. Antivir. Res. 2023, 214, 105609. [Google Scholar] [CrossRef]
- Del Borgo, C.; Garattini, S.; Bortignon, C.; Carraro, A.; Di Trento, D.; Gasperin, A.; Grimaldi, A.; De Maria, S.G.; Corazza, S.; Tieghi, T.; et al. Effectiveness, Tolerability and Prescribing Choice of Antiviral Molecules Molnupiravir, Remdesivir and Nirmatrelvir/r: A Real-World Comparison in the First Ten Months of Use. Viruses 2023, 15, 1025. [Google Scholar] [CrossRef]
- Li, G.; Hilgenfeld, R.; Whitley, R.; De Clercq, E. Therapeutic Strategies for COVID-19: Progress and Lessons Learned. Nat. Rev. Drug Discov. 2023, 22, 449–475. [Google Scholar] [CrossRef]
- Shyr, Z.A.; Cheng, Y.-S.; Lo, D.C.; Zheng, W. Drug Combination Therapy for Emerging Viral Diseases. Drug Discov. Today 2021, 26, 2367–2376. [Google Scholar] [CrossRef]
- Gidari, A.; Sabbatini, S.; Schiaroli, E.; Bastianelli, S.; Pierucci, S.; Busti, C.; Comez, L.; Libera, V.; Macchiarulo, A.; Paciaroni, A.; et al. The Combination of Molnupiravir with Nirmatrelvir or GC376 Has a Synergic Role in the Inhibition of SARS-CoV-2 Replication In Vitro. Microorganisms 2022, 10, 1475. [Google Scholar] [CrossRef] [PubMed]
- Nguyenla, X.; Wehri, E.; Van Dis, E.; Biering, S.B.; Yamashiro, L.H.; Zhu, C.; Stroumza, J.; Dugast-Darzacq, C.; Graham, T.G.W.; Wang, X.; et al. Discovery of SARS-CoV-2 Antiviral Synergy between Remdesivir and Approved Drugs in Human Lung Cells. Sci. Rep. 2022, 12, 18506. [Google Scholar] [CrossRef] [PubMed]
- Wagoner, J.; Herring, S.; Hsiang, T.-Y.; Ianevski, A.; Biering, S.B.; Xu, S.; Hoffmann, M.; Pöhlmann, S.; Gale, M.; Aittokallio, T.; et al. Combinations of Host- and Virus-Targeting Antiviral Drugs Confer Synergistic Suppression of SARS-CoV-2. Microbiol. Spectr. 2022, 10, e0333122. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sacramento, C.Q.; Jockusch, S.; Chaves, O.A.; Tao, C.; Fintelman-Rodrigues, N.; Chien, M.; Temerozo, J.R.; Li, X.; Kumar, S.; et al. Combination of Antiviral Drugs Inhibits SARS-CoV-2 Polymerase and Exonuclease and Demonstrates COVID-19 Therapeutic Potential in Viral Cell Culture. Commun. Biol. 2022, 5, 154. [Google Scholar] [CrossRef] [PubMed]
- Abdelnabi, R.; Maes, P.; de Jonghe, S.; Weynand, B.; Neyts, J. Combination of the Parent Analogue of Remdesivir (GS-441524) and Molnupiravir Results in a Markedly Potent Antiviral Effect in SARS-CoV-2 Infected Syrian Hamsters. Front. Pharmacol. 2022, 13, 1072202. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.H.; Chokkakula, S.; Min, S.C.; Kim, B.K.; Choi, W.-S.; Oh, S.; Yun, Y.S.; Kang, D.H.; Lee, O.-J.; Kim, E.-G.; et al. Combination Therapy with Nirmatrelvir and Molnupiravir Improves the Survival of SARS-CoV-2 Infected Mice. Antivir. Res. 2022, 208, 105430. [Google Scholar] [CrossRef] [PubMed]
- Gidari, A.; Sabbatini, S.; Schiaroli, E.; Bastianelli, S.; Pierucci, S.; Busti, C.; Saraca, L.M.; Capogrossi, L.; Pasticci, M.B.; Francisci, D. Synergistic Activity of Remdesivir-Nirmatrelvir Combination on a SARS-CoV-2 In Vitro Model and a Case Report. Viruses 2023, 15, 1577. [Google Scholar] [CrossRef] [PubMed]
- Lanzafame, M.; Gottardi, M.; Guella, L.; Collini, L.; Costa, G.; Guella, A.; Vento, S. Successful Treatment of Persistent SARS-CoV-2 Infection with Nirmatrelvir/Ritonavir plus Sotrovimab in Four Immunocompromised Patients. J. Chemother. 2023, 35, 623–626. [Google Scholar] [CrossRef]
- Marangoni, D.; Antonello, R.M.; Coppi, M.; Palazzo, M.; Nassi, L.; Streva, N.; Povolo, L.; Malentacchi, F.; Zammarchi, L.; Rossolini, G.M.; et al. Combination Regimen of Nirmatrelvir/Ritonavir and Molnupiravir for the Treatment of Persistent SARS-CoV-2 Infection: A Case Report and a Scoping Review of the Literature. Int. J. Infect. Dis. 2023, 133, 53–56. [Google Scholar] [CrossRef]
- Mikulska, M.; Sepulcri, C.; Dentone, C.; Magne, F.; Balletto, E.; Baldi, F.; Labate, L.; Russo, C.; Mirabella, M.; Magnasco, L.; et al. Triple Combination Therapy with 2 Antivirals and Monoclonal Antibodies for Persistent or Relapsed Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Immunocompromised Patients. Clin. Infect. Dis. 2023, 77, 280–286. [Google Scholar] [CrossRef]
- Zhu, Y.; Binder, J.; Yurgelonis, I.; Rai, D.K.; Lazarro, S.; Costales, C.; Kobylarz, K.; McMonagle, P.; Steppan, C.M.; Aschenbrenner, L.; et al. Generation of a VeroE6 Pgp Gene Knock out Cell Line and Its Use in SARS-CoV-2 Antiviral Study. Antivir. Res. 2022, 208, 105429. [Google Scholar] [CrossRef] [PubMed]
- Fiaschi, L.; Dragoni, F.; Schiaroli, E.; Bergna, A.; Rossetti, B.; Giammarino, F.; Biba, C.; Gidari, A.; Lai, A.; Nencioni, C.; et al. Efficacy of Licensed Monoclonal Antibodies and Antiviral Agents against the SARS-CoV-2 Omicron Sublineages BA.1 and BA.2. Viruses 2022, 14, 1374. [Google Scholar] [CrossRef] [PubMed]
- Vicenti, I.; Martina, M.G.; Boccuto, A.; De Angelis, M.; Giavarini, G.; Dragoni, F.; Marchi, S.; Trombetta, C.M.; Crespan, E.; Maga, G.; et al. System-Oriented Optimization of Multi-Target 2,6-Diaminopurine Derivatives: Easily Accessible Broad-Spectrum Antivirals Active against Flaviviruses, Influenza Virus and SARS-CoV-2. Eur. J. Med. Chem. 2021, 224, 113683. [Google Scholar] [CrossRef] [PubMed]
- Ianevski, A.; Giri, A.K.; Aittokallio, T. SynergyFinder 3.0: An Interactive Analysis and Consensus Interpretation of Multi-Drug Synergies across Multiple Samples. Nucleic Acids Res. 2022, 50, W739–W743. [Google Scholar] [CrossRef] [PubMed]
- Yadav, B.; Wennerberg, K.; Aittokallio, T.; Tang, J. Searching for Drug Synergy in Complex Dose-Response Landscapes Using an Interaction Potency Model. Comput. Struct. Biotechnol. J. 2015, 13, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Koszalka, P.; Subbarao, K.; Baz, M. Preclinical and Clinical Developments for Combination Treatment of Influenza. PLoS Pathog. 2022, 18, e1010481. [Google Scholar] [CrossRef]
- Yan, D.; Yan, B. Viral Target and Metabolism-Based Rationale for Combined Use of Recently Authorized Small Molecule COVID-19 Medicines: Molnupiravir, Nirmatrelvir, and Remdesivir. Fundam. Clin. Pharmacol. 2023, 37, 726–738. [Google Scholar] [CrossRef]
- Ahmadi, A.S.; Zadheidar, S.; Sadeghi, K.; Nejati, A.; Salimi, V.; Hajiabdolbaghi, M.; Mokhtari-Azad, T.; Yavarian, J. SARS-CoV-2 Intrahost Evolution in Immunocompromised Patients in Comparison with Immunocompetent Populations after Treatment. J. Med. Virol. 2023, 95, e28877. [Google Scholar] [CrossRef]
- Hogan, J.I.; Duerr, R.; Dimartino, D.; Marier, C.; Hochman, S.E.; Mehta, S.; Wang, G.; Heguy, A. Remdesivir Resistance in Transplant Recipients with Persistent Coronavirus Disease 2019. Clin. Infect. Dis. 2023, 76, 342–345. [Google Scholar] [CrossRef]
- Yang, S.; Multani, A.; Garrigues, J.M.; Oh, M.S.; Hemarajata, P.; Burleson, T.; Green, N.M.; Oliai, C.; Gaynor, P.T.; Beaird, O.E.; et al. Transient SARS-CoV-2 RNA-Dependent RNA Polymerase Mutations after Remdesivir Treatment for Chronic COVID-19 in Two Transplant Recipients: Case Report and Intra-Host Viral Genomic Investigation. Microorganisms 2023, 11, 2096. [Google Scholar] [CrossRef]
- Zuckerman, N.S.; Bucris, E.; Keidar-Friedman, D.; Amsalem, M.; Brosh-Nissimov, T. Nirmatrelvir Resistance-de Novo E166V/L50V Mutations in an Immunocompromised Patient Treated with Prolonged Nirmatrelvir/Ritonavir Monotherapy Leading to Clinical and Virological Treatment Failure—A Case Report. Clin. Infect. Dis. 2023, ciad494. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Carr, E.J.; Harvey, R.; Mears, H.V.; Kjaer, S.; Townsley, H.; Hobbs, A.; Ragno, M.; Herman, L.S.; Adams, L.; et al. WHO’s Therapeutics and COVID-19 Living Guideline on MAbs Needs to Be Reassessed. Lancet 2022, 400, 2193–2196. [Google Scholar] [CrossRef] [PubMed]
- Foucquier, J.; Guedj, M. Analysis of Drug Combinations: Current Methodological Landscape. Pharmacol. Res. Perspect. 2015, 3, e00149. [Google Scholar] [CrossRef] [PubMed]
- Fuentealba-Manosalva, O.; Mansilla, M.; Buelvas, N.; Martin-Martin, A.; Torres, C.G.; López-Muñoz, R.A. Mind the Curve: Dose-Response Fitting Biases the Synergy Scores across Software Used for Chemotherapy Combination Studies. Int. J. Mol. Sci. 2023, 24, 9705. [Google Scholar] [CrossRef]
- Wooten, D.J.; Meyer, C.T.; Lubbock, A.L.R.; Quaranta, V.; Lopez, C.F. MuSyC Is a Consensus Framework That Unifies Multi-Drug Synergy Metrics for Combinatorial Drug Discovery. Nat. Commun. 2021, 12, 4607. [Google Scholar] [CrossRef]
- Plebani, R.; Bai, H.; Si, L.; Li, J.; Zhang, C.; Romano, M. 3D Lung Tissue Models for Studies on SARS-CoV-2 Pathophysiology and Therapeutics. Int. J. Mol. Sci. 2022, 23, 10071. [Google Scholar] [CrossRef]
- Lin, Q.; Lu, C.; Hong, Y.; Li, R.; Chen, J.; Chen, W.; Chen, J. Animal models for studying coronavirus infections and developing antiviral agents and vaccines. Antivir. Res. 2022, 203, 105345. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| CC50 µM Mean ± SD | CC10 µM Mean ± SD | IC50 µM vs. B.1 Mean ± SD | IC90 µM vs. B.1 Mean ± SD | IC50 µM vs. BQ.1.1 Mean ± SD | IC90 µM vs. BQ.1.1 Mean ± SD | |
|---|---|---|---|---|---|---|
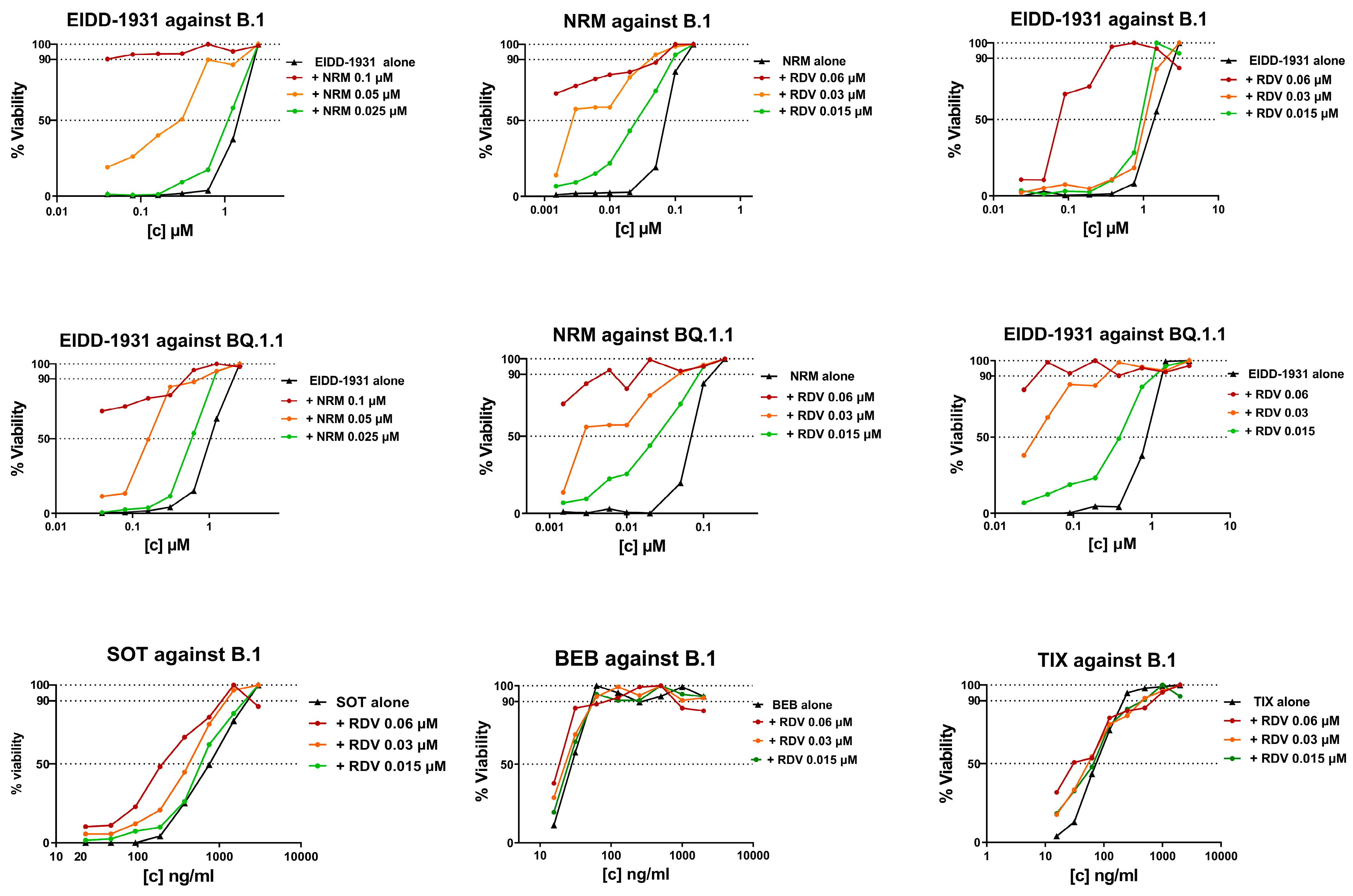
| NRM | 40.7 ± 4.0 | 2.9 ± 0.2 | 0.1 ± 0.03 | 0.2 ± 0.1 | 0.1 ± 0.01 | 0.2 ± 0.01 |
| EIDD-1931 | 43.3 ± 6.0 | 3.1 ± 0.4 | 2.4 ± 0.4 | 2.5 ± 0.1 | 1.6 ± 0.4 | 1.8 ± 0.7 |
| RDV | 17.2 ± 0.2 | 4.2 ± 0.6 | 0.06 ± 0.03 | 0.2 ± 0.05 | 0.03 ± 0.01 | 0.1 ± 0.01 |
| CC50 ng/mL Mean ± SD | CC10 ng/mL Mean ± SD | IC50 ng/mL vs. B.1 Mean ± SD | IC90 ng/mL vs. B.1 Mean ± SD | IC50 µM vs. BQ.1.1 Mean ± SD | IC90 µM vs. BQ.1.1 Mean ± SD | |
| SOT | >2400 | >2400 | 813 ± 324 | 1718 ± 594 | NA | NA |
| BEB | >60 | >60 | 33 ± 7 | 89 ± 9 | NA | NA |
| CIL | >360 | >360 | 204 ±1354 | 1385 ± 862 | NA | NA |
| TIX | >360 | >360 | 68 ± 41 | 305 ± 71 | NA | NA |
| Summary SS vs. B.1 Mean ± SD | Weighted SS vs. B.1 Mean ± SD | Summary SS vs. BQ.1.1 Mean ± SD | Weighted SS vs. BQ.1.1 Mean ± SD | |
|---|---|---|---|---|
| NRM/EIDD-1931 | −3.1 ± 3.1 | 2.1 ± 0.4 | −2.7 ± 1.3 | 0.0 ± 0.7 |
| RDV/EIDD-1931 | 0.4 ± 6.2 | 0.9 ± 0.7 | 2.6 ± 6.5 | 1.7 ± 2.5 |
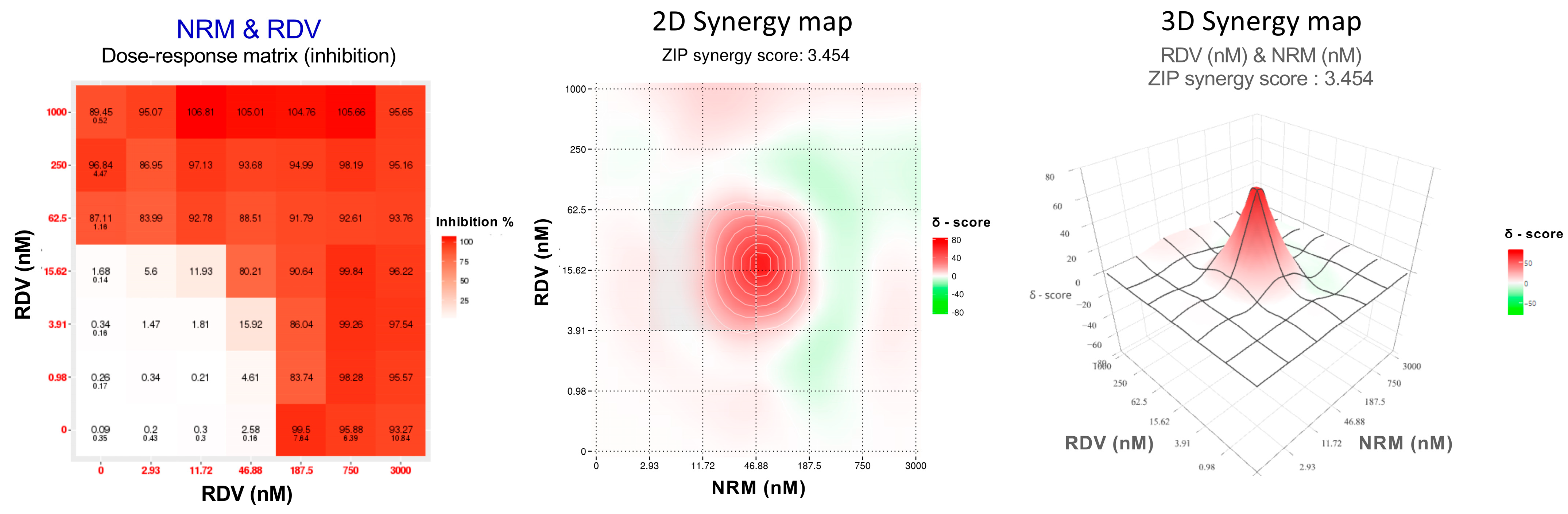
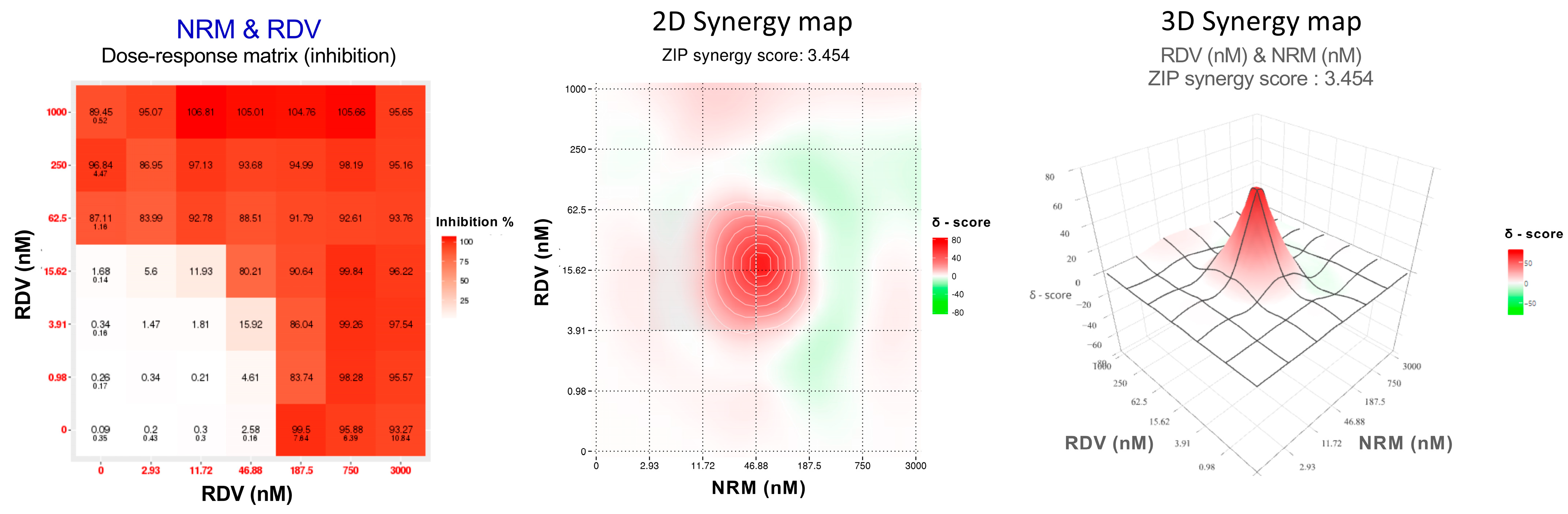
| NRM/RDV | 2.0 ± 2.0 | 1.9 ± 1.4 | −0.2 ± 3.7 | 2.1 ± 2.1 |
| RDV/SOT | 8.8 ± 10.3 | 6.1 ± 2.9 | NP | NP |
| RDV/BEB | 5.7 ± 2.6 | 4.2 ± 3.3 | NP | NP |
| RDV/TIX | 0.6 ± 6.4 | 2.6 ± 2.7 | NP | NP |
| RDV/CIL | −2.0 ± 0.5 | 0.8 ± 0.1 | NP | NP |
| Synergy Score Stratum | Drug Combination | Concentrations a | Viral Variant |
|---|---|---|---|
| >50 | RDV/NRM | 0.02/0.05 | B.1 and BQ1.1 |
| RDV/SOT | 0.04/8.8 | B.1 | |
| 0.04/35.2 | |||
| 0.04/140.6 | |||
| RDV/BEB | 0.04/0.6 | B.1 | |
| 0.04/2.2 | |||
| 0.04/8.9 | |||
| RDV/TIX | 0.04/2.2 | B.1 | |
| 0.04/8.8 | |||
| 30–50 | NRM/EIDD-1931 | 0.05/0.75 | B.1 |
| 0.05/1.50 | B.1 and BQ.1.1 | ||
| RDV/SOT | 0.01/562.5 | B.1 | |
| 0.04/562.5 | B.1 | ||
| RDV/TIX | 0.04/35 | B.1 | |
| 10–29.9 | NRM/EIDD-1931 | 0.003/0.07 | B.1 |
| 0.01/0.08 | B.1 | ||
| 0.05/0.09 | B.1 | ||
| RDV/EIDD-1931 | 0.02/1.5 | B.1 and BQ.1.1 | |
| 0.03/0.75 | BQ.1.1 | ||
| RDV/NRM | 0.02/0.05 | B.1 | |
| 0.004/0.05 | B.1 and BQ.1.1 | ||
| 0.006/0.05 | BQ.1.1 | ||
| 0.02/0.03 | BQ.1.1 | ||
| 0.02/0.01 | BQ.1.1 | ||
| RDV/BEB | 0.01/8.9 | B.1 | |
| RDV/TIX | 0.01/35 | B.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiaschi, L.; Biba, C.; Varasi, I.; Bartolini, N.; Paletti, C.; Giammarino, F.; Saladini, F.; Zazzi, M.; Vicenti, I. In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants. Viruses 2024, 16, 168. https://doi.org/10.3390/v16020168
Fiaschi L, Biba C, Varasi I, Bartolini N, Paletti C, Giammarino F, Saladini F, Zazzi M, Vicenti I. In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants. Viruses. 2024; 16(2):168. https://doi.org/10.3390/v16020168
Chicago/Turabian StyleFiaschi, Lia, Camilla Biba, Ilenia Varasi, Niccolò Bartolini, Chiara Paletti, Federica Giammarino, Francesco Saladini, Maurizio Zazzi, and Ilaria Vicenti. 2024. "In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants" Viruses 16, no. 2: 168. https://doi.org/10.3390/v16020168
APA StyleFiaschi, L., Biba, C., Varasi, I., Bartolini, N., Paletti, C., Giammarino, F., Saladini, F., Zazzi, M., & Vicenti, I. (2024). In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants. Viruses, 16(2), 168. https://doi.org/10.3390/v16020168