
Is San Diego California on Track to Reach HCV Elimination? A Modeling Analysis of Combination Prevention Strategies

 ,
, 
Abstract
1. Introduction
2. Methods
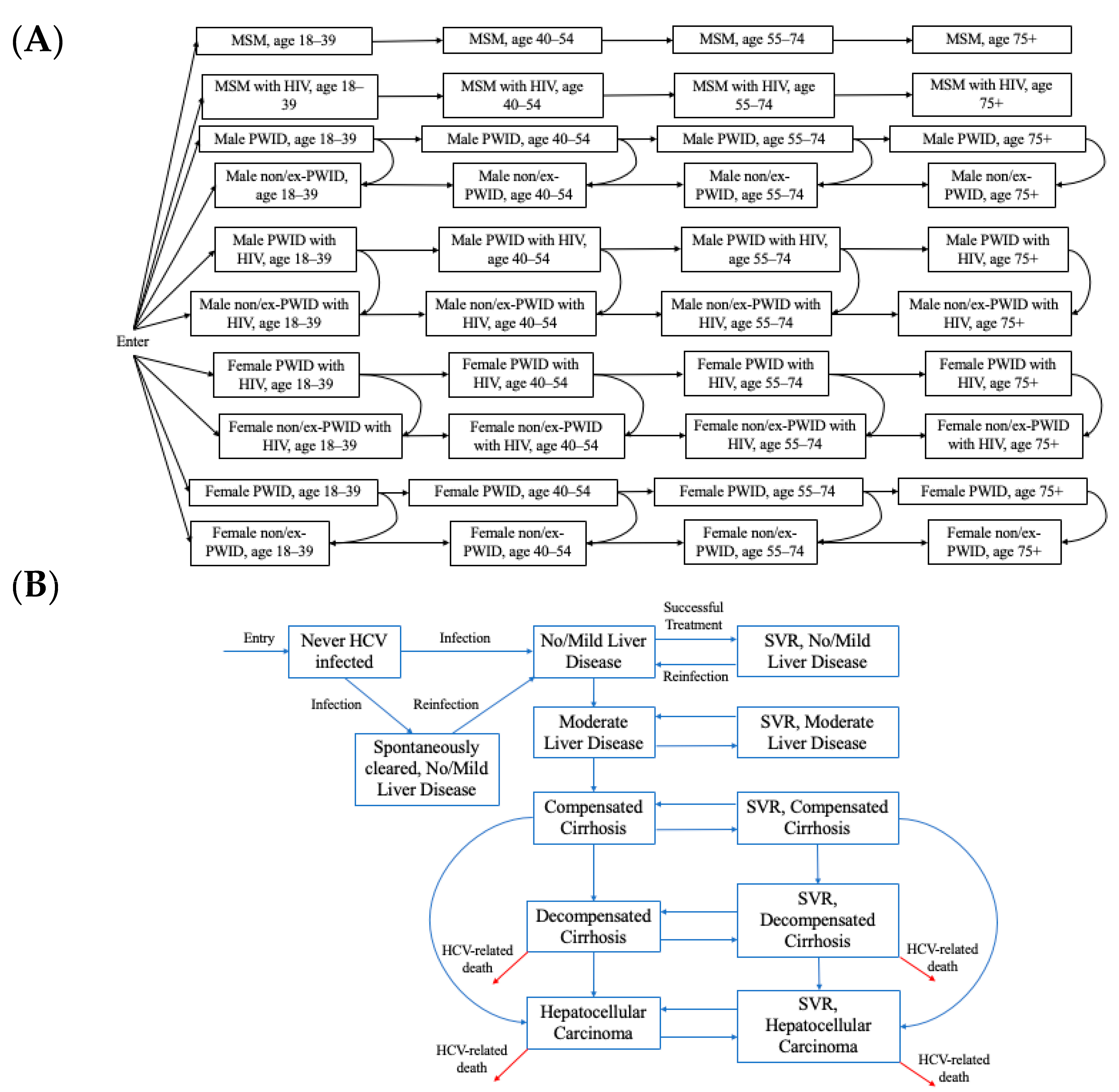
2.1. Model Description
2.2. Model Parameterization and Calibration
2.3. Modeled Scenarios
- Scenario 1 (status quo): Continuation of current treatment rates (65.1% among people coinfected with HCV and HIV, 0% among PWID and MSM without HIV, and 5%/year among ex/non-PWID without HIV).
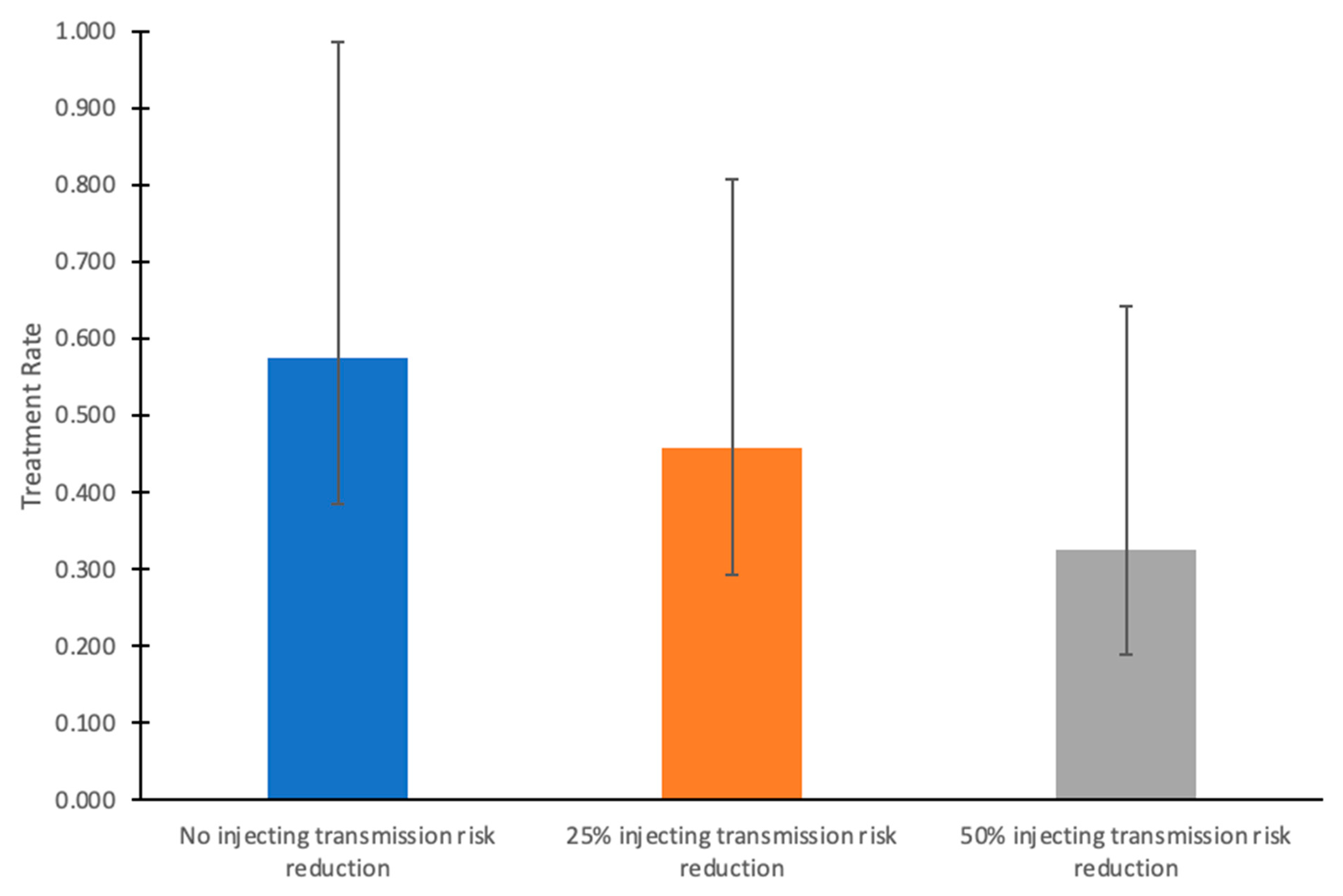
- Scenario 2 (scale-up to meet the 80% incidence elimination goal without injecting transmission risk reduction from 2024 onward): Scale-up of HCV treatment among people without HIV from 2024 onward to a rate that achieves an 80% reduction in new HCV infections from 2030 compared to 2015. This rate was determined through model calibration. Treatment among people coinfected with HCV and HIV is held constant at 65%/year.
- Scenario 3 (scale-up to meet the 80% incidence elimination goal with 25% injecting transmission risk reduction from 2024 onward): Reduction in injecting transmission risk by 25% from 2024 onward combined with scale-up of HCV treatment among people without HIV from 2024 onward to a rate that achieves an 80% reduction in new HCV infections from 2030 compared to 2015. This rate was determined through model calibration. Treatment among people coinfected with HCV and HIV is held constant at 65%/year.
- Scenario 4 (scale-up to meet the 80% incidence elimination goal with 50% injecting transmission risk reduction from 2024 onward): Reduction in injecting transmission risk by 50% from 2024 onward combined with scale-up of HCV treatment among people without HIV from 2024 onward to a rate that achieves an 80% reduction in new HCV infections from 2030 compared to 2015. This rate was determined through model calibration. Treatment among people coinfected with HCV and HIV is held constant at 65%/year.
2.4. Sensitivity and Uncertainty Analyses
3. Results
3.1. Treatment Needed to Reach Elimination
3.2. Uncertainty Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajarizadeh, B.; Grebely, J.; Dore, G. Epidemiology and natural history of HCV infection. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 553–562. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Consolidated Strategic Information Guidelines for Viral Hepatitis: Planning and Tracking Progress Towards Elimination. 2018. Available online: https://www.who.int/publications/i/item/9789241515191 (accessed on 22 May 2021).
- Leslie, M. White House budget includes push to eliminate hepatitis C. Science 2023, 379, 1077. [Google Scholar] [CrossRef]
- Alcorn, T. Lags Behind Other Countries in Hepatitis-C Treatment. The New York Times. Updated 29 April 2024. Available online: https://www.nytimes.com/2024/04/28/health/hepatitis-c.html (accessed on 20 June 2024).
- Wynn, A.; Tweeten, S.; McDonald, E.; Wooten, W.; Lucas, K.; Cyr, C.L.; Hernandez, M.; Ramirez, F.; VanWormer, C.; Suckow, S.; et al. The estimated hepatitis C seroprevalence and key population sizes in San Diego in 2018. PLoS ONE 2021, 16, e0251635. [Google Scholar] [CrossRef]
- Suckow, S.; Ramers, C. Eliminate Hepatitis C COSD Initiative. Live Well San Diego. 2019. Available online: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/bhs/documents/NOC/bhab/Eliminate%20Hepatitis%20C%20San%20Diego%20County%20Inititiative%20PPT_BHAB.pdf (accessed on 22 May 2021).
- Cheema, J.S.; Mathews, W.C.; Wynn, A.; Bamford, L.B.; Torriani, F.J.; Hill, L.A.; Rajagopal, A.V.; Yin, J.; Jain, S.; Garfein, R.S.; et al. Hepatitis C Virus Micro-elimination Among People With HIV in San Diego: Are We on Track? Open Forum Infect. Dis. 2023, 10, ofad153. [Google Scholar] [CrossRef]
- San Diego Health and Human Services Agency. HIV/AIDS Epidemiology Report—2016. 2017. Available online: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/EpiReport2017final.pdf (accessed on 22 May 2021).
- U.S. Centers for Disease Control and Prevention. NCHHSTP AtlasPlus. Updated 1 October 2021. Available online: https://gis.cdc.gov/grasp/nchhstpatlas/charts.html (accessed on 5 January 2021).
- Vanhommerig, J.W.; Bezemer, D.; Molenkamp, R.; Van Sighem, A.I.; Smit, C.; Arends, J.E.; Lauw, F.N.; Brinkman, K.; Rijnders, B.J.; Newsum, A.M.; et al. Limited overlap between phylogenetic HIV and hepatitis C virus clusters illustrates the dynamic sexual network structure of Dutch HIV-infected MSM. AIDS 2017, 31, 2147–2158. [Google Scholar] [CrossRef] [PubMed]
- Benova, L.; Mohamoud, Y.A.; Calvert, C.; Abu-Raddad, L.J. Vertical transmission of hepatitis C virus: Systematic review and meta-analysis. Clin. Infect. Dis. 2014, 59, 765–773. [Google Scholar] [CrossRef]
- Frederick, T.; Burian, P.; Terrault, N.; Cohen, M.; Augenbraun, M.; Young, M.; Seaberg, E.; Justman, J.; Levine, A.M.; Mack, W.J.; et al. Factors associated with prevalent hepatitis C infection among HIV-infected women with no reported history of injection drug use: The Women’s Interagency HIV Study (WIHS). AIDS Patient Care STDS 2009, 23, 915–923. [Google Scholar] [CrossRef]
- Marquez, L.K.; Martin, N.K.; Strathdee, S.A.; Skaathun, B. Differences in characteristics and interactions with close contacts among PWID in the San Diego Border Region before and during the COVID-19 pandemic. J. Migr. Health 2024, 10, e100267. [Google Scholar] [CrossRef] [PubMed]
- County of San Diego Health and Human Services Agency. Opioid-Related Overdoses & Encounters in COSD, 2016–2020. Updated April 2023. Available online: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/CHS/OD2A%202016-2020%20Retrospective%20Analysis.pdf (accessed on 16 May 2024).
- Walker, J.G.; Kuchuloria, T.; Sergeenko, D.; Fraser, H.; Lim, A.G.; Shadaker, S.; Hagan, L.; Gamkrelidze, A.; Kvaratskhelia, V.; Gvinjilia, L.; et al. Interim effect evaluation of the hepatitis C elimination programme in Georgia: A modelling study. Lancet Glob. Health 2020, 8, e244–e253. [Google Scholar] [CrossRef]
- van der Meer, A.J.; Veldt, B.J.; Feld, J.J.; Wedemeyer, H.; Dufour, J.F.; Lammert, F.; Duarte-Rojo, A.; Heathcote, E.J.; Manns, M.P.; Kuske, L.; et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA 2012, 308, 2584–2593. [Google Scholar] [CrossRef]
- Thomas, D.L. State of the Hepatitis C Virus Care Cascade. Clin. Liver Dis. 2020, 16, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Facente, S.N.; Grebe, E.; Burk, K.; Morris, M.D.; Murphy, E.L.; Mirzazadeh, A.; Smith, A.A.; Sanchez, M.A.; Evans, J.L.; Nishimura, A.; et al. Estimated hepatitis C prevalence and key population sizes in San Francisco: A foundation for elimination. PLoS ONE 2018, 13, e0195575. [Google Scholar] [CrossRef] [PubMed]
- Cachay, E.T.F.; Hill, L.; Ballard, C.; Aquino, A.; Qin, H.; Jain, S.; Martin, S.; Mathews, W.m.C. Progress and real-life challenges for HCV elimination in People living with HIV. In Proceedings of the Conferences on Retrovirus and Opportunistic Infections, Boston, MA, USA, 8–11 March 2020. [Google Scholar]
- Tempalski, B.; Pouget, E.R.; Cleland, C.M.; Brady, J.E.; Cooper, H.L.F.; Hall, H.I.; Lansky, A.; West, B.S.; Friedman, S.R. Trends in the population prevalence of people who inject drugs in US metropolitan areas 1992–2007. PLoS ONE 2013, 8, e64789. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. National Vital Statistics System, Mortality 1999–2020 on CDC WONDER Online Database. Available online: http://wonder.cdc.gov/ucd-icd10.html (accessed on 1 July 2022).
- Cachay, E.R.; Hill, L.; Wyles, D.; Colwell, B.; Ballard, C.; Torriani, F.; Mathews, W.C. The hepatitis C cascade of care among HIV infected patients: A call to address ongoing barriers to care. PLoS ONE 2014, 9, e102883. [Google Scholar] [CrossRef] [PubMed]
- FDAPermits Marketing of First Point-of-Care Hepatitis CRNATest, U.S. Food & Drug Administration. Updated 27 June 2024. 2024. Available online: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-first-point-care-hepatitis-c-rna-test (accessed on 12 July 2024).
- Platt, L.; Minozzi, S.; Reed, J.; Vickerman, P.; Hagan, H.; French, C.; Jordan, A.; Degenhardt, L.; Hope, V.; Hutchinson, S.; et al. Needle and syringe programmes and opioid substitution therapy for preventing HCV transmission among people who inject drugs: Findings from a Cochrane Review and meta-analysis. Addiction 2018, 113, 545–563. [Google Scholar] [CrossRef]
- Fraser, H.; Vellozzi, C.; Hoerger, T.J.; Evans, J.L.; Kral, A.H.; Havens, J.; Young, A.M.; Stone, J.; Handanagic, S.; Hariri, S.; et al. Scaling Up Hepatitis C Prevention and Treatment Interventions for Achieving Elimination in the United States: A Rural and Urban Comparison. Am. J. Epidemiol. 2019, 188, 1539–1551. [Google Scholar] [CrossRef]
- Cheema, J.S.; Flores Ortega, R.; Reau, N.; Bradley, H.; Hall, E.W.; Hoenigl, M.; Strathdee, S.A.; Martin, N.K. Modeling Hepatitis C Virus Elimination in the United States: Are we on track to reach incidence targets? In Proceedings of the 12th International Conference on Health and Hepatitis in Substance Users, Athens, Greece, 8–11 October 2024. [Google Scholar]
- Friedman, J.R.; Abramovitz, D.; Skaathun, B.; Rangel, G.; Harvey-Vera, A.; Vera, C.F.; Artamonova, I.; Muñoz, S.; Martin, N.K.; Eger, W.H.; et al. Illicit Fentanyl Use and Hepatitis C Virus Seroconversion Among People Who Inject Drugs in Tijuana and San Diego: Results From a Binational Cohort Study. Clin. Infect. Dis. 2024, 79, 1109–1116. [Google Scholar] [CrossRef]
- Artenie, A.; Luhmann, N.; Lim, A.G.; Fraser, H.; Ward, Z.; Stone, J.; MacGregor, L.; Walker, J.G.; Trickey, A.; Marquez, L.K.; et al. Methods indicators to validate country reductions in incidence of hepatitis C virus infection to elimination levels set by, WHO. Lancet Gastroenterol. Hepatol. 2022, 7, 353–366. [Google Scholar] [CrossRef]
- Kåberg, M.; Weiland, O. Hepatitis C elimination—Macro-elimination. Liver Int. 2020, 40 (Suppl. S1), 61–66. [Google Scholar] [CrossRef]
- Huang, C.-F.; Chen, G.-J.; Hung, C.-C.; Yu, M.-L. HCV Microelimination for High-risk Special Populations. J. Infect. Dis. 2023, 228, S168–S179. [Google Scholar] [CrossRef]
- Blach, S.; Razavi-Shearer, D.; Mooneyhan, E.; Estes, C.; Razavi-Shearer, K.; Gamkrelidze, I.; Razavi, H. Updated Evaluation of Global Progress Towards HBV and HCV Elimination, Preliminary Data Through 2021; American Association for the Study of Liver Diseases: Alexandria, VA, USA, 2022. [Google Scholar]
- Trickey, A.; Fraser, H.; Lim, A.G.; Peacock, A.; Colledge, S.; Walker, J.G.; Leung, J.; Grebely, J.; Larney, S.; Martin, N.K.; et al. The contribution of injection drug use to hepatitis C virus transmission globally, regionally, and at country level: A modelling study. Lancet Gastroenterol. Hepatol. 2019, 4, 435–444. [Google Scholar] [CrossRef] [PubMed]
- Borroni, G.; Andreoletti, M.; Casiraghi, M.A.; Ceriani, R.; Guerzoni, P.; Omazzi, B.; Terreni, N.; Salerno, F. Effectiveness of pegylated interferon/ribavirin combination in ‘real world’ patients with chronic hepatitis C virus infection. Aliment. Pharmacol. Ther. 2008, 27, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Scotto, R.; Buonomo, A.R.; Moriello, N.S.; Maraolo, A.E.; Zappulo, E.; Pinchera, B.; Gentile, I.; Borgia, G. Real-World Efficacy and Safety of Pangenotypic Direct-Acting Antivirals Against Hepatitis C Virus Infection. Rev. Recent Clin. Trials 2019, 14, 173–182. [Google Scholar] [CrossRef]
- Hézode, C. Treatment of hepatitis C: Results in real life. Liver Int. 2018, 38, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Singh, K.P.; Shubber, Z.; Ducros, P.; Mills, E.J.; Cooke, G.; Ford, N. Treatment Outcomes of Treatment-Naïve Hepatitis C Patients Co-Infected with HIV: A Systematic Review and Meta-Analysis of Observational Cohorts. PLoS ONE 2013, 8, e55373. [Google Scholar] [CrossRef] [PubMed]
- Micallef, J.M.; Kaldor, J.M.; Dore, G.J. Spontaneous viral clearance following acute hepatitis C infection: A systematic review of longitudinal studies. J. Viral Hepat. 2005, 13, 34–41. [Google Scholar] [CrossRef]
- Thomson, E.C.; Fleming, V.M.; Main, J.; Klenerman, P.; Weber, J.; Eliahoo, J.; Smith, J.; McClure, M.O.; Karayiannis, P. Predicting spontaneous clearance of acute hepatitis C virus in a large cohort of HIV-1-infected men. Gut 2010, 60, 837–845. [Google Scholar] [CrossRef]
- Shepherd, J.; Jones, J.; Hartwell, D.; Davidson, P.; Price, A.; Waugh, N. Interferon alfa (pegylated and non-pegylated) and ribavirin for the treatment of mild chronic hepatitis C: A systematic review and economic evaluation. Heal. Technol. Assess. 2007, 11, 1–205. [Google Scholar] [CrossRef]
- Morgan, R.L.; Baack, B.; Smith, B.D.; Yartel, A.; Pitasi, M.; Falck-Ytter, Y. Eradication of Hepatitis C Virus Infection and the Development of Hepatocellular Carcinoma. Ann. Intern. Med. 2013, 158, 329–337. [Google Scholar] [CrossRef]
- Bradley, H.; Hall, E.W.; Asher, A.; Furukawa, N.W.; Jones, C.M.; Shealey, J.; Buchacz, K.; Handanagic, S.; Crepaz, N.; Rosenberg, E.S. Estimated Number of People Who Inject Drugs in the United States. Clin. Infect. Dis. 2022, 76, 96–102. [Google Scholar] [CrossRef]
- Chaillon, A.; Bojorquez, I.; Sepúlveda, J.; Harvey-Vera, A.Y.; Rangel, M.G.; Skaathun, B.; Mehta, S.R.; Ignacio, C.; Porrachia, M.; Smith, D.M.; et al. Cocirculación y reemplazo de variantes de SARS-CoV-2 en espacios hacinados y poblaciones marginadas en la frontera México-EUA. Salud Pública México 2022, 65, 10–18. Available online: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=110208 (accessed on 22 May 2021). [CrossRef] [PubMed]
- Arias, E.; Xu, J.Q. United States Life Tables, 2019; National Vital Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2022; Volume 70, Number 19. [Google Scholar]
- Understanding the Current HIV Epidemic. Available online: https://aidsvu.org/local-data/united-states/west/california/san-diego-county/ (accessed on 21 May 2021).
- HIV Disease Among Adult/Adolescent Males, San Diego County, 2017. Available online: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/Adult_Adol_Male_Through_12312017_final.pdf (accessed on 21 May 2021).
- Robertson, A.M.; Garfein, R.S.; Wagner, K.D.; Mehta, S.R.; Magis-Rodriguez, C.; Cuevas-Mota, J.; Moreno-Zuniga, P.G.; Strathdee, S.A.; Proyecto El Cuete IV and STAHR II. Evaluating the impact of Mexico’s drug policy reforms on people who inject drugs in Tijuana, B.C., Mexico, and San Diego, CA, United States: A binational mixed methods research agenda. Harm Reduct. J. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- HIV Disease Among Females in San Diego County, 2017. Available online: https://www.sandiegocounty.gov/content/dam/sdc/hhsa/programs/phs/documents/Females_Through_12312017v04-11-19.pdf (accessed on 21 May 2021).
- Horyniak, D.; Wagner, K.D.; Armenta, R.F.; Cuevas-Mota, J.; Hendrickson, E.; Garfein, R.S. Cross-border injection drug use and HIV and hepatitis C virus seropositivity among people who inject drugs in San Diego, California. Int. J. Drug Policy 2017, 47, 9–17. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Year | Observed Data Used for Model Calibration [95% C.I.] | Calibrated Model Output [95% C.I.] | Reference | |
|---|---|---|---|---|
| HCV seroprevalence among MSM coinfected with HIV | 2015 | 0.165 [0.155, 0.176] | 0.157 [0.122, 0.172] | [5] |
| HCV seroprevalence among all MSM | 2015 | 0.046 [0.030, 0.061] | 0.071 [0.050, 0.103] | [5] |
| HCV seroprevalence among PWID [age 18–39] | 2021 | 0.46 [0.39, 0.53] | 0.450 [0.407, 0.479] | La Frontera PWID cohort with residence in SD, unpublished [13] |
| HCV seroprevalence among PWID [age 40–74] | 2021 | 0.36 [0.30, 0.43] | 0.395 [0.363, 0.428] | La Frontera PWID cohort with residence in SD, unpublished [13] |
| HCV viremia prevalence among HCV seropositive people coinfected with HIV | 2010 | 0.3091 [0.2705, 0.3506] | 0.3082 [0.2633, 0.3400] | [19] |
| 2018 | 0.1849 [0.1534, 0.2212] | 0.193 [0.159, 0.266] | [19] | |
| 2021 | 0.0857 [0.0636, 0.1146] | 0.095 [0.082, 0.118] | [19] | |
| Number of PWID | 2007 | 24,991 | 30,075 [25,055, 37,948] | [5,20] |
| HCV primary incidence rate among PWID (per 100 person-years) | 2021 | 17.14 [12.52, 21.75] | 9.592 [5.184, 16.561] | La Frontera PWID cohort with residence in SD, unpublished [13] |
| HCV-related deaths | 2015 | 290 | 289 [253, 316] | CDC [21] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheema, J.S.; Suckow, S.; Ramers, C.; Loose, P.; Tomada, A.; Tweeten, S.; Stamos-Buesig, T.; Abramovitz, D.; Eger, W.H.; Strathdee, S.A.; et al. Is San Diego California on Track to Reach HCV Elimination? A Modeling Analysis of Combination Prevention Strategies. Viruses 2024, 16, 1819. https://doi.org/10.3390/v16121819
Cheema JS, Suckow S, Ramers C, Loose P, Tomada A, Tweeten S, Stamos-Buesig T, Abramovitz D, Eger WH, Strathdee SA, et al. Is San Diego California on Track to Reach HCV Elimination? A Modeling Analysis of Combination Prevention Strategies. Viruses. 2024; 16(12):1819. https://doi.org/10.3390/v16121819
Chicago/Turabian StyleCheema, Jaskaran S., Scott Suckow, Christian Ramers, Patrick Loose, Andrea Tomada, Samantha Tweeten, Tara Stamos-Buesig, Daniela Abramovitz, William H. Eger, Steffanie A. Strathdee, and et al. 2024. "Is San Diego California on Track to Reach HCV Elimination? A Modeling Analysis of Combination Prevention Strategies" Viruses 16, no. 12: 1819. https://doi.org/10.3390/v16121819
APA StyleCheema, J. S., Suckow, S., Ramers, C., Loose, P., Tomada, A., Tweeten, S., Stamos-Buesig, T., Abramovitz, D., Eger, W. H., Strathdee, S. A., & Martin, N. K. (2024). Is San Diego California on Track to Reach HCV Elimination? A Modeling Analysis of Combination Prevention Strategies. Viruses, 16(12), 1819. https://doi.org/10.3390/v16121819