
The Association of HHV-6 and the TNF-α (-308G/A) Promotor with Major Depressive Disorder Patients and Healthy Controls in Thailand

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
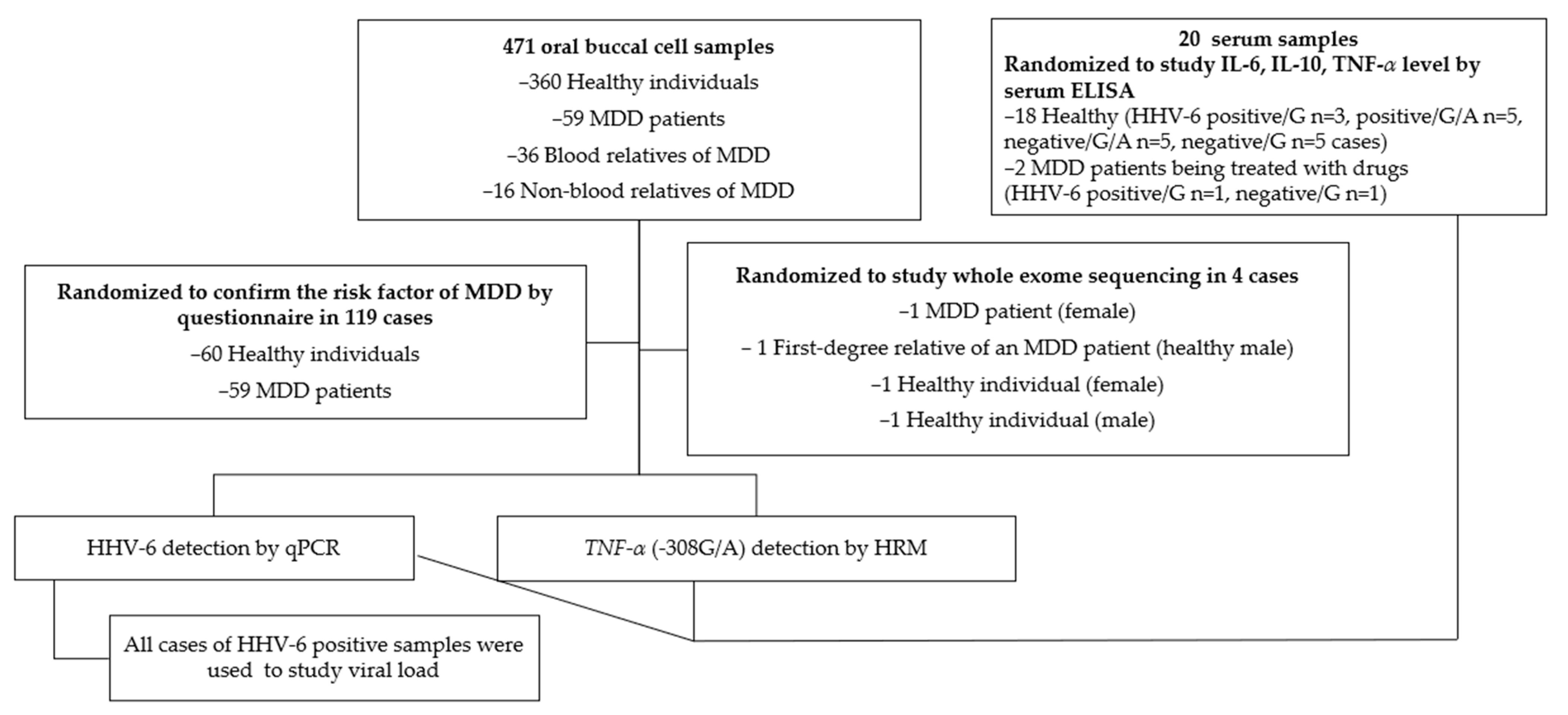
2.1. Specimens
2.2. DNA Extraction
2.3. HHV-6 DNA Detection by Quantitative PCR (qPCR) and Viral Load
2.4. TNF-α Promoter (-308G/A; rs1800629) Detection by High-Resolution Melt (HRM) Analysis
2.5. DNA Sequencing
2.6. Screening Effect of HHV-6 Status and TNF-α Promoter (-308G/A) Mutation by ELISA
2.7. Whole-Exome Sequencing (WES)
2.8. Statistical Analysis
3. Results
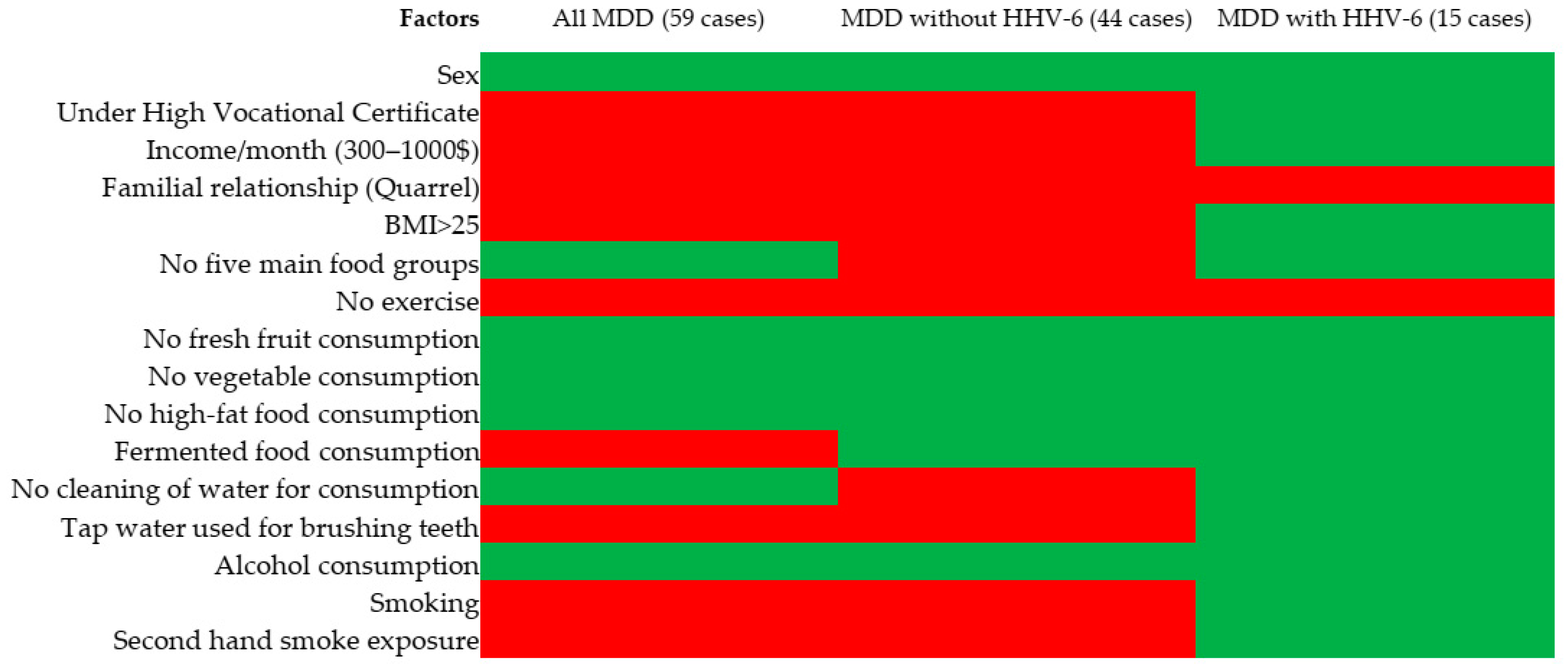
3.1. Risk Factor for MDD
3.2. HHV-6 Detection by qPCR
3.3. TNF-α (-308G/A; rs1800629) Promoter Detection by HRM Analysis
3.4. HHV-6 Viral Load
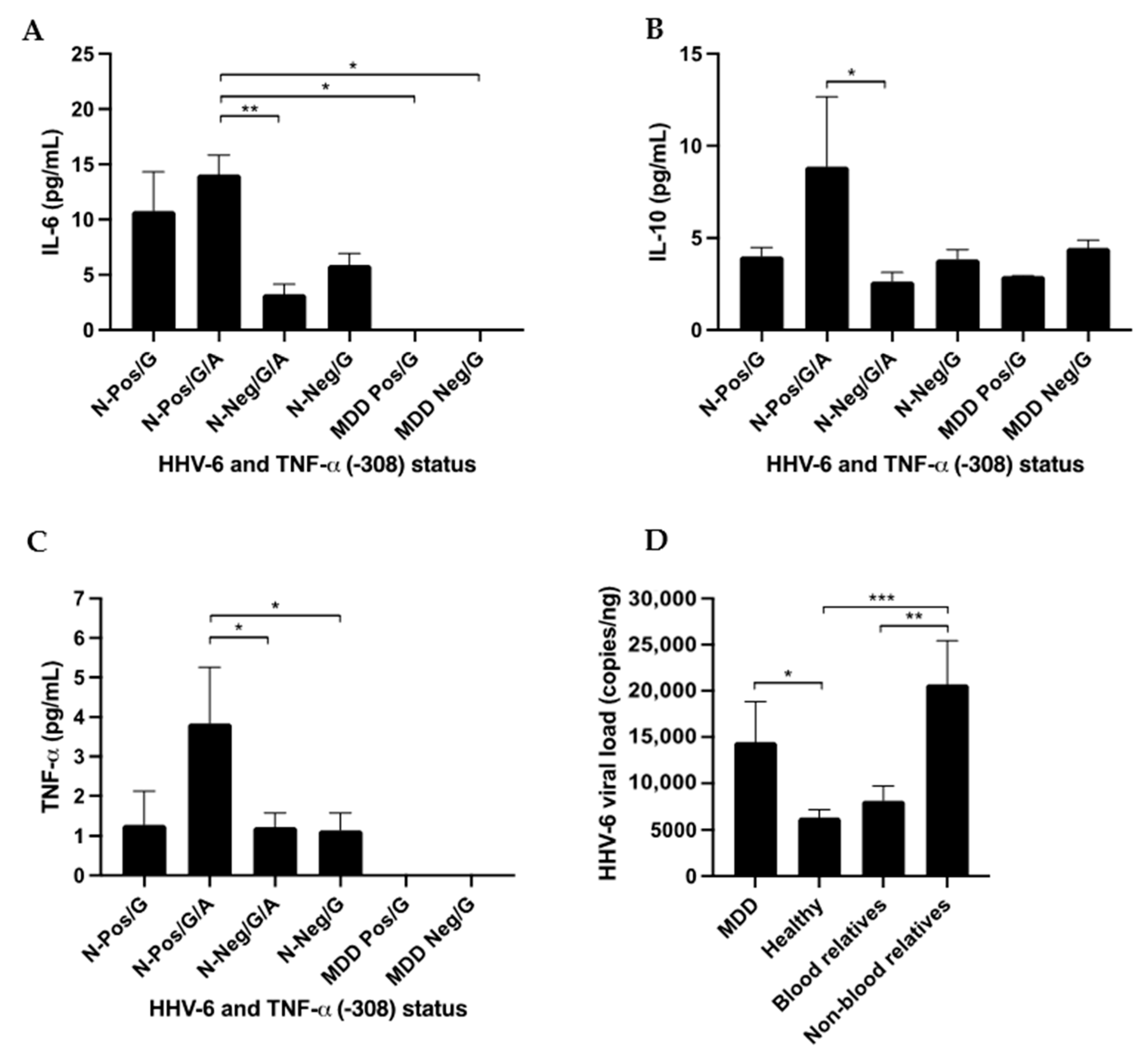
3.5. ELISA
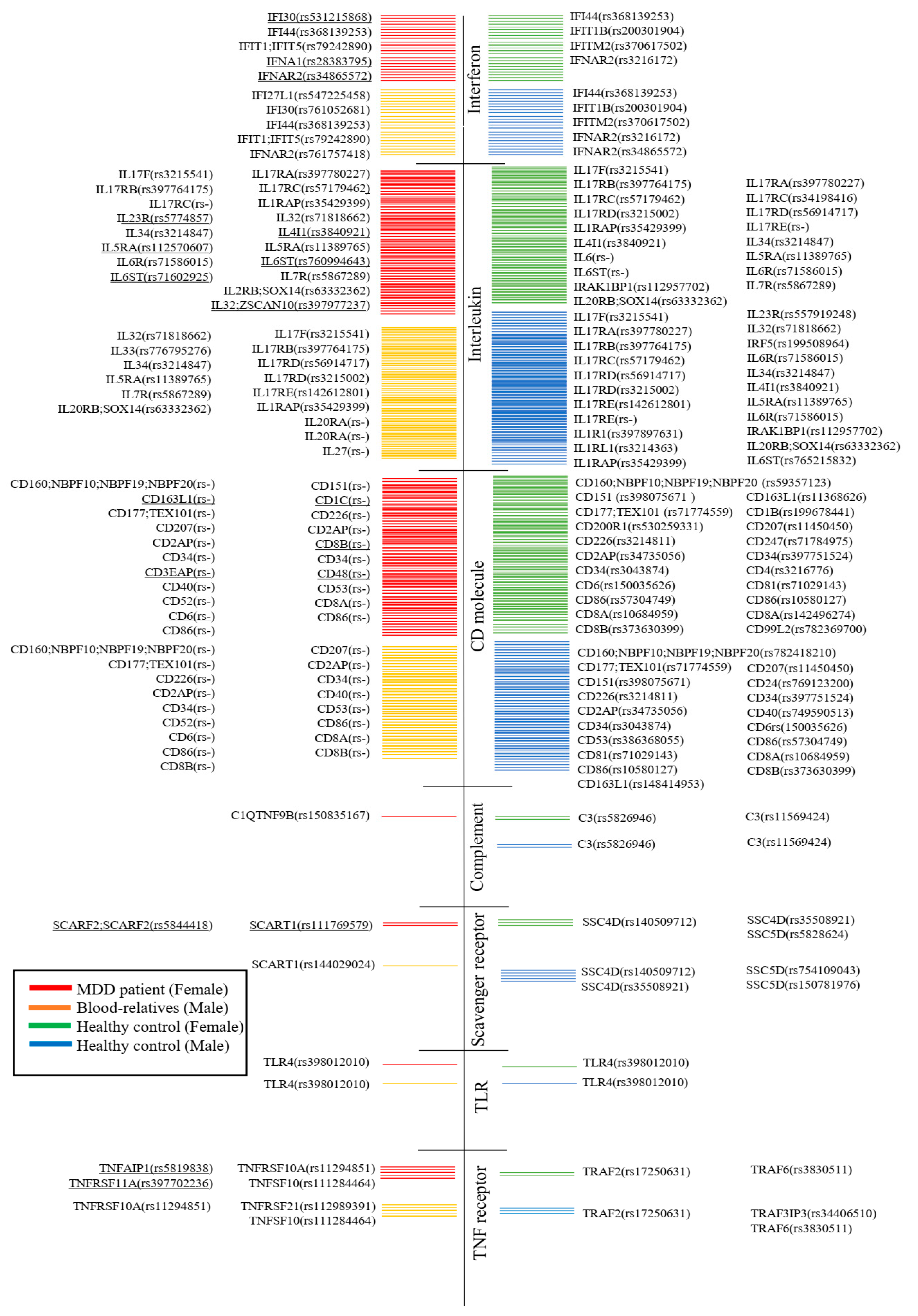
3.6. Whole-Exome Sequencing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health organization. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 20 July 2023).
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 4 March 2023).
- Abdoli, N.; Salari, N.; Darvishi, N.; Jafarpour, S.; Solaymani, M.; Mohammadi, M.; Shohaimi, S. The global prevalence of major depressive disorder (MDD) among the elderly: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2022, 132, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Musumari, P.M.; Tangmunkongvorakul, A.; Srithanaviboonchai, K.; Techasrivichien, T.; Suguimoto, S.P.; Ono-Kihara, M.; Kihara, M. Grit is associated with lower level of depression and anxiety among university students in Chiang Mai, Thailand: A cross-sectional study. PLoS ONE 2018, 13, e0209121. [Google Scholar] [CrossRef] [PubMed]
- Siripongpan, A.; Phattaramarut, K.; Namvichaisirikul, N.; Poochaya, S.; Horkaew, P. Prevalence of depression and stress among the first year students in Suranaree University of Technology, Thailand. Health Psychol. Res. 2022, 10, 35464. [Google Scholar] [CrossRef]
- Phomprasith, S.; Karawekpanyawong, N.; Pinyopornpanish, K.; Jiraporncharoen, W.; Maneeton, B.; Phinyo, P.; Lawanaskol, S. Prevalence and Associated Factors of Depression in Medical Students in a Northern Thailand University: A Cross-Sectional Study. Healthcare 2022, 10, 488. [Google Scholar] [CrossRef] [PubMed]
- Chomchoei, C.; Apidechkul, T.; Keawdounglek, V.; Wongfu, C.; Khunthason, S.; Kullawong, N.; Tamornpark, R.; Upala, P.; Yeemard, F. Prevalence of and factors associated with depression among hill tribe individuals aged 30 years and over in Thailand. Heliyon 2020, 6, e04273. [Google Scholar] [CrossRef] [PubMed]
- Singkhorn, O.; Apidechkul, T.; Pitchalard, K.; Moonpanane, K.; Hamtanon, P.; Sunsern, R.; Leaungsomnapa, Y.; Thepsaw, J. Prevalence of and factors associated with depression in the hill tribe population aged 40 years and older in northern Thailand. Int. J. Ment. Health Syst. 2021, 15, 62. [Google Scholar] [CrossRef]
- Aung, T.N.N.; Moolphate, S.; Koyanagi, Y.; Angkurawaranon, C.; Supakankunti, S.; Yuasa, M.; Aung, M.N. Depression and Associated Factors among Community-Dwelling Thai Older Adults in Northern Thailand: The Relationship between History of Fall and Geriatric Depression. Int. J. Environ. Res. Public Health 2022, 19, 10574. [Google Scholar] [CrossRef]
- Wangtongkum, S.; Sucharitakul, P.; Wongjaroen, S.; Maneechompoo, S. Prevalence of depression among a population aged over 45 years in Chiang Mai, Thailand. J. Med. Assoc. Thail. 2008, 91, 1812. [Google Scholar]
- Charoensakulchai, S.; Usawachoke, S.; Kongbangpor, W.; Thanavirun, P.; Mitsiriswat, A.; Pinijnai, O.; Kaensingh, S.; Chaiyakham, N.; Chamnanmont, C.; Ninnakala, N.; et al. Prevalence and associated factors influencing depression in older adults living in rural Thailand: A cross-sectional study. Geriatr. Gerontol. Int. 2019, 19, 1248–1253. [Google Scholar] [CrossRef]
- Köhler, C.A.; Evangelou, E.; Stubbs, B.; Solmi, M.; Veronese, N.; Belbasis, L.; Bortolato, B.; Melo, M.C.; Coelho, C.A.; Fernandes, B.S.; et al. Mapping risk factors for depression across the lifespan: An umbrella review of evidence from meta-analyses and Mendelian randomization studies. J. Psychiatr. Res. 2018, 103, 189–207. [Google Scholar] [CrossRef]
- Alexopoulos, G.S. Mechanisms and treatment of late-life depression. Transl Psychiatry. 2019, 9, 188. [Google Scholar] [CrossRef] [PubMed]
- Ménard, C.; Hodes, G.; Russo, S. Pathogenesis of depression: Insights from human and rodent studies. Neuroscience 2016, 321, 138–162. [Google Scholar] [CrossRef] [PubMed]
- Weissman, M.M.; Bland, R.C.; Canino, G.J.; Faravelli, C.; Greenwald, S.; Hwu, H.-G.; Joyce, P.R.; Karam, E.G.; Lee, C.-K.; Lellouch, J.; et al. Cross-national epidemiology of major depression and bipolar disorder. JAMA 1996, 276, 293–299. [Google Scholar] [CrossRef]
- Hawton, K.; Comabella, C.C.I.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Jun, T.-Y.; Pae, C.-U.; Chae, J.-H.; Bahk, W.-M.; Kim, K.-S.; Serretti, A. Possible association between—G308A tumour necrosis factor-alpha gene polymorphism and major depressive disorder in the Korean population. Psychiatr. Genet. 2003, 13, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-M.; Stewart, R.; Kim, S.-Y.; Kang, H.-J.; Jang, J.-E.; Kim, S.-W.; Shin, I.-S.; Park, M.-H.; Yoon, J.-H.; Park, S.-W.; et al. A one year longitudinal study of cytokine genes and depression in breast cancer. J. Affect. Disord. 2013, 148, 57–65. [Google Scholar] [CrossRef]
- Oxenkrug, G.F. Genetic and hormonal regulation of tryptophan kynurenine metabolism: Implications for vascular cognitive impairment, major depressive disorder, and aging. Ann. N. Y. Acad. Sci. 2007, 1122, 35–49. [Google Scholar] [CrossRef]
- Schmidt, F.M.; Koch, J.; Nowak, C.; Holdt, L.M.; Teupser, D.; Hegerl, U.; Himmerich, H. Ligands and receptors of the TNF superfamily are decreased in major depression and during early antidepressant therapy. J. Psychiatr. Res. 2019, 119, 116–121. [Google Scholar] [CrossRef]
- Ma, K.; Zhang, H.; Baloch, Z. Pathogenetic and Therapeutic Applications of Tumor Necrosis Factor-α (TNF-α) in Major Depressive Disorder: A Systematic Review. Int. J. Mol. Sci. 2016, 17, 733. [Google Scholar] [CrossRef]
- Chen, H.; Wilkins, L.M.; Aziz, N.; Cannings, C.; Wyllie, D.H.; Bingle, C.; Rogus, J.; Beck, J.D.; Offenbacher, S.; Cork, M.J.; et al. Single nucleotide polymorphisms in the human interleukin-1B gene affect transcription according to haplotype context. Hum. Mol. Genet. 2006, 15, 519–529. [Google Scholar] [CrossRef]
- Fishman, D.; Faulds, G.; Jeffery, R.; Mohamed-Ali, V.; Yudkin, J.S.; Humphries, S.; Woo, P. The effect of novel polymorphisms in the interleukin-6 (IL-6) gene on IL-6 transcription and plasma IL-6 levels, and an association with systemic-onset juvenile chronic arthritis. J. Clin. Investig. 1998, 102, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Flint, J.; Kendler, K.S. The genetics of major depression. Neuron 2014, 81, 484–503. [Google Scholar] [CrossRef] [PubMed]
- Kraft, J.B.; Slager, S.L.; McGrath, P.J.; Hamilton, S.P. Sequence analysis of the serotonin transporter and associations with antidepressant response. Biol. Psychiatry 2005, 58, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Lohoff, F.W. Overview of the genetics of major depressive disorder. Curr. Psychiatry Rep. 2010, 12, 539–546. [Google Scholar] [CrossRef]
- Kendler, K.S.; Gatz, M.; Gardner, C.O.; Pedersen, N.L.; Ohlsson, H.; Lichtenstein, P.; Sundquist, J.; Sundquist, K.; Keverne, J.; Czamara, D.; et al. A Swedish national twin study of lifetime major depression. Am. J. Psychiatry 2006, 163, 109–114. [Google Scholar] [CrossRef]
- Sullivan, P.F.; Neale, M.C.; Kendler, K.S.; Bauer, A.E.; Maegbaek, M.L.; Liu, X.; Wray, N.R.; Miller, W.C.; Meltzer-Brody, S.; Munk-Olsen, T.; et al. Genetic epidemiology of major depression: Review and meta-analysis. Am. J. Psychiatry 2000, 157, 1552–1562. [Google Scholar] [CrossRef]
- Baillargeon, J.; Piper, J.; Leach, C.T. Epidemiology of human herpesvirus 6 (HHV-6) infection in pregnant and nonpregnant women. J. Clin. Virol. 2000, 16, 149–157. [Google Scholar] [CrossRef]
- Pancharoen, C.; Mekmullica, J.; Bhattarakosol, P. Seroprevalence of anti-human herpes virus-6 IgG antibody in children of Bangkok, Thailand. Southeast Asian J. Trop. Med. Public Health 2001, 32, 143–147. [Google Scholar]
- Chua, K.B.; Khairullah, N.S.; Hooi, P.S. Seroepidemiology of human herpesvirus 6 in a population seen in the University Hospital, Kuala Lumpur, Malaysia. Southeast Asian J. Trop. Med. Public Health 1996, 27, 91–95. [Google Scholar]
- Yoshikawa, T.; Asano, Y.; Akimoto, S.; Ozaki, T.; Iwasaki, T.; Kurata, T.; Goshima, F.; Nishiyama, Y. Latent infection of human herpesvirus 6 in astrocytoma cell line and alteration of cytokine synthesis. J. Med. Virol. 2002, 66, 497–505. [Google Scholar] [CrossRef]
- Köhler, C.A.; Freitas, T.H.; Stubbs, B.; Maes, M.; Solmi, M.; Veronese, N.; de Andrade, N.Q.; Morris, G.; Fernandes, B.S.; Brunoni, A.R.; et al. Peripheral Alterations in Cytokine and Chemokine Levels After Antidepressant Drug Treatment for Major Depressive Disorder: Systematic Review and Meta-Analysis. Mol. Neurobiol. 2018, 55, 4195–4206. [Google Scholar] [CrossRef]
- Morris, G.; Berk, M.; Walder, K.; Maes, M. The Putative Role of Viruses, Bacteria, and Chronic Fungal Biotoxin Exposure in the Genesis of Intractable Fatigue Accompanied by Cognitive and Physical Disability. Mol. Neurobiol. 2016, 53, 2550–2571. [Google Scholar] [CrossRef] [PubMed]
- Santpere, G.; Telford, M.; Andrés-Benito, P.; Navarro, A.; Ferrer, I. The Presence of Human Herpesvirus 6 in the Brain in Health and Disease. Biomolecules 2020, 10, 1520. [Google Scholar] [CrossRef] [PubMed]
- Fotheringham, J.; Williams, E.L.; Akhyani, N.; Jacobson, S. Human herpesvirus 6 (HHV-6) induces dysregulation of glutamate uptake and transporter expression in astrocytes. J. Neuroimmune Pharmacol. 2008, 3, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Prusty, B.K.; Gulve, N.; Govind, S.; Krueger, G.R.F.; Feichtinger, J.; Larcombe, L.; Aspinall, R.; Ablashi, D.V.; Toro, C.T. Active HHV-6 Infection of Cerebellar Purkinje Cells in Mood Disorders. Front. Microbiol. 2018, 9, 1955. [Google Scholar] [CrossRef] [PubMed]
- Toro, C.T.; Eliassen, E.; Prusty, B.K. Does infection of cerebellar Purkinje neurons with human herpes virus 6A or 6B (HHV-6) increase the risk of developing mood disorders? Future Microbiol. 2019, 14, 85–88. [Google Scholar] [CrossRef]
- Kobayashi, N.; Oka, N.; Takahashi, M.; Shimada, K.; Ishii, A.; Tatebayashi, Y.; Shigeta, M.; Yanagisawa, H.; Kondo, K. Human Herpesvirus 6B Greatly Increases Risk of Depression by Activating Hypothalamic-Pituitary -Adrenal Axis during Latent Phase of Infection. iScience 2020, 23, 101187. [Google Scholar] [CrossRef]
- Han, K.-M.; Ham, B.-J. How Inflammation Affects the Brain in Depression: A Review of Functional and Structural MRI Studies. J. Clin. Neurol. 2021, 17, 503–515. [Google Scholar] [CrossRef]
- Maes, M. Major depression and activation of the inflammatory response system. Cytokines Stress Depress. 1999, 461, 25–46. [Google Scholar] [CrossRef]
- McGeer, P.L.; McGeer, E.G. The inflammatory response system of brain: Implications for therapy of Alzheimer and other neurodegenerative diseases. Brain Res. Rev. 1995, 21, 195–218. [Google Scholar] [CrossRef]
- Arena, A.; Liberto, M.C.; Iannello, D.; Capozza, A.B.; Focà, A. Altered cytokine production after human herpes virus type 6 infection. New Microbiol. 1999, 22, 293–300. [Google Scholar] [PubMed]
- Bortolotti, D.; Gentili, V.; Rotola, A.; Caselli, E.; Rizzo, R. HHV-6A infection induces amyloid-beta expression and activation of microglial cells. Alzheimers Res. Ther. 2019, 11, 104. [Google Scholar] [CrossRef] [PubMed]
- Kikuta, H.; Nakane, A.; Lu, H.; Taguchi, Y.; Minagawa, T.; Matsumoto, S. Interferon induction by human herpesvirus 6 in human mononuclear cells. J. Infect. Dis. 1990, 162, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Goodrich, J.M.; Yang, X. Interferon-gamma (IFN-γ) regulates production of IL-10 and IL-12 in human herpesvirus-6 (HHV-6)-infected monocyte/macrophage lineage. Clin. Exp. Immunol. 1997, 109, 421–425. [Google Scholar] [CrossRef]
- Mayne, M.; Cheadle, C.; Soldan, S.S.; Cermelli, C.; Yamano, Y.; Akhyani, N.; Nagel, J.E.; Taub, D.D.; Becker, K.G.; Jacobson, S. Gene expression profile of herpesvirus-infected T cells obtained using immunomicroarrays: Induction of proinflammatory mechanisms. J. Virol. 2001, 75, 11641–11650. [Google Scholar] [CrossRef]
- Gosselin, J.; Flamand, L.; D’Addario, M.; Hiscott, J.; Stefanescu, I.; Ablashi, D.V.; Gallo, R.C.; Menezes, J. Modulatory effects of Epstein-Barr, herpes simplex, and human herpes-6 viral infections and coinfections on cytokine synthesis: A comparative study. J. Immunol. 1992, 149, 181–187. [Google Scholar] [CrossRef]
- Arena, A.; Liberto, M.C.; Capozza, A.B.; Focà, A. Productive HHV-6 infection in differentiated U937 cells: Role of TNF alpha in regulation of HHV-6. New Microbiol. 1997, 20, 13–20. [Google Scholar]
- Duh, E.J.; Maury, W.J.; Folks, T.M.; Fauci, A.S.; Rabson, A.B. Tumor necrosis factor alpha activates human immunodeficiency virus type 1 through induction of nuclear factor binding to the NF-kappa B sites in the long terminal repeat. Proc. Natl. Acad. Sci. USA 1989, 86, 5974–5978. [Google Scholar] [CrossRef]
- Bahramian, E.; Furr, M.; Wu, J.T.; Ceballos, R.M. Differential Impacts of HHV-6A versus HHV-6B Infection in Differentiated Human Neural Stem Cells. Front. Immunol. 2022, 13, 847106. [Google Scholar] [CrossRef]
- Kawabe, S.; Ito, Y.; Ohta, R.; Sofue, A.; Gotoh, K.; Morishima, T.; Kimura, H. Comparison of the levels of human herpesvirus 6 (HHV-6) DNA and cytokines in the cerebrospinal fluid and serum of children with HHV-6 encephalopathy. J. Med. Virol. 2010, 82, 1410–1415. [Google Scholar] [CrossRef]
- Tavakoli, N.P.; Nattanmai, S.; Hull, R.; Fusco, H.; Dzigua, L.; Wang, H.; Dupuis, M. Detection and typing of human herpesvirus 6 by molecular methods in specimens from patients diagnosed with encephalitis or meningitis. J. Clin. Microbiol. 2007, 45, 3972–3978. [Google Scholar] [CrossRef] [PubMed]
- De Bolle, L.; Naesens, L.; De Clercq, E. Update on human herpesvirus 6 biology, clinical features, and therapy. Clin. Microbiol. Rev. 2005, 18, 217–245. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.S.; Peiris, K.Y.; Yuen, R.H.; Liang, Y.L.; Lau, F.E.; Chen, S.K.; Lo, C.Y.; Chan, T.K.; Ng, M.H. Human herpesvirus-6 and human herpesvirus-7 infections in bone marrow transplant recipients. J. Med. Virol. 1997, 53, 295–305. [Google Scholar] [CrossRef]
- Ljungman, P.; Wang, F.Z.; Clark, D.A.; Emery, V.C.; Remberger, M.; Ringden, O.; Linde, A. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br. J. Haematol. 2000, 111, 774–781. [Google Scholar]
- Zerr, D.M.; Huang, M.-L.; Corey, L.; Erickson, M.; Parker, H.L.; Frenkel, L.M. Sensitive method for detection of human herpesviruses 6 and 7 in saliva collected in field studies. J. Clin. Microbiol. 2000, 38, 1981–1983. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Kosugi, S.; Koide, R.; Kawamura, Y. Endogenization and excision of human herpesvirus 6 in human genomes. PLoS Genet. 2020, 16, e1008915. [Google Scholar] [CrossRef]
- Tantivanich, S.; Laohapand, P.; Thaweeboon, S.; Desakorn, V.; Wuthinuntiwong, P.; Chalermtaranukul, S.; Pansri, P.; Amarapal, P.; Balachandra, K.; Chantratita, W.; et al. Prevalence of cytomegalovirus, human herpesvirus-6, and Epstein-Barr virus in periodontitis patients and healthy subjects in the Thai population. Southeast Asian J. Trop. Med. Public Health 2004, 35, 635–640. [Google Scholar] [PubMed]
- Thawaranantha, D.; Chimabutra, K.; Balachandra, K.; Warachit, P.; Pantuwatana, S.; Inagi, R.; Kurata, T.; Yamanishi, K. Prevalences of human herpesvirus 6 and human herpesvirus 7 in normal Thai population. Southeast Asian J. Trop. Med. Public Health 1999, 30, 259–264. [Google Scholar]
- Chantaratin, S.; Trimetha, K.; Werarak, P.; Lapphra, K.; Maleesatharn, A.; Rungmaitree, S.; Wittawatmongkol, O.; Phongsamart, W.; Kongstan, N.; Khumcha, B.; et al. Depression and Anxiety in Youth and Young Adults Living with HIV: Frequency and Associated Factors in Thai Setting. J. Int. Assoc. Provid. AIDS Care 2022, 21, 23259582221101811. [Google Scholar] [CrossRef]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef]
- Pongpakdeesakul, S.; Ekalaksananan, T.; Pientong, C.; Iamchuen, N.; Buddhisa, S.; Mahingsa, K.; Pingyod, A.; Sangsrijun, W.; Passorn, S.; Chopjitt, P.; et al. Human Oncogenic Epstein–Barr Virus in Water and Human Blood Infection of Communities in Phayao Province, Thailand. Water 2023, 15, 323. [Google Scholar] [CrossRef]
- Bon, M.A.M.; van Oeveren-Dybicz, A.; van den Bergh, F.A. Genotyping of HLA-B27 by real-time PCR without hybridization probes. Clin. Chem. 2000, 46, 1000–1002. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-S.; Lee, K.-S.; Park, J.-H.; Kim, M.-Y.; Shin, W.-S. Detection of human herpesvirus 6 variant A in peripheral blood mononuclear cells from multiple sclerosis patients. Eur. Neurol. 2000, 43, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Most Depressed Countries 2023—Wisevoter. Available online: https://wisevoter.com/country-rankings/most-depressed-countries/?fbclid=IwAR37FvIlUOM-XdUM4IT4hClUn3DtJzklYK4jEcE8ntzAhNBHMFMbowdWQH8 (accessed on 21 July 2023).
- Pengpid, S.; Peltzer, K.; Anantanasuwong, D. Prevalence and determinants of incident and persistent depressive symptoms among middle-aged and older adults in Thailand: Prospective cohort study. BJPsych Open 2023, 9, e99. [Google Scholar] [CrossRef] [PubMed]
- Kamdee, K.; Panadsako, N.; Mueangson, O.; Nuinoon, M.; Janwan, P.; Poonsawat, W.; Pongpanitanont, P.; Kitkumthorn, N.; Thongsroy, J.; Chunglok, W. Promoter polymorphism of TNF-α (rs1800629) is associated with ischemic stroke susceptibility in a southern Thai population. Biomed. Rep. 2021, 15, 78. [Google Scholar] [CrossRef] [PubMed]
- Karawekpanyawong, N.; Kaewkitikul, K.; Maneeton, B.; Maneeton, N.; Siriaree, S. The prevalence of depressive disorder and its association in Thai cervical cancer patients. PLoS ONE 2021, 16, e0252779. [Google Scholar] [CrossRef] [PubMed]
- Chinchai, T.; Homchan, K.; Sopipong, W.; Chansaenroj, J.; Swangvaree, S.; Junyangdikul, P.; Vongpunsawad, S.; Poovorawan, Y. Lack of Associations between TNF-αPolymorphisms and Cervical Cancer in Thai women. Asian Pac. J. Cancer Prev. 2016, 17, 953–956. [Google Scholar] [CrossRef]
- Wongpakaran, N.; Wongpakaran, T. Prevalence of major depressive disorders and suicide in long-term care facilities: A report from northern Thailand. Psychogeriatrics 2012, 12, 11–17. [Google Scholar] [CrossRef]
- Miura, H.; Kawamura, Y.; Ohye, T.; Hattori, F.; Kozawa, K.; Ihira, M.; Yatsuya, H.; Nishizawa, H.; Kurahashi, H.; Yoshikawa, T. Inherited Chromosomally Integrated Human Herpesvirus 6 Is a Risk Factor for Spontaneous Abortion. J. Infect. Dis. 2021, 223, 1717–1723. [Google Scholar] [CrossRef]
- Aoki, T.; Hirota, T.; Tamari, M.; Ichikawa, K.; Takeda, K.; Arinami, T.; Shibasaki, M.; Noguchi, E. An association between asthma and TNF-308G/A polymorphism: Meta-analysis. J. Hum. Genet. 2006, 51, 677–685. [Google Scholar] [CrossRef]
- Abe, Y.; Fujise, N.; Fukunaga, R.; Nakagawa, Y.; Ikeda, M. Comparisons of the prevalence of and risk factors for elderly depression between urban and rural populations in Japan. Int. Psychogeriatr. 2012, 24, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Miura, H.; Kawamura, Y.; Hattori, F.; Kozawa, K.; Ihira, M.; Ohye, T.; Kurahashi, H.; Yoshikawa, T. Chromosomally integrated human herpesvirus 6 in the Japanese population. J. Med. Virol. 2018, 90, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Kamizono, S.; Yamada, K.; Seki, N.; Higuchi, T.; Kimura, A.; Nonaka, K.; Itoh, K. Susceptible locus for obese type 2 diabetes mellitus in the 5′-flanking region of the tumor necrosis factor-α gene. Tissue Antigens 2000, 55, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Suto, M.; Isogai, E.; Mizutani, F.; Kakee, N.; Misago, C.; Takehara, K. Prevalence and Factors Associated with Postpartum Depression in Fathers: A Regional, Longitudinal Study in Japan. Res. Nurs. Health 2016, 39, 253–262. [Google Scholar] [CrossRef]
- Kawamura, Y.; Hashimoto, T.; Miura, H.; Kozawa, K.; Yoshikawa, A.; Ikeda, N.; Yatsuya, H.; Yasuoka, H.; Yoshikawa, T. Inherited chromosomally integrated human herpesvirus 6 and autoimmune connective tissue diseases. J. Clin. Virol. 2020, 132, 104656. [Google Scholar] [CrossRef]
- Tokushige, K.; Takakura, M.; Tsuchiya-Matsushita, N.; Taniai, M.; Hashimoto, E.; Shiratori, K. Influence of TNF gene polymorphisms in Japanese patients with NASH and simple steatosis. J. Hepatol. 2007, 46, 1104–1110. [Google Scholar] [CrossRef]
- The WHO World Mental Health Survey Consortium. Prevalence, severity, and unmet need for treatment of mental disorders in the World Health Organization World Mental Health Surveys. JAMA 2004, 291, 2581–2590. [Google Scholar] [CrossRef]
- Kessler, R.C.; Bromet, E.J. The epidemiology of depression across cultures. Annu. Rev. Public Health 2013, 34, 119–138. [Google Scholar] [CrossRef]
- Lezhnyova, V.; Davidyuk, Y.; Mullakhmetova, A.; Markelova, M.; Zakharov, A.; Khaiboullina, S.; Martynova, E. Analysis of herpesvirus infection and genome single nucleotide polymorphism risk factors in multiple sclerosis, Volga federal district, Russia. Front. Immunol. 2022, 13, 1010605. [Google Scholar] [CrossRef]
- Churnosov, M.I.; Belousova, O.N.; Sirotina, S.S. Study of the associations between polymorphic markers rs1800629 TNFα, rs909253 Ltα, rs767455 TNFR1, rs1061624 TNFR2 and the development of type 2 diabetes. Diabetes Mellitus 2017, 20, 166–171. [Google Scholar] [CrossRef]
- Pakriev, S.; Kovalev, J.; Mozhaev, M. Prevalence of depression in a general hospital in Izhevsk, Russia. Nord. J. Psychiatry 2009, 63, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Al-Sadeq, D.W.; Zedan, H.T.; Aldewik, N.; Elkhider, A.; Hicazi, A.; Younes, N.; Ayoub, H.H.; Abu Raddad, L.; Yassine, H.M.; Nasrallah, G.K. Human herpes simplex virus-6 (HHV-6) detection and seroprevalence among Qatari nationals and immigrants residing in Qatar. IJID Reg. 2022, 2, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Algamdi, A.A.; Abdi, S.; Almutairi, R.M.; Sarwar, S.; Aldaghri, N.; Haq, S.H.; Alamro, A.; Muayqil, T.A. Clusterin, TNF-α, and IL-6 polymorphism and implications on Alzheimer’s disease risk determination in Saudi population. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Al-Ali, F.; Elshirbeny, M.; Hamad, A.; Kaddourah, A.; Ghonimi, T.; Ibrahim, R.; Fouda, T. Prevalence of Depression and Sleep Disorders in Patients on Dialysis: A Cross-Sectional Study in Qatar. Int. J. Nephrol. 2021, 2021, 5533416. [Google Scholar] [CrossRef] [PubMed]
- Tran, X.D.; Hoang, V.T.; Dang, T.T.D.; Vu, T.P.; To, M.M.; Tran, T.K.; Do, M.D.; Nguyen, D.C.; Nguyen, Q.T.; Colson, P.; et al. Aetiology of Acute Undifferentiated Fever Among Children Under the Age of Five in Vietnam: A Prospective Study. J. Epidemiol. Glob. Health 2023, 13, 163–172. [Google Scholar] [CrossRef]
- Dunstan, S.J.; Stephens, H.A.; Blackwell, J.M.; Duc, C.M.; Lanh, M.N.; Dudbridge, F.; Phuong, C.X.T.; Luxemburger, C.; Wain, J.; Ho, V.A.; et al. Genes of the class II and class III major histocompatibility complex are associated with typhoid fever in Vietnam. J. Infect. Dis. 2001, 183, 261–268. [Google Scholar] [CrossRef]
- Pham, T.; Bui, L.; Nguyen, A.; Nguyen, B.; Tran, P.; Vu, P.; Dang, L. The prevalence of depression and associated risk factors among medical students: An untold story in Vietnam. PLoS ONE 2019, 14, e0221432. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhao, Y.; Wang, Y.; Rao, J. A multiplex real-time PCR quantitation of human herpesvirus-6, 7, 8 viruses: Application in blood transfusions. Virol. J. 2021, 18, 38. [Google Scholar] [CrossRef]
- Wang, D.; He, L.; Zhang, X. -308G/A polymorphism of tumor necrosis factor alpha (TNF-α) gene and metabolic syndrome susceptibility: A meta-analysis. Sci. Rep. 2021, 11, 3840. [Google Scholar] [CrossRef]
- Nisar, A.; Yin, J.; Waqas, A.; Bai, X.; Wang, D.; Rahman, A.; Li, X. Prevalence of perinatal depression and its determinants in Mainland China: A systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 1022–1037. [Google Scholar] [CrossRef]
- Lou, J.; Wu, Y.; Cai, M.; Wu, X.; Shang, S. Subtype-specific, probe-based, real-time PCR for detection and typing of human herpesvirus-6 encephalitis from pediatric patients under the age of 2 years. Diagn. Microbiol. Infect. Dis. 2011, 70, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Ko, G.T.C.; Lee, S.C.; Pu, Y.B.; Ng, M.C.Y.; So, W.; Thomas, N.; Chan, W.B.; Cockram, C.S.; Chan, J.C.N. Tumour necrosis factor-alpha promoter gene polymorphism at—308 (genotype AA) in Chinese subjects with Type 2 diabetes. Diabet. Med. 2003, 20, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.C.; Zhang, M.Y.; Huang, Y.Q.; He, Y.L.; Liu, Z.R.; Cheng, H.; Tsang, A.; Lee, S.; Kessler, R.C. Twelve-month prevalence, severity, and unmet need for treatment of mental disorders in metropolitan China. Psychol Med. 2006, 36, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Chuh, A.A.; Chan, H.H.; Chiu, S.S.; Ng, H.Y.; Peiris, J.S. A prospective case control study of the association of Gianotti-Crosti syndrome with human herpesvirus 6 and human herpesvirus 7 infections. Pediatr. Dermatol. 2002, 19, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Heneghan, M.A.; Johnson, P.J.; Clare, M.; Ho, S.; Harrison, P.M.; Donaldson, P.T. Frequency and nature of cytokine gene polymorphisms in hepatocellular carcinoma in Hong Kong Chinese. Int. J. Gastrointest. Cancer 2004, 34, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Maeno, T.; Kizawa, Y.; Ueno, Y.; Nakata, Y.; Sato, T. Depression among primary care patients with complaints of headache and general fatigue. Prim. Care Psychiatry 2002, 8, 69–72. [Google Scholar] [CrossRef]
- Oktafiani, D.; Megasari, N.L.A.; Ana, E.F.; Nasronudin; Lusida, M.I.; Soetjipto. First Report on HHV-6 Infection Among HIV-Infected Individuals Residing in Surabaya, Indonesia. HIV/AIDS-Res. Palliat. Care 2020, 12, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Rubiati, W.N.; Gani, A.Z.; Sulijaya, B.; Suhartono, W.A.; Auerkari, E.I. Relation of Susceptibility to Periodontitis and Tumor Necrosis Factor Alpha G-308A Polymorphism in Indonesian Males. J. Int. Dent. Med. Research 2020, 13, 1515–1518. [Google Scholar]
- Handajani, Y.S.; Schröder-Butterfill, E.; Hogervorst, E.; Turana, Y.; Hengky, A. Depression among Older Adults in Indonesia: Prevalence, Role of Chronic Conditions and Other Associated Factors. Clin. Pract. Epidemiol. Ment. Health 2022, 18, e174501792207010. [Google Scholar] [CrossRef]
- Mahdinejad-Yazdi, M.; Sobhan, M.R.; Dastgheib, S.A.; Bahrami, R.; Shaker, S.H.; Mirjalili, H.; Sadeghizadeh-Yazdi, J.; Zare-Shehneh, M.; Neamatzadeh, H. A meta-analysis for association of TNF-α -308G>A polymorphism with susceptibility to Ankylosing Spondylitis. J. Orthop. 2021, 26, 79–87. [Google Scholar] [CrossRef]
- Kim, H.; Lee, H.; Lee, S. The prevalence and correlates of depression in Korean adults with rheumatoid arthritis: Results from the Korea National Health and Nutrition Examination Surveys. Int. J. Rheum. Dis. 2022, 25, 454–465. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Shim, J. Predictors of Depression among Individuals Receiving the Basic Livelihood Security Program Benefits in Korea: A Study Based on the Sixth and Seventh Korea National Health and Nutrition Examination Survey (2013–2018). Int. J. Environ. Res. Public Health 2022, 20, 194. [Google Scholar] [CrossRef]
- Bartolini, L.; Piras, E.; Sullivan, K.; Gillen, S.; Bumbut, A.; Lin, C.-T.M.; Leibovitch, E.C.; Graves, J.S.; Waubant, E.L.; Chamberlain, J.M.; et al. Detection of HHV-6 and EBV and Cytokine Levels in Saliva from Children with Seizures: Results of a Multi-Center Cross-Sectional Study. Front. Neurol. 2018, 9, 834. [Google Scholar] [CrossRef] [PubMed]
- Dayal, A.D.; Sodimalla, K.V.; Chelerkar, V.; Deshpande, M. Prevalence of Anxiety and Depression in Patients with Primary Glaucoma in Western India. Eur. J. Gastroenterol. Hepatol. 2021, 31, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Shanquan, C.; Yuqi, W.; Rui, S. Prevalence and gender disparity of those who screen positive for depression in China by the classification of the employer and industry: A cross-sectional, population-based study. BMC Psychiatry 2023, 23, 62. [Google Scholar]
- Chen, Y.C.; Chiang, H.H.; Cho, Y.T.; Chang, C.Y.; Chen, K.L.; Yang, C.W.; Lee, Y.H.; Chu, C.-Y. Human herpes virus reactivations and dynamic cytokine profiles in patients with cutaneous adverse drug reactions—A prospective comparative study. Allergy 2015, 70, 568–575. [Google Scholar] [CrossRef]
- Hwu, H.-G.; Yeh, E.-K.; Chang, L.-Y. Prevalence of psychiatric disorders in Taiwan defined by the Chinese Diagnostic Interview Schedule. Acta Psychiatr. Scand. 1989, 79, 136–147. [Google Scholar] [CrossRef]
- Yadav, M.; Arivananthan, M.; Chandrashekran, A.; Tan, B.S.; Hashim, B.Y. Human herpesvirus-6 (HHV-6) DNA and virus-encoded antigen in oral lesions. J. Oral Pathol. Med. 1997, 26, 393–401. [Google Scholar] [CrossRef]
- Mojtaba, G. Association between TNF-a-308 G/A Polymorphism and Oral Cancer Risk among Malaysian Indian and Indigenous. Masters’s Thesis, University of Malaya, Kuala Lumpur, Malaysia, 2011. [Google Scholar]
- Gan, G.G.; Ling, H.Y. Anxiety, Depression and quality of life of medical students in Malaysia. Med. J. Malays. 2019, 74, 57–61. [Google Scholar]
- Huang, X.; Yu, T.; Li, X.; Cao, Y.; Li, X.; Liu, B.; Yang, F.; Li, W.; Zhao, X.; Feng, G.; et al. ABCB6, ABCB1 and ABCG1 genetic polymorphisms and antidepressant response of SSRIs in Chinese depressive patients. Pharmacogenomics 2013, 14, 1723–1730. [Google Scholar] [CrossRef]
- Gałecki, P.; Talarowska, M.; Szemraj, J.; Zajączkowska, M. ASMT gene expression correlates with cognitive impairment in patients with recurrent depressive disorder. Med. Sci. Monit. 2014, 20, 905–912. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Andrade, A.; Brennecke, A.; Mallat, S.; Brown, J.; Gomez-Rivadeneira, J.; Czepiel, N.; Londrigan, L. Genetic Associations between Voltage-Gated Calcium Channels and Psychiatric Disorders. Int. J. Mol. Sci. 2019, 20, 3537. [Google Scholar] [CrossRef]
- Fu, Y.; Zhou, N.; Bai, W.; Sun, Y.; Chen, X.; Wang, Y.; Zhang, M.; Kou, C.; Yu, Y.; Yu, Q. Association of the CACNA2D2 gene with schizophrenia in Chinese Han population. PeerJ 2020, 8, e8521. [Google Scholar] [CrossRef] [PubMed]
- Timón-Gómez, A.; Nývltová, E.; Abriata, L.A.; Vila, A.J.; Hosler, J.; Barrientos, A. Mitochondrial cytochrome c oxidase biogenesis: Recent developments. Semin. Cell Dev. Biol. 2018, 76, 163–178. [Google Scholar] [CrossRef] [PubMed]
- Selimi, F.; Lohof, A.M.; Heitz, S.; Lalouette, A.; Jarvis, C.I.; Bailly, Y.; Mariani, J. Lurcher GRID2-induced death and depolarization can be dissociated in cerebellar Purkinje cells. Neuron 2003, 37, 813–819. [Google Scholar] [CrossRef]
- Guan, T.; Li, T.; Cai, W.; Huang, D.; Ouyang, P.; Wang, Y.; Chen, H.; Wu, K.; Ma, X. HTR3A and HTR3E gene polymorphisms and diarrhea predominant irritable bowel syndrome risk: Evidence from a meta-analysis. Oncotarget 2017, 8, 100459–100468. [Google Scholar] [CrossRef]
- Doddato, G.; Fabbiani, A.; Scandurra, V.; Canitano, R.; Mencarelli, M.A.; Renieri, A.; Ariani, F. Identification of a Novel SHANK2 Pathogenic Variant in a Patient with a Neurodevelopmental Disorder. Genes 2022, 13, 688. [Google Scholar] [CrossRef]
- Gao, J.; Pan, Z.; Jiao, Z.; Li, F.; Zhao, G.; Wei, Q.; Pan, F.; Evangelou, E. TPH2 gene polymorphisms and major depression--a meta-analysis. PLoS ONE 2012, 7, e36721. [Google Scholar] [CrossRef]
- Bozzola, E.; Krzysztofiak, A.; Bozzola, M.; Calcaterra, V.; Quondamcarlo, A.; Lancella, L.; Villani, A. HHV6 meningoencephalitis sequelae in previously healthy children. Infection 2012, 40, 563–566. [Google Scholar] [CrossRef]
- Osaki, T.; Morikawa, T.; Kajita, H.; Kobayashi, N.; Kondo, K.; Maeda, K. Caregiver burden and fatigue in caregivers of people with dementia: Measuring human herpesvirus (HHV)-6 and -7 DNA levels in saliva. Arch. Gerontol. Geriatr. 2016, 66, 42–48. [Google Scholar] [CrossRef]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Aizenstein, H.; Reynolds, C.F., III; Butters, M.A.; Erickson, K.I. Exercise effects on depression: Possible neural mechanisms. Gen. Hosp. Psychiatry 2017, 49, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, N.A.L.; Del Ángel, D.S.; Brizuela, N.O.; Peraza, A.V.; Olguín, H.J.; Soto, M.P.; Guzmán, D.C. Inflammatory Process and Immune System in Major Depressive Disorder. Int. J. Neuropsychopharmacol. 2021, 25, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-K.; Won, E. The influence of stress on neuroinflammation and alterations in brain structure and function in major depressive disorder. Behav. Brain Res. 2017, 329, 6–11. [Google Scholar] [CrossRef]
- Farooq, R.K.; Asghar, K.; Kanwal, S.; Zulqernain, A. Role of inflammatory cytokines in depression: Focus on interleukin-1β. Biomed. Rep. 2016, 6, 15–20. [Google Scholar] [CrossRef]
- Cassano, P.; Bui, E.; Rogers, A.H.; Walton, Z.E.; Ross, R.; Zeng, M.; Nadal-Vicens, M.; Mischoulon, D.; Baker, A.W.; Keshaviah, A.; et al. Inflammatory cytokines in major depressive disorder: A case–control study. Aust. N. Z. J. Psychiatry 2016, 51, 23–31. [Google Scholar] [CrossRef]
- Lovelace, M.D.; Varney, B.; Sundaram, G.; Lennon, M.J.; Lim, C.K.; Jacobs, K.; Guillemin, G.J.; Brew, B.J. Recent evidence for an expanded role of the kynurenine pathway of tryptophan metabolism in neurological diseases. Neuropharmacology 2017, 112, 373–388. [Google Scholar] [CrossRef]
- Ning, L.; Yang, Z.; Chen, J.; Hu, Z.; Jiang, W.; Guo, L.; Xu, Y.; Li, H.; Xu, F.; Deng, D. A novel 4 immune-related genes as diagnostic markers and correlated with immune infiltrates in major depressive disorder. BMC Immunol. 2022, 23, 6. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Group | N | MDD | Healthy | p-Value | Odds Ratio |
|---|---|---|---|---|---|---|
| Sex | Male | 18 | 6 (33%) | 12 (67%) | 0.135 | 0.453 (0.158–1.300) |
| Female | 101 | 53 (52%) | 48 (48%) | |||
| Age | 119 | 31 ± 6.4 | 22 ± 1.7 | 0.000 | NA | |
| Education level | No–High Vocational Certificate | 23 | 16 (70%) | 7 (30%) | 0.033 | 2.817 (1.063–7.469) |
| >High Vocational Certificate | 96 | 43 (45%) | 53 (55%) | |||
| Income/month ($) | 300–1000 | 67 | 41 (61%) | 26 (39%) | 0.004 | 2.979 (1.402–6.328) |
| No–299 | 34 | 18 (53%) | 16 (47%) | |||
| Familial relationship | Quarrel | 15 | 15 (100%) | 0 (0%) | <0.001 | NA |
| No Quarrel | 104 | 44 (42%) | 60 (58%) | |||
| BMI | >25 | 41 | 26 (63%) | 15 (37%) | 0.029 | 2.364 (1.085–5.147) |
| <25 | 78 | 33 (42%) | 45 (58%) | |||
| Five main food groups | No | 58 | 33 (57%) | 25 (43%) | 0.120 | 1.777 (0.859–3.674) |
| Yes | 61 | 26 (43%) | 35 (57%) | |||
| Exercise | No | 59 | 37 (63%) | 22 (37%) | 0.004 | 2.905 (1.380–6.115) |
| 1–7 times/week | 60 | 22 (37%) | 38 (63%) | |||
| Fresh fruit consumption (per week) | No–1 to 2 times | 67 | 34 (51%) | 33 (49%) | 0.773 | 1.113 (0.539–2.297) |
| 3–7 times | 52 | 25 (48%) | 27 (52%) | |||
| Vegetable consumption (per week) | No–1 to 2 times | 40 | 20 (50%) | 20 (50%) | 0.948 | 1.026 (0.479–2.195) |
| 3–7 times | 79 | 39 (49%) | 40 (51%) | |||
| High-fat food consumption (per week) | No–1 to 2 times | 68 | 30 (44%) | 38 (56%) | 0.169 | 0.599 (0.288–1.246) |
| 3–7 times | 51 | 29 (57%) | 22 (43%) | |||
| Fermented food consumption (per week) | 3–7 times | 59 | 10 (17%) | 49 (83%) | 0.014 | 5.918 (1.237–28.308) |
| No–1 to 2 times | 60 | 2 (3%) | 58 (97%) | |||
| Cleaning of water for consumption | No | 36 | 13 (36%) | 23 (64%) | 0.053 | 0.455 (0.203–1.018) |
| Yes | 83 | 46 (55%) | 37 (45%) | |||
| Tap water used for brushing teeth | Yes | 101 | 56 (55%) | 45 (45%) | 0.002 | 6.222 (1.695–22.836) |
| No | 18 | 3 (17%) | 15 (83%) | |||
| Alcohol consumption | Yes | 85 | 41 (48%) | 44 (52%) | 0.643 | 0.828 (0.373–1.837) |
| No | 34 | 18 (53%) | 16 (47%) | |||
| Secondhand smoke exposure | Yes | 46 | 33 (72%) | 13 (28%) | <0.001 | 4.589 (2.060–10.221) |
| No | 73 | 26 (36%) | 47 (64%) |
| Group | HHV-6 Positive | HHV-6 Negative | Total |
|---|---|---|---|
| MDD patients | 15 (25.42%) | 44 (74.58%) | 59 |
| Healthy subjects | 51 (14.17%) | 309 (85.83%) | 360 |
| Blood relatives of patients | 17 (47.22%) | 19 (52.78%) | 36 |
| Non-blood relatives of patients | 7 (43.75%) | 9 (56.25%) | 16 |
| Total | 90 (19.11%) | 381 (80.89%) | 471 |
| Group | TNF-α (-308G/A) | TNF-α (-308G) | Total |
|---|---|---|---|
| MDD patients | 3 (7.69%) | 36 (92.31%) | 39 |
| Healthy participants | 15 (6.82%) | 205 (93.18%) | 220 |
| Blood relatives of patients | 6 (30.00%) | 14 (70.00%) | 20 |
| Non-blood relatives of patients | 2 (14.29%) | 12 (85.71%) | 14 |
| Total | 26 (8.87%) | 267 (91.13%) | 293 |
| Country | Sample | Prevalence of HHV-6 | Prevalence of TNF-α (-308G/A) | Prevalence of Depression | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Method | Disease | Normal | Ref. | Disease | Normal | Ref. | Review Papers | Global Report [66] | ||
| Thailand | Saliva | Nested-PCR | - | 5.7–8.6% | [60] | G/G = 166 (83.0%) G/A = 31 (15.5%) A/A = 3 (1.5%) | G/G = 181 (92.1%) G/A = 19 (7.9%) A/A = 0 (0.0%) | [67,68] | 13.5% [69] | 3.7% |
| PBMC | Nested-PCR | - | 45.5–78.3% | [60] | G/G = 108 (89.3%) G/A = 11 (9.1%) A/A = 2 (1.7%) | G/G = 113 (86.9%) G/A = 15 (11.5%) A/A = 2 (1.5%) | [70] | 23.5 % [71] | ||
| Japan | PBMC | qPCR | 10–27% | - | [72] | G/G = 441 (96%) G/A = 19 (4%) A/A = 1 (0%) | G/G = 454 (98%) G/A = 10 (2%) A/A = 1 (0) | [73] | 28.2% [74] | 2.7% |
| Blood & serum | qPCR& FISH | 1/12 (8.3%) | 46/85 (54.1%) | [75] | G/G = 57 (96.6%) G/A = 2 (3.4%) A/A = 0 (0.0%) | G/G = 556 (97%) G/A = 18 (3.1%) A/A = 1 (0.2%) | [76] | 17% [77] | ||
| Blood | qPCR | 0.6% | 0.2% | [78] | G/G = 97% G/A = 4% A/A = 1% | G/G = 95% G/A = 5% A/A = 0% | [79] | 3.1–6.6% [80,81] | ||
| Russia | Blood | qPCR | 1/124 (0.81%) | 1/70 (1.7%) | [82] | G/G = 176 (74.6%) G/A = 53 (22.5%) A/A = 7 (3.0%) | G/G = 242 (79.9%) G/A = 55 (18.2%) A/A = 6 (2.0%) | [83] | 20.7% [84] | 3.9% |
| Qatar | Serum | ELISA | - | 71.7% | [85] | G/G = 26 (70.3%) G/A = 10 (27.0%) A/A = 1 (2.7%) | G/G = 12 (52.2%) G/A = 11 (47.8%) A/A = 0 | [86] | 48% [87] | 4.9% |
| Vietnam | Blood | qPCR | 12.6% | - | [88] | G = 182 (87%) A = 28 (13%) G/G = 79 (75%) G/A = 24 (23%) A/A = 2 (2%) | G = 378 (93%) A = 30 (7%) G/G = 174 (85%) G/A = 30 (15%) A/A = 0 | [89] | 15.2% [90] | 2.8% |
| China | Blood | qPCR | 40% | 16.2% | [91] | G = 1083 (90%) A = 117 (10%) G/G = 488 (81%) G/A = 107 (18%) A/A = 5 (1%) | G = 1142 (95%) A = 58 (5%) G/G = 543 (91%) G/A = 56 (9%) A/A = 1 (0%) | [92] | 16.3–18.7% [93] | - |
| CSF | qPCR | 23/405 (5.7%) | - | [94] | G/G = 284 (83.8%) G/A = 50 (14.7%) A/A = 5 (1.5%) | G/G = 171 (84.7%) G/A = 31 (15.3%) A/A = 0 (0.0%) | [95] | 2.0–2.5% [80,96] | - | |
| Hong Kong | Blood | qPCR | 4/10 (40%) | 2/10 (20%) | [97] | G/G = 88 (90%) G/A = 10 (10%) A/A = 0 (0%) | G/G = 90 (93%) G/A = 6 (6%) A/A = 0 (0.0%) | [98] | 3.7% [99] | - |
| Indonesia | PBMC | qPCR | 15/85 (17.6%) | 3/85 (3.5%) | [100] | G/G = 78% G/A = 22% A/A = 0% | G/G = 92% G/A = 8% A/A = 0% | [101] | 16.3%[102] | 2.6% |
| Korea | PBMC | PCR | 7/34 (20.6%) | 0/20 (0%) | [65] | G/G = 110 (92%) G/A = 9 (8%) A/A = 0 (0%) | G/G = 115 (85%) G/A = 20 (15%) A/A = 0 (0%) | [103] | 10.1–14.3% [104,105] | - |
| India | Saliva | PCR | 40% | 35% | [106] | G = 429 (80%) A = 109 (20%) G/G = 169 (63%) G/A = 91 (34%) A/A = 9 (3%) | G = 502 (92%) A = 42 (8%) G/G = 230 (85%) G/A = 42 (15%) A/A = 0 (0%) | [92] | 6–9% [81,107,108] | 3.7% |
| Taiwan | PBMC | qPCR | 43.5% | - | [109] | G/G = 121 (85%) G/A = 22 (15%) A/A = 0 (0%) | G/G = 31 (53%) G/A = 25 (42%) A/A = 3 (5%) | [103] | 1.3–2.4% [110] | 3.6% |
| Malaysia | Oral cell | PCR | 19/24 (79%) | 0/7 (0%) | [111] | G/G = 85 (86.7%) G/A = 11 (11.2%) A/A = 2 (2%) | G/G = 49 (86%) G/A = 7 (12.3%) A/A = 1 (1.8%) | [112] | 11% [113] | 3.9% |
| Gene | Disease | MDD Mutation | Rs | Healthy Mutation | Rs | ||
|---|---|---|---|---|---|---|---|
| Patient | Relative | Female | Male | ||||
| ATP Binding Cassette Transporter G1 (ABCG1) [114] | Major depressive disorder (MDD) | / | - | rs- | - | - | - |
| Acetylserotonin O-Methyltransferase (ASMTL) [115] | Recurrent depressive disorder | / | / | rs13329185 | - | - | - |
| Calcium Voltage-Gated Channel Subunit Alpha1 F (CACNA1F) [116] | Psychiatric disorders | / | - | rs371501501 | - | - | - |
| Calcium Voltage-Gated Channel Subunit Alpha1 I (CACNA1I) [116] | Psychiatric disorders | / | - | rs- | - | / | rs- |
| Calcium Voltage-Gated Channel Auxiliary Subunit Alpha 2 Delta 2 (CACNA2D2) [117] | Schizophrenia | - | / | rs- | - | - | - |
| Cytochrome C Oxidase Subunit 7A1 (COX7A1) [118] | Neurodegeneration | / | rs112834485 | / | - | rs755756126 | |
| Cytochrome C Oxidase Subunit 7A2 (COX7A2) [118] | Neurodegeneration | / | / | rs554727448 | - | - | - |
| Glutamate Ionotropic Receptor Delta Type Subunit 2 (GRID2) [119] | Depolarization of neurons | / | - | rs- | - | - | - |
| 5-Hydroxytryptamine Receptor 3E (HTR3E) [120] | Schizophrenia | / | / | rs150341032 | - | / | rs187832026 |
| SH3 And Multiple Ankyrin Repeat Domains 2 (SHANK2) [121] | Neurodevelopmental disorder | / | / | rs35132270 | - | - | - |
| Tryptophan Hydroxylase-2 (TPH2) [122] | MDD | / | - | rs397897324 | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumala, S.; Ekalaksananan, T.; Pientong, C.; Buddhisa, S.; Passorn, S.; Duangjit, S.; Janyakhantikul, S.; Suktus, A.; Bumrungthai, S. The Association of HHV-6 and the TNF-α (-308G/A) Promotor with Major Depressive Disorder Patients and Healthy Controls in Thailand. Viruses 2023, 15, 1898. https://doi.org/10.3390/v15091898
Sumala S, Ekalaksananan T, Pientong C, Buddhisa S, Passorn S, Duangjit S, Janyakhantikul S, Suktus A, Bumrungthai S. The Association of HHV-6 and the TNF-α (-308G/A) Promotor with Major Depressive Disorder Patients and Healthy Controls in Thailand. Viruses. 2023; 15(9):1898. https://doi.org/10.3390/v15091898
Chicago/Turabian StyleSumala, Sasiwimon, Tipaya Ekalaksananan, Chamsai Pientong, Surachat Buddhisa, Supaporn Passorn, Sureewan Duangjit, Somwang Janyakhantikul, Areeya Suktus, and Sureewan Bumrungthai. 2023. "The Association of HHV-6 and the TNF-α (-308G/A) Promotor with Major Depressive Disorder Patients and Healthy Controls in Thailand" Viruses 15, no. 9: 1898. https://doi.org/10.3390/v15091898
APA StyleSumala, S., Ekalaksananan, T., Pientong, C., Buddhisa, S., Passorn, S., Duangjit, S., Janyakhantikul, S., Suktus, A., & Bumrungthai, S. (2023). The Association of HHV-6 and the TNF-α (-308G/A) Promotor with Major Depressive Disorder Patients and Healthy Controls in Thailand. Viruses, 15(9), 1898. https://doi.org/10.3390/v15091898