
Expert Consensus: Main Risk Factors for Poor Prognosis in COVID-19 and the Implications for Targeted Measures against SARS-CoV-2

 , ,
, ,  , , , , , , ,
, , , , , , ,  , ,
, ,
Abstract
1. Introduction
2. Therapeutic Virus-Targeted Measures against SARS-CoV-2
3. Main Objective
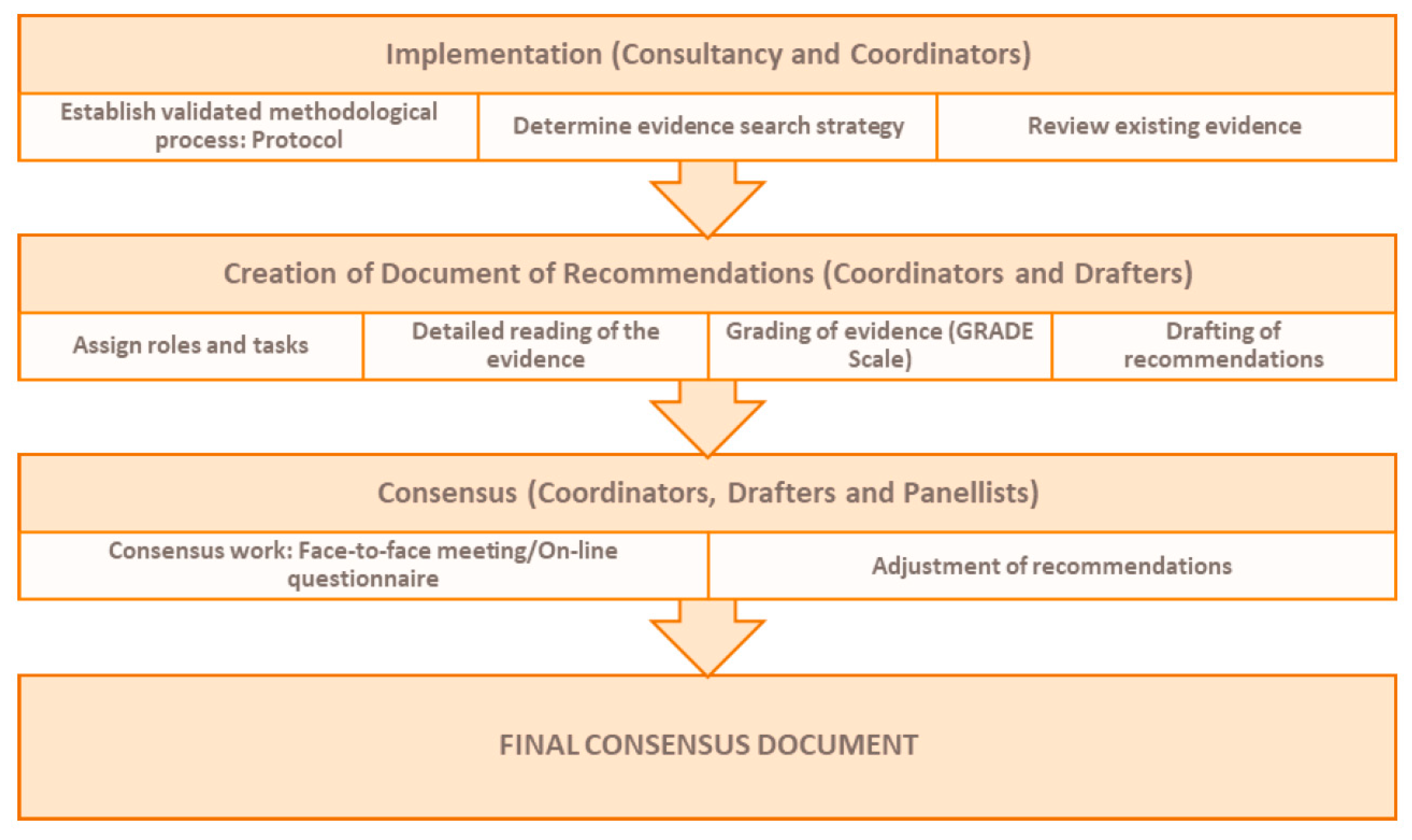
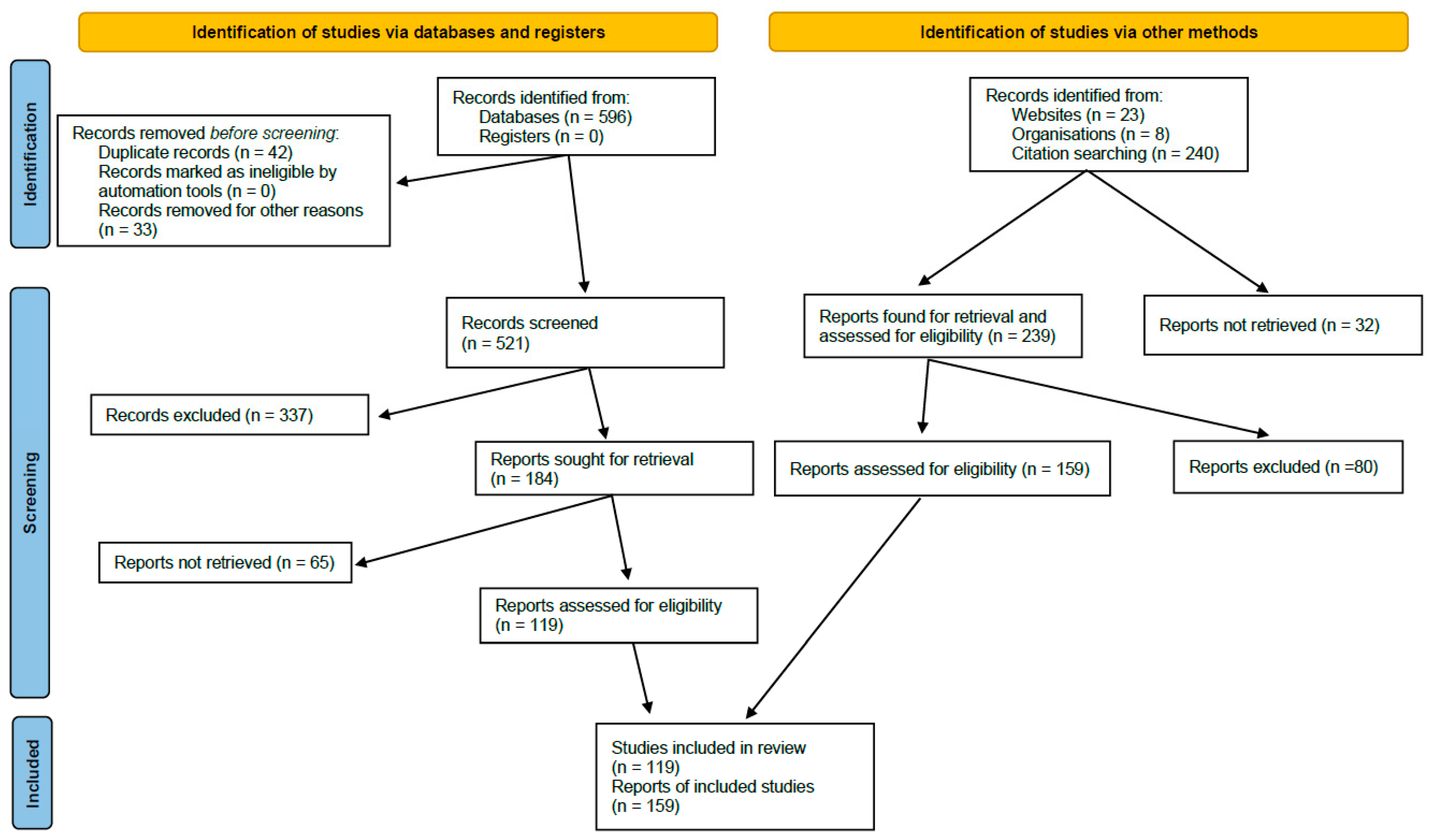
4. Methods
5. Results
- Elderly, frail and institutionalized patients
- Body weight
- Kidney function
- Liver function
- Solid organ transplantation
- SARS-CoV-2 PCR-positive graft donors or recipients
- Hematopoietic stem cell transplantation
- Oncologic patients
- HIV infection
- Primary and other secondary immunodeficiencies
- Immune-mediated inflammatory diseases
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. 2022. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 September 2020).
- COVID-19 Situation Update for the EU/EEA, as of 31 August 2022. European Centre for Disease Prevention and Control. 2022. Available online: https://www.ecdc.europa.eu/en/cases-2019-ncov-eueea (accessed on 5 September 2020).
- Centro de Coodinación de Alertas y Emergencias Sanitarias, Ministerio de Sanidad de España. Actualización No 589. Enfermedad por el Coronavirus (COVID-19). 2022. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/Actualizacion_589_COVID-19.pdf (accessed on 15 October 2022).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA J. Am. Med. Assoc. 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef] [PubMed]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Arribas, J.R.; Garcia-Vidal, C.; Paño, J.R.; Baño, J.R. Recomendaciones SEIMC Para El Manejo Clínico de Pacientes Con COVID-19. 2020, Volume 2. Available online: https://seimc.org/contenidos/documentoscientificos/recomendaciones/seimc-rc-2020-COVID19-manejoclinico.pdf (accessed on 15 October 2022).
- Yek, C.; Warner, S.; Wiltz, J.L.; Sun, J.; Adjei, S.; Mancera, A.; Silk, B.J.; Gundlapalli, A.V.; Harris, A.M.; Boehmer, T.K.; et al. Risk Factors for Severe COVID-19 Outcomes Among Persons Aged ≥ 18 Years Who Completed a Primary COVID-19 Vaccination Series—465 Health Care Facilities, United States, December 2020–October 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 19–25. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef]
- Bonanad, C.; García-Blas, S.; Tarazona-Santabalbina, F.; Sanchis, J.; Bertomeu-González, V.; Fácila, L.; Ariza, A.; Núñez, J.; Cordero, A. The Effect of Age on Mortality in Patients with COVID-19: A Meta-Analysis with 611,583 Subjects. J. Am. Med. Dir. Assoc. 2020, 21, 915–918. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Nandy, K.; Salunke, A.; Pathak, S.K.; Pandey, A.; Doctor, C.; Puj, K.; Sharma, M.; Jain, A.; Warikoo, V. Coronavirus disease (COVID-19): A systematic review and meta-analysis to evaluate the impact of various comorbidities on serious events. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1017–1025. [Google Scholar] [CrossRef]
- Westblade, L.F.; Brar, G.; Pinheiro, L.C.; Paidoussis, D.; Rajan, M.; Martin, P.; Goyal, P.; Sepulveda, J.L.; Zhang, L.; George, G.; et al. SARS-CoV-2 Viral Load Predicts Mortality in Patients with and without Cancer Who Are Hospitalized with COVID-19. Cancer Cell 2020, 38, 661–671.e2. [Google Scholar] [CrossRef]
- Sharma, A.; Bhatt, N.S.; Martin, A.S.; Abid, M.B.; Bloomquist, J.; Chemaly, R.F.; Dandoy, C.; Gauthier, J.; Gowda, L.; Perales, M.-A.; et al. Clinical characteristics and outcomes of COVID-19 in haematopoietic stem-cell transplantation recipients: An observational cohort study. Lancet Haematol. 2021, 8, e185–e193. [Google Scholar] [CrossRef] [PubMed]
- Daoussis, D.; Leonidou, L.; Kalogeropoulou, C.; Paliogianni, F.; Tzouvelekis, A. Protracted severe COVID-19 pneumonia following rituximab treatment: Caution needed. Rheumatol. Int. 2021, 41, 1839–1843. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Sawalha, A.H.; Lu, Q. COVID-19 and autoimmune diseases. Curr. Opin. Rheumatol. 2020, 33, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Gil, B.M.; Fernández-Ruiz, M.M.; Hernández, D.M.; Crespo, M.M.; Colmenero, J.M.; Coll, E.M.; Rubio, J.J. Organ Donation and Transplantation During the COVID-19 Pandemic: A Summary of the Spanish Experience. Transplantation 2021, 105, 29–36. [Google Scholar] [CrossRef]
- Garg, S.; Kim, L.; Whitaker, M.; O’halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.J.; Kirley, P.D.; Alden, N.B.; et al. Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019—COVID-NET, 14 States, March 1–30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2022, 69, 458–464. [Google Scholar] [CrossRef] [PubMed]
- Bialek, S.; Boundy, E.; Bowen, V.; Chow, N.; Cohn, A.; Dowling, N.; Ellington, S.; Gierke, R.; Hall, A.; MacNeil, J.; et al. Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)—United States, February 12–March 16, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 343–346. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Liguoro, I.; Pilotto, C.; Bonanni, M.; Ferrari, M.E.; Pusiol, A.; Nocerino, A.; Vidal, E.; Cogo, P. SARS-CoV-2 infection in children and newborns: A systematic review. Eur. J. Pediatr. 2020, 179, 1029–1046. [Google Scholar] [CrossRef]
- Bhopal, S.S.; Bagaria, J.; Olabi, B.; Bhopal, R. Children and young people remain at low risk of COVID-19 mortality. Lancet Child Adolesc. Health 2021, 5, e12–e13. [Google Scholar] [CrossRef]
- Hamer, M.; Gale, C.R.; Kivimäki, M.; Batty, G.D. Overweight, obesity, and risk of hospitalization for COVID-19: A community-based cohort study of adults in the United Kingdom. Proc. Natl. Acad. Sci. USA 2020, 117, 21011–21013. [Google Scholar] [CrossRef]
- Fadini, G.P.; Morieri, M.L.; Boscari, F.; Fioretto, P.; Maran, A.; Busetto, L.; Bonora, B.M.; Selmin, E.; Arcidiacono, G.; Pinelli, S.; et al. Newly-diagnosed diabetes and admission hyperglycemia predict COVID-19 severity by aggravating respiratory deterioration. Diabetes Res. Clin. Pract. 2020, 168, 108374. [Google Scholar] [CrossRef]
- Sardu, C.; D’onofrio, N.; Balestrieri, M.L.; Barbieri, M.; Rizzo, M.R.; Messina, V.; Maggi, P.; Coppola, N.; Paolisso, G.; Marfella, R. Outcomes in Patients with Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control? Diabetes Care 2020, 43, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Aveyard, P.; Gao, M.; Lindson, N.; Hartmann-Boyce, J.; Watkinson, P.; Young, D.; Coupland, C.A.C.; Tan, P.S.; Clift, A.K.; Harrison, D.; et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: A population cohort study. Lancet Respir. Med. 2021, 9, 909–923. [Google Scholar] [CrossRef]
- Beltramo, G.; Cottenet, J.; Mariet, A.-S.; Georges, M.; Piroth, L.; Tubert-Bitter, P.; Bonniaud, P.; Quantin, C. Chronic respiratory diseases are predictors of severe outcome in COVID-19 hospitalised patients: A nationwide study. Eur. Respir. J. 2021, 58, 2004474. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of cardiovascular disease and 10 other pre-existing comorbidities with COVID-19 mortality: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0238215. [Google Scholar] [CrossRef]
- Herman, C.; Mayer, K.; Sarwal, A. Scoping review of prevalence of neurologic comorbidities in patients hospitalized for COVID-19. Neurology 2020, 95, 77–84. [Google Scholar] [CrossRef]
- Candel, F.J.; Barreiro, P.; Román, J.S.; Carretero, M.D.M.; Sanz, J.C.; Pérez-Abeledo, M.; Ramos, B.; Viñuela-Prieto, J.M.; Canora, J.; Martínez-Peromingo, F.J.; et al. The demography and characteristics of SARS-CoV-2 seropositive residents and staff of nursing homes for older adults in the Community of Madrid: The SeroSOS study. Age Ageing 2021, 50, 1038–1047. [Google Scholar] [CrossRef]
- Belsky, J.A.; Tullius, B.P.; Lamb, M.G.; Sayegh, R.; Stanek, J.R.; Auletta, J.J. COVID-19 in immunocompromised patients: A systematic review of cancer, hematopoietic cell and solid organ transplant patients. J. Infect. 2021, 82, 329–338. [Google Scholar] [CrossRef]
- Dandachi, D.; Geiger, G.; Montgomery, M.W.; Karmen-Tuohy, S.; Golzy, M.; Antar, A.A.; Llibre, J.M.; Camazine, M.; Santiago, D.-D.; Carlucci, P.M.; et al. Characteristics, Comorbidities, and Outcomes in a Multicenter Registry of Patients with Human Immunodeficiency Virus and Coronavirus Disease 2019. Clin. Infect. Dis. 2021, 73, e1964–e1972. [Google Scholar] [CrossRef] [PubMed]
- Zarifkar, P.; Kamath, A.; Robinson, C.; Morgulchik, N.; Shah, S.; Cheng, T.; Dominic, C.; Fehintola, A.; Bhalla, G.; Ahillan, T.; et al. Clinical Characteristics and Outcomes in Patients with COVID-19 and Cancer: A Systematic Review and Meta-analysis. Clin. Oncol. (R Coll Radiol) 2021, 33, e180–e191. [Google Scholar] [CrossRef] [PubMed]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C.A.C.; Mehta, N.; Keogh, R.H.; Diaz-Ordaz, K.; Khunti, K.; Lyons, R.A.; Kee, F.; Sheikh, A.; Rahman, S.; et al. Risk prediction of COVID-19 related death and hospital admission in adults after COVID-19 vaccination: National prospective cohort study. BMJ 2021, 374, n2244. [Google Scholar] [CrossRef] [PubMed]
- Centres for Disease Control and Prevention (CDC). Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 6 September 2022).
- Kompaniyets, L.; Pennington, A.F.; Goodman, A.B.; Rosenblum, H.G.; Belay, B.; Ko, J.Y.; Chevinsky, J.R.; Schieber, L.Z.; Summers, A.D.; Lavery, A.M.; et al. Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized with COVID-19, March 2020–March 2021. Prev. Chronic Dis. 2021, 18, E66. [Google Scholar] [CrossRef] [PubMed]
- González Del Castillo, J.; Salmerón, P.P.; Jiménez, S.; Losa, J.E.; Berenguer, J.; Moreno, S.; Vázquez-Lima, M.; Burillo-Putze, G.; Grupo de Infecciones de la Sociedad Española de Medicina de Urgencias y Emergencias (INFURG-SEMES). Manejo de la Infección por SARS-CoV-2 en Urgencias. Rev. Española Urgenc. Emerg. 2022, 1, 23–27. Available online: www.cdc.gov/mmwr/volumes/71/wr/mm7101a4.htm (accessed on 6 September 2022).
- Bierle, D.M.; Ganesh, R.; Tulledge-Scheitel, S.; Hanson, S.N.; Arndt, L.L.; Wilker, C.G.; Razonable, R.R. Monoclonal Antibody Treatment of Breakthrough COVID-19 in Fully Vaccinated Individuals with High-Risk Comorbidities. J. Infect. Dis. 2022, 225, 598–602. [Google Scholar] [CrossRef]
- SEIMC Score Mortality—SEIMC—COVID-19. 2021. Available online: https://covid19.seimc.org/index.php/seimc-score-mortalidad/ (accessed on 6 September 2022).
- QCovidTM Risk Calculator. 2021. Available online: https://qcovid.org/ (accessed on 6 September 2022).
- Shinyapps. PrediCOVID-ED. Available online: https://predicovid.shinyapps.io/RISK_MODEL_COVID/ (accessed on 6 September 2022).
- Cevik, M.; Kuppalli, K.; Kindrachuk, J.; Peiris, M. Virology, transmission, and pathogenesis of SARS-CoV-2. BMJ 2020, 371, m3862. [Google Scholar] [CrossRef]
- Gupta, A.; González-Rojas, Y.; Juárez, E.; Casal, M.C.; Sarkis, E.; Solis, J.; Falci, D.R.; Moya, H.Z.J.; Scott, N.; Cathcart, A.L.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Case, J.B.; Mackin, S.; Errico, J.; Chong, Z.; Madden, E.A.; Guarino, B.; Schmid, M.A.; Rosenthal, K.; Ren, K.; Jung, A.; et al. Resilience of S309 and AZD7442 monoclonal antibody treatments against infection by SARS-CoV-2 Omicron lineage strains. Nat. Commun. 2022, 13, 3824. [Google Scholar] [CrossRef]
- Wu, M.Y.; Carr, E.J.; Harvey, R.; Mears, H.V.; Kjaer, S.; Townsley, H.; Hobbs, A.; Ragno, M.; Herman, L.S.; Adams, L.; et al. WHO’s Therapeutics and COVID-19 Living Guideline on mAbs needs to be reassessed. Lancet 2022, 400, 2193–2196. [Google Scholar] [CrossRef] [PubMed]
- Zheng, B.; Green, A.C.; Tazare, J.; Curtis, H.; Fisher, L.; Nab, L.; Schultze, A.; Mahalingasivam, V.; Parker, E.P.; Hulme, W.; et al. Comparative effectiveness of sotrovimab and molnupiravir for prevention of severe COVID-19 outcomes in non-hospitalised patients: An observational cohort study using the OpenSAFELY platform. BMJ 2022, 379, e071932. [Google Scholar] [CrossRef] [PubMed]
- Martin-Blondel, G.; Marcelin, A.-G.; Soulié, C.; Kaisaridi, S.; Lusivika-Nzinga, C.; Dorival, C.; Nailler, L.; Boston, A.; Melenotte, C.; Cabié, A.; et al. Sotrovimab to prevent severe COVID-19 in high-risk patients infected with Omicron BA.2. J. Infect. 2022, 85, e104–e108. [Google Scholar] [CrossRef] [PubMed]
- UK Health Security Agency. SARS-CoV-2 Therapeutics Technical Briefing 3. Genomic Surveillance; 2022. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1074186/therapeutics-programme-technical-briefing-3.pdf (accessed on 18 October 2022).
- Bruel, T.; Stéfic, K.; Nguyen, Y.; Toniutti, D.; Staropoli, I.; Porrot, F.; Guivel-Benhassine, F.; Bolland, W.-H.; Planas, D.; Hadjadj, J.; et al. Longitudinal analysis of serum neutralization of SARS-CoV-2 Omicron BA.2, BA.4 and BA.5 in patients receiving monoclonal antibodies. Cell. Rep. Med. 2022, 3, 100850. [Google Scholar] [CrossRef]
- Barnes, C.O.; Jette, C.A.; Abernathy, M.E.; Dam, K.-M.A.; Esswein, S.R.; Gristick, H.B.; Malyutin, A.G.; Sharaf, N.G.; Huey-Tubman, K.E.; Lee, Y.E.; et al. SARS-CoV-2 neutralizing antibody structures inform therapeutic strategies. Nature 2020, 588, 682–687. [Google Scholar] [CrossRef]
- Stanford University. Stanford Coronavirus Antiviral & Resistance Database (CoVDB). 2022. Available online: https://covdb.stanford.edu/ (accessed on 6 September 2022).
- Nguyen, Y.; Flahault, A.; Chavarot, N.; Melenotte, C.; Cheminant, M.; Deschamps, P.; Carlier, N.; Lafont, E.; Thomas, M.; Flamarion, E.; et al. Pre-exposure prophylaxis with tixagevimab and cilgavimab (Evusheld) for COVID-19 among 1112 severely immunocompromised patients. Clin. Microbiol. Infect. 2022, 28, 1654.e1–1654.e4. [Google Scholar] [CrossRef]
- Montgomery, H.; Hobbs, F.D.R.; Padilla, F.; Arbetter, D.; Templeton, A.; Seegobin, S.; Kim, K.; Campos, J.A.S.; Arends, R.H.; Brodek, B.H.; et al. Efficacy and safety of intramuscular administration of tixagevimab-cilgavimab for early outpatient treatment of COVID-19 (TACKLE): A phase 3, randomised, double-blind, placebo-controlled trial. Lancet Respir. Med. 2022, 10, 985–996. [Google Scholar] [CrossRef]
- Bartsch, Y.C.; Tong, X.; Kang, J.; Avendaño, M.J.; Serrano, E.F.; García-Salum, T.; Pardo-Roa, C.; Riquelme, A.; Cai, Y.; Renzi, I.; et al. Omicron variant Spike-specific antibody binding and Fc activity are preserved in recipients of mRNA or inactivated COVID-19 vaccines. Sci. Transl. Med. 2022, 14, eabn9243. [Google Scholar] [CrossRef]
- Maher, M.C.; Soriaga, L.B.; Gupta, A.; Chen, Y.-P.; di Iulio, J.; Ledoux, S.; Smithey, M.J.; Cathcart, A.L.; McKusick, K.; Sun, D.; et al. Antibody therapy reverses biological signatures of COVID-19 progression. Cell. Rep. Med. 2022, 3, 100721. [Google Scholar] [CrossRef]
- Lamers, M.M.; Haagmans, B.L. SARS-CoV-2 pathogenesis. Nat. Rev. Microbiol. 2022, 20, 270–284. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Hongchao, P.; Peto, R.; Ana-Maria, H.-R.; Marie-Pierre, P.; Vasee, S.; Quarraisha, A.K.; Marissa, M.A.; César, H.G.; Marie-Paule, K.; Reza, M.; et al. Repurposed Antiviral Drugs for COVID-19—Interim WHO Solidarity Trial Results. N. Engl. J. Med. 2021, 384, 497. [Google Scholar]
- Siemieniuk, R.A.; Bartoszko, J.J.; Zeraatkar, D.; Kum, E.; Qasim, A.; Martinez, J.P.D.; Izcovich, A.; Lamontagne, F.; Han, M.A.; Agarwal, A.; et al. Drug treatments for COVID-19: Living systematic review and network meta-analysis. BMJ 2020, 370, m2980.49. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Malani, P.N.; del Rio, C. COVID-19 Therapeutics for Nonhospitalized Patients. JAMA 2022, 327, 617. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, D.D.; Du, G.; Du, R.; Zhao, J.; Jin, Y.; Fu, S.; Gao, L.; Cheng, Z.; Lu, Q.; et al. Remdesivir in adults with severe COVID-19: A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2020, 395, 1569–1578. [Google Scholar] [CrossRef]
- Rochwerg, B.; Agarwal, A.; Zeng, L.; Leo, Y.-S.; Appiah, J.A.; Agoritsas, T.; Bartoszko, J.; Brignardello-Petersen, R.; Ergan, B.; Ge, L.; et al. Remdesivir for severe COVID-19: A clinical practice guideline. BMJ 2020, 370, m2924. [Google Scholar] [CrossRef]
- Grundeis, F.; Ansems, K.; Dahms, K.; Thieme, V.; Metzendorf, M.I.; Skoetz, N.; Benstoem, C.; Mikolajewska, A.; Griesel, M.; Fichtner, F.; et al. Remdesivir for the treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 8, CD014962. [Google Scholar]
- Ader, F.; Bouscambert-Duchamp, M.; Hites, M.; Peiffer-Smadja, N.; Poissy, J.; Belhadi, D.; Diallo, A.; Lê, M.-P.; Peytavin, G.; Staub, T.; et al. Remdesivir plus standard of care versus standard of care alone for the treatment of patients admitted to hospital with COVID-19 (DisCoVeRy): A phase 3, randomised, controlled, open-label trial. Lancet Infect. Dis. 2022, 22, 209–221. [Google Scholar] [CrossRef]
- Kaka, A.S.; MacDonald, R.; Linskens, B.E.J.; Langsetmo, L.; Vela, M.K.; Duan-Porter, W.; Wilt, T.J. Major Update 2: Remdesivir for Adults with COVID-19: A Living Systematic Review and Meta-analysis for the American College of Physicians Practice Points. Ann. Intern. Med. 2022, 175, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Amstutz, A.; Speich, B.; Mentré, F.; Rueegg, C.S.; Belhadi, D.; Assoumou, L.; Burdet, C.; Murthy, S.; Dodd, L.E.; Wang, Y.; et al. Effects of remdesivir in patients hospitalised with COVID-19: A systematic review and individual patient data meta-analysis of randomised controlled trials. Lancet Respir. Med. 2023, 11, 453–464. [Google Scholar] [CrossRef]
- Ali, K.; Azher, T.; Baqi, M.; Binnie, A.; Borgia, S.; Carrier, F.M.; Cavayas, Y.A.; Chagnon, N.; Cheng, M.P.; Conly, J.; et al. Remdesivir for the treatment of patients in hospital with COVID-19 in Canada: A randomized controlled trial. Can. Med. Assoc. J. 2022, 194, E242–E251. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, E.; Chandak, A.; Zhang, Z.; Liang, S.; Thrun, M.; Gottlieb, R.L.; Kuritzkes, D.R.; Sax, P.E.; Wohl, D.A.; Casciano, R.; et al. Remdesivir Treatment in Hospitalized Patients with Coronavirus Disease 2019 (COVID-19): A Comparative Analysis of In-hospital All-cause Mortality in a Large Multicenter Observational Cohort. Clin. Infect. Dis. 2022, 75, e450–e458. [Google Scholar] [CrossRef]
- Hogan, J.I.; Duerr, R.; Dimartino, D.; Marier, C.; Hochman, S.E.; Mehta, S.; Wang, G.; Heguy, A. Remdesivir Resistance in Transplant Recipients with Persistent Coronavirus Disease 2019. Clin. Infect. Dis. 2023, 76, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. 2023, 76, e342–e349. [Google Scholar] [CrossRef]
- Ganatra, S.; Dani, S.S.; Ahmad, J.; Kumar, A.; Shah, J.; Abraham, G.M.; McQuillen, D.P.; Wachter, R.M.; Sax, P.E. Oral Nirmatrelvir and Ritonavir in Nonhospitalized Vaccinated Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2023, 76, 563–572. [Google Scholar] [CrossRef]
- Rubin, R. From Positive to Negative to Positive Again—The Mystery of Why COVID-19 Rebounds in Some Patients Who Take Paxlovid. JAMA 2022, 327, 2380–2382. [Google Scholar] [CrossRef]
- Butler, C.C.; Hobbs, F.D.R.; Gbinigie, O.A.; Rahman, N.M.; Hayward, G.; Richards, D.B.; Dorward, J.; Lowe, D.M.; Standing, J.F.; Breuer, J.; et al. Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): An open-label, platform-adaptive randomised controlled trial. Lancet 2023, 401, 281–293. [Google Scholar] [CrossRef]
- Wong, C.K.H.; Au, I.C.H.; Lau, K.T.K.; Lau, E.H.Y.; Cowling, B.J.; Leung, G.M. Real-world effectiveness of molnupiravir and nirmatrelvir plus ritonavir against mortality, hospitalisation, and in-hospital outcomes among community-dwelling, ambulatory patients with confirmed SARS-CoV-2 infection during the omicron wave in Hong Kong: An observational study. Lancet 2022, 400, 1213–1222. [Google Scholar]
- Khoo, S.H.; FitzGerald, R.; Saunders, G.; Middleton, C.; Ahmad, S.; Edwards, C.J.; Hadjiyiannakis, D.; Walker, L.; Lyon, R.; Shaw, V.; et al. Molnupiravir versus placebo in unvaccinated and vaccinated patients with early SARS-CoV-2 infection in the UK (AGILE CST-2): A randomised, placebo-controlled, double-blind, phase 2 trial. Lancet Infect. Dis. 2023, 23, 183. [Google Scholar] [CrossRef] [PubMed]
- Flisiak, R.; Zarębska-Michaluk, D.; Rogalska, M.; Kryńska, J.A.; Kowalska, J.; Dutkiewicz, E.; Dobrowolska, K.; Jaroszewicz, J.; Moniuszko-Malinowska, A.; Rorat, M.; et al. Real-world experience with molnupiravir during the period of SARS-CoV-2 Omicron variant dominance. Pharmacol. Rep. 2022, 74, 1279–1285. [Google Scholar] [CrossRef]
- EMA. Refusal of the Marketing Authorisation for Lagevrio (Molnupiravir). 2023. Available online: www.ema.europa.eu/en/documents/smop-initial/questions-answers-refusal-marketing-authorisation-lagevrio-molnupiravir_en.pdf (accessed on 21 April 2023).
- Shah, V.P.; Farah, W.H.; Hill, J.C.; Hassett, L.C.; Binnicker, M.J.; Yao, J.D.; Murad, M.H. Association between SARS-CoV-2 cycle threshold values and clinical outcomes in patients with COVID-19: A systematic review and meta-analysis. Open Forum. Infect. Dis. 2021, 8, ofab453. [Google Scholar] [CrossRef]
- Alonso-Navarro, R.; Cuesta, G.; Santos, M.; Cardozo, C.; Rico, V.; Garcia-Pouton, N.; Tuset, M.; Bodro, M.; Morata, L.; Puerta-Alcalde, P.; et al. Qualitative subgenomic RNA to monitor the response to remdesivir in hos-pitalized patients with COVID-19: Impact on the length of hospital stay and mortality. Clin. Infect. Dis. 2022, 76, 32–38. [Google Scholar] [CrossRef]
- Kim, J.Y.; Bae, J.Y.; Bae, S.; Cha, H.H.; Kwon, J.S.; Suh, M.H.; Lee, H.J.; Jung, J.; Kim, M.J.; Cui, C.; et al. Diagnostic usefulness of subgenomic RNA detection of viable SARS-CoV-2 in patients with COVID-19. Clin. Microbiol. Infect. 2022, 28, 101–106. [Google Scholar] [CrossRef]
- Dai, C.L.; Kornilov, S.A.; Roper, R.T.; Cohen-Cline, H.; Jade, K.; Smith, B.; Heath, J.R.; Diaz, G.; Goldman, J.D.; Magis, A.T.; et al. Characteristics and Factors Associated with Coronavirus Disease 2019 Infection, Hospitalization, and Mortality Across Race and Ethnicity. Clin. Infect. Dis. 2021, 73, 2193–2204. [Google Scholar] [CrossRef]
- Gray, W.K.; Navaratnam, A.V.; Day, J.; Wendon, J.; Briggs, T.W.R. Changes in COVID-19 in-hospital mortality in hospitalised adults in England over the first seven months of the pandemic: An observational study using administrative data. Lancet Reg. Health Eur. 2021, 5, 100104. [Google Scholar] [CrossRef] [PubMed]
- Khamis, F.; Memish, Z.; Al Bahrani, M.; Al Dowaiki, S.; Pandak, N.; Al Bolushi, Z.; Al Salmi, I.; Al-Zakwani, I. Prevalence and predictors of in-hospital mortality of patients hospitalized with COVID-19 infection. J. Infect. Public Health 2021, 14, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Castilla, J.; Guevara, M.; Miqueleiz, A.; Baigorria, F.; Ibero-Esparza, C.; Navascués, A.; Trobajo-Sanmartín, C.; Martínez-Baz, I.; Casado, I.; Burgui, C.; et al. Risk Factors of Infection, Hospitalization and Death from SARS-CoV-2: A Population-Based Cohort Study. J. Clin. Med. 2021, 10, 2608. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, E.; Asgary, A.; Tavakoli, N.; Zali, A.; Dastan, F.; Daaee, A.; Badakhshan, M.; Esmaily, H.; Jamaldini, S.H.; Safari, S.; et al. Symptom Prediction and Mortality Risk Calculation for COVID-19 Using Machine Learning. Front. Artif. Intell. 2021, 4, 673527. [Google Scholar] [CrossRef]
- Agrawal, U.; Katikireddi, S.V.; McCowan, C.; Mulholland, R.H.; Azcoaga-Lorenzo, A.; Amele, S.; Fagbamigbe, A.F.; Vasileiou, E.; Grange, Z.; Shi, T.; et al. COVID-19 hospital admissions and deaths after BNT162b2 and ChAdOx1 nCoV-19 vaccinations in 2·57 million people in Scotland (EAVE II): A prospective cohort study. Lancet Respir. Med. 2021, 9, 1439–1449. [Google Scholar] [CrossRef]
- Lana, R.M.; Freitas, L.P.; Codeço, C.T.; Pacheco, A.G.; de Carvalho, L.M.F.; Villela, D.A.M.; Coelho, F.C.; Cruz, O.G.; Niquini, R.P.; Porto, V.B.G.; et al. Identification of priority groups for COVID-19 vaccination in Brazil. Cad Saude Publica 2021, 37, e00049821. [Google Scholar] [CrossRef]
- Agrawal, U.; Azcoaga-Lorenzo, A.; Fagbamigbe, A.F.; Vasileiou, E.; Henery, P.; Simpson, C.R.; Stock, S.J.; Shah, S.A.; Robertson, C.; Woolhouse, M.; et al. Association between multimorbidity and mortality in a cohort of patients admitted to hospital with COVID-19 in Scotland. J. R. Soc. Med. 2022, 115, 22–30. [Google Scholar] [CrossRef]
- Ouattara, E.; Bruandet, A.; Borde, A.; Lenne, X.; Binder-Foucard, F.; Le-Bourhis-Zaimi, M.; Muller, J.; Loc, P.T.B.; Séguret, F.; du Montcel, S.T.; et al. Risk factors of mortality among patients hospitalised with COVID-19 in a critical care or hospital care unit: Analysis of the French national medico administrative database. BMJ Open Respir. Res. 2021, 8, e001002. [Google Scholar] [CrossRef]
- Lapi, F.; Domnich, A.; Marconi, E.; Rossi, A.; Grattagliano, I.; Lagolio, E.; Medea, G.; Sessa, A.; Cricelli, I.; Icardi, G.; et al. Predicting the risk of severe COVID-19 outcomes in primary care: Development and validation of a vulnerability index for equitable allocation of effective vaccines. Expert Rev. Vaccines 2022, 21, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Discacciati, M.G.; Siani, S.; Campa, A.; Nakaya, H.I. Why should obese youth be prioritized in COVID-19 vaccination programs? A nationwide retrospective study. Lancet Reg. Health Am. 2022, 7, 100167. [Google Scholar] [CrossRef] [PubMed]
- Israel, A.; Schäffer, A.A.; Merzon, E.; Green, I.; Magen, E.; Golan-Cohen, A.; Vinker, S.; Ruppin, E. A calculator for COVID-19 severity prediction based on patient risk factors and number of vaccines received. Microorganisms 2022, 10, 1238. [Google Scholar] [CrossRef]
- Davies, M.A.; Kassanjee, R.; Rousseau, P.; Morden, E.; Johnson, L.; Solomon, W.; Hsiao, N.Y.; Hussey, H.; Meintjes, G.; Paleker, M.; et al. Western Cape and South African National Departments of Health in collaboration with the National Institute for Communicable Diseases in South Africa Affiliations. Outcomes of laboratory-confirmed SARS-CoV-2 infection in the Omicron-driven fourth wave compared with previous waves in the Western Cape Province, South Africa. Trop. Med. Int. Health 2022, 27, 564–573. [Google Scholar] [CrossRef]
- Esteban, C.; Villanueva, A.; García-Gutierrez, S.; Aramburu, A.; Gorordo, I.; Quintana, J.M. Working Group TC. COPD in SARS-CoV-2 pandemic. baseline characteristics related to hospital admissions. Expert Rev. Respir. Med. 2022, 16, 477–484. [Google Scholar] [PubMed]
- Portuondo-Jimenez, J.; Bilbao-González, A.; Tíscar-González, V.; Garitano-Gutiérrez, I.; García-Gutiérrez, S.; Martínez-Mejuto, A.; Santiago-Garin, J.; Arribas-García, S.; García-Asensio, J.; Chart-Pascual, J.; et al. Modelling the risk of hospital admission of lab confirmed SARS-CoV-2-infected patients in primary care: A population-based study. Intern. Emerg. Med. 2022, 17, 1211–1221. [Google Scholar] [CrossRef]
- Moreno-Perez, O.; Ribes, I.; Boix, V.; Martinez-García, M.; Otero-Rodriguez, S.; Reus, S.; Sánchez-Martínez, R.; Ramos, J.M.; Chico-Sánchez, P.; Merino, E. Hospitalized patients with breakthrough COVID-19: Clinical features and poor outcome predictors. Int. J. Infect. Dis. 2022, 118, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Antoon, J.W.; Grijalva, C.G.; Thurm, C.; Richardson, T.; Spaulding, A.B.; Ii, R.J.T.; Reyes, M.A.; Shah, S.S.; Burns, J.E.; Kenyon, C.C.; et al. Factors Associated with COVID-19 Disease Severity in US Children and Adolescents. J. Hosp. Med. 2021, 16, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R.; Yan, H.T.; Da Camara, N.T.; Smith, C.; Ward, J.; Tudur-Smith, C.; Linney, M.; Clark, M.; Whittaker, E.; Saatci, D.; et al. Which children and young people are at higher risk of severe disease and death after hospitalisation with SARS-CoV-2 infection in children and young people: A systematic review and individual patient meta-analysis. Eclinicalmedicine 2022, 44, 101287. [Google Scholar] [CrossRef]
- Boudou, M.; Óhaiseadha, C.; Garvey, P.; O’dwyer, J.; Hynds, P. Modelling COVID-19 severity in the Republic of Ireland using patient co-morbidities, socioeconomic profile and geographic location, February to November 2020. Sci. Rep. 2021, 11, 18474. [Google Scholar] [CrossRef]
- Ge, E.; Li, Y.; Wu, S.; Candido, E.; Wei, X. Association of pre-existing comorbidities with mortality and disease severity among 167,500 individuals with COVID-19 in Canada: A population-based cohort study. PLoS ONE 2021, 16, e0258154. [Google Scholar] [CrossRef]
- Agrawal, U.; Bedston, S.; McCowan, C.; Oke, J.; Patterson, L.; Robertson, C.; Akbari, A.; Azcoaga-Lorenzo, A.; Bradley, D.T.; Fagbamigbe, A.F.; et al. Severe COVID-19 outcomes after full vaccination of primary schedule and initial boosters: Pooled analysis of national prospective cohort studies of 30 million individuals in England, Northern Ireland, Scotland, and Wales. Lancet 2022, 400, 1305–1320. [Google Scholar] [CrossRef]
- Semenzato, L.; Botton, J.; Drouin, J.; Cuenot, F.; Dray-Spira, R.; Weill, A.; Zureik, M. Chronic diseases, health conditions and risk of COVID-19-related hospitalization and in-hospital mortality during the first wave of the epidemic in France: A cohort study of 66 million people. Lancet Reg. Health Eur. 2021, 8, 100158. [Google Scholar] [CrossRef]
- Yates, T.; Zaccardi, F.; Islam, N.; Razieh, C.; Gillies, C.L.; Lawson, C.A.; Chudasama, Y.; Rowlands, A.; Davies, M.J.; Docherty, A.B.; et al. Obesity, Ethnicity, and Risk of Critical Care, Mechanical Ventilation, and Mortality in Patients Admitted to Hospital with COVID-19: Analysis of the ISARIC CCP-UK Cohort. Obesity (Silver Spring) 2021, 29, 1223–1230. [Google Scholar] [CrossRef]
- Treskova-Schwarzbach, M.; Haas, L.; Reda, S.; Pilic, A.; Borodova, A.; Karimi, K.; Koch, J.; Nygren, T.; Scholz, S.; Schönfeld, V.; et al. Pre-existing health conditions and severe COVID-19 outcomes: An umbrella review approach and meta-analysis of global evidence. BMC Med. 2021, 19, 212. [Google Scholar] [CrossRef] [PubMed]
- Antos, A.; Kwong, M.L.; Balmorez, T.; Villanueva, A.; Murakami, S. Unusually High Risks of COVID-19 Mortality with Age-Related Comorbidities: An Adjusted Meta-Analysis Method to Improve the Risk Assessment of Mortality Using the Comorbid Mortality Data. Infect. Dis. Rep. 2021, 13, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Román, J.S.; Candel, F.J.; Carretero, M.D.M.; Sanz, J.C.; Pérez-Abeledo, M.; Barreiro, P.; Viñuela-Prieto, J.M.; Ramos, B.; Canora, J.; Barba, R.; et al. Cross-Sectional Analysis of Risk Factors for Outbreak of COVID-19 in Nursing Homes for Older Adults in the Community of Madrid. Gerontology 2023, 69, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Henrina, J.; Lim, M.A.; Lawrensia, S.; Yonas, E.; Vania, R.; Huang, I.; Lukito, A.A.; Suastika, K.; Kuswardhani, R.T.; et al. Clinical frailty scale and mortality in COVID-19: A systematic review and dose-response meta-analysis. Arch. Gerontol. Geriatr. 2021, 93, 104324. [Google Scholar] [CrossRef]
- Díez-Villanueva, P.; Arizá-Solé, A.; Vidán, M.T.; Bonanad, C.; Formiga, F.; Sanchis, J.; Sánchez, F.J.M.; Ros, V.R.; Fernández, M.S.; Bueno, H.; et al. Recomendaciones de la Sección de Cardiología Geriátrica de la Sociedad Española de Cardiología para la valoración de la fragilidad en el anciano con cardiopatía. Rev. Esp. Cardiol. 2019, 72, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Vinson, A.J.M.; Agarwal, G.; Dai, R.; Anzalone, A.J.M.; Lee, S.B.; French, E.B.; Olex, A.M.; Madhira, V.M.; Mannon, R.B. COVID-19 in Solid Organ Transplantation: Results of the National COVID Cohort Collaborative. Transplant. Direct 2021, 7, e775. [Google Scholar] [CrossRef]
- Coll, E.; Fernández-Ruiz, M.; Padilla, M.; Moreso, F.; Hernández-Vicente, A.; Yañez, I.; Molina, M.; Vázquez-Sánchez, T.; Crespo, M.; Facundo, C.; et al. COVID-19 in Solid Organ Transplant Recipients in Spain Throughout 2020: Catching the Wave? Transplantation 2021, 105, 2146–2155. [Google Scholar] [CrossRef] [PubMed]
- Ao, G.; Wang, Y.; Qi, X.; Nasr, B.; Bao, M.; Gao, M.; Sun, Y.; Xie, D. The association between severe or death COVID-19 and solid organ transplantation: A systematic review and meta-analysis. Transplant. Rev. (Orlando) 2021, 35, 100628. [Google Scholar] [CrossRef] [PubMed]
- Linares, L.; Cofan, F.; Diekmann, F.; Herrera, S.; Marcos, M.A.; Castel, M.A.; Farrero, M.; Colmenero, J.; Ruiz, P.; Crespo, G.; et al. A propensity score-matched analysis of mortality in solid organ transplant patients with COVID-19 compared to non-solid organ transplant patients. PLoS ONE 2021, 16, e0247251. [Google Scholar] [CrossRef]
- Kates, O.S.; Haydel, B.M.; Florman, S.S.; Rana, M.M.; Chaudhry, Z.S.; Ramesh, M.S.; Safa, K.; Kotton, C.N.; Blumberg, E.A.; Besharatian, B.D.; et al. Coronavirus Disease 2019 in Solid Organ Transplant: A Multicenter Cohort Study. Clin. Infect. Dis. 2021, 73, e4090–e4099. [Google Scholar] [CrossRef]
- Swai, J.; Gui, M.; Long, M.; Wei, Z.; Hu, Z.; Liu, S. Humoral and cellular immune response to severe acute respiratory syndrome coronavirus-2 vaccination in haemodialysis and kidney transplant patients. Nephrology (Carlton) 2022, 27, 7–24. [Google Scholar] [CrossRef]
- Hamm, S.R.; Møller, D.L.; Pérez-Alós, L.; Hansen, C.B.; Pries-Heje, M.M.; Heftdal, L.D.; Hasselbalch, R.B.; Fogh, K.; Madsen, J.R.; Armenteros, J.J.A.; et al. Decline in Antibody Concentration 6 Months After Two Doses of SARS-CoV-2 BNT162b2 Vaccine in Solid Organ Transplant Recipients and Healthy Controls. Front. Immunol. 2022, 13, 832501. [Google Scholar] [CrossRef]
- Callaghan, C.J.; Mumford, L.; Curtis, R.M.K.; Williams, S.V.; Whitaker, H.; Andrews, N.; Bernal, J.L.; Ushiro-Lumb, I.; Pettigrew, G.J.; Thorburn, D.; et al. Real-world Effectiveness of the Pfizer-BioNTech BNT162b2 and Oxford-AstraZeneca ChAdOx1-S Vaccines Against SARS-CoV-2 in Solid Organ and Islet Transplant Recipients. Transplantation 2022, 106, 436–446. [Google Scholar] [CrossRef]
- Yetmar, Z.A.; Bhaimia, E.; Bierle, D.M.; Ganesh, R.; Razonable, R.R. Breakthrough COVID-19 after SARS-CoV-2 vaccination in solid organ transplant recipients: An analysis of symptomatic cases and monoclonal antibody therapy. Transpl. Infect. Dis. 2022, 24, e13779. [Google Scholar] [CrossRef] [PubMed]
- Qin, C.X.; Moore, L.W.; Anjan, S.; Rahamimov, R.; Sifri, C.D.; Ali, N.M.; Morales, M.K.; Tsapepas, D.S.; Basic-Jukic, N.; Miller, R.A.; et al. Risk of Breakthrough SARS-CoV-2 Infections in Adult Transplant Recipients. Transplantation 2021, 105, E265–E266. [Google Scholar] [CrossRef]
- Pinchera, B.; Buonomo, A.R.; Scotto, R.; Carrano, R.; Salemi, F.; Galluccio, F.; Guarino, M.; Viceconte, G.; Moriello, N.S.; Giaccone, A.; et al. Sotrovimab in Solid Organ Transplant Patients with Early, Mild/Moderate SARS-CoV-2 Infection: A Single-center Experience. Transplantation 2022, 106, e343–e345. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.J.; Hardesty, A.; Vieira, K.; Farmakiotis, D. Use of anti-spike monoclonal antibodies in kidney transplant recipients with COVID-19: Efficacy, ethnic and racial disparities. Am. J. Transplant. 2022, 22, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Chavarot, N.; Melenotte, C.; Amrouche, L.; Rouzaud, C.; Sberro-Soussan, R.; Pavie, J.; Martinez, F.; Pouvaret, A.; Leruez-Ville, M.; Cantin, D.; et al. Early treatment with sotrovimab monoclonal antibody in kidney transplant recipients with Omicron infection. Kidney Int. 2022, 101, 1290–1293. [Google Scholar] [CrossRef] [PubMed]
- Gaussen, A.; Hornby, L.M.; Rockl, G.M.; O’brien, S.; Delage, G.; Sapir-Pichhadze, R.M.; Drews, S.J.; Weiss, M.J.; Lewin, A. Evidence of SARS-CoV-2 Infection in Cells, Tissues, and Organs and the Risk of Transmission Through Transplantation. Transplantation 2021, 105, 1405–1422. [Google Scholar] [CrossRef] [PubMed]
- Neidlinger, N.A.; Smith, J.A.; D’alessandro, A.M.; Roe, D.; Taber, T.E.; Pereira, M.R.; Friedman, A.L. Organ recovery from deceased donors with prior COVID-19: A case series. Transpl. Infect. Dis. 2021, 23, e13503. [Google Scholar] [CrossRef]
- Romagnoli, R.; Gruttadauria, S.; Tisone, G.; Ettorre, G.M.; De Carlis, L.; Martini, S.; Tandoi, F.; Trapani, S.; Saracco, M.; Luca, A.; et al. Liver transplantation from active COVID-19 donors: A lifesaving opportunity worth grasping? Am. J. Transplant. 2021, 21, 3919–3925. [Google Scholar] [CrossRef]
- Sigler, R.; Shah, M.; Schnickel, G.; Pretorius, V.; Dan, J.; Taremi, M.; Aslam, S. Successful heart and kidney transplantation from a deceased donor with PCR positive COVID-19. Transpl. Infect. Dis. 2021, 23, e13707. [Google Scholar] [CrossRef]
- Koval, C.E.; Poggio, E.D.; Lin, Y.C.; Kerr, H.; Eltemamy, M.; Wee, A. Early success transplanting kidneys from donors with new SARS-CoV-2 RNA positivity: A report of 10 cases. Am. J. Transplant. 2021, 21, 3743–3749. [Google Scholar] [CrossRef] [PubMed]
- Saracco, M.; Romagnoli, R.; Martini, S. Solid non-lung organs from COVID-19 donors in seropositive or naive recipients: Where do we stand? Transpl. Infect. Dis. 2022, 24, e13761. [Google Scholar] [CrossRef] [PubMed]
- Dhand, A.; Gass, A.; Nishida, S.; Kai, M.; Berger, K.; Wolf, D.; Ohira, S.; Sogawa, H.; Lee, L.; Lebovics, E.; et al. Successful transplantation of organs from a deceased donor with early SARS-CoV-2 infection. Am. J. Transplant. 2021, 21, 3804–3805. [Google Scholar] [CrossRef] [PubMed]
- Eichenberger, E.M.; Kaul, D.R.; Wolfe, C.R. The pandemic provides a pathway: What we know and what we need to know about using COVID positive donors. Transpl. Infect. Dis. 2021, 23, e13727. [Google Scholar] [CrossRef]
- Kaul, D.R.; Valesano, A.L.; Petrie, J.G.; Sagana, R.; Lyu, D.; Lin, J.; Stoneman, E.; Smith, L.M.; Lephart, P.; Lauring, A.S. Donor to recipient transmission of SARS-CoV-2 by lung transplantation despite negative donor upper respiratory tract testing. Am. J. Transplant. 2021, 21, 2885–2889. [Google Scholar] [CrossRef]
- Kumar, D.; Humar, A.; Keshavjee, S.; Cypel, M. A call to routinely test lower respiratory tract samples for SARS-CoV-2 in lung donors. Am. J. Transplant. 2021, 21, 2623–2624. [Google Scholar] [CrossRef]
- Shah, G.L.; DeWolf, S.; Lee, Y.J.; Tamari, R.; Dahi, P.B.; Lavery, J.A.; Ruiz, J.D.; Devlin, S.M.; Cho, C.; Peled, J.U.; et al. Favorable outcomes of COVID-19 in recipients of hematopoietic cell transplantation. J. Clin. Investig. 2020, 130, 6656–6667. [Google Scholar] [CrossRef]
- Lupo-Stanghellini, M.T.; Xue, E.; Mastaglio, S.; Oltolini, C.; Angelillo, P.; Messina, C.; Piemontese, S.; Girlanda, S.; Farina, F.; Lazzari, L.; et al. COVID-19 in recipients of allogeneic stem cell transplantation: Favorable outcome. Bone Marrow Transplant. 2021, 56, 2312–2315. [Google Scholar] [CrossRef]
- Camargo, J.F.; Mendoza, M.A.; Lin, R.; Moroz, I.V.; Anderson, A.D.; Morris, M.I.; Natori, Y.; Natori, A.; Raja, M.; Lekakis, L.; et al. Clinical presentation and outcomes of COVID-19 following hematopoietic cell transplantation and cellular therapy. Transpl. Infect. Dis. 2021, 23, e13625. [Google Scholar] [CrossRef]
- Ljungman, P.; de la Camara, R.; Mikulska, M.; Tridello, G.; Aguado, B.; Al Zahrani, M.; Apperley, J.; Berceanu, A.; Bofarull, R.M.; Calbacho, M.; et al. COVID-19 and stem cell transplantation; results from an EBMT and GETH multicenter prospective survey. Leukemia 2021, 35, 2885–2894. [Google Scholar] [CrossRef]
- Orchard, K.; Dignan, F.L.; Lee, J.; Pearce, R.; Desai, M.; McFarlane, E.; Parkin, A.; Shearn, P.; Snowden, J.A. The NICE COVID-19 rapid guideline on haematopoietic stem cell transplantation: Development, implementation and impact. Br. J. Haematol. 2021, 192, 467–473. [Google Scholar] [CrossRef]
- Ljungman, P.; Transplantation, F.T.E.S.F.B.A.M.; Mikulska, M.; De La Camara, R.; Basak, G.W.; Chabannon, C.; Corbacioglu, S.; Duarte, R.; Dolstra, H.; Lankester, A.C.; et al. The challenge of COVID-19 and hematopoietic cell transplantation; EBMT recommendations for management of hematopoietic cell transplant recipients, their donors, and patients undergoing CAR T-cell therapy. Bone Marrow Transplant. 2020, 55, 2071–2076. [Google Scholar] [CrossRef]
- Tehrani, D.M.; Wang, X.; Rafique, A.M.; Hayek, S.S.; Herrmann, J.; Neilan, T.G.; Desai, P.; Morgans, A.; Lopez-Mattei, J.; Parikh, R.V.; et al. Impact of cancer and cardiovascular disease on in-hospital outcomes of COVID-19 patients: Results from the american heart association COVID-19 cardiovascular disease registry. Cardio-Oncology 2021, 7, 28. [Google Scholar] [CrossRef]
- Bushman, D.; Davidson, A.; Pathela, P.; Greene, S.K.; Weiss, D.; Reddy, V.; New York City Fatal Case-Control St New York City Fatal Case-Control Study Team; Latash, J. Risk Factors for Death Among Hospitalized Patients Aged 21–64 Years Diagnosed with COVID-19—New York City, March 13–April 9, 2020. J. Racial Ethn. Health Disparities 2022, 9, 1584–1599. [Google Scholar] [CrossRef]
- Roel, E.; Pistillo, A.; Recalde, M.; Fernández-Bertolín, S.; Aragón, M.; Soerjomataram, I.; Jenab, M.; Puente, D.; Prieto-Alhambra, D.; Burn, E.; et al. Cancer and the risk of coronavirus disease 2019 diagnosis, hospitalisation and death: A population-based multistate cohort study including 4 618 377 adults in Catalonia, Spain. Int. J. Cancer 2022, 150, 782–794. [Google Scholar] [CrossRef]
- Mittelman, M.; Magen, O.; Barda, N.; Dagan, N.; Oster, H.S.; Leader, A.; Balicer, R. Effectiveness of the BNT162b2mRNA COVID-19 vaccine in patients with hematological neoplasms in a nationwide mass vaccination setting. Blood 2022, 139, 1439–1451. [Google Scholar] [CrossRef]
- Martínez, J.C.; Sica, R.A.; Stockerl-Goldstein, K.; Rubinstein, S.M. COVID-19 in Patients with Hematologic Malignancies: Outcomes and Options for Treatments. Acta Haematol. 2022, 145, 244–256. [Google Scholar] [CrossRef]
- Elkrief, A.; Wu, J.T.; Jani, C.; Enriquez, K.T.; Glover, M.; Shah, M.R.; Shaikh, H.G.; Beeghly-Fadiel, A.; French, B.; Jhawar, S.R.; et al. Learning through a Pandemic: The Current State of Knowledge on COVID-19 and Cancer. Cancer Discov. 2022, 12, 303–330. [Google Scholar] [CrossRef]
- Arellano-Llamas, A.A.; Vela-Ojeda, J.; Hernandez-Caballero, A. Chronic Lymphocytic Leukemia in the SARS-CoV-2 Pandemic. Curr. Oncol. Rep. 2022, 24, 209–213. [Google Scholar] [CrossRef]
- Pinato, D.J.; Scotti, L.; Gennari, A.; Colomba-Blameble, E.; Dolly, S.; Loizidou, A.; Chester, J.; Mukherjee, U.; Zambelli, A.; Aguilar-Company, J.; et al. Determinants of enhanced vulnerability to coronavirus disease 2019 in UK patients with cancer: A European study. Eur. J. Cancer 2021, 150, 190–202. [Google Scholar] [CrossRef]
- Ribera, J.-M.; Morgades, M.; Coll, R.; Barba, P.; López-Lorenzo, J.-L.; Montesinos, P.; Foncillas, M.-A.; Cabrero, M.; Gómez-Centurión, I.; Morales, M.-D.; et al. Frequency, Clinical Characteristics and Outcome of Adults with Acute Lymphoblastic Leukemia and COVID 19 Infection in the First vs. Second Pandemic Wave in Spain. Clin. Lymphoma Myeloma Leuk. 2021, 21, e801–e809. [Google Scholar] [CrossRef]
- Shmueli, E.S.; Itay, A.; Margalit, O.; Berger, R.; Halperin, S.; Jurkowicz, M.; Levin, E.G.; Levy, I.; Olmer, L.; Regev-Yochay, G.; et al. Efficacy and safety of BNT162b2 vaccination in patients with solid cancer receiving anticancer therapy—A single center prospective study. Eur. J. Cancer 2021, 157, 124–131. [Google Scholar] [CrossRef]
- Brosh-Nissimov, T.; Orenbuch-Harroch, E.; Chowers, M.; Elbaz, M.; Nesher, L.; Stein, M.; Maor, Y.; Cohen, R.; Hussein, K.; Weinberger, M.; et al. BNT162b2 vaccine breakthrough: Clinical characteristics of 152 fully vaccinated hospitalized COVID-19 patients in Israel. Clin. Microbiol. Infect. 2021, 27, 1652–1657. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; Verbruggen, L.; Teuwen, L.; Vanhoutte, G.; Kerckhove, S.V.; Raats, S.; Van der Massen, I.; De Keersmaecker, S.; Debie, Y.; Huizing, M.; et al. Reduced humoral immune response after BNT162b2 coronavirus disease 2019 messenger RNA vaccination in cancer patients under antineoplastic treatment. ESMO Open 2021, 6, 100274. [Google Scholar] [CrossRef]
- Duléry, R.; Lamure, S.; Delord, M.; Di Blasi, R.; Chauchet, A.; Hueso, T.; Rossi, C.; Drenou, B.; Fischer, B.D.; Soussain, C.; et al. Prolonged in-hospital stay and higher mortality after COVID-19 among patients with non-Hodgkin lymphoma treated with B-cell depleting immunotherapy. Am. J. Hematol. 2021, 96, 934–944. [Google Scholar] [CrossRef]
- Safari, M.; Faradmal, J.; Bashirian, S.; Soltanian, A.R.; Khazaei, S.; Roshanaei, G. Identifying the Risk Factors for Mortality in Patients with Cancer and COVID-19 in Hamadan, the West of Iran. J. Gastrointest. Cancer 2022, 53, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Ambrosioni, J.; Blanco, J.L.; Reyes-Urueña, J.M.; Davies, M.-A.; Sued, O.; Marcos, M.A.; Martínez, E.; Bertagnolio, S.; Alcamí, J.; Miro, J.M.; et al. Overview of SARS-CoV-2 infection in adults living with HIV. Lancet HIV 2021, 8, e294–e305. [Google Scholar] [CrossRef]
- Gervasoni, C.; Meraviglia, P.; Riva, A.; Giacomelli, A.; Oreni, L.; Minisci, D.; Atzori, C.; Ridolfo, A.; Cattaneo, D. Clinical Features and Outcomes of Patients with Human Immunodeficiency Virus with COVID-19. Clin. Infect. Dis. 2020, 71, 2276–2278. [Google Scholar] [CrossRef] [PubMed]
- Karmen-Tuohy, S.; Carlucci, P.M.; Zervou, F.N.; Zacharioudakis, I.M.; Rebick, G.; Klein, E.; Reich, J.; Jones, S.; Rahimian, J. Outcomes Among HIV-Positive Patients Hospitalized with COVID-19. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 85, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Byrd, K.M.; Beckwith, C.G.; Garland, J.M.; Johnson, J.E.; Aung, S.; Cu-Uvin, S.; Farmakiotis, D.; Flanigan, T.; Gillani, F.S.; Macias-Gil, R.; et al. SARS-CoV-2 and HIV coinfection: Clinical experience from Rhode Island, United States. J. Int. AIDS Soc. 2020, 23, e25573. [Google Scholar] [CrossRef]
- Inciarte, A.; Gonzalez-Cordon, A.; Rojas, J.; Torres, B.; De Lazzari, E.; De La Mora, L.; Martinez-Rebollar, M.; Laguno, M.; Callau, P.; Gonzalez-Navarro, A.; et al. Clinical characteristics, risk factors, and incidence of symptomatic coronavirus disease 2019 in a large cohort of adults living with HIV: A single-center, prospective observational study. AIDS 2020, 34, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Cooper, T.J.; Woodward, B.L.; Alom, S.; Harky, A. Coronavirus disease 2019 (COVID-19) outcomes in HIV/AIDS patients: A systematic review. HIV Med. 2020, 21, 567–577. [Google Scholar] [CrossRef]
- Shalev, N.; Scherer, M.; Lasota, E.D.; Antoniou, P.; Yin, M.T.; Zucker, J.; Sobieszczyk, M.E. Clinical Characteristics and Outcomes in People Living with Human Immunodeficiency Virus Hospitalized for Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2294–2297. [Google Scholar] [CrossRef]
- Sigel, K.; Swartz, T.; Golden, E.; Paranjpe, I.; Somani, S.; Richter, F.; De Freitas, J.K.; Miotto, R.; Zhao, S.; Polak, P.; et al. Coronavirus 2019 and People Living with Human Immunodeficiency Virus: Outcomes for Hospitalized Patients in New York City. Clin. Infect. Dis. 2020, 71, 2933–2938. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, D.; Mara, E.; Hsu, L.; Scheer, S.; Rutherford, G.; Enanoria, W.; Gandhi, M. COVID-19 Susceptibility and Outcomes Among People Living with HIV in San Francisco. J. Acquir. Immune. Defic. Syndr. 2021, 86, 19–21. [Google Scholar] [CrossRef]
- Berenguer, J.; Díez, C.; Martín-Vicente, M.; Micán, R.; Pérez-Elías, M.J.; García-Fraile, L.J.; Vidal, F.; Suárez-García, I.; Podzamczer, D.; Del Romero, J.; et al. Prevalence and factors associated with SARS-CoV-2 seropositivity in the Spanish HIV Research Network Cohort. Clin. Microbiol. Infect. 2021, 27, 1678–1684. [Google Scholar] [CrossRef]
- Martín-Vicente, M.; Berenguer, J.; Muñoz-Gómez, M.J.; Díez, C.; Micán, R.; Pérez-Elías, M.J.; García-Fraile, L.J.; Peraire, J.; Suárez-García, I.; Jiménez-Sousa, M.; et al. Similar humoral immune responses against the SARS-CoV-2 spike protein in HIV and non-HIV individuals after COVID-19. J. Infect. 2022, 84, 418–467. [Google Scholar] [CrossRef] [PubMed]
- Blanco, J.L.; Ambrosioni, J.; Garcia, F.; Martínez, E.; Soriano, A.; Mallolas, J.; Miro, J.M. COVID-19 in patients with HIV: Clinical case series. Lancet HIV 2020, 7, e314–e316. [Google Scholar] [CrossRef]
- Western Cape Department of Health in collaboration with the National Institute for Communicable Diseases (South Africa). Risk Factors for Coronavirus Disease 2019 (COVID-19) Death in a Population Cohort Study from the Western Cape Province, South Africa. Clin Infect Dis. 2021, 73, e2005–e2015. [Google Scholar] [CrossRef]
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordóñez-Mena, J.M.; Reith, A.J.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of adverse coronavirus disease 2019 outcomes for people living with HIV. AIDS 2021, 35, F1–F10. [Google Scholar] [CrossRef]
- Braunstein, S.L.; Lazar, R.; Wahnich, A.; Daskalakis, D.C.; Blackstock, O.J. Coronavirus Disease 2019 (COVID-19) Infection Among People with Human Immunodeficiency Virus in New York City: A Population-Level Analysis of Linked Surveillance Data. Clin. Infect. Dis. 2021, 72, E1021–E1029. [Google Scholar] [CrossRef] [PubMed]
- Triant, V.A.; Gandhi, R.T. When Epidemics Collide: Why People with Human Immunodeficiency Virus May Have Worse Coronavirus Disease 2019 Outcomes and Implications for Vaccination. Clin. Infect. Dis. 2021, 72, e1030–e1034. [Google Scholar] [CrossRef] [PubMed]
- Varshney, K.; Ghosh, P.; Stiles, H.; Iriowen, R. Risk Factors for COVID-19 Mortality Among People Living with HIV: A Scoping Review. AIDS Behav. 2022, 26, 2256–2265. [Google Scholar] [CrossRef] [PubMed]
- Brown, A.E.; Croxford, S.E.; Nash, S.; Khawam, J.; Kirwan, P.; Kall, M.; Bradshaw, D.; Sabin, C.; Miller, R.F.; Post, F.A.; et al. COVID-19 mortality among people with diagnosed HIV compared to those without during the first wave of the COVID-19 pandemic in England. HIV Med. 2022, 23, 90–102. [Google Scholar] [CrossRef] [PubMed]
- Vizcarra, P.; Pérez-Elías, M.J.; Quereda, C.; Moreno, A.; Vivancos, M.J.; Dronda, F.; Casado, J.L.; Moreno, S.; Fortún, J.; Navas, E.; et al. Description of COVID-19 in HIV-infected individuals: A single-center, prospective cohort. Lancet HIV 2020, 7, e554–e564. [Google Scholar] [CrossRef]
- Meyerowitz, E.A.; Kim, A.Y.; Ard, K.L.; Basgoz, N.; Chu, J.T.; Hurtado, R.M.; Lee, C.K.; He, W.; Minukas, T.; Nelson, S.; et al. Disproportionate burden of coronavirus disease 2019 among racial minorities and those in congregate settings among a large cohort of people with HIV. AIDS 2020, 34, 1781–1787. [Google Scholar] [CrossRef]
- Di Biagio, A.; Ricci, E.; Calza, L.; Squillace, N.; Menzaghi, B.; Rusconi, S.; Orofino, G.; Bargiacchi, O.; Molteni, C.; Valsecchi, L.; et al. Factors associated with hospital admission for COVID-19 in HIV patients. AIDS 2020, 34, 1983–1985. [Google Scholar] [CrossRef]
- Etienne, N.; Karmochkine, M.; Slama, L.; Pavie, J.; Batisse, D.; Usubillaga, R.; Letembet, V.-A.; Brazille, P.; Canouï, E.; Slama, D.; et al. HIV infection and COVID-19: Risk factors for severe disease. AIDS 2020, 34, 1771–1774. [Google Scholar] [CrossRef]
- Hadi, Y.B.; Naqvi, S.F.Z.; Kupec, J.T.; Sarwari, A.R. Characteristics and outcomes of COVID-19 in patients with HIV: A multicentre research network study. AIDS 2020, 34, F3–F8. [Google Scholar] [CrossRef]
- Mirzaei, H.; McFarland, W.; Karamouzian, M.; Sharifi, H. COVID-19 Among People Living with HIV: A Systematic Review. AIDS Behav. 2021, 25, 85–92. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2021, 8, e24–e32. [Google Scholar] [CrossRef] [PubMed]
- Tesoriero, J.M.; Swain, C.A.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among Persons Living with or without Diagnosed HIV Infection in New York State. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.E.; Peluso, M.J.; Margus, C.; Lopes, J.P.M.; He, C.; Gaisa, M.M.; Osorio, G.; Aberg, J.A.; Mullen, M.P. Clinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People with Human Immunodeficiency Virus. J. Infect. Dis. 2021, 223, 403–408. [Google Scholar] [CrossRef] [PubMed]
- BHIVA DEGPSAS and PA for the Clinical Study of A (APECS). BHIVA, DAIG, EACS, GESIDA, Polish Scientific AIDS Society and Portuguese Association for the clinical study of AIDS (APECS). Available online: https://www.bhiva.org/joint-statement-on-risk-of-COVID-19-for-PLWH-and-SARS-CoV-2-vaccine-advice (accessed on 6 September 2022).
- del Amo, J.; Polo, R.; Moreno, S.; Jarrín, I.; Hernán, M.A. SARS-CoV-2 infection and coronavirus disease 2019 severity in persons with HIV on antiretroviral treatment. AIDS 2022, 36, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.E.; Ignacio, R.A.B.; Whitney, B.M.; Delaney, J.A.; Nance, R.M.; Bamford, L.; Wooten, D.; Keruly, J.C.; Burkholder, G.; Napravnik, S.; et al. Factors Associated with Severity of COVID-19 Disease in a Multicenter Cohort of People with HIV in the United States, March–December 2020. JAIDS J. Acquir. Immune Defic. Syndr. 2022, 90, 369–376. [Google Scholar] [CrossRef]
- Childs, K.; Post, F.A.; Norcross, C.; Ottaway, Z.; Hamlyn, E.; Quinn, K.; Juniper, T.; Taylor, C. Hospitalized Patients with COVID-19 and Human Immunodeficiency Virus: A Case Series. Clin. Infect. Dis. 2020, 71, 2021–2022. [Google Scholar] [CrossRef]
- Díez, C.; Del Romero-Raposo, J.; Mican, R.; López, J.C.; Blanco, J.R.; Calzado, S.; Samperiz, G.; Portilla, J.; García-Fraile, L.J.; Gutiérrez, F.; et al. COVID-19 in hospitalized HIV-positive and HIV-negative patients: A matched study. HIV Med. 2021, 22, 867–876. [Google Scholar] [CrossRef]
- Lang, R.; Humes, E.; Coburn, S.B.; Horberg, M.A.; Fathi, L.F.; Watson, E.; Jefferson, C.R.; Park, L.S.; Gordon, K.S.; Akgün, K.M.; et al. Analysis of Severe Illness After Postvaccination COVID-19 Breakthrough Among Adults with and without HIV in the US. JAMA Netw. Open 2022, 5, e2236397. [Google Scholar] [CrossRef]
- Jassat, W.; Cohen, C.; Tempia, S.; Masha, M.; Goldstein, S.; Kufa, T.; Murangandi, P.; Savulescu, D.; Walaza, S.; Bam, J.-L.; et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV 2021, 8, e554–e567. [Google Scholar] [CrossRef]
- Yang, X.; Sun, J.; Patel, R.C.; Zhang, J.; Guo, S.; Zheng, Q.; Olex, A.L.; Olatosi, B.; Weissman, S.B.; Islam, J.Y.; et al. Associations between HIV infection and clinical spectrum of COVID-19: A population level analysis based on US National COVID Cohort Collaborative (N3C) data. Lancet HIV 2021, 8, e690–e700. [Google Scholar] [CrossRef]
- Danwang, C.; Noubiap, J.J.; Robert, A.; Yombi, J.C. Outcomes of patients with HIV and COVID-19 co-infection: A systematic review and meta-analysis. AIDS Res. Ther. 2022, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, C.; Casado, J.L.; Härter, G.; Vizcarra, P.; Moreno, A.; Cattaneo, D.; Meraviglia, P.; Spinner, C.D.; Schabaz, F.; Grunwald, S.; et al. Immune deficiency is a risk factor for severe COVID-19 in people living with HIV. HIV Med. 2021, 22, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.V.; Felsen, U.R.; Fisher, M.; Fazzari, M.J.; Ginsberg, M.S.; Beil, R.; Akiyama, M.J.; Anastos, K.; Hanna, D.B. Clinical Outcomes and Inflammatory Markers by HIV Serostatus and Viral Suppression in a Large Cohort of Patients Hospitalized with COVID-19. J. Acquir. Immune Defic. Syndr. 2021, 86, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.Y.; Jouanguy, E.; Zhang, Q.; Abel, L.; Puel, A.; Casanova, J.L. Human inborn errors of immunity to infection affecting cells other than leukocytes: From the immune system to the whole organism. Curr. Opin. Immunol. 2019, 59, 88–100. [Google Scholar] [CrossRef]
- Moens, L.; Meyts, I. Recent human genetic errors of innate immunity leading to increased susceptibility to infection. Curr. Opin. Immunol. 2020, 62, 79–90. [Google Scholar] [CrossRef]
- Zhang, S.Y. Herpes simplex virus encephalitis of childhood: Inborn errors of central nervous system cell-intrinsic immunity. Hum. Genet. 2020, 139, 911–918. [Google Scholar] [CrossRef]
- Tangye, S.G.; Latour, S. Primary immunodeficiencies reveal the molecular requirements for effective host defense against EBV infection. Blood 2020, 135, 644–655. [Google Scholar] [CrossRef]
- Lamborn, I.T.; Su, H.C. Genetic determinants of host immunity against human rhinovirus infections. Hum. Genet. 2020, 139, 949–959. [Google Scholar] [CrossRef] [PubMed]
- El-Sayed, Z.A.; Abramova, I.; Aldave, J.C.; Al-Herz, W.; Bezrodnik, L.; Boukari, R.; Bousfiha, A.A.; Cancrini, C.; Condino-Neto, A.; Dbaibo, G.; et al. X-linked agammaglobulinemia (XLA): Phenotype, diagnosis, and therapeutic challenges around the world. World Allergy Organ. J. 2019, 12, 100018. [Google Scholar] [CrossRef]
- Marcus, N.; Frizinsky, S.; Hagin, D.; Ovadia, A.; Hanna, S.; Farkash, M.; Maoz-Segal, R.; Agmon-Levin, N.; Broides, A.; Nahum, A.; et al. Minor Clinical Impact of COVID-19 Pandemic on Patients with Primary Immunodeficiency in Israel. Front. Immunol. 2021, 11, 614086. [Google Scholar] [CrossRef]
- Meyts, I.; Bucciol, G.; Quinti, I.; Neven, B.; Fischer, A.; Seoane, E.; Lopez-Granados, E.; Gianelli, C.; Robles-Marhuenda, A.; Jeandel, P.-Y.; et al. Coronavirus disease 2019 in patients with inborn errors of immunity: An international study. J. Allergy Clin. Immunol. 2021, 147, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Katzenstein, T.L.; Rasmussen, L.D.; Drabe, C.H.; Larsen, C.S.; Hansen, A.E.; Stærkind, M.; Knudsen, L.S.; Hansen, C.H.; Obel, N. Outcome of SARS-CoV-2 infection among patients with common variable immunodeficiency and a matched control group: A Danish nationwide cohort study. Front Immunol. 2022, 13, 994253. [Google Scholar] [CrossRef] [PubMed]
- Tangye, S.G.; Bucciol, G.; Meyts, I. Mechanisms underlying host defense and disease pathology in response to severe acute respiratory syndrome (SARS)-CoV2 infection: Insights from inborn errors of immunity. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 515–524. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [PubMed]
- Pardhan, S.; Wood, S.; Vaughan, M.; Trott, M. The Risk of COVID-19 Related Hospitalsation, Intensive Care Unit Admission and Mortality in People with Underlying Asthma or COPD: A Systematic Review and Meta-Analysis. Front. Med. (Lausanne) 2021, 8, 668808. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.J.; Menon, A.A.; Ghosh, A.J.; Putman, R.K.; Fredenburgh, L.E.; El-Chemaly, S.Y.; Goldberg, H.J.; Baron, R.M.; Hunninghake, G.M.; Doyle, T.J. Increased Odds of Death for Patients with Interstitial Lung Disease and COVID-19: A Case–Control Study. Am. J. Respir. Crit. Care Med. 2020, 202, 1710–1713. [Google Scholar] [CrossRef] [PubMed]
- Lemarquis, A.; Campbell, T.; Aranda-Guillén, M.; Hennings, V.; Brodin, P.; Kämpe, O.; Blennow, K.; Zetterberg, H.; Wennerås, C.; Eriksson, K.; et al. Severe COVID-19 in an APS1 patient with interferon autoantibodies treated with plasmapheresis. J. Allergy Clin. Immunol. 2021, 148, 96–98. [Google Scholar] [CrossRef]
- Bastard, P.; Orlova, E.; Sozaeva, L.; Lévy, R.; James, A.; Schmitt, M.M.; Ochoa, S.; Kareva, M.; Rodina, Y.; Gervais, A.; et al. Preexisting autoantibodies to type I IFNs underlie critical COVID-19 pneumonia in patients with APS-1. J. Exp. Med. 2021, 218, e20210554. [Google Scholar] [CrossRef]
- Meisel, C.; Akbil, B.; Meyer, T.; Lankes, E.; Corman, V.M.; Staudacher, O.; Unterwalder, N.; Kölsch, U.; Drosten, C.; Mall, M.A.; et al. Mild COVID-19 despite autoantibodies against type I IFNs in autoimmune polyendocrine syndrome type 1. J. Clin. Investig. 2021, 131, e150867. [Google Scholar] [CrossRef]
- du Bois, H.; Heim, T.A.; Rahman, S.A.; Yagnik, B.; Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Manry, J.; et al. Autoantibodies neutralizing type I IFNs are present in ~4% of uninfected individuals over 70 years old and account for ~20% of COVID-19 deaths. Sci. Immunol. 2021, 6, eabl4340. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.-H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Auto-antibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef] [PubMed]
- Manry, J.; Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Michailidis, E.; Hoffmann, H.-H.; Eto, S.; Garcia-Prat, M.; et al. The risk of COVID-19 death is much greater and age dependent with type I IFN autoantibodies. Proc. Natl. Acad. Sci. USA 2022, 119, e2200413119. [Google Scholar] [CrossRef] [PubMed]
- van der Made, C.I.; Simons, A.; Schuurs-Hoeijmakers, J.; Heuvel, G.V.D.; Mantere, T.; Kersten, S.; van Deuren, R.C.; Steehouwer, M.; van Reijmersdal, S.V.; Jaeger, M.; et al. Presence of Genetic Variants Among Young Men with Severe COVID-19. JAMA 2020, 324, 663–673. [Google Scholar] [CrossRef]
- Asano, T.; Boisson, B.; Onodi, F.; Matuozzo, D.; Moncada-Velez, M.; Renkilaraj, M.R.L.M.; Zhang, P.; Meertens, L.; Bolze, A.; Materna, M.; et al. X-linked recessive TLR7 deficiency in ~1% of men under 60 years old with life-threatening COVID-19. Sci. Immunol. 2021, 6, eabl4348. [Google Scholar] [CrossRef] [PubMed]
- Holter, J.C.; Pischke, S.E.; de Boer, E.; Lind, A.; Jenum, S.; Holten, A.R.; Tonby, K.; Barratt-Due, A.; Sokolova, M.; Schjalm, C.; et al. Systemic complement activation is associated with respiratory failure in COVID-19 hospitalized patients. Proc. Natl. Acad. Sci. USA 2020, 117, 25018–25025. [Google Scholar] [CrossRef]
- Karimi, M.; De Sanctis, V. Implications of SARSr-CoV 2 infection in thalassemias: Do patients fall into the “high clinical risk” category? Acta Biomed. 2020, 91, 50–56. [Google Scholar] [CrossRef]
- Ramlall, V.; Thangaraj, P.M.; Meydan, C.; Foox, J.; Butler, D.; Kim, J.; May, B.; De Freitas, J.K.; Glicksberg, B.S.; Mason, C.E.; et al. Immune complement and coagulation dysfunction in adverse outcomes of SARS-CoV-2 infection. Nat. Med. 2020, 26, 1609–1615. [Google Scholar] [CrossRef]
- Grumach, A.S.; Goudouris, E.; Junior, S.D.; Marcelino, F.C.; Alonso, M.L.O.; Martins, R.D.O.; Arpon, M.A.; Valle, S.O.R. COVID-19 affecting hereditary angioedema patients with and without C1 inhibitor deficiency. J. Allergy Clin. Immunol. Pract. 2021, 9, 508–510. [Google Scholar] [CrossRef]
- Goudouris, E.S.; Pinto-Mariz, F.; Mendonça, L.O.; Aranda, C.S.; Guimarães, R.R.; Kokron, C.; Barros, M.T.; Anísio, F.; Alonso, M.L.O.; Marcelino, F.; et al. Outcome of SARS-CoV-2 Infection in 121 Patients with Inborn Errors of Immunity: A Cross-Sectional Study. J. Clin. Immunol. 2021, 41, 1479–1489. [Google Scholar] [CrossRef]
- Pablos, J.L.; Galindo, M.; Carmona, L.; Lledó, A.; Retuerto, M.; Blanco, R.; Gonzalez, A.; Martinez-Lopez, D.; Castrejón, I.; Alvaro-Gracia, J.M.; et al. Clinical outcomes of hospitalised patients with COVID-19 and chronic inflammatory and autoimmune rheumatic diseases: A multicentric matched cohort study. Ann. Rheum. Dis. 2020, 79, 1544–1549. [Google Scholar] [CrossRef]
- Bachiller-Corral, J.; Boteanu, A.; Garcia-Villanueva, M.J.; de la Puente, C.; Revenga, M.; Diaz-Miguel, M.C.; Rodriguez-Garcia, A.; Morell-Hita, J.L.; Valero, M.; Larena, C.; et al. Risk of Severe COVID-19 Infection in Patients with Inflammatory Rheumatic Diseases. J. Rheumatol. 2021, 48, 1098–1102. [Google Scholar] [CrossRef] [PubMed]
- Bjornsson, A.H.; Grondal, G.; Kristjansson, M.; Jonsdottir, T.; Love, T.J.; Gudbjornsson, B. Prevalence, admission rates and hypoxia due to COVID-19 in patients with rheumatic disorders treated with targeted synthetic or biologic disease modifying antirheumatic drugs or methotrexate: A nationwide study from Iceland. Ann. Rheum. Dis. 2021, 80, 671–672. [Google Scholar] [CrossRef] [PubMed]
- Bower, H.; Frisell, T.; Di Giuseppe, D.; Delcoigne, B.; Ahlenius, G.-M.; Baecklund, E.; Chatzidionysiou, K.; Feltelius, N.; Forsblad-D’Elia, H.; Kastbom, A.; et al. Impact of the COVID-19 pandemic on morbidity and mortality in patients with inflammatory joint diseases and in the general population: A nationwide Swedish cohort study. Ann. Rheum. Dis. 2021, 80, 1086–1093. [Google Scholar] [CrossRef]
- Cordtz, R.; Lindhardsen, J.; Soussi, B.G.; Vela, J.; Uhrenholt, L.; Westermann, R.; Kristensen, S.; Nielsen, H.; Torp-Pedersen, C.; Dreyer, L. Incidence and severeness of COVID-19 hospitalization in patients with inflammatory rheumatic disease: A nationwide cohort study from Denmark. Rheumatology (Oxford) 2021, 60, SI59–SI67. [Google Scholar] [CrossRef]
- Conway, R.; Grimshaw, A.A.; Konig, M.F.; Putman, M.; Duarte-García, A.; Tseng, L.Y.; Cabrera, D.M.; Chock, Y.P.E.; Degirmenci, H.B.; Duff, E. SARS–CoV-2 Infection and COVID-19 Outcomes in Rheumatic Diseases: A Systematic Literature Review and Meta-Analysis. Arthritis Rheumatol. 2022, 74, 766–775. [Google Scholar] [CrossRef]
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Patidar, R.; Younis, K.; Desai, P.; Hosein, Z.; Padda, I.; Mangat, J.; Altaf, M. Comorbidity and its Impact on Patients with COVID-19. SN Compr. Clin. Med. 2020, 2, 1069–1076. [Google Scholar] [CrossRef]
- Fredi, M.; Cavazzana, I.; Moschetti, L.; Andreoli, L.; Franceschini, F.; Airò, P.; Bazzani, C.; Crisafulli, F.; Filippini, M.; Frassi, M.; et al. COVID-19 in patients with rheumatic diseases in northern Italy: A single-center observational and case–control study. Lancet Rheumatol. 2020, 2, e549–e556. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeld, M.; Tincani, A.; Andreoli, L.; Cattalini, M.; Greenbaum, A.; Kanduc, D.; Alijotas-Reig, J.; Zinserling, V.; Semenova, N.; Amital, H.; et al. COVID-19 and autoimmunity. Autoimmun. Rev. 2020, 19, 102597. [Google Scholar] [CrossRef] [PubMed]
- Emmi, G.; Bettiol, A.; Mattioli, I.; Silvestri, E.; Di Scala, G.; Urban, M.L.; Vaglio, A.; Prisco, D. SARS-CoV-2 infection among patients with systemic autoimmune diseases. Autoimmun. Rev. 2020, 19, 102575. [Google Scholar] [CrossRef]
- Lu, C.; Li, S.; Liu, Y. Role of immunosuppressive therapy in rheumatic diseases concurrent with COVID-19. Ann. Rheum. Dis. 2020, 79, S737–S739. [Google Scholar] [CrossRef]
- MacKenna, B.; Kennedy, N.A.; Mehrkar, A.; Rowan, A.; Galloway, J.; Matthewman, J.; Mansfield, K.E.; Bechman, K.; Yates, M.; Brown, J.; et al. Risk of severe COVID-19 outcomes associated with immune-mediated inflammatory diseases and immune-modifying therapies: A nationwide cohort study in the OpenSAFELY platform. Lancet Rheumatol. 2022, 4, e490–e506. [Google Scholar] [CrossRef]
- Jovani, V.; Calabuig, I.; Peral-Garrido, M.L.; Tovar-Sugrañes, E.; López-González, M.-D.; Bernabeu, P.; Martínez, A.; Esteve-Vives, J.; León-Ramírez, J.-M.; Moreno-Perez, O.; et al. Incidence of severe COVID-19 in a Spanish cohort of 1037 patients with rheumatic diseases treated with biologics and JAK-inhibitors. Ann. Rheum. Dis. 2022, 81, e131. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, G.A.; Gerosa, M.; Beretta, L.; Bellocchi, C.; Argolini, L.M.; Moroni, L.; Della Torre, E.; Artusi, C.; Nicolosi, S.; Caporali, R.; et al. COVID-19 in systemic lupus erythematosus: Data from a survey on 417 patients. Semin. Arthritis Rheum. 2020, 50, 1150–1157. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Bajocchi, G.; Mancuso, P.; Galli, E.; Muratore, F.; Boiardi, L.; Catanoso, M.; Pipitone, N.; Cassone, G.; Girolimetto, N.; et al. Susceptibility and severity of COVID-19 in patients treated with bDMARDS and tsDMARDs: A population-based study. Ann. Rheum. Dis. 2020, 79, 986–988. [Google Scholar] [CrossRef] [PubMed]
- FAI2R /SFR/SNFMI/SOFREMIP/CRI/IMIDIATE Consortium and Contributors. Severity of COVID-19 and survival in patients with rheumatic and inflammatory diseases: Data from the French RMD COVID-19 cohort of 694 patients. Ann. Rheum. Dis. 2021, 80, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Stastna, D.; Menkyova, I.; Drahota, J.; Mazouchova, A.; Adamkova, J.; Ampapa, R.; Grunermelova, M.; Peterka, M.; Recmanova, E.; Rockova, P.; et al. Multiple sclerosis, neuromyelitis optica spectrum disorder and COVID-19: A pandemic year in Czechia. Mult. Scler. Relat. Disord. 2021, 54, 103104. [Google Scholar] [CrossRef]
- Wetwittayakhlang, P.; Albader, F.; Golovics, P.A.; Hahn, G.D.; Bessissow, T.; Bitton, A.; Afif, W.; Wild, G.; Lakatos, P.L. Clinical Outcomes of COVID-19 and Impact on Disease Course in Patients with Inflammatory Bowel Disease. Can. J. Gastroenterol. Hepatol. 2021, 2021, 7591141. [Google Scholar] [CrossRef]
- Brenner, E.J.; Ungaro, R.C.; Gearry, R.B.; Kaplan, G.G.; Kissous-Hunt, M.; Lewis, J.D.; Ng, S.C.; Rahier, J.-F.; Reinisch, W.; Ruemmele, F.M.; et al. Corticosteroids, But Not TNF Antagonists, Are Associated with Adverse COVID-19 Outcomes in Patients with Inflammatory Bowel Diseases: Results from an International Registry. Gastroenterology 2020, 159, 481–491.e3. [Google Scholar] [CrossRef]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.I.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2020, 79, 859–866. [Google Scholar] [CrossRef]
- Strangfeld, A.; Schäfer, M.; Gianfrancesco, M.A.; Lawson-Tovey, S.; Liew, J.W.; Ljung, L.; Mateus, E.F.; Richez, C.; Santos, M.J.; Schmajuk, G.; et al. Factors associated with COVID-19-related death in people with rheumatic diseases: Results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Ann. Rheum. Dis. 2021, 80, 930–942. [Google Scholar] [CrossRef]
- Hasseli, R.; Mueller-Ladner, U.; Hoyer, B.F.; Krause, A.; Lorenz, H.-M.; Pfeil, A.; Richter, J.; Schäfer, M.; Schmeiser, T.; Strangfeld, A.; et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open 2021, 7, e001464. [Google Scholar] [CrossRef] [PubMed]
- Attauabi, M.; Seidelin, J.B.; Felding, O.K.; Wewer, M.D.; Arp, L.K.V.; Sarikaya, M.Z.; Egeberg, A.; Vladimirova, N.; Bendtsen, F.; Burisch, J. Coronavirus disease 2019, immune-mediated inflammatory diseases and immunosuppressive therapies—A Danish population-based cohort study. J. Autoimmun. 2021, 118, 102613. [Google Scholar] [CrossRef] [PubMed]
- Shi, T.; Pan, J.; Vasileiou, E.; Robertson, C.; Sheikh, A. Risk of serious COVID-19 outcomes among adults with asthma in Scotland: A national incident cohort study. Lancet Respir. Med. 2022, 10, 347–354. [Google Scholar] [CrossRef]
- Spiera, R.; Jinich, S.; Jannat-Khah, D. Rituximab, but not other antirheumatic therapies, is associated with impaired serological response to SARS- CoV-2 vaccination in patients with rheumatic diseases. Ann. Rheum. Dis. 2021, 80, 1357–1359. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High antibody response to two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef]
- Raiker, R.; DeYoung, C.; Pakhchanian, H.; Ahmed, S.; Kavadichanda, C.; Gupta, L.; Kardeş, S. Outcomes of COVID-19 in patients with rheumatoid arthritis: A multicenter research network study in the United States. Semin. Arthritis Rheum. 2022, 51, 1057–1066. [Google Scholar] [CrossRef]
- Andersen, K.M.; Bates, B.A.; Rashidi, E.S.; Olex, A.L.; Mannon, R.B.; Patel, R.C.; Singh, J.; Sun, J.; Auwaerter, P.G.; Ng, D.K.; et al. Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: A retrospective cohort study using data from the National COVID Cohort Collaborative. Lancet Rheumatol. 2022, 4, e33–e41. [Google Scholar] [CrossRef]
- Garcillán, B.; Salavert, M.; Regueiro, J.R.; Díaz-Castroverde, S. Response to Vaccines in Patients with Immune-Mediated Inflammatory Diseases: A Narrative Review. Vaccines 2022, 10, 297. [Google Scholar] [CrossRef]
- Bournia, V.-K.; Fragoulis, G.E.; Mitrou, P.; Mathioudakis, K.; Tsolakidis, A.; Konstantonis, G.; Tseti, I.; Vourli, G.; Tektonidou, M.G.; Paraskevis, D.; et al. Different COVID-19 outcomes among systemic rheumatic diseases: A nation-wide cohort study. Rheumatology (Oxford) 2023, 62, 1047–1056. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation * (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) |
|---|---|---|
| Age, frailty and institutionalized persons | ||
| HIGH | STRONG—VERY STRONG |
| HIGH | STRONG |
| HIGH | STRONG |
| MODERATE | MODERATE |
| MODERATE | MODERATE |
| Obesity | ||
| LOW | MODERATE |
| Renal failure | ||
| LOW | MODERATE |
| LOW | MODERATE |
| Liver failure | ||
| LOW | MODERATE |
| Solid organ transplantation | ||
| LOW | MODERATE |
| PCR-positive hematological or solid organ donors/recipients | ||
| LOW | MODERATE |
| Hematopoietic Stem Cell Transplantation (HSCT) | ||
| LOW | MODERATE |
| Oncology/oncohematology patient | ||
| MODERATE—HIGH | STRONG |
| MODERATE—HIGH | STRONG |
| Poorly controlled HIV infection with one or more comorbidities | ||
| MODERATE | STRONG |
| MODERATE | MODERATE |
| VERY LOW | WEAK |
| LOW | WEAK |
| HIGH | STRONG |
| Poorly controlled primary or secondary immunodeficiencies | ||
| LOW | WEAK |
| LOW | WEAK |
| Chronic steroid therapy and immune-mediated diseases | ||
| LOW | MODERATE |
| MODERATE | MODERATE |
| HIGH | STRONG |
| LOW | STRONG(as there is no evidence to recommend its use) |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 13) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient over 80 years of age, regardless of vaccination status or history of SARS-CoV-2 infection | HIGH | STRONG–VERY STRONG RECOMMENDATION | 100% | 100% |
| Being a patient over 65 years of age, regardless of vaccination status or history of SARS-CoV-2 infection, with three or more chronic-risk diseases ** | HIGH | STRONG | 100% | 100% |
| Being a patient over 65 years of age with a chronic-risk disease ** and without vaccination or previous infection *** | HIGH | STRONG | 100% | 100% |
| Being a person residing in a nursing home, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | MODERATE | 100% | 90.90% |
| Being a person with moderate–severe frailty (>4 on the Clinical Frailty Scale), regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | MODERATE | 100% | 90.90% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Disease) | Meeting (n = 13) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient with a BMI > 35 and without vaccination or previous infection ** | LOW | MODERATE | 100% | 100% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 13) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient on replacement therapy (hemodialysis/peritoneal dialysis) for chronic kidney disease, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | MODERATE | 100% | 100% |
| Being a patient with chronic kidney disease and glomerular filtration rate < 30 mL/min, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | MODERATE | 100% | 96.96% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 13) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient with liver failure in a state of cirrhosis or liver failure (Child–Pugh B or C, ≥7 points) and without vaccination or previous immunity ** | LOW | MODERATE | 100% | 96.96% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 6) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a solid organ transplant recipient, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | MODERATE | 100% | 100% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of Disease) | Meeting (n = 6) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a solid organ or hematopoietic progenitor donor with a positive PCR for SARS-CoV-2 is NOT considered an increased risk factor for SARS-CoV-2 transmission | LOW | MODERATE | 100% | 90.90% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 6) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a hematopoietic stem cell transplant (HSCT) recipient, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | MODERATE | 100% | 100% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of Disease) | Meeting (n = 6) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being an oncology patient undergoing antineoplastic chemotherapy, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | STRONG | 100% | 100% |
| Being an oncohematology patient with active malignancy, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | STRONG | 100% | 96.96% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 6) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being an HIV-infected patient with a CD4+ cell count < 200/mm3, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | STRONG | 100% | 96.96% |
| Being an HIV-infected patient with a CD4+ cell count of 200–350/mm3, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | MODERATE | 100% | 78.78% |
| Being a patient with HIV infection and poorly maintained virological control of HIV, regardless of vaccination status or history of SARS-CoV-2 infection | VERY LOW | WEAK | 100% | 84.84% |
| Being an HIV-infected patient with CD4+ cell count > 350/mm3 is NOT considered to be an increased risk factor | LOW | WEAK | 100% | 100% |
| Being a patient with HIV infection and having had a CD4+ nadir <200/mm3 is NOT considered to be an increased risk factor | HIGH | STRONG | 100% | 78.78% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Stages of the Disease) | Meeting (n = 7) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient with primary congenital immunodeficiency, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | WEAK | 100% | 100% |
| Being a patient with functional or anatomical asplenia, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | WEAK | 100% | 93.93% |
| Profile of Patients with an Increased Risk Factor for Severe Forms of COVID-19 | Quality of the Evidence | Strength of the Recommendation (Therapeutic Action to Prevent Progression to More Severe Disease) | Meeting (n = 7) * | Online Consensus (n = 33) * |
|---|---|---|---|---|
| Being a patient with certain systemic or immune-mediated autoimmune diseases **, depending on their stage and treatment modality, regardless of vaccination status or history of SARS-CoV-2 infection | LOW | MODERATE | 86% | 81.81% |
| Being a patient on chronic glucocorticoid therapy, regardless of vaccination status or history of SARS-CoV-2 infection | MODERATE | MODERATE | 86% | 90.90% |
| Being a patient on anti-CD20 treatment, regardless of vaccination status or history of SARS-CoV-2 infection | HIGH | STRONG | 100% | 100% |
| There is NOT enough published evidence to consider patients on treatment with other immunosuppressants than those previously indicated (e.g., JAK or TNF inhibitors) as an increased risk factor. | LOW | STRONG (as there is no evidence to recommend its use) | 100% | 87.87% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Candel, F.J.; Barreiro, P.; Salavert, M.; Cabello, A.; Fernández-Ruiz, M.; Pérez-Segura, P.; San Román, J.; Berenguer, J.; Córdoba, R.; Delgado, R.; et al. Expert Consensus: Main Risk Factors for Poor Prognosis in COVID-19 and the Implications for Targeted Measures against SARS-CoV-2. Viruses 2023, 15, 1449. https://doi.org/10.3390/v15071449
Candel FJ, Barreiro P, Salavert M, Cabello A, Fernández-Ruiz M, Pérez-Segura P, San Román J, Berenguer J, Córdoba R, Delgado R, et al. Expert Consensus: Main Risk Factors for Poor Prognosis in COVID-19 and the Implications for Targeted Measures against SARS-CoV-2. Viruses. 2023; 15(7):1449. https://doi.org/10.3390/v15071449
Chicago/Turabian StyleCandel, Francisco Javier, Pablo Barreiro, Miguel Salavert, Alfonso Cabello, Mario Fernández-Ruiz, Pedro Pérez-Segura, Jesús San Román, Juan Berenguer, Raúl Córdoba, Rafael Delgado, and et al. 2023. "Expert Consensus: Main Risk Factors for Poor Prognosis in COVID-19 and the Implications for Targeted Measures against SARS-CoV-2" Viruses 15, no. 7: 1449. https://doi.org/10.3390/v15071449
APA StyleCandel, F. J., Barreiro, P., Salavert, M., Cabello, A., Fernández-Ruiz, M., Pérez-Segura, P., San Román, J., Berenguer, J., Córdoba, R., Delgado, R., España, P. P., Gómez-Centurión, I. A., González del Castillo, J. M., Heili, S. B., Martínez-Peromingo, F. J., Menéndez, R., Moreno, S., Pablos, J. L., Pasquau, J., ... on behalf of the MODUS Investigators (Adenda). (2023). Expert Consensus: Main Risk Factors for Poor Prognosis in COVID-19 and the Implications for Targeted Measures against SARS-CoV-2. Viruses, 15(7), 1449. https://doi.org/10.3390/v15071449