

New Generation of Systemic Inflammatory Markers for Respiratory Syncytial Virus Infection in Children


Abstract
1. Introduction
2. Material and Method
2.1. Study Design and Participants
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. RSV Diagnosis
2.5. Analysis of Complete Blood Count (CBC)
2.6. Analysis of C-Reactive Protein (CRP)
2.7. Other Variables
2.8. Statistical Analysis
3. Results
4. Discussion
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention (CDC). Brief report: Respiratory syncytial virus activity—United States, 2004–2005. MMWR Morb. Mortal. Wkly. Rep. 2005, 54, 1259–1260. [Google Scholar]
- McIntosh, K. Respiratory Syncytial Virus. In Viral Infections of Humans Epidemiology and Control, 4th ed.; Evans, A.S., Kaslow, R.A., Eds.; Springer: Boston, MA, USA, 1997; pp. 691–711. [Google Scholar]
- Borchers, A.T.; Chang, C.; Gershwin, M.E.; Gershwin, L.J. Respiratory Syncytial Virus—A Comprehensive Review. Clin. Rev. Allergy Immunol. 2013, 45, 331–379. [Google Scholar] [CrossRef] [PubMed]
- Panda, S.; Mohakud, N.K.; Suar, M.; Kumar, S. Etiology, seasonality, and clinical characteristics of respiratory viruses in children with respiratory tract infections in Eastern India (Bhubaneswar, Odisha). J. Med. Virol. 2016, 89, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Simoes, E.A. Respiratory syncytial virus infection. Lancet 1999, 354, 847–852. [Google Scholar] [CrossRef]
- You, D.; Siefker, D.T.; Shrestha, B.; Saravia, J.; Cormier, S.A. Building a better neonatal mouse model to understand infant respiratory syncytial virus disease. Respir. Res. 2015, 16, 91. [Google Scholar] [CrossRef]
- Prozan, L.; Shusterman, E.; Ablin, J.; Mitelpunkt, A.; Weiss-Meilik, A.; Adler, A.; Choshen, G.; Kehat, O. Prognostic value of neutrophil-to-lymphocyte ratio in COVID-19 compared with Influenza and respiratory syncytial virus infection. Sci. Rep. 2021, 11, 21519. [Google Scholar] [CrossRef]
- Muhammad, S.; Fischer, I.; Naderi, S.; Faghih Jouibari, M.; Abdolreza, S.; Karimialavijeh, E.; Aslzadeh, S.; Mashayekhi, M.; Zojaji, M.; Kahlert, U.D.; et al. Systemic Inflammatory Index Is a Novel Predictor of Intubation Requirement and Mortality after SARS-CoV-2 Infection. Pathogens 2021, 10, 58. [Google Scholar] [CrossRef]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; A Madhi, S.; Omer, S.B.; Simões, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Zhong, P.; Zhang, H.; Chen, X.; Lv, F. Clinical characteristics of the lower respiratory tract infection caused by a single infection or coinfection of the human parainfluenza virus in children. J. Med. Virol. 2019, 91, 1625–1632. [Google Scholar] [CrossRef]
- Welliver, T.P.; Garofalo, R.P.; Hosakote, Y.; Hintz, K.H.; Avendano, L.; Sanchez, K.; Velozo, L.; Jafri, H.; Chavez-Bueno, S.; Ogra, P.L.; et al. Severe human lower respiratory tract illness caused by respiratory syncytial virus and influenza virus is characterized by the absence of pulmonary cytotoxic lymphocyte responses. J. Infect. Dis. 2007, 195, 1126–1136. [Google Scholar] [CrossRef]
- Meissner, H.C.; Hall, C.B. Respiratory syncytial virus. In Feigin & Cherry’s Textbook of Pediatric Infectious Diseases, 7th ed.; Cherry, J.D., Harrison, G.J., Kaplan, S.L., Steinbach, W.J., Hotez, P.J., Eds.; Elsevier Saunders: Philadelphia, PE, USA, 2014; pp. 2407–2434. [Google Scholar]
- Saijo, M.; Ishii, T.; Kokubo, M.; Murono, K.; Takimoto, M.; Fujita, K. White blood cell count, C-reactive protein and erythrocyte sedimentation rate in respiratory syncytial virus infection of the lower respiratory tract. Acta Paediatr. Jpn. 1996, 38, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Purcell, K.; Fergie, J. Lack of usefulness of an abnormal white blood cell count for predicting a concurrent serious bacterial infection in infants and young children hospitalized with respiratory syncytial virus lower respiratory tract infection. Pediatr. Infect. Dis. J. 2007, 26, 311–315. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, J.; Wang, C.; Yang, Q.; Xu, Y.; Xu, J.; Li, Y.; Yu, X.; Zhu, H.; Liu, J. Characteristics of respiratory virus infection during the outbreak of 2019 novel coronavirus in Beijing. Int. J. Infect. Dis. 2020, 96, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.C.; Liang, W.G.; Chen, F.W.; Hsu, J.H.; Yang, J.J.; Chang, M.S. IL-19 induces production of IL-6 and TNF-alpha and results in cell apoptosis through TNF-alpha. J. Immunol. 2002, 169, 4288–4297. [Google Scholar] [CrossRef] [PubMed]
- Channappanavar, R.; Perlman, S. Pathogenic human coronavirus infections: Causes and consequences of cytokine storm and immunopathology. Semin. Immunopathol. 2017, 39, 529–539. [Google Scholar] [CrossRef] [PubMed]
- Kumarasamy, C.; Sabarimurugan, S.; Madurantakam, R.M.; Lakhotiya, K.; Samiappan, S.; Baxi, S.; Nachimuthu, R.; Gothandam, K.M.; Jayaraj, R. Prognostic significance of blood inflammatory biomarkers NLR, PLR, and LMR in cancer-A protocol for systematic review and meta-analysis. Medicine 2019, 98, e14834. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.P.; Liu, J.P.; Tao, W.Q.; Li, H.M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients. Int. Immunopharmacol. 2020, 84, 106504. [Google Scholar] [CrossRef] [PubMed]
- Russell, C.D.; Unger, S.A.; Walton, M.; Schwarze, J. The human immune response to respiratory syncytial virus infection. Clin. Microbiol. Rev. 2017, 30, 481–502. [Google Scholar] [CrossRef]
- Liao, Y.; Liu, C.; He, W.; Wang, D. Study on the Value of Blood Biomarkers NLR and PLR in the Clinical Diagnosis of Influenza a Virus Infection in Children. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef]
- Lagunas-Alvarado, M.; Mijangos-Huesca, F.J.; Terán-González, J.O.; Lagunas-Alvarado, M.G.; Martínez-Zavala, N.; Reyes-Franco, I.; Hernández-Mendiola, R.; Santillán-Fragoso, W.J.; Copca-Nieto, D.V.; López y López, L.R.; et al. Systemic immune inflammatory index in sepsis. Med. Int. Méx. 2017, 33, 303–309. [Google Scholar]
- Aydogan, S.; Dilli, D.; Soysal, C.; Akduman, H.; Örün, U.A.; Taşar, M.; Taşoglu, I.; Zenciroglu, A. Role of systemic immune-inflammatory index in early diagnosis of sepsis in newborns with CHD. Cardiol. Young 2022, 32, 1826–1832. [Google Scholar] [CrossRef] [PubMed]
- Tekeli, A.; Çalışkan, M.B.; Bahadır, G.B.; Erdemir, Ö.K. Evaluation of systemic immune-inflammation index efficacy in predicting complicated appendicitis in pediatric emergency department. Çocuk acilde komplike apandisiti öngörmede sistemik immün inflamasyon indeks etkinliğinin değerlendirilmesi. Ulus Travma. Acil. Cerrahi. Derg. 2023, 29, 566–573. [Google Scholar]
- Güngör, A.; Göktuğ, A.; Yaradılmış, R.M.; Güneylioğlu, M.M.; Öztürk, B.; Bodur, İ.; Karacan, C.D.; Tuygun, N. Utility of the systemic immune-inflammation index to predict serious bacterial infections in infants with fever without a source. Postgrad. Med. 2022, 134, 698–702. [Google Scholar] [CrossRef] [PubMed]
- de Souza Pires-Neto, O.; Amoras, E.D.; Queiroz, M.A.; Demachki, S.; da Silva Conde, S.R.; Ishak, R.; Cayres-Vallinoto, I.M.; Vallinoto, A.C. Hepatic TLR4, MBL and CRP gene expression levels are associated with chronic hepatitis C. Infect. Genet. Evol. 2020, 80, 104200. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Huang, Y.; Shi, F.; Tan, K.; Ma, Q.; Chen, Y.; Jiang, X.; Li, X. C-reactive protein correlates with CT findings and predicts severe COVID19 early. J. Med. Virol. 2020, 92, 856–862. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Papan, C.; Willersinn, M.; Weiß, C.; Karremann, M.; Schroten, H.; Tenenbaum, T. Antibiotic utilization in hospitalized children under 2 years of age with influenza or respiratory syncytial virus infection—A comparative, retrospective analysis. BMC Infect. Dis. 2020, 20, 606. [Google Scholar] [CrossRef]
- Higdon, M.M.; Le, T.; O’Brien, K.L.; Murdoch, D.R.; Prosperi, C.; Baggett, H.C.; Brooks, W.A.; Feikin, D.R.; Hammitt, L.L.; Howie, S.R.; et al. Association of C-Reactive Protein With Bacterial and Respiratory Syncytial Virus-Associated Pneumonia Among Children Aged < 5 Years in the PERCH Study. Clin. Infect. Dis. 2017, 64 (Suppl. 3), S378–S386. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| RSV (−) (n: 148; 51.7%) | RSV (+) (n: 138; 48.3%) | p-Value | |
|---|---|---|---|
| Gender | |||
| Male | 87 (58.8%) | 73 (52.9%) | 0.316 † |
| Female | 61 (41.2%) | 65 (47.1%) | |
| Age(months) | 8 (5–11); 8.6 ± 8.9 | 13 (5–31.3); 23.2 ± 25.2 | <0.001 * |
| ≤24 | 145 (98.0%) | 92 (66.7%) | |
| 25–59 | 2 (1.4%) | 30 (21.7%) | <0.001 † |
| ≥60 | 1 (0.7%) | 16 (11.6%) | |
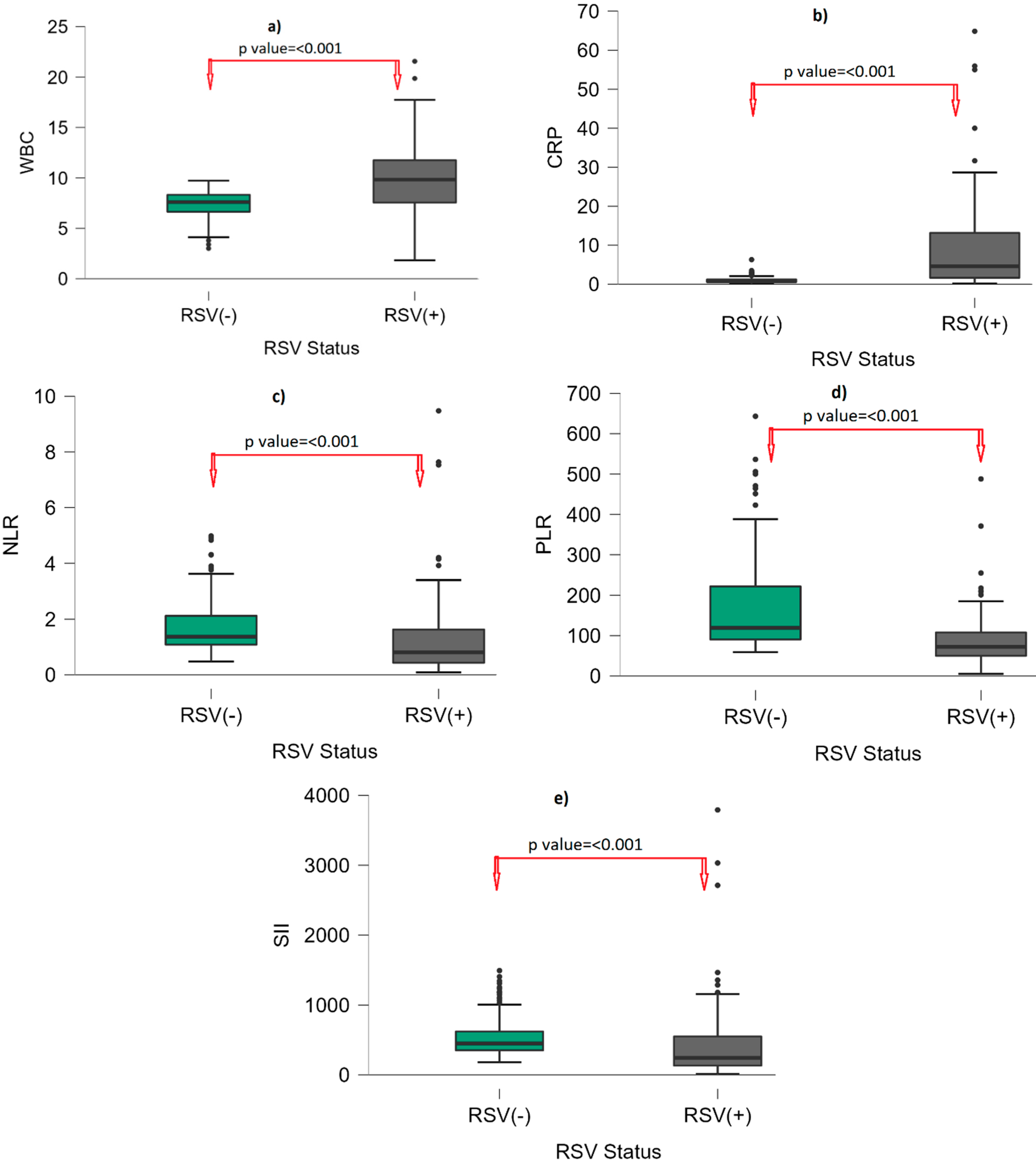
| WBC (×106/µL) | 7.6 (6.61–8.39) | 9.83 (7.53–11.83) | <0.001 * |
| HGB (g/dL) | 12 (11.1–12.88) | 11.6 (10.8–12.2) | 0.004 * |
| HCT (%) | 35.5 (33.15–38.78) | 34.1 (32.1–35.7) | <0.001 * |
| PLT (×103/mL) | 324.4 (292.5–357) | 317 (256–396.5) | 0.723 * |
| Lymphocyte (103/µL) | 2.78 (1.4–3.6) | 4.34 (2.65–6.36) | <0.001 * |
| Neutrophil (103/µL) | 3.83 (2.85–4.49) | 3.51 (2.26–5.85) | 0.999 * |
| Monocyte (103/µL) | 0.9 (0.65–1.19) | 0.92 (0.71–1.24) | 0.444 * |
| CRP (mg/L) | 0.72 (0.55–1.25) | 4.59 (1.57–13.63) | <0.001 * |
| NLR | 1.37 (1.08–2.16) | 0.81 (0.41–1.64) | <0.001 * |
| PLR | 119.31 (90.32–223.07) | 72.17 (49.63–108.26) | <0.001 * |
| SII | 449.5 (349.25–622) | 243.40 (127.03–554.42) | <0.001 * |
| RSV (−) (n: 148; 51.7%) | RSV (+) (n: 138; 48.3%) | p | |
|---|---|---|---|
| Fever | 111 (75%) | 138 (100%) | 0.001 |
| Cough | 127 (85.8%) | 138 (100%) | 0.001 |
| Vomiting | 39 (26.3%) | 20 (14.5%) | 0.013 |
| Wheezing | 148 (100%) | 138 (100%) | - |
| Apnea | 15 (10.1%) | 9 (6.5%) | 0.271 |
| Cyanosis | 53 (35.8%) | 55 (40%) | 0.481 |
| Groan | 143 (96.6%) | 136 (98.5%) | 0.291 |
| Acute otitis media | 24 (16.2%) | 40 (29.0%) | 0.010 |
| Rhinorrhea | 37 (25.0%) | 31 (22.5%) | 0.615 |
| Dyspnea | 83 (56%) | 94 (68%) | 0.036 |
| Infiltration on chest X-ray | 84 (56.7%) | 40 (29.0%) | 0.001 |
| Hospitalization | - | 16 (11.6%) | - |
| Length hospitalization | - | 1 (3–9); (Min: 2; Max: 20) | - |
| AUC | CI 95% | p-Value | Cutoff | Sensitivity | Specificity | |
|---|---|---|---|---|---|---|
| WBC | 0.841 | 0.765, 0.917 | <0.001 | 9 a | 63.7% | 87.8% |
| LYM | 0.703 | 0.618, 0.788 | <0.001 | 4.1 a | 57.5% | 87.8% |
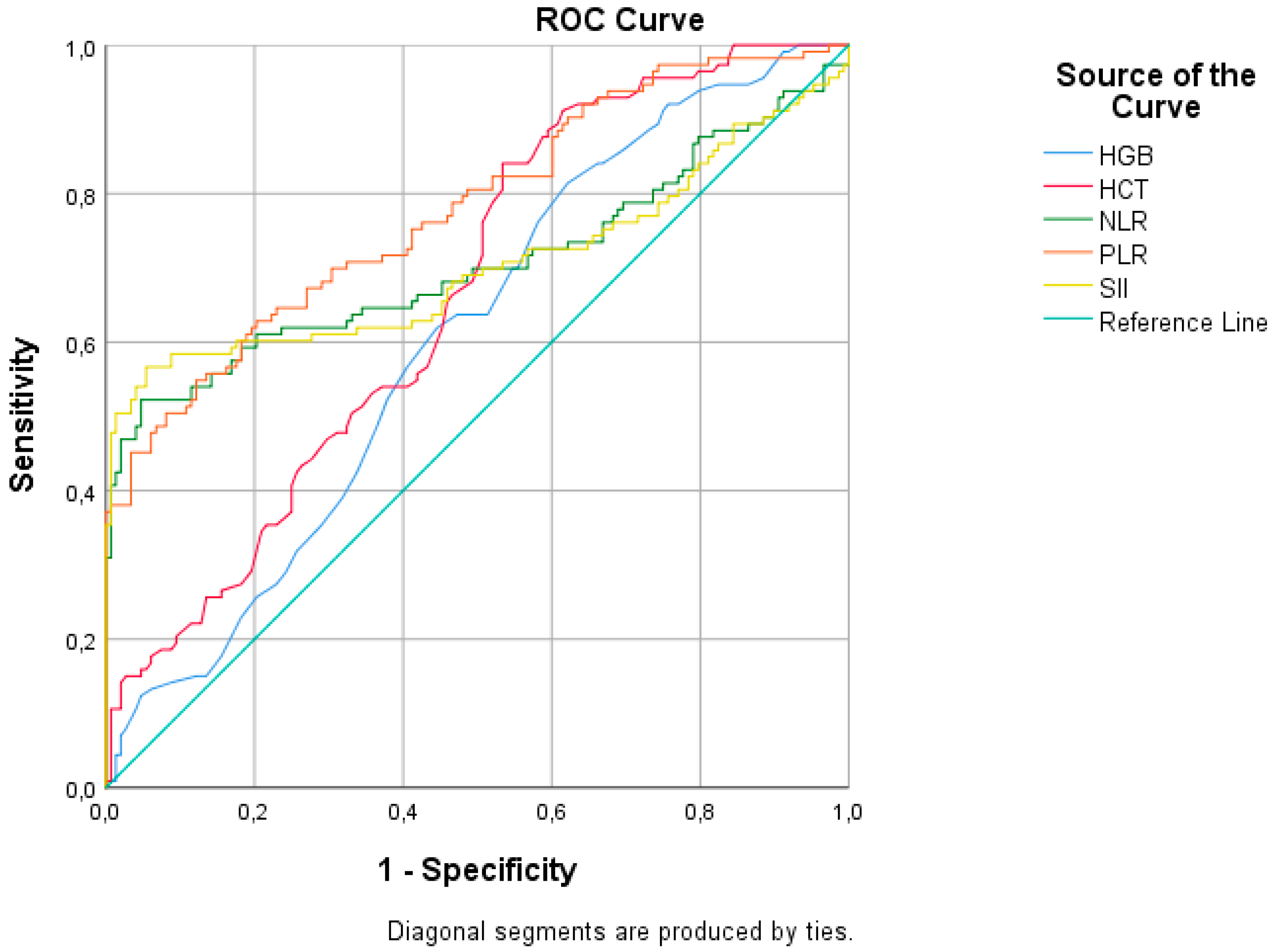
| HGB | 0.604 | 0.536, 0.672 | 0.004 | 12.5 b | 84.1% | 33.1% |
| HCT | 0.661 | 0.596, 0.726 | <0.001 | 37.5 b | 92.0% | 36.5% |
| NLR | 0.706 | 0.636, 0.776 | <0.001 | 0.85 b | 51.3% | 95.3% |
| PLR | 0.779 | 0.722, 0.836 | <0.001 | 73 b | 50.4% | 90.5% |
| SII | 0.705 | 0.633, 0.776 | <0.001 | 280 b | 56.6% | 93.9% |
| CRP | 0.869 | 0.800, 0.937 | <0.001 | 1.5 a | 80.4% | 82.4% |
| Age Group (Years) | ||||||
|---|---|---|---|---|---|---|
| ≤2 (n: 237; %82.9) | >2 (n: 49; %17.1) | |||||
| RSV (−) (n: 145; %61.2) | RSV (+) (n: 92; %38.8) | RSV (−) (n: 3; %6.1) | RSV (+) (n: 46; %93.9) | |||
| Median (25–75p) | Median (25–75p) | p | Median (25–75p) | Median (25–75p) | p | |
| WBC (×106/µL) | 7.6 (6.65–8.42) | 10.38 (8.56–12.1) | <0.001 | 7.32 (6.19–7.8) | 8.6 (6.81–10.72) | 0.342 |
| HGB (g/dL) | 12 (11.1–12.8) | 11.4 (10.65–12) | <0.001 | 12.2 (11.5–13.9) | 12.2 (11.6–12.5) | 0.719 |
| HCT (%) | 35.5 (33.1–38.7) | 33.2 (31.3–35.35) | <0.001 | 36.9 (33.9–39.6) | 35.1 (33.8–36.9) | 0.441 |
| PLT (×103/mL) | 324.2 (292–354) | 349 (271.5–420.5) | 0.089 | 358 (298–368) | 289 (238–339) | 0.111 |
| Lymphocyte (103/µL) | 2.7 (1.4–3.6) | 5.5 (4.265–7.387) | <0.001 | 3.47 (2.88–3.74) | 2.49 (2.077–3.19) | 0.158 |
| Neutrophil (103/µL) | 3.82 (2.88–4.43) | 2.86 (2.1–4.63) | 0.061 | 4.52 (2.61–4.75) | 4.73 (2.97–6.74) | 0.456 |
| Monocyte (103/µL) | 0.9 (0.67–1.19) | 0.995 (0.8–1.29) | 0.066 | 0.89 (0.58–0.9) | 0.84 (0.63–1.03) | 0.98 |
| CRP (mg/L) | 0.74 (0.55–1.26) | 2.78 (1.49–12.92) | <0.001 | 0.62 (0.6–0.7) | 7.93 (3.96–13.86) | 0.013 |
| NLR | 1.39 (1.09–2.18) | 0.56 (0.31–0.99) | <0.001 | 1.21 (0.91–1.37) | 1.63 (1.17–2.34) | 0.19 |
| PLR | 119.33 (90.51–223.53) | 57.82 (46.74–85.94) | <0.001 | 98.4 (85.88–124.31) | 102.66 (77.58–143.98) | 0.939 |
| SII | 455 (353–623) | 185.08 (95.86–384) | <0.001 | 408 (324–445) | 460.74 (275.05–774.62) | 0.488 |
| Age Group (Years) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤2 (n: 237; %82.9) | >2 (n: 49; %17.1) | |||||||||||
| AUC | CI 95% | p | Cutoff | Sensitivity | Specificity | AUC | CI 95% | p | Cutoff | Sensitivity | Specificity | |
| WBC | 0.915 | 0.843, 0.986 | <0.001 | 9 a | 72.4% | 87.6% | 0.787 | 0.620, 0.953 | 0.11 | - | - | - |
| LYM | 0.852 | 0.765, 0.940 | <0.001 | 4.1 a | 77.6% | 87.6% | 0.72 | 0.540, 0.900 | 0.22 | - | - | - |
| HGB | 0.669 | 0.598, 0.741 | <0.001 | 12.5 b | 89.5% | 33.1% | 0.593 | 0.273, 0.913 | 0.603 | - | - | - |
| HCT | 0.720 | 0.653, 0.787 | <0.001 | 37 b | 93.4% | 41.4% | 0.633 | 0.337, 0.930 | 0.458 | - | - | - |
| NLR | 0.840 | 0.773, 0.908 | <0.001 | 0.85 b | 71.1% | 95.2% | 0.867 | 0.710, 1.000 | 0.041 | 1.5 a | 54.1% | 100% |
| PLR | 0.853 | 0.797, 0.909 | <0.001 | 73 b | 64.5% | 90.3% | 0.52 | 0.280, 0.760 | 0.911 | - | - | - |
| SII | 0.806 | 0.730, 0.881 | <0.001 | 280 b | 71.1% | 93.8% | 0.773 | 0.603, 0.944 | 0.128 | - | - | - |
| CRP | 0.831 | 0.731, 0.931 | <0.001 | 1.5 a | 74.2% | 82.1% | 0.947 | 0.861, 1.000 | 0.013 | 1 a | 92% | 100% |
| 1.3 a | 80.6% | 75.9% | ||||||||||
| 2.1 a | 64.5% | 91.7% | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuyan, O.; Elgormus, Y.; Dumur, S.; Sayili, U.; Uzun, H. New Generation of Systemic Inflammatory Markers for Respiratory Syncytial Virus Infection in Children. Viruses 2023, 15, 1245. https://doi.org/10.3390/v15061245
Okuyan O, Elgormus Y, Dumur S, Sayili U, Uzun H. New Generation of Systemic Inflammatory Markers for Respiratory Syncytial Virus Infection in Children. Viruses. 2023; 15(6):1245. https://doi.org/10.3390/v15061245
Chicago/Turabian StyleOkuyan, Omer, Yusuf Elgormus, Seyma Dumur, Ugurcan Sayili, and Hafize Uzun. 2023. "New Generation of Systemic Inflammatory Markers for Respiratory Syncytial Virus Infection in Children" Viruses 15, no. 6: 1245. https://doi.org/10.3390/v15061245
APA StyleOkuyan, O., Elgormus, Y., Dumur, S., Sayili, U., & Uzun, H. (2023). New Generation of Systemic Inflammatory Markers for Respiratory Syncytial Virus Infection in Children. Viruses, 15(6), 1245. https://doi.org/10.3390/v15061245