

Epidemiological Transition and Strategies for the Control of Hepatitis A in Serbia


 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Area and Population Characteristics
2.2. Surveillance of HA in Serbia
2.3. Study Setting, Data Sources and Analysis
2.4. Socioeconomic, National Health Indicators, and HAV Incidence
2.5. Ethics Statement
3. Results
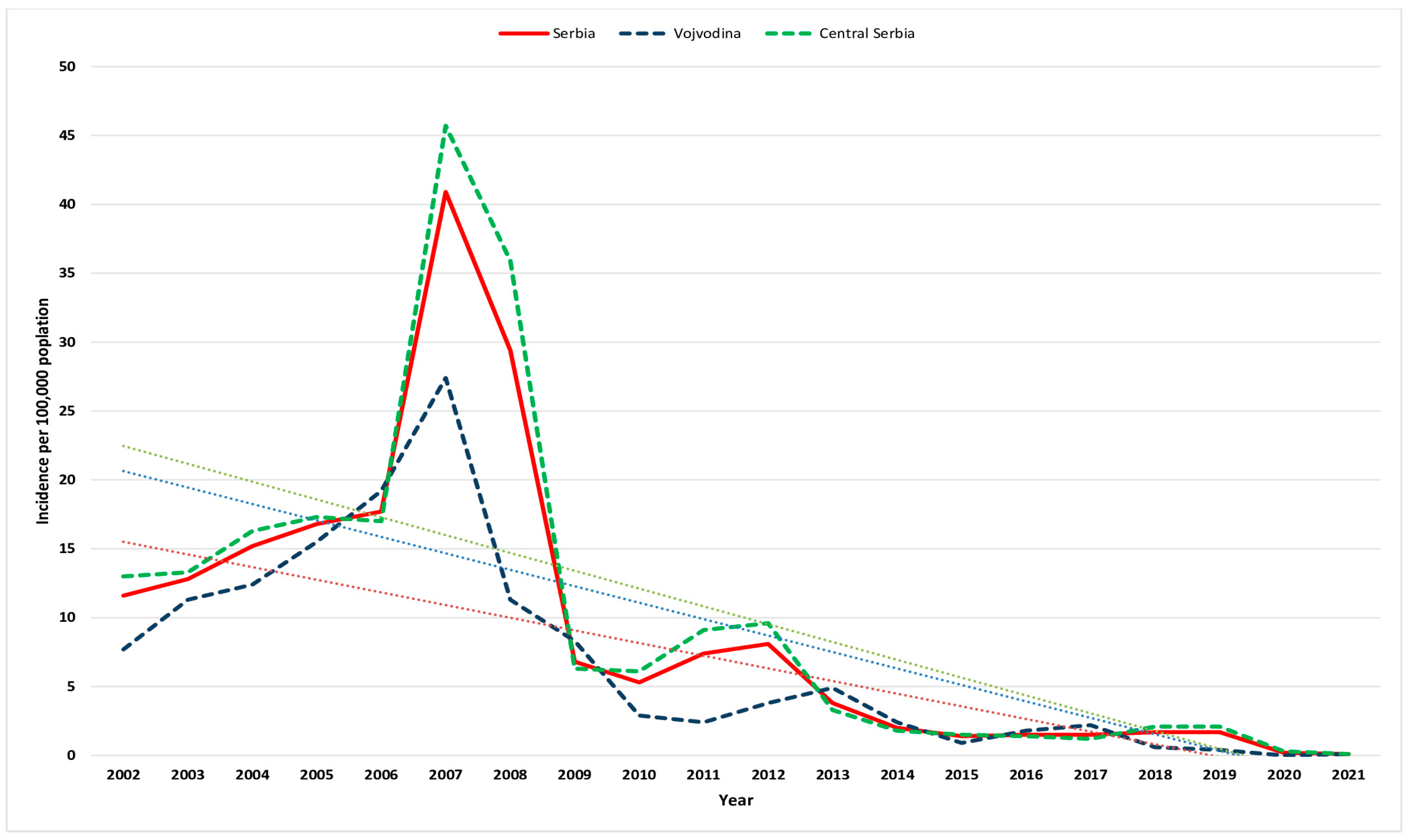
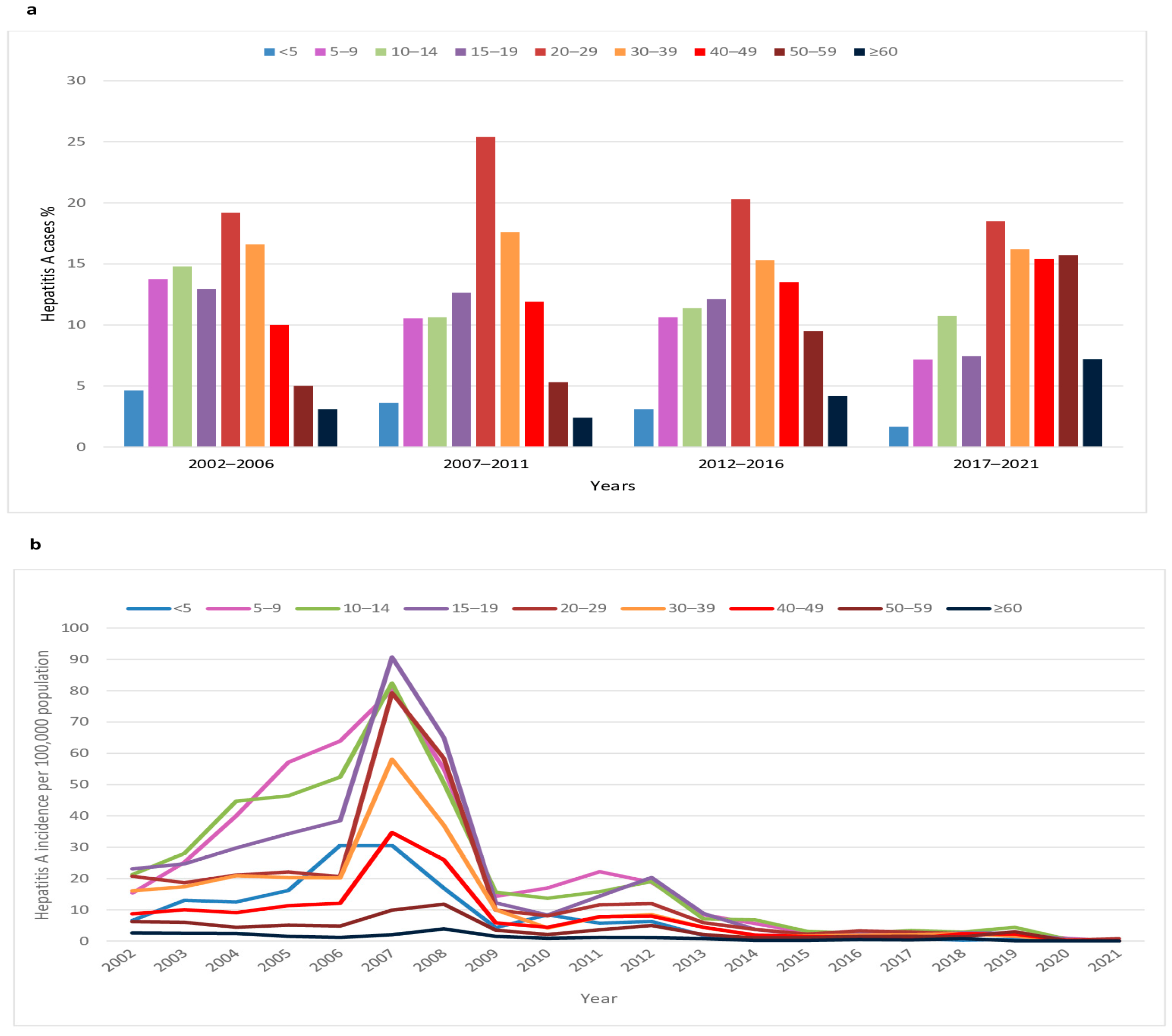
3.1. Hepatitis A Incidence Trends and Characteristics of Cases
3.2. Outbreaks of Hepatitis A in Serbia
3.3. Characteristics of Hepatitis A cases and Outbreaks in Vojvodina
3.4. Economic, National Health Data and the Incidence of Hepatitis A in Serbia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Hepatitis A Fact Sheet. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 19 December 2022).
- Jacobsen, K.H.; Wiersma, S.T. Hepatitis A virus seroprevalence by age and world region, 1990 and 2005. Vaccine 2010, 28, 6653–6657. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Position Paper on Hepatitis A Vaccines—October 2022. Wkly Epidemiol. Rec. 2022, 97, 493–512. [Google Scholar]
- Nelson, N.P.; Weng, M.K.; Hofmeister, M.G.; Moore, K.L.; Doshani, M.; Kamili, S.; Koneru, A.; Haber, P.; Hagan, L.; Romero, J.R.; et al. Prevention of Hepatitis A Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR Recomm. Rep. 2020, 69, 1–38. [Google Scholar] [CrossRef]
- Hollinger, F.; Fields, B.; Knipe, D.; Howley, P. (Eds.) Fields Virology, 6th ed.; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2013; pp. 550–581. [Google Scholar]
- Webb, G.W.; Kelly, S.; Dalton, H.R. Hepatitis A and Hepatitis E: Clinical and Epidemiological Features, Diagnosis, Treatment, and Prevention. Clin. Microbiol. Newsl. 2020, 42, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, K.H. Globalization and the Changing Epidemiology of Hepatitis A Virus. Cold Spring Harb. Perspect. Med. 2018, 8, a031716. [Google Scholar] [CrossRef] [PubMed]
- Mellou, K.; Chrysostomou, A.; Sideroglou, T.; Kyritsi, M.; Georgakopoulou, T.; Tsiodras, S.; Hadjichristodolou, C. Epidemiology of hepatitis A in Greece in the last decade: Management of reported cases and outbreaks and lessons learned. Epidemiol. Infect. 2020, 148, e58. [Google Scholar] [CrossRef]
- Carrillo-Santisteve, P.; Tavoschi, L.; Severi, E.; Bonfigli, S.; Edelstein, M.; Byström, E.; Lopalco, P. ECDC HAV Expert Panel. Seroprevalence and susceptibility to hepatitis A in the European Union and European Economic Area: A systematic review. Lancet Infect. Dis. 2017, 17, e306–e319. [Google Scholar] [CrossRef]
- Anastassopoulou, C.G.; Kafatos, G.; Nardone, A.; Andrews, N.; Pebody, R.G.; Mossong, J.; Davidkin, I.; Gelb, D.; DE Ory, F.; Thierfelder, W.; et al. The European Sero-Epidemiology Network 2 (ESEN2): Standardization of assay results for hepatitis A virus (HAV) to enable comparisons of seroprevalence data across 15 countries. Epidemiol. Infect. 2009, 137, 485–494. [Google Scholar] [CrossRef]
- Kurkela, S.; Pebody, R.; Kafatos, G.; Andrews, N.; Barbara, C.; Bruzzone, B.; Butur, D.; Caplinskas, S.; Davidkin, I.; Hatzakis, A.; et al. Comparative hepatitis A seroepidemiology in 10 European countries. Epidemiol. Infect. 2012, 140, 2172–2181. [Google Scholar] [CrossRef]
- Kafatos, G.; Andrews, N.; McConway, K.J.; Anastassopoulou, C.; Barbara, C.; De Ory, F.; Johansen, K.; Mossong, J.; Prosenc, K.; Vranckx, R.; et al. Estimating seroprevalence of vaccine-preventable infections: Is it worth standardizing the serological outcomes to adjust for different assays and laboratories? Epidemiol. Infect. 2015, 143, 2269–2278. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Hepatitis A. In ECDC. Annual Epidemiological Report for 2021; ECDC: Stockholm, Sweden, 2022; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/HEPA_AER_2021.pdf (accessed on 12 November 2022).
- Medić, S.; Anastassopoulou, C.; Milošević, V.; Dragnić, N.; Rajčević, S.; Ristić, M.; Petrović, V. Declining seroprevalence of hepatitis A in Vojvodina, Serbia. PLoS ONE 2019, 14, e0217176. [Google Scholar] [CrossRef]
- Official Gazette of the Republic of Serbia No. 65/2020. Rulebook on the Program of Mandatory and Recommended Immunization of the Population against Certain Infectious Diseases. (In Serbian). Available online: https://www.paragraf.rs/glasila/rs/sluzbeni-glasnik-republike-srbije-65-2020.html (accessed on 5 January 2023).
- Institute of Public Health of Serbia. “Dr Milan Jovanović Batut”. Professional and Methodological Guideline for Implementation of Mandatory and Recommended Immunization 2022. (In Serbian). Available online: https://www.batut.org.rs/download/SMUzaRedovnuImunizaciju2022.pdf (accessed on 20 December 2022).
- Schmutz, C.; Mäusezahl, D.; Jost, M. Hepatitis A in Switzerland: An analysis of 29 years of surveillance data and contemporary challenges. Travel Med. Infect. Dis. 2019, 27, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Statistical Office of the Republic of Serbia. Population Estimates by Age, Sex and Type of Settlement in 2021. Available online: https://data.stat.gov.rs/Home/Result/18010502?languageCode=en-US (accessed on 3 December 2022).
- Statistical Office of the Republic of Serbia. Statistical Yearbook of the Republic of Serbia. 2022. Available online: https://publikacije.stat.gov.rs/G2022/Pdf/G20222055.pdf (accessed on 1 November 2022).
- Uvalić, M.; Bartlett, W. Regional Disparities and Regional Development Policies in Serbia. 2021. Available online: https://library.fes.de/pdf-files/bueros/belgrad/18413-20211130.pdf (accessed on 12 December 2022).
- Statistical Office of the Republic of Serbia and UNICEF. Research on Multiple Indicators of the Position of Women and Children in Serbia and Research on Multiple Indicators of the Position of Women and Children in Roma Settlements in Serbia, 2019, Report on Research Findings. Available online: https://www.unicef.org/serbia/media/16056/file/MICS%206%20Istra%C5%BEivanje%20vi%C5%A1estrukih%20pokazatelja%20za%202019.%20godinu.pdf (accessed on 11 February 2023).
- Institute of Public Health of Vojvodina. Communicable Diseases in Vojvodina for 2018. Annual Report. 2019, p. 64. (In Serbian). Available online: http://izjzv.org.rs/publikacije/ZarazneBolesti/ZB_2018.pdf (accessed on 19 November 2022).
- Institute for Public Health of Serbia “Dr Milan Jovanović Batut”. Definitions of Cases of Infectious Diseases, Belgrade. 2017. (In Serbian). Available online: https://www.batut.org.rs/download/publikacije/20170807SrbijaDefinicijeSlucajevaZarazneBolesti.pdf (accessed on 18 December 2022).
- Official Journal of the European Union (Commission Implementing Decision (EU) 2012/506/EU). Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2012:262:0001:0057:EN:PDF (accessed on 11 December 2022).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Fifth Edition, 2016. World Health Organization, 2015. Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 15 December 2022).
- International Comparison Program. World Bank|World Development Indicators Database. World Bank|Eurostat-OECD PPP Programme. GDP per Capita, PPP (Current International $)- Serbia. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.PP.CD?locations=RS (accessed on 3 December 2022).
- United Nations Interagency Group for Child Mortality Estimation. Infant Mortality Rate, Serbia. 2021. Available online: https://childmortality.org/data/Serbia (accessed on 1 December 2022).
- Macrotrends. Serbia Infant Mortality Rate 1950–2023. Available online: https://www.macrotrends.net/countries/SRB/serbia/infant-mortality-rate (accessed on 2 December 2022).
- Official Gazette of the Republic of Serbia No. 136/2020. Law on the Protection of the Population from Infectious Diseases. (In Serbian). Available online: https://www.paragraf.rs/propisi/zakon_o_zastiti_stanovnistva_od_zaraznih_bolesti.html (accessed on 4 January 2023).
- Gossner, C.M.; Severi, E.; Danielsson, N.; Hutin, Y.; Coulombier, D. Changing hepatitis A epidemiology in the European Union: New challenges and opportunities. Eurosurveillance 2015, 20, 21101. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bruni, R.; Taffon, S.; Equestre, M.; Cella, E.; Lo Presti, A.; Costantino, A.; Chionne, P.; Madonna, E.; Golkocheva-Markova, E.; Bankova, D.; et al. Hepatitis a virus genotypes and strains from an endemic area of Europe, Bulgaria 2012–2014. BMC Infect. Dis. 2017, 17, 497. [Google Scholar] [CrossRef]
- Severi, E.; Verhoef, L.; Thornton, L.; Guzman-Herrador, B.R.; Faber, M.; Sundqvist, L.; Rimhanen-Finne, R.; Roque-Afonso, A.M.; Ngui, S.L.; Allerberger, F.; et al. Large and prolonged food-borne multistate hepatitis A outbreak in Europe associated with consumption of frozen berries, 2013 to 2014. Eurosurveillance 2015, 20, 21192. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Disease Prevention and Control. Disease Name. In ECDC. Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2022; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/HEPA_AER_2018_Report.pdf (accessed on 10 December 2022).
- Abutaleb, A.; Kottilil, S. Hepatitis A: Epidemiology, Natural History, Unusual Clinical Manifestations, and Prevention. Gastroenterol. Clin. N. Am. 2020, 49, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Hofmeister, M.G.; Xing, J.; Foster, M.A.; Augustine, R.J.; Burkholder, C.; Collins, J.; McBee, S.; Thomasson, E.D.; Thoroughman, D.; Weng, M.K.; et al. Hepatitis A Person-to-Person Outbreaks: Epidemiology, Morbidity Burden, and Factors Associated with Hospitalization-Multiple States, 2016–2019. J. Infect. Dis. 2021, 223, 426–434. [Google Scholar] [CrossRef] [PubMed]
- Lima, L.R.; De Almeida, A.J.; Tourinho Rdos, S.; Hasselmann, B.; Ximenez, L.L.; De Paula, V.S. Evidence of hepatitis A virus person-to-person transmission in household outbreaks. PLoS ONE 2014, 9, e102925. [Google Scholar] [CrossRef] [PubMed]
- Victor, J.C.; Surdina, T.Y.; Suleimenova, S.Z.; Favorov, M.O.; Bell, B.P.; Monto, A.S. Person-to-person transmission of hepatitis A virus in an urban area of intermediate endemicity: Implications for vaccination strategies. Am. J. Epidemiol. 2005, 163, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Fournet, N.; Baas, D.; van Pelt, W.; Swaan, C.; Ober, H.; Isken, L.; Cremer, J.; Friesema, I.; Vennema, H.; Boxman, I.; et al. Another possible food-borne outbreak of hepatitis A in the Netherlands indicated by two closely related molecular sequences, July to October 2011. Eurosurveillance 2012, 17, 20079. [Google Scholar] [CrossRef]
- Petrignani, M.; Harms, M.; Verhoef, L.; van Hunen, R.; Swaan, C.; van Steenbergen, J.; Boxman, I.; i Sala, R.P.; Ober, H.J.; Vennema, H.; et al. Update: A food-borne outbreak of hepatitis A in the Netherlands related to semi-dried tomatoes in oil, January–February 2010. Eurosurveillance 2010, 15, 19572. [Google Scholar] [CrossRef]
- Collective Nordic Outbreak Investigation Team. Joint analysis by the Nordic countries of a hepatitis A outbreak, October 2012 to June 2013: Frozen strawberries suspected. Eurosurveillance 2013, 18, 20520. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). European Food Safety Authority. Update: Outbreak of hepatitis A Virus Infection in Italy and Ireland. Rapid Outbreak Assessment. Stockholm: ECDC; July 2013. Available online: http://ecdc.europa.eu/en/publications/Publications/ROAupdate_HAV_Italy_Ireland-final.pdf (accessed on 2 January 2023).
- Perevoscikovs, J.; Lucenko, I.; Magone, S.; Brila, A.; Curikova, J.; Vennema, H. Community-wide outbreak of hepatitis A in Latvia in 2008—An update. Eurosurveillance 2009, 14, 19092. [Google Scholar] [CrossRef] [PubMed]
- Puoti, M.; Rossotti, R.; Merli, M. Hepatitis A Virus in men who have sex with men: Need for awareness and vaccination. Liver Int. 2018, 38, 581–584. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Hepatitis A Outbreaks in the EU/EEA Mostly Affecting Men Who Have Sex with Men. Rapid Risk Assessment; ECDC: Stockholm, Sweden, 2016; Available online: http://ecdc.europa.eu/en/publications/Publications/13-12-2016-RRA-Hepatitis%20A-United%20Kingdom.pdf (accessed on 21 December 2022).
- Institute of Public Health of Serbia. “Dr Milan Jovanović Batut”. Report on Immunization Carried out on the Territory of the Republic of Serbia in 2021. 2022. (In Serbian). Available online: https://www.batut.org.rs/download/izvestaji/Godisnji%20izvestaj%20o%20sprovedenoj%20imunizaciji%202021.pdf (accessed on 21 December 2022).
- Mello, V.M.; Bianchi, L.M.; Sousa, P.S.F.; Tavares, P.S.; Di Salvo, D.R.G.; Ginuino, C.F.; Almeida, N.A.A.; Fernandes, C.A.S.; Mello, F.C.A.; Villar, L.M.; et al. Increase in Hepatitis A Cases Linked to Imported Strains to Rio de Janeiro, Brazil: A Cross-Sectional Study. Viruses 2022, 14, 303. [Google Scholar] [CrossRef]
- Beebeejaun, K.; Degala, S.; Balogun, K.; Simms, I.; Woodhall, S.C.; Heinsbroek, E.; Crook, P.D.; Kar-Purkayastha, I.; Treacy, J.; Wedgwood, K.; et al. Outbreak of hepatitis A associated with men who have sex with men (MSM), England, July 2016 to January 2017. Eurosurveillance 2017, 22, 2100186. [Google Scholar] [CrossRef]
- Fares, A. Seasonality of hepatitis: A review update. J. Fam. Med. Prim. Care 2015, 4, 96–100. [Google Scholar] [CrossRef]
- Sa-nguanmoo, P.; Posuwan, N.; Vichaiwattana, P.; Vuthitanachot, V.; Saelao, S.; Foonoi, M.; Fakthongyoo, A.; Makaroon, J.; Srisingh, K.; Asawarachun, D.; et al. Declining Trend of Hepatitis A Seroepidemiology in Association with Improved Public Health and Economic Status of Thailand. PLoS ONE 2016, 11, e0151304. [Google Scholar] [CrossRef]
- Regional Economic Development Agency for Šumadija and Pomoravlje. Action Plan to Ensure Equitable Access to Water and Sanitation in the Region of Šumadija and Pomoravlje. Available online: https://unece.org/DAM/env/water/activities/Equitable_access/Action_plan_Serbia__final_Ang_27_02.pdf (accessed on 11 February 2023).
- Fangcheng, Z.; Xuanyi, W.; Mingding, C.; Liming, J.; Jie, W.; Qi, J.; Yuanping, G.; Wen, Q.; Yajuan, X.; Jiangsen, M. Era of vaccination heralds a decline in incidence of hepatitis A in high-risk groups in China. Hepat. Mon. 2012, 12, 100–105. [Google Scholar] [CrossRef]
- Background Document for the SAGE April 2022 Session on Hepatitis A Vaccines. Geneva: World Health Organization. 2022. Available online: https://who.int/publications/m/item/sage-april-2022-background-hepatitis-a-vaccines (accessed on 16 December 2022).
- Institute for Public Health of Serbia “Dr Milan Jovanović Batut”. The Report of Infectious Diseases for 2020. 2021. (In Serbian). Available online: https://www.batut.org.rs/download/izvestaji/IzvestajZarazneBolesti2020.pdf (accessed on 19 December 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2002–2006 | 2007–2011 | 2012–2016 | 2017–2021 | Total | |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| Cases | 5524 (40.4) | 6596 (48.2) | 1196 (8.7) | 363 (2.7) | 13,679 (100) |
| Sex | |||||
| Male | 2991 (54.1) | 3916 (59.4) | 654 (50) | 193 (54.0) | 7754 (56.7) |
| Female | 2533 (45.9) | 2680 (40.6) | 542 (50) | 170 (46.0) | 5925 (43.3) |
| HA-related deaths | |||||
| n | 2 | 3 | 0 | 0 | 5 |
| Mortality 1 | 0.02 | 0.04 | 0 | 0 | 0.06 |
| Average Incidence (95% CI) 1 | |||||
| Republic of Serbia | 14.8 (14.4–15.2) | 18.0 (17.6–18.5) | 3.4 (3.2–3.6) | 1.0 (0.9–1.1) | 9.5 (9.3–9.6) |
| Vojvodina | 13.2 (12.5–13.9) | 10.6 (9.9–11.2) | 2.8 (2.4–3.1) | 0.7 (0.5–0.8) | 7.0 (6.7–7.2) |
| Central Serbia | 15.4 (14.9–15.9) | 20.7(20.2–21.2) | 3.6(3.3–3.8) | 1.2(1.0–1.3) | 10.4(10.2–10.6) |
| Average Sex-specific Incidence (95% CI) 1 | |||||
| Male | 16.5 (15.9–17.1) | 22 (21.3–22.7) | 3.8 (3.5–4.1) | 1.1 (1.0–1.3) | 11.0 (10.8–11.3) |
| Female | 13.2 (12.7–13.7) | 14.3 (13.7–14.8) | 3.0 (2.7–3.2) | 1.0 (0.8–1.1) | 8.0 (7.8–8.2) |
| Subperiod (Years) | Hepatitis A Outbreaks n (%) | Outbreaks per Transmission Route | Overall Hepatitis A Cases | Cases Reported in Outbreaks | Cases per Transmission Routes | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Contact | Foodborne | Waterborne | Contact | Foodborne | Waterborne | |||||||||||
| n | % 1 | n | % 1 | n | % 1 | n (%) | n | % 2 | n | % 3 | n | % 3 | n | % 3 | ||
| 2002–2006 | 174 (41.5) | 170 | 97.7 | 0 | 0 | 4 | 2.3 | 5524 (40.4) | 1252 | 22.7 | 1215 | 97.0 | 0 | 0 | 37 | 3.0 |
| 2007–2011 | 175 (41.8) | 171 | 97.7 | 1 | 0.6 | 3 | 1.7 | 6596 (48.2) | 1329 | 20.1 | 1305 | 98.2 | 14 | 1.0 | 10 | 0.8 |
| 2012–2016 | 56 (13.4) | 55 | 98.2 | 1 | 1.8 | 0 | 0 | 1196 (8.7) | 363 | 30.4 | 361 | 99.4 | 2 | 3.6 | 0 | 0 |
| 2017–2021 | 14 (3.3) | 14 | 100 | 0 | 0 | 0 | 0 | 363 (2.7) | 46 | 12.7 | 46 | 100 | 0 | 0 | 0 | 0 |
| Total | 419 (100) | 410 | 97.8 | 2 | 0.5 | 7 | 1.7 | 13,679 (100) | 2990 | 21.9 | 2927 | 97.9 | 16 | 0.5 | 47 | 1.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medić, S.; Anastassopoulou, C.; Pustahija, T.; Petrović, V.; Dragnić, N.; Boufidou, F.; Tsakris, A.; Šaponjić, V. Epidemiological Transition and Strategies for the Control of Hepatitis A in Serbia. Viruses 2023, 15, 753. https://doi.org/10.3390/v15030753
Medić S, Anastassopoulou C, Pustahija T, Petrović V, Dragnić N, Boufidou F, Tsakris A, Šaponjić V. Epidemiological Transition and Strategies for the Control of Hepatitis A in Serbia. Viruses. 2023; 15(3):753. https://doi.org/10.3390/v15030753
Chicago/Turabian StyleMedić, Snežana, Cleo Anastassopoulou, Tatjana Pustahija, Vladimir Petrović, Nataša Dragnić, Fotini Boufidou, Athanasios Tsakris, and Vladan Šaponjić. 2023. "Epidemiological Transition and Strategies for the Control of Hepatitis A in Serbia" Viruses 15, no. 3: 753. https://doi.org/10.3390/v15030753
APA StyleMedić, S., Anastassopoulou, C., Pustahija, T., Petrović, V., Dragnić, N., Boufidou, F., Tsakris, A., & Šaponjić, V. (2023). Epidemiological Transition and Strategies for the Control of Hepatitis A in Serbia. Viruses, 15(3), 753. https://doi.org/10.3390/v15030753