
Longitudinal Analysis of Antibody Response Following SARS-CoV-2 Infection Depending on Disease Severity: A Prospective Cohort Study

 , ,
, ,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Measurement of Immune Responses
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
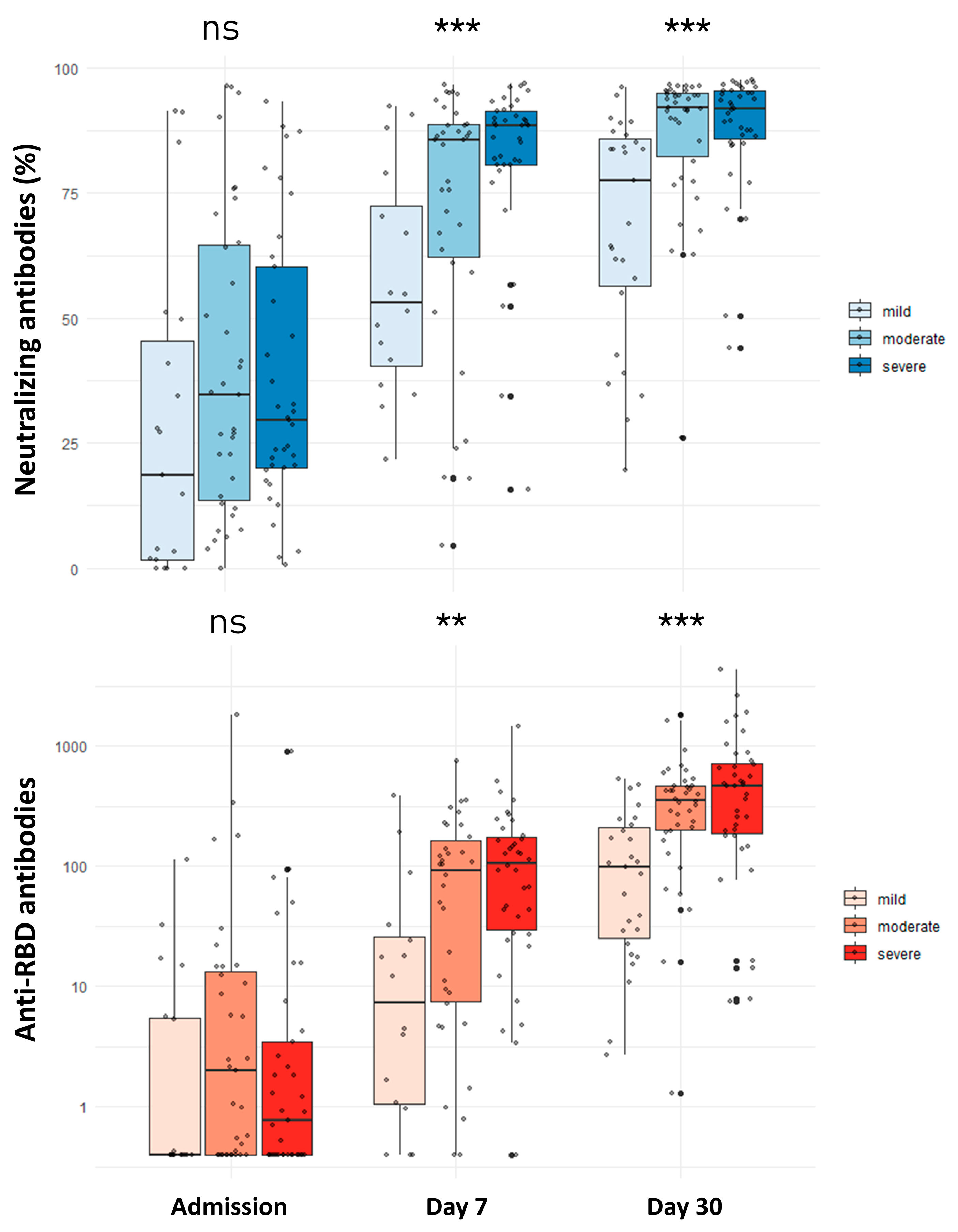
3.2. Antibody Levels before Vaccination
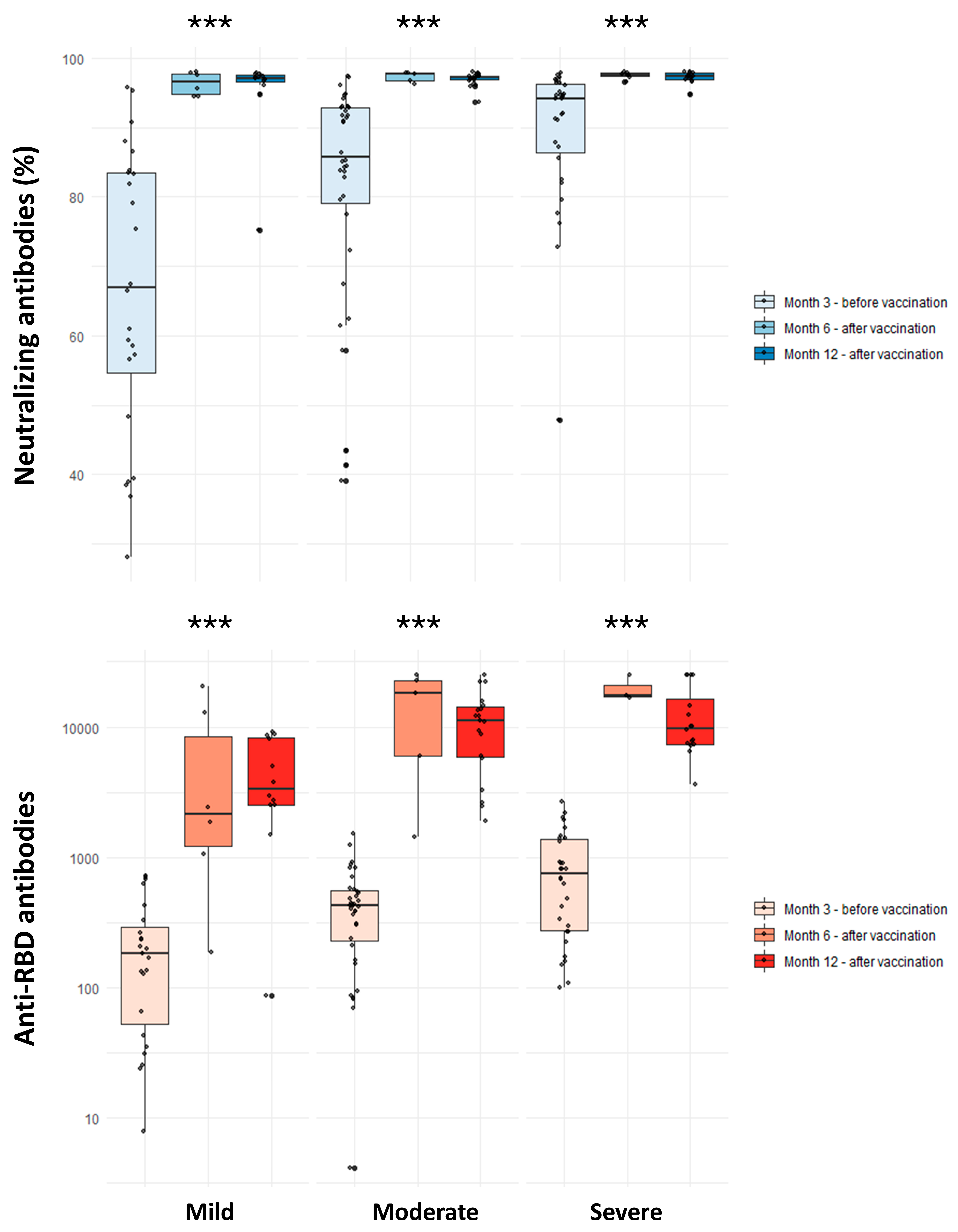
3.3. Antibody Levels after Vaccination
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, C.; Liu, X.; Chen, Q.; Sun, Y.; Su, Y.; Huang, S.; Wu, T.; Xia, N. Protection Duration of COVID-19 Vaccines: Waning Effectiveness and Future Perspective. Front. Microbiol. 2022, 13, 828806. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Karalis, V.; Ntanasis-Stathopoulos, I.; Apostolakou, F.; Gumeni, S.; Gavriatopoulou, M.; Papadopoulos, D.; Malandrakis, P.; Papanagnou, E.D.; Korompoki, E.; et al. Sustained but Declining Humoral Immunity Against SARS-CoV-2 at 9 Months Postvaccination With BNT162b2: A Prospective Evaluation in 309 Healthy Individuals. HemaSphere 2021, 6, E677. [Google Scholar] [CrossRef] [PubMed]
- Devasundaram, S.; Terpos, E.; Rosati, M.; Ntanasis-Stathopoulos, I.; Bear, J.; Burns, R.; Skourti, S.; Malandrakis, P.; Trougakos, I.P.; Dimopoulos, M.A.; et al. XBB.1.5 neutralizing antibodies upon bivalent COVID-19 vaccination are similar to XBB but lower than BQ.1.1. Am. J. Hematol. 2023, 98, E123–E126. [Google Scholar] [CrossRef]
- Rosati, M.; Terpos, E.; Agarwal, M.; Karalis, V.; Bear, J.; Burns, R.; Hu, X.; Papademetriou, D.; Ntanasis-Stathopoulos, I.; Trougakos, I.P.; et al. Distinct neutralization profile of spike variants by antibodies induced upon SARS-CoV-2 infection or vaccination. Am. J. Hematol. 2022, 97, E3. [Google Scholar] [CrossRef]
- Asteris, P.G.; Kokoris, S.; Gavriilaki, E.; Tsoukalas, M.Z.; Houpas, P.; Paneta, M.; Koutzas, A.; Argyropoulos, T.; Alkayem, N.F.; Armaghani, D.J.; et al. Early prediction of COVID-19 outcome using artificial intelligence techniques and only five laboratory indices. Clin. Immunol. 2023, 246, 109218. [Google Scholar] [CrossRef]
- Sattar, N.; Valabhji, J. Obesity as a Risk Factor for Severe COVID-19: Summary of the Best Evidence and Implications for Health Care. Curr. Obes. Rep. 2021, 10, 282. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Zhang, J.-J.; Dong, X.; Dong, X.; Liu, G.-H.; Liu, G.-H.; Gao, Y.-D.; Gao, Y.-D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The immunology and immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Gil-Etayo, F.J.; Suàrez-Fernández, P.; Cabrera-Marante, O.; Arroyo, D.; Garcinuño, S.; Naranjo, L.; Pleguezuelo, D.E.; Allende, L.M.; Mancebo, E.; Lalueza, A.; et al. T-Helper Cell Subset Response Is a Determining Factor in COVID-19 Progression. Front. Cell. Infect. Microbiol. 2021, 11, 624483. [Google Scholar] [CrossRef]
- Filippatos, C.; Ntanasis-Stathopoulos, I.; Sekeri, K.; Ntanasis-Stathopoulos, A.; Gavriatopoulou, M.; Psaltopoulou, T.; Dounias, G.; Sergentanis, T.N.; Terpos, E. Convalescent Plasma Therapy for COVID-19: A Systematic Review and Meta-Analysis on Randomized Controlled Trials. Viruses 2023, 15, 765. [Google Scholar] [CrossRef] [PubMed]
- Pappa, V.; Bouchla, A.; Terpos, E.; Thomopoulos, T.P.; Rosati, M.; Stellas, D.; Antoniadou, A.; Mentis, A.; Papageorgiou, S.G.; Politou, M.; et al. A Phase II Study on the Use of Convalescent Plasma for the Treatment of Severe COVID-19- A Propensity Score-Matched Control Analysis. Microorganisms 2021, 9, 806. [Google Scholar] [CrossRef] [PubMed]
- Nasrollahi, H.; Talepoor, A.G.; Saleh, Z.; Eshkevar Vakili, M.; Heydarinezhad, P.; Karami, N.; Noroozi, M.; Meri, S.; Kalantar, K. Immune responses in mildly versus critically ill COVID-19 patients. Front. Immunol. 2023, 14, 1077236. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Kitagawa, Y.; Tabata, S.; Kubota, K.; Nagura-Ikeda, M.; Matsuoka, M.; Miyoshi, K.; Sakai, J.; Ishibashi, N.; Tarumoto, N.; et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J. Med. Virol. 2021, 93, 3211. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Politou, M.; Sergentanis, T.N.; Mentis, A.; Rosati, M.; Stellas, D.; Bear, J.; Hu, X.; Felber, B.K.; Pappa, V.; et al. Anti-SARS-CoV-2 Antibody Responses in Convalescent Plasma Donors Are Increased in Hospitalized Patients; Subanalyses of a Phase 2 Clinical Study. Microorganisms 2020, 8, 1885. [Google Scholar] [CrossRef]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A Prediction Rule to Identify Low-Risk Patients with Community-Acquired Pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.D.; Bagratuni, T.; Liacos, C.I.; et al. Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical notes for clinical researchers: Chi-squared test and Fisher’s exact test. Restor. Dent. Endod. 2017, 42, 152. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Cha, M.J.; Choi, H.; Kim, M.-C.; Chung, J.-W.; Lee, K.-S.; Jeong, D.G.; Baek, M.S.; Kim, W.-Y.; Lim, Y.; et al. Relationship between SARS-CoV-2 antibody titer and the severity of COVID-19. J. Microbiol. Immunol. Infect. 2022, 55, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, M.C.; Ramonell, R.P.; Nguyen, D.C.; Cashman, K.S.; Saini, A.S.; Haddad, N.S.; Ley, A.M.; Kyu, S.; Howell, J.C.; Ozturk, T.; et al. Extrafollicular B cell responses correlate with neutralizing antibodies and morbidity in COVID-19. Nat. Immunol. 2020, 21, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Beltran, W.F.; Lam, E.C.; Astudillo, M.G.; Yang, D.; Miller, T.E.; Feldman, J.; Hauser, B.M.; Caradonna, T.M.; Clayton, K.L.; Nitido, A.D.; et al. COVID-19-neutralizing antibodies predict disease severity and survival. Cell 2021, 184, 476–488.e11. [Google Scholar] [CrossRef]
- Hendriks, J.; Schasfoort, R.; Koerselman, M.; Dannenberg, M.; Cornet, A.D.; Beishuizen, A.; van der Palen, J.; Krabbe, J.; Mulder, A.H.L.; Karperien, M. High Titers of Low Affinity Antibodies in COVID-19 Patients Are Associated With Disease Severity. Front. Immunol. 2022, 13, 867716. [Google Scholar] [CrossRef]
- Ravichandran, S.; Lee, Y.; Grubbs, G.; Coyle, E.M.; Klenow, L.; Akasaka, O.; Koga, M.; Adachi, E.; Saito, M.; Nakachi, I.; et al. Longitudinal antibody repertoire in “mild” versus “severe” COVID-19 patients reveals immune markers associated with disease severity and resolution. Sci. Adv. 2021, 7, eabf2467. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Coyle, P.; Malek, J.A.; Ahmed, A.A.; Mohamoud, Y.A.; Younuskunju, S.; Ayoub, H.H.; Al Kanaani, Z.; Al Kuwari, E.; et al. SARS-CoV-2 antibody-positivity protects against reinfection for at least seven months with 95% efficacy. EClinicalMedicine 2021, 35, 100861. [Google Scholar] [CrossRef]
- Egbert, E.R.; Xiao, S.; Colantuoni, E.; Caturegli, P.; Gadala, A.; Milstone, A.M.; Debes, A.K. Durability of Spike Immunoglobin G Antibodies to SARS-CoV-2 Among Health Care Workers With Prior Infection. JAMA Netw. Open. 2021, 4, e2123256. [Google Scholar] [CrossRef]
- Pradenas, E.; Trinité, B.; Urrea, V.; Marfil, S.; Ávila-Nieto, C.; de la Concepción, M.L.R.; Tarrés-Freixas, F.; Pérez-Yanes, S.; Rovirosa, C.; Ainsua-Enrich, E.; et al. Stable neutralizing antibody levels 6 months after mild and severe COVID-19 episodes. Med 2021, 2, 313. [Google Scholar] [CrossRef]
- Turner, J.S.; Kim, W.; Kalaidina, E.; Goss, C.W.; Rauseo, A.M.; Schmitz, A.J.; Hansen, L.; Haile, A.; Klebert, M.K.; Pusic, I.; et al. SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans. Nature 2021, 595, 421–425. [Google Scholar] [CrossRef]
- Feikin, D.R.; Feikin, D.R.; Higdon, M.M.; Higdon, M.M.; Abu-Raddad, L.J.; Abu-Raddad, L.J.; Andrews, N.; Andrews, N.; Araos, R.; Araos, R.; et al. Duration of effectiveness of vaccines against SARS-CoV-2 infection and COVID-19 disease: Results of a systematic review and meta-regression. Lancet 2022, 399, 924. [Google Scholar] [CrossRef] [PubMed]
- Dulipsingh, L.; Schaefer, E.J.; Wakefield, D.; Williams, K.; Halilovic, A.; Crowell, R. Comparing SARS-CoV-2 neutralizing antibody levels in convalescent unvaccinated, convalescent vaccinated, and naive vaccinated subjects. Heliyon 2023, 9, e17410. [Google Scholar] [CrossRef]
- Keeshan, A.; Galipeau, Y.; Heiskanen, A.; Collins, E.; McCluskie, P.S.; Arnold, C.; Saginur, R.; Booth, R.; Little, J.; McGuinty, M.; et al. Results of the Stop the Spread Ottawa (SSO) cohort study: A Canadian urban-based prospective evaluation of antibody responses and neutralisation efficiency to SARS-CoV-2 infection and vaccination. BMJ Open 2023, 13, e077714. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zein, J.; Ji, X.; Lin, D.-Y. Impact of Vaccination, Prior Infection, and Therapy on Omicron Infection and Mortality. J. Infect. Dis. 2023, 227, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Herzel, E.; Alapi, H.; Cohen, D.; Muhsen, K.; et al. The Incidence of SARS-CoV-2 Reinfection in Persons With Naturally Acquired Immunity With and Without Subsequent Receipt of a Single Dose of BNT162b2 Vaccine: A Retrospective Cohort Study. Ann. Intern. Med. 2022, 175, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Hammerman, A.; Sergienko, R.; Friger, M.; Beckenstein, T.; Peretz, A.; Netzer, D.; Yaron, S.; Arbel, R. Effectiveness of the BNT162b2 Vaccine after Recovery from COVID-19. N. Engl. J. Med. 2022, 386, 1221–1229. [Google Scholar] [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after Covid-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef]
- Dehgani-Mobaraki, P.; Wang, C.; Floridi, A.; Floridi, E.; Dawoodi, S.; Zaidi, A.K. Long-term persistence of IgG antibodies in recovered COVID-19 individuals at 18 months post-infection and the impact of two-dose BNT162b2 (Pfizer-BioNTech) mRNA vaccination on the antibody response: Analysis using fixed-effects linear regression model. Virology 2023, 578, 111–116. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variable | Overall (N = 106) | COVID-19 Severity | |||
|---|---|---|---|---|---|
| Mild (N = 28) | Moderate (N = 38) | Severe (N = 40) | p-Value | ||
| Age (years) | 52 [42.3–59] | 42.5 [32–53] | 53 [45.3–59] | 56 [50–59.5] | 0.001 a |
| Male sex | 71 (67.0) | 15 (53.6) | 25 (65.8) | 31 (77.5) | 0.116 b |
| Caucasian ethnicity | 97 (91.5) | 26 (92.9) | 35 (92.1) | 36 (90.0) | 1 b |
| Hypertension | 24 (22.6) | 5 (17.9) | 7 (18.4) | 12 (30.0) | 0.370 b |
| Diabetes mellitus | 15 (14.2) | 1 (3.6) | 2 (5.3) | 12 (30.0) | 0.002 c |
| Dyslipidemia | 29 (27.4) | 3 (10.7) | 12 (31.6) | 14 (35.0) | 0.067 c |
| Heart disease | 8 (7.5) | 1 (3.6) | 1 (2.6) | 6 (15.0) | 0.106 c |
| Respiratory disease | 12 (11.3) | 1 (3.6) | 3 (7.9) | 8 (20.0) | 0.104 c |
| Malignancy | 1 (0.9) | 0 (0.0) | 0 (0.0) | 1 (2.5) | 1 c |
| Charlson Comorbidity Index | 1 [0–2] | 0 [0–1] | 1 [0–2] | 2 [1–2.25] | 0.003 a |
| Obesity | 34 (32.1) | 3 (10.7) | 12 (31.6) | 19 (47.5) | 0.006 c |
| Smoking | |||||
| Former | 35 (33.0) | 3 (10.7) | 16 (42.1) | 16 (40.0) | 0.036 c |
| Current | 10 (9.4) | 3 (10.7) | 4 (10.5) | 3 (7.5) | |
| Days from symptom onset | 10 [8–13] | 8.5 [7.8–12] | 11 [8–13] | 10 [8–13] | 0.477 a |
| Fever | 101 (95.3) | 23 (82.1) | 38 (100) | 40 (100) | <0.001 b |
| Cough | 71 (67.0) | 16 (57.1) | 27 (71.1) | 28 (70.0) | 0.433 b |
| Dyspnea | 25 (23.6) | 3 (10.7) | 5 (13.2) | 17 (42.5) | 0.002 b |
| Chest pain | 16 (15.1) | 6 (21.4) | 6 (15.8) | 4 (10.0) | 0.430 c |
| Anosmia/Ageusia | 23 (21.7) | 5 (17.9) | 5 (13.2) | 13 (32.5) | 0.099 b |
| Diarrhea | 24 (22.6) | 6 (21.4) | 7 (18.4) | 11 (27.5) | 0.622 b |
| PSI/PORT score | 68 [51–78] | 52 [41.5–67.5] | 66.5 [47.5–74] | 78 [60.75–89.5] | <0.001 a |
| Remdesivir | 84 (79.2) | 11 (39.3) | 34 (89.5) | 39 (97.5) | <0.001 b |
| Corticosteroids | 80 (75.5) | 5 (17.9) | 35 (92.1) | 40 (100) | <0.001 b |
| Antibiotics | 57 (53.8) | 5 (17.9) | 23 (60.5) | 29 (72.5) | <0.001 b |
| Hospital stay (days) | 11 [7–14] | 6 [5,6] | 10 [7.25–11] | 14 [12–19.5] | <0.001 a |
| ICU admission | 6 (5.7) | 0 (0.0) | 0 (0.0) | 6 (15.0) | 0.006 c |
| Mechanical ventilation | 4 (3.8) | 0 (0.0) | 0 (0.0) | 4 (10.0) | 0.037 c |
| Death | 2 (1.9) | 0 (0.0) | 0 (0.0) | 2 (5.0) | 0.334 c |
| Vaccination | 58 (54.7) | 15 (53.6) | 23 (60.5) | 20 (50.0) | 0.640 b |
| 1st dose | 50 (47.2) | 11 (39.3) | 23 (60.5) | 16 (40.0) | 0.078 c |
| 2nd dose | 8 (7.5) | 4 (14.3) | 0 (0.0) | 4 (10.0) | |
| Type of vaccine | |||||
| BNT162b2 | 48 (45.3) | 14 (50.0) | 19 (50.0) | 15 (37.5) | 0.133 c |
| mRNA-1273 | 7 (6.6) | 0 (0.0) | 4 (10.5) | 3 (7.5) | |
| ChAdOx1 | 2 (1.9) | 0 (0.0) | 0 (0.0) | 2 (5.0) | |
| Ad26.COV2-S | 1 (0.9) | 1 (3.6) | 0 (0.0) | 0 (0.0) | |
| Time from infection (months) | 6.4 [5.7–6.8] | 5.9 [5.0–6.5] | 6.5 [5.9–7.6] | 6.4 [5.7–6.8] | 0.162 a |
| Outcome | Overall | COVID-19 Severity | |||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | p-Value | ||
| Neutralizing antibodies without vaccination | |||||
| Admission | 28.01 [13.95–58.64] | 18.65 [1.69–45.32] N = 11 | 34.57 [13.49–64.49] N = 35 | 29.63 [20.02–60.32] N = 37 | 0.190 |
| Day 7 | 84.85 [60.51–89.76] | 53.18 [40.32–72.46] N = 16 | 85.54 [62.27–88.71] N = 35 | 88.47 [80.69–91.48] N = 37 | 0.001 |
| Day 30 | 89.38 [77.49–94.65] | 77.56 [56.45–85.92] N = 27 | 92.00 [82.33–95.01] N = 38 | 91.90 [85.81–95.44] N = 39 | <0.001 |
| Month 3 | 86.40 [74.03–94.23] | 66.92 [54.56–83.56] N = 24 | 85.80 [79.09–92.86] N = 36 | 94.21 [86.46–96.28] N = 31 | <0.001 |
| Month 6 | 80.80 [69.93–90.89] | 75.96 [64.18–89.02] N = 19 | 78.13 [62.82–89.89] N = 19 | 90.23 [76.65–94.27] N = 24 | 0.026 |
| Month 12 | 73.35 [46.90–87.03] | 14.6 [14.6–14.6] N = 1 | 90.05 [81.89–96.35] N = 4 | 49.72 [44.08–60.43] N = 3 | 0.054 |
| Anti-RBD antibodies without vaccination | |||||
| Admission | 0.73 [0.40–8.38] | 0.40 [0.40–5.46] N = 18 | 2.00 [0.40–13.39] N = 35 | 0.76 [0.40–3.48] N = 37 | 0.160 |
| Day 7 | 67.62 [8.49–162.23] | 8.26 [1.05–25.92] N = 16 | 93.00 [7.55–165.03] N = 34 | 106.15 [29.89–173.70] N = 38 | 0.004 |
| Day 30 | 277.25 [104.36–499.73] | 99.13 [25.54–207.95] N = 27 | 352.55 [197.57–462.73] N = 38 | 463.90 [186.90–717.75] N = 39 | <0.001 |
| Month 3 | 419.40 [169.30–711.50] | 181.80 [54.23–294.80] N = 23 | 426.95 [230.10–550.65] N = 36 | 747.05 [276.20–1381.00] N = 30 | <0.001 |
| Month 6 | 417.75 [184.68–662.60] | 348.60 [177.05–631.35] N = 19 | 414.10 [219.40–532.70] N = 29 | 558.30 [256.07–1141.50] N = 24 | 0.151 |
| Month 12 | 518.60 [130.36–1271.28] | 4339.36 [2193.04–6485.86] N = 2 | 542.4 [518.6–1914.2] N = 3 | 158.1 [102.61–378.90] N = 3 | 0.707 |
| Neutralizing antibodies after vaccination | |||||
| Month 6 | 97.59 [96.72–97.85] | 96.59 [94.76–97.77] N = 6 | 97.81 [96.82–97.86] N = 5 | 97.59 [97.42–97.86] N = 7 | 0.584 |
| Month 12 | 97.32 [96.88–97.62] | 97.11 [96.65–97.52] N = 12 | 97.33 [96.89–97.47] N = 20 | 97.37 [96.98–97.85] N = 15 | 0.496 |
| Anti-RBD antibodies after vaccination | |||||
| Month 6 | 14,858 [19–839,839–2008] | 2150 [10–252,252–1263] N = 6 | 18,262 [22–550,550–5982] N = 5 | 17,367 [17,21–114,184] N = 3 | 0.140 |
| Month 12 | 8800 [4392.5–12,912] | 3379 [2532–8198.5] N = 12 | 11,107 [14–206,206–5846] N = 9 | 9816 [17–68,68–7392] N = 16 | 0.004 |
| Outcome | Unadjusted Model | Age- and Sex-Adjusted Model | Fully Adjusted Model | |||
|---|---|---|---|---|---|---|
| Moderate Disease | Severe Disease | Moderate Disease | Severe Disease | Moderate Disease | Severe Disease | |
| Neutralizing antibodies | ||||||
| Admission | 11.32 (−5.31; 27.94) | 9.60 (−6.87; 26.07) | 8.18 (−9.63; 25.99) | 5.27 (−13.10; 23.64) | 6.69 (−12.05; 25.42) R2: 0.04 | 4.46 (−15.02; 23.95) |
| Day 7 | 14.87 (1.68; 28.05) | 25.54 (12.47; 38.61) | 13.03 (−0.81; 26.87) | 22.99 (8.66; 37.32) | 11.07 (−3.19; 25.32) R2: 0.21 | 23.02 (8.17; 37.88) |
| Day 30 | 18.13 (10.15; 26.11) | 19.58 (11.65; 27.52) | 15.59 (7.33; 23.85) | 16.72 (8.12; 25.31) | 13.87 (6.05; 21.70) R2: 0.40 | 18.26 (9.87; 26.65) |
| 3rd month | 15.19 (6.89; 23.50) | 22.87 (14.30; 31.44) | 13.02 (4.47; 21.57) | 20.31 (11.11; 29.51) | 12.44 (3.96; 20.92) R2: 0.35 | 21.47 (12.04; 30.90) |
| Anti-RBD antibodies | ||||||
| Admission | 64.87 (−59.91; 189.65) | 22.69 (−100.94; 146.31) | 27.22 (−103.41; 157.85) | −28.84 (−163.41; 105.73) | 47.77 (−88.31; 183.85) R2: 0.07 | −7.97 (−149.80; 133.86) |
| Day 7 | 72.42 (−44.70; 189.53) | 112.10 (−3.02; 227.23) | 54.08 (−68.17; 176.34) | 85.67 (−68.17; 176.34) | 32.11 (−97.70; 161.94) R2: 0.07 | 69.43 (−63.93; 202.79) |
| Day 30 | 271.19 (−9.32; 551.69) | 525.61 (246.61; 804.62) | 197.80 (−97.00; 492.60) | 438.95 (132.25; 745.65) | 200.66 (−109.06; 510.38) R2: 0.15 | 427.35 (95.32; 759.37) |
| 3rd month | 215.16 (−35.42; 465.73) | 631.62 (371.46; 891.78) | 178.28 (−84.42; 440.48) | 586.61 (301.93; 870.69) | 159.83 (−113.65; 433.30) R2: 0.25 | 563.09 (257.02; 869.17) |
| Outcome | Unadjusted Model | Age- and Sex-Adjusted Model | Fully Adjusted Model | |||
|---|---|---|---|---|---|---|
| Moderate Disease | Severe Disease | Moderate Disease | Severe Disease | Moderate Disease | Severe Disease | |
| Neutralizing antibodies | ||||||
| Month 6 | 1.06 (−0.39; 2.41) | 1.23 (−0.06; 2.51) | 0.99 (−0.80; 2.77) | 1.16 (−0.43; 2.76) | 1.44 (−1.73; 4.62) R2: 0.50 | 1.50 (−1.29; 4.29) |
| Month 12 | 1.81 (−0.59; 4.22) | 2.05 (−0.50; 4.59) | 1.68 (−0.83; 4.18) | 1.93 (−0.81; 4.67) | 1.10 (−1.87; 4.07) R2: 0.17 | 1.04 (−2.23; 4.30) |
| Anti-RBD antibodies | ||||||
| Month 6 | 8186.33 (−3276.43; 19,649.10) | 13,280.67 (−104.96; 26,666.29) | 6291.59 (−9978.57; 22,561.76) | 11,820.99 (−4140.53; 27,782.52) | 6007.56 (−9479.11; 21,494.23) R2: 0.85 | 9686.75 (−5563.35; 24,936.86) |
| Month 12 | 6591.63 (1786.05; 11,397.21) | 8137.58 (3160.65; 13,114.50) | 6185.36 (1229.85; 11,140.87) | 7266.22 (1956.65; 12,575.80) | 5615.19 (657.92; 10,572.46) R2: 0.41 | 3900.99 (−1519.85; 9321.84) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zirou, C.; Gumeni, S.; Bellos, I.; Ntanasis-Stathopoulos, I.; Sklirou, A.D.; Bagratuni, T.; Korompoki, E.; Apostolakou, F.; Papassotiriou, I.; Trougakos, I.P.; et al. Longitudinal Analysis of Antibody Response Following SARS-CoV-2 Infection Depending on Disease Severity: A Prospective Cohort Study. Viruses 2023, 15, 2250. https://doi.org/10.3390/v15112250
Zirou C, Gumeni S, Bellos I, Ntanasis-Stathopoulos I, Sklirou AD, Bagratuni T, Korompoki E, Apostolakou F, Papassotiriou I, Trougakos IP, et al. Longitudinal Analysis of Antibody Response Following SARS-CoV-2 Infection Depending on Disease Severity: A Prospective Cohort Study. Viruses. 2023; 15(11):2250. https://doi.org/10.3390/v15112250
Chicago/Turabian StyleZirou, Christina, Sentiljana Gumeni, Ioannis Bellos, Ioannis Ntanasis-Stathopoulos, Aimilia D. Sklirou, Tina Bagratuni, Eleni Korompoki, Filia Apostolakou, Ioannis Papassotiriou, Ioannis P. Trougakos, and et al. 2023. "Longitudinal Analysis of Antibody Response Following SARS-CoV-2 Infection Depending on Disease Severity: A Prospective Cohort Study" Viruses 15, no. 11: 2250. https://doi.org/10.3390/v15112250
APA StyleZirou, C., Gumeni, S., Bellos, I., Ntanasis-Stathopoulos, I., Sklirou, A. D., Bagratuni, T., Korompoki, E., Apostolakou, F., Papassotiriou, I., Trougakos, I. P., & Terpos, E. (2023). Longitudinal Analysis of Antibody Response Following SARS-CoV-2 Infection Depending on Disease Severity: A Prospective Cohort Study. Viruses, 15(11), 2250. https://doi.org/10.3390/v15112250