

Biomarkers in a Cohort of HIV-Infected Patients Single- or Co-Infected with HTLV-1, HTLV-2, and/or HCV: A Cross-Sectional, Observational Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Population, Samples, Groups for Analysis and Data Collection
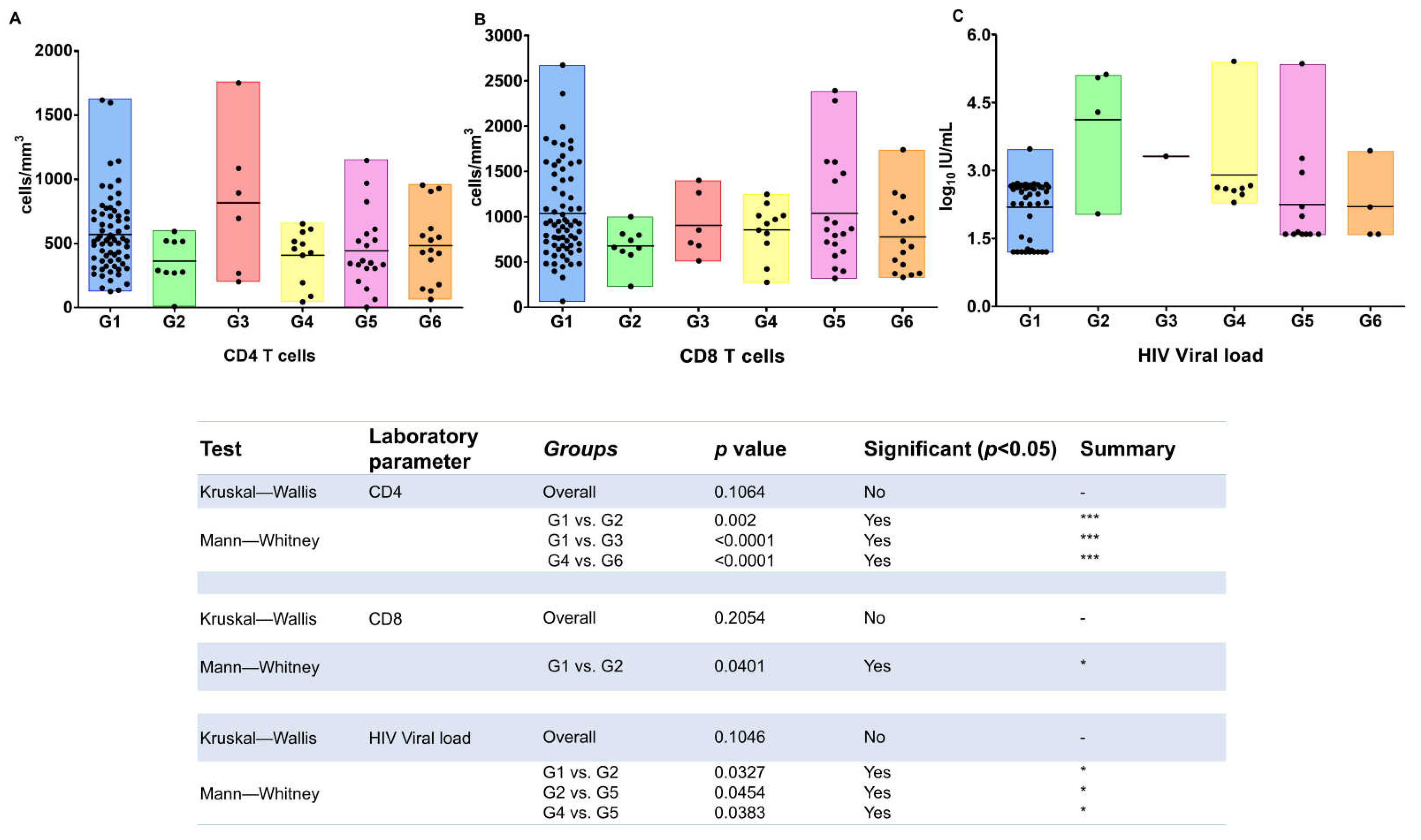
2.2. CD4+ and CD8+ T-Cells Immunophenotyping
2.3. HIV-1 Viral Load Quantification
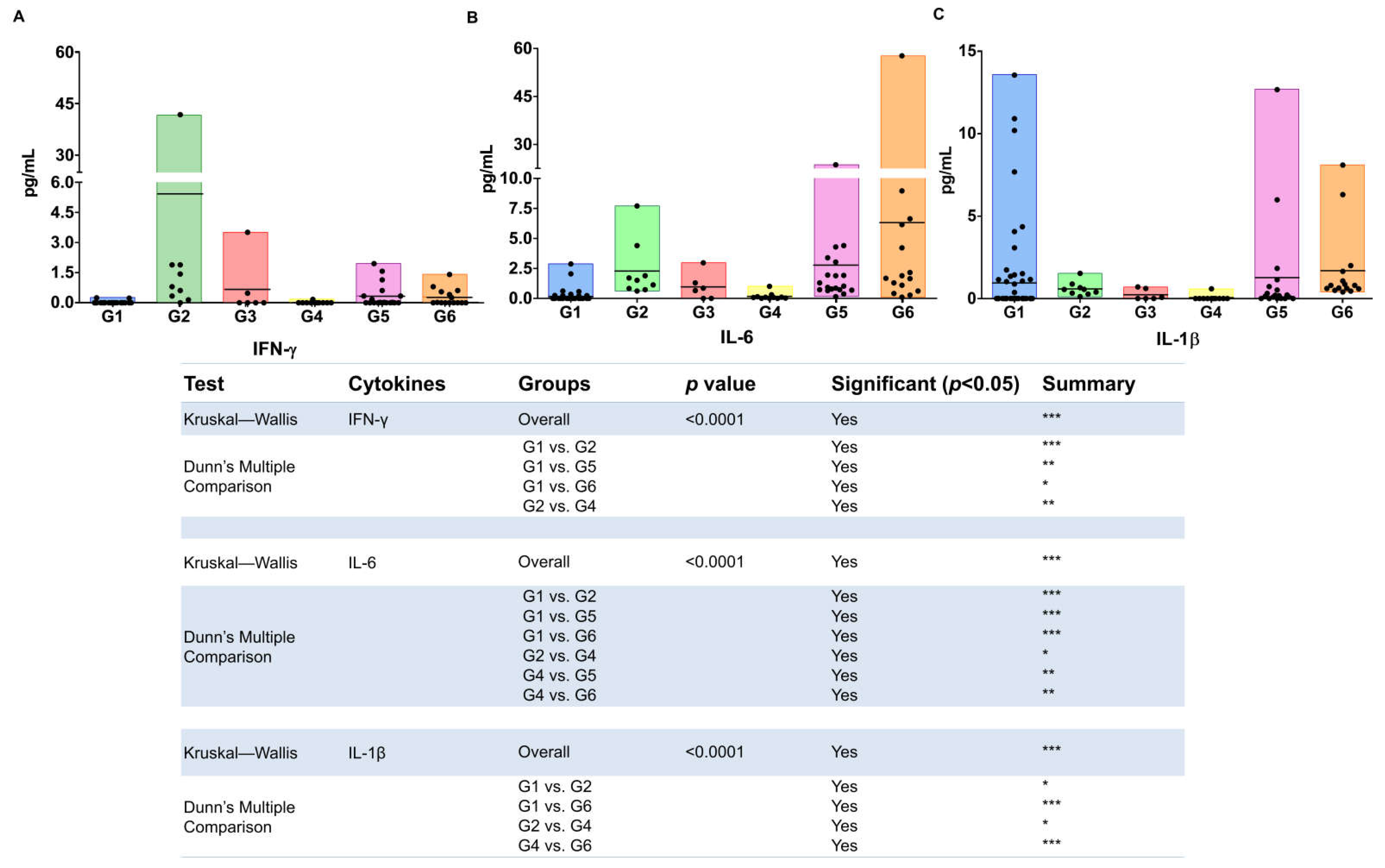
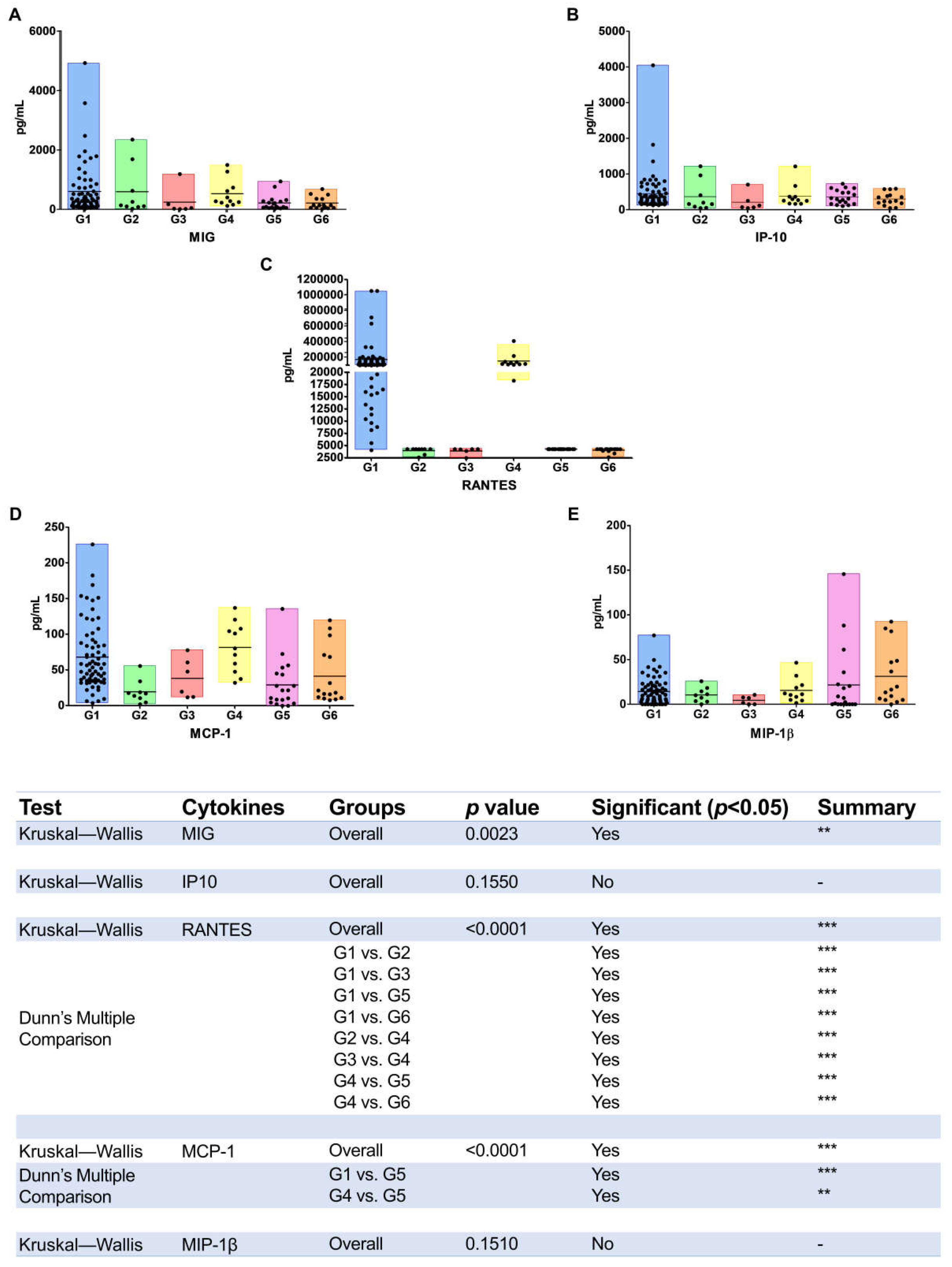
2.4. Cytokines and Chemokines Determination
2.5. Statistical Analyses
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gallo, R.C. The discovery of the first human retrovirus: HTLV-1 and HTLV. Retrovirology 2005, 2, 17. [Google Scholar] [CrossRef] [PubMed]
- Barre-Sinoussi, F.; Chermann, J.C.; Rey, F.; Nugeyre, M.T.; Chamaret, S.; Gruest, J.; Dauguet, C.; Axler-Blin, C.; Vézinet-Brun, F.; Rouzioux, C.; et al. Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS). Science 1983, 220, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Choo, Q.-L.; Kuo, G.; Weiner, A.J.; Overby, L.R.; Bradley, D.W.; Houghton, M. Isolation of a cDNA cLone Derived from a Blood-Borne Non-A, Non-B Viral Hepatitis Genome. Science 1989, 244, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Caterino-De-Araujo, A.; Sacchi, C.T.; Gonçalves, M.G.; Campos, K.; Magri, M.; Alencar, W.K.; the Group of Surveillance and Diagnosis of HTLV of São Paulo (GSuDiHTLV-SP). Current Prevalence and Risk Factors Associated with Human T Lymphotropic Virus Type 1 and Human T Lymphotropic Virus Type 2 Infections among HIV/AIDS Patients in São Paulo, Brazil. AIDS Res. Hum. Retrovir. 2015, 31, 543–549. [Google Scholar] [CrossRef]
- Caterino-de-Araujo, A.; Alves, F.A.; Campos, K.R.; Lemos, M.F.; Moreira, R.C. Making the invisible visible: Searching for human T-cell lymphotropic virus types 1 and 2 (HTLV-1 and HTLV-2) in Brazilian patients with viral hepatitis B and C. Mem. Inst. Oswaldo Cruz 2018, 113, 130–134. [Google Scholar] [CrossRef]
- Hisada, M.; Chatterjee, N.; Zhang, M.; Battjes, R.; Goedert, J. Increased Hepatitis C Virus Load among Injection Drug Users Infected with Human Immunodeficiency Virus and Human T Lymphotropic Virus Type II. J. Infect. Dis. 2003, 188, 891–897. [Google Scholar] [CrossRef][Green Version]
- Brites, C.; Sampaio, J.; Oliveira, A. HIV/human T-cell lymphotropic virus coinfection revisited: Impact on AIDS progression. AIDS Rev. 2009, 11, 8–16. Available online: https://www.aidsreviews.com/resumen.php?id=1030&indice=2009111&u=unp (accessed on 28 August 2009).
- Beilke, M.A. Retroviral Coinfections: HIV and HTLV: Taking Stock of More Than a Quarter Century of Research. AIDS Res. Hum. Retrovir. 2012, 28, 139–147. [Google Scholar] [CrossRef]
- Montaño-Castellón, I.; Marconi, C.S.C.; Saffe, C.; Brites, C. Clinical and Laboratory Outcomes in HIV-1 and HTLV-1/2 Coinfection: A Systematic Review. Front. Public Health 2022, 10, 820727. [Google Scholar] [CrossRef]
- Castro, E.; Roger, E. Hepatitis C virus/human T lymphotropic virus 1/2 co-infection: Regional burden and virological outcomes in people who inject drugs. World J. Virol. 2016, 5, 68–72. [Google Scholar] [CrossRef]
- Cardoso, D.F.; De Souza, F.V.; Fonseca, L.A.M.; Duarte, A.J.S.; Casseb, J. Influence of human T-cell lymphotropic virus type 1 (HTLV-1) infection on laboratory parameters of patients with chronic hepatitis C virus. Rev. Inst. Med. Trop. São Paulo 2009, 51, 325–329. [Google Scholar] [CrossRef][Green Version]
- Moreira, M.; Ramos, A.; Netto, E.M.; Brites, C. Characteristics of co-infections by HCV and HBV among Brazilian patients infected by HIV-1 and/or HTLV. Braz. J. Infect. Dis. 2013, 17, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Le Marchand, C.; Bahia, F.; Page, K.; Brites, C. Hepatitis C virus infection and spontaneous clearance in HTLV-1 and HIV co-infected patients in Salvador, Bahia, Brazil. Braz. J. Infect. Dis. 2015, 19, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Espíndola, O.M.; Vizzoni, A.G.; Lampe, E.; Andrada-Serpa, M.J.; Araújo, A.Q.C.; Leite, A.C.C. Hepatitis C virus and human T-cell lymphotropic virus type 1 co-infection: Impact on liver disease, virological markers, and neurological outcomes. Int. J. Infect. Dis. 2017, 57, 116–122. [Google Scholar] [CrossRef][Green Version]
- Boschi-Pinto, C.; Stuver, S.; Okayama, A.; Trichopoulos, D.; Orav, E.J.; Tsubouchi, H.; Mueller, N. A Follow-Up Study of Morbidity and Mortality Associated with Hepatitis C Virus Infection and Its Interaction with Human T Lymphotropic Virus Type I in Miyazaki, Japan. J. Infect. Dis. 2000, 181, 35–41. [Google Scholar] [CrossRef]
- Alves, F.A.; Campos, K.R.; Lemos, M.F.; Moreira, R.C.; Caterino-De-Araujo, A. Hepatitis C viral load in HCV-monoinfected and HCV/HIV-1-, HCV/HTLV-1/-2-, and/or HCV/HIV/HTLV-1/-2-co-infected patients from São Paulo, Brazil. Braz. J. Infect. Dis. 2018, 22, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Campos, K.R.; Alves, F.A.; Lemos, M.F.; Moreira, R.C.; Marcusso, R.M.N.; Caterino-De-Araujo, A. The reasons to include the serology of human T-lymphotropic virus types 1 and 2 (HTLV-1 and HTLV-2) in the clinical follow-up of patients with viral hepatitis B and C in Brazil. PLoS Negl. Trop. Dis. 2020, 14, e0008245. [Google Scholar] [CrossRef]
- Brites, C.; Abrahão, M.; Bozza, P.; Netto, E.M.; Lyra, A.; Bahia, F. Infection by HTLV-1 Is Associated with High Levels of Proinflammatory Cytokines in HIV-HCV–Coinfected Patients. JAIDS J. Acquir. Immune Defic. Syndr. 2018, 77, 230–234. [Google Scholar] [CrossRef]
- Oo, Z.; Barrios, C.S.; Castillo, L.; Beilke, M.A. High levels of CC-chemokine expression and downregulated levels of CCR5 during HIV-1/HTLV-1 and HIV-1/HTLV-2 coinfections. J. Med Virol. 2015, 87, 790–797. [Google Scholar] [CrossRef]
- Coelho-dos-Reis, J.G.A.; Passos, L.; Duarte, M.C.; Araújo, M.G.; Campi-Azevedo, A.C.; Teixeira-Carvalho, A.; Magalhāes, V.P.; Trindade, B.C.; Dias, R.S.; Martins, M.L.; et al. Immunological Profile of HTLV-1-Infected Patients Associated with Infectious or Autoimmune Dermatological Disorders. PLoS Negl. Trop. Dis. 2013, 7, e2328. [Google Scholar] [CrossRef]
- Rafatpanah, H.; Felegari, M.; Azarpazhooh, M.Z.; Vakili, R.; Rajaei, T.; Hampson, I.; Hassanshahi, G.; Valizadeh, N.; Gerayli, S.; Hamid, F.; et al. Altered expression of CXCR3 and CCR6 and their ligands in HTLV-1 carriers and HAM/TSP patients. J. Med. Virol. 2017, 89, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Abrahão, M.H.N.; Lima, R.G.; Netto, E.; Brites, C. Human Lymphotropic Virus Type 1 Coinfection Modulates the Synthesis of Cytokines by Peripheral Blood Mononuclear Cells from HIV Type 1-Infected Individuals. AIDS Res. Hum. Retrovir. 2012, 28, 806–808. [Google Scholar] [CrossRef]
- Caterino-de-Araujo, A.; Campos, K.R.; Petrucci, T.V.B.; Silva, R.X.; Lemos, M.F.; Moreira, R.C. Surveillance of human retroviruses in blood samples from patients with hepatitis B and C in São Paulo, Brazil. Rev. Soc. Bras. Med. Trop. 2020, 53, e20190378. [Google Scholar] [CrossRef] [PubMed]
- Bahia, F.; Novais, V.; Evans, J.; Marchand, C.L.; Netto, E.; Page, K.; Brites, C. The Impact of Human T-Cell Lymphotropic Virus I Infection on Clinical and Immunologic Outcomes in Patients Coinfected with HIV and Hepatitis C Virus. JAIDS J. Acquir. Immune Defic. Syndr. 2011, 57, S202–S207. [Google Scholar] [CrossRef] [PubMed]
- Chaves, D.G.; Sales, C.C.; Gonçalves, P.C.; Silva-Malta, M.C.F.; Romanelli, L.C.; Ribas, J.G.; Carneiro-Proietti, A.B.F.; Martins, M.L. Plasmatic proinflammatory chemokines levels are tricky markers to monitoring HTLV-1 carriers. J. Med. Virol. 2016, 88, 1438–1447. [Google Scholar] [CrossRef]
- Silva, M.C.; Silva, C.A.C.; Machado, G.U.; Atta, A.; Freire, S.M.; Carvalho, E.; Schinoni, M.I.; Paraná, R. HCV/HTLV coinfection: Does HTLV-1 interfere in the natural history of HCV-related diseases? J. Med. Virol. 2016, 88, 1967–1972. [Google Scholar] [CrossRef]
- Casoli, C.; Pilotti, E.; Bertazzoni, U. Molecular and cellular interactions of HIV-1/HTLV coinfection and impact on AIDS progression. AIDS Rev. 2007, 9, 140–149. Available online: https://www.aidsreviews.com/resultados_autor.php?Keyword=Casoli (accessed on 16 October 2018).
- Brites, C.; Miranda, F.; Luz, E.; Netto, E.M. Early and Successful Combination Antiretroviral Therapy Normalizes Survival Time in Patients Coinfected with Human Immunodeficiency Virus and Human T-cell Lymphotrophic Virus Type 1. Clin. Infect. Dis. 2020, 71, 196–200. [Google Scholar] [CrossRef]
- Ticona, E.; Huaman, M.A.; Yanque, O.; Zunt, J.R. HIV and HTLV-1 Coinfection: The Need to Initiate Antiretroviral Therapy. J. Int. Assoc. Provid. AIDS Care 2013, 12, 373–374. [Google Scholar] [CrossRef]
- Falconer, K.; Askarieh, G.; Weis, N.; Hellstrand, K.; Alaeus, A.; Lagging, M.; for the Dico Study Group. IP-10 predicts the first phase decline of HCV RNA and overall viral response to therapy in patients co-infected with chronic hepatitis C virus infection and HIV. Scand. J. Infect. Dis. 2010, 42, 896–901. [Google Scholar] [CrossRef]
- Freeman, M.L.; Shive, C.L.; Nguyen, T.P.; Younes, S.-A.; Panigrahi, S.; Lederman, M.M. Cytokines and T-Cell Homeostasis in HIV Infection. J. Infect. Dis. 2016, 214, S51–S57. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Narazaki, M.; Kishimoto, T. IL-6 in Inflammation, Immunity, and Disease. Cold Spring Harb. Perspect. Biol. 2014, 6, a016295. [Google Scholar] [CrossRef] [PubMed]
- Borges, Á.H.; O’Connor, J.L.; Phillips, A.N.; Neaton, J.D.; Grund, B.; Neuhaus, J.; Vjecha, M.J.; Calmy, A.; Koelsch, K.K.; Lundgren, J.D.; et al. Interleukin 6 Is a Stronger Predictor of Clinical Events Than High-Sensitivity C-Reactive Protein or D-Dimer during HIV Infection. J. Infect. Dis. 2016, 214, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Stacey, A.R.; Norris, P.J.; Qin, L.; Haygreen, E.A.; Taylor, E.; Heitman, J.; Lebedeva, M.; DeCamp, A.; Li, D.; Grove, D.; et al. Induction of a Striking Systemic Cytokine Cascade prior to Peak Viremia in Acute Human Immunodeficiency Virus Type 1 Infection, in Contrast to More Modest and Delayed Responses in Acute Hepatitis B and C Virus Infections. J. Virol. 2009, 83, 3719–3733. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Yin, X.; Shang, H.; Jiang, Y. IP-10 is highly involved in HIV infection. Cytokine 2019, 115, 97–103. [Google Scholar] [CrossRef]
- Jiao, Y.; Zhang, T.; Wang, R.; Zhang, H.; Huang, X.; Yin, J.; Zhang, L.; Xu, X.; Wu, H. Plasma IP-10 Is Associated with Rapid Disease Progression in Early HIV-1 Infection. Viral Immunol. 2012, 25, 333–337. [Google Scholar] [CrossRef]
- Ansari, A.W.W.; Schmidt, R.E.; Shankar, E.M.; Kamarulzaman, A. Immuno-pathomechanism of liver fibrosis: Targeting chemokine CCL2-mediated HIV:HCV nexus. J. Transl. Med. 2014, 12, 341. [Google Scholar] [CrossRef]
- Turci, M.; Pilotti, E.; Ronzi, P.; Magnani, G.; Boschini, A.; Parisi, S.G.; Zipeto, D.; Lisa, A.; Casoli, C.; Bertazzoni, U. Coinfection with HIV-1 and Human T-Cell Lymphotropic Virus Type II in Intravenous Drug Users Is Associated with Delayed Progression to AIDS. JAIDS J. Acquir. Immune Defic. Syndr. 2006, 41, 100–106. [Google Scholar] [CrossRef]
- Pilotti, E.; Elviri, L.; Vicenzi, E.; Bertazzoni, U.; Re, M.C.; Allibardi, S.; Poli, G.; Casoli, C. Postgenomic up-regulation of CCL3L1 expression in HTLV-2–infected persons curtails HIV-1 replication. Blood 2007, 109, 1850–1856. [Google Scholar] [CrossRef]
- Ruiz-Mateos, E.; Ruiz-León, M.J.; Tarancón-Díez, L.; Gutiérrez, C.; Dronda, F.; Domínguez-Molina, B.; Pérez-Elías, M.J.; Moreno, A.; Leal, M.; Moreno, S.; et al. High CD8 T cell percentage and HCV replication control are common features in HIV-1 controllers and HTLV-2-co-infected patients with a history of injection drug use. Virus Res. 2019, 264, 40–44. [Google Scholar] [CrossRef]
- Morgan, E.; Varro, R.; Sepulveda, H.; Ember, J.A.; Apgar, J.; Wilson, J.; Lowe, L.; Chen, R.; Shivraj, L.; Agadir, A.; et al. Cytometric bead array: A multiplexed assay platform with applications in various areas of biology. Clin. Immunol. 2004, 110, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Leng, S.X.; McElhaney, J.E.; Walston, J.D.; Xie, D.; Fedarko, N.S.; Kuchel, G.A. ELISA and Multiplex Technologies for Cytokine Measurement in Inflammation and Aging Research. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2008, 63, 879–884. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Groups | Age * (Years) | Sex | ||||
|---|---|---|---|---|---|---|
| Male | Female | CD4 ** | CD8 ** | HIV Viral Load ** | ||
| n (%) | n (%) | Cells/mm³ | Cells/mm³ | log10 IU/mL | ||
| G1 (n = 69) | 46.0 (31–65) | 39 (57.4) | 29 (42.6) | 571.6 (±296.5) a,b | 1034.0 (±510.6) d | 2.19 (±0.64) e |
| G2 (n = 9) | 48.2 (28–63) | 4 (44.5) | 5 (55.5) | 363.7 (±187.0) | 675.6 (±209.9) | 4.12 (±1.43) f |
| G3 (n = 6) | 46.2 (41–50) | 1 (16.7) | 5 (83.3) | 818.3 (±575.2) | 902.5 (±350.9) | 3.31 (0.00) *** |
| G4 (n = 11) | 48.2 (36–59) | 5 (45.4) | 6 (54.6) | 409.6 (±209.7) c | 851.9 (±291.7) | 2.90 (±1.02) g |
| G5 (n = 19) | 50.3 (42–66) | 12 (63.2) | 7 (36.8) | 444.7 (±293.7) | 1037.0 (±597.4) | 2.24 (±1.13) |
| G6 (n = 15) | 50.7 (43–61) | 8 (53.3) | 7 (46.7) | 484.3 (±287.7) | 774.8 (±414.5) | 2.20 (±0.87) |
| Cytokines and Chemokines * pg/mL | Groups | ||||||
|---|---|---|---|---|---|---|---|
| G1 (n = 69) | G2 (n = 9) | G3 (n = 6) | G4 (n = 11) | G5 (n = 19) | G6 (n = 15) | p ** | |
| IFN-γ | 0.01 | 5.42 | 0.66 | 0.02 | 0.33 | 0.27 | <0.0001 |
| (0.0–0.0) | (0.25–1.89) | (0.0–1.24) | (0.0–0.0) | (0.0–0.34) | (0.0–0.55) | ||
| IL-6 | 0.16 | 2.28 | 0.96 | 0.17 | 2.78 | 6.32 | <0.0001 |
| (0.02–0.14) | (0.78–3.15) | (0.0–1.72) | (0.01–0.14) | (0.73–3.04) | (0.62–6.15) | ||
| IL-1β | 0.95 | 0.59 | 0.23 | 0.05 | 1.27 | 1.69 | <0.0001 |
| (0.0–0.19) | (0.30–0.77) | (0.0–0.64) | (0.0–0.0) | (0.0–0.73) | (0.59–1.65) | ||
| MIG | 601.2 | 593.9 | 241.8 | 526.8 | 215.3 | 213.8 | 0.0023 |
| (125.9–722.4) | (89.23–1154) | (14.10–425.3) | (223.9–729.2) | (56.71–274.9) | (49.66–354.0) | ||
| IP-10 | 450.0 | 366.6 | 211.2 | 382.3 | 360.3 | 302.9 | 0.155 |
| (209.4–506.2) | (71.92–685.4) | (63.47–365.9) | (175.2–366.3) | (164.3–545.2) | (182.5–407.0) | ||
| MCP-1 | 68.12 | 19.55 | 38.45 | 81.82 | 29.24 | 41.44 | <0.0001 |
| (35.24–88.43) | (7.77–26.61) | (12.32–65.04) | (47.75–107.9) | (4.66–45.30) | (11.06–71.21) | ||
| MIP-1β | 14.32 | 10.45 | 4.51 | 15.61 | 21.66 | 31.32 | 0.151 |
| (3.53–21.35) | (3.33–16.41) | (0.0–8.47) | (4.95–21.57) | (0.0–22.38) | (4.98–48.76) | ||
| RANTES | 102549 | 4049 | 3996 | 82512 | 4366 | 4148 | <0.0001 |
| (20768–90364) | (3786–4366) | (3636–4366) | (34444–72660) | (4366–4366) | (4033–4366) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caterino-de-Araujo, A.; Campos, K.R.; Oliveira, L.M.S.; Rigato, P.O. Biomarkers in a Cohort of HIV-Infected Patients Single- or Co-Infected with HTLV-1, HTLV-2, and/or HCV: A Cross-Sectional, Observational Study. Viruses 2022, 14, 1955. https://doi.org/10.3390/v14091955
Caterino-de-Araujo A, Campos KR, Oliveira LMS, Rigato PO. Biomarkers in a Cohort of HIV-Infected Patients Single- or Co-Infected with HTLV-1, HTLV-2, and/or HCV: A Cross-Sectional, Observational Study. Viruses. 2022; 14(9):1955. https://doi.org/10.3390/v14091955
Chicago/Turabian StyleCaterino-de-Araujo, Adele, Karoline R. Campos, Luanda M. S. Oliveira, and Paula O. Rigato. 2022. "Biomarkers in a Cohort of HIV-Infected Patients Single- or Co-Infected with HTLV-1, HTLV-2, and/or HCV: A Cross-Sectional, Observational Study" Viruses 14, no. 9: 1955. https://doi.org/10.3390/v14091955
APA StyleCaterino-de-Araujo, A., Campos, K. R., Oliveira, L. M. S., & Rigato, P. O. (2022). Biomarkers in a Cohort of HIV-Infected Patients Single- or Co-Infected with HTLV-1, HTLV-2, and/or HCV: A Cross-Sectional, Observational Study. Viruses, 14(9), 1955. https://doi.org/10.3390/v14091955