
Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Updated Analysis Involving 22,607 Blood Donors Covering the Period October 2021 to April 2022

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Population
3.2. Seroprevalence of Anti-S IgG Antibodies by Time
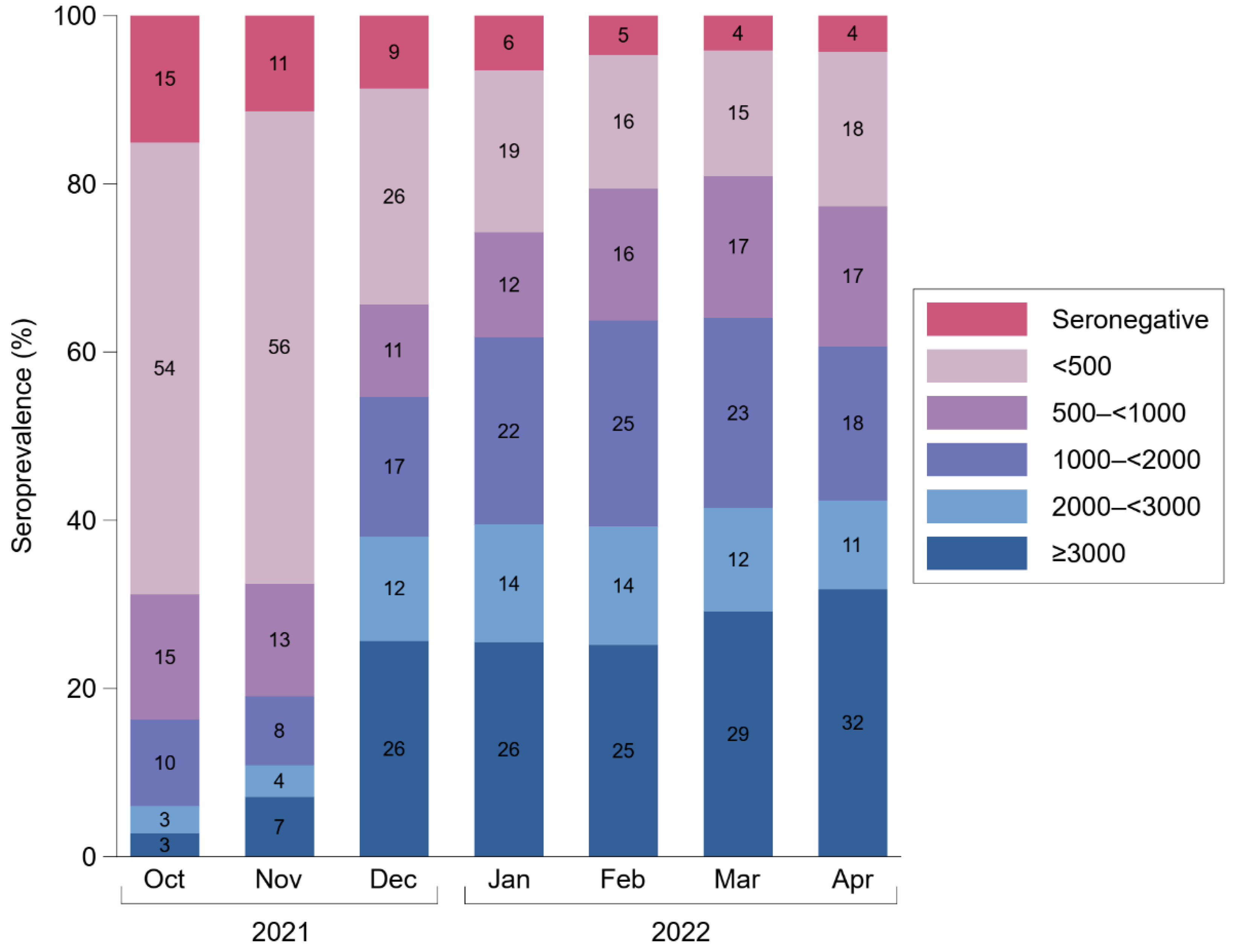
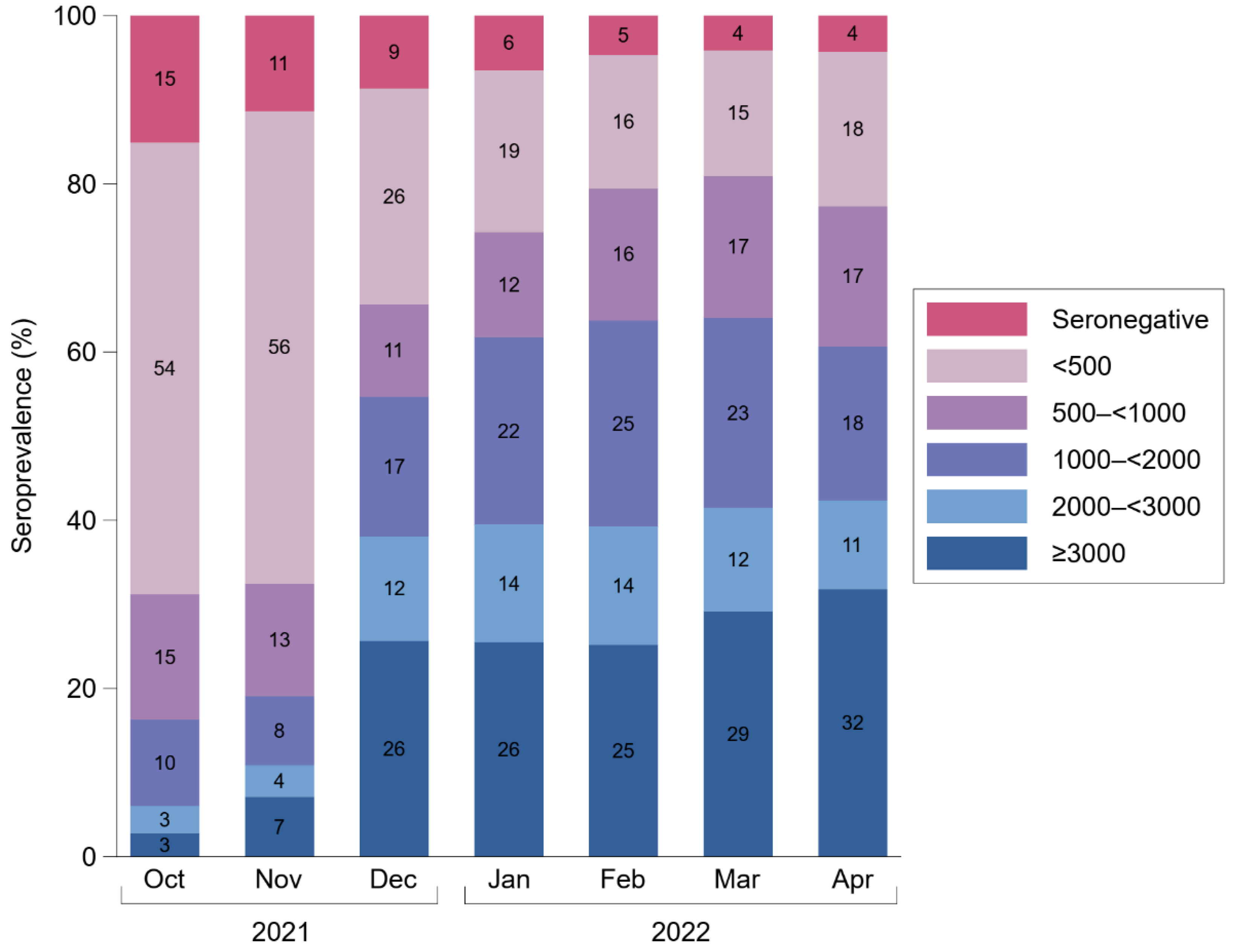
3.3. Anti-S IgG Antibody Levels
3.4. Cross-Sectional Correlates of Anti-S IgG Seroprevalence and Antibody Levels
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Seekircher, L.; Bánki, Z.; Kimpel, J.; Rössler, A.; Schäfer, H.; Falkensammer, B.; Bante, D.; Forer, L.; Schönherr, S.; Harthaller, T.; et al. Immune response to 2-dose BNT162b2 vaccination and risk of SARS-CoV-2 breakthrough infection: The Shieldvacc-2 study. medRxiv 2022. [Google Scholar] [CrossRef]
- Wei, J.; Pouwels, K.B.; Stoesser, N.; Matthews, P.C.; Diamond, I.; Studley, R.; Rourke, E.; Cook, D.; Bell, J.I.; Newton, J.N.; et al. Antibody responses and correlates of protection in the general population after two doses of the ChAdOx1 or BNT162b2 vaccines. Nat. Med. 2022, 28, 1072–1082. [Google Scholar] [CrossRef] [PubMed]
- Stærke, N.B.; Reekie, J.; Nielsen, H.; Benfield, T.; Wiese, L.; Knudsen, L.S.; Iversen, M.B.; Iversen, K.K.; Fogh, K.; Bodilsen, J.; et al. Levels of SARS-CoV-2 antibodies among fully vaccinated individuals with Delta or Omicron variant breakthrough infections. Nat. Commun. 2022, 13, 4466. [Google Scholar] [CrossRef] [PubMed]
- Lumley, S.F.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; Warren, F.; et al. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N. Engl. J. Med. 2021, 384, 533–540. [Google Scholar] [CrossRef]
- Gallais, F.; Gantner, P.; Bruel, T.; Velay, A.; Planas, D.; Wendling, M.-J.; Bayer, S.; Solis, M.; Laugel, E.; Reix, N.; et al. Evolution of antibody responses up to 13 months after SARS-CoV-2 infection and risk of reinfection. EBioMedicine 2021, 71, 103561. [Google Scholar] [CrossRef]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef]
- Campbell, F.; Archer, B.; Laurenson-Schafer, H.; Jinnai, Y.; Konings, F.; Batra, N.; Pavlin, B.; Vandemaele, K.; van Kerkhove, M.D.; Jombart, T.; et al. Increased transmissibility and global spread of SARS-CoV-2 variants of concern as at June 2021. Euro. Surveill. 2021, 26, 2100509. [Google Scholar] [CrossRef]
- Cao, Y.; Wang, J.; Jian, F.; Xiao, T.; Song, W.; Yisimayi, A.; Huang, W.; Li, Q.; Wang, P.; An, R.; et al. Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies. Nature 2022, 602, 657–663. [Google Scholar] [CrossRef]
- Lustig, Y.; Zuckerman, N.; Nemet, I.; Atari, N.; Kliker, L.; Regev-Yochay, G.; Sapir, E.; Mor, O.; Alroy-Preis, S.; Mendelson, E.; et al. Neutralising capacity against Delta (B.1.617.2) and other variants of concern following Comirnaty (BNT162b2, BioNTech/Pfizer) vaccination in health care workers, Israel. Euro. Surveill. 2021, 26, 2100557. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Nagelkerke, N.; Ayoub, H.; Coyle, P.; Tang, P.; YASSINE, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Hasan, M.R.; Al-Kanaani, Z.; et al. Duration of immune protection of SARS-CoV-2 natural infection against reinfection in Qatar. medRxiv 2022. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine 2021, 36, 100928. [Google Scholar] [CrossRef] [PubMed]
- Servellita, V.; Syed, A.M.; Morris, M.K.; Brazer, N.; Saldhi, P.; Garcia-Knight, M.; Sreekumar, B.; Khalid, M.M.; Ciling, A.; Chen, P.-Y.; et al. Neutralizing immunity in vaccine breakthrough infections from the SARS-CoV-2 Omicron and Delta variants. Cell 2022, 185, 1539–1548.e5. [Google Scholar] [CrossRef] [PubMed]
- Turelli, P.; Zaballa, M.-E.; Raclot, C.; Fenwick, C.; Kaiser, L.; Eckerle, I.; Pantaleo, G.; Guessous, I.; Stringhini, S.; Trono, D. Omicron infection induces low-level, narrow-range SARS-CoV-2 neutralizing activity. medRxiv 2022. [Google Scholar] [CrossRef]
- Horton, D.B.; Barrett, E.S.; Roy, J.; Gennaro, M.L.; Andrews, T.; Greenberg, P.; Bruiners, N.; Datta, P.; Ukey, R.; Velusamy, S.K.; et al. Determinants and Dynamics of SARS-CoV-2 Infection in a Diverse Population: 6-Month Evaluation of a Prospective Cohort Study. J. Infect. Dis. 2021, 224, 1345–1356. [Google Scholar] [CrossRef]
- Chia, W.N.; Zhu, F.; Ong, S.W.X.; Young, B.E.; Fong, S.-W.; Le Bert, N.; Tan, C.W.; Tiu, C.; Zhang, J.; Tan, S.Y.; et al. Dynamics of SARS-CoV-2 neutralising antibody responses and duration of immunity: A longitudinal study. Lancet Microbe. 2021, 2, e240–e249. [Google Scholar] [CrossRef]
- Evans, J.P.; Zeng, C.; Carlin, C.; Lozanski, G.; Saif, L.J.; Oltz, E.M.; Gumina, R.J.; Liu, S.-L. Neutralizing antibody responses elicited by SARS-CoV-2 mRNA vaccination wane over time and are boosted by breakthrough infection. Sci. Transl. Med. 2022, 14, eabn8057. [Google Scholar] [CrossRef]
- Liu, X.; Shaw, R.H.; Stuart, A.S.V.; Greenland, M.; Aley, P.K.; Andrews, N.J.; Cameron, J.C.; Charlton, S.; Clutterbuck, E.A.; Collins, A.M.; et al. Safety and immunogenicity of heterologous versus homologous prime-boost schedules with an adenoviral vectored and mRNA COVID-19 vaccine (Com-COV): A single-blind, randomised, non-inferiority trial. Lancet 2021, 398, 856–869. [Google Scholar] [CrossRef]
- van Gils, M.J.; Lavell, A.; van der Straten, K.; Appelman, B.; Bontjer, I.; Poniman, M.; Burger, J.A.; Oomen, M.; Bouhuijs, J.H.; van Vught, L.A.; et al. Antibody responses against SARS-CoV-2 variants induced by four different SARS-CoV-2 vaccines in health care workers in the Netherlands: A prospective cohort study. PLoS Med. 2022, 19, e1003991. [Google Scholar] [CrossRef]
- Parry, H.; Bruton, R.; Stephens, C.; Bentley, C.; Brown, K.; Amirthalingam, G.; Hallis, B.; Otter, A.; Zuo, J.; Moss, P. Extended interval BNT162b2 vaccination enhances peak antibody generation. NPJ Vaccines 2022, 7, 14. [Google Scholar] [CrossRef]
- Payne, R.P.; Longet, S.; Austin, J.A.; Skelly, D.T.; Dejnirattisai, W.; Adele, S.; Meardon, N.; Faustini, S.; Al-Taei, S.; Moore, S.C.; et al. Immunogenicity of standard and extended dosing intervals of BNT162b2 mRNA vaccine. Cell 2021, 184, 5699–5714.e11. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, B.; Lotan, R.; Kalkstein, N.; Peretz, A.; Perez, G.; Ben-Tov, A.; Chodick, G.; Gazit, S.; Patalon, T. Correlation of SARS-CoV-2-breakthrough infections to time-from-vaccine. Nat. Commun. 2021, 12, 6379. [Google Scholar] [CrossRef] [PubMed]
- Siller, A.; Wachter, G.A.; Neururer, S.; Pfeifer, B.; Astl, M.; Borena, W.; Kimpel, J.; Elmer, S.; Spöck, F.; Vales, A.; et al. Prevalence of SARS-CoV-2 antibodies in healthy blood donors from the state of Tyrol, Austria, in summer 2020. Wien Klin. Wochenschr. 2021, 133, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Siller, A.; Seekircher, L.; Wachter, G.A.; Astl, M.; Tschiderer, L.; Pfeifer, B.; Gaber, M.; Schennach, H.; Willeit, P. Seroprevalence, Waning and Correlates of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Large-Scale Study of 35,193 Blood Donors Conducted between June 2020 and September 2021. Viruses 2022, 14, 568. [Google Scholar] [CrossRef] [PubMed]
- data.gv.at—Open Data Österreich. Katalog COVID-19: Zeitreihe der Verabreichten Impfdosen der Corona-Schutzimpfung. Available online: https://www.data.gv.at/COVID-19/ (accessed on 14 July 2022).
- data.gv.at—Open Data Österreich. Katalog COVID-19: Zeitliche Darstellung von Daten zu Covid19-Fällen je Bundesland. Available online: https://www.data.gv.at/COVID-19/ (accessed on 21 July 2022).
- Statistik Austria. Bevölkerung nach Alter und Geschlecht. Available online: http://www.statistik.at/web_de/statistiken/menschen_und_gesellschaft/bevoelkerung/bevoelkerungsstruktur/bevoelkerung_nach_alter_geschlecht/index.html (accessed on 31 May 2022).
- Shang, W.; Kang, L.; Cao, G.; Wang, Y.; Gao, P.; Liu, J.; Liu, M. Percentage of Asymptomatic Infections among SARS-CoV-2 Omicron Variant-Positive Individuals: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1049. [Google Scholar] [CrossRef]
- Sigal, A. Milder disease with Omicron: Is it the virus or the pre-existing immunity? Nat. Rev. Immunol. 2022, 22, 69–71. [Google Scholar] [CrossRef]
- Suryawanshi, R.K.; Chen, I.P.; Ma, T.; Syed, A.M.; Brazer, N.; Saldhi, P.; Simoneau, C.R.; Ciling, A.; Khalid, M.M.; Sreekumar, B.; et al. Limited cross-variant immunity from SARS-CoV-2 Omicron without vaccination. Nature 2022, 607, 351–355. [Google Scholar] [CrossRef]
- Garrett, N.; Tapley, A.; Andriesen, J.; Seocharan, I.; Fisher, L.H.; Bunts, L.; Espy, N.; Wallis, C.L.; Randhawa, A.K.; Ketter, N.; et al. High Rate of Asymptomatic Carriage Associated with Variant Strain Omicron. medRxiv 2022. [Google Scholar] [CrossRef]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef]
- Brown, L.D.; Cai, T.T.; DasGupta, A. Interval Estimation for a Binomial Proportion. Statist. Sci. 2001, 16, 101–133. [Google Scholar] [CrossRef]
- Borena, W.; Bánki, Z.; Bates, K.; Winner, H.; Riepler, L.; Rössler, A.; Pipperger, L.; Theurl, I.; Falkensammer, B.; Ulmer, H.; et al. Persistence of immunity to SARS-CoV-2 over time in the ski resort Ischgl. EBioMedicine 2021, 70, 103534. [Google Scholar] [CrossRef] [PubMed]
- Knabl, L.; Mitra, T.; Kimpel, J.; Rössler, A.; Volland, A.; Walser, A.; Ulmer, H.; Pipperger, L.; Binder, S.C.; Riepler, L.; et al. High SARS-CoV-2 seroprevalence in children and adults in the Austrian ski resort of Ischgl. Commun. Med. 2021, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Breyer, M.-K.; Breyer-Kohansal, R.; Hartl, S.; Kundi, M.; Weseslindtner, L.; Stiasny, K.; Puchhammer-Stöckl, E.; Schrott, A.; Födinger, M.; Binder, M.; et al. Low SARS-CoV-2 seroprevalence in the Austrian capital after an early governmental lockdown. Sci. Rep. 2021, 11, 10158. [Google Scholar] [CrossRef] [PubMed]
- Szépfalusi, Z.; Schmidthaler, K.; Sieber, J.; Kopanja, S.; Götzinger, F.; Schoof, A.; Hoz, J.; Willinger, B.; Makristathis, A.; Weseslindtner, L.; et al. Lessons from low seroprevalence of SARS-CoV-2 antibodies in schoolchildren: A cross-sectional study. Pediatr. Allergy Immunol. 2021, 32, 762–770. [Google Scholar] [CrossRef]
- Ladage, D.; Höglinger, Y.; Ladage, D.; Adler, C.; Yalcin, I.; Harzer, O.; Braun, R.J. SARS-CoV-2-Specific Antibody Prevalence and Symptoms in a Local Austrian Population. Front. Med. 2021, 8, 632942. [Google Scholar] [CrossRef]
- Statistik Austria. Mehr als die Hälfte der SARS-CoV-2-Infektionen Kurz vor Dem Zweiten Lockdown Sind Behördlich Nicht erfasst. Available online: https://www.statistik.at/web_de/presse/124846.html (accessed on 10 December 2021).
- Weidner, L.; Nunhofer, V.; Jungbauer, C.; Hoeggerl, A.D.; Grüner, L.; Grabmer, C.; Zimmermann, G.; Rohde, E.; Laner-Plamberger, S. Seroprevalence of anti-SARS-CoV-2 total antibody is higher in younger Austrian blood donors. Infection 2021, 49, 1187–1194. [Google Scholar] [CrossRef]
- Rebholz, H.; Braun, R.J.; Saha, T.; Harzer, O.; Schneider, M.; Ladage, D. Longitudinal monitoring of SARS-CoV-2 spike protein-specific antibody responses in Lower Austria. PLoS ONE 2022, 17, e0271382. [Google Scholar] [CrossRef]
- Nunhofer, V.; Weidner, L.; Hoeggerl, A.D.; Zimmermann, G.; Badstuber, N.; Grabmer, C.; Jungbauer, C.; Lindlbauer, N.; Held, N.; Pascariuc, M.; et al. Persistence of Naturally Acquired and Functional SARS-CoV-2 Antibodies in Blood Donors One Year after Infection. Viruses 2022, 14, 637. [Google Scholar] [CrossRef]
- Kerbl, R.; Strenger, V.; Bernar, B.; Zurl, C.; Simma, B. SARS-CoV-2 seroprevalence in Austria. The situation before the omicron wave. Monatsschr. Kinderheilkd. 2022, 170, 487–489. [Google Scholar] [CrossRef]
- Perry, J.; Osman, S.; Wright, J.; Richard-Greenblatt, M.; Buchan, S.A.; Sadarangani, M.; Bolotin, S. Does a humoral correlate of protection exist for SARS-CoV-2? A systematic review. PLoS ONE 2022, 17, e0266852. [Google Scholar] [CrossRef]
- Takheaw, N.; Liwsrisakun, C.; Chaiwong, W.; Laopajon, W.; Pata, S.; Inchai, J.; Duangjit, P.; Pothirat, C.; Bumroongkit, C.; Deesomchok, A.; et al. Correlation Analysis of Anti-SARS-CoV-2 RBD IgG and Neutralizing Antibody against SARS-CoV-2 Omicron Variants after Vaccination. Diagnostics 2022, 12, 1315. [Google Scholar] [CrossRef]
- Hachmann, N.P.; Miller, J.; Collier, A.-R.Y.; Ventura, J.D.; Yu, J.; Rowe, M.; Bondzie, E.A.; Powers, O.; Surve, N.; Hall, K.; et al. Neutralization Escape by SARS-CoV-2 Omicron Subvariants BA.2.12.1, BA.4, and BA.5. N. Engl. J. Med. 2022, 387, 86–88. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Jian, F.; Song, W.; Xiao, T.; Wang, L.; Du, S.; Wang, J.; Li, Q.; Chen, X.; et al. 2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Nature 2022, 608, 593–602. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- AGES—Austrian Agency Health Food Safety. Effectiveness of Vaccine- and Infection-Induced Immunity against Omicron SARS-CoV2 Infection A Prospective, Population-Based Cohort Study, Austria, Calendar Week 01–12. Available online: https://wissenaktuell.ages.at/download/0/0/4dde38a7e33ef14540d722dfaff1fd2df3c46e63/fileadmin/AGES2015/Wissen-Aktuell/Wissen_aktuell_2022/Impfeffektivit%C3%A4t_Kohorten.pdf (accessed on 15 July 2022).
- Wratil, P.R.; Stern, M.; Priller, A.; Willmann, A.; Almanzar, G.; Vogel, E.; Feuerherd, M.; Cheng, C.-C.; Yazici, S.; Christa, C.; et al. Three exposures to the spike protein of SARS-CoV-2 by either infection or vaccination elicit superior neutralizing immunity to all variants of concern. Nat. Med. 2022, 28, 496–503. [Google Scholar] [CrossRef]
- Bates, T.A.; McBride, S.K.; Leier, H.C.; Guzman, G.; Lyski, Z.L.; Schoen, D.; Winders, B.; Lee, J.-Y.; Lee, D.X.; Messer, W.B.; et al. Vaccination before or after SARS-CoV-2 infection leads to robust humoral response and antibodies that effectively neutralize variants. Sci. Immunol. 2022, 7, eabn8014. [Google Scholar] [CrossRef]
- Miyamoto, S.; Arashiro, T.; Adachi, Y.; Moriyama, S.; Kinoshita, H.; Kanno, T.; Saito, S.; Katano, H.; Iida, S.; Ainai, A.; et al. Vaccination-infection interval determines cross-neutralization potency to SARS-CoV-2 Omicron after breakthrough infection by other variants. Clin. Transl. Rep. 2022, 3, 249–261.e4. [Google Scholar] [CrossRef]
- Anichini, G.; Terrosi, C.; Gandolfo, C.; Gori Savellini, G.; Fabrizi, S.; Miceli, G.B.; Franchi, F.; Cusi, M.G. Omicron Infection Evokes Cross-Protection against SARS-CoV-2 Variants in Vaccinees. Vaccines 2022, 10, 808. [Google Scholar] [CrossRef]
- Varese, A.; Mazzitelli, B.; Díaz, F.E.; Kjolhede, M.V.; Ojeda, D.; Vellicce, A.; Arto, P.; Cicero, C.; Pascowski, M.; Figueras, L.; et al. Omicron breakthrough infection after heterologous prime-boost vaccination induces a vigorous antibody response. J. Infect. Dis. 2022, jiac250. [Google Scholar] [CrossRef]
- Nordström, P.; Ballin, M.; Nordström, A. Risk of SARS-CoV-2 reinfection and COVID-19 hospitalisation in individuals with natural and hybrid immunity: A retrospective, total population cohort study in Sweden. Lancet Infect. Dis. 2022, 22, 781–790. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.S.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and Waning of Natural and Hybrid Immunity to SARS-CoV-2. N. Engl. J. Med. 2022, 386, 2201–2212. [Google Scholar] [CrossRef] [PubMed]
- Rodda, L.B.; Morawski, P.A.; Pruner, K.B.; Fahning, M.L.; Howard, C.A.; Franko, N.; Logue, J.; Eggenberger, J.; Stokes, C.; Golez, I.; et al. Imprinted SARS-CoV-2-specific memory lymphocytes define hybrid immunity. Cell 2022, 185, 1588–1601.e14. [Google Scholar] [CrossRef] [PubMed]
- data.gv.at—Open Data Österreich. Katalog COVID-19: Zeitliche Darstellung von Daten zu Verabreichte Impfdosen Nach Demografischen Gruppen. Available online: https://www.data.gv.at/COVID-19/ (accessed on 21 July 2022).


{kind=link}
{kind=link}
| No. of Participants | No. (%) or Median (IQR) | |
|---|---|---|
| Baseline data | ||
| Age in years—median (IQR) | 22,607 | 45.3 (30.9–55.1) |
| Female sex—no. (%) | 22,607 | 9477 (41.9%) |
| Vaccinated against SARS-CoV-2 *—no. (%) | 22,597 | 19,181 (84.9%) |
| First donation since July 2017—no. (%) | 22,607 | 4843 (21.4%) |
| Repeat donations during study | ||
| Participants with ≥2 donations—no. (%) | 22,607 | 2711 (12.0%) |
| Follow-up duration in months—median (IQR) | 2711 | 4.2 (3.0–5.3) |
| Month | No. of Measurements | % Seropositive (95% CI) | Geometric Mean (95% CI) in BAU/mL * |
|---|---|---|---|
| 2021 | |||
| October | 4230 | 84.9 (83.8–86.0) | 283 (271–296) |
| November | 3833 | 88.7 (87.6–89.6) | 313 (298–329) |
| December | 3363 | 91.3 (90.3–92.3) | 1036 (981–1094) |
| 2022 | |||
| January | 4567 | 93.5 (92.8–94.2) | 1215 (1163–1268) |
| February | 3059 | 95.3 (94.5–96.0) | 1354 (1291–1421) |
| March | 3753 | 95.9 (95.2–96.5) | 1489 (1426–1555) |
| April | 2756 | 95.8 (94.9–96.4) | 1437 (1360–1518) |
| Seropositivity (n = 2753) | Anti-S IgG Antibody Levels * (n = 2636) | |||||
|---|---|---|---|---|---|---|
| N | % Seropositive (95% CI) | N | Geometric Mean (95% CI) in BAU/mL | % Difference (95% CI) vs. Reference | p-Value | |
| Age groups (years) | ||||||
| <25 | 342 | 98.8 (96.9–99.7) | 338 | 2013 (1769–2290) | (Reference) | |
| 25–< 35 | 480 | 95.2 (92.9–96.8) | 457 | 1341 (1174–1531) | −33 (−46 to −18) | <0.001 |
| 35–< 45 | 508 | 94.3 (91.9–96.0) | 479 | 1188 (1036–1362) | −41 (−52 to −28) | <0.001 |
| 45–< 55 | 707 | 93.9 (91.9–95.5) | 664 | 1444 (1294–1611) | −28 (−41 to −13) | <0.001 |
| 55–< 65 | 617 | 97.7 (96.2–98.7) | 603 | 1469 (1307–1651) | −27 (−40 to −12) | 0.001 |
| ≥65 | 99 | 96.0 (89.7–98.7) | 95 | 1338 (975–1837) | −34 (−52 to −8) | 0.014 |
| Sex | ||||||
| Female | 1125 | 96.1 (94.8–97.1) | 1081 | 1421 (1302–1550) | (Reference) | |
| Male | 1628 | 95.5 (94.4–96.4) | 1555 | 1449 (1350–1556) | +2 (−9 to +14) | 0.726 |
| SARS-CoV-2 vaccination | ||||||
| No | 325 | 66.6 (61.3–71.5) | 216 | 108 (86–136) | (Reference) | |
| Yes | 2428 | 99.7 (99.3–99.8) | 2420 | 1813 (1731–1899) | +1579 (+1317 to +1888) | <0.001 |
| District in Tyrol | ||||||
| Schwaz | 366 | 95.6 (93.0–97.3) | 350 | 1710 (1461–2001) | (Reference) | |
| Innsbruck-Land | 497 | 95.0 (92.6–96.6) | 472 | 1530 (1353–1730) | −11 (−27 to 9) | 0.275 |
| Innsbruck-Stadt | 193 | 97.4 (94.0–99.1) | 188 | 1681 (1403–2014) | −2 (−24 to +27) | 0.897 |
| Kufstein | 212 | 95.8 (92.0–97.9) | 203 | 1467 (1200–1792) | −14 (−33 to +10) | 0.228 |
| Kitzbühel | 596 | 95.8 (93.9–97.2) | 571 | 1251 (1104–1418) | −27 (−40 to −11) | 0.001 |
| Imst | 315 | 95.9 (93.0–97.6) | 302 | 1339 (1135–1580) | −22 (−37 to −2) | 0.031 |
| Landeck | 15 | 93.3 (68.2–100.0) | 14 | 2117 (1038–4320) | +24 (−43 to +167) | 0.586 |
| Reutte | 169 | 95.3 (90.8–97.7) | 161 | 1401 (1129–1738) | −18 (−37 to +7) | 0.147 |
| Lienz | 390 | 96.2 (93.7–97.7) | 375 | 1345 (1161–1559) | −21 (−36 to −3) | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seekircher, L.; Siller, A.; Astl, M.; Tschiderer, L.; Wachter, G.A.; Pfeifer, B.; Huber, A.; Gaber, M.; Schennach, H.; Willeit, P. Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Updated Analysis Involving 22,607 Blood Donors Covering the Period October 2021 to April 2022. Viruses 2022, 14, 1877. https://doi.org/10.3390/v14091877
Seekircher L, Siller A, Astl M, Tschiderer L, Wachter GA, Pfeifer B, Huber A, Gaber M, Schennach H, Willeit P. Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Updated Analysis Involving 22,607 Blood Donors Covering the Period October 2021 to April 2022. Viruses. 2022; 14(9):1877. https://doi.org/10.3390/v14091877
Chicago/Turabian StyleSeekircher, Lisa, Anita Siller, Manfred Astl, Lena Tschiderer, Gregor A. Wachter, Bernhard Pfeifer, Andreas Huber, Manfred Gaber, Harald Schennach, and Peter Willeit. 2022. "Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Updated Analysis Involving 22,607 Blood Donors Covering the Period October 2021 to April 2022" Viruses 14, no. 9: 1877. https://doi.org/10.3390/v14091877
APA StyleSeekircher, L., Siller, A., Astl, M., Tschiderer, L., Wachter, G. A., Pfeifer, B., Huber, A., Gaber, M., Schennach, H., & Willeit, P. (2022). Seroprevalence of Anti-SARS-CoV-2 IgG Antibodies in Tyrol, Austria: Updated Analysis Involving 22,607 Blood Donors Covering the Period October 2021 to April 2022. Viruses, 14(9), 1877. https://doi.org/10.3390/v14091877