
The Predictive Role of Hepatitis B Biomarkers on HBV Reactivation following Direct-Acting Antiviral Therapy in HBV/HCV Coinfected Patients

 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
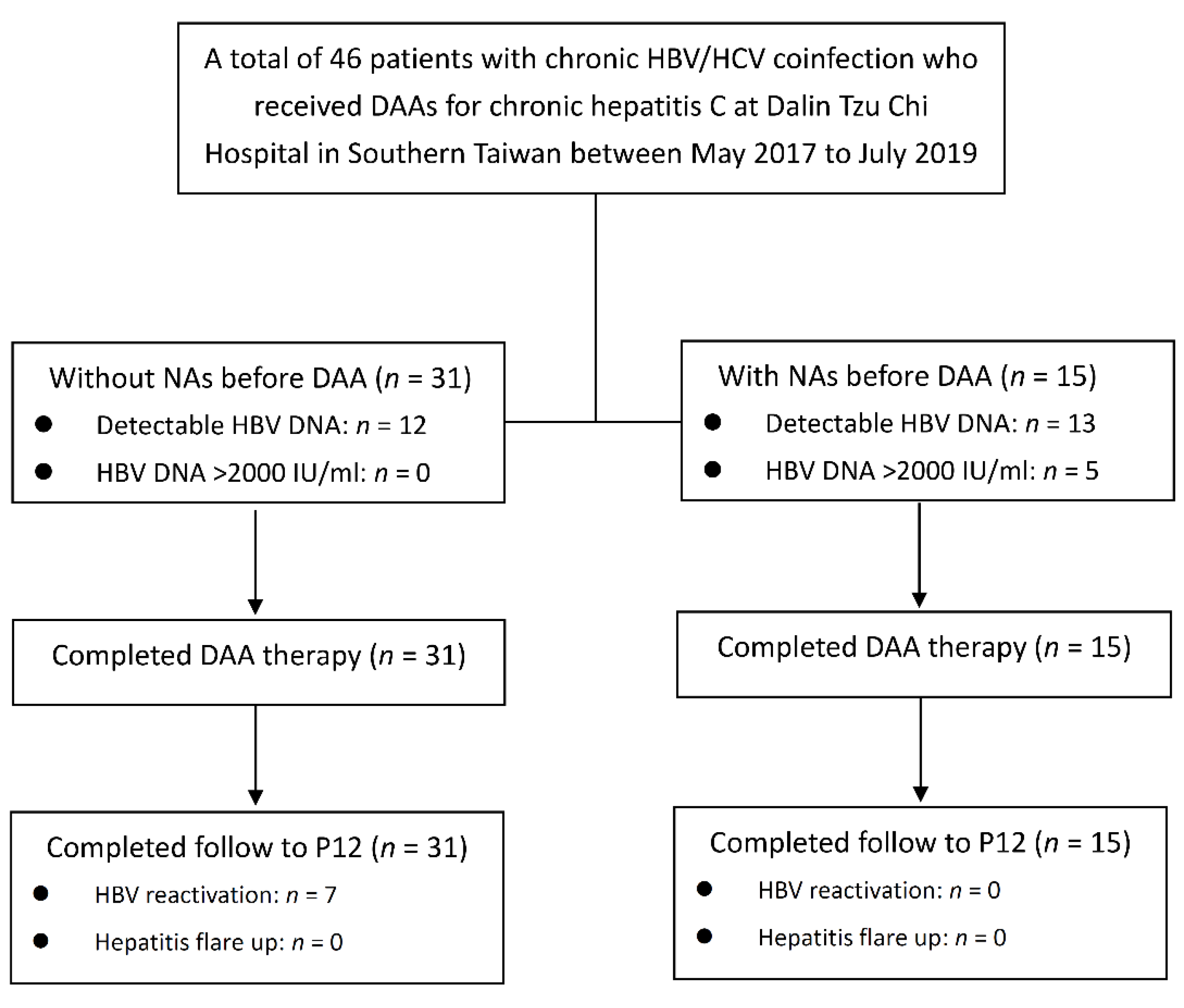
2.1. Patients
2.2. Ethical Considerations
2.3. Clinical Monitoring
2.4. HBV/HCV Quantification and HCV Genotyping
2.5. HBsAg Quantification
2.6. HBcrAg Quantification
2.7. Extraction and Reverse Transcription (RT) of HBV pgRNA
2.8. Quantification of Serum HBV pgRNA
2.9. Statistical Analysis
3. Results
3.1. Patient Characteristics
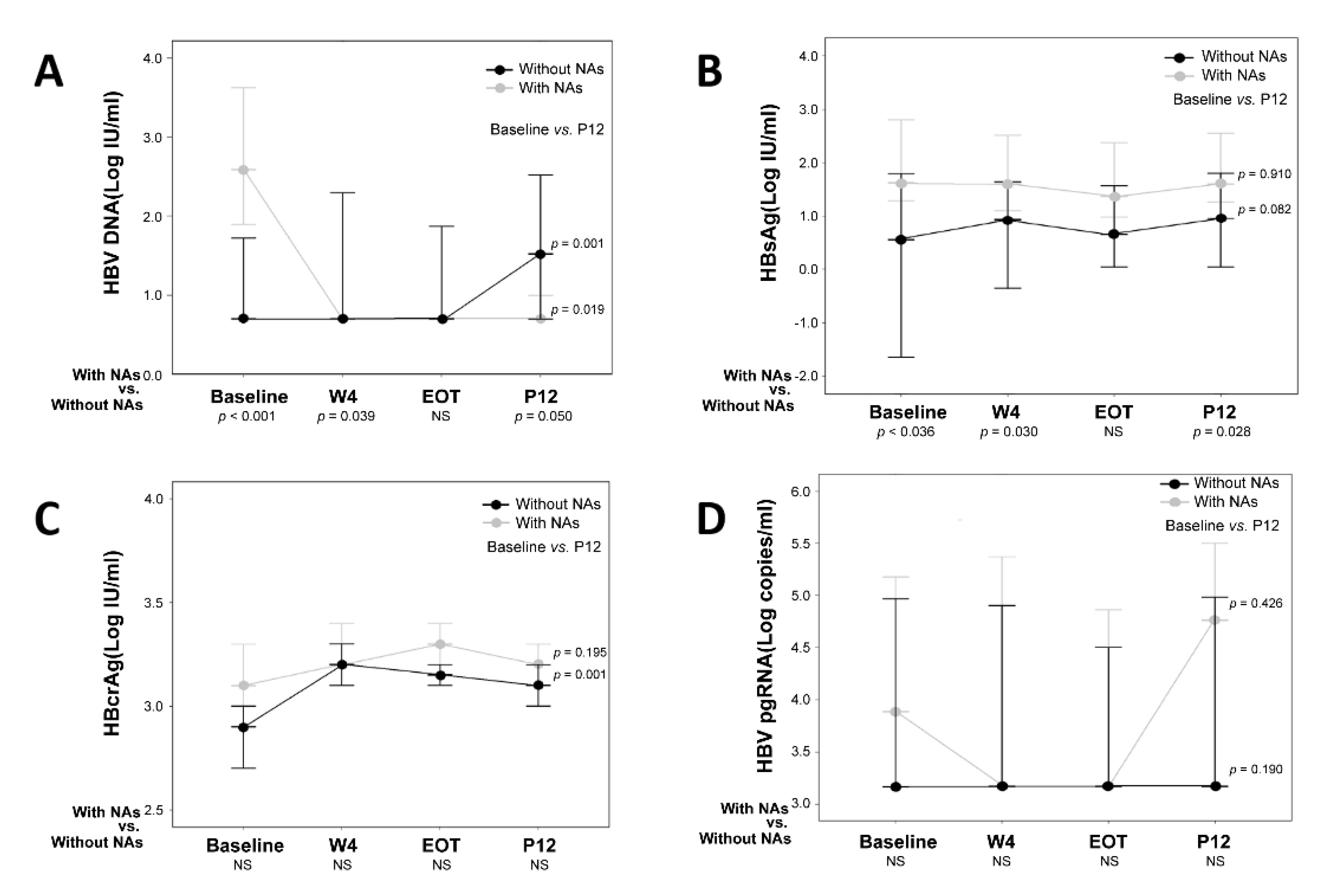
3.2. HBV Biomarkers in Patients with and without NA Treatment
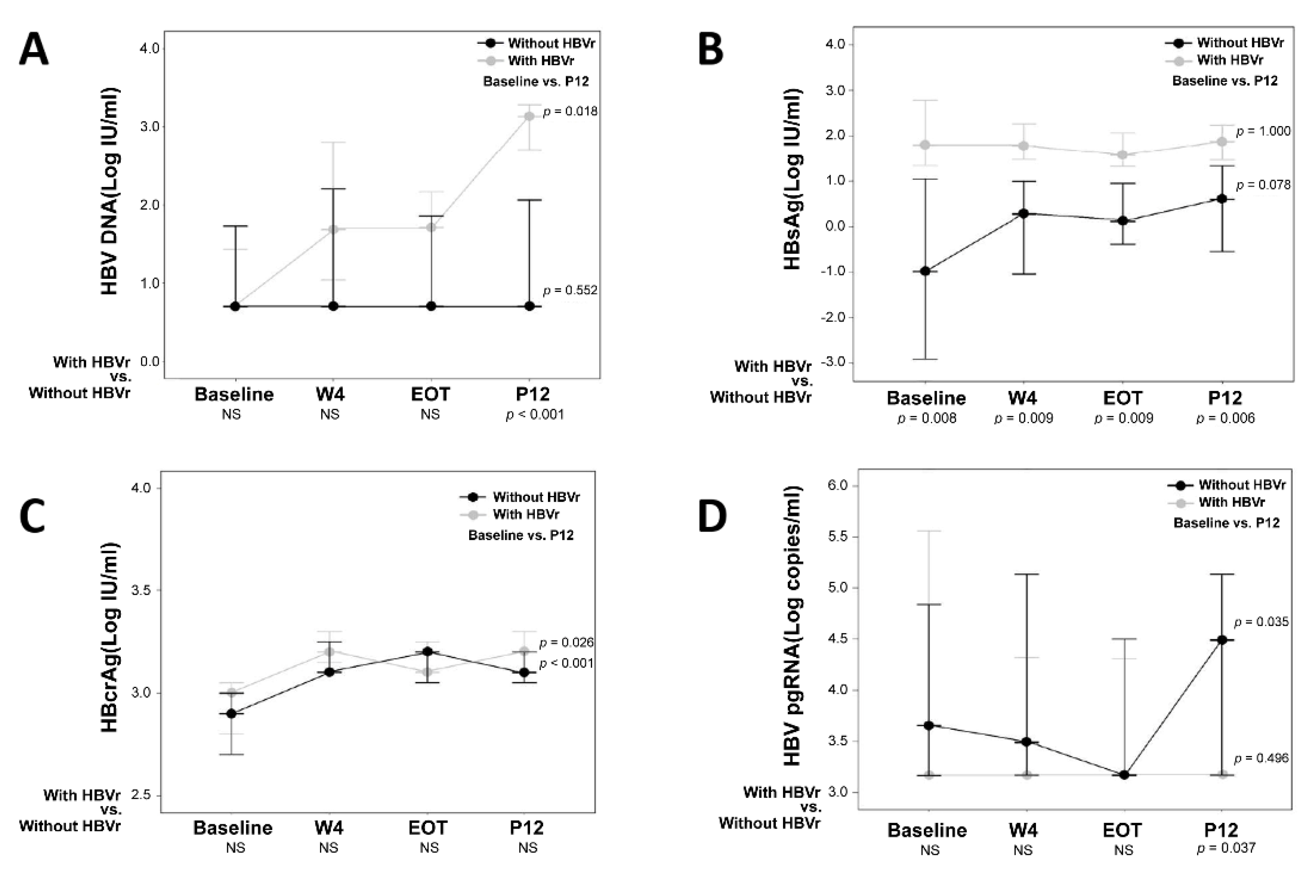
3.3. Subgroup Analysis in Patients without NA Treatment
3.4. Factors Associated with HBV Reactivation among the Patients without NAs Treatment
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Hepatitis C Virus | HCV |
| Hepatitis B Virus | HBV |
| Direct Antiviral Agents | DAAs |
| HBV reactivation | HBVr |
| Covalently Closed Circular DNA | cccDNA |
| Hepatitis B Surface Antigen | HBsAg |
| Hepatitis B Core-Related Antigen | HBcrAg |
| HBV Pregenomic RNA | HBV pgRNA |
| Nucleos(t)ide Analogues | NA |
| Hepatitis E Antigen | HBeAg |
| 4th Week During DAA Treatment | W4 |
| End of DAA Treatment | EOT |
| 12th Week Post-DAA Treatment | P12 |
| Aspartate Aminotransferase | AST |
| Alanine Aminotransferase | ALT |
| Estimated Glomerular Filtration Rate | eGFR |
| Alpha-Fetoprotein | AFP |
| Fibrosis-4 | FIB-4 |
| Hepatocellular Carcinoma | HCC |
| lower limit of detection | LLOD |
| Reverse Transcription | RT |
References
- Liu, C.J.; Chen, P.J.; Chen, D.S.; Tseng, T.C.; Kao, J.H. Perspectives on dual hepatitis B and C infection in Taiwan. J. Formos Med. Assoc. 2016, 115, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.Y.; Yu, M.L.; Chuang, W.L.; Lin, Z.Y.; Chen, S.C.; Hsieh, M.Y.; Wang, L.Y.; Tsai, J.F.; Chang, W.Y. Influence of hepatitis C virus on the profiles of patients with chronic hepatitis B virus infection. J. Gastroenterol. Hepatol. 2001, 16, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Mavilia, M.G.; Wu, G.Y. HBV-HCV Coinfection: Viral Interactions, Management, and Viral Reactivation. J. Clin. Transl. Hepatol. 2018, 6, 296–305. [Google Scholar] [CrossRef]
- Jung, M.K.; Shin, E.C. Regulatory T cells in hepatitis B and C virus infections. Immune Netw. 2016, 16, 330–336. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.J.; Kao, J.H. Hepatitis C and hepatitis B coinfection. In Clinical Dilemmas in Viral Liver Disease; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2020; pp. 182–188. [Google Scholar]
- Pisaturo, M.; Macera, M.; Alessio, L.; Calò, F.; Coppola, N. Hepatitis B Virus (HBV) reactivation following pharmacological eradication of Hepatitis C Virus (HCV). Viruses 2019, 11, 850. [Google Scholar] [CrossRef]
- Cheng, P.N.; Liu, C.J.; Chen, C.Y.; Tseng, K.C.; Lo, C.C.; Peng, C.Y.; Lin, C.L.; Chiu, H.C.; Chiu, Y.C.; Chen, P.J. Entecavir prevents HBV reactivation during direct acting antivirals for HCV/HBV dual infection: A randomized trial. Clin. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef]
- Mücke, M.M.; Backus, L.I.; Mücke, V.T.; Coppola, N.; Preda, C.M.; Yeh, M.L.; Tang, L.S.Y.; Belperio, P.S.; Wilson, E.M.; Yu, M.L.; et al. Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 172–180. [Google Scholar] [CrossRef]
- Balagopal, A.; Thio, C.L. When viruses collide: Hepatitis B virus reactivation after hepatitis C treatment. J. Clin. Investig. 2020, 130, 2823–2826. [Google Scholar] [CrossRef]
- Cheng, X.; Uchida, T.; Xia, Y.; Umarova, R.; Liu, C.J.; Chen, P.J.; Gaggar, A.; Suri, V.; Mücke, M.M.; Vermehren, J.; et al. Diminished hepatic IFN response following HCV clearance triggers HBV reactivation in coinfection. J. Clin. Investig. 2020, 130, 3205–3220. [Google Scholar] [CrossRef]
- Mak, L.Y.; Wong, D.K.; Cheung, K.S.; Seto, W.K.; Lai, C.L.; Yuen, M.F. Review article: Hepatitis B core-related antigen (HBcrAg): An emerging marker for chronic hepatitis B virus infection. Aliment. Pharmacol. Ther. 2018, 47, 43–54. [Google Scholar] [CrossRef]
- Ou, Q.; Guo, J.; Zeng, Y.; Chen, H. Insights for clinical diagnostic indicators of virus and host in chronic hepatitis B infection. J. Viral Hepat. 2020, 27, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.Q.; Kew, G.S.; Lim, S.G. Controversies in treating chronic hepatitis B virus: The role of hepatitis B virus DNA and surface antigen titer. Clin. Liver Dis. 2021, 25, 763–784. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Cao, X.; Wang, Z.; Gao, Y.; Deng, J.; Liu, X.; Zhuang, H. Correlation of HBcrAg with intrahepatic hepatitis B virus total DNA and covalently closed circular DNA in HBeAg-positive chronic hepatitis B patients. J. Clin. Microbiol. 2019, 57, e01303-18. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Q.; Wang, M.L.; Tao, Y.C.; Wu, D.B.; Liao, J.; He, M.; Tang, H. Serum HBcrAg is better than HBV RNA and HBsAg in reflecting intrahepatic covalently closed circular DNA. J. Viral Hepat. 2019, 26, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, F.; Miyakoshi, H.; Kobayashi, M.; Kumada, H. Correlation between serum hepatitis B virus core-related antigen and intrahepatic covalently closed circular DNA in chronic hepatitis B patients. J. Med. Virol. 2009, 81, 27–33. [Google Scholar] [CrossRef]
- Cornberg, M.; Wong, V.W.; Locarnini, S.; Brunetto, M.; Janssen, H.L.A.; Chan, H.L. The role of quantitative hepatitis B surface antigen revisited. J. Hepatol. 2017, 66, 398–411. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.L.; Huang, C.F.; Huang, C.I.; Holmes, J.A.; Hsieh, M.H.; Tsai, Y.S.; Liang, P.C.; Tsai, P.C.; Hsieh, M.Y.; Lin, Z.Y.; et al. Hepatitis B-related outcomes following direct-acting antiviral therapy in Taiwanese patients with chronic HBV/HCV co-infection. J. Hepatol. 2020, 73, 62–71. [Google Scholar] [CrossRef]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef]
- Chou, R.; Wasson, N. Blood tests to diagnose fibrosis or cirrhosis in patients with chronic hepatitis C virus infection: A systematic review. Ann. Intern. Med. 2013, 158, 807–820. [Google Scholar] [CrossRef]
- Tseng, C.W.; Wu, S.F.; Chen, C.Y.; Ho, Y.C.; He, Y.T.; Tseng, K.C. Characteristics of regulatory T-cell function in patients with chronic hepatitis B and C coinfection. J. Viral Hepat. 2020, 27, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, M.; Kojima, T.; Itoh, Y.; Harano, Y.; Fujii, K.; Nakajima, T.; Kato, T.; Takeda, N.; Okuda, J.; Ida, K.; et al. The severity of ultrasonographic findings in nonalcoholic fatty liver disease reflects the metabolic syndrome and visceral fat accumulation. Am. J. Gastroenterol. 2007, 102, 2708–2715. [Google Scholar] [CrossRef] [PubMed]
- Wu, I.C.; Liu, W.C.; Chiu, Y.C.; Chiu, H.C.; Cheng, P.N.; Chang, T.T. Clinical implications of serum hepatitis B virus pregenomic RNA kinetics in chronic hepatitis B patients receiving antiviral treatment and those achieving HBsAg loss. Microorganisms 2021, 9, 1146. [Google Scholar] [CrossRef] [PubMed]
- Mak, L.Y.; Seto, W.K.; Fung, J.; Yuen, M.F. New biomarkers of chronic hepatitis B. Gut Liver 2019, 13, 589–595. [Google Scholar] [CrossRef]
- Chen, S.Y.; Kao, C.F.; Chen, C.M.; Shih, C.M.; Hsu, M.J.; Chao, C.H.; Wang, S.H.; You, L.R.; Lee, Y.H. Mechanisms for inhibition of hepatitis B virus gene expression and replication by hepatitis C virus core protein. J. Biol. Chem. 2003, 278, 591–607. [Google Scholar] [CrossRef] [PubMed]
- Shih, C.M.; Chen, C.M.; Chen, S.Y.; Lee, Y.H. Modulation of the trans-suppression activity of hepatitis C virus core protein by phosphorylation. J. Virol. 1995, 69, 1160–1171. [Google Scholar] [CrossRef]
- Hu, J.; Boyer, M. Hepatitis B virus reverse transcriptase and epsilon RNA sequences required for specific interaction in vitro. J. Virol. 2006, 80, 2141–2150. [Google Scholar] [CrossRef] [PubMed]
- Konstantinou, D.; Deutsch, M. The spectrum of HBV/HCV coinfection: Epidemiology, clinical characteristics, viralinteractions and management. Ann. Gastroenterol. 2015, 28, 221–228. [Google Scholar] [PubMed]
- Watanabe, T.; Inoue, T.; Tanaka, Y. Hepatitis B core-related antigen and new therapies for hepatitis B. Microorganisms 2021, 9, 2083. [Google Scholar] [CrossRef]
- Wong, D.K.; Tanaka, Y.; Lai, C.L.; Mizokami, M.; Fung, J.; Yuen, M.F. Hepatitis B virus core-related antigens as markers for monitoring chronic hepatitis B infection. J. Clin. Microbiol. 2007, 45, 3942–3947. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.Q.; Feng, S.; Wang, M.L.; Liang, L.B.; Zhou, L.Y.; Du, L.Y.; Yan, L.B.; Tao, C.M.; Tang, H. Serum hepatitis B core-related antigen is a satisfactory surrogate marker of intrahepatic covalently closed circular DNA in chronic hepatitis B. Sci. Rep. 2017, 7, 173. [Google Scholar] [CrossRef] [PubMed]
- Vachon, A.; Osiowy, C. Novel biomarkers of hepatitis B virus and their use in chronic hepatitis B patient management. Viruses 2021, 13, 951. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F. Role of hepatitis C virus in dual and triple hepatitis virus infection. Hepatology 1995, 22, 1101–1108. [Google Scholar] [PubMed]
- Chan, C.Y.; Lee, S.D.; Wu, J.C.; Hwang, S.J.; Wang, Y.J.; Huang, Y.S.; Lo, K.J. Superinfection with hepatitis C virus in patients with symptomatic chronic hepatitis B. Scand. J. Infect. Dis. 1991, 23, 421–424. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 46) | Without NAs Treatment (n = 31) | With NAs Treatment (n = 15) | p Value | |
|---|---|---|---|---|
| Age (years) & | 65.9 (41–82) | 66.1 (41–82) | 64.2 (49–81) | 0.535 § |
| Male (n, %) | 20 (43.5) | 11 (35.5) | 9 (60.0) | 0.116 † |
| Cirrhosis (n, %) | 19 (41.3) | 13 (41.9) | 6 (40.0) | 0.901 † |
| HCC (n, %) | 6 (13.0) | 3 (9.7) | 3 (20.0) | 0.375 ‡ |
| Fatty liver (n, %) | 15 (32.6) | 11 (35.5) | 4 (26.7) | 0.740 ‡ |
| Alcoholism (n, %) | 5 (10.9) | 4 (12.9) | 1 (6.7) | >0.999 ‡ |
| HCV RNA (Log IU/mL) & | 5.9 (3.7–7.2) | 5.9 (3.7–7.2) | 6.1 (4.9–7.0) | 0.716 § |
| Genotype (n, %) | 0.381 † | |||
| Type 1 | 29 (63.0) | 18 (58.1) | 11 (73.3) | |
| Type 2 | 14 (30.4) | 10 (32.3) | 4 (26.7) | |
| Type 6 | 3 (6.5) | 3 (9.7) | 0 (0) | |
| HBeAg-negative chronic infection (n, %) | 41 (89.1) | 31 (100) | 10 (66.7) | 0.002 † |
| HBeAg-negative chronic hepatitis (n, %) | 5.0 (10.9) | 0 (0) | 5 (33.3) | 0.002 † |
| HBV DNA (Log IU/mL) | 1.4 (0.7–7.1) | 0.7 (0.7–3.2) | 2.6 (0.7–7.1) | <0.001 § |
| Detectable HBV DNA (n, %) | 25 (54.3) | 12 (38.7) | 13 (86.7) | 0.002 † |
| HBV DNA (Log IU/mL) in patients with detectable HBV DNA & | 2.3 (1.4–7.1) | 2.2 (1.4–3.2) | 2.9 (1.6–7.1) | 0.030 § |
| HBsAg (IU/mL) & | 13.2 (3 × 10−4–2347.7) | 5.2 (3 × 10−4–2178.3) | 35.0 (7 × 10−4–2347.7) | 0.036 § |
| HBsAg (Log IU/mL) & | 1.1 (−3.5–3.4) | 0.7 (-3.5–3.3) | 1.5 (-3.2–3.4) | 0.036 § |
| HBcrAg (Log IU/mL) & | 3.0 (2.5–6.5) | 2.9 (2.5–3.6) | 3.0 (2.7–6.5) | 0.063 § |
| HBV pgRNA (Log copies/mL) & | 3.3 (3.2–6.8) | 3.2 (3.2–6.4) | 3.9 (3.2–6.8) | 0.523 § |
| Detectable HBV pgRNA (n, %) | 23 (50.0) | 14 (45.2) | 9 (60.0) | 0.365 † |
| HBV pgRNA (Log copies/mL) in patients with detectable HBV pgRNA & | 5.0 (3.4–6.8) | 5.0 (4.1–6.4) | 4.9 (3.4–6.8) | 0.600 § |
| FIB-4 & | 2.4 (0.5–12.3) | 2.2 (0.5–12.3) | 3.6 (1.3–6.3) | 0.059 § |
| Total bilirubin (mg/dL) & | 0.7 (0.3–1.7) | 0.7 (0.3–1.7) | 0.8 (0.5–1.2) | 0.530 § |
| ALT (U/L) & | 69 (25–281) | 69.5 (25–235) | 72 (25–281) | 0.824 § |
| AST (U/L) & | 47 (17–282) | 47 (17–144) | 58 (24–282) | 0.566 § |
| Albumin (g/dL) & | 4.4 (3.0–4.9) | 4.3 (3.0–4.9) | 4.4 (3.6–4.7) | 0.598 § |
| Prothrombin time (sec) & | 10.7 (9.7–12.4) | 10.7 (9.7–12.4) | 10.8 (10.0–12.2) | 0.814 § |
| AFP (U/L) & | 4.5 (1.3–1812.5) | 4.2 (1.3–1812.5) | 8.5 (1.8–75.5) | 0.320 § |
| Platelets (× 103/mm3) & | 176.5 (56–316) | 181 (56–316) | 160 (80–210) | 0.071 § |
| eGFR (mL/min/1.73 m2) & | 83.7 (26.7–142.5) | 87.3 (39–118.1) | 72.5 (26.7–128.0) | 0.598 § |
| DAA regimen (n, %) | 0.529 † | |||
| Ledipasvir/sofosbuvir | 27 (58.7) | 18 (58.1) | 9 (60.0) | |
| Daclatasvir + sofosbuvir | 4 (8.7) | 2 (6.5) | 2 (13.3) | |
| Paritaprevir/ritonavir/ombitasvir + dasabuvir | 5 (10.9) | 4 (12.9) | 1 (6.7) | |
| Elbasvir/grazoprevir | 6 (13.0) | 4 (12.9) | 2 (13.3) | |
| Sofosbuvir + ribavirin | 3 (6.5) | 2 (6.5) | 1 (6.7) | |
| Glecaprevir/pibrentasvir | 1 (2.2) | 1 (3.2) | 0 (0) |
| Without HBV Reactivation (n = 24) | With HBV Reactivation (n = 7) | p Value | |
|---|---|---|---|
| Age (years) & | 67.9 (44–82) | 58.3 (41–66) | 0.008 § |
| Age < 65 Y/O (n, %) | 7 (29.2) | 6 (85.7) | 0.012 ‡ |
| Male (n, %) | 7 (29.2) | 4 (57.1) | 0.210 ‡ |
| Cirrhosis (n, %) | 11 (45.8) | 2 (28.6) | 0.667 ‡ |
| HCC (n, %) | 3 (12.5) | 0 (0) | >0.999 ‡ |
| Fatty liver (n, %) | 7 (29.2) | 4 (57.1) | 0.216 ‡ |
| Alcoholism (n, %) | 2 (8.3) | 2 (28.6) | 0.212 ‡ |
| Genotype 1 (n, %) | 14 (58.3) | 4 (57.1) | >0.999 ‡ |
| HCV RNA (Log IU/mL) & | 6.0 (3.9–7.2) | 5.7 (3.7–7.0) | 0.139 § |
| Sofosbuvir-containing Regimen (n, %) | 17 (70.8) | 5 (71.4) | >0.999 ‡ |
| HBV DNA (Log IU/mL) | 0.7 (0.7–3.2) | 0.7 (0.7–2.4) | 0.764 § |
| Detectable HBV DNA (n, %) | 10 (41.7) | 2 (28.6) | 0.535 ‡ |
| HBV DNA (Log IU/mL) in patients with detectable HBV DNA & | 2.0 (1.4–3.2) | 2.3 (2.2–2.4) | 0.485 § |
| HBsAg (IU/mL) & | 0.12 (3 × 10−4–1053.1) | 62.7 (8.1–2178.3) | 0.008 § |
| HBsAg (Log IU/mL) & | −0.9 (−3.5–3.0) | 1.8 (0.9–3.3) | 0.008 § |
| HBcrAg (Log IU/mL) & | 2.9 (2.5–3.6) | 3.0 (2.7–3.1) | 0.661 § |
| HBV pgRNA (Log copies/mL) & | 3.2 (3.2–6.4) | 3.2 (3.2–6.2) | 0.800 § |
| Detectable HBV pgRNA (n, %) | 11 (45.8) | 3 (42.8) | >0.999 ‡ |
| HBV pgRNA (Log copies/mL) in patients with detectable HBV pgRNA & | 4.8 (4.1–6.4) | 6.1 (5.0–6.2) | 0.225 § |
| FIB-4 & | 2.2 (0.5–12.3) | 1.4 (0.5–5.0) | 0.317 § |
| Total bilirubin (mg/dL) & | 0.7 (0.3–1.7) | 0.6 (0.5–1.1) | 0.473 § |
| ALT (U/L) & | 64 (25–204) | 73 (42–235) | 0.695 § |
| AST (U/L) & | 46 (17–144) | 52 (17–141) | 0.729 § |
| Albumin (g/dL) & | 4.4 (3.0–4.9) | 4.2 (3.8–4.6) | 0.764 § |
| Prothrombin time (sec) & | 10.7 (9.7–12.4) | 10.7 (10.1–12.3) | 0.872 § |
| AFP (U/L) & | 4.8 (1.5–1812.5) | 2.4 (1.3–67.3) | 0.118 § |
| Platelets (x 103/mm3) & | 188 (56–316) | 177 (87–243) | 0.595 § |
| eGFR (mL/min/1.73 m2) & | 75.8 (38.9–118.1) | 91.8 (87.4–100.3) | 0.139 § |
| Single Variable Logistic Regression | Multivariable Logistic Regression | |||
|---|---|---|---|---|
| HR (95% CI) | p Value * | HR (95% CI) | p Value * | |
| Age > 65 Y/O | 0.069 (0.007–0.068) | 0.022 | ||
| Male | 3.218 (0.570–18.385) | 0.185 | ||
| Cirrhosis | 0.473 (0.076–2.935) | 0.421 | ||
| Fatty liver | 3.238 (0.570–18.385) | 0.185 | ||
| Alcoholism | 4.400 (0.494–39.210) | 0.184 | ||
| Genotype 1 | 0.952 (0.174–5.228) | 0.955 | ||
| HCV RNA (Log IU/mL) | 0.570 (0.231–1.407) | 0.223 | ||
| Sofosbuvir-containing regimen | 1.029 (0.160–6.620) | 0.976 | ||
| HBV DNA (Log IU/mL) | 0.826 (0.255–2.676) | 0.750 | ||
| HBsAg (Log IU/mL) | 2.303 (1.086–4.882) | 0.030 | 2.303 (1.086–4.882) | 0.030 |
| HBcrAg (Log IU/mL) | 0.991 (0.034–28.628) | 0.996 | ||
| HBV pgRNA (Log copies/mL) | 1.195 (0.585–2.441) | 0.625 | ||
| FIB-4 | 0.793 (0.485–1.299) | 0.358 | ||
| Total bilirubin (mg/dL) | 0.290 (0.011–7.507) | 0.456 | ||
| ALT (U/L) | 1.005 (0.990–1.019) | 0.545 | ||
| AST (U/L) | 0.996 (0.974–1.019) | 0.743 | ||
| Albumin (g/dL) | 1.014 (0.090–11.456) | 0.991 | ||
| Prothrombin time (sec) | 1.183 (0.363–3.857) | 0.780 | ||
| AFP (U/L) | 0.998 (0.988–1.009) | 0.725 | ||
| Platelets (×103/mm3) | 0.996 (0.981–1.010) | 0.579 | ||
| eGFR (mL/min/1.73 m2) | 1.041 (0.988–1.098) | 0.134 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tseng, C.-W.; Liu, W.-C.; Ko, P.-H.; Chen, Y.-C.; Tseng, K.-C.; Chang, T.-T. The Predictive Role of Hepatitis B Biomarkers on HBV Reactivation following Direct-Acting Antiviral Therapy in HBV/HCV Coinfected Patients. Viruses 2022, 14, 1812. https://doi.org/10.3390/v14081812
Tseng C-W, Liu W-C, Ko P-H, Chen Y-C, Tseng K-C, Chang T-T. The Predictive Role of Hepatitis B Biomarkers on HBV Reactivation following Direct-Acting Antiviral Therapy in HBV/HCV Coinfected Patients. Viruses. 2022; 14(8):1812. https://doi.org/10.3390/v14081812
Chicago/Turabian StyleTseng, Chih-Wei, Wen-Chun Liu, Ping-Hung Ko, Yen-Chun Chen, Kuo-Chih Tseng, and Ting-Tsung Chang. 2022. "The Predictive Role of Hepatitis B Biomarkers on HBV Reactivation following Direct-Acting Antiviral Therapy in HBV/HCV Coinfected Patients" Viruses 14, no. 8: 1812. https://doi.org/10.3390/v14081812
APA StyleTseng, C.-W., Liu, W.-C., Ko, P.-H., Chen, Y.-C., Tseng, K.-C., & Chang, T.-T. (2022). The Predictive Role of Hepatitis B Biomarkers on HBV Reactivation following Direct-Acting Antiviral Therapy in HBV/HCV Coinfected Patients. Viruses, 14(8), 1812. https://doi.org/10.3390/v14081812