
Impact of HIV-1 Infection on the Natural Progress of an Anti-HCV Positive Population in an Impoverished Village in China from 2009 to 2017


Abstract
:1. Introduction
2. Materials and Methods
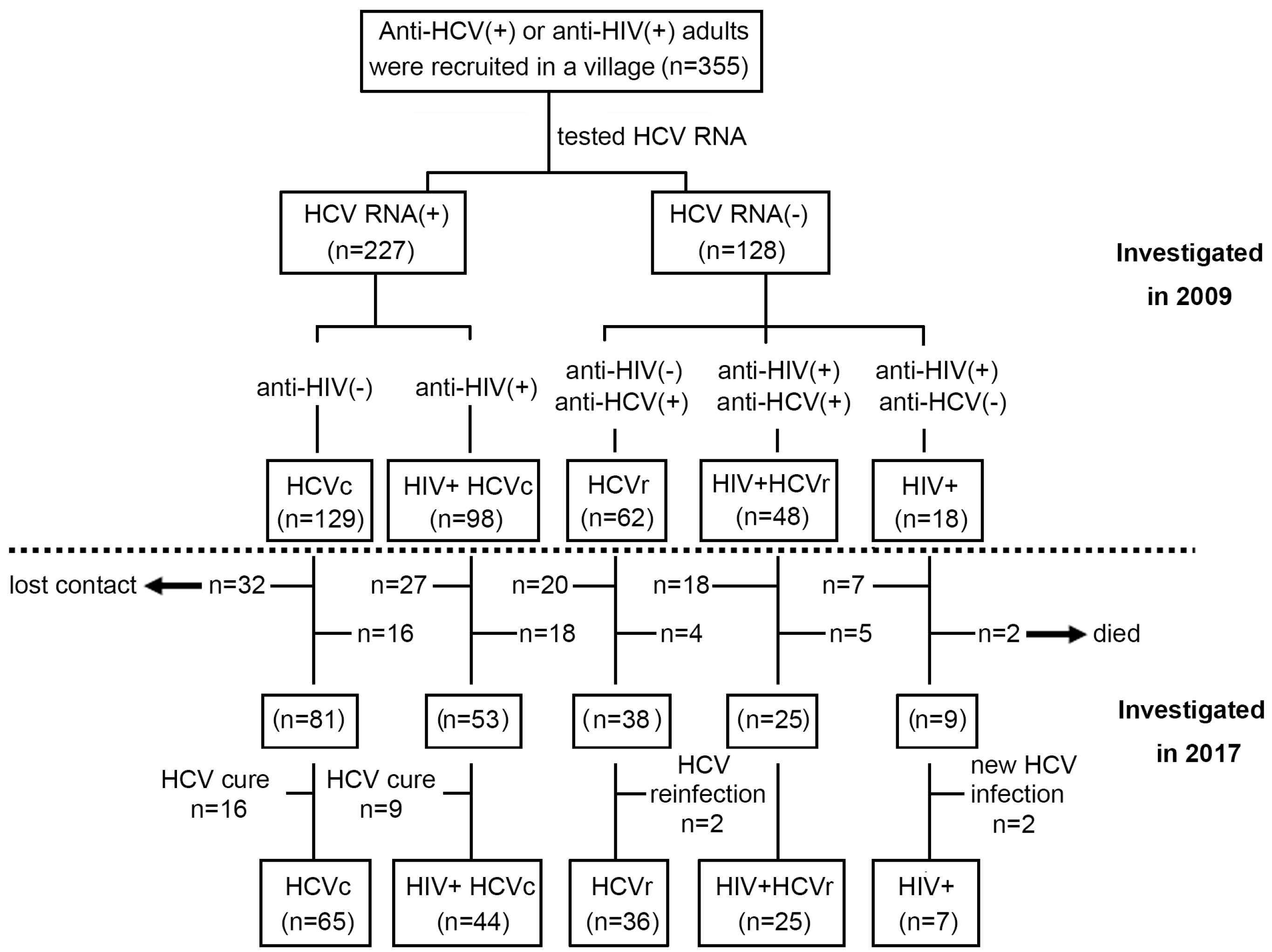
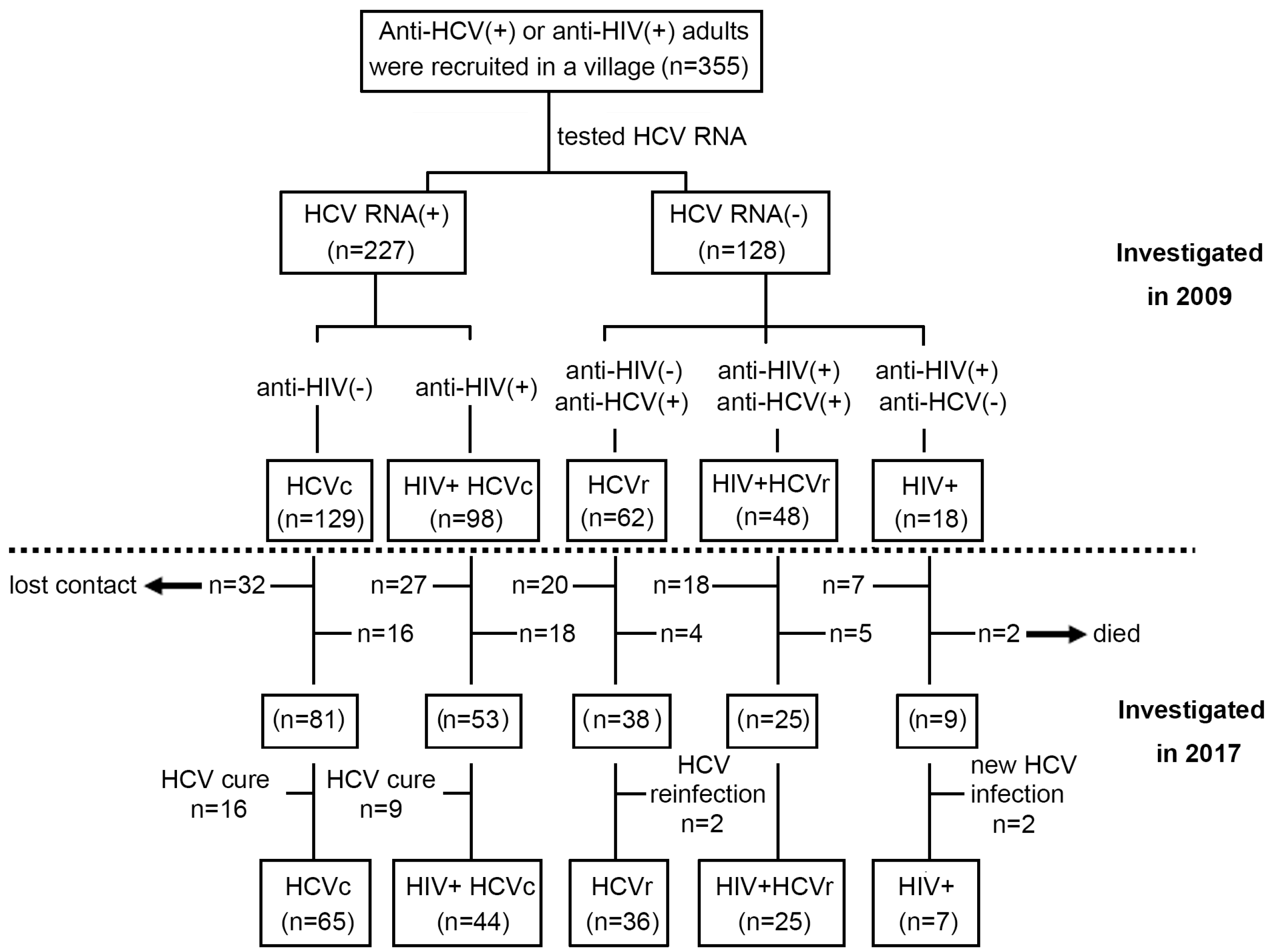
2.1. Study Population
2.2. HIV and HCV Seropositive Screening and Confirmation
2.3. Quantification of HCV-RNA, HIV-RNA, and CD4+/ CD8+ T-Cell Counts
2.4. Evaluation of Liver Fibrosis
2.5. Statistical Analyses
3. Results
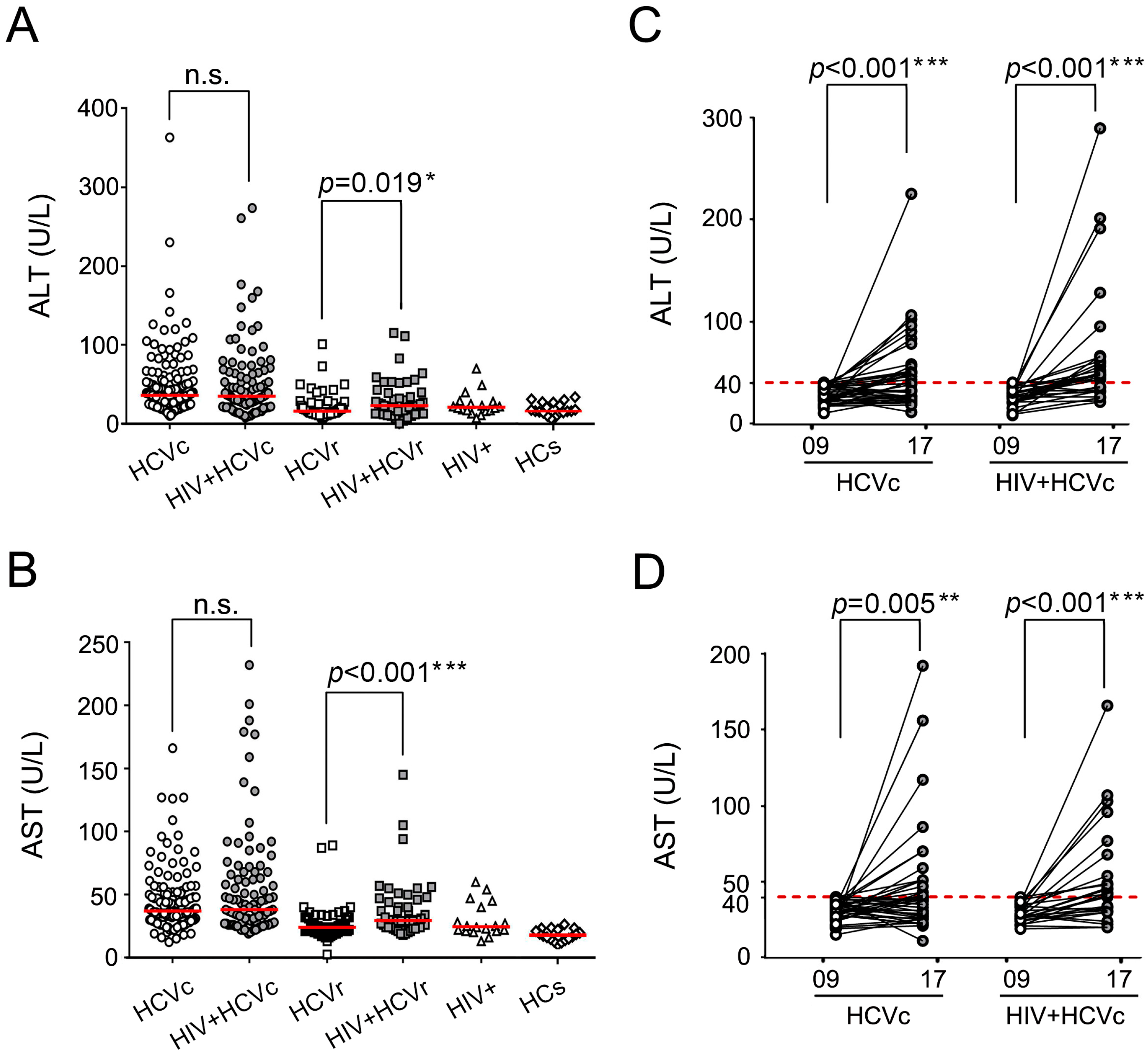
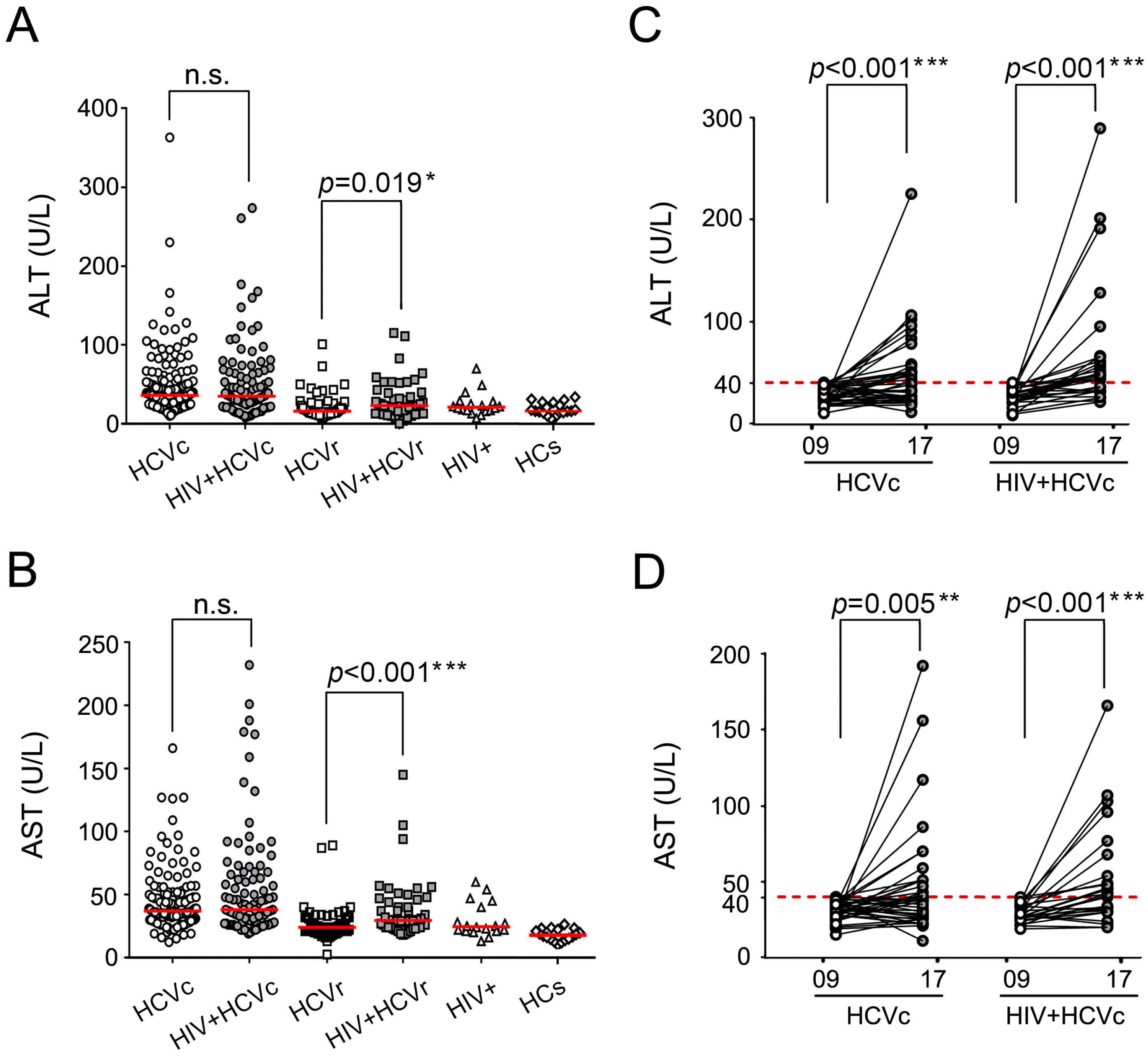
3.1. The HIV/HCV Coinfection Group Had Higher Transaminase Levels than the HCV Mono-Infection Group
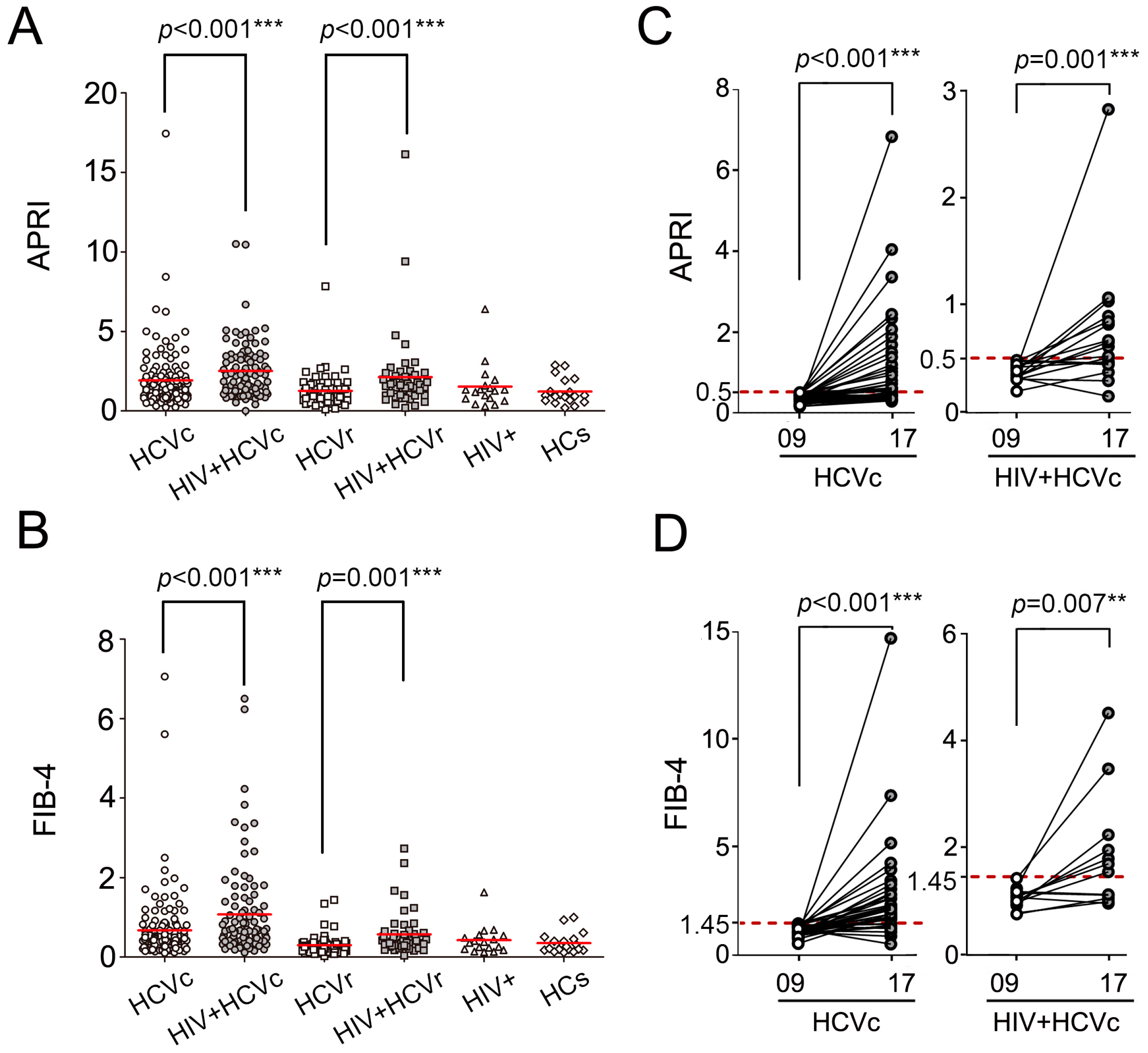
3.2. The HIV/HCV Coinfection Group Had Higher APRI and FIB-4 Levels than the HCV Mono-Infection Group
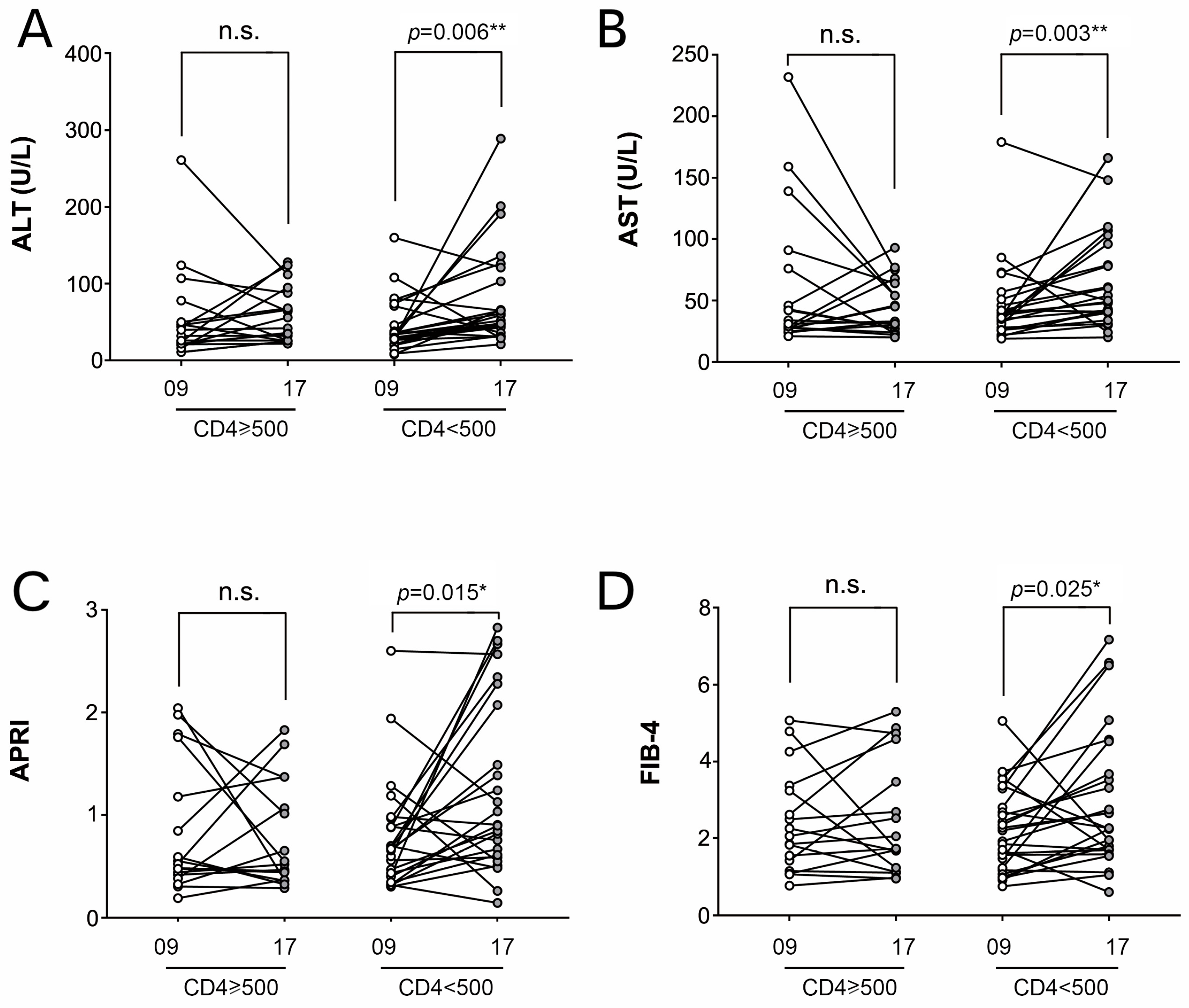
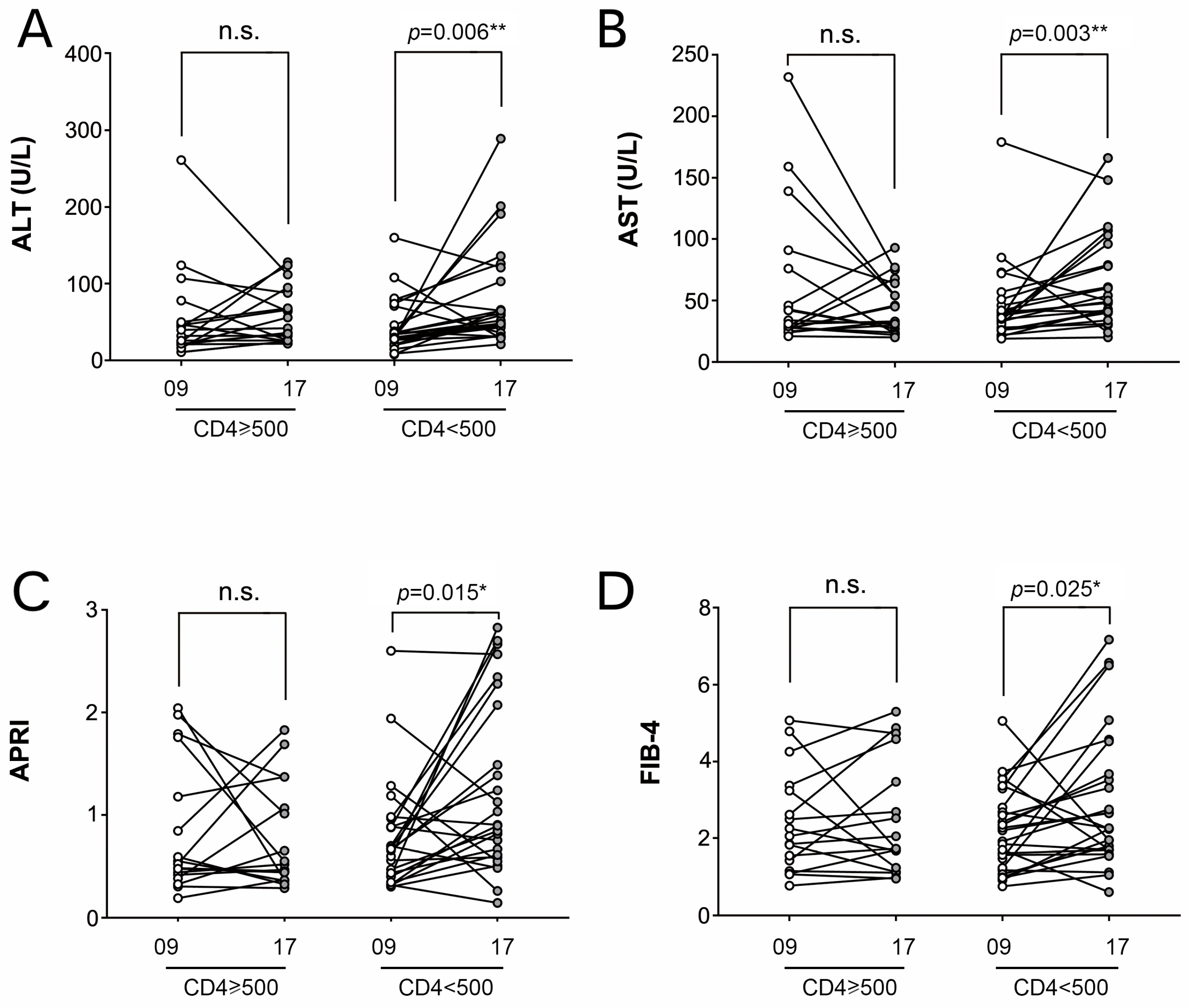
3.3. HIV Disease Progression Contributes to HCV Liver Fibrosis
3.4. HIV/HCV Coinfection Was Associated with Higher Mortality in ESLD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, A.Y.; Chung, R.T. Coinfection with HIV-1 and HCV—A one-two punch. Gastroenterology 2009, 137, 795–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.Y.; Feeney, E.R.; Chung, R.T. HCV and HIV co-infection: Mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 362–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, W.; Weinberg, E.M.; Chung, R.T. Pathogenesis of accelerated fibrosis in HIV/HCV co-infection. J. Infect. Dis. 2013, 207 (Suppl. S1), S13–S18. [Google Scholar] [CrossRef] [PubMed]
- Schuppan, D.; Ruehl, M.; Somasundaram, R.; Hahn, E.G. Matrix as a modulator of hepatic fibrogenesis. Semin. Liver Dis. 2001, 21, 351–372. [Google Scholar] [CrossRef]
- Bataller, R.; Ginès, P. New therapeutic strategies in liver fibrosis: Pathogenic basis. Med. Clin. 2002, 118, 339–346. [Google Scholar] [CrossRef]
- Hernandez, M.D.; Sherman, K.E. HIV/hepatitis C coinfection natural history and disease progression. Curr. Opin. HIV AIDS 2011, 6, 478–482. [Google Scholar] [CrossRef] [Green Version]
- Avihingsanon, A.; Jitmitraparp, S.; Tangkijvanich, P.; Ramautarsing, R.A.; Apornpong, T.; Jirajariyavej, S.; Putcharoen, O.; Treeprasertsuk, S.; Akkarathamrongsin, S.; Poovorawan, Y.; et al. Advanced liver fibrosis by transient elastography, fibrosis 4, and alanine aminotransferase/platelet ratio index among Asian hepatitis C with and without human immunodeficiency virus infection: Role of vitamin D levels. J. Gastroenterol. Hepatol. 2014, 29, 1706–1714. [Google Scholar] [CrossRef]
- Li Vecchi, V.; Giannitrapani, L.; Di Carlo, P.; Mazzola, G.; Colletti, P.; La Spada, E.; Vizzini, G.; Montalto, G.; Soresi, M. Non-invasive assessment of liver steatosis and fibrosis in HIV/HCV- and HCV- infected patients. Ann. Hepatol. 2013, 12, 740–748. [Google Scholar] [CrossRef]
- Mazzocato, S.; Orsetti, E.; Gesuita, R.; Piraccini, F.; Drenaggi, D.; Barchiesi, F. Comparison of liver fibrosis progression in HIV/HCV co-infected and HCV mono-infected patients by transient elastometry. Scand. J. Infect. Dis. 2014, 46, 797–802. [Google Scholar] [CrossRef]
- Tovo, C.V.; Becker, S.C.; Almeida, P.R.; Galperim, B.; Chaves, S. Progression of liver fibrosis in monoinfected patients by hepatitis C virus and coinfected by HCV and human immunodeficiency virus. Arq. De Gastroenterol. 2013, 50, 19–22. [Google Scholar] [CrossRef] [Green Version]
- Lewden, C.; Chene, G.; Morlat, P.; Raffi, F.; Dupon, M.; Dellamonica, P.; Pellegrin, J.L.; Katlama, C.; Dabis, F.; Leport, C. HIV-infected adults with a CD4 cell count greater than 500 cells/mm3 on long-term combination antiretroviral therapy reach same mortality rates as the general population. J. Acquir. Immune Defic. Syndr. 2007, 46, 72–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ucar, F.; Erden, G.; Ginis, Z.; Ozturk, G.; Sezer, S.; Gurler, M.; Guneyk, A. Estimation of biological variation and reference change value of glycated hemoglobin (HbA1c) when two analytical methods are used. Clin. Biochem. 2013, 46, 1548–1553. [Google Scholar] [CrossRef] [PubMed]
- Shin, W.G.; Park, S.H.; Jang, M.K.; Hahn, T.H.; Kim, J.B.; Lee, M.S.; Kim, D.J.; Jun, S.Y.; Park, C.K. Aspartate aminotransferase to platelet ratio index (APRI) can predict liver fibrosis in chronic hepatitis B. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2008, 40, 267–274. [Google Scholar] [CrossRef]
- Puoti, M.; Bonacini, M.; Spinetti, A.; Putzolu, V.; Govindarajan, S.; Zaltron, S.; Favret, M.; Callea, F.; Gargiulo, F.; Donato, F.; et al. Liver fibrosis progression is related to CD4 cell depletion in patients coinfected with hepatitis C virus and human immunodeficiency virus. J. Infect. Dis. 2001, 183, 134–137. [Google Scholar] [CrossRef]
- EASL Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [CrossRef] [PubMed] [Green Version]
- Ghany, M.G.; Morgan, T.R. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef] [Green Version]
- Aiuti, F.; Mezzaroma, I. Failure to reconstitute CD4+ T-cells despite suppression of HIV replication under HAART. AIDS Rev. 2006, 8, 88–97. [Google Scholar]
- Sherman, K.E.; Rockstroh, J.; Thomas, D. Human immunodeficiency virus and liver disease: An update. Hepatology 2015, 62, 1871–1882. [Google Scholar] [CrossRef] [Green Version]
- Matthews, G.V.; Neuhaus, J.; Bhagani, S.; Mehta, S.H.; Vlahakis, E.; Doroana, M.; Naggie, S.; Arenas-Pinto, A.; Peters, L.; Rockstroh, J.K. Baseline prevalence and predictors of liver fibrosis among HIV-positive individuals: A substudy of the INSIGHT Strategic Timing of AntiRetroviral Treatment (START) trial. HIV Med. 2015, 16 (Suppl. S1), 129–136. [Google Scholar] [CrossRef]
- Heetun, Z.S.; Byrnes, C.; Neary, P.; O’Morain, C. Review article: Reproduction in the patient with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2007, 26, 513–533. [Google Scholar] [CrossRef]
- Sandler, N.G.; Douek, D.C. Microbial translocation in HIV infection: Causes, consequences and treatment opportunities. Nat. Rev. Microbiol. 2012, 10, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Zarracina, T.; Valle-Garay, E.; Collazos, J.; Montes, A.H.; Cárcaba, V.; Carton, J.A.; Asensi, V. Didanosine (ddI) associates with increased liver fibrosis in adult HIV-HCV coinfected patients. J. Viral Hepat. 2012, 19, 685–693. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | HCVc (n = 129) | HCVc/HIV (n = 98) | HCVr (n = 62) | HCVr/HIV (n = 48) | HIV (n = 18) | HCs (n = 18) |
|---|---|---|---|---|---|---|
| Age (y) 1 | 50.4 (12.8) | 45.2 (9.8) | 46.7 (12.7) | 44.1 (9.2) | 42 (13.1) | 40.5 (13.5) |
| Gender (M/F) | 61/68 | 45/53 | 13/49 | 20/28 | 8/10 | 4/14 |
| Anti-HIV | Negative | Positive | Negative | Positive | Positive | Negative |
| HCV VL (log10 IU/mL) 1 | 6 (0.9) | 6.2 (0.9) | None | None | None | None |
| Anti-HCV (S/CO) 1 | 14.4 (1.8) | 13.2(3.2) | 7.6 (4.1) | 7.2 (3.5) | Negative | Negative |
| HCV genotype, n (%) | ||||||
| 1b | 83 | 44 | U.D. | U.D. | N.A. | N.A. |
| 2a | 46 | 54 | U.D. | U.D. | N.A. | N.A. |
| Others | None | None | U.D. | U.D. | N.A. | N.A. |
| Biochemistry analyses 1 | ||||||
| ALT (IU/L) | 49.7 (43.9) | 51.5 (47.8) | 21.3 (15.9) | 30.5 (24.6) | 24.8 (15) | 21.1 (8.5) |
| AST (IU/L) | 44.5 (24.7) | 53.8 (42.5) | 26.5 (13.2) | 37.6 (23.5) | 29.6 (13.5) | 24.6 (6.8) |
| ALP (IU/L) | 97.6 (50.3) | 124.1 (59.7) | 88.9 (34.9) | 111.9 (58.4) | 88.6 (31.2) | 81.4 (33.5) |
| GGT (IU/L) | 29.5 (26.7) | 63.1 (73.8) | 21.7 (27.3) | 45 (45.9) | 32.7 (20) | 16.8 (6.8) |
| TBIL (μmol/L) | 13.7 (3.5) | 13.6 (5.2) | 13.3 (3.4) | 13.9 (3.4) | 13.6 (4.9) | 13.5 (3.2) |
| DBIL (μmol/L) | 4.3 (1.3) | 4.4 (1.7) | 4.5 (2.4) | 4.1 (1.4) | 5.5 (1.6) | 4.5 (1.5) |
| TP (g/L) | 76.5 (7.8) | 78.5 (6.7) | 75.5 (6.1) | 77.5 (5.2) | 77.1 (8.4) | 75.8 (2.7) |
| ALB (g/L) | 44.2 (5.8) | 44.6 (8.4) | 42.8 (5.6) | 44.6 (7.1) | 44.8 (5.6) | 39.9 (4.7) |
| CD4+T cell (cells/μL) | 836 (315) | 451 (238) | 894 (339) | 416 (233) | 521 (344) | 926 (379) |
| CD8+T cell (cells/μL) | 653 (335) | 994 (582) | 697 (353) | 1028 (378) | 805 (263) | 751 (357) |
| CD4+/CD8+ T cell | 1.5 (0.7) | 0.6 (0.5) | 1.5 (0.7) | 0.4 (0.2) | 0.7 (0.5) | 1.4 (0.6) |
| Variable | HCVc | HIV + HCVc | p-Value |
|---|---|---|---|
| Total patients in 2009 (n) | 129 | 98 | |
| Total death (n (% of total death)) | 16 (12.4%) | 18 (18.4%) | 0.213 |
| AIDS-related death (n (% of total death)) | 0 (0%) | 3 (16.6%) | 0.087 |
| Non-AIDS-related death (n (% of total death)) | 16 (100%) | 15 (83.4%) | 0.087 |
| ESLD-related death (n (% of non-AIDS-related death)) | 5 (31.3%) | 11 (73.3%) | 0.009 ** |
| Other cause of death (n (% of non-AIDS-related death)) 1 | 11 (68.7%) | 4 (26.7%) | 0.009 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Li, Y.; Zhang, Y.; Yin, Y.; Tu, J.; Xu, Q.; Liang, H.; Shen, T. Impact of HIV-1 Infection on the Natural Progress of an Anti-HCV Positive Population in an Impoverished Village in China from 2009 to 2017. Viruses 2022, 14, 1621. https://doi.org/10.3390/v14081621
Li X, Li Y, Zhang Y, Yin Y, Tu J, Xu Q, Liang H, Shen T. Impact of HIV-1 Infection on the Natural Progress of an Anti-HCV Positive Population in an Impoverished Village in China from 2009 to 2017. Viruses. 2022; 14(8):1621. https://doi.org/10.3390/v14081621
Chicago/Turabian StyleLi, Xinjie, Yuantao Li, Yuqi Zhang, Yue Yin, Jing Tu, Qiang Xu, Hua Liang, and Tao Shen. 2022. "Impact of HIV-1 Infection on the Natural Progress of an Anti-HCV Positive Population in an Impoverished Village in China from 2009 to 2017" Viruses 14, no. 8: 1621. https://doi.org/10.3390/v14081621
APA StyleLi, X., Li, Y., Zhang, Y., Yin, Y., Tu, J., Xu, Q., Liang, H., & Shen, T. (2022). Impact of HIV-1 Infection on the Natural Progress of an Anti-HCV Positive Population in an Impoverished Village in China from 2009 to 2017. Viruses, 14(8), 1621. https://doi.org/10.3390/v14081621