
A Thorough Synthesis of Phage Therapy Unit Activity in Poland—Its History, Milestones and International Recognition

 , ,
, ,
Abstract
:1. Preface
2. Methodology
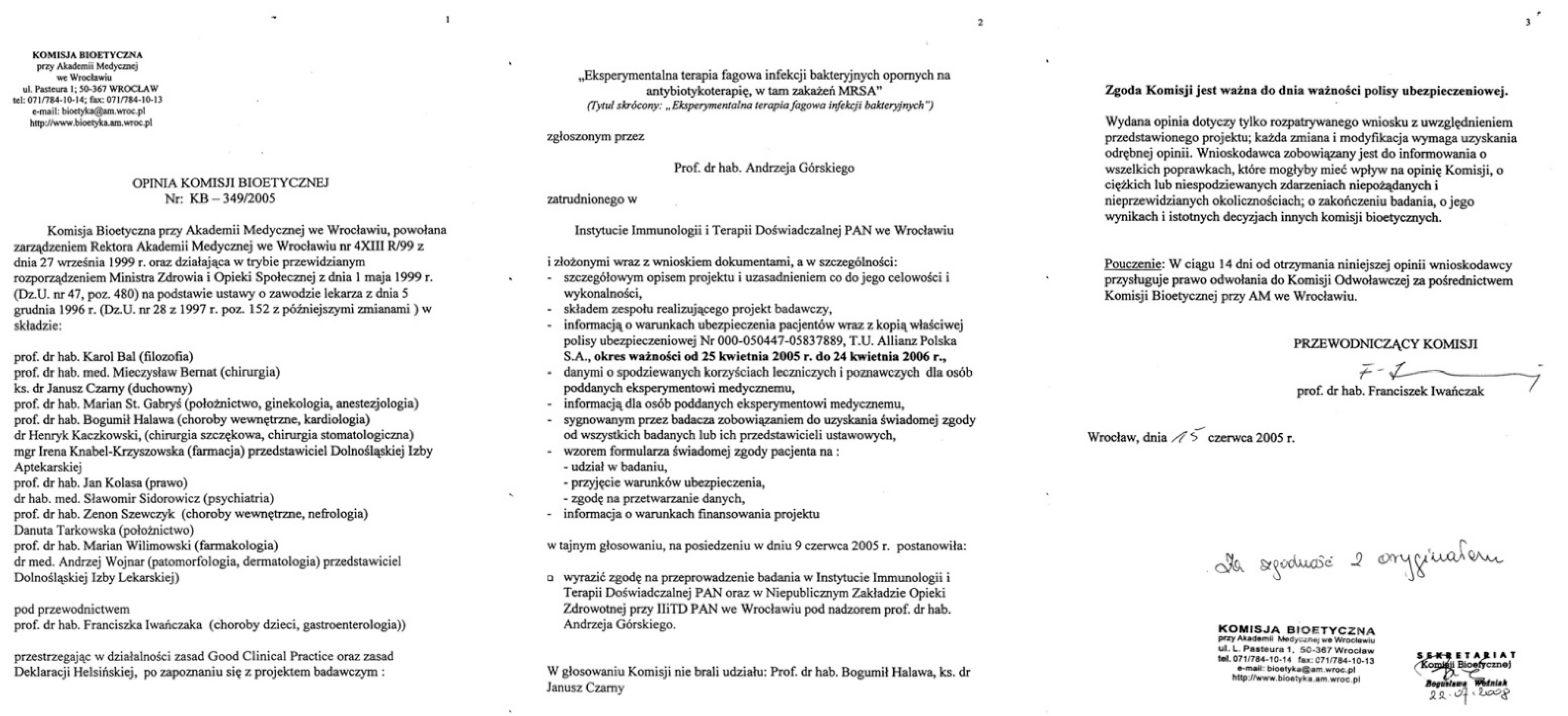
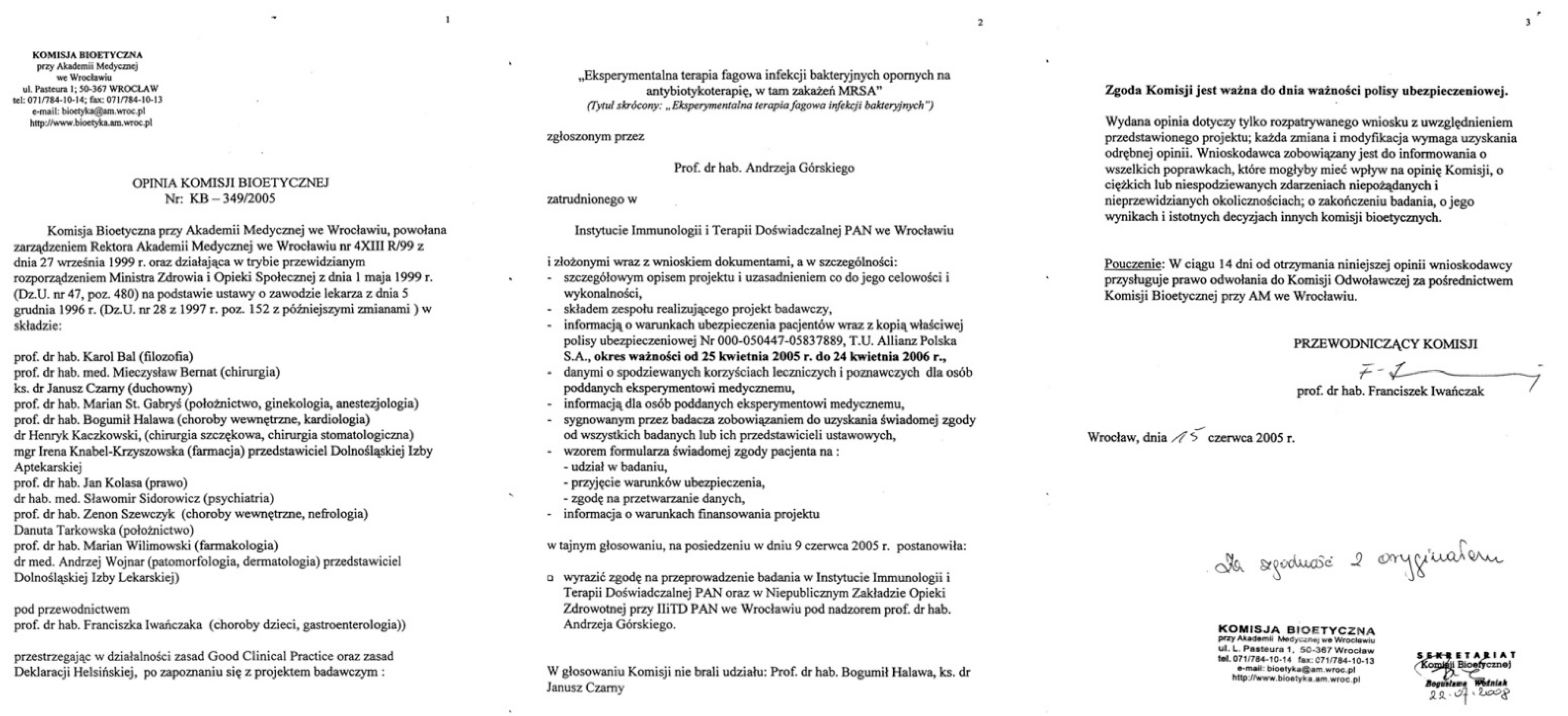
3. Legal Aspects of Experimental Treatments
4. Phage Therapy Unit
4.1. Establishment of PTU in Poland
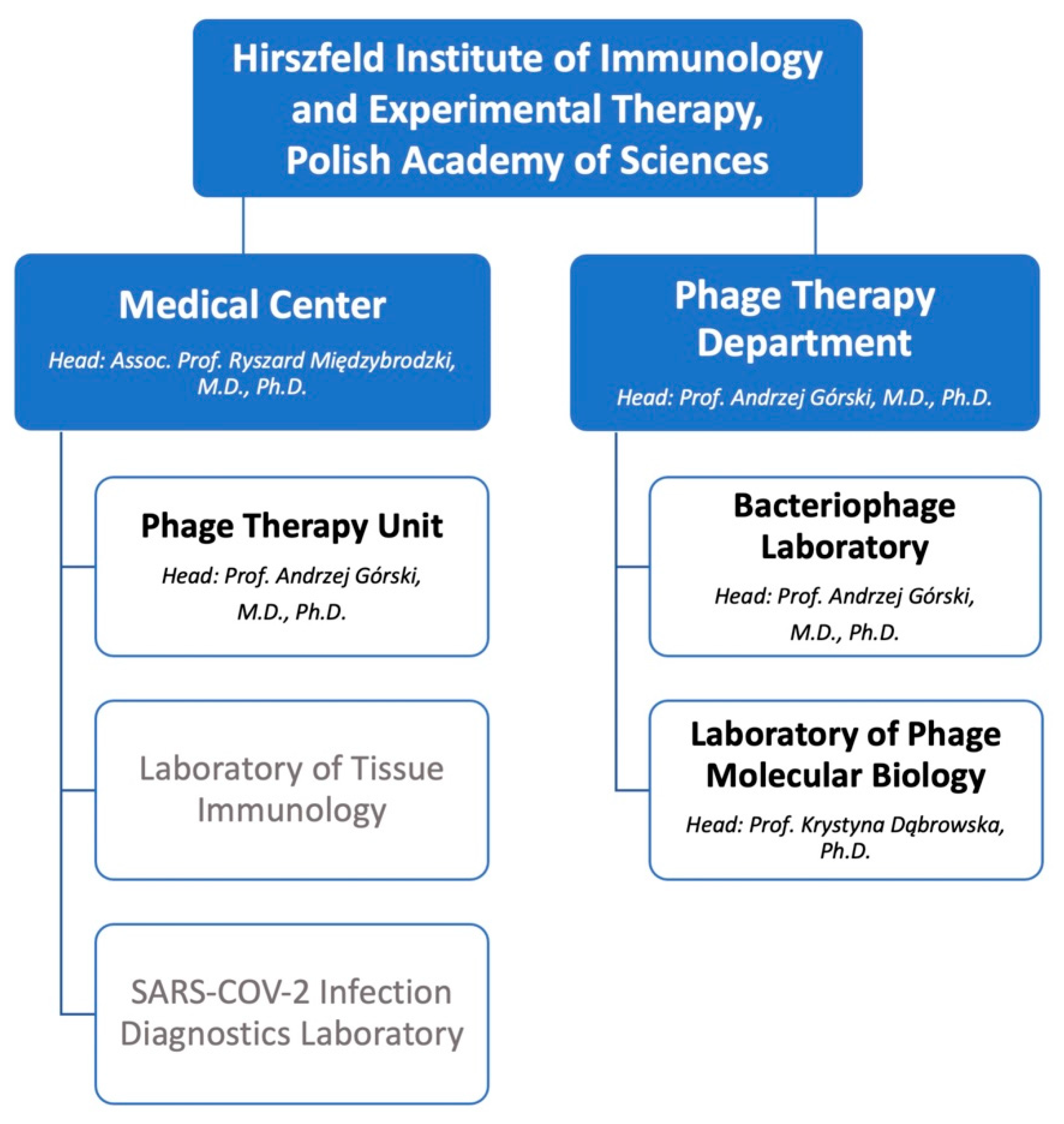
4.2. Organizational Structure, Team Members and Educational Activity
4.3. Treatment Regimen
- The purpose and basics of experimental phage therapy (including a brief description of the method of producing phage preparations);
- The principles of conducting experimental phage therapy (including admission criteria, ways of administering the formulation and follow-up visit description);
- Possible risks and undesired effects that patients may encounter while undergoing phage treatment;
- Mandatory insurance and protection of patients’ rights;
- The costs of the experimental treatment;
- The right to withdraw from the treatment at any time;
- Description of cases when treatment is terminated by the physician;
- Procedures in the event of patient doubts and the appearance of new information;
- Contact details for the PTU and physician supervising the experiment;
- A two-page informed consent form which also includes consent to the storage and processing of the patient’s personal data (in accordance with the General Data Protection Regulation) to be signed by the patient (or their legal representative) and the physician who provided information on the experimental phage therapy.
4.4. Treatment-Related Activity
4.5. Research Activity
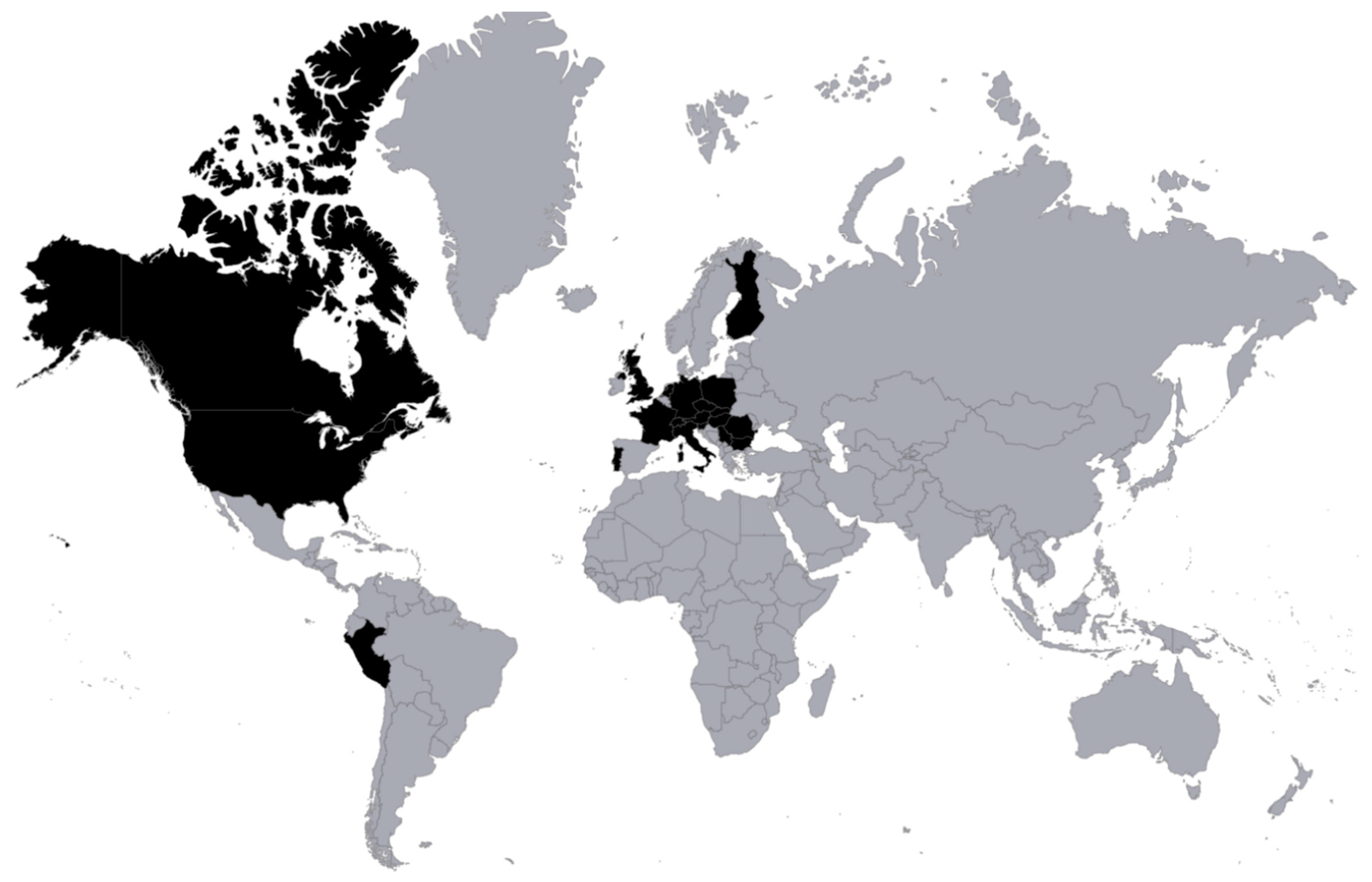
4.6. Polish and International Recognition
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Żaczek, M.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Łusiak-Szelachowska, M.; Górski, A. Phage Therapy in Poland—A Centennial Journey to the First Ethically Approved Treatment Facility in Europe. Front. Microbiol. 2020, 11, 1056. [Google Scholar] [CrossRef]
- Rubisz-Brzezińska, J.; Wilk-Czyż, R.; Brzezińska-Wcisło, L.; Kasprowicz, A. Ocena kliniczna ciezkich postaci tradzika leczonych autoszczepionka [Clinical evaluation of serious forms of acne treated with autovaccine]. Med. Dosw. Mikrobiol. 1994, 46, 35–42. (In Polish) [Google Scholar]
- Załuga, E. Odczyny skórne na antygeny Propionibacterium acnes u pacjentów z tradzikiem pospolitym leczonych autoszczepionka [Skin reactions to antigens of propionibacterium acnes in patients with acne vulgaris treated with autovaccine]. Ann. Acad. Med. Stetin. 1998, 44, 65–85. (In Polish) [Google Scholar]
- Letkiewicz, S. Phage Therapy of Antibiotic-Resistant Bacterial Infections as a Therapeutic Experiment—Ethical Aspects; Publishing House of the Medical University of Warsaw: Warsaw, Poland, 2015; ISBN 978-83-7637-322-5. [Google Scholar]
- Ślopek, S.; Weber-Dąbrowska, B.; Dąbrowski, M.; Kucharewicz-Krukowska, A. Results of bacteriophage treatment of suppurative bacterial infections in the years 1981–1986. Arch. Immunol. Ther. Exp. 1987, 35, 569–583. [Google Scholar]
- Ślopek, S.; Durlakowa, I.; Weber-Dąbrowska, B.; Kucharewicz-Krukowska, A.; Dąbrowski, M.; Bisikiewicz, R. Results of bacteriophage treatment of suppurative bacterial infections. I. General evaluation of the results. Arch. Immunol. Ther. Exp. 1983, 31, 267–291. [Google Scholar]
- Ślopek, S.; Durlakowa, I.; Weber-Dąbrowska, B.; Kucharewicz-Krukowska, A.; Dąbrowski, M.; Bisikiewicz, R. Results of bacteriophage treatment of suppurative bacterial infections. II. Detailed evaluation of the results. Arch. Immunol. Ther. Exp. 1983, 31, 293–327. [Google Scholar]
- Ślopek, S.; Durlakowa, I.; Weber-Dąbrowska, B.; Dąbrowski, M.; Kucharewicz- Krukowska, A. Results of bacteriophage treatment of suppurative bacterial infections. III. Detailed evaluation of the results obtained in further 150 cases. Arch. Immunol. Ther. Exp. 1984, 32, 317–335. [Google Scholar]
- Ślopek, S.; Durlakowa, I.; Weber-Dąbrowska, B.; Dąbrowski, M. Results of bacteriophage treatment of suppurative bacterial infections. IV. Evaluation of the results obtained in 370 cases. Arch. Immunol. Ther. Exp. 1985, 33, 219–240. [Google Scholar]
- Ślopek, S.; Durlakowa, I.; Weber-Dąbrowska, B.; Dąbrowski, M. Results of bacteriophage treatment of suppurative bacterial infections. V. Evaluation of the results obtained in children. Arch. Immunol. Ther. Exp. 1985, 33, 241–259. [Google Scholar]
- Ślopek, S.; Kucharewicz-Krukowska, A.; Weber-Dąbrowska, B.; Dąbrowski, M. Results of bacteriophage treatment of suppurative bacterial infections. VI. Analysis of treatment of suppurative staphylococcal infections. Arch. Immunol. Ther. Exp. 1985, 33, 261–273. [Google Scholar]
- Weber-Dąbrowska, B.; Dąbrowski, M.; Ślopek, S. Studies on bacteriophage penetration in patients subjected to phage therapy. Arch. Immunol. Ther. Exp. 1987, 35, 563–568. [Google Scholar]
- Weber-Dąbrowska, B.; Mulczyk, M.; Gόrski, A. Bacteriophage therapy of bacterial infections: An update of our institute’s experience. Arch. Immunol. Ther. Exp. 2000, 48, 547–551. [Google Scholar]
- Aulisio, M.P. Why Did Hospital Ethics Committees Emerge in the US? AMA J. Ethics 2016, 18, 546–553. [Google Scholar] [CrossRef] [Green Version]
- Moon, M. Institutional Ethics Committees. Pediatrics 2019, 143, e20190659. [Google Scholar] [CrossRef] [Green Version]
- Crico, C.; Sanchini, V.; Casali, P.G.; Pravettoni, G. Evaluating the effectiveness of clinical ethics committees: A systematic review. Med. Health Care Philos. 2021, 24, 135–151. [Google Scholar] [CrossRef]
- Gobel, C.; Baier, D.; Ruhfus, B.; Hundt, F. GCP inspections in Germany and Europe following the implementation of the Directive 2001/20/EC. Ger. Med. Sci. 2009, 7, Doc01. [Google Scholar] [CrossRef]
- Borysowski, J.; Hans-Jorg, E.; Górski, A. Ethics review in compassionate use. BMC Med. 2017, 15, 136. [Google Scholar] [CrossRef] [Green Version]
- Verbeken, G.; Pirnay, J.P. European regulatory aspects of phage therapy: Magistral phage preparations. Curr. Opin. Virol. 2021, 52, 24–29. [Google Scholar] [CrossRef]
- Borysowski, J.; Górski, A. Compassionate use of unauthorized drugs: Legal regulations and ethical challenges. Eur. J. Intern. Med. 2019, 65, 12–16. [Google Scholar] [CrossRef]
- Singh, J.A.; Upshur, R.E.G. The granting of emergency use designation to COVID-19 candidate vaccines: Implications for COVID-19 vaccine trials. Lancet Infect. Dis. 2021, 21, e103–e109. [Google Scholar] [CrossRef]
- Gill, J.; Young, R.F. Therapeutic applications of phage biology: History, practice, and recommendations. In Emerging Trends in Antibacterial Discovery: Answering the Call to Arms; Miller, A.A., Miller, P.F., Eds.; Caister Academic Press: Norfolk, UK, 2011; pp. 367–410. [Google Scholar]
- Schmidt, H.; Mehring, S.; McMillan, J. Interpreting the declaration of Helsinki (2008): “must”, “should” and different kinds of obligation. Med. Law 2010, 29, 565–591. [Google Scholar]
- WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 10 February 2022).
- Międzybrodzki, R.; Hoyle, N.; Zhvaniya, F.; Łusiak-Szelachowska, M.; Weber-Dąbrowska, B.; Łobocka, M.; Borysowski, J.; Alavidze, Z.; Kutter, E.; Górski, A.; et al. Current Updates from the Long-Standing Phage Research Centers in Georgia, Poland, and Russia. In Bacteriophages; Harper, D., Abedon, S., Burrowes, B., McConville, M., Eds.; Springer: Cham, Switzerland, 2018; pp. 1–31. [Google Scholar] [CrossRef]
- Brodniewicz, T. Badania Kliniczne; CeDeWu: Warsaw, Poland, 2016; ISBN 978-83-7556-894-3. (In Polish) [Google Scholar]
- Drzycimski, A. Bioethical Committees and the Progress in Biomedicine. Studia Pelplińskie 2014, 47, 73–96. (In Polish) [Google Scholar]
- European Network of Research Ethics Committees. Available online: http://www.eurecnet.org/information/poland.html (accessed on 10 February 2022).
- Ślęczek-Czakon, D. The role of bioethics committee in evaluating the reliability of medical experiments on people. Rocz. Lubus. 2020, 46, 219–231. (In Polish) [Google Scholar] [CrossRef]
- Information on Medical Center Activity. Available online: https://hirszfeld.pl/en/structure/iitd-pan-medical-center/ (accessed on 5 March 2022).
- Międzybrodzki, R.; Borysowski, J.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Szufnarowski, K.; Pawełczyk, Z.; Rogόż, P.; Kłak, M.; Wojtasik, E.; et al. Clinical aspects of phage therapy. Adv. Virus. Res. 2012, 83, 73–121. [Google Scholar] [CrossRef]
- Łusiak-Szelachowska, M.; Żaczek, M.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Kłak, M.; Fortuna, W.; Letkiewicz, S.; Rogόż, P.; Szufnarowski, K.; Jończyk-Matysiak, E.; et al. Phage neutralization by sera of patients receiving phage therapy. Viral. Immunol. 2014, 27, 295–304. [Google Scholar] [CrossRef] [Green Version]
- Łusiak-Szelachowska, M.; Żaczek, M.; Weber-Dąbrowska, B.; Kłak, M.; Międzybrodzki, R.; Fortuna, W.; Rogόż, P.; Szufnarowski, K.; Jończyk-Matysiak, E.; Gόrski, A. Antiphage activity of sera from patients receiving staphylococcal phage preparations. In Microbes in the Spotlight: Recent Progress in the Understanding of Beneficial and Harmful Microorganisms; Méndez-Vilas, A., Ed.; BrownWalker Press: Boca Raton, FL, USA, 2016; pp. 245–249. [Google Scholar]
- Łusiak-Szelachowska, M.; Żaczek, M.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Letkiewicz, S.; Fortuna, W.; Rogόż, P.; Szufnarowski, K.; Jończyk-Matysiak, E.; Olchawa, E.; et al. Antiphage activity of sera during phage therapy in relations to its outcome. Future Microbiol. 2017, 12, 109–117. [Google Scholar] [CrossRef]
- Letkiewicz, S.; Łusiak-Szelachowska, M.; Międzybrodzki, R.; Żaczek, M.; Weber-Dąbrowska, B.; Górski, A. Low Immunogenicity of Intravesical Phage Therapy for Urogenitary Tract Infections. Antibiotics 2021, 10, 627. [Google Scholar] [CrossRef]
- Żaczek, M.; Łusiak-Szelachowska, M.; Jończyk-Matysiak, E.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Owczarek, B.; Kopciuch, A.; Fortuna, W.; Rogόż, P.; Gόrski, A. Antibody production in response to staphylococcal MS-1 phage cocktail in patients undergoing phage therapy. Front. Microbiol. 2016, 7, 1681. [Google Scholar] [CrossRef] [Green Version]
- Żaczek, M.; Łusiak-Szelachowska, M.; Weber-Dąbrowska, B.; Międzybrodzki, R.; Fortuna, W.; Rogóż, P.; Letkiewicz, S.; Górski, A. Humoral Immune Response to Phage-Based Therapeutics. In Phage Therapy: A Practical Approach; Górski, A., Międzybrodzki, R., Borysowski, J., Eds.; Springer: Cham, Switzerland, 2019; pp. 123–143. [Google Scholar]
- Abedon, S.T.; Kuhl, S.J.; Blasdel, B.G.; Kutter, E.M. Phage treatment of human infections. Bacteriophage 2011, 1, 66–85. [Google Scholar] [CrossRef] [Green Version]
- Rohde, C.; Wittmann, J.; Kutter, E. Bacteriophages: A Therapy Concept against Multi-Drug-Resistant Bacteria. Surg. Infect. 2018, 19, 737–744. [Google Scholar] [CrossRef] [Green Version]
- Rogóż, P.; Amanatullah, D.F.; Międzybrodzki, R.; Manasherob, R.; Tikunova, N.V.; Weber-Dąbrowska, B.; Fortuna, W.; Letkiewicz, S.; Górski, A. Phage Therapy in Orthopaedic Implant-Associated Infections. In Phage Therapy: A Practical Approach; Górski, A., Międzybrodzki, R., Borysowski, J., Eds.; Springer: Cham, Switzerland, 2019; pp. 189–211. [Google Scholar]
- Letkiewicz, S.; Międzybrodzki, R.; Fortuna, W.; Weber-Dąbrowska, B.; Górski, A. Eradication of Enterococcus faecalis by phage therapy in chronic prostatitis—Case report. Folia Microbiol. 2009, 54, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Łusiak-Szelachowska, M.; Międzybrodzki, R.; Fortuna, W.; Borysowski, J.; Górski, A. Anti-phage serum antibody responses and the outcome of phage therapy. Folia Microbiol. 2021, 66, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Międzybrodzki, R.; Fortuna, W.; Weber-Dąbrowska, B.; Górski, A. A retrospective analysis of the changes in inflammatory markers in patients treated with bacterial viruses. Clin. Exp. Med. 2009, 9, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Rostkowska, O.M.; Międzybrodzki, R.; Miszewska-Szyszkowska, D.; Górski, A.; Durlik, M. Treatment of recurrent urinary tract infections in a 60-year-old kidney transplant recipient. The use of phage therapy. Transpl. Infect. Dis. 2021, 23, e13391. [Google Scholar] [CrossRef]
- Weber-Dąbrowska, B.; Jończyk-Matysiak, E.; Żaczek, M.; Łobocka, M.; Łusiak-Szelachowska, M.; Gόrski, A. Bacteriophage Procurement for Therapeutic Purposes. Front. Microbiol. 2016, 7, 1177. [Google Scholar] [CrossRef]
- National Centre for Research and Development “Innovative 2013” Newsletter. Available online: https://archiwum.ncbr.gov.pl/fileadmin/gfx/ncbir/userfiles/_public/monitoring/publikacje/innowacyjni2013_220713_ang_22.07.2013.pdf (accessed on 13 March 2022).
- Borysowski, J.; Międzybrodzki, R.; Górski, A. Phage Therapy: Current Research and Applications; Caister Academic Press: Norfolk, UK, 2014; ISBN 978-1-908230-40-9. [Google Scholar]
- Górski, A.; Międzybrodzki, R.; Borysowski, J. PhageTherapy: A Practical Approach; Springer: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Keen, E.C.; Adhya, S.L. Phage Therapy: Current Research and Applications. Clin. Infect. Dis. 2015, 61, 141–142. [Google Scholar] [CrossRef] [Green Version]
- Asavarut, P.; Hajitou, A. The phage revolution against antibiotic resistance. Lancet Infect. Dis. 2014, 14, 686. [Google Scholar] [CrossRef]
- Abedon, S.T. Bringing phage therapy soon to a clinic near you. Lancet Infect. Dis. 2020, 20, 551. [Google Scholar] [CrossRef]
- Hausler, T. Bug killers. Nat. Med. 2006, 12, 600–601. [Google Scholar] [CrossRef]
- Augustyn, A. Wrocławskie fagi dla obcokrajowców. Gaz. Wybor. 2007, 16, 5. (In Polish) [Google Scholar]
- Grand Prix Plebiscytu Travelery 2007 Dla Elżbiety Dzikowskiej. Available online: https://www.press.pl/tresc/11662,grand-prix-plebiscytu-travelery-2007-dla-elzbiety-dzikowskiej (accessed on 2 March 2022). (In Polish).
- Koton-Czarnecka, M. Wygrała terapia fagowa. Puls. Med. 2009, 10, 7–10. (In Polish) [Google Scholar]
- Pirnay, J.P.; De Vos, D.; Verbeken, G. Clinical application of bacteriophages in Europe. Microbiol. Aust. 2019, 40, 8–15. [Google Scholar] [CrossRef] [Green Version]
- Michael Mosley, vs. The Superbugs. Available online: https://www.bbc.co.uk/programmes/b08qkz77 (accessed on 10 April 2022).
- Heilen Ohne Antibiotika. Available online: https://www.phoenix.de/sendungen/dokumentationen/heilen-ohne-antibiotika-a-1384555.html (accessed on 10 April 2022).
- Dokters van Morgen. Available online: https://www.npostart.nl/dokters-van-morgen/05-02-2019/AT_2114969 (accessed on 10 April 2022).
- 19-Letni Peruwiańczyk Przybył Do Polski, By Poddać Się Terapii Ratującej Życie. Available online: https://everethnews.pl/newsy/19-letni-peruwianczyk-przybyl-do-polski-by-poddac-sie-terapii-ratujacej-zycie/ (accessed on 10 April 2022). (In Polish).
- Górski, A.; Bollyky, P.L.; Przybylski, M.; Borysowski, J.; Międzybrodzki, R.; Jończyk-Matysiak, E.; Weber-Dąbrowska, B. Perspectives of Phage Therapy in Non-bacterial Infections. Front. Microbiol. 2019, 9, 3306. [Google Scholar] [CrossRef] [PubMed]
- Górski, A.; Borysowski, J.; Międzybrodzki, R. The contribution of phage therapy to medical knowledge. J. Glob. Antimicrob. Resist. 2022, 28, 238–240. [Google Scholar] [CrossRef]
- Górski, A.; Jończyk-Matysiak, E.; Łusiak-Szelachowska, M.; Międzybrodzki, R.; Weber-Dąbrowska, B.; Borysowski, J.; Letkiewicz, S.; Bagińska, N.; Sfanos, K.S. Phage Therapy in Prostatitis: Recent Prospects. Front. Microbiol. 2018, 9, 1434. [Google Scholar] [CrossRef]
- Górski, A.; Międzybrodzki, R.; Węgrzyn, G.; Jończyk-Matysiak, E.; Borysowski, J.; Weber-Dąbrowska, B. Phage therapy: Current status and perspectives. Med. Res. Rev. 2020, 40, 459–463. [Google Scholar] [CrossRef]
- Petrovic Fabijan, A.; Lin, R.C.Y.; Ho, J.; Maddocks, S.; Ben Zakour, N.L.; Iredell, J.R.; Westmead Bacteriophage Therapy Team. Safety of bacteriophage therapy in severe Staphylococcus aureus infection. Nat. Microbiol. 2020, 5, 465–472. [Google Scholar] [CrossRef]
- Chen, P.; Liu, Z.; Tan, X.; Wang, H.; Liang, Y.; Kong, Y.; Sun, W.; Sun, L.; Ma, Y.; Lu, H. Bacteriophage therapy for empyema caused by carbapenem-resistant Pseudomonas aeruginosa. BioSci. Trends. 2022, 16, 158–162. [Google Scholar] [CrossRef]
- Sweere, J.M.; Van Belleghem, J.D.; Ishak, H.; Bach, M.S.; Popescu, M.; Sunkari, V.; Kaber, G.; Manasherob, R.; Suh, G.A.; Cao, X.; et al. Bacteriophage trigger antiviral immunity and prevent clearance of bacterial infection. Science. 2019, 363, eaat9691. [Google Scholar] [CrossRef]
- Adiliaghdam, F.; Amatullah, H.; Digumarthi, S.; Saunders, T.L.; Rahman, R.U.; Wong, L.P.; Sadreyev, R.; Droit, L.; Paquette, J.; Goyette, P.; et al. Human enteric viruses autonomously shape inflammatory bowel disease phenotype through divergent innate immunomodulation. Sci Immunol. 2022, 7, eabn6660. [Google Scholar] [CrossRef]
- Bao, H.; Zhang, H.; Zhou, Y.; Zhu, S.; Pang, M.; Zhang, X.; Wang, Y.; Wang, J.; Olaniran, A.; Xiao, Y.; et al. Dysbiosis and intestinal inflammation caused by Salmonella Typhimurium in mice can be alleviated by preadministration of a lytic phage. Microbiol. Res. 2022, 260, 127020. [Google Scholar] [CrossRef]
- Safari, Z.; Sadeghizadeh, M.; Asgaritarghi, G.; Bardania, H.; Sadeghizadeh, D.; Soudi, S. M13 phage coated surface elicits an anti-inflammatory response in BALB/c and C57BL/6 peritoneal macrophages. Int. Immunopharmacol. 2022, 107, 108654. [Google Scholar] [CrossRef] [PubMed]
- Górski, A.; Międzybrodzki, R.; Jończyk-Matysiak, E.; Żaczek, M.; Borysowski, J. Phage-specific diverse effects of bacterial viruses on the immune system. Future Microbiol. 2019, 14, 1171–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du Toit, A. Remember the phages. Nat. Rev. Microbiol. 2022, 20, 254. [Google Scholar] [CrossRef] [PubMed]
- Thompson, T. The staggering death toll of drug-resistant bacteria. Nature 2022. online article. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Numbers |
|---|---|
| Patients registered at the PTU | 2207 (including 126 in Kraków branch and 13 in Częstochowa branch) |
| Visits/consultations registered at the PTU | 6207 (including 303 in Kraków branch and 16 in Częstochowa branch) |
| Patients qualified for experimental phage therapy at the PTU | 791 (including 37 in Kraków branch and 0 in Częstochowa branch) |
| Type of Infection | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | UTI | GTI | PI | URTI | LRTI | P | SI | C ^ | O | BNI | BLI |
| 2006 | 25 | 7 | 61 | 30 | 6 | 12 | 10 | - | 3 | 4 | 2 |
| 2007 | 9 | 2 | 27 | 3 | 5 | 11 | - | - | 2 | 3 | - |
| 2008 | 19 | 6 | 55 | 22 | - | 16 | 7 | 1 | 3 | 5 | - |
| 2009 | 21 | 7 | 5 | 17 | - | 16 | 57 | - | 3 | 3 | 1 |
| 2010 | 15 | 9 | 7 | 21 | - | 6 | 42 | 1 | 4 | 6 | 2 |
| 2011 | 13 | 10 | 11 | 25 | - | 14 | 27 | - | 3 | 14 | 2 |
| 2012 | 19 | 5 | 19 | 20 | 2 | 13 | 37 | 1 | 3 | 12 | - |
| 2013 | 9 | 2 | 7 | 13 | 1 | 15 | 29 | - | 2 | 9 | - |
| 2014 | 19 | 9 | 10 | 16 | 3 | 11 | 41 | - | 3 | 7 | 1 |
| 2015 | 31 | 10 | 15 | 22 | - | 16 | 41 | - | 3 | 21 | 2 |
| 2016 | 41 | 8 | 10 | 24 | - | 22 | 48 | - | 6 | 13 | 1 |
| 2017 | 31 | 11 | 2 | 20 | - | 15 | 36 | 2 | 2 | 10 | - |
| 2018 | 38 | 5 | 5 | 20 | - | 21 | 36 | - | 6 | 10 | 1 |
| 2019 | 57 | 11 | 11 | 23 | - | 18 | 40 | - | 3 | 12 | - |
| 2020 | 25 | 3 | 1 | 7 | - | 18 | 21 | - | 9 | - | |
| 2021 | 47 | 3 | 5 | 13 | - | 21 | 27 | - | 3 | 11 | - |
| Total | 419 | 108 | 251 | 296 | 17 | 245 | 499 | 5 | 49 | 149 | 12 |
| Phage Typing | |||
|---|---|---|---|
| Year | Positive Results (%) | Negative Results (%) | Total Number of Typed Isolates |
| 2006 | 203 (79.0) | 54 (21.0) | 257 |
| 2007 | 216 (82.4) | 46 (17.6) | 262 |
| 2008 | 196 (78.4) | 54 (21.6) | 250 |
| 2009 | 188 (82.0) | 41 (18.0) | 229 |
| 2010 | 162 (92.0) | 14 (8.0) | 176 |
| 2011 | 130 (80.8) | 31 (19.2) | 161 |
| 2012 | 146 (84.3) | 27 (15.7) | 173 |
| 2013 | 123 (85.4) | 21 (14.6) | 144 |
| 2014 | 164 (81.6) | 37 (18.4) | 201 |
| 2015 | 165 (84.7) | 30 (15.3) | 195 |
| 2016 | 209 (82.0) | 46 (18.0) | 255 |
| 2017 | 134 (77.4) | 39 (22.6) | 173 |
| 2018 | 130 (79.2) | 34 (20.8) | 164 |
| 2019 | 120 (76.4) | 37 23.6) | 157 |
| 2020 | 78 (79.6) | 20 (20.4) | 98 |
| 2021 | 79 (85.0) | 14 (15.0) | 93 |
| Total | 2443 (81.8) | 545 (18.2) | 2988 |
| Bacterial Strain | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | S. aureus | E. faecalis | E. coli | Kl. pneum. | Ent. cloac. | P. mirabilis | P. aeruginosa | S. marcescens | A. baumannii | M. morganii | Total |
| 2006 | 129 | 37 | 34 | 6 | 2 | 5 | 24 | 2 | 3 | 1 | 243 |
| 2007 | 111 | 37 | 35 | 1 | 1 | 5 | 44 | 3 | 2 | 2 | 241 |
| 2008 | 103 | 38 | 42 | 1 | 4 | 5 | 31 | 2 | 2 | - | 228 |
| 2009 | 115 | 30 | 31 | - | 3 | 2 | 31 | - | 1 | - | 219 |
| 2010 | 30 | 24 | 18 | 8 | 2 | 2 | 35 | 2 | 3 | 3 | 127 |
| 2011 | 69 | 22 | 19 | 6 | 1 | 3 | 36 | 2 | 2 | 2 | 162 |
| 2012 | 89 | 14 | 27 | 7 | - | 3 | 36 | 1 | 2 | 2 | 181 |
| 2013 | 69 | 17 | 12 | 3 | 3 | 4 | 44 | 1 | 1 | - | 154 |
| 2014 | 81 | 29 | 23 | 11 | 5 | 3 | 45 | - | 1 | - | 198 |
| 2015 | 66 | 26 | 38 | 19 | 3 | 6 | 28 | - | 1 | - | 187 |
| 2016 | 86 | 27 | 38 | 34 | 6 | 5 | 44 | 2 | 1 | 3 | 246 |
| 2017 | 58 | 24 | 43 | 30 | 3 | 5 | 30 | 2 | 7 | 2 | 204 |
| 2018 | 55 | 32 | 39 | 26 | 4 | 4 | 32 | 5 | 2 | 1 | 200 |
| 2019 | 42 | 19 | 36 | 34 | 4 | 4 | 43 | 4 | - | 2 | 188 |
| 2020 | 25 | 19 | 24 | 17 | 3 | 4 | 6 | - | - | 2 | 100 |
| 2021 | 24 | 18 | 31 | 20 | 3 | 5 | 18 | 1 | 1 | 1 | 122 |
| Total | 1152 | 413 | 490 | 223 | 47 | 72 | 527 | 26 | 29 | 21 | 3000 |
| Type of Phage Preparation | ||||||
|---|---|---|---|---|---|---|
| Year | Staphylococcus | Enterococcus | Escherichia | Klebsiella | Pseudomonas | Total |
| 2006 | 105 | 35 | 26 | 0 | 4 | 170 |
| 2007 | 102 | 30 | 17 | 0 | 15 | 164 |
| 2008 | 98 | 21 | 17 | 0 | 10 | 146 |
| 2009 | 120 | 21 | 16 | 2 | 21 | 180 |
| 2010 | 67 | 35 | 18 | 9 | 20 | 149 |
| 2011 | 46 | 28 | 19 | 4 | 11 | 108 |
| 2012 | 73 | 9 | 43 | 11 | 22 | 158 |
| 2013 | 80 | 24 | 18 | 3 | 45 | 170 |
| 2014 | 84 | 33 | 30 | 6 | 39 | 192 |
| 2015 | 58 | 27 | 59 | 12 | 15 | 171 |
| 2016 | 84 | 33 | 34 | 14 | 20 | 185 |
| 2017 | 59 | 18 | 32 | 9 | 18 | 136 |
| 2018 | 66 | 21 | 23 | 19 | 22 | 151 |
| 2019 | 50 | 27 | 27 | 18 | 27 | 149 |
| 2020 | 24 | 20 | 10 | 9 | 1 | 64 |
| 2021 | 27 | 18 | 32 | 12 | 16 | 105 |
| Total | 1143 | 400 | 421 | 128 | 306 | 2398 * |
| Employee | Citations and H-Index acc. to Scopus | Citations and H-Index acc. to Web of Science |
|---|---|---|
| Prof. Andrzej Górski, M.D., Ph.D. | 5698 (44) | 5405 (43) |
| Beata Weber-Dąbrowska, Ph.D. | 3691 (40) | 2752 (33) |
| Assoc. Prof. Ryszard Międzybrodzki, M.D., Ph.D. | 2522 (27) | 2302 (26) |
| Prof. Krystyna Dąbrowska, Ph.D. | 2072 (27) | 2218 (30) |
| Wojciech Fortuna, M.D., Ph.D. | 1517 (19) | 1396 (17) |
| Marzanna Łusiak-Szelachowska, Ph.D. | 1026 (17) | 964 (17) |
| Ewa Jończyk-Matysiak, Ph.D. | 993 (19) | 965 (19) |
| Assoc. Prof. Sławomir Letkiewicz, M.D., Ph.D. | 937 (12) | 923 (11) |
| Paweł Rogóż, M.D. | 670 (8) | 660 (8) |
| Barbara Owczarek, M.Sc., Eng. | 569 (13) | 514 (13) |
| Maciej Żaczek, M.Sc. | 545 (12) | 505 (11) |
| Paulina Miernikiewicz, Ph.D. | 542 (12) | 522 (12) |
| Zuzanna Kaźmierczak, Ph.D. | 475 (9) | 457 (9) |
| Project Title | Principal Investigator | Funds (PLN) * | Funding Institution | Years |
|---|---|---|---|---|
| Optimization of the production and characterization of bacteriophage preparation for therapeutic use | Prof. Andrzej Górski, M.D., Ph.D. | 6,026,360 | National Centre for Research and Development | 2009–2014 |
| Use of bacteriophages to develop antibacterial preparations in veterinary | Beata Weber-Dąbrowska, Ph.D. | 3,170,000 | Polish Agency for Enterprise Development | 2013–2015 |
| Biological stabilization of drinking water | Beata Weber-Dąbrowska, Ph.D. | 2,200,000 | National Centre for Research and Development | 2013–2015 |
| Identification of the influence of bacteriophages with therapeutic potential on mammalian cellular functions and the immune system | Prof. Krystyna Dąbrowska, Ph.D. | 1,445,000 | National Science Centre | 2013–2017 |
| Innovative bacteriophage preparation for the treatment of diabetic foot | Beata Weber-Dąbrowska, Ph.D. | 6,188,704 | National Centre for Research and Development | 2013–2015 |
| Antiviral activity of bacteriophages | Prof. Andrzej Górski, M.D., Ph.D. | 929,600 | National Science Centre | 2014–2017 |
| The differentiation of the immunological reactivity of endolysins as a factor determining the differences in their antimicrobial efficacy in vivo | Prof. Krystyna Dąbrowska, Ph.D. | 1,108,800 | National Science Centre | 2016–2019 |
| Development and implementation of a bacteriophage preparation used in the treatment and prevention of American foulbrood | Ewa Jończyk-Matysiak, Ph.D. | 4,524,769 | National Centre for Research and Development | 2017–2019 |
| Gastric microbiome in people infected with Helicobacter pylori | Prof. Krystyna Dąbrowska, Ph.D. | 1,751,400 | National Science Centre | 2019–2022 |
| PhageScan: Identification of bacteriophage epitopes significant to human health | Prof. Krystyna Dąbrowska, Ph.D. | 2,361,600 | National Science Centre | 2020–2024 |
| Study of the composition of a bacteriophage preparation specific to multidrug-resistant Acinetobacter baumannii clinical strains | Natalia Bagińska, M.Sc. Eng. | 800,000 | National Centre for Research and Development | 2021–2023 |
| Mechanisms of phage-derived “dark matter” interactions with the immune system of mammals | Prof. Krystyna Dąbrowska, Ph.D. | 2,038,200 | National Science Centre | 2021–2024 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żaczek, M.; Górski, A.; Weber-Dąbrowska, B.; Letkiewicz, S.; Fortuna, W.; Rogóż, P.; Pasternak, E.; Międzybrodzki, R. A Thorough Synthesis of Phage Therapy Unit Activity in Poland—Its History, Milestones and International Recognition. Viruses 2022, 14, 1170. https://doi.org/10.3390/v14061170
Żaczek M, Górski A, Weber-Dąbrowska B, Letkiewicz S, Fortuna W, Rogóż P, Pasternak E, Międzybrodzki R. A Thorough Synthesis of Phage Therapy Unit Activity in Poland—Its History, Milestones and International Recognition. Viruses. 2022; 14(6):1170. https://doi.org/10.3390/v14061170
Chicago/Turabian StyleŻaczek, Maciej, Andrzej Górski, Beata Weber-Dąbrowska, Sławomir Letkiewicz, Wojciech Fortuna, Paweł Rogóż, Edyta Pasternak, and Ryszard Międzybrodzki. 2022. "A Thorough Synthesis of Phage Therapy Unit Activity in Poland—Its History, Milestones and International Recognition" Viruses 14, no. 6: 1170. https://doi.org/10.3390/v14061170
APA StyleŻaczek, M., Górski, A., Weber-Dąbrowska, B., Letkiewicz, S., Fortuna, W., Rogóż, P., Pasternak, E., & Międzybrodzki, R. (2022). A Thorough Synthesis of Phage Therapy Unit Activity in Poland—Its History, Milestones and International Recognition. Viruses, 14(6), 1170. https://doi.org/10.3390/v14061170