
Alpha-1 Acid Glycoprotein Reduction Differentiated Recovery from Remission in a Small Cohort of Cats Treated for Feline Infectious Peritonitis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Cases
2.2. FIP Diagnosis
2.3. Treatment
2.4. Outcomes: Death, Recovery, or Remission
2.5. AGP
2.6. Statistics
3. Results
3.1. FIP Diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cat | FIP Presentation | How FIP Diagnosed | Survival in Years or Months | Time to Normal AGP | Treatments | Prednisolone/Corticosteroids | |
|---|---|---|---|---|---|---|---|
| 1 | Basil 1 | Non-effusive (icterus) | mRNA RT-PCR on PBMC positive thrice. | 11y † (Died of chronic kidney disease aged 15y.) | <22d | 5 × 104 units of rFeIFN-ω (Virbagen Omega, Virbac, Nice, France) per os q24h for 13m until FCoV antibody titre reduced from >1280 to <1:10. | 2 mg/kg q24h for 7d then 1 mg/kg for 7d |
| 2 | Boris | Non-effusive but initially effusive FIP suspected | RT-qPCR on MLN FNA CT 33.7. RT-qPCR on ascites negative. | >2.2y | <3m | 1 MU units rFeIFN-ω per os q24h. PI 3 mg/kg per os q72h. Weekly cobalamin injections. Effusion was negative on RT-PCR and was found to be due to cardiomyopathy. | No |
| 3 | Mars | Non-effusive | RT-qPCR on MLN FNA CT 30. | >5.5y | <6m | PI 3 mg/kg twice per week. | No |
| 4 | Chester | Effusive (pleural effusion) | RT-qPCR on pleural effusion CT 34. | >3.1y | <8m | 1 MU/kg rFeIFN-ω s/c q48h reduced to q4d then 1 × 105 units per os q24h for 28m. Meloxicam. SAMe (Denamarin®, Nutramax Laboratories, Inc., Lancaster, SC, USA) Cobalamin (Cobalaplex, Protexin® Veterinary, Somerset, UK). Tramadol hydrochloride (Bova Specials, London, UK) 10 mg/cat q24h per os. [48] Liquorice tea was attempted but cat did not like it. | 1 mg/kg q12h for 2w, weaned off for another 3w and replaced by meloxicam |
| 5 | Amy | Non-effusive | FIP profile. | >1.3y | <4m | 1 MU units rFeIFN-ω s/c q48h. | Sliding doses |
| 6 | Brook | Non-effusive | FIP profile. | >1.1y | <41d | Unknown. | Unknown |
| 7 | Basil 2 | Effusive (ascites) | RT-qPCR on ascites positive. | >3.0y | <10w | 1 MU/kg rFeIFN-ω s/c q24h for 36d, reducing to every 3d, followed by 1 × 105 units of rFeIFN-ω per os q24h for 2y. PI at 3 mg/kg q48h during 10d. Mirtazapine (Summit Veterinary Pharmaceuticals, Kidlington, UK.) Ursodeoxychloic acid. Cobalamin injections weekly. Itraconazole 10 mg/kg from days 4–87. One Darbepoetin injection. GC-376 s/c Days 17–100. Doxycycline 10 mg/kg bid per os from d.32 for 30d (to treat haemotropic mycoplasmosis). | Only for 3d: meloxicam used in preference from Day 4 |
| 8 | Kitten 2 | Effusive (ascites) then non-effusive | FIP Profile. | >2y | <6m | 57d of Mutian X (Xraphconn®, Mutian Biotechnology Co., Ltd., Nantong, China) at 80 mg/kg. Following her neurological relapse, she was re-treated with 160 mg/kg for 2 m then 1 × 105 units of rFeIFN-ω per os q24h. | No |
| 9 | Skywise | Non-effusive | RT-qPCR on MLN FNA positive for mutation M1058L, negative for S1060A. | >2.0y | <35d | 50d Mutian X starting 160 mg/kg q24h per os in divided doses, reduced to 120 mg/kg on Day 25; followed by 1 × 105 units of rFeIFN-ω per os q24h. Cobalamin (Cobalaplex). | 6d per os, then in eye drops for 14d |
| 10 | Betsy | Effusive (ascites) | RT-qPCR on ascites CT 25.6. | >1.5y | <39d | 38d Mutian X 80 mg/kg per os for 31d and 160 mg/kg for 7d followed by 1 × 105 units of rFeIFN-ω per os q24h for 1y. Doxycycline. | 5 mg/cat q24h for 10d replaced by meloxicam |
| 11 | Dante | Colonic FIP | Histopath of biopsies positive. | >7m | <28d | 84d of Mutian X 80 mg/kg per os. Protexin pro-kolin enterogenic probiotics 2 mL per os q12h. Cobalamin (Cobalaplex). | No: gabapentin 25 mg q8h |
| 12 | Elmo | Non-effusive | Biopsy histopath reported pyogranuloma. | >17m | <31d | 54d Mutian X (160 mg/kg for 37d, then 80 mg/kg) followed by 1 × 105 units of rFeIFN-ω per os q24h. | One injection and one 5 mg pill given once only |
| 13 | Lyra | Effusive (ascites) | RT-qPCR on ascites: low positive CT 33. | >13m | <20d | 47d Mutian X 80 mg/kg q24h (divided doses) per os followed by 1 × 105 units of rFeIFN-ω per os q24h for 5m. | No: meloxicam given instead |
| 14 | Molly | Non-effusive | FIP profile. RT-PCR positive feces over 24m. | >3.3y | <16m | 1 × 105 units of rFeIFN-ω per os q24h, gabapentin, cefovecin (Convenia, Zoetis, Surrey, UK), Synbiotic D-C probiotics (Protexin). | Sliding doses (unspecified) then meloxicam |
| 15 | Bea | Effusive (ascites) | RT-PCR on ascites positive. Histopath biopsy positive. | 13m † (died of cancer, aged 8y) | <69d | 94d of Mutian X: 40 mg/kg (i.e., half dose) for 4d, then 80 mg/kg for 90d, except for one week of double dose, followed by 1 × 105 units of rFeIFN-ω per os q24h for 6 m. Robenacoxib (Onsior, Elanco Animal Health, Hampshire, UK) given once only. | No |
| 16 | Buddie | Effusive (ascites) | RT-PCR on ascites: CT 33. Histopath of MLN, spleen, liver biopsies positive. | >14m | <51d | 69d of Mutian X 80 mg/kg with 160 mg/kg in the 3rd week of treatment; followed by 1 × 105 units of rFeIFN-ω per os q24h for 6m. Cobalamin (Cobalaplex); SAMe (Denamarin). | One dexamethasone injection only |
| 17 | Nelson | Non-effusive becoming effusive | IHC of MLN biopsy positive. | >6m | <36d | 52d of Mutian X: 7d at 160 mg/kg, reduced to 120 mg/kg then 80 mg/kg; followed by 1 × 105 units of rFeIFN-ω per os q24h. Also cobalamin (Cobalaplex); amoxycillin and clavulanic acid (Synulox, Zoetis, Surrey, UK), mirtazapine; cobalamin (Cobalaplex); SAMe (Denamarin). | No: meloxicam instead |
| 18 | Wish | Non-effusive | IHC of MLN biopsy positive, RT-PCR positive (negative for mutations). | >12m | <13d but no initial test, so no proof it was ever raised | 29d of Mutian X: 7d at 160 mg/kg and 22d at 80 mg/kg; followed by 1 × 105 units of rFeIFN-ω per os q24h. Cobalamin (Cobalaplex); Denamarin. | For 7d only |
| 19 | Mike | Non-effusive (colonic) | Biopsy histopath positive. | >2.5y | unknown: AGP tested only once after 1 y of treatment | 1 × 105 units rFeIFN-ω per os q24h for 5m, meloxicam and PI, followed by 12 w of GS-441524 injections (DC Chemicals, USA), followed by 1 × 105 units of rFeIFN-ω per os q24h, and PI. | No |
| 20. | Chynah | Effusive (pleural effusion) | RT-PCR on pleural effusion CT 33. | >7m | remained raised > 3m | rFeIFN-ω 1 MU/kg s/c q48h, reducing to twice weekly for 5m. Repeated drainage of effusion. | 2.5 mg/cat q24h sliding doses |
| 21 | Tabitha | Non-effusive | FIP profile. | >12m | <29d | 58d of Mutian X starting at 160 mg/kg for 8d, then 120 mg/kg for 20d then 80 mg/kg; followed by 1 × 105 units of rFeIFN-ω per os q24h. Protexin pro-kolin enterogenic probiotics. | No: meloxicam |
| 22 | Harry | Small amount of ascites and enlarged MLN | FCoV RT-PCR positive. Cytology and IHC MLN biopsy inconclusive. | >8m | <30d | 50d of Mutian X: 43d at 80 mg/kg then 7d at 160 mg/kg; followed by 1 × 105 units of rFeIFN-ω per os q24h. Cobalamin, SAMe. | 5.0 mg /cat q12h for 5d |
| 23 | Mr Twinkles | Effusive (ascites) | FIP profile. | >8m | <117d | 7 mg/kg Spark [53] injection s/c for 10d, followed by 4 Spark 5 mg tablets (i.e., 7 mg/kg) per os q24h for 84d. Cobalamin (Cobalaplex). Denamarin. | No |
| 24 | Tyra | Non-effusive (uveitis) | FIP profile. | >10m | <68d | Pine and Lucky 9 [53] injections (12–14 mg/kg): Pine for 4d, Lucky injections for 68d. Then 9 Lucky red pills per os q24h for 13d. | No |
| 25 | Munchie | Effusive (ascites) | FIP profile. | >1.5y | <108d | Spark 8 mg/kg per os q24h for 84d. | No |
| 26 | Edward | Effusive (pleural effusion) | FIP profile incuding cytology. | 10m († RTA) | <7m | rFeIFN-ω 1 MU/kg s/c q48h, meloxicam per os q24h. | No |
| Cat | FIP Presentation | How FIP Diagnosed | Survival in Months | Treatments | Prednisolone/Corticosteroids | |
|---|---|---|---|---|---|---|
| 1 | Yrael | Effusive | RT-qPCR on effusion CT 32. | 1.5 † | Coconut oil and draining the effusion. | Unknown |
| 2 | Charlie Chaplin | Non-effusive | RT-qPCR on MLN FNA CT 25. Histopath positive. | 1.5 † | 1 × 105 rFeIFN-ω per os q24h. Clindamycin for toxoplasmosis co-infection. | ✓ |
| 3 | Smokey | Non-effusive | RT-qPCR on MLN FNA CT 28. Histopath positive. | 1.8 † | Adipose stem cell therapy. | Unknown |
| 4 | Rowley | Effusive (ascites), then non-effusive (uveitis, finally severe haemolytic anaemia) | RT-qPCR on ascites CT 28.4. Histopath positive. | 2.25 † | 1 MU/kg rFeIFN-ω s/c q48h resulted in resolution of his ascites then 1 × 105 units per os q24h. Mirtazapine 3 times. Anti-TNF-alpha monoclonal antibody infliximab, (Remicade®, MSD, London, UK) 4 mg/kg in a 0.9% saline infusion over a 4h period. Type B blood transfusion. | ✓ 5 mg q12h, dose not reduced |
| 5 | Claude | Effusive (pleural effusion initially then also ascites) | Partial FIP profile. | 3.0 † | 1 MU/kg rFeIFN-ω s/c q48h. Thoracentesis. | ✓ 1 mg/kg sliding doses |
| 6 | Alfie | Non-effusive (chronic diarrhoea, enlarged MLN) | RT-qPCR on MLN FNA CT 31, on feces CT 29. Histopath positive. | 3.5 † | rFeIFN-ω given per os, but dose not recorded. Fortiflora probiotics (Purina). | ✓ dose not recorded |
| 7 | Holly | Non-effusive to effusive ascites | mRNA and 3′UTR RT-PCR on ascites positive. | 4 † | 5 × 104 rFeIFN-ω per os. Colloidal silver (dose unknown). | Unknown |
| 8 | Bugsy | Non-effusive | FIP Profile. | 6 † | 1 MU/kg rFeIFN-ω s/c q48h then 1 × 105 units per os q24h. | ✓5 mg eod |
| 9 | Daisy | Non-effusive | RT-qPCR on MLN FNA CT 27. | 5 † | 1 MU/kg rFeIFN-ω s/c q48h then once a week, then 5 × 104 units rFeIFN-ω per os q24h. | ✓ higher dose reduced to 0.5 mg/kg q24h after 14d |
| 10 | Levi | Effusive (ascites) | RT-qPCR on ascites CT 33. | 5.5 † | 1 MU/kg rFeIFN-ω s/c twice a week. Ascites drained. | ✓dose not recorded |
| 11 | Roxanne | Non-effusive and FGS | RT-qPCR on PBMC CT 42 (very low positive), on faeces CT 23. | 11 † | 1 MU/kg rFeIFN-ω s/c twice weekly. Clindamycin (Antirobe, Zoetis, Surrey, UK), meloxicam. | No: meloxicam |
| 12 | Pip | Non-effusive | RT-qPCR on PBMC CT 40 (very low positive) twice. | >12 | 5 × 104 units rFeIFN-ω per os q24h. | ✓10 mg/cat pred q24h reducing to 5 mg q24h |
| 13 | Pharaoh | Non-effusive | RT-PCR on MLN biopsy CT 27. MLN biopsy inconclusive. | 8 † | Adipose stem cell therapy. | Unknown |
| 14 | Maximus | Non-effusive | RT-PCR on MLN FNA positive. | 14 † | 1 MU /kg rFeIFN-ω s/c q48h | 5 mg/cat q24h |
| 15 | Ragamuffin | Non-effusive | Biopsy MLN & intestine inconclusive. | >60 | 1 MU/kg rFeIFN-ω s/c q48h then 1 × 105 units per os q24h then 1 MU/kg rFeIFN-ω twice a week | ✓Sliding doses |
| 16 | Tinkerbell | Non-effusive | FIP Profile. RT-qPCR on feces CT 31–34. | >36 | 1 MU/kg rFeIFN-ω s/c q48h then 1 × 105 units per os q24h. PI. Mirtazapine 2 mg/cat q48h. | ✓For over 1y at 2 mg/kg q24h |
| Cat | Clinical Signs | FCoV Antibody Titre (Interval First to Last) | Anaemia i.e., Hct <30% | Lymphopenia <1.5 × 109/L | Hyperglobulinaemia i.e., >45 g/L | Score | ||
|---|---|---|---|---|---|---|---|---|
| Before | After | |||||||
| 1 | Basil 1 | Icterus | 1280/10 (13m) | ✓/✗ (22d) | ✓/✗ | ✓/✗ (63–43) | 5 | 0 |
| 2 | Boris | Poor appetite, diarrhoea | >1280/160 (4m) | ✗ | ✗ | ✗ (34–40) | 2 | 1 |
| 3 | Mars | Anorexia | >1280/320 (18m) | ✗ | ✓/✗ | ✓/✗ (69–42) | 4 | 1 |
| 4 | Chester | Pleural effusion, pyrexia | >1280/1280 (28m) | ✗ * | ✗ | NA/✗ (NA–43) | 2 | 1 |
| 5 | Amy | Weight loss, pyrexia, tender abdomen. Icteric plasma. | 1280/640 (16m) | ✗ | ✓/✗ | ✓/✗ (55–38) | 4 | 1 |
| 6 | Brook | Recurring pyrexia | 1280/0 (13m) | ✓/✗ (33d) | ✓/✗ | ✓/✓ (57–51) | 5 | 1 |
| 7 | Basil 2 | Ascites | >1280/>1280 (27m) | ✓/✗ ** | ✓/✗ | ✓/✗ (63–42) | 5 | 1 |
| 8 | Kitten 2 | Ascites. Relapse: painful tail, ataxia, seizures. Full recovery. | >1280/640 (8m) | ✗ | ✗ | ✓/✗ (58–39) | 5 | 1 |
| 9 | Skywise | Weight loss, uveitis | >10,240/640 (9m) | ✓/✗ (12d) | ✓/✗ | ✓/✗ (91–47) | 5 | 0 |
| 10 | Betsy | Ascites, profound anaemia (Hct 14%), underweight: BCS 2/9. | >1280/>1280 (2m) | ✓/✗ (20d) | ✓/✗ | ✗ (41–44) | 4 | 1 |
| 11 | Dante | Vomiting and diarrhoea | 1280/>1280 (2m) | ✗/✗ | ✗ | ✓/✓ (68–53) | 3 | 1 |
| 12 | Elmo | Quiet purr, poor appetite, listless. Pyrexia, mesenteric lymph node enlargement, anaemia. | >10,240/0 (8m) | ✓/✗ (31d) | ✗ | ✓/✗ (72–42) | 4 | 0 |
| 13 | Lyra | Ascites | >10,240/2560 (8m) | ✓/✗ (47d) | ✓/✗ | ✓/✗ (69–35) | 5 | 0 |
| 14 | Molly | Uveitis, chronic diarrhoea: carrier cat shedding virus in faeces >23m | >1280/1280 (15m) | ✗ | ✗/✗ (low) | ✓/✗ (57–56) | 3 | 2 |
| 15 | Bea | Ascites, sudden weakness in limbs. Trichobezoar caused vomiting. | >1280/640 (11m) | ✓/✗ (26d) | ✗ | ✓/✓ (78–53) | 4 | 1 |
| 16 | Buddie | Ascites | >1280/1280 (7m) | ✓/✗ (26d) | 2 of 7 samples | ✓/✓ (106–74) | 4 | 1 |
| 17 | Nelson | Dull, reduced appetite, enlarged MLN, ascites after biopsy. | 640/>1280 (6m) | ✗ | ✗ | ✓/✗ (79–33) | 3 | 1 |
| 18 | Wish | Enlarged MLN, chronic diarrhoea | >1280/not re-tested yet | ✗ | ✓/✗ | ✓/✓ (85–51) | 4 | 2 |
| 19 | Mike | Chronic diarrhea, haematochezia, continuous virus shedding two years later although cat is well. | >1280/not re-tested | ✓/✗ (154d) | ✓/✗ | ✓/✗ (105–45) | 5 | 2 |
| 20 | Chynah | Cough, pneumonia, nasal discharge, dyspnoea, pleural effusion. | 1280/>1280 (8m) | NA | NA | ✓/✓ (64–47) | 3 | 2 |
| 21 | Tabitha | Underweight, pyrexic, watery diarrhoea, ataxic episode, possible uveitis. | >1280/not re-tested | ✗ * | ✗ (but initial count low at 1.89) | ✓/✓ (88–59) | 3 | 2 |
| 22 | Harry | Small amount of ascites and enlarged MLN | >1280/>1280 (2m) | ✓/✗ (30d) | ✓/✗ | ✓/✓ (99–54) | 5 | 2 |
| 23 | Mr Twinkles | Ascites | >1280/1280 (6m) | ✓/✗ (57d) | ✓/✗ | ✓/✓ (58–51) | 5 | 2 |
| 24 | Tyra | Uveitis | >1280/320 (5m) | ✗ | ✗ | ✓/✓ (58–54) | 3 | 1 |
| 25 | Munchie | Ascites, pyrexia, lethargy | >1280/>1280 (4m) | ✗ | ✗ | ✓/✗ (51–38) | 3 | 1 |
| 26 | Edward | Pleural effusion | >1280/>1280 (7m) | ✗ but 1st count 2m into treatment | ✗ but 1st count 2m into treatment | ✓/✗ (59–44) | 3 | 1 |
| Summary | 7 of 26 FCoV antibody titres reduced significantly (at least 3-fold) | 12 of 25 cats anaemic: anaemia resolved in all | 9 of 24 cats lymphopenic on at least one test | 22/25 cats had raised globulins, one NA. Reduced in all 22 and to WNL in 15 cats. | ||||
| Cat | Clinical Signs | FCoV Antibody Titre | Anaemia i.e., Hct < 30% | Lymphopenia <1.5 × 109/L | Hyperglobulinaemia i.e., >45 g/L | Score | ||
|---|---|---|---|---|---|---|---|---|
| First | Last | |||||||
| 1 | Yrael | Effusion | >1280/>1280 | NA | NA | NA | 2 | 2 |
| 2 | Charlie Chaplin | Neurological signs. Toxoplasmosis co-infection. | >1280/>1280 | NA/✓ | NA/✓ | ✓/✗ | insufficient data | |
| 3 | Smokey | Failure to gain weight and enlarged MLN. | >1280/>1280 | ✓/✓ | ✓/✓ | ✓/✓ | 5 | 5 |
| 4 | Rowley | Ascites, then uveitis, then haemolytic anaemia, euthanasia. | >1280/640 | ✓/✓ | ✓/✓ | ✓/✗ | 4 | 3 |
| 5 | Claude | Pleural effusion, deteriorated and ascites appeared. | NA | NA | NA | NA | insufficient data | |
| 6 | Alfie | Vomiting but bright initially, chronic diarrhoea, enlarged MLN. | >1280/1280 | NA | NA | NA | insufficient data | |
| 7 | Holly | Persistent pyrexia, weight loss then ascites. | >1280/1280 | ✗/✗ | ✗/✗ | ✓ /✗ | 3 | 2 |
| 8 | Bugsy | Pyrexia, poor body condition, variable appetite. | >1280/>1280 | ✗/✓ | ✗/✓ | ✗/✓ | 2 | 5 |
| 9 | Daisy | Weight loss, intestinal granuloma, raised MLN. Intestinal granuloma resolved with treatment, but cat still died. | >1280/>1280 | ✓/✓ | ✓/✓ | ✓/✓ | 5 | 5 |
| 10 | Levi | Ascites. | >1280/not repeated | ✓/✓ (improved though) | ✓/✓ | ✓/✗ | 5 | 4 |
| 11 | Roxanne | Chronic gingivostomatitis, poor condition, poor appetite, jaundice which resolved, but she suddenly developed ataxia and was euthanased. | >1280/320 | ✓/✓ | ✓/✓ | ✓/✓ | 5 | 4 |
| 12 | Pip | Biopsied 2004. February 2005: enlarged MLN, weight loss, anaemia, reported well in February 2006 although pyrexic (39.2 °C). | >1280/>1280 | ✓/✓ | low/✗ | ✓/✓ | 5 | 4 |
| 13 | Pharaoh | Weight loss, gut biopsy showed inflammation. | 640/>1280 | ✓/✓ | ✗/✓ | ✗/✓ | 3 | 5 |
| 14 | Maximus | Chronic diarrhoea, poor appetite. Collapsed and was euthanased. | >1280/>1280 | ✓/✓ | ✗/✗ | ✓/✓ | 4 | 4 |
| 15 | Ragamuffin | Weight loss. MLN enlarged, diarrhoea, always shed low amounts of virus in faeces, chronic anaemia. | >1280/>1280 | ✗/✓ | ✓/✓ (sometimes low normal) | ✓/✓ | 4 | 5 |
| 16 | Tinkerbell | Underweight, chronic poor appetite. | >1280/1280 | ✓/✗ | ✗/✗ | ✓/✓ | 4 | 3 |
| Summary | 15 of 15/ 13 of 14 | 9 of 12/ 11 of 13 | 6 of 11/ 10 of 13 | 11 of 13/ 9 of 13 | ||||
3.2. FIP Treatment
3.3. Recovery, Remission, and Death
- The cat returned to clinical normality, specifically resolution of the clinical signs of FIP.
- Globulin levels were reduced to normal (≤45 g/L) or at least significantly reduced (often by over 15 g/L as shown in Table 3).
- Resolution of lymphopenia, where present, (normal defined as ≥1.5 × 109/L).
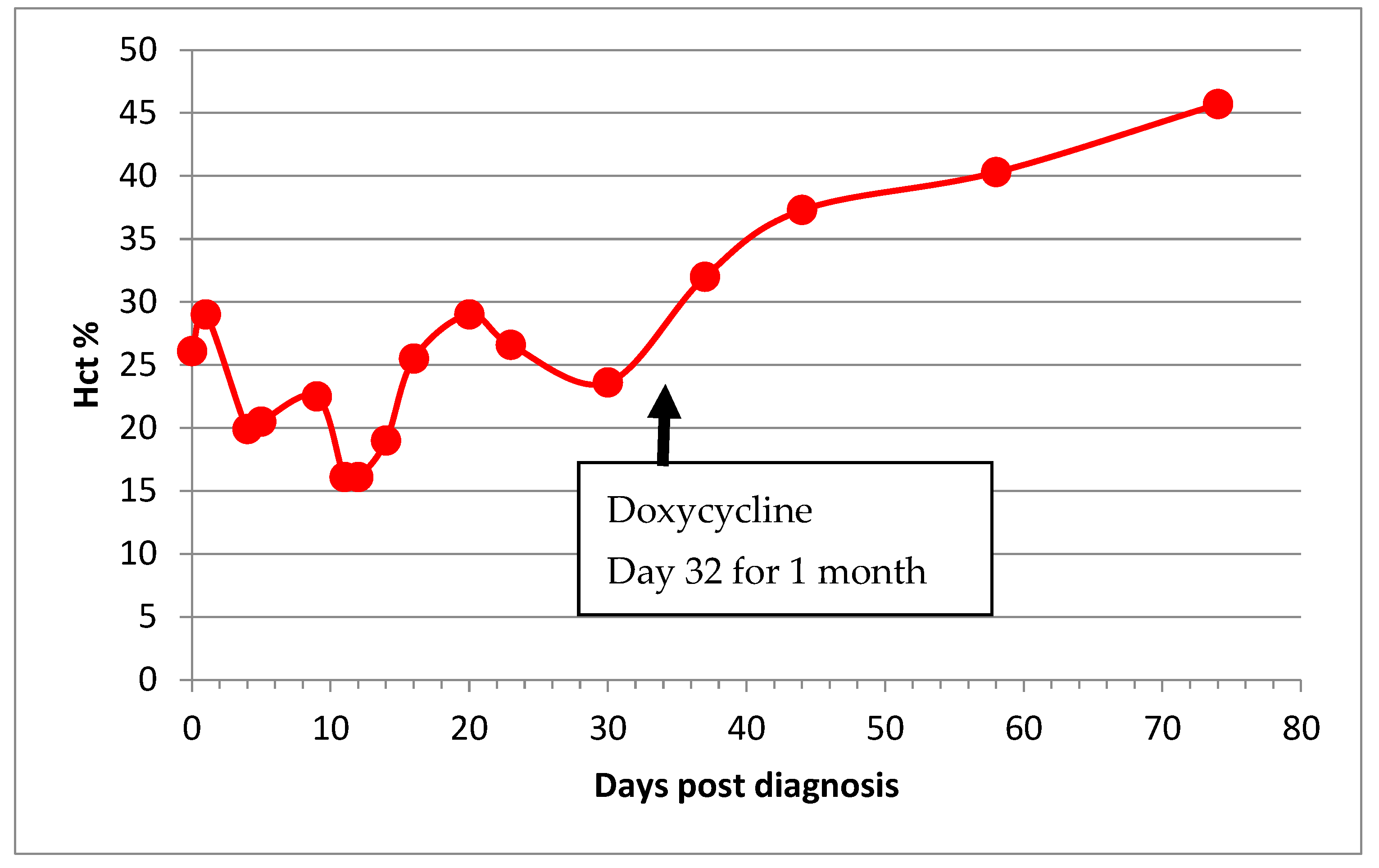
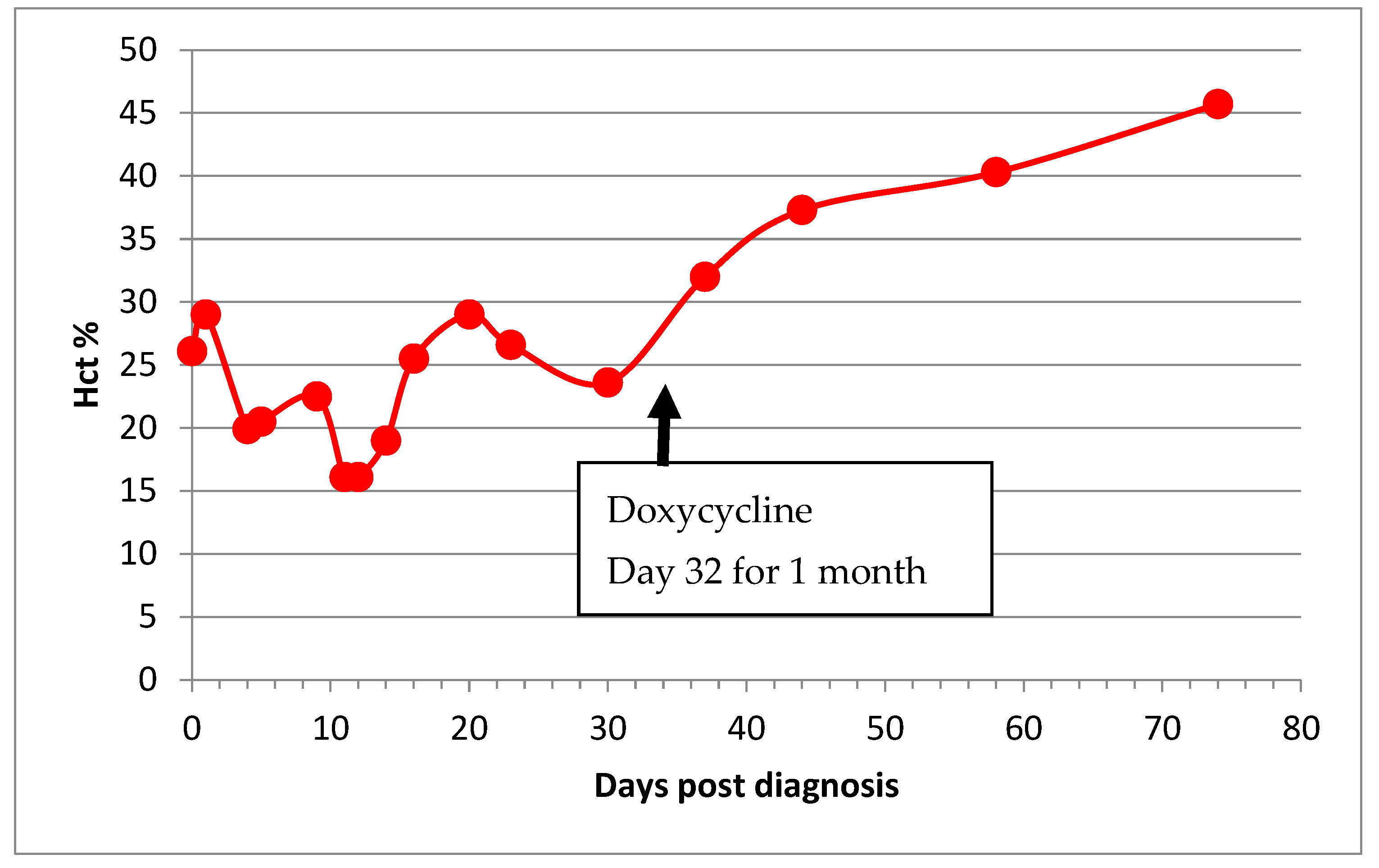
- Haematocrit level increased to normal (defined as ≥30%), with reversal of non-regenerative anaemia where present.
- At least three-fold reduction in FCoV antibody titre.
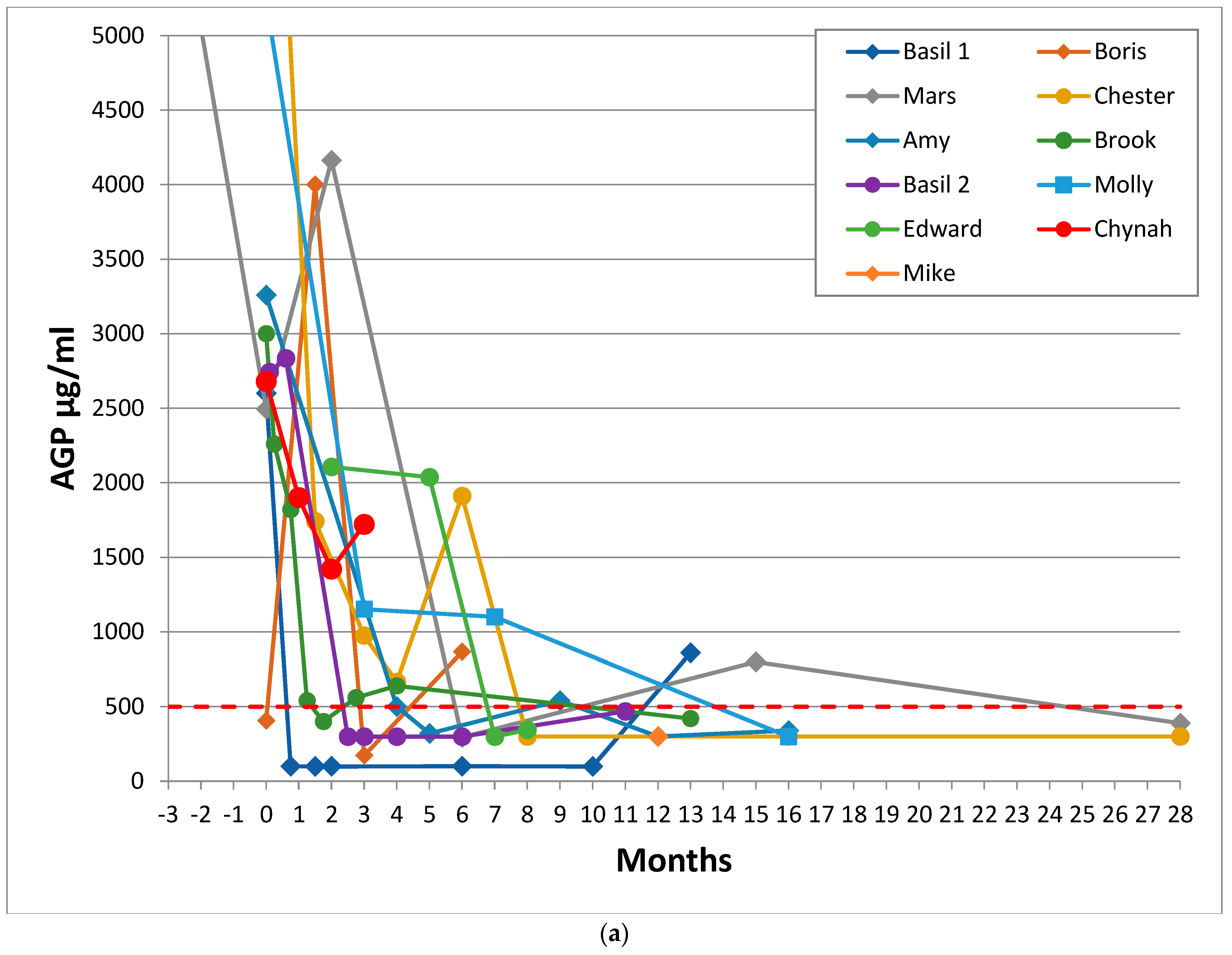
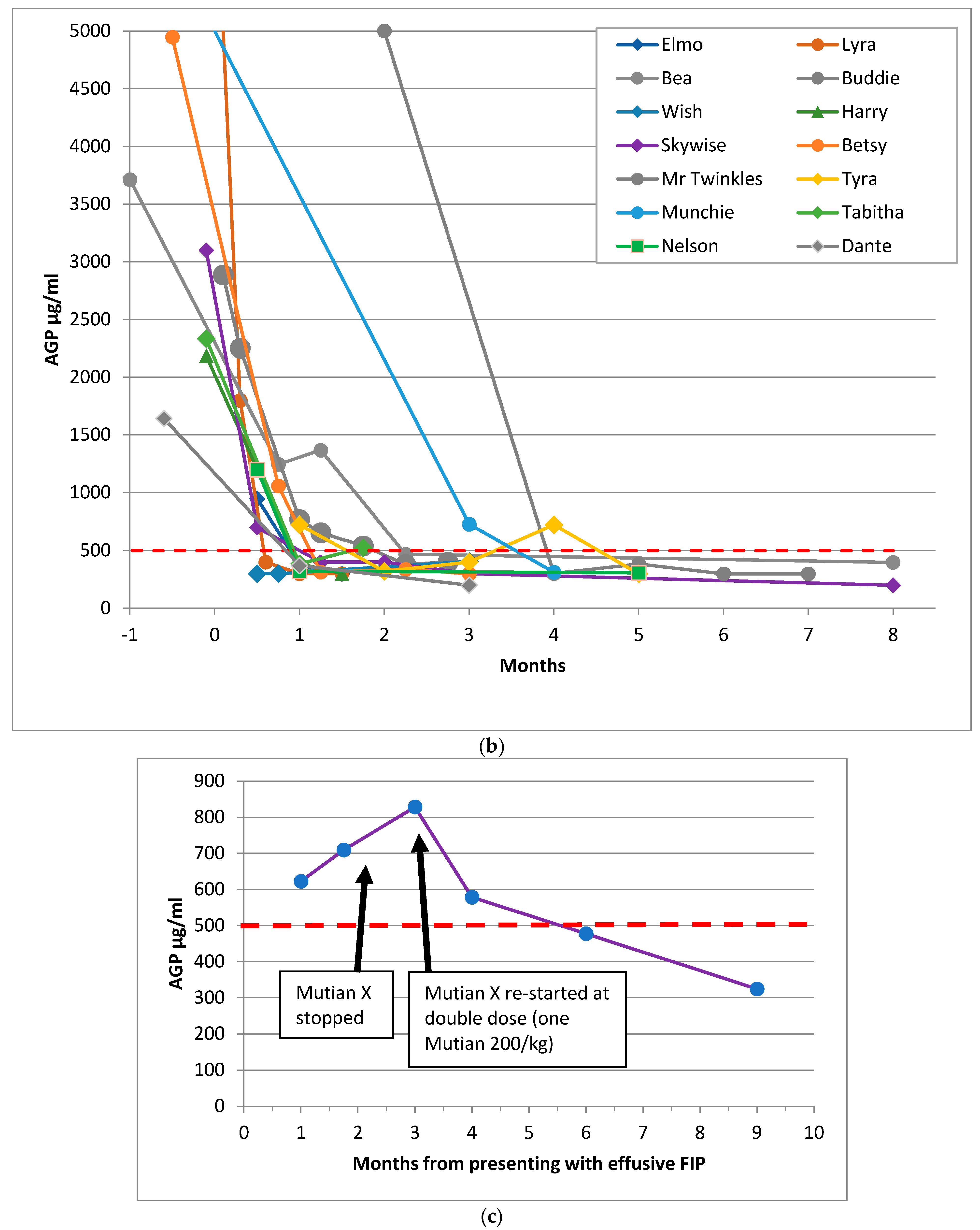
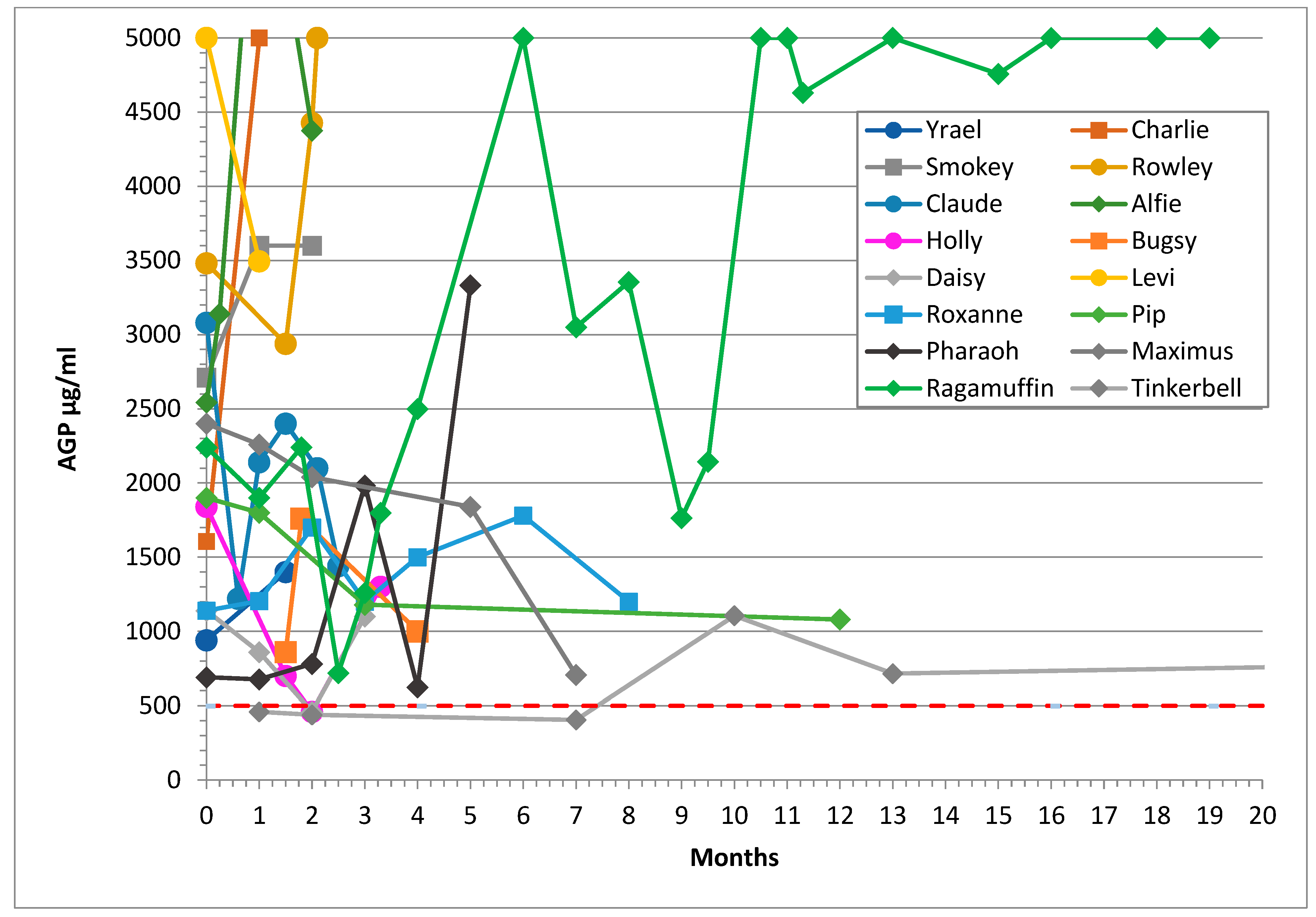
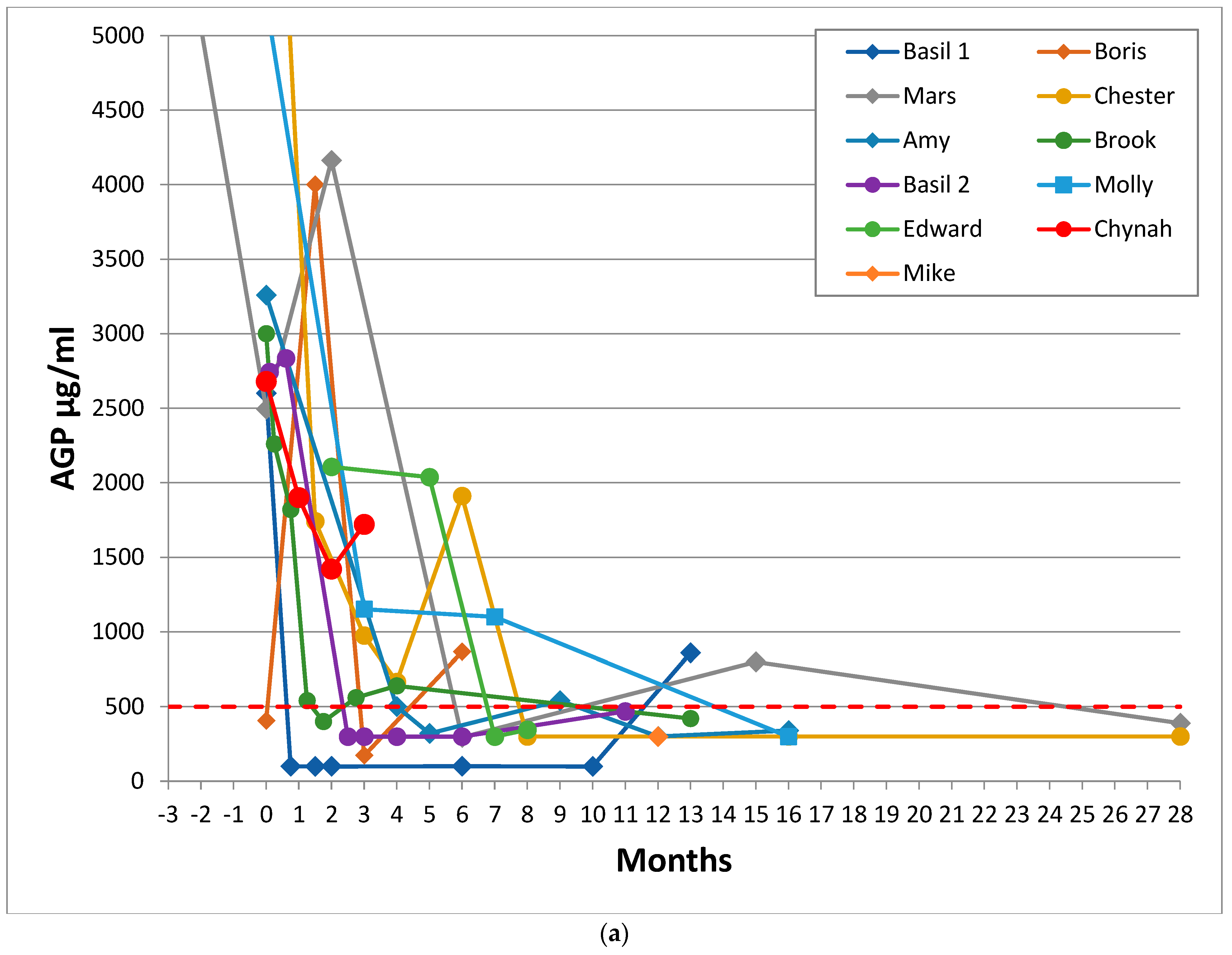
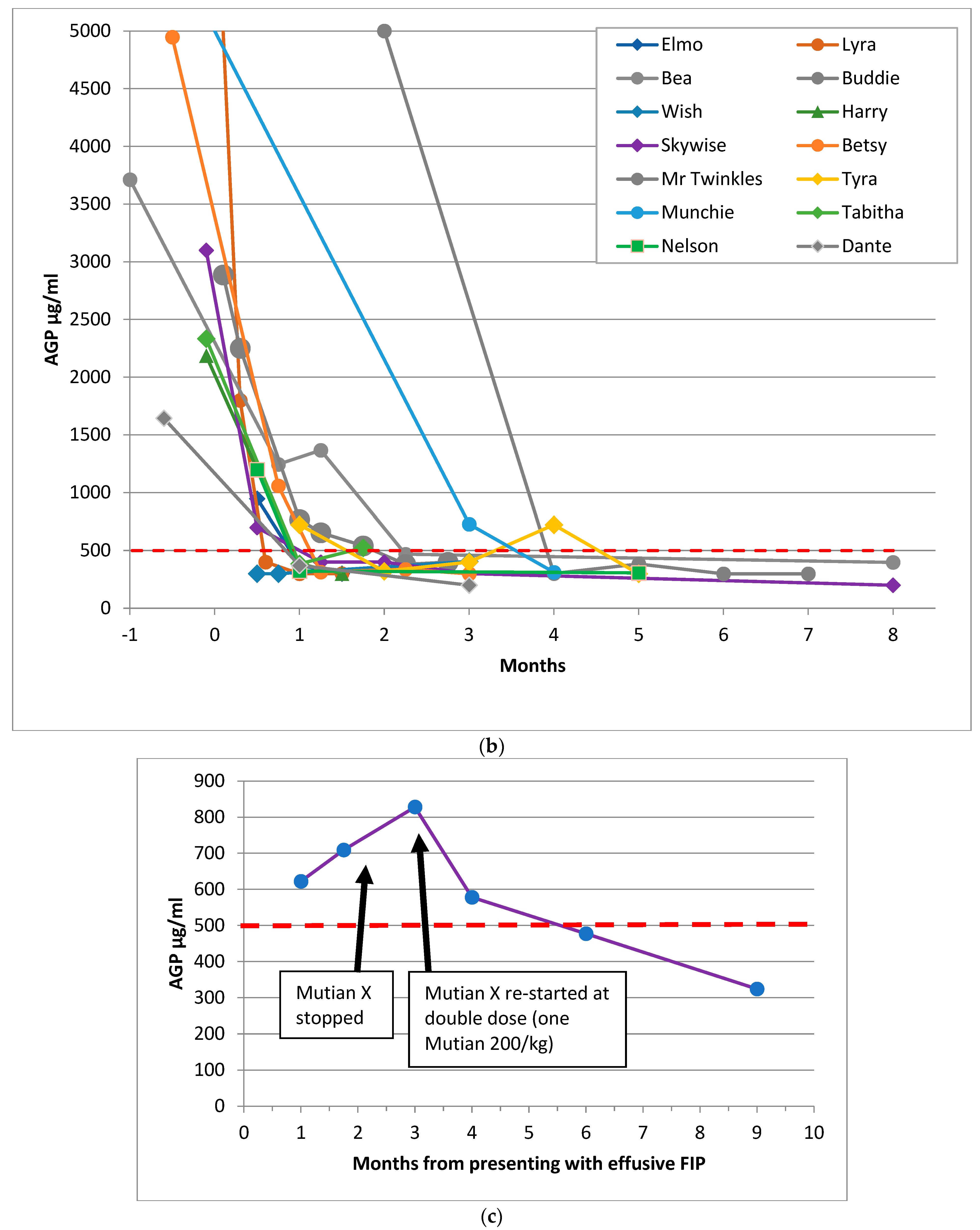
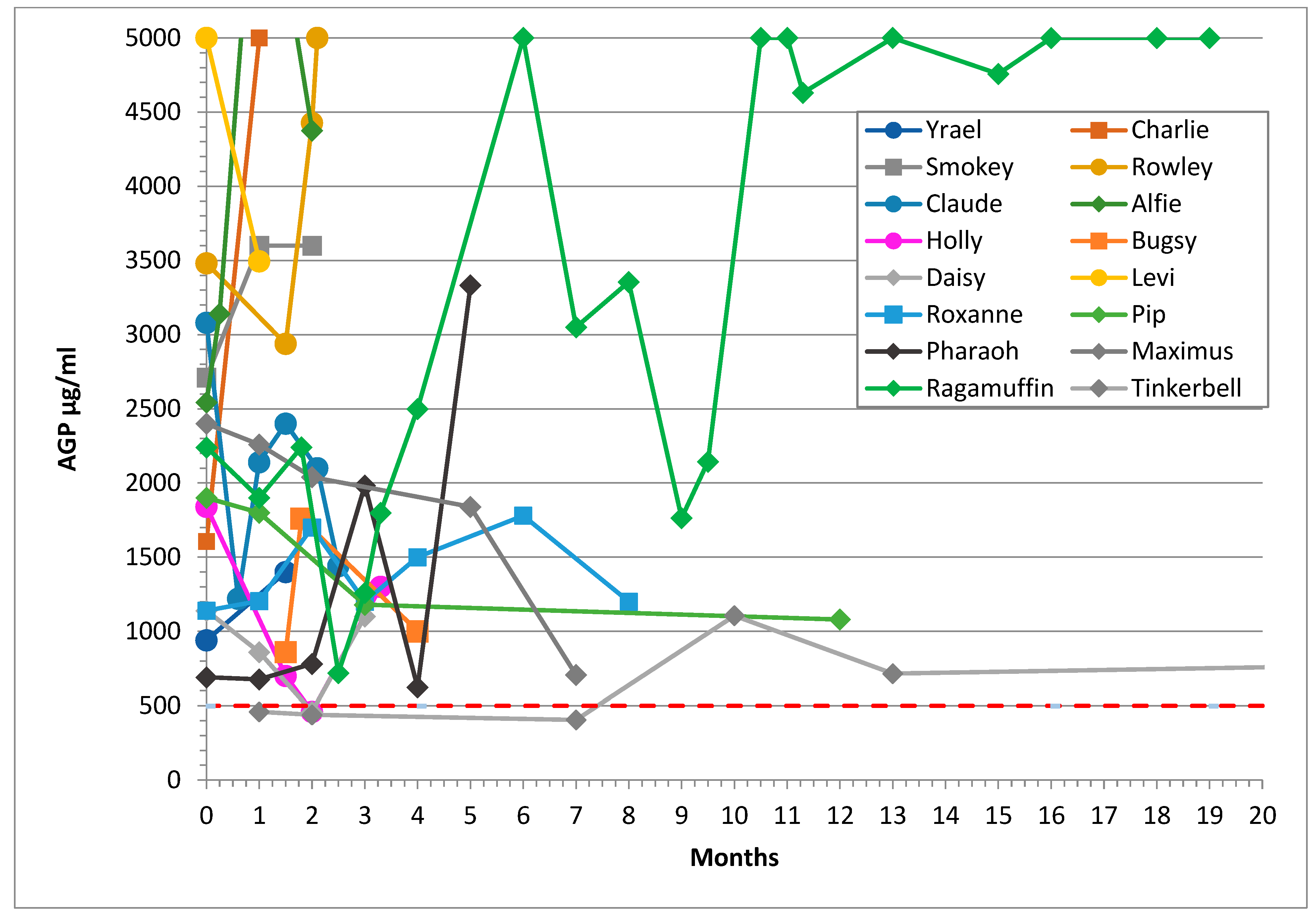
- AGP levels returned to normal levels (≤500 μg/mL) [40].
3.4. AGP Levels
3.5. Haematocrit
3.6. Lymphopenia
3.7. Hyperglobulinaemia
3.8. FCoV Antibody Titre
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Ethical Approval
Acknowledgments
Conflicts of Interest
References
- Herrewegh, A.A.P.M.; Smeenk, I.; Horzinek, M.C.; Rottier, P.J.M.; de Groot, R.J. Feline coronavirus type II strains 79-1683 and 79-1146 originate from a double recombination between feline coronavirus type I and canine coronavirus. J. Virol. 1998, 72, 4508–4514. [Google Scholar] [CrossRef] [Green Version]
- Terada, Y.; Matsui, N.; Noguchi, K.; Kuwata, R.; Shimoda, H.; Soma, T.; Mochizuki, M.; Maeda, K. Emergence of pathogenic coronaviruses in cats by homologous recombination between feline and canine coronaviruses. PLoS ONE 2014, 9, e106534. [Google Scholar] [CrossRef] [Green Version]
- Kipar, A.; May, H.; Menger, S.; Weber, M.; Leukert, W.; Reinacher, M. Morphologic features and development of granulomatous vasculitis in feline infectious peritonitis. Vet. Pathol. 2005, 42, 321–330. [Google Scholar] [CrossRef]
- Addie, D.D.; Toth, S.; Murray, G.D.; Jarrett, O. The risk of feline infectious peritonitis in cats naturally infected with feline coronavirus. Am. J. Vet. Res. 1995, 56, 429–434. [Google Scholar]
- Pedersen, N.C.; Boyle, J.F.; Floyd, K.; Fudge, A.; Barker, J. An enteric coronavirus infection of cats and its relationship to feline infectious peritonitis. Am. J. Vet. Res. 1981, 42, 368–377. [Google Scholar]
- Pedersen, N.C.; Liu, H.; Dodd, K.A.; Pesavento, P.A. Significance of coronavirus mutants in feces and diseased tissues of cats suffering from feline infectious peritonitis. Viruses 2009, 1, 166–184. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.W.; Egberink, H.F.; Halpin, R.; Spiro, D.J.; Rottier, P.J. Spike protein fusion peptide and feline coronavirus virulence. Emerg. Infect. Dis. 2012, 18, 1089–1095. [Google Scholar] [CrossRef]
- Felten, S.; Leutenegger, C.M.; Balzer, H.J.; Pantchev, N.; Matiasek, K.; Wess, G.; Egberink, H.; Hartmann, K. Sensitivity and specificity of a real-time reverse transcriptase polymerase chain reaction detecting feline coronavirus mutations in effusion and serum/plasma of cats to diagnose feline infectious peritonitis. BMC Vet. Res. 2017, 13, 228. [Google Scholar] [CrossRef]
- Porter, E.; Tasker, S.; Day, M.J.; Harley, R.; Kipar, A.; Siddell, S.G.; Helps, C.R. Amino acid changes in the spike protein of feline coronavirus correlate with systemic spread of virus from the intestine and not with feline infectious peritonitis. Vet. Res. 2014, 45, 49. [Google Scholar] [CrossRef] [Green Version]
- Barker, E.N.; Stranieri, A.; Helps, C.R.; Porter, E.L.; Davidson, A.D.; Day, M.J.; Knowles, T.; Kipar, A.; Tasker, S. Limitations of using feline coronavirus spike protein gene mutations to diagnose feline infectious peritonitis. Vet. Res. 2017, 48, 60. [Google Scholar] [CrossRef] [Green Version]
- Stranieri, A.; Giordano, A.; Paltrinieri, S.; Giudice, C.; Cannito, V.; Lauzi, S. Comparison of the performance of laboratory tests in the diagnosis of feline infectious peritonitis. J. Vet. Diagn. Investig. 2018, 30, 459–463. [Google Scholar] [CrossRef] [Green Version]
- Decaro, N.; Mari, V.; Lanave, G.; Lorusso, E.; Lucente, M.S.; Desario, C.; Colaianni, M.L.; Elia, G.; Ferringo, F.; Alfano, F.; et al. Mutation analysis of the spike protein in Italian feline infectious peritonitis virus and feline enteric coronavirus sequences. Res. Vet. Sci. 2021, 135, 15–19. [Google Scholar] [CrossRef]
- Tasker, S. Diagnosis of feline infectious peritonitis: Update on evidence supporting available tests. J. Feline Med. Surg. 2018, 20, 228–243. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.A.; Troyer, J.L.; Pecon-Slattery, J.; Roelke, M.; O’Brien, S.J. Genetics and pathogenesis of feline infectious peritonitis virus. Emerg. Infect. Dis. 2009, 15, 1445–1452. [Google Scholar] [CrossRef]
- Healey, E.A.; Andre, N.M.; Miller, A.D.; Whitaker, G.R.; Berliner, E.A. Outbreak of feline infectious peritonitis (FIP) in shelter-housed cats: Molecular analysis of the feline coronavirus S1/S2 cleavage site consistent with a ‘circulating virulent-avirulent theory’ of FIP pathogenesis. JFMS Open Rep. 2022, 8. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Black, J.W. Attempted immunization of cats against feline infectious peritonitis, using avirulent live virus or sublethal amounts of virulent virus. Am. J. Vet. Res. 1983, 44, 229–234. [Google Scholar]
- Barker, E.N.; Tasker, S.; Gruffydd-Jones, T.J.; Tuplin, C.K.; Burton, K.; Porter, E.; Day, M.J.; Harley, R.; Fews, D.; Helps, C.R.; et al. Phylogenetic analysis of feline coronavirus strains in an epizootic outbreak of feline infectious peritonitis. J. Vet. Intern. Med. 2013, 27, 445–450. [Google Scholar] [CrossRef] [Green Version]
- Graham, E.M.; Went, K.; Serra, F.; Dunbar, D.; Fuentes, M.; McDonald, M.; Jackson, M.W. Early molecular diagnosis of an effusive FIP outbreak in antibody-negative kittens. J. Feline Med. Surg. 2012, 14, 652. [Google Scholar]
- Wang, Y.T.; Su, B.L.; Hsieh, L.E.; Chueh, L.L. An outbreak of feline infectious peritonitis in a Taiwanese shelter: Epidemiologic and molecular evidence for horizontal transmission of a novel type II feline coronavirus. Vet. Res. 2013, 44, 57. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, N.C.; Sato, R.; Foley, J.E.; Poland, A.M. Common virus infections in cats, before and after being placed in shelters, with emphasis on Feline Enteric Coronavirus. J. Feline Med. Surg. 2004, 6, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Rohrer, C.; Suter, P.F.; Lutz, H. The diagnosis of feline infectious peritonitis (FIP): A retrospective and prospective study. Kleinterpraxis 1993, 38, 379–389. [Google Scholar]
- Riemer, F.; Kuehner, K.A.; Ritz, S.; Sauter-Louis, C.; Hartmann, K. Clinical and laboratory features of cats with feline infectious peritonitis—A retrospective study of 231 confirmed cases (2000–2010). J. Feline Med. Surg. 2016, 18, 348–356. [Google Scholar] [CrossRef] [Green Version]
- De Groot-Mijnes, J.D.; van Dun, J.M.; van der Most, R.G.; de Groot, R.J. Natural history of a recurrent feline coronavirus infection and the role of cellular immunity in survival and disease. J. Virol. 2005, 79, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Dewerchin, H.L.; Cornelissen, E.; Nauwynck, H.J. Replication of feline coronaviruses in peripheral blood monocytes. Arch. Virol. 2005, 150, 2483–2500. [Google Scholar] [CrossRef] [Green Version]
- Fischer, Y.; Wess, G.; Hartmann, K. Perikarderguss bei einer Katze mit feliner infektiöser Peritonitis [Pericardial effusion in a cat with feline infectious peritonitis]. Schweiz. Arch. Tierheilkd. 2012, 154, 27–31. [Google Scholar] [CrossRef]
- Pedersen, N.C. A review of feline infectious peritonitis virus infection: 1963–2008. J. Feline Med. Surg. 2009, 11, 225–258. [Google Scholar] [CrossRef]
- Penderis, J. The Wobbly Cat: Diagnostic and therapeutic approach to generalised ataxia. J. Feline Med. Surg. 2009, 11, 349–359. [Google Scholar] [CrossRef]
- Crawford, A.H.; Stoll, A.L.; Sanchez-Masian, D.; Shea, A.; Michaels, J.; Fraser, A.R.; Beltran, E. Clinicopathologic Features and Magnetic Resonance Imaging Findings in 24 Cats with Histopathologically Confirmed Neurologic Feline Infectious Peritonitis. J. Vet. Intern. Med. 2017, 31, 1477–1486. [Google Scholar] [CrossRef]
- Kipar, A.; Bellman, S.; Kremendahl, J.; Kohler, K.; Reinacher, M. Cellular composition, coronavirus antigen expression and production of specific antibodies in lesions in feline infectious peritonitis. Vet. Immunol. Immunopathol. 1998, 65, 243–257. [Google Scholar] [CrossRef]
- Takano, T.; Hohdatsu, T.; Hashida, Y.; Kaneko, Y.; Tanabe, M.; Koyama, H. A “possible” involvement of TNF-alpha in apoptosis induction in peripheral blood lymphocytes of cats with feline infectious peritonitis. Vet. Microbiol. 2007, 119, 121–131. [Google Scholar] [CrossRef]
- Takano, T.; Azuma, N.; Satoh, M.; Toda, A.; Hashida, Y.; Satoh, R.; Hohdatsu, T. Neutrophil survival factors (TNF-alpha, GM-CSF, and G-CSF) produced by macrophages in cats infected with feline infectious peritonitis virus contribute to the pathogenesis of granulomatous lesions. Arch. Virol. 2009, 154, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Goitsuka, R.; Ohashi, T.; Ono, K.; Yasukawa, K.; Koishibara, Y.; Fukui, H.; Ohsugi, Y.; Hasegawa, A. IL-6 activity in feline infectious peritonitis. J. Immunol. 1990, 144, 2599–2603. [Google Scholar] [PubMed]
- Haagmans, B.L.; Egberink, H.F.; Horzinek, M.C. Apoptosis and T-cell depletion during feline infectious peritonitis. J. Virol. 1996, 70, 8977–8983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, H.Y.; Chueh, L.L.; Lin, C.N.; Su, B.L. Clinicopathological findings and disease staging of feline infectious peritonitis: 51 cases from 2003 to 2009 in Taiwan. J. Feline Med. Surg. 2011, 13, 74–80. [Google Scholar] [CrossRef]
- Yin, Y.; Li, T.; Wang, C.; Liu, X.; Ouyang, H.; Ji, W.; Liu, J.; Liao, X.; Li, J.; Hu, C. A retrospective study of clinical and laboratory features and treatment on cats highly suspected of feline infectious peritonitis in Wuhan, China. Nat. Sci. Rep. 2021, 11, 5208. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Eckstrand, C.; Liu, H.; Leutenegger, C.; Murphy, B. Levels of feline infectious peritonitis virus in blood, effusions, and various tissues and the role of lymphopenia in disease outcome following experimental infection. Vet. Microbiol. 2015, 175, 157–166. [Google Scholar] [CrossRef]
- Paltrinieri, S.; Giordano, A.; Tranquillo, V.; Guazzetti, S. Critical assessment of the diagnostic value of feline alpha1-acid glycoprotein for feline infectious peritonitis using the likelihood ratios approach. J. Vet. Diagn. Investig. 2007, 19, 266–272. [Google Scholar]
- Paltrinieri, S. The feline acute phase reaction. Vet. J. 2008, 177, 26–35. [Google Scholar] [CrossRef]
- Korman, R.M.; Cerón, J.J.; Knowles, T.G.; Barker, E.N.; Eckersall, P.D.; Tasker, S. Acute phase response to Mycoplasma haemofelis and ‘Candidatus Mycoplasma haemominutum’ infection in FIV-infected and non-FIV-infected cats. Vet. J. 2012, 193, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Duthie, S.; Eckersall, P.D.; Addie, D.D.; Lawrence, C.E.; Jarrett, O. Value of α1-acid glycoprotein in the diagnosis of feline infectious peritonitis. Vet. Rec. 1997, 141, 299–303. [Google Scholar] [CrossRef]
- Giordano, A.; Spagnolo, V.; Colombo, A.; Paltrinieri, S. Changes in some acute phase protein and immunoglobulin concentrations in cats affected by feline infectious peritonitis (FIP) or exposed to feline coronavirus infection. Vet. J. 2004, 167, 38–44. [Google Scholar] [CrossRef]
- Paltrinieri, S.; Metzger, C.; Battilani, M.; Pocacqua, V.; Gelain, M.E.; Giordano, A. Serum alpha1-acid glycoprotein (AGP) concentration in non-symptomatic cats with feline coronavirus (FCoV) infection. J. Feline Med. Surg. 2007, 9, 271–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giori, L.; Giordano, A.; Giudice, C.; Grieco, V.; Paltrinieri, S. Performances of different diagnostic tests for feline infectious peritonitis in challenging clinical cases. J. Small Anim. Pract. 2011, 52, 152–157. [Google Scholar] [CrossRef]
- Hazuchova, K.; Held, S.; Neiger, R. Usefulness of acute phase proteins in differentiating between feline infectious peritonitis and other diseases in cats with body cavity effusions. J. Feline Med. Surg. 2017, 19, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, S.Y.; Lai, Y.R.; Kung, C.T.; Tsai, N.W.; Su, C.M.; Huang, C.C.; Wang, H.C.; Cheng, B.C.; Su, Y.J.; Lin, W.C.; et al. α-1-Acid Glycoprotein Concentration as an Outcome Predictor in Adult Patients with Sepsis. Biomed. Res. Int. 2019, 3174896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, T.; Shibanai, A.; Tanaka, S.; Uchida, K.; Mochizuki, M. Use of recombinant feline interferon and glucocorticoid in the treatment of feline infectious peritonitis. J. Feline Med. Surg. 2004, 6, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Legendre, A.M.; Kuritz, T.; Galyon, G.; Baylor, V.M.; Heidel, R.E. Polyprenyl Immunostimulant Treatment of Cats with Presumptive Non-Effusive Feline Infectious Peritonitis in a Field Study. Front. Vet. Sci. 2017, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Hugo, T.B.; Heading, K.L. Prolonged survival of a cat diagnosed with feline infectious peritonitis by immunohistochemistry. Can. Vet. J. 2015, 56, 53–58. [Google Scholar]
- Pedersen, N.C.; Kim, Y.; Liu, H.; Galasiti Kankanamalage, A.C.; Eckstrand, C.; Groutas, W.C.; Bannasch, M.; Meadows, J.M.; Chang, K.O. Efficacy of a 3C-like protease inhibitor in treating various forms of acquired feline infectious peritonitis. J. Feline Med. Surg. 2018, 20, 378–392. [Google Scholar] [CrossRef]
- Pedersen, N.C.; Perron, M.; Bannasch, M.; Montgomery, E.; Murakami, E.; Liepnieks, M.; Liu, H. Efficacy and safety of the nucleoside analog GS-441524 for treatment of cats with naturally occurring feline infectious peritonitis. J. Feline Med. Surg. 2019, 21, 271–281. [Google Scholar] [CrossRef] [Green Version]
- Dickinson, P.J.; Bannasch, M.; Thomasy, S.M.; Murthy, V.D.; Vernau, K.M.; Liepnieks, M.; Montgomery, E.; Knickelbein, K.E.; Murphy, B.; Pedersen, N.C. Antiviral treatment using the adenosine nucleoside analogue GS-441524 in cats with clinically diagnosed neurological feline infectious peritonitis. J. Vet. Intern. Med. 2020, 34, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Krentz, D.; Zenger, K.; Alberer, M.; Felten, S.; Bergmann, M.; Dorsch, R.; Matiasek, K.; Kolberg, L.; Hofmann-Lehmann, R.; Meli, M.L.; et al. Curing Cats with Feline Infectious Peritonitis with an Oral Multi-Component Drug Containing GS-441524. Viruses 2021, 13, 2228. [Google Scholar] [CrossRef] [PubMed]
- Jones, S.; Novicoff, W.; Nadeau, J.; Evans, S.W. Unlicensed GS-441524-Like Antiviral Therapy Can Be Effective for at-Home Treatment of Feline Infectious Peritonitis. Animals 2021, 11, 2257. [Google Scholar] [CrossRef] [PubMed]
- Doenges, S.J.; Weber, K.; Dorsch, R.; Fux, R.; Hartmann, K. Comparison of real-time reverse transcriptase polymerase chain reaction of peripheral blood mononuclear cells, serum and cell-free body cavity effusion for the diagnosis of feline infectious peritonitis. J. Feline Med. Surg. 2017, 19, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Longstaff, L.; Porter, E.; Crossley, V.J.; Hayhow, S.E.; Helps, C.R.; Tasker, S. Feline coronavirus quantitative reverse transcriptase polymerase chain reaction on effusion samples in cats with and without feline infectious peritonitis. J. Feline Med. Surg. 2017, 19, 240–245. [Google Scholar] [CrossRef] [Green Version]
- Yen, S.-J.; Chen, H.-W. Feline Coronaviruses Identified in Feline Effusions in Suspected Cases of Feline Infectious Peritonitis. Microorganisms 2021, 9, 1801. [Google Scholar] [CrossRef]
- Dunbar, D.; Kwok, W.; Graham, E.; Armitage, A.; Irvine, R.; Johnston, P.; McDonald, M.; Montgomery, D.; Nicolson, L.; Robertson, E.; et al. Diagnosis of non-effusive feline infectious peritonitis by reverse transcriptase quantitative polymerase chain reaction from mesenteric lymph node fine needle aspirates. J. Feline Med. Surg. 2019, 21, 910–921. [Google Scholar] [CrossRef] [Green Version]
- Simons, F.A.; Vennema, H.; Rofina, J.E.; Pol, J.M.; Horzinek, M.C.; Rottier, P.J.; Egberink, H.F. A mRNA PCR for the diagnosis of feline infectious peritonitis. J. Virol. Methods 2005, 124, 111–116. [Google Scholar] [CrossRef] [Green Version]
- Fish, E.J.; Diniz, P.P.V.; Juan, Y.C.; Bossong, F.; Collisson, E.W.; Drechsler, Y.; Kaltenboeck, B. Cross-sectional quantitative RT-PCR study of feline coronavirus viremia and replication in peripheral blood of healthy shelter cats in Southern California. J. Feline Med. Surg. 2018, 20, 295–301. [Google Scholar] [CrossRef] [Green Version]
- Herrewegh, A.A.P.M.; de Groot, R.J.; Cepica, A.; Egberink, H.F.; Horzinek, M.C.; Rottier, P.J.M. Detection of feline coronavirus RNA in feces, tissue, and body fluids of naturally infected cats by reverse transcriptase PCR. J. Clin. Microbiol. 1995, 33, 684–689. [Google Scholar] [CrossRef] [Green Version]
- Gut, M.; Leutenegger, C.M.; Huder, J.; Pedersen, N.C.; Lutz, H. One-tube fluorogenic reverse transcription-polymerase chain reaction for the quantitation of feline coronaviruses. J. Virol. Methods 1999, 77, 37–46. [Google Scholar] [CrossRef]
- Addie, D.; Belak, S.; Boucrat-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Hosie, M.J.; Marsilio, F.; Lloret, A.; et al. Feline infectious peritonitis. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 594–604. [Google Scholar] [CrossRef]
- Addie, D.D. Available online: www.catvirus.com (accessed on 29 January 2022).
- Hartmann, K.; Ritz, S. Treatment of cats with feline infectious peritonitis. Vet. Immunol. Immunopathol. 2008, 123, 172–175. [Google Scholar] [CrossRef]
- Addie, D.D.; Curran, S.; Bellini, F.; Crowe, B.; Sheehan, E.; Ukrainchuk, L.; Decaro, N. Oral Mutian® X stopped faecal feline coronavirus shedding by naturally infected cats. Res. Vet. Sci. 2020, 130, 222–229. [Google Scholar] [CrossRef]
- Rissi, D.R. A retrospective study of the neuropathology and diagnosis of naturally occurring feline infectious peritonitis. J. Vet. Diagn. Investig. 2018, 30, 392–399. [Google Scholar] [CrossRef]
- Amengual Batle, P.; Rusbridge, C.; Nuttall, T.; Heath, S.; Marioni-Henry, K. Feline hyperaesthesia syndrome with self-trauma to the tail: Retrospective study of seven cases and proposal for an integrated multidisciplinary diagnostic approach. J. Feline Med. Surg. 2019, 21, 178–185. [Google Scholar] [CrossRef]
- André, N.M.; Cossic, B.; Davies, E.; Miller, A.D.; Whittaker, G.R. Distinct mutation in the feline coronavirus spike protein cleavage activation site in a cat with feline infectious peritonitis-associated meningoencephalomyelitis. JFMS Open Rep. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Drancourt, M.; Cortaredona, S.; Melenotte, C.; Amrane, S.; Eldin, C.; La Scola, B.; Parola, P.; Million, M.; Lagier, J.C.; Raoult, D.; et al. SARS-CoV-2 Persistent Viral Shedding in the Context of Hydroxychloroquine-Azithromycin Treatment. Viruses 2021, 13, 890. [Google Scholar] [CrossRef]
- Choi, B.; Choudhary, M.C.; Regan, J.; Sparks, J.A.; Padera, R.F.; Qiu, X.; Solomon, I.H.; Kuo, H.H.; Boucau, J.; Bowman, K.; et al. Persistence and Evolution of SARS-CoV-2 in an Immunocompromised Host. N. Engl. J. Med. 2020, 383, 2291–2293. [Google Scholar] [CrossRef]
- Behera, P.; Patro, B.K.; Padhy, B.M.; Mohapatra, P.R.; Bal, S.K.; Chandanshive, P.D.; Mohanty, R.R.; Ravikumar, S.R.; Singh, A.K.; Singh, S.R.; et al. Prophylactic Role of Ivermectin in Severe Acute Respiratory Syndrome Coronavirus 2 Infection Among Healthcare Workers. Cureus 2021, 13, e16897. [Google Scholar] [CrossRef]
- Kerr, L.; Cadegiani, F.A.; Baldi, F.; Lobo, R.B.; Assagra, W.L.O.; Proença, F.C.; Kory, P.; Hibberd, J.A.; Chamie-Quintero, J.J. Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223, 128 Subjects Using Propensity Score Matching. Cureus 2022, 14, e21272. [Google Scholar]
| Title 1 | Anaemic | Not Anaemic | Total |
|---|---|---|---|
| Recovered effusive | 6 | 1 | 7 |
| Recovered non-effusive | 5 | 5 | 10 |
| Remission effusive (but 1 became non-effusive) | 2 | 0 | 2 |
| Remission non-effusive (but one became effusive) | 10 | 1 | 11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Addie, D.D.; Silveira, C.; Aston, C.; Brauckmann, P.; Covell-Ritchie, J.; Felstead, C.; Fosbery, M.; Gibbins, C.; Macaulay, K.; McMurrough, J.; et al. Alpha-1 Acid Glycoprotein Reduction Differentiated Recovery from Remission in a Small Cohort of Cats Treated for Feline Infectious Peritonitis. Viruses 2022, 14, 744. https://doi.org/10.3390/v14040744
Addie DD, Silveira C, Aston C, Brauckmann P, Covell-Ritchie J, Felstead C, Fosbery M, Gibbins C, Macaulay K, McMurrough J, et al. Alpha-1 Acid Glycoprotein Reduction Differentiated Recovery from Remission in a Small Cohort of Cats Treated for Feline Infectious Peritonitis. Viruses. 2022; 14(4):744. https://doi.org/10.3390/v14040744
Chicago/Turabian StyleAddie, Diane D., Carla Silveira, Charlotte Aston, Pauline Brauckmann, Johanna Covell-Ritchie, Chris Felstead, Mark Fosbery, Caryn Gibbins, Kristina Macaulay, James McMurrough, and et al. 2022. "Alpha-1 Acid Glycoprotein Reduction Differentiated Recovery from Remission in a Small Cohort of Cats Treated for Feline Infectious Peritonitis" Viruses 14, no. 4: 744. https://doi.org/10.3390/v14040744
APA StyleAddie, D. D., Silveira, C., Aston, C., Brauckmann, P., Covell-Ritchie, J., Felstead, C., Fosbery, M., Gibbins, C., Macaulay, K., McMurrough, J., Pattison, E., & Robertson, E. (2022). Alpha-1 Acid Glycoprotein Reduction Differentiated Recovery from Remission in a Small Cohort of Cats Treated for Feline Infectious Peritonitis. Viruses, 14(4), 744. https://doi.org/10.3390/v14040744