
Human Protoparvovirus DNA and IgG in Children and Adults with and without Respiratory or Gastrointestinal Infections

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohorts
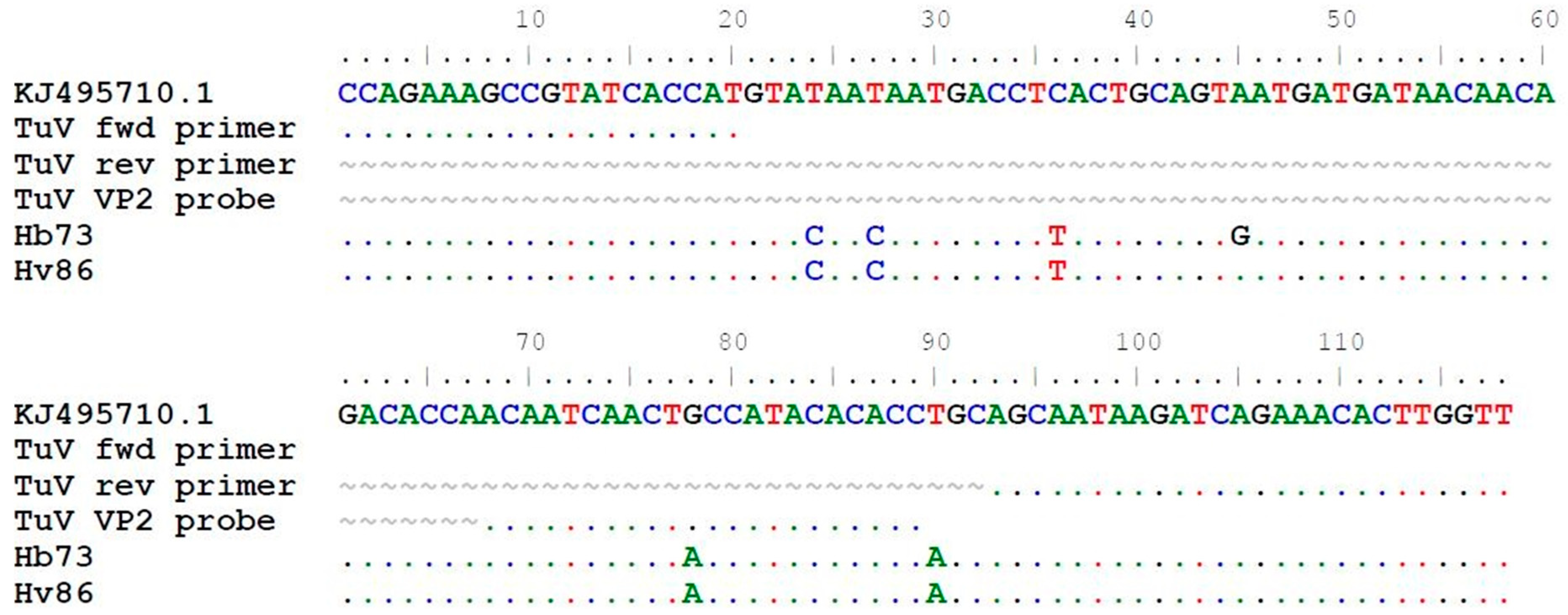
2.2. CuV-BuV-TuV qPCR Assay
2.3. CuV-BuV1-3-TuV IgG EIA
2.4. Statistical Analysis
3. Results
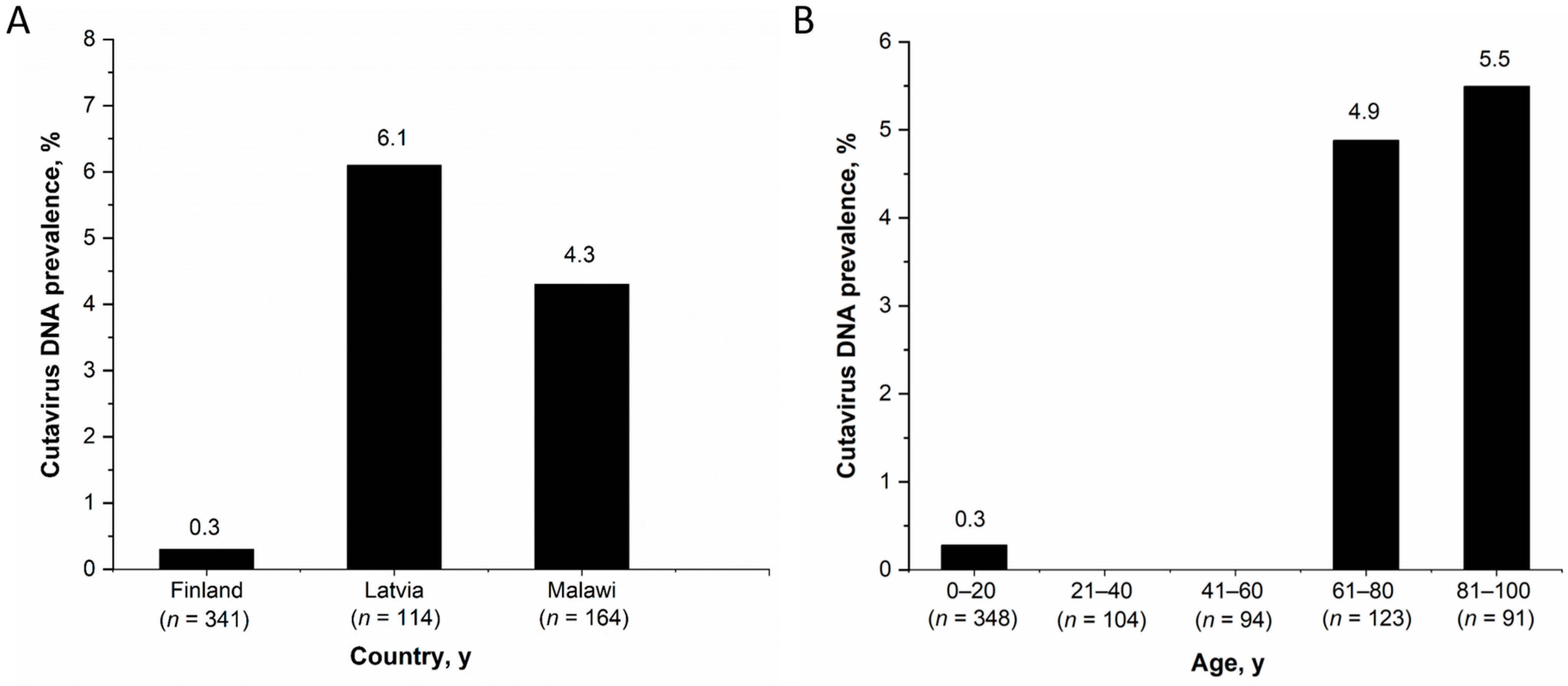
3.1. CuV DNA in Stool and Respiratory Samples
3.2. BuV and TuV DNA in Stool and Respiratory Samples
3.3. Protoparvovirus IgG in Children
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Qiu, J.; Söderlund-Venermo, M.; Young, N.S. Human parvoviruses. Clin. Microbiol. Rev. 2017, 30, 43–113. [Google Scholar] [CrossRef]
- Phan, T.G.; Vo, N.P.; Bonkoungou, I.J.; Kapoor, A.; Barro, N.; O’Ryan, M.; Kapusinszky, B.; Wang, C.; Delwart, E. Acute diarrhea in West African children: Diverse enteric viruses and a novel parvovirus genus. J. Virol. 2012, 86, 11024–11030. [Google Scholar] [CrossRef]
- Phan, T.G.; Sdiri-Loulizi, K.; Aouni, M.; Ambert-Balay, K.; Pothier, P.; Deng, X.; Delwart, E. New parvovirus in child with unexplained diarrhea, Tunisia. Emerg. Infect. Dis. 2014, 20, 1911–1913. [Google Scholar] [CrossRef]
- Phan, T.G.; Dreno, B.; da Costa, A.C.; Li, L.; Orlandi, P.; Deng, X.; Kapusinszky, B.; Siqueira, J.; Knol, A.C.; Halary, F.; et al. A new protoparvovirus in human fecal samples and cutaneous T cell lymphomas (mycosis fungoides). Virology 2016, 496, 299–305. [Google Scholar] [CrossRef]
- Yahiro, T.; Wangchuk, S.; Tshering, K.; Bandhari, P.; Zangmo, S.; Dorji, T.; Tshering, K.; Matsumoto, T.; Nishizono, A.; Söderlund-Venermo, M.; et al. Novel human bufavirus genotype 3 in children with severe diarrhea, Bhutan. Emerg. Infect. Dis. 2014, 20, 1037–1039. [Google Scholar] [CrossRef]
- Väisänen, E.; Fu, Y.; Hedman, K.; Söderlund-Venermo, M. Human protoparvoviruses. Viruses 2017, 9, 354. [Google Scholar] [CrossRef]
- Okitsu, S.; Khamrin, P.; Takanashi, S.; Thongprachum, A.; Hoque, S.A.; Takeuchi, H.; Khan, M.A.; Hasan, S.M.T.; Iwata, T.; Shimizu, H.; et al. Molecular detection of enteric viruses in the stool samples of children without diarrhea in Bangladesh. Infect. Genet. Evol. 2020, 77, 104055. [Google Scholar] [CrossRef]
- Mohammad, H.A.; Madi, N.M.; Al-Nakib, W. Analysis of viral diversity in stool samples from infants and children with acute gastroenteritis in Kuwait using Metagenomics approach. Virol. J. 2020, 17, 10. [Google Scholar] [CrossRef]
- Smits, S.L.; Schapendonk, C.M.E.; van Beek, J.; Vennema, H.; Schürch, A.C.; Schipper, D.; Bodewes, R.; Haagmans, B.L.; Osterhaus, A.D.M.E.; Koopmans, M.P. New viruses in idiopathic human diarrhea cases, the Netherlands. Emerg. Infect. Dis. 2014, 20, 1218–1222. [Google Scholar] [CrossRef]
- Chieochansin, T.; Vutithanachot, V.; Theamboonlers, A.; Poovorawan, Y. Bufavirus in fecal specimens of patients with and without diarrhea in Thailand. Arch. Virol. 2015, 160, 1781–1784. [Google Scholar] [CrossRef]
- Ayouni, S.; Estienney, M.; Hammami, S.; Guediche, M.N.; Pothier, P.; Aouni, M.; Belliot, G.; De Rougemont, A. Cosavirus, Salivirus and Bufavirus in diarrheal Tunisian infants. PLoS ONE 2016, 11, e0162255. [Google Scholar] [CrossRef] [PubMed]
- Väisänen, E.; Kuisma, I.; Phan, T.G.; Delwart, E.; Lappalainen, M.; Tarkka, E.; Hedman, K.; Söderlund-Venermo, M. Bufavirus in feces of patients with gastroenteritis, Finland. Emerg. Infect. Dis. 2014, 20, 1077–1079. [Google Scholar] [CrossRef] [PubMed]
- Väisänen, E.; Paloniemi, M.; Kuisma, I.; Lithovius, V.; Kumar, A.; Franssila, R.; Ahmed, K.; Delwart, E.; Vesikari, T.; Hedman, K.; et al. Epidemiology of two human protoparvoviruses, bufavirus and tusavirus. Sci Rep 2016, 6, 39267. [Google Scholar] [CrossRef] [PubMed]
- Altay, A.; Yahiro, T.; Bozdayi, G.; Matsumoto, T.; Sahin, F.; Ozkan, S.; Nishizono, A.; Söderlund-Venermo, M.; Ahmed, K. Bufavirus genotype 3 in Turkish children with severe diarrhoea. Clin. Microbiol. Infect. 2015, 21, 965.e1–965.e4. [Google Scholar] [CrossRef]
- Huang, D.D.; Wang, W.; Lu, Q.B.; Zhao, J.; Guo, C.T.; Wang, H.Y.; Zhang, X.A.; Tong, Y.G.; Liu, W.; Cao, W.C. Identification of Bufavirus-1 and Bufavirus-3 in feces of patients with acute diarrhea, China. Sci. Rep. 2015, 5, 13272. [Google Scholar] [CrossRef] [PubMed]
- Altan, E.; Del Valle Mendoza, J.; Deng, X.; Phan, T.G.; Sadeghi, M.; Delwarta, E.L. Small circular rep-encoding single-stranded DNA genomes in peruvian diarrhea virome. Genome Announc. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Altan, E.; Aiemjoy, K.; Phan, T.G.; Deng, X.; Aragie, S.; Tadesse, Z.; Callahan, K.E.; Keenan, J.; Delwart, E. Enteric virome of Ethiopian children participating in a clean water intervention trial. PLoS ONE 2018, 13, e0202054. [Google Scholar] [CrossRef]
- Siqueira, J.D.; Dominguez-Bello, M.G.; Contreras, M.; Lander, O.; Caballero-Arias, H.; Xutao, D.; Noya-Alarcon, O.; Delwart, E. Complex virome in feces from Amerindian children in isolated Amazonian villages. Nat. Commun. 2018, 9, 4270. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Latorre, L.; Romero, B.; Bonifaz, E.; Timoneda, N.; Rusiñol, M.; Girones, R.; Rios-Touma, B. Quito’s virome: Metagenomic analysis of viral diversity in urban streams of Ecuador’s capital city. Sci. Total Environ. 2018, 645, 1334–1343. [Google Scholar] [CrossRef]
- Phan, T.; Nagaro, K. Cutavirus: A newly discovered parvovirus on the rise. Infect. Genet. Evol. 2020, 80, 104175. [Google Scholar] [CrossRef]
- Väisänen, E.; Fu, Y.; Koskenmies, S.; Fyhrquist, N.; Wang, Y.; Keinonen, A.; Mäkisalo, H.; Väkevä, L.; Pitkänen, S.; Ranki, A. Cutavirus DNA in malignant and nonmalignant skin of cutaneous T-cell lymphoma and organ transplant patients but not of healthy adults. Clin. Infect. Dis. 2019, 68, 1904–1910. [Google Scholar] [CrossRef]
- Kreuter, A.; Nasserani, N.; Tigges, C.; Oellig, F.; Silling, S.; Akgul, B.; Wieland, U. Cutavirus infection in primary cutaneous B- and T-Cell lymphoma. JAMA Dermatol. 2018, 154, 965–967. [Google Scholar] [CrossRef]
- Mollerup, S.; Fridholm, H.; Vinner, L.; Kjartansdottir, K.R.; Friis-Nielsen, J.; Asplund, M.; Herrera, J.A.; Steiniche, T.; Mourier, T.; Brunak, S.; et al. Cutavirus in cutaneous malignant melanoma. Emerg. Infect. Dis. 2017, 23, 363–365. [Google Scholar] [CrossRef]
- Wieland, U.; Silling, S.; Hufbauer, M.; Mauch, C.; Zigrino, P.; Oellig, F.; Kreuter, A.; Akgül, B. No evidence for role of cutavirus in malignant melanoma. Emerg. Infect. Dis. 2019, 25, 1600–1610. [Google Scholar] [CrossRef]
- Väisänen, E.; Mohanraj, U.; Kinnunen, P.M.; Jokelainen, P.; Al-Hello, H.; Barakat, A.M.; Sadeghi, M.; Jalilian, F.A.; Majlesi, A.; Masika, M.; et al. Global distribution of human protoparvoviruses. Emerg. Infect. Dis. 2018, 24, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Paloniemi, M.; Lappalainen, S.; Salminen, M.; Kätkä, M.; Kantola, K.; Hedman, L.; Hedman, K.; Söderlund-Venermo, M.; Vesikari, T. Human bocaviruses are commonly found in stools of hospitalized children without causal association to acute gastroenteritis. Eur. J. Pediatr. 2014, 173, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Nora-Krukle, Z.; Vilmane, A.; Xu, M.; Rasa, S.; Ziemele, I.; Silina, E.; Söderlund-Venermo, M.; Gardovska, D.; Murovska, M. Human bocavirus infection markers in peripheral blood and stool samples of children with acute gastroenteritis. Viruses 2018, 10, 639. [Google Scholar] [CrossRef] [PubMed]
- Koskenvuo, M.; Möttönen, M.; Rahiala, J.; Saarinen-Pihkala, U.M.; Riikonen, P.; Waris, M.; Ziegler, T.; Uhari, M.; Ruuskanen, O.; Salmi, T.T. Mixed bacterial-viral infections in septic children with leukemia. Pediatr. Infect. Dis. J. 2007, 26, 1133–1136. [Google Scholar] [CrossRef]
- Zanella, M.C.; Cordey, S.; Laubscher, F.; Docquier, M.; Vieille, G.; Van Delden, C.; Braunersreuther, V.; TA, M.K.; Lobrinus, J.A.; Masouridi-Levrat, S.; et al. Unmasking viral sequences by metagenomic next-generation sequencing in adult human blood samples during steroid-refractory/dependent graft-versus-host disease. Microbiome 2021, 9, 28. [Google Scholar] [CrossRef] [PubMed]
- Meriluoto, M.; Hedman, L.; Tanner, L.; Simell, V.; Mäkinen, M.; Simell, S.; Mykkänen, J.; Korpelainen, J.; Ruuskanen, O.; Ilonen, J.; et al. Association of human bocavirus 1 infection with respiratory disease in childhood follow-up study Finland. Emerg. Infect. Dis. 2012, 18, 264–271. [Google Scholar] [CrossRef]
- Li, X.; Kantola, K.; Hedman, L.; Arku, B.; Hedman, K.; Söderlund-Venermo, M. Original antigenic sin with human bocaviruses 1–4. J. Gen. Virol. 2015, 96, 3099–3108. [Google Scholar] [CrossRef]
- Inaba, H.; Pei, D.; Wolf, J.; Howard, S.C.; Hayden, R.T.; Go, M.; Varechtchouk, O.; Hahn, T.; Buaboonnam, J.; Metzger, M.L.; et al. Infection-related complications during treatment for childhood acute lymphoblastic leukemia. Ann. Oncol. 2017, 28, 386–392. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Cohort | No. of Individuals Studied (N = 1098) | Health Status * | Age Range (Median age, y) | Gender | Time of Sample Collection | Sample Type Analyzed * |
|---|---|---|---|---|---|---|
| Helsinki-B | 212 | GE | 1 to 94 years (36) | Female, N = 113, Male, N = 99 | October 2012–March 2013 | Stool |
| Helsinki-V | 285 | GE | 0 to 99 years (74) | Female N = 154, Male N = 131 | April-June, 2013 | Stool |
| Tampere | 228 | GE and/or RTI | 0 to 15 years (1.3) | Female, N = 94, Male, N = 134 | September 2009–August 2011 | Stool, nasal swab and serum |
| Latvia | 159 | GE and/or RTI | 0 to 5 years (1.7) | Female, N = 59, Male, N = 100 | November 2013–April 2017 | Stool, NPA and plasma |
| Malawi | 164 | Healthy or diseased | 6 or 12 months | Female, N = 73 Male, N = 91 | January 2008–November 2009 | Stool |
| Leukemia | 50 | AML or ALL | 0 to 15 years (5.7) † | Female, N = 17 Male, N = 33 | April 2001–October 2004 | Stool, nasal swab and serum |
| Cohort | Sample Type | CuV DNA Positive Patients (Prevalence; 95% CI) | BuV DNA Positive Patients (Prevalence; 95% CI) | TuV DNA Positive Patients (Prevalence; 95% CI) |
|---|---|---|---|---|
| Helsinki-B | Stool | 1/212 (0.5%; 0.0–2.7) | 4/243 (1.6%; 0.0–4.5) † | 1/212 (0.47%; 0.0–2.7) |
| Helsinki-V ¶ | Stool | 10/285 (3.5%; 0.6–7.3) | 3/386 (0.7%; 0.0–2.0) ‡ | 1/285 (0.35%; 0.0–1.7) |
| Tampere | Stool | 1/228 (0.4%; 0.0–2.4) | 3/955 (0.3%; 0.0–0.5) § | 0/228 |
| Nasal swab | 0/228 | 1/955 (0.1%; 0.0–0.2) § | 0/228 | |
| Latvia | Stool | 7/115 (6.1%; 2.2–15.1) | 0/115 | 0/115 |
| NPA | 2/44 (4.5%; 0.0–20.1) | 0/44 | 0/44 | |
| Malawi | Stool | 7/164 (4.3%; 0.8–10.4) | 1/164 (0.6%; 0.0–3.7) | 0/164 |
| Leukemia | Stool | 0/35 | 0/35 | 0/35 |
| Nasal swab | 0/32 | 0/32 | 0/32 |
| Patient No. | Copies per ml † | Age/Gender | Sampling Date | Other Pathogens Found | Symptoms and Signs |
|---|---|---|---|---|---|
| CuV DNA positives | |||||
| Hb40 | 1.69 × 102 | 79 years/F | 2013 Feb 07 | GE | |
| Hv61 | 7.99 × 103 | 77 years/F | 2013 Apr 18 | - | GE |
| Hv99 | 1.05 × 104 | 89 years/M | 2013 Apr 16 | - | GE |
| Hv92 | NA | 90 years/M | 2013 Apr 20 | NoV | GE |
| Hv57 | 2.65 × 102 | 78 years/M | 2013 Apr 29 | - | GE |
| Hv93 | 3.57 × 102 | 87 years/M | 2013 May 04 | - | GE |
| Hv05 | 1.93 × 102 | 80 years/M | 2013 May 02 | - | GE |
| Hv65 | 9.61 × 102 | 77 years/M | 2013 May 10 | - | GE |
| Hv69 | 1.30 × 103 | 81 years/M | 2013 May 13 | - | GE |
| Hv78 | 9.93 × 103 | 67 years/M | 2013 May 13 | - | GE |
| Hv31 | 1.24 × 102 | 99 years/F | 2013 May 24 | - | GE |
| Ta13 | 1.43 × 103 | 10 years/M | 2009 May 04 | - | GE/RTI |
| La42 | 1.50 × 102 | 1 year/F | 2015 Jan 20 | RSVB | RTI, Fever |
| La46 | 3.22 × 103 | 1 year/M | 2015 Feb 03 | HBoV1 | RTI, Fever |
| La82 | 9.28 × 102 | 7 months/M | 2016 Jan 26 | - | GE, fever, RTI |
| La03 | 5.15 × 102 | 3 years/M | 2016 Mar 24 | HBoV1 and RoV | GE |
| La14 | 1.40 × 103 | 2 years/M | 2016 May 19 | - | GE and fever |
| La43 | 1.37 × 103 | 2 years/M | 2016 Oct 05 | - | GE and fever |
| La63 | 6.27 × 103 | 3 years/M | 2016 Nov 03 | NoV | GE and fever |
| La49 | 8.62 × 102 ‡ | 45 months/M | 2016 Oct 18 | HBoV1 | Fever, RTI |
| La50 | 2.04 × 103 ‡ | 39 months/M | 2016 Oct 19 | HBoV1; HRV | Fever, RTI |
| Ma25 | 9.57 × 102 | 6 months/M | 2008 Apr 07 | - | Data not available |
| Ma40 § | 4.35 × 102 | 1 year/M | 2008 Dec 18 | - | Healthy |
| Ma61 | 5.44 × 103 | 1 year/F | 2008 Dec 31 | - | Data not available |
| Ma99 | 1.41 × 103 | 1 year/M | 2009 Jan 14 | - | Healthy |
| Ma66 | 2.20 × 103 | 1 year/M | 2009 Mar 17 | - | Healthy |
| Ma45 | 2.76 × 103 | 6 months/F | 2008 Nov 27 | - | Fever |
| Ma06 | 5.21 × 102 | 6 months/F | 2009 Jan 16 | - | Healthy |
| BuV DNA positives# | |||||
| Ma14 | 1.23 × 103 | 6 months/M | 2009 Jul 02 | - | Healthy |
| TuV DNA positives | |||||
| Hb73 ¶ | 4.42 × 101 | 27 years/F | 2013 Feb 25 | - | GE |
| Hv86 | 8.90 × 101 ** | 22 years/F | 2013 May 14 | - | GE |
| Patient (Symptoms) | Sample Type | Sampling Date of Stool/NPA and sera | CuV DNA (Copies/mL of Supernatant) | CuV IgG EIA Absorbances ‡ |
|---|---|---|---|---|
| La49 (RTI) | Stool | NA | 0.038 | |
| NPA | 2016 Oct 18 | Pos (8.62 ×102) | ||
| La50 (RTI) | Stool | NA | 0.039 | |
| NPA | 2016 Oct 19 | Pos (2.04 ×103) | ||
| La42 (RTI) | Stool | 2015 Jan 20 | Pos (1.50 × 102) | NA |
| NPA | 2015 Jan 20 | Neg | ||
| La46 (RTI) | Stool | 2015 Feb 03 | Pos (3.22 × 103) | NA |
| NPA | NA | |||
| La82 (GE and RTI) | Stool | 2016 Jan 26 | Pos (9.28 × 102) | 0.018 |
| NPA | NA | |||
| La03 (GE) | Stool | 2016 Mar 24 | Pos (5.15 × 102) | 0.015 |
| NPA | NA | |||
| La14 (GE) | Stool | 2016 May 19 | Pos (1.40 × 103) | 0.527 † |
| NPA | NA | |||
| La43 (GE) | Stool | 2016 Oct 05 | Pos (1.37 × 103) | NA |
| NPA | NA | |||
| La63 (GE) | Stool | 2016 Nov 03 | Pos (6.27 × 103) | NA |
| NPA | NA | |||
| La00 (GE) | Stool | 2016 Mar 04 | Neg | 0.228 |
| NPA | NA | |||
| La78 (GE) | Stool | 2016 Jan 15 | Neg | 0.976 |
| NPA | NA | |||
| La34 (RTI) | Stool | NA | 0.326 | |
| NPA | ||||
| Ta13 (GE and RTI) | Stool | 2009 Nov 04 | Pos (1.43 × 103) | 0.050 |
| Nasal swab | 2009 Nov 04 | Neg | ||
| Ta47 (RTI) | Stool | 2009 Sep 28 | Neg | 0.873 |
| Nasal swab | 2009 Sep 28 | Neg | ||
| Ta69 (RTI) | Stool | 2011 Feb 21 | Neg | 2.683 |
| Nasal swab | 2011 Feb 20 | Neg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohanraj, U.; Jokinen, M.; Thapa, R.R.; Paloniemi, M.; Vesikari, T.; Lappalainen, M.; Tarkka, E.; Nora-Krūkle, Z.; Vilmane, A.; Vettenranta, K.; et al. Human Protoparvovirus DNA and IgG in Children and Adults with and without Respiratory or Gastrointestinal Infections. Viruses 2021, 13, 483. https://doi.org/10.3390/v13030483
Mohanraj U, Jokinen M, Thapa RR, Paloniemi M, Vesikari T, Lappalainen M, Tarkka E, Nora-Krūkle Z, Vilmane A, Vettenranta K, et al. Human Protoparvovirus DNA and IgG in Children and Adults with and without Respiratory or Gastrointestinal Infections. Viruses. 2021; 13(3):483. https://doi.org/10.3390/v13030483
Chicago/Turabian StyleMohanraj, Ushanandini, Maija Jokinen, Rajita Rayamajhi Thapa, Minna Paloniemi, Timo Vesikari, Maija Lappalainen, Eveliina Tarkka, Zaiga Nora-Krūkle, Anda Vilmane, Kim Vettenranta, and et al. 2021. "Human Protoparvovirus DNA and IgG in Children and Adults with and without Respiratory or Gastrointestinal Infections" Viruses 13, no. 3: 483. https://doi.org/10.3390/v13030483
APA StyleMohanraj, U., Jokinen, M., Thapa, R. R., Paloniemi, M., Vesikari, T., Lappalainen, M., Tarkka, E., Nora-Krūkle, Z., Vilmane, A., Vettenranta, K., Mangani, C., Oikarinen, S., Fan, Y.-M., Ashorn, P., Väisänen, E., & Söderlund-Venermo, M. (2021). Human Protoparvovirus DNA and IgG in Children and Adults with and without Respiratory or Gastrointestinal Infections. Viruses, 13(3), 483. https://doi.org/10.3390/v13030483