
Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Population
3.2. COVID-19 Outcomes According to SARS-CoV-2 Ct
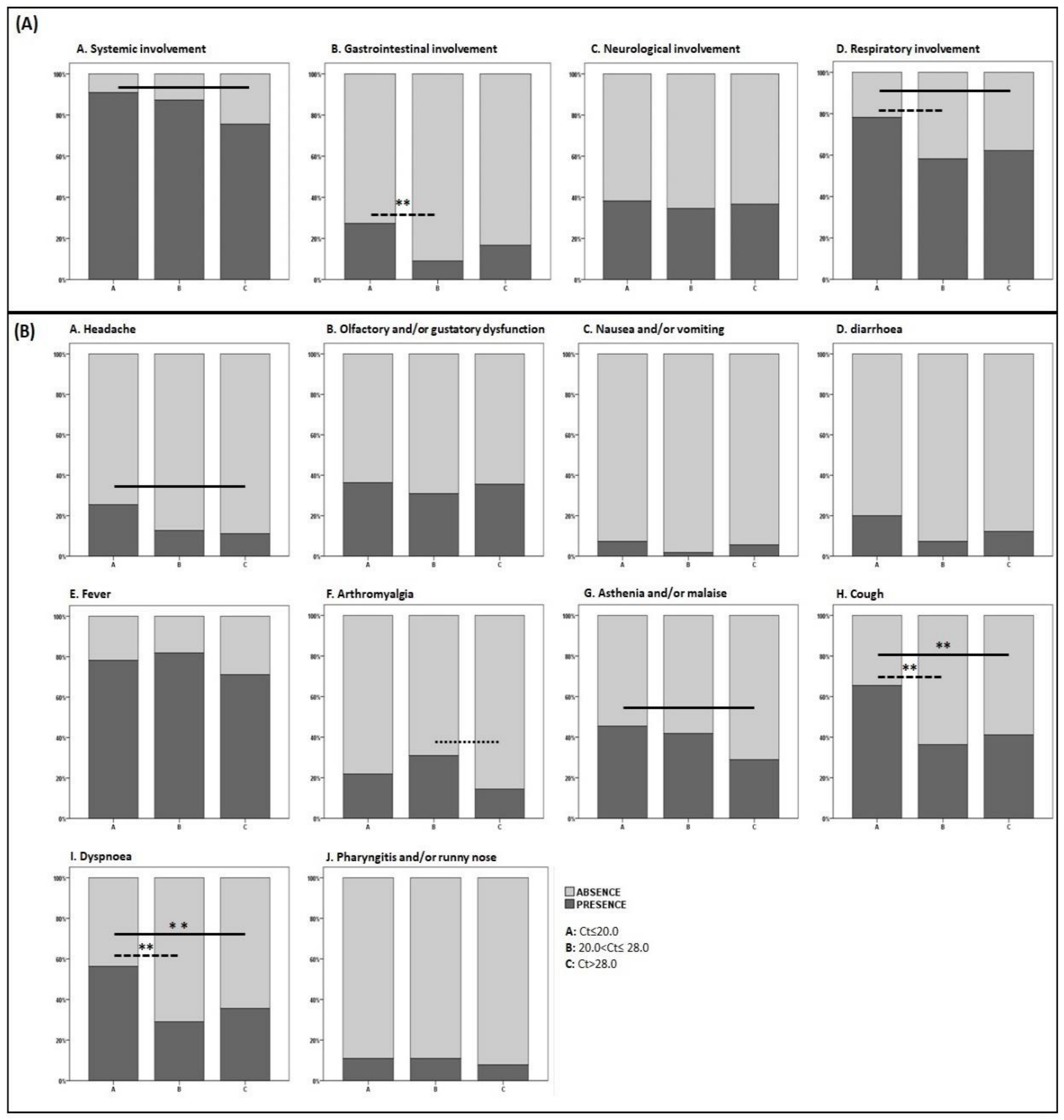
3.3. Clinical Presentation at Diagnosis According to SARS-CoV-2 Ct
3.4. Six-Month Sequelae According to SARS-CoV-2 Ct
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Ssentongo, P.; Ssentongo, A.E.; Heilbrunn, E.S.; Ba, D.M.; Chinchilli, V.M. Association of Cardiovascular Disease and 10 Other Pre-Existing Comorbidities with COVID-19 Mortality: A Systematic Review and Meta-Analysis. PLoS One 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Tu, C.; Zhou, F.; Liu, Z.; Wang, Y.; Song, B.; Gu, X.; Wang, Y.; Wei, Y.; Li, H.; et al. Comparison of Severity Scores for COVID-19 Patients with Pneumonia: A Retrospective Study. Eur. Respir. J. 2020, 56. [Google Scholar] [CrossRef]
- Wendel Garcia, P.D.; Fumeaux, T.; Guerci, P.; Heuberger, D.M.; Montomoli, J.; Roche-Campo, F.; Schuepbach, R.A.; Hilty, M.P. RISC-19-ICU Investigators Prognostic Factors Associated with Mortality Risk and Disease Progression in 639 Critically Ill Patients with COVID-19 in Europe: Initial Report of the International RISC-19-ICU Prospective Observational Cohort. EClinicalMedicine 2020, 25, 100449. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 Illness in Native and Immunosuppressed States: A Clinical–Therapeutic Staging Proposal. J. Heart Lung Transpl. 2020, 39, 405–407. [Google Scholar] [CrossRef]
- Rao, S.N.; Manissero, D.; Steele, V.R.; Pareja, J. A Narrative Systematic Review of the Clinical Utility of Cycle Threshold Values in the Context of COVID-19. Infect. Dis. Ther. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Magleby, R.; Westblade, L.F.; Trzebucki, A.; Simon, M.S.; Rajan, M.; Park, J.; Goyal, P.; Safford, M.M.; Satlin, M.J. Impact of SARS-CoV-2 Viral Load on Risk of Intubation and Mortality Among Hospitalized Patients with Coronavirus Disease 2019. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Salvatore, P.P.; Dawson, P.; Wadhwa, A.; Rabold, E.M.; Buono, S.; Dietrich, E.A.; Reses, H.E.; Vuong, J.; Pawloski, L.; Dasu, T.; et al. Epidemiological Correlates of PCR Cycle Threshold Values in the Detection of SARS-CoV-2. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Brar, G.; Pinheiro, L.C.; Paidoussis, D.; Rajan, M.; Martin, P.; Goyal, P.; Sepulveda, J.L.; Zhang, L.; George, G.; et al. SARS-CoV-2 Viral Load Predicts Mortality in Patients with and without Cancer Who Are Hospitalized with COVID-19. Cancer Cell 2020. [Google Scholar] [CrossRef] [PubMed]
- Pujadas, E.; Chaudhry, F.; McBride, R.; Richter, F.; Zhao, S.; Wajnberg, A.; Nadkarni, G.; Glicksberg, B.S.; Houldsworth, J.; Cordon-Cardo, C. SARS-CoV-2 Viral Load Predicts COVID-19 Mortality. Lancet Respir. Med. 2020, 8, e70. [Google Scholar] [CrossRef]
- Faíco-Filho, K.S.; Passarelli, V.C.; Bellei, N. Is Higher Viral Load in SARS-CoV-2 Associated with Death? Am. J. Trop. Med. Hyg. 2020. [Google Scholar] [CrossRef]
- Shlomai, A.; Ben-Zvi, H.; Glusman Bendersky, A.; Shafran, N.; Goldberg, E.; Sklan, E.H. Nasopharyngeal Viral Load Predicts Hypoxemia and Disease Outcome in Admitted COVID-19 Patients. Crit. Care 2020, 24, 539. [Google Scholar] [CrossRef] [PubMed]
- Lesho, E.; Reno, L.; Newhart, D.; Clifford, R.; Vasylyeva, O.; Hanna, J.; Yu, S.; Bress, J.; Walsh, E. Temporal, Spatial, and Epidemiologic Relationships of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Gene Cycle Thresholds: A Pragmatic Ambi-Directional Observation. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Argyropoulos, K.V.; Serrano, A.; Hu, J.; Black, M.; Feng, X.; Shen, G.; Call, M.; Kim, M.J.; Lytle, A.; Belovarac, B.; et al. Association of Initial Viral Load in Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Patients with Outcome and Symptoms. Am. J. Pathol. 2020, 190, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- Ra, S.H.; Lim, J.S.; Kim, G.; Kim, M.J.; Jung, J.; Kim, S.-H. Upper Respiratory Viral Load in Asymptomatic Individuals and Mildly Symptomatic Patients with SARS-CoV-2 Infection. Thorax 2020. [Google Scholar] [CrossRef]
- Asai, N.; Sakanashi, D.; Ohashi, W.; Nakamura, A.; Yamada, A.; Kawamoto, Y.; Miyazaki, N.; Ohno, T.; Koita, I.; Suematsu, H.; et al. Could Threshold Cycle Value Correctly Reflect the Severity of Novel Coronavirus Disease 2019 (COVID-19)? J. Infect. Chemother. 2021, 27, 117–119. [Google Scholar] [CrossRef]
- De la Calle, C.; Lalueza, A.; Mancheño-Losa, M.; Maestro-de la Calle, G.; Lora-Tamayo, J.; Arrieta, E.; García-Reyne, A.; Losada, I.; de Miguel, B.; Díaz-Simón, R.; et al. Impact of Viral Load at Admission on the Development of Respiratory Failure in Hospitalized Patients with SARS-CoV-2 Infection. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 1–8. [Google Scholar] [CrossRef]
- Han, A.; Czajkowski, L.M.; Donaldson, A.; Baus, H.A.; Reed, S.M.; Athota, R.S.; Bristol, T.; Rosas, L.A.; Cervantes-Medina, A.; Taubenberger, J.K.; et al. A Dose-Finding Study of a Wild-Type Influenza A(H3N2) Virus in a Healthy Volunteer Human Challenge Model. Clin. Infect. Dis. 2019, 69, 2082–2090. [Google Scholar] [CrossRef]
- Chu, C.-M.; Poon, L.L.M.; Cheng, V.C.C.; Chan, K.-S.; Hung, I.F.N.; Wong, M.M.L.; Chan, K.-H.; Leung, W.-S.; Tang, B.S.F.; Chan, V.L.; et al. Initial Viral Load and the Outcomes of SARS. CMAJ 2004, 171, 1349–1352. [Google Scholar] [CrossRef]
- Shi, F.; Wu, T.; Zhu, X.; Ge, Y.; Zeng, X.; Chi, Y.; Du, X.; Zhu, L.; Zhu, F.; Zhu, B.; et al. Association of Viral Load with Serum Biomakers among COVID-19 Cases. Virology 2020, 546, 122–126. [Google Scholar] [CrossRef]
- Chen, X.; Zhao, B.; Qu, Y.; Chen, Y.; Xiong, J.; Feng, Y.; Men, D.; Huang, Q.; Liu, Y.; Yang, B.; et al. Detectable Serum SARS-CoV-2 Viral Load (RNAaemia) Is Closely Correlated with Drastically Elevated Interleukin 6 (IL-6) Level in Critically Ill COVID-19 Patients. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-Month Consequences of COVID-19 in Patients Discharged from Hospital: A Cohort Study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Cerutti, F.; Burdino, E.; Milia, M.G.; Allice, T.; Gregori, G.; Bruzzone, B.; Ghisetti, V. Urgent Need of Rapid Tests for SARS CoV-2 Antigen Detection: Evaluation of the SD-Biosensor Antigen Test for SARS-CoV-2. J. Clin. Virol. 2020, 132, 104654. [Google Scholar] [CrossRef] [PubMed]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.W.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 Novel Coronavirus (2019-NCoV) by Real-Time RT-PCR. Euro Surveill. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Binnicker, M.J. Can the SARS-CoV-2 PCR Cycle Threshold Value and Time from Symptom Onset to Testing Predict Infectivity? Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Singanayagam, A.; Patel, M.; Charlett, A.; Lopez Bernal, J.; Saliba, V.; Ellis, J.; Ladhani, S.; Zambon, M.; Gopal, R. Duration of Infectiousness and Correlation with RT-PCR Cycle Threshold Values in Cases of COVID-19, England, January to May 2020. Euro Surv. 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Arons, M.M.; Hatfield, K.M.; Reddy, S.C.; Kimball, A.; James, A.; Jacobs, J.R.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; et al. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Kimball, A.; Hatfield, K.M.; Arons, M.; James, A.; Taylor, J.; Spicer, K.; Bardossy, A.C.; Oakley, L.P.; Tanwar, S.; Chisty, Z.; et al. Asymptomatic and Presymptomatic SARS-CoV-2 Infections in Residents of a Long-Term Care Skilled Nursing Facility—King County, Washington, March 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 377–381. [Google Scholar] [CrossRef]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses during Infection by SARS-CoV-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef]
- Jacot, D.; Greub, G.; Jaton, K.; Opota, O. Viral Load of SARS-CoV-2 across Patients and Compared to Other Respiratory Viruses. Microbes Infect. 2020. [Google Scholar] [CrossRef]
- Karahasan Yagci, A.; Sarinoglu, R.C.; Bilgin, H.; Yanılmaz, Ö.; Sayın, E.; Deniz, G.; Guncu, M.M.; Doyuk, Z.; Barıs, C.; Kuzan, B.N.; et al. Relationship of the Cycle Threshold Values of SARS-CoV-2 Polymerase Chain Reaction and Total Severity Score of Computerized Tomography in Patients with COVID 19. Int. J. Infect. Dis. 2020, 101, 160–166. [Google Scholar] [CrossRef]
- Zacharioudakis, I.M.; Zervou, F.N.; Prasad, P.J.; Shao, Y.; Basu, A.; Inglima, K.; Weisenberg, S.A.; Aguero-Rosenfeld, M.E. Association of SARS-CoV-2 Genomic Load Trends with Clinical Status in COVID-19: A Retrospective Analysis from an Academic Hospital Center in New York City. PLoS One 2020, 15, e0242399. [Google Scholar] [CrossRef] [PubMed]
- Zacharioudakis, I.M.; Prasad, P.J.; Zervou, F.N.; Basu, A.; Inglima, K.; Weisenberg, S.A.; Aguero-Rosenfeld, M.E. Association of SARS-CoV-2 Genomic Load with COVID-19 Patient Outcomes. Ann. Am. Thorac. Soc. 2020. [Google Scholar] [CrossRef]
- Nakagawara, K.; Masaki, K.; Uwamino, Y.; Kabata, H.; Uchida, S.; Uno, S.; Asakura, T.; Funakoshi, T.; Kanzaki, S.; Ishii, M.; et al. Acute Onset Olfactory/Taste Disorders Are Associated with a High Viral Burden in Mild or Asymptomatic SARS-CoV-2 Infections. Int. J. Infect. Dis. 2020, 99, 19. [Google Scholar] [CrossRef] [PubMed]
- Cho, R.H.; To, Z.W.; Yeung, Z.W.; Tso, E.Y.; Fung, K.S.; Chau, S.K.; Leung, E.Y.; Hui, T.S.; Tsang, S.W.; Kung, K.N.; et al. COVID-19 Viral Load in the Severity of and Recovery from Olfactory and Gustatory Dysfunction. Laryngoscope 2020. [Google Scholar] [CrossRef] [PubMed]
- Lv, H.; Zhang, W.; Zhu, Z.; Xiong, Q.; Xiang, R.; Wang, Y.; Shi, W.; Deng, Z.; Xu, Y. Prevalence and Recovery Time of Olfactory and Gustatory Dysfunction in Hospitalized Patients with COVID-19 in Wuhan, China. Int. J. Infect. Dis. 2020, 100, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.K.; Stoltey, J.E.; Scott, H.M.; Trammell, S.; Ememu, E.; Samuel, M.C.; Aragon, T.J.; Masinde, G. Comparison of Symptomatic and Asymptomatic Infections Due to Severe Acute Respiratory Coronavirus Virus 2 (SARS-CoV-2) in San Francisco Long-Term Care Facilities. Infect. Control. Hosp. Epidemiol. 1–3. [CrossRef]
- Long, Q.-X.; Tang, X.-J.; Shi, Q.-L.; Li, Q.; Deng, H.-J.; Yuan, J.; Hu, J.-L.; Xu, W.; Zhang, Y.; Lv, F.-J.; et al. Clinical and Immunological Assessment of Asymptomatic SARS-CoV-2 Infections. Nat. Med. 2020, 26, 1200–1204. [Google Scholar] [CrossRef]
- Saponaro, F.; Rutigliano, G.; Sestito, S.; Bandini, L.; Storti, B.; Bizzarri, R.; Zucchi, R. ACE2 in the Era of SARS-CoV-2: Controversies and Novel Perspectives. Front. Mol. Biosci. 2020, 7. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Wang, H.; Liu, Z. Expression of ACE2 in Airways: Implication for COVID-19 Risk and Disease Management in Patients with Chronic Inflammatory Respiratory Diseases. Clin. Exp. Allergy 2020. [Google Scholar] [CrossRef]
- Han, M.S.; Byun, J.-H.; Cho, Y.; Rim, J.H. RT-PCR for SARS-CoV-2: Quantitative versus Qualitative. Lancet Infect. Dis. 2021, 21. [Google Scholar] [CrossRef]
- Favalli, E.G.; Biggioggero, M.; Maioli, G.; Caporali, R. Baricitinib for COVID-19: A Suitable Treatment? Lancet Infect. Dis. 2020, 20, 1012–1013. [Google Scholar] [CrossRef]
- Trunfio, M.; Salvador, E.; Gaviraghi, A.; Audagnotto, S.; Marinaro, L.; Motta, I.; Casciaro, R.; Ghisetti, V.; Fava, C.; Bonora, S.; et al. Early Low-Molecular-Weight Heparin Administration Is Associated with Shorter Time to SARS-CoV-2 Swab Negativity. Antivir. Ther. 2021. [Google Scholar] [CrossRef] [PubMed]
- Cubeddu, L.X.; Cubeddu, R.J. Early Remdesivir Treatment in Covid-19: Why Wait Another Day? J. Med. Virol. 2021. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Population |
|---|---|
| (n = 200) | |
| Median SARS-CoV-2 PCR Ct | |
| Group A, Ct ≤ 20.0 | 18.9 (17.9–19.5) |
| Group B, 20.0 < Ct ≤ 28.0 | 22.9 (22.0–25.2) |
| Group C, Ct > 28.0 | 34.0 (30.8–36.9) |
| Hospital admissions, n | 127 (63.5%) |
| Symptomatic, n | 180 (90.0%) |
| Signs and symptoms according to main systems, n | |
| Systemic inflammatory involvement | 166 (83.0%) |
| Neurological involvement | 73 (36.5%) |
| Gastroenterological involvement | 35 (17.5%) |
| Respiratory involvement | 131 (65.5%) |
| Time between symptoms onset and diagnostic swab collection, days * | 5 (3–8) |
| Outcomes, n | |
| Complete recovery | 127 (63.5%) |
| Sequelae | 41 (20.5%) |
| Death | 32 (16.0%) |
| Type of Sequelae, n | |
| Dyspnea | 21 (12.5%) |
| Olfactory and/or gustatory dysfunction | 13 (7.7%) |
| Chronic cough | 7 (4.2%) |
| Others | 6 (3.6%) |
| Worst oxygen support, n | |
| None | 99 (49.5%) |
| Wall low-flow oxygen to reservoir | 60 (30.0%) |
| CPAP | 29 (14.5%) |
| Intubation | 12 (6.0%) |
| Comorbidities, n | |
| None | 82 (41.0%) |
| Hypertension | 56 (28.0%) |
| COPD/asthma | 33 (16.5%) |
| Overweight/obesity | 27 (13.5%) |
| Active smoking | 23 (11.5%) |
| Diabetes | 19 (9.5%) |
| Cancer | 17 (8.5%) |
| Others | 46 (23.0%) |
| Disease severity, n | |
| Home isolation | 73 (36.5%) |
| Hospital admission without oxygen support | 26 (13.0%) |
| Hospital admission with low-flow oxygen to reservoir | 39 (19.5%) |
| Hospital admission with CPAP | 20 (10.0%) |
| Hospital admission with intubation | 10 (5.0%) |
| Death | 32 (16.0%) |
| A | B | C | p | η2 | A vs. B * | A vs. C * | B vs. C * | |
|---|---|---|---|---|---|---|---|---|
| Ct ≤ 20 | 20 < Ct ≤ 28 | Ct > 28 | ||||||
| (n = 55) | (n = 55) | (n = 90) | ||||||
| Age, years | 64 (39–78) | 57 (50–67) | 52 (40–63) | 0.017 | 0.396 | 0.381 | 0.011 | 0.025 |
| Male sex, n | 31 (56.4%) | 32 (58.2%) | 53 (58.9%) | 0.956 | - | 0.848 | 0.766 | 0.933 |
| Comorbidity, n | ||||||||
| None | 15 (27.3%) | 23 (41.8%) | 49 (54.4%) | 0.006 | 0.052 | 0.375 | 0.004 | 0.413 |
| Hypertension | 27 (49.1%) | 13 (23.6%) | 16 (17.8%) | <0.0005 | 0.077 | <0.0005 | 0.009 | 0.999 |
| COPD/asthma | 12 (21.8%) | 6 (10.9%) | 15 (16.7%) | 0.306 | - | 0.124 | 0.441 | 0.341 |
| Overweight/obesity | 8 (14.5%) | 8 (14.5%) | 11 (12.2%) | 0.892 | - | 0.999 | 0.689 | 0.689 |
| Active Smoking | 12 (21.8%) | 2 (3.6%) | 9 (10.0%) | 0.01 | 0.017 | 0.009 | 0.093 | 0.735 |
| Diabetes | 8 (14.5%) | 6 (10.9%) | 5 (5.6%) | 0.186 | - | 0.569 | 0.067 | 0.239 |
| Cancer | 5 (9.1%) | 5 (9.1%) | 7 (7.8%) | 0.947 | - | 0.999 | 0.781 | 0.781 |
| Others | 11 (20.0%) | 19 (34.5%) | 16 (17.8%) | 0.08 | - | 0.164 | 0.515 | 0.028 |
| Time from COVID-19 onset to swab collection, days | 3 (2–5) | 5 (3–9) | 5 (3–10) | 0.011 | 0.144 | 0.02 | 0.026 | 0.999 |
| Number of signs and symptoms at diagnosis, n | 4 (3–6) | 3 (2–4) | 3 (2–3) | 0.007 | 0.058 | 0.037 | 0.008 | 0.977 |
| Hospital admissions, n | 41 (74.5%) | 35 (63.6%) | 51 (56.7%) | 0.096 | - | 0.218 | 0.031 | 0.409 |
| Worst oxygen support, n | 0.495 | - | 0.923 | 0.28 | 0.377 | |||
| None | 24 (43.6%) | 28 (50.9%) | 47 (52.2%) | |||||
| Low-flow wall oxygen to reservoir | 20 (36.4%) | 11 (20.0%) | 29 (32.2%) | |||||
| CPAP | 7 (12.7%) | 11 (20.0%) | 11 (12.2%) | |||||
| Intubation | 4 (7.3%) | 5 (9.1%) | 3 (3.3%) | |||||
| Outcomes, n | <0.0005 | 0.191 | <0.0005 | <0.0005 | 0.678 | |||
| Complete recovery | 16 (29.1%) | 39 (70.9%) | 72 (80.0%) | |||||
| Sequelae | 19 (34.5%) | 9 (16.4%) | 13 (14.4%) | |||||
| Death | 20 (36.4%) | 7 (12.7%) | 5 (5.6%) | |||||
| Disease severity, n | 0.004 | 0.169 | 0.204 | 0.003 | 0.62 | |||
| Home isolation | 14 (25.4%) | 20 (36.4%) | 39 (43.3%) | |||||
| Hospital admission: | ||||||||
| Without oxygen support | 10 (18.2%) | 8 (14.5%) | 8 (8.9%) | |||||
| With low-flow wall oxygen to reservoir | 5 (9.1%) | 8 (14.5%) | 26 (28.9%) | |||||
| With CPAP | 3 (5.4%) | 7 (12.7%) | 10 (11.1%) | |||||
| With intubation | 3 (5.4%) | 5 (9.1%) | 2 (2.2%) | |||||
| Death | 20 (36.4%) | 7 (12.7%) | 5 (5.6%) | |||||
| A | B | C | p | η2 | A vs. B * | A vs. C * | B vs. C * | |
| Ct ≤ 20 | 20 < Ct ≤ 28 | Ct > 28 | ||||||
| (n = 35) | (n = 48) | (n = 85) | ||||||
| Outcomes among survivors, n | <0.0005 | 0.162 | 0.001 | <0.0005 | 0.999 | |||
| Complete recovery | 16 (45.7%) | 39 (81.2%) | 72 (84.7%) | |||||
| Sequelae | 19 (54.3%) | 9 (18.8%) | 13 (15.3%) | |||||
| Type of Sequelae, n | ||||||||
| Dyspnea | 11 (57.9%) | 1 (11.1%) | 9 (69.2%) | 0.022 | 0.004 | 0.067 | 0.999 | 0.024 |
| O/G dysfunction | 6 (31.6%) | 4 (44.4%) | 3 (23.1%) | 0.579 | - | 0.677 | 0.704 | 0.376 |
| Chronic cough | 3 (15.8%) | 3 (33.3%) | 1 (7.7%) | 0.294 | - | 0.352 | 0.264 | 0.264 |
| Others | 3 (15.8%) | 1 (11.1%) | 2 (15.4%) | 0.945 | - | 0.998 | 0.976 | 0.999 |
| COVID-19-Related Death (n 180) * | ||
| aOR (95CI) | p | |
| SARS-CoV-2 Ct | 0.84 (0.72–0.97) | 0.023 |
| Age | 1.25 (1.11–1.40) | <0.01 |
| Sex | 1.26 (0.21–7.55) | 0.80 |
| Time from COVID-19 onset to diagnostic swab | 1.03 (0.91–1.18) | 0.63 |
| Number of comorbidities | 2.44 (1.18–5.04) | 0.016 |
| Worst oxygen support None Low-flow wall oxygen-reservoir CPAP Intubation | – 2.01 (0.14–8.98) 2.14 (0.65–7.01) 2.38 (0.94–6.06) | - 0.61 0.34 0.068 |
| COVID-19 Severity (n 180) * | ||
| aOR (95CI) | p | |
| SARS-CoV-2 Ct | 0.95 (0.91–0.99) | 0.023 |
| Age | 1.08 (1.06–1.11) | <0.01 |
| Sex | 0.31 (0.17–0.58) | <0.01 |
| Time from COVID-19 onset to diagnostic swab | 1.04 (0.98–1.11) | 0.21 |
| Number of comorbidities | 1.6 (1.29–2.03) | <0.01 |
| Number of signs and symptoms at diagnosis (n 180) * | ||
| β (95CI) | p | |
| SARS-CoV-2 Ct | −0.060 (−0.10; −0.018) | <0.01 |
| Age | −0.013 (−0.32; 0.006) | 0.17 |
| Sex | −0.12 (−0.69; 0.44) | 0.67 |
| Number of comorbidities | 0.24 (−0.013; 0.50) | 0.063 |
| Time from COVID-19 onset to diagnostic swab | −0.12 (−0.62; 0.51) | 0.99 |
| 6-month sequelae in survivors (n 149) * | ||
| aOR (95CI) | p | |
| SARS-CoV-2 Ct | 0.90 (0.85–0.96) | <0.01 |
| Age | 1.02 (0.98–1.04) | 0.30 |
| Sex | 0.59 (0.26–1.35) | 0.21 |
| Time from COVID-19 onset to diagnostic swab | 0.98 (0.89–1.07) | 0.63 |
| Number of comorbidities | 1.01 (0.68–1.48) | 0.97 |
| Worst oxygen support None Low-flow wall oxygen-reservoir CPAP Intubation | – 1.02 (0.37–2.82) 1.27 (0.37–4.38) 1.72 (0.41–7.29) | - 0.97 0.71 0.46 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trunfio, M.; Venuti, F.; Alladio, F.; Longo, B.M.; Burdino, E.; Cerutti, F.; Ghisetti, V.; Bertucci, R.; Picco, C.; Bonora, S.; et al. Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients. Viruses 2021, 13, 281. https://doi.org/10.3390/v13020281
Trunfio M, Venuti F, Alladio F, Longo BM, Burdino E, Cerutti F, Ghisetti V, Bertucci R, Picco C, Bonora S, et al. Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients. Viruses. 2021; 13(2):281. https://doi.org/10.3390/v13020281
Chicago/Turabian StyleTrunfio, Mattia, Francesco Venuti, Francesca Alladio, Bianca Maria Longo, Elisa Burdino, Francesco Cerutti, Valeria Ghisetti, Roberto Bertucci, Carlo Picco, Stefano Bonora, and et al. 2021. "Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients" Viruses 13, no. 2: 281. https://doi.org/10.3390/v13020281
APA StyleTrunfio, M., Venuti, F., Alladio, F., Longo, B. M., Burdino, E., Cerutti, F., Ghisetti, V., Bertucci, R., Picco, C., Bonora, S., Di Perri, G., & Calcagno, A. (2021). Diagnostic SARS-CoV-2 Cycle Threshold Value Predicts Disease Severity, Survival, and Six-Month Sequelae in COVID-19 Symptomatic Patients. Viruses, 13(2), 281. https://doi.org/10.3390/v13020281