Environmental Surveillance for Poliovirus and Other Enteroviruses: Long-Term Experience in Moscow, Russian Federation, 2004–2017

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
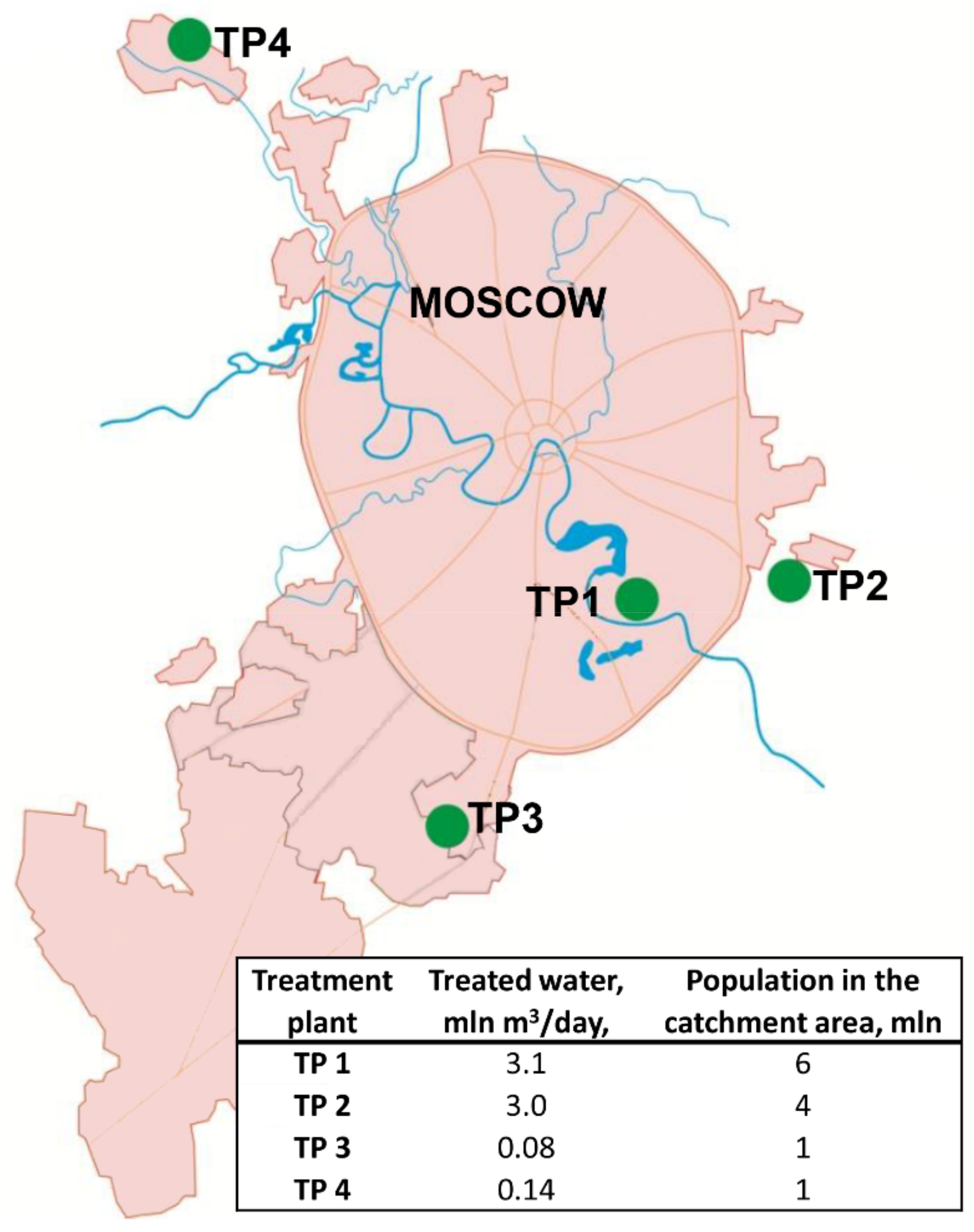
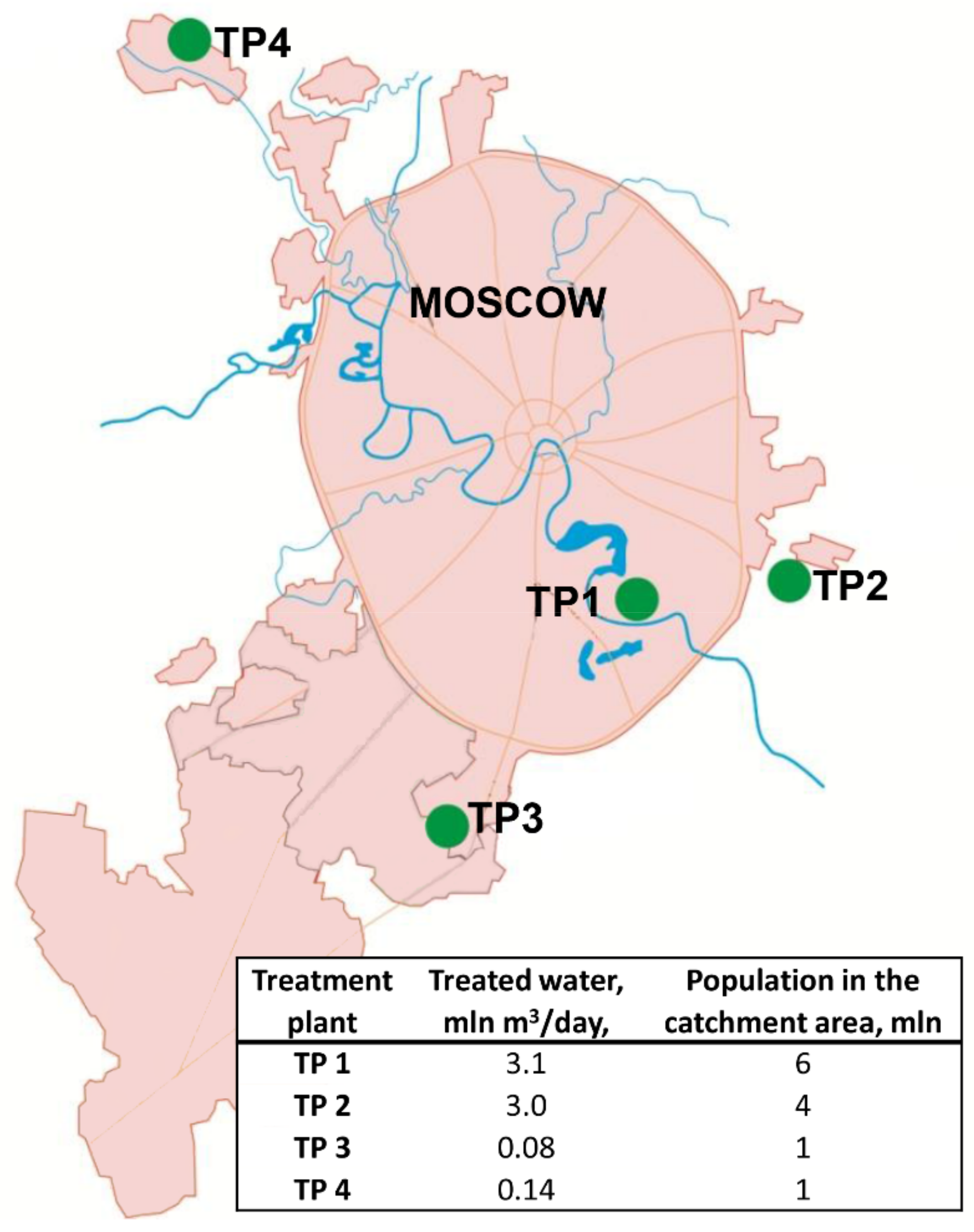
2.1. Sample Collection and Concentration
2.2. Virus Isolation
2.3. Virus Identification and Characterization
2.4. Statistical Methods
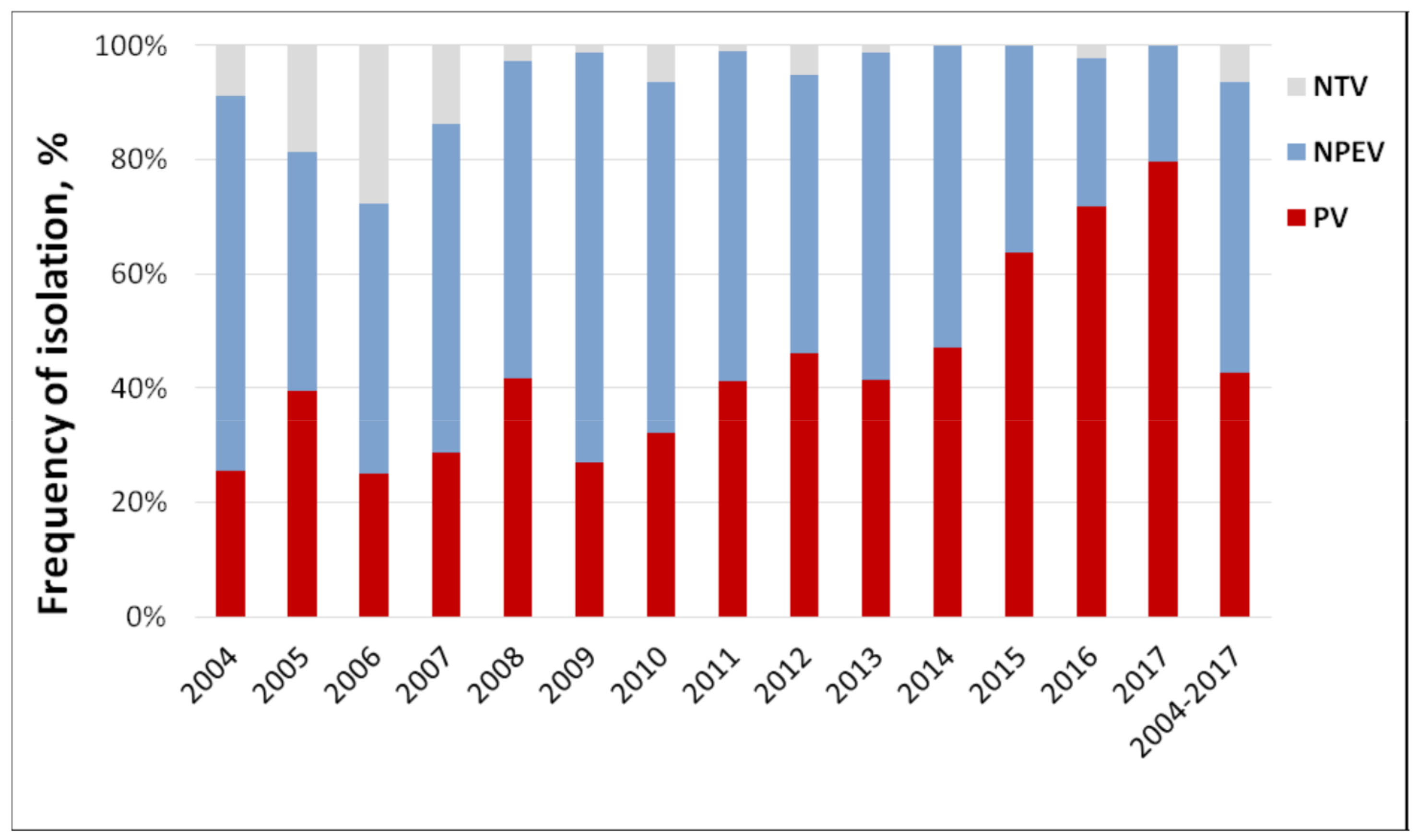
3. Results
4. Discussion
4.1. Sewage Monitoring in Poliovirus Surveillance
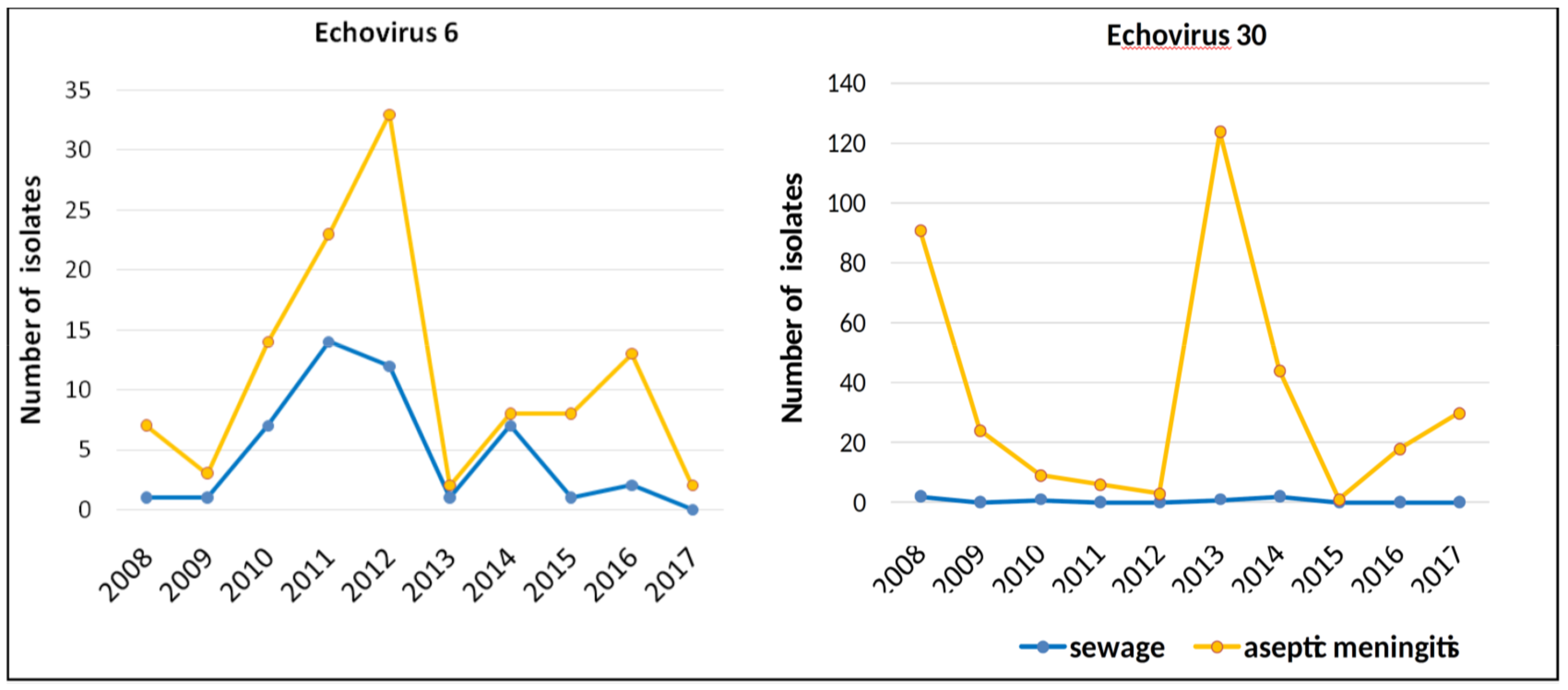
4.2. Sewage Monitoring of Enteroviruses
4.3. Methodology and Technical Efficiency.
4.4. Other Findings
4.5. Cost-Efficiency
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Asghar, H.; Diop, O.M.; Weldegebriel, G.; Malik, F.; Shetty, S.; El Bassioni, L.; Akande, A.O.; Al Maamoun, E.; Zaidi, S.; Adeniji, A.J.; et al. Environmental Surveillance for Polioviruses in the Global Polio Eradication Initiative. J. Infect. Dis. 2014, 210, 294–303. [Google Scholar] [CrossRef]
- Duintjer Tebbens, R.J.; Zimmermann, M.; Pallansch, M.A.; Thompson, K.M. Insights from a Systematic Search for Information on Designs, Costs, and Effectiveness of Poliovirus Environmental Surveillance Systems. Food Environ. Virol. 2017, 9, 361–382. [Google Scholar] [CrossRef]
- Hovi, T.; Shulman, L.M.; van der Avoort, H.; Deshpande, J.; Roivainen, M.; de Gourville, E.M. Role of environmental poliovirus surveillance in global polio eradication and beyond. Epidemiol. Infect. 2012, 140, 1–13. [Google Scholar] [CrossRef]
- Benschop, K.S.M.; van der Avoort, H.G.; Jusic, E.; Vennema, H.; van Binnendijk, R.; Duizer, E. Polio and measles down the drain: Environmental enterovirus surveillance in the Netherlands, 2005 to 2015. Appl. Environ. Microbiol. 2017, 83. [Google Scholar] [CrossRef]
- Blomqvist, S.; El Bassioni, L.; Nasr, E.M.E.M.; Paananen, A.; Kaijalainen, S.; Asghar, H.; De Gourville, E.; Roivainen, M. Detection of Imported Wild Polioviruses and of Vaccine-Derived Polioviruses by Environmental Surveillance in Egypt. Appl. Environ. Microbiol. 2012, 78, 5406–5409. [Google Scholar] [CrossRef] [PubMed]
- Esteves-Jaramillo, A.; Estivariz, C.F.; Peñaranda, S.; Richardson, V.L.; Reyna, J.; Coronel, D.L.; Carrion, V.; Landaverde, J.M.; Wassilak, S.G.F.; Perez-Sanchez, E.E.; et al. Detection of Vaccine-Derived Polioviruses in Mexico Using Environmental Surveillance. J. Infect. Dis. 2014, 210, 210. [Google Scholar] [CrossRef] [PubMed]
- Manor, Y.; Shulman, L.M.; Kaliner, E.; Hindiyeh, M.; Ram, D.; Sofer, D.; Moran-Gilad, J.; Lev, B.; Grotto, I.; Gamzu, R.; et al. Intensified environmental surveillance supporting the response to wild poliovirus type 1 silent circulation in Israel, 2013. Eur. Surveill. 2014, 19, 20708. [Google Scholar] [CrossRef] [PubMed]
- Roivainen, M.; Blomqvist, S.; Al-Hello, H.; Paananen, A.; Delpeyroux, F.; Delpeyreux, F.; Kuusi, M.; Hovi, T. Highly divergent neurovirulent vaccine-derived polioviruses of all three serotypes are recurrently detected in Finnish sewage. Eur. Surveill. 2010, 15, 19566. [Google Scholar]
- Zurbriggen, S.; Tobler, K.; Abril, C.; Diedrich, S.; Ackermann, M.; Pallansch, M.A.; Metzler, A. Isolation of Sabin-Like Polioviruses from Wastewater in a Country Using Inactivated Polio Vaccine. Appl. Environ. Microbiol. 2008, 74, 5608–5614. [Google Scholar] [CrossRef]
- Kaliner, E.; Kopel, E.; Anis, E.; Mendelson, E.; Moran-Gilad, J.; Shulman, L.M.; Singer, S.R.; Manor, Y.; Somekh, E.; Rishpon, S.; et al. The Israeli public health response to wild poliovirus importation. Lancet Infect. Dis. 2015, 15, 1236–1242. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Guidelines for environmental surveillance of poliovirus circulation; WHO/V&B/03.03.WHO: Geneva, Switzerland, 2003; Available online: http://apps.who.int/iris/bitstream/handle/10665/67854/WHO_V-B_03.03_eng.pdf?sequence=1 (accessed on 1 February 2019).
- Federal Service for Surveillance on Consumer Rights Protection and Human Wellbeing (Rospotrebnadzor). Organizing and conducting virological studies of materials from environmental on polioviruses, other (non-polio) enteroviruses, Guidelines 4.2.2357-08; Moscow, Russia, 2008. [Google Scholar]
- World Health Organization (WHO). Manual for the virological investigation of polio, 4th ed.; WHO: Geneva, Switzerland, 2004; Available online: http://whqlibdoc.who.int/hq/2004/WHO_IVB_04.10.pdf (accessed on 1 February 2019).
- Van der Avoort, H.G.A.M.; Hull, B.P.; Hovi, T.; Pallansch, M.A.; Kew, O.M.; Crainic, R.; Wood, D.J.; Mulders, M.N.; van Loon, A.M. A comparative study of five methods of intratypic differentiation of polioviruses. J. Clin. Microbiol. 1995, 33, 2562–2566. [Google Scholar]
- Kilpatrick, D.R.; Yang, C.-F.; Ching, K.; Vincent, A.; Iber, J.; Campagnoli, R.; Mandelbaum, M.; De, L.; Yang, S.-J.; Nix, A.; et al. Rapid Group-, Serotype-, and Vaccine Strain-Specific Identification of Poliovirus Isolates by Real-Time Reverse Transcription-PCR Using Degenerate Primers and Probes Containing Deoxyinosine Residues. J. Clin. Microbiol. 2009, 47, 1939–1941. [Google Scholar] [CrossRef]
- Gerloff, N.; Sun, H.; Mandelbaum, M.; Maher, C.; Nix, W.A.; Zaidi, S.; Shaukat, S.; Seakamela, L.; Nalavade, U.P.; Sharma, D.K.; et al. Diagnostic Assay Development for Poliovirus Eradication. J. Clin. Microbiol. 2018, 56, e01624-17. [Google Scholar] [CrossRef]
- Yakovenko, M.L.; Gmyl, A.P.; Ivanova, O.; Eremeeva, T.P.; Ivanov, A.P.; Prostova, M.A.; Baykova, O.Y.; Isaeva, O.V.; Lipskaya, G.Y.; Shakaryan, A.K.; et al. The 2010 outbreak of poliomyelitis in Tajikistan: Epidemiology and lessons learnt. Eur. Surveill. 2014, 19, 20706. [Google Scholar] [CrossRef]
- Oberste, M.S.; Maher, K.; Kilpatrick, D.R.; Flemister, M.R.; Brown, B.A.; Pallansch, M.A. Typing of Human Enteroviruses by Partial Sequencing of VP1. J. Clin. Microbiol. 1999, 37, 1288–1293. [Google Scholar]
- Gubler, E.V. Computational Methods of Analysis and Recognition of Pathological Processes; Meditsina: Leningrad, Russia, 1978. [Google Scholar]
- Jorba, J.; Campagnoli, R.; De, L.; Kew, O. Calibration of Multiple Poliovirus Molecular Clocks Covering an Extended Evolutionary Range. J. Virol. 2008, 82, 4429–4440. [Google Scholar] [CrossRef]
- Gavrilin, G.V.; Cherkasova, E.A.; Lipskaya, G.Y.; Kew, O.M.; Agol, V.I. Evolution of Circulating Wild Poliovirus and of Vaccine-Derived Poliovirus in an Immunodeficient Patient: A Unifying Model. J. Virol. 2000, 74, 7381–7390. [Google Scholar] [CrossRef] [PubMed]
- Federal Service for Surveillance on Consumer Rights Protection and Human Wellbeing (Rospotrebnadzor). Epidemiological surveillance and prophylaxis of enterovirus (non-polio) infection, Guidelines 3.1.1.2363-08; Moscow, Russia, 2008. [Google Scholar]
- Nathanson, N.; Kew, O.M. From Emergence to Eradication: The Epidemiology of Poliomyelitis Deconstructed. Am. J. Epidemiol. 2010, 172, 1213–1229. [Google Scholar] [CrossRef]
- Kalkowska, D.A.; Duintjer Tebbens, R.J.; Grotto, I.; Shulman, L.M.; Anis, E.; Wassilak, S.G.; Pallansch, M.A.; Thompson, K.M. Modeling options to manage type 1 wild poliovirus imported into Israel in 2013. J. Infect. Dis. 2015, 211, 1800–1812. [Google Scholar] [CrossRef] [PubMed]
- Lukashev, A.N.; Yarmolskaya, M.S.; Shumilina, E.Y.; Sychev, D.A.; Kozlovskaya, L.I. Antibody titers against vaccine and contemporary wild poliovirus type 1 in children immunized with IPV+OPV and young adults immunized with OPV. Virus Res. 2015, 213, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Ivanova, O.; Driss, N.; Tiongco-Recto, M.; Da Silva, R.; Shahmahmoodi, S.; Sazzad, H.M.S.; Mach, O.; Kahn, A.-L.; Sutter, R.W. Poliovirus Excretion Among Persons With Primary Immune Deficiency Disorders: Summary of a Seven-Country Study Series. J. Infect. Dis. 2014, 210, 368–372. [Google Scholar] [CrossRef] [PubMed]
- Aghamohammadi, A.; Abolhassani, H.; Kutukculer, N.; Wassilak, S.G.; Pallansch, M.A.; Kluglein, S.; Quinn, J.; Sutter, R.W.; Wang, X.; Sanal, O.; et al. Patients with primary immunodeficiencies are a reservoir of poliovirus and a risk to polio eradication. Front. Immunol. 2017, 8, 685. [Google Scholar] [CrossRef]
- Blake, I.M.; Pons-Salort, M.; Molodecky, N.A.; Diop, O.M.; Chenoweth, P.; Bandyopadhyay, A.S.; Zaffran, M.; Sutter, R.W.; Grassly, N.C. Type 2 poliovirus detection after global withdrawal of trivalent oral vaccine. New Engl. J. Med. 2018, 379, 834–845. [Google Scholar] [CrossRef] [PubMed]
- Berchenko, Y.; Manor, Y.; Freedman, L.S.; Kaliner, E.; Grotto, I.; Mendelson, E.; Huppert, A. Estimation of polio infection prevalence from environmental surveillance data. Sci. Transl. Med. 2017, 9, eaaf6786. [Google Scholar] [CrossRef]
- Belguith, K.; Hassen, A.; Bouslama, L.; Khira, S.; Aouni, M. Enterovirus circulation in wastewater and behavior of some serotypes during sewage treatment in Monastir, Tunisia. J. Environ. Heal. 2007, 69, 52–56. [Google Scholar]
- Yarmolskaya, M.S.; Shumilina, E.Y.; Ivanova, O.E.; Drexler, J.F.; Lukashev, A.N. Molecular epidemiology of echoviruses 11 and 30 in Russia: Different properties of genotypes within an enterovirus serotype. Infect. Genet. Evol. 2015, 30, 244–248. [Google Scholar] [CrossRef]
- Pennino, F.; Nardone, A.; Montuori, P.; Aurino, S.; Torre, I.; Battistone, A.; Delogu, R.; Buttinelli, G.; Fiore, S.; Amato, C.; et al. Large-scale survey of human enteroviruses in wastewater treatment plants of a metropolitan area of southern Italy. Food Environ. Virol. 2018, 10, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Battistone, A.; Buttinelli, G.; Bonomo, P.; Fiore, S.; Amato, C.; Mercurio, P.; Cicala, A.; Simeoni, J.; Foppa, A.; Triassi, M.; et al. Detection of enteroviruses in influent and effluent flow samples from wastewater treatment plants in Italy. Food Environ. Virol. 2014, 6, 13–22. [Google Scholar] [CrossRef]
- Pogka, V.; Labropoulou, S.; Emmanouil, M.; Voulgari-Kokota, A.; Vernardaki, A.; Georgakopoulou, T.; Mentis, A.F. Laboratory Surveillance of Polio and Other Enteroviruses in High-Risk Populations and Environmental Samples. Appl. Environ. Microbiol. 2017, 83, e02872-16. [Google Scholar] [CrossRef]
- Cesari, C.; E Colucci, M.; Veronesi, L.; Giordano, R.; Paganuzzi, F.; Affanni, P.; Bracchi, M.T.; Capobianco, E.; Ferrari, G.; Tanzi, M.L. Detection of enteroviruses from urban sewage in Parma. Acta Bio-Medica: Atenei Parm. 2010, 81, 40–46. [Google Scholar]
- Mocé-Llivina, L.; Avellón, A.; Jofre, J.; Lucena, F.; Costán-Longares, A.; Moce-Llivina, L.; Costán-Longares, A.; Mocé-Llivina, L. Occurrence and distribution of culturable enteroviruses in wastewater and surface waters of north-eastern Spain. J. Appl. Microbiol. 2008, 105, 1945–1955. [Google Scholar]
- Wieczorek, M.; Ciąćka, A.; Witek, A.; Kuryk, Łukasz; Żuk-Wasek, A. Environmental Surveillance of Non-polio Enteroviruses in Poland, 2011. Food Environ. Virol. 2015, 7, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Harvala, H.; Calvert, J.; Van Nguyen, D.; Clasper, L.; Gadsby, N.; Molyneaux, P.; Templeton, K.; McWilliams Leitch, C.; Simmonds, P. Comparison of diagnostic clinical samples and environmental sampling for enterovirus and parechovirus surveillance in Scotland, 2010 to 2012. Eur. Surveill. 2014, 19. [Google Scholar] [CrossRef]
- Bisseux, M.; Colombet, J.; Mirand, A.; Roque-Afonso, A.-M.; Abravanel, F.; Izopet, J.; Archimbaud, C.; Peigue-Lafeuille, H.; Debroas, D.; Bailly, J.-L.; et al. Monitoring human enteric viruses in wastewater and relevance to infections encountered in the clinical setting: A one-year experiment in central France, 2014 to 2015. Eur. Surveill. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Brinkman, N.E.; Fout, G.S.; Keely, S.P. Retrospective Surveillance of Wastewater To Examine Seasonal Dynamics of Enterovirus Infections. mSphere 2017, 2, 3. [Google Scholar] [CrossRef]
- Majumdar, M.; Sharif, S.; Klapsa, D.; Wilton, T.; Alam, M.M.; Fernandez-Garcia, M.D.; Rehman, L.; Mujtaba, G.; McAllister, G.; Harvala, H.; et al. Environmental Surveillance Reveals Complex Enterovirus Circulation Patterns in Human Populations. Open Forum Infect. Dis. 2018, 5, ofy250. [Google Scholar] [CrossRef]
- Ng, T.F.F.; Marine, R.; Wang, C.; Simmonds, P.; Kapusinszky, B.; Bodhidatta, L.; Oderinde, B.S.; Wommack, K.E.; Delwart, E.; Ng, T.F.F. High Variety of Known and New RNA and DNA Viruses of Diverse Origins in Untreated Sewage. J. Virol. 2012, 86, 12161–12175. [Google Scholar] [CrossRef]
- Victoria, J.G.; Kapoor, A.; Li, L.; Blinkova, O.; Slikas, B.; Wang, C.; Naeem, A.; Zaidi, S.; Delwart, E. Metagenomic Analyses of Viruses in Stool Samples from Children with Acute Flaccid Paralysis. J. Virol. 2009, 83, 4642–4651. [Google Scholar] [CrossRef] [PubMed]
- Furtak, V.; Roivainen, M.; Mirochnichenko, O.; Zagorodnyaya, T.; Laassri, M.; Zaidic, S.Z.; Rehman, L.; Alam, M.M.; Chizhikov, V.; Chumakov, K. Environmental surveillance of viruses by tangential flow filtration and metagenomic reconstruction. Eur. Surveill. 2016, 21, 15. [Google Scholar] [CrossRef]
- Pellegrinelli, L.; Bubba, L.; Primache, V.; Pariani, E.; Battistone, A.; Delogu, R.; Fiore, S.; Binda, S. Surveillance of poliomyelitis in Northern Italy: Results of acute flaccid paralysis surveillance and environmental surveillance, 2012-2015. Hum. Vaccin. Immunother. 2017, 13, 332–338. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| TP | Year | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2004–2017 | |
| 1 | 44/ 159 27.7 | 39/ 195 20.0 | 30/ 146 20.5 | 25/ 153 16.3 | 17/ 147 11.6 | 14/ 143 9.8 | 15/ 132 11.4 | 28/ 136 20.6 | 30/ 154 19.5 | 27/ 139 19.4 | 24/ 133 18.0 | 27/ 109 24.8 | 23/ 254 9.1 | 49/ 153 32.0 | 392/ 2153 18.2 |
| 2 | 16/ 159 10.1 | 28/ 156 17.9 | 17/ 153 11.1 | 23/ 159 14.5 | 16/ 153 10.5 | 21/ 156 13.5 | 36/ 150 24.0 | 19/ 153 12.4 | 29/ 153 19.0 | 30/ 153 19.6 | 18/ 141 12.8 | 18/ 150 12.0 | 12/ 156 7.7 | 27/ 156 17.3 | 310/ 2148 14.4 |
| 3 | 24/ 36 66.7 | 4/ 22 18.2 | 21/ 40 52.5 | 11/ 50 22.0 | 25/ 48 52.1 | 24/ 51 47.1 | 26/ 52 50.0 | 27/ 51 52.9 | 25/ 45 55.6 | 10/ 50 20.0 | 3/ 48 6.3 | 12/ 50 24.0 | 5/ 57 8.8 | 4/ 39 10.3 | 221/ 639 34.6 |
| 4 | 5/ 8 62.5 | 4/ 18 22.2 | 4/ 18 22.2 | 16/ 38 42.1 | 13/ 34 38.2 | 17/ 44 38.6 | 25/ 41 61.0 | 24/ 42 57.1 | 21/ 43 48.8 | 12/ 42 28.6 | 7/ 39 17.9 | 4/ 50 8.0 | 6/ 49 12.2 | 8/ 44 18.2 | 166/ 510 32.5 |
| Total | 89/ 362 24.6 | 75/ 391 19.2 | 72/ 357 20.2 | 75/ 400 18.8 | 71/ 382 18.6 | 76/ 394 19.3 | 102/ 375 27.2 | 98/ 382 25.7 | 105/ 395 26.6 | 79/ 384 20.6 | 52/ 361 14.4 | 61/ 359 17.0 | 46/ 516 8.9 | 88/ 392 22.4 | 1089/ 5450 20.0 |
| Year | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Species | Type | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2004–2017 |
| EV-A n = 28 | CVA3 | 1 | 1 | 1 | 3 | |||||||||||
| CVA7 | 6 | 2 | 4 | 1 | 13 | |||||||||||
| CVA10 | 1 | 1 | 2 | |||||||||||||
| CVA16 | 1 | 4 | 3 | 1 | 1 | 10 | ||||||||||
| EV-B n = 556 | CVB1 | 1 | 1 | 1 | 3 | |||||||||||
| CVB2 | 1 | 1 | ||||||||||||||
| CVB3 | 2 | 2 | 2 | 8 | 3 | 2 | 19 | |||||||||
| CVB4 | 1 | 3 | 1 | 2 | 1 | 2 | 1 | 5 | 16 | |||||||
| CVB5 | 2 | 2 | 1 | 9 | 5 | 1 | 3 | 2 | 25 | |||||||
| CVB6 | 1 | 1 | 2 | |||||||||||||
| E1 | 1 | 1 | 2 | |||||||||||||
| E2 | 1 | 1 | ||||||||||||||
| E3 | 20 | 5 | 3 | 3 | 3 | 3 | 3 | 2 | 42 | |||||||
| E4 | 2 | 3 | 1 | 1 | 7 | |||||||||||
| E6 | 8 | 3 | 9 | 4 | 1 | 1 | 7 | 14 | 12 | 1 | 7 | 1 | 2 | 70 | ||
| E7 | 13 | 12 | 10 | 20 | 5 | 23 | 21 | 9 | 11 | 11 | 2 | 9 | 4 | 3 | 153 | |
| E11 | 9 | 3 | 5 | 3 | 17 | 9 | 9 | 12 | 9 | 16 | 8 | 6 | 2 | 5 | 113 | |
| E12 | 1 | 1 | 2 | 5 | 1 | 1 | 2 | 13 | ||||||||
| E13 | 1 | 1 | 1 | 1 | 1 | 1 | 6 | |||||||||
| E14 | 1 | 1 | 1 | 3 | ||||||||||||
| E17 | 1 | 3 | 4 | |||||||||||||
| E19 | 5 | 5 | 9 | 2 | 3 | 1 | 25 | |||||||||
| E20 | 1 | 1 | 1 | 1 | 4 | 8 | ||||||||||
| E25 | 2 | 1 | 3 | 5 | 3 | 1 | 1 | 16 | ||||||||
| E29 | 2 | 1 | 2 | 2 | 1 | 2 | 4 | 14 | ||||||||
| E30 | 1 | 1 | 2 | 2 | 1 | 1 | 2 | 10 | ||||||||
| E33 | 1 | 1 | 2 | |||||||||||||
| EV31 | 1 | 1 | ||||||||||||||
| EV-C n = 11 | CVA17 | 1 | 1 | 2 | ||||||||||||
| CVA21 | 1 | 1 | ||||||||||||||
| CVA24 | 1 | 1 | 3 | 3 | 8 | |||||||||||
| Total | 2004–2017 | 59 | 34 | 36 | 46 | 43 | 56 | 67 | 65 | 57 | 47 | 28 | 25 | 12 | 20 | 595 |
| Patient-Based | Environmental | |
|---|---|---|
| Cost per sample | About equal. Higher material costs of sewage sampling are balanced by indirect costs of AFP reporting. | |
| Isolation efficiency per sample tested | 3%: 8 polio isolates from 250 AFP cases screened | 9%: 499 isolates from 5450 samples tested in 2004–2017 |
| Isolation efficiency per population | 0.05 isolates/million persons/year | 3 isolates/million persons/year |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ivanova, O.E.; Yarmolskaya, M.S.; Eremeeva, T.P.; Babkina, G.M.; Baykova, O.Y.; Akhmadishina, L.V.; Krasota, A.Y.; Kozlovskaya, L.I.; Lukashev, A.N. Environmental Surveillance for Poliovirus and Other Enteroviruses: Long-Term Experience in Moscow, Russian Federation, 2004–2017. Viruses 2019, 11, 424. https://doi.org/10.3390/v11050424
Ivanova OE, Yarmolskaya MS, Eremeeva TP, Babkina GM, Baykova OY, Akhmadishina LV, Krasota AY, Kozlovskaya LI, Lukashev AN. Environmental Surveillance for Poliovirus and Other Enteroviruses: Long-Term Experience in Moscow, Russian Federation, 2004–2017. Viruses. 2019; 11(5):424. https://doi.org/10.3390/v11050424
Chicago/Turabian StyleIvanova, Olga E., Maria S. Yarmolskaya, Tatiana P. Eremeeva, Galina M. Babkina, Olga Y. Baykova, Lyudmila V. Akhmadishina, Alexandr Y. Krasota, Liubov I. Kozlovskaya, and Alexander N. Lukashev. 2019. "Environmental Surveillance for Poliovirus and Other Enteroviruses: Long-Term Experience in Moscow, Russian Federation, 2004–2017" Viruses 11, no. 5: 424. https://doi.org/10.3390/v11050424
APA StyleIvanova, O. E., Yarmolskaya, M. S., Eremeeva, T. P., Babkina, G. M., Baykova, O. Y., Akhmadishina, L. V., Krasota, A. Y., Kozlovskaya, L. I., & Lukashev, A. N. (2019). Environmental Surveillance for Poliovirus and Other Enteroviruses: Long-Term Experience in Moscow, Russian Federation, 2004–2017. Viruses, 11(5), 424. https://doi.org/10.3390/v11050424