1. Introduction
In recent years, the success of deep learning models across a wide range of application domains has spurred the creation of numerous large datasets. However, these datasets often exhibit various forms of bias [
1], which can broadly be categorized as operational or systemic. Operational biases stem from factors like the instruments used for data collection, the labeling strategies, and the definition of different data classes [
2]. On the other hand, systemic biases in AI can be attributed to data collection that inadvertently reinforces societal prejudices, including those related to sexism, racism, and ageism. To address these issues, the field of fairness [
3] and ethical artificial intelligence (AI) [
4] approaches are becoming mainstream, aiming to mitigate some of the biases persisting in datasets. The general idea in many of these approaches is to learn a ‘sensitive attribute’ agnostic representation that can be generalized to the rest of the data [
5]. While many of these approaches are designed as classification problems, dealing with binary or multi-class scenarios like sex or ethnicity, they often overlook the consideration of numerical attributes, particularly in the context of age, when developing fair AI models.
In the context of skin lesion detection, addressing age-related bias and digital ageism is critical [
3,
6,
7] in developing fair AI models. Unfair models with respect to age could result in multiple issues. One major issue is the difficulty in collecting sufficient data from older adults, which limits the model’s ability to generalize across different age groups. Chu et al. [
8] describe the presence of sampling bias in several databases containing very few data from older people. The other crucial aspect is the misrepresentation of age as a category, the reinforcement of stereotypes, a lack of awareness, and the neglect of the older population. These factors, in most cases, lead to the predominance of training data from younger people [
9]. In a health-sensitive application, such as skin lesion detection, this systemic data imbalance could lead to algorithms that are less sensitive to the nuances of skin lesions in older demographics, potentially resulting in higher misdiagnosis rates. Another significant issue is the deployment of medical devices using unfair AI algorithms. As an example, if a medical treatment requires the use of a digital device (i.e., a mobile phone, web services) and the digital literacy and education of older adults is not considered, such devices risk producing discriminatory results regarding older people and may have negative impacts on their health [
10].
For skin lesion detection problems, it appears that older people who are more exposed to sunlight may have a higher likelihood of developing skin cancer [
11]. However, an important question is whether the publicly available datasets on skin lesions contain equal or larger numbers of older people in their cohorts. To test this, we plotted the age distributions of the PAD20 [
12] and ISIC2019 [
13] datasets (more details are given in
Section 3.5).
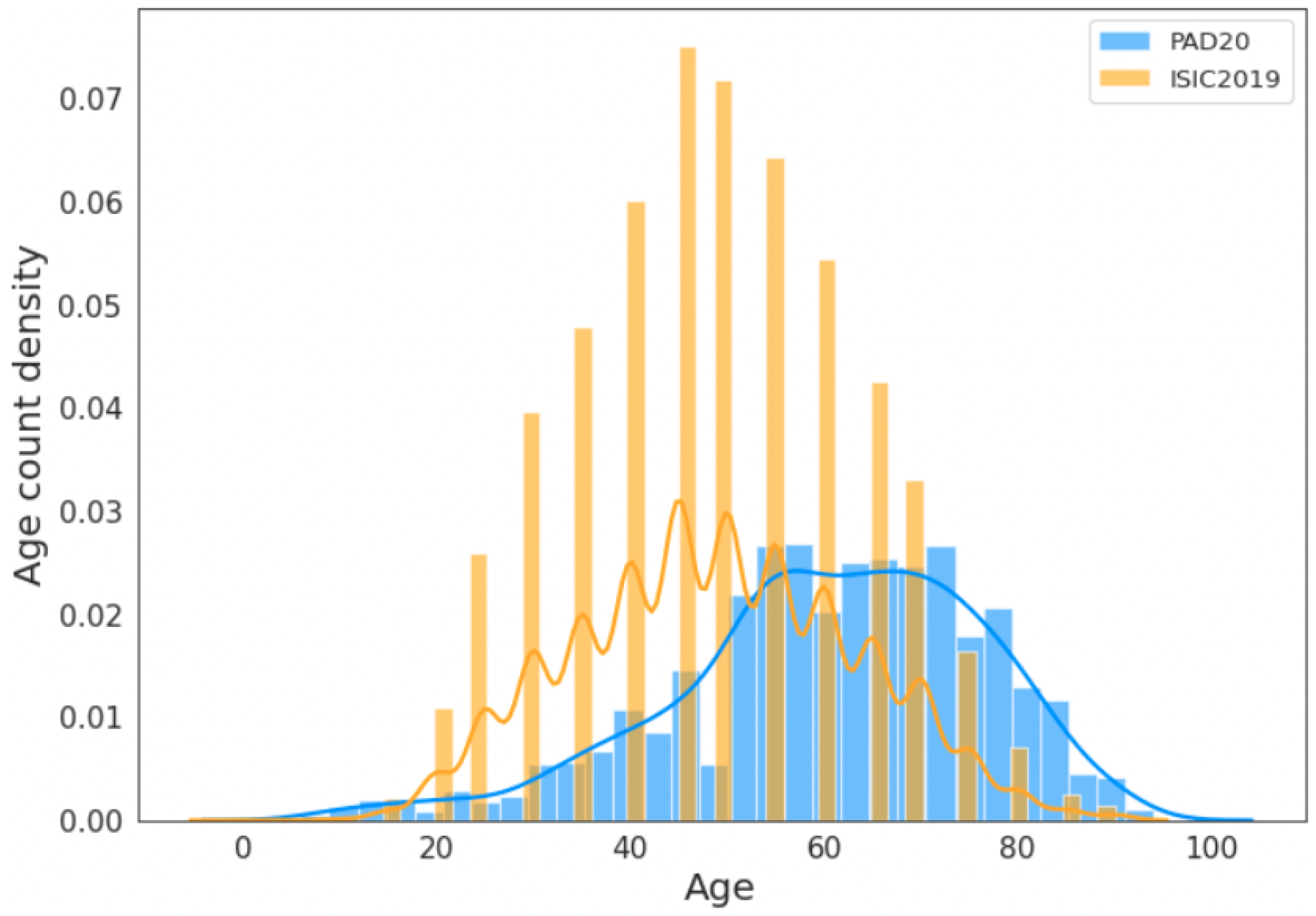
Figure 1 shows the combined age distribution in the ISIC2019 and PAD20 datasets. It can be seen that the representation of older adult people (more than 65 years) is small. In the PAD20 dataset, the age distribution of people above 80 is very small. Therefore, it is not clear if the skewed age distribution in these datasets reflects the prevalence of skin lesions in the older population. This could potentially lead to age-biased AI models. Furthermore, it is not clear whether the models trained on these datasets, predominately comprising younger people, generalize well to older people.
Adversarial learning is one of the most commonly used techniques to mitigate general biases, and it can achieve fair and transferable performance [
14]. In this setting, an adversarial network can be employed as an encoder before or after the classifier to learn a fair latent representation for sensitive attributes [
14,
15,
16]. While effective for tabular data, this approach is not well suited to handle image inputs. On the other hand, an adversarial network can also be appended to the end of an encoder or classifier to forecast protected or sensitive attributes (e.g., age, sex), creating a minimax game (see
Section 3.5). This game aims to maximize the network’s performance in predicting the class label, while simultaneously minimizing the ability of the adversarial network to predict the sensitive attributes [
15,
16]. However, if a model is required to ignore features pertaining to a protected attribute, this may have a negative impact on its classification accuracy, as those features could potentially contain vital information necessary for accurate predictions. Furthermore, most related works consider sex, gender, or race as the selected (binary) sensitive attribute [
14,
17]. These models are limited in their ability to handle continuous sensitive variables, such as age, which cannot be arbitrarily divided into categories as there is a lack of consistency in the labeling of age groups [
18]. Manually binning data into age groups can also introduce human biases and inconsistent categorization [
19]; thus, previous approaches are not suitable for this problem. Age as a continuous attribute could be incorporated into an adversarial loss function for bias mitigation purposes (e.g., BR-Net [
20], AMAT-Net [
21]); these are based on Pearson and/or cosine correlations between the true and predicted values of a protected variable. Furthermore, it is challenging to directly use the previous fairness criteria for continuous attributes (e.g., age). Therefore, alternative approaches are required to address fairness concerns related to continuous attributes.
In this paper, we present a new method, called Mitigating Digital Ageism using Adversarially Learned Representation (MA-ADReL), to handle a continuous sensitive attribute in an adversarial learning setting for the mitigation of age-related bias in skin lesion problems. We introduce a mutual information penalty term that can mitigate bias for sensitive continuous attributes to improve the fairness while maintaining the accuracy. To further improve the performance, we utilize the information fusion of both low- and high-resolution inputs for medical image encoding in order to learn a more transferable latent representation. Various experiments on two skin lesion datasets demonstrate the consistent effectiveness of our method in mitigating bias and achieving comparable performance.
2. Related Work
Several studies have focused on mitigating bias in training their predictive models. From a dataset perspective, a commonly used method is data augmentation. Georgopoulos et al. [
22] used a generative adversarial network (GAN) that included a style-based generator and discriminator. Images were categorized into four age groups, and the GAN was employed to produce digitally aged images to balance the training dataset among each group. In another study, Smith and Ricanek [
23] utilized two augmentation methods, random Gaussian tinting and random cropping, to expand their training dataset for a deep neural network model. However, the effectiveness of data augmentation in mitigating bias is impacted by the quality and diversity of the original data augmentation techniques employed; it could also lead to overfitting problems.
From a model learning perspective, bias mitigation methods usually involve modifying the training loss function to regularize the model for fairness. Corral et al. [
24] added a task-specific prior to implicitly regularize the model to not pay attention to the sensitive attribute-related information for its prediction. Adversarial training has been applied in several works ([
20,
25,
26]) to achieve fairness by removing sensitive information with an adversarial learner or calculating correlations between actual and predicted protected variables. Bevan and Amir [
27] proposed a method for the mitigation of skin tone bias in skin lesion classification. They first detected the skin tones of the lesion images and then debiased the feature representations to reduce the impact of the skin tone on the final prediction. However, it addressed bias related to skin tone and did not consider age-related bias. In this paper, we present a new adversarial method that accounts for age as a continuous attribute and reduces the bias while maintaining the classification performance.
3. Methods
3.1. Fair Skin Lesion Detection
Consider a medical image with metadata consisting of tuples in , , where is the input skin lesion image, denotes the metadata, is the class label from the set X, Y, and A, and a pretrained encoder yields the representations Z. Each is a high-resolution image represented as a 3-dimensional matrix of dimensions , where W, H, and C are the width, height, and the number of color channels (typically C = 3 for RGB images). The metadata consist of vectors of real-valued attributes associated with each image. They are represented as , where M is the number of metadata attributes, such as age, gender, weight, and height. The class label is a binary indicator representing the diagnosis of a skin lesion in the image . It takes values from the set A 0,1, where 0 corresponds to ‘benign’ and 1 to ‘malignant’. The classifier learns to predict based on the representation Z from the input image. In the context of mitigating age-related bias in skin lesion detection, the encoder , decoder , and classifier work together to minimize both the classification loss and the reconstruction error, while also minimizing the objective of the adversary .
In the adversarial framework, we establish a competitive yet collaborative environment between the classifier and the adversary. The classifier aims to maximize its predictive accuracy to detect skin lesions, while the adversary strives to minimize the classifier’s ability to discern sensitive attributes, such as age, from the latent representation. This dynamic creates a minimax game, where the objective is to find a balance where the classifier performs well on the primary task without relying on sensitive attributes that the adversary is trying to ‘protect’ from being predictive. However, there are several operational challenges when working with adversarial networks that should be proactively considered, including vanishing gradients, mode collapse, and convergence problems [
28]. Furthermore, data poisoning and other malicious data injections can severely undermine the predictive abilities of adversarial networks [
29].
Unlike Madras et al. [
14], in our problem, input
is not a tabular dataset [
30] but skin lesion images with metadata. Moreover, our sensitive attribute is age, which is a continuous variable rather than a discrete variable (e.g., ethnicity, sex, or gender). We aim to maximize the prediction performance while minimizing the bias against sensitive attributes:
In this equation, represents the encoder that extracts features from the input images , g is the classifier that predicts the class labels , and is an optional decoder that may reconstruct the images from the latent features. The adversary h attempts to predict the sensitive attribute (such as age) from the features to ensure fairness. The expectation is taken over the input images X, labels Y, and sensitive attributes A, while is the loss function that balances both prediction accuracy and fairness.
Our objective function is expressed as
The classification loss
ensures accurate classification; the
reconstruction loss enhances the accuracy of data reconstruction by the deep variational autoencoder (VAE), promoting meaningful representation learning and improving the data quality. The adversarial loss
promotes fairness. The hyperparameters
,
, and
are used to control the trade-off in the performance of the model in detecting skin lesions, reconstructing the input images, and achieving fairness in the prediction results, respectively. In the following section, we investigate different
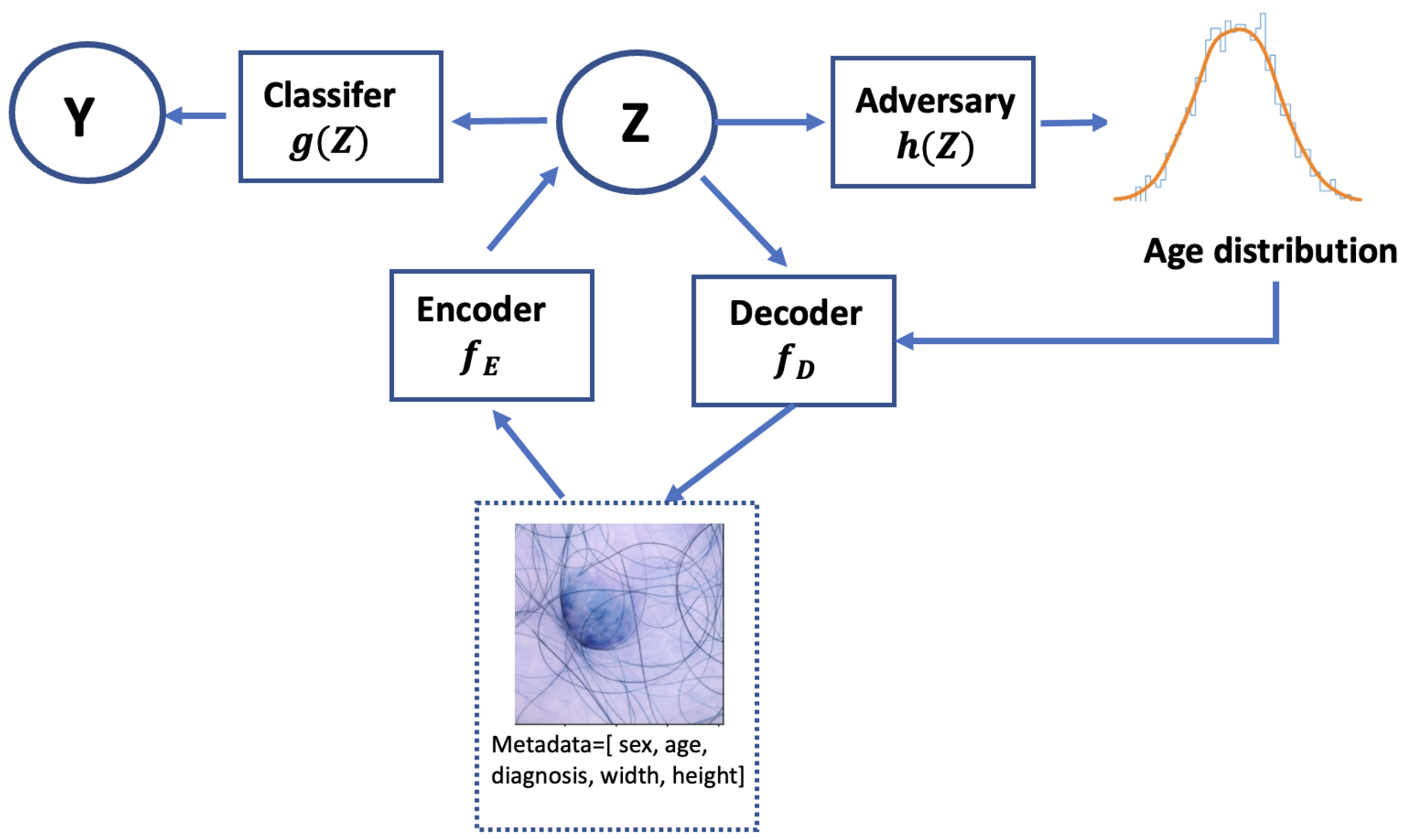
values to balance model performance and fairness. The overall framework is shown in
Figure 2. Following the framework from [
13], the metadata undergo processing through two fully connected layers before being combined with the CNN features from the skin lesion image. Training with the adversary, we then input the latent representations
Z into the classifier.
3.2. Fairness Criteria Definitions
In the context of skin lesion detection, the fairness criteria proposed by Madras et al. [
14] are as follows.
Demographic Parity: This criterion ensures that the probability of positive predictions is approximately equal across different sensitive attribute groups. In other words, the model should not favor one group over another. The difference in the true positive rates for the sensitive (
) and non-sensitive (
) groups should be within a specified bound
. This can be formulated as follows:
where
is the predicted class label,
A is the sensitive attribute (e.g., race, gender), and
is the maximum allowed difference.
Equalized Odds: This criterion ensures that the probability of false positives and true positives is similar across the sensitive and non-sensitive groups. The idea is to ensure that the model’s error rates (false positives or negatives) are evenly distributed across the groups. The difference in the false positive rates for the sensitive and non-sensitive groups should be within a certain bound. This can be formulated as follows:
where
Y is the true class label (e.g.,
indicates a benign lesion,
indicates a malignant lesion).
is the predicted class label (e.g.,
is a prediction of malignancy).
A represents the sensitive attribute (e.g., gender, where
might represent male and
female).
again represents the acceptable difference between the false positive rates, ensuring equalized odds across groups.
The fairness criteria defined in Equations (
3) and (
4) are straightforward to integrate for gender or racial bias mitigation by labeling them in discrete categories. However, dealing with continuously protected attributes, such as age, can be more challenging than with categorical attributes, because the fairness constraint needs to be defined over a continuous range of values. Manually classifying a continuous age distribution into different groups will also induce bias [
1].
3.3. Protecting Continuous Sensitive Attributes with Mutual Information Penalty
To address bias related to continuous sensitive attributes such as age, we propose incorporating a mutual information loss term in the objective function of the learning algorithm. The core idea is that, by minimizing the mutual information between the sensitive attribute (age) and the latent representation, we can reduce the model’s dependence on age when making predictions. This ensures that the model focuses more on relevant skin lesion features rather than age, thus mitigating the impact of age-related bias in skin lesion detection. Given the input features, which include the skin image and metadata
X, the target label
Y, and the continuous sensitive attribute
A (in this case, age), we can calculate the mutual information between
X and
A as
where
is the entropy of
X and
is the conditional entropy of
X given
A. To mitigate the bias, we wish to minimize the mutual information between
A and the hidden representation
Z, while preserving the mutual information between
X and
Z,
Y, and
Z. This can be formulated as the following optimization problem:
where
is the mutual information between the latent representation
Z and the sensitive attribute
A. Minimizing this term helps to reduce age bias.
is the mutual information between the latent representation
Z and the input
X. This term should be maintained above a certain threshold
, ensuring that the representation
Z retains enough information from the input
X for accurate classification.
is the mutual information between the latent representation
Z and the target label
Y, and it should also be above a threshold
to ensure that
Z contains enough information to make correct predictions.
and
are constants that define the minimum acceptable levels of mutual information, balancing the model’s ability to use the input and target label information.
As a result, we can formulate the adversarial loss term; this is achieved by minimizing the following objective function:
where
and
are hyperparameters that balance the trade-off between the classification and reconstruction accuracy and the fairness of the model from the level of mutual information. Finally, we can integrate Equation (
7) into Equation (
2).
3.4. Training Deep VAE Model for Fairness
Previous works aimed at learning fair representations via adversarial learning primarily focused on tabular data [
14,
31] or low-resolution images [
25,
32]. However, when dealing with high-resolution medical images, such as those used in skin lesion detection, directly applying traditional variational autoencoders (VAE) can introduce several challenges. First, high-resolution images typically contain a large amount of pixel-level detail, resulting in a high-dimensional input space. Training a model on such data can become computationally expensive and difficult due to the increased complexity and dimensionality of the input [
33]. Second, traditional VAE architectures often struggle to capture the fine-grained details that are critical for the accurate classification and diagnosis of skin lesions. The loss of this crucial information during encoding can negatively impact the model’s performance, leading to suboptimal predictions. Therefore, specialized architectures and techniques are required to effectively encode high-resolution medical images in a way that preserves essential details while ensuring fairness in the model’s predictions. To address these issues, we propose using a deep hierarchical VAE architecture. A deep hierarchical VAE is capable of learning more complex and structured representations of the data by encoding the input at multiple levels of abstraction. This allows the model to capture both coarse- and fine-grained details of the image by progressively refining the latent representation across different layers. By encoding at multiple abstraction levels, the VAE can generate data at different levels of detail by sampling from different layers of the latent representation [
33]. This hierarchical structure is particularly beneficial for high-resolution medical images, as it allows for the effective capture of both global and local image features. The Very Deep VAE (VDVAE) uses the hierarchical factorization of the prior and approximate posterior distributions, where
K stochastic layers are employed to progressively capture more complex information from the input data. The factorization of the prior distribution
and the approximate posterior distribution
for a model with
K layers are expressed as follows:
where
is the prior distribution for the latent variable at the first layer, and
is the conditional prior for each subsequent latent variable, conditioned on the latent variables from previous layers.
K represents the total number of stochastic layers in the model, with each layer refining the latent representation learned by the model.
represents all latent variables from the layers before layer
K, capturing hierarchical information.
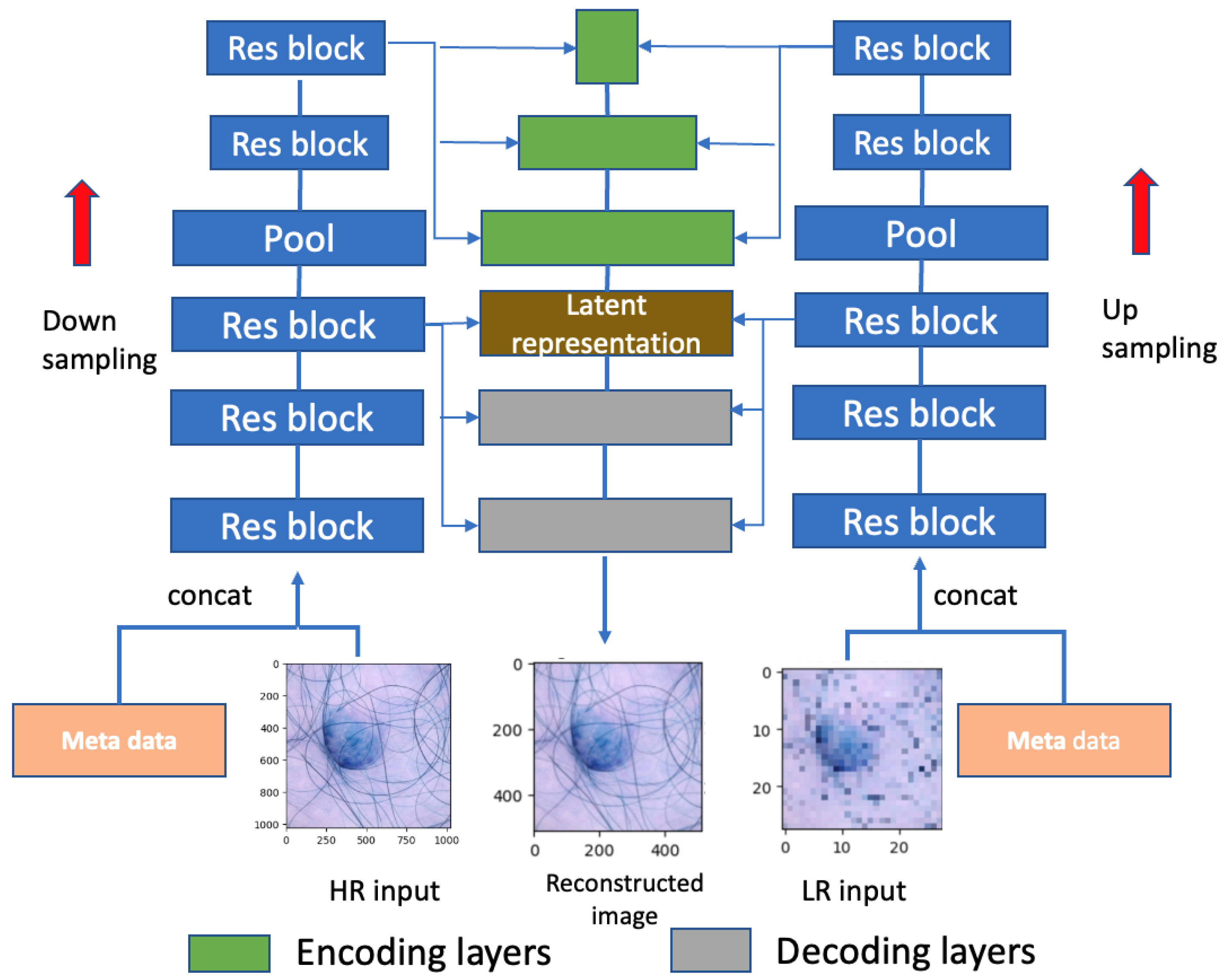
As depicted in
Figure 3, the model comprises both a high-resolution (HR) branch, with dimensions
, and a low-resolution (LR) branch, with dimensions
. The pooling layer is employed for the downsampling of the HR input and upsampling of the LR input. The distribution
is modeled as a diagonal Gaussian,
is sampled from
, and the group of latent variables
is positioned at the top layer, featuring a smaller number of variables for the low-resolution input. Conversely,
resides at the bottom of the network, encompassing a greater number of latent variables for the high-resolution input. This hierarchical arrangement offers enhanced flexibility in capturing intricate relationships between the input and the latent variables.
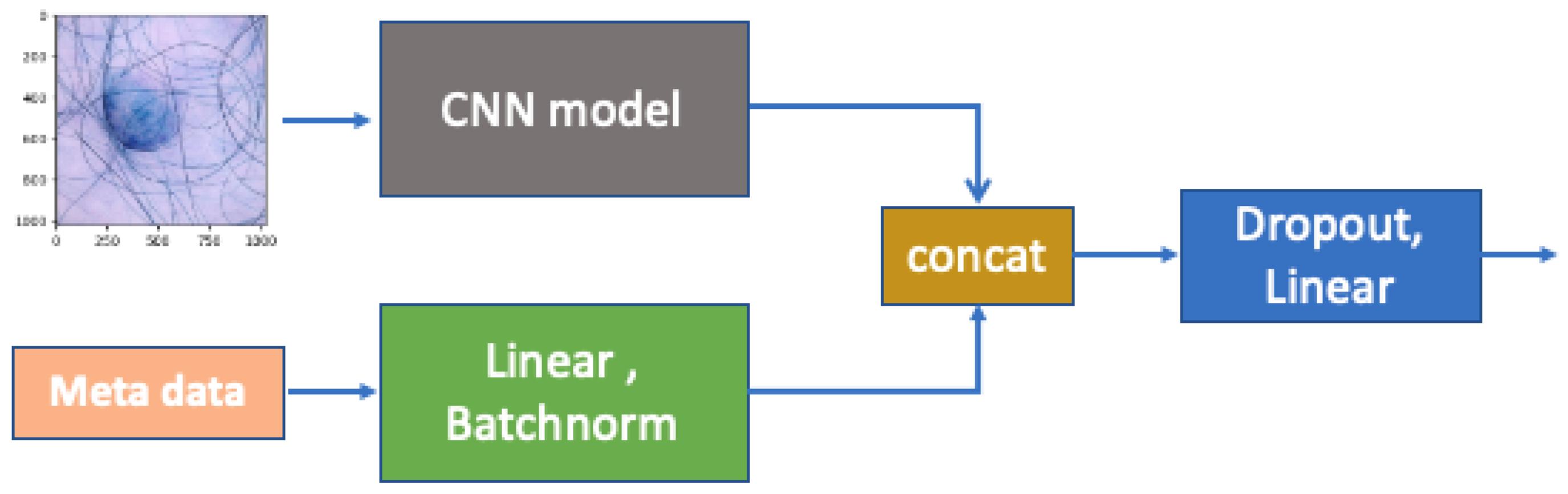
To be more specific, as shown in
Figure 4, we follow a similar procedure to that proposed by [
13] to conduct information fusion for the image and metadata. After passing through the fully connected layers, the metadata are combined with the CNN features extracted from the raw images through concatenation and then forwarded to the final fully connected layer. The CNN model has a 7 × 7 kernel with stride 2 for broad feature extraction, followed by 3 × 3 residual blocks with 64, 128, and 256 filters; global average pooling; and a 128-neuron fully connected layer. Batch normalization ensures stable and efficient training, with outputs via softmax for binary classification. To train our model, we used 5-fold cross-validation to select the optimal subsets of models based on the cross-validation performance. We tuned different parameters of
, as shown in Equation (
2), to achieve the best outcomes in balancing the prediction performance and fairness.
3.5. Datasets
We implement our framework on the ISIC2019 challenge’s Skin Lesion Classification dataset [
34], which is a compilation of skin lesion images utilized for the identification and categorization of melanoma. The dataset comprises 33,126 images with dimensions of
pixels, with binary labels indicating whether each lesion is benign (0) or malignant (1). Additional metadata are also provided with other information, including the approximate ages of the participants. We performed 5-fold cross-validation on the dataset and report the mean and standard deviation. To demonstrate the transferability of MA-ADRel, we also used the PAD20 dataset for testing [
35], which contains dermatoscopic images of skin lesions collected from a public health center in Brazil using smartphones. It contains 2298 images with various metadata, including age.
3.6. Dataset Exploration
First, we analyzed the age distribution of the images within these datasets.
Figure 1 shows that the age distributions in these two datasets follow normal distributions. The blue curve represents the distribution of PAD20, while the yellow curve represents the distribution of ISIC2019. The median age from the ISIC2019 dataset is 43 years old, while the median age from PAD20 is 63 years old. It appears that ISIC2019 comprises a greater number of middle-aged adults, whereas PAD20 has a larger sample of older adults.
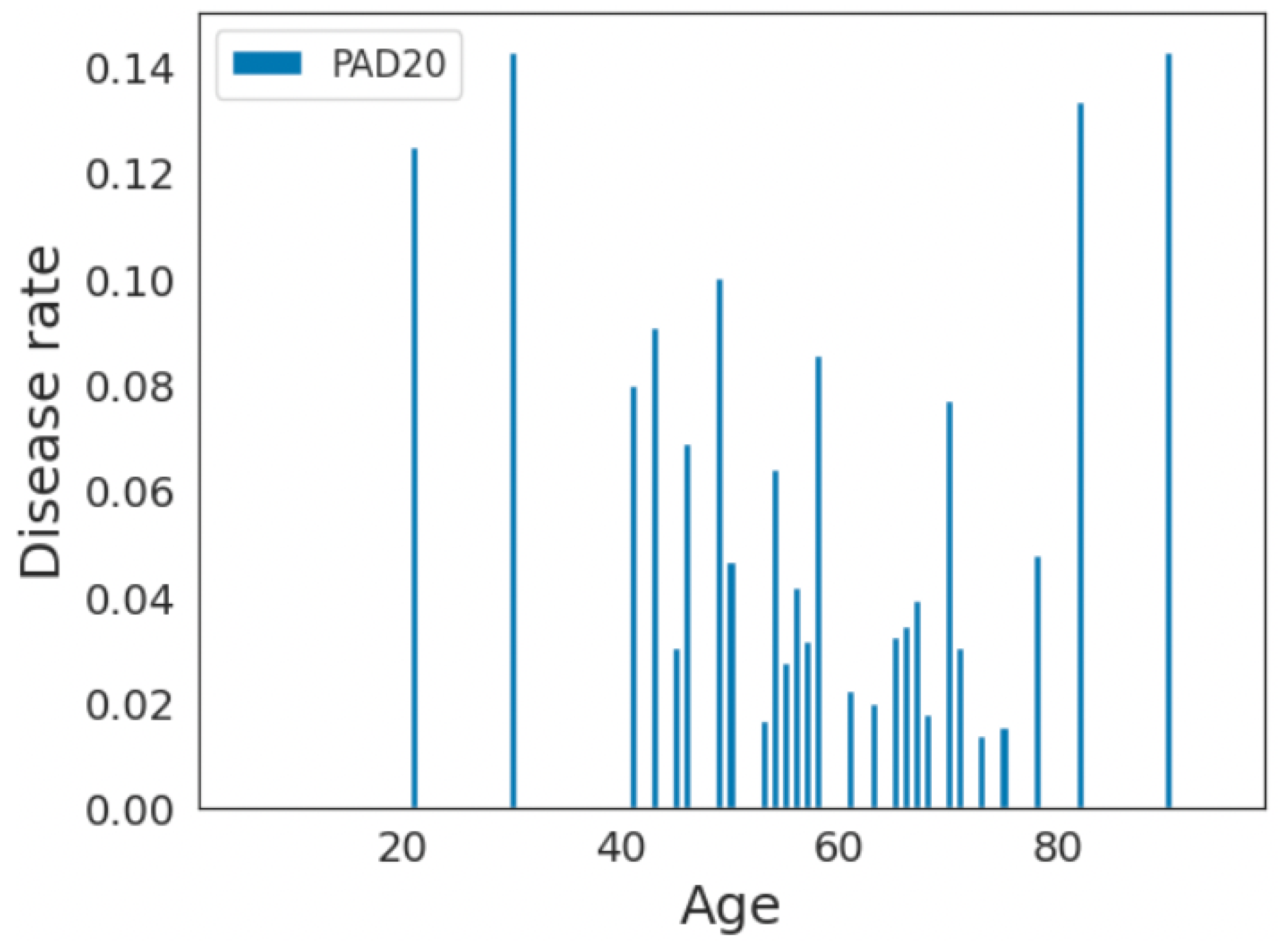
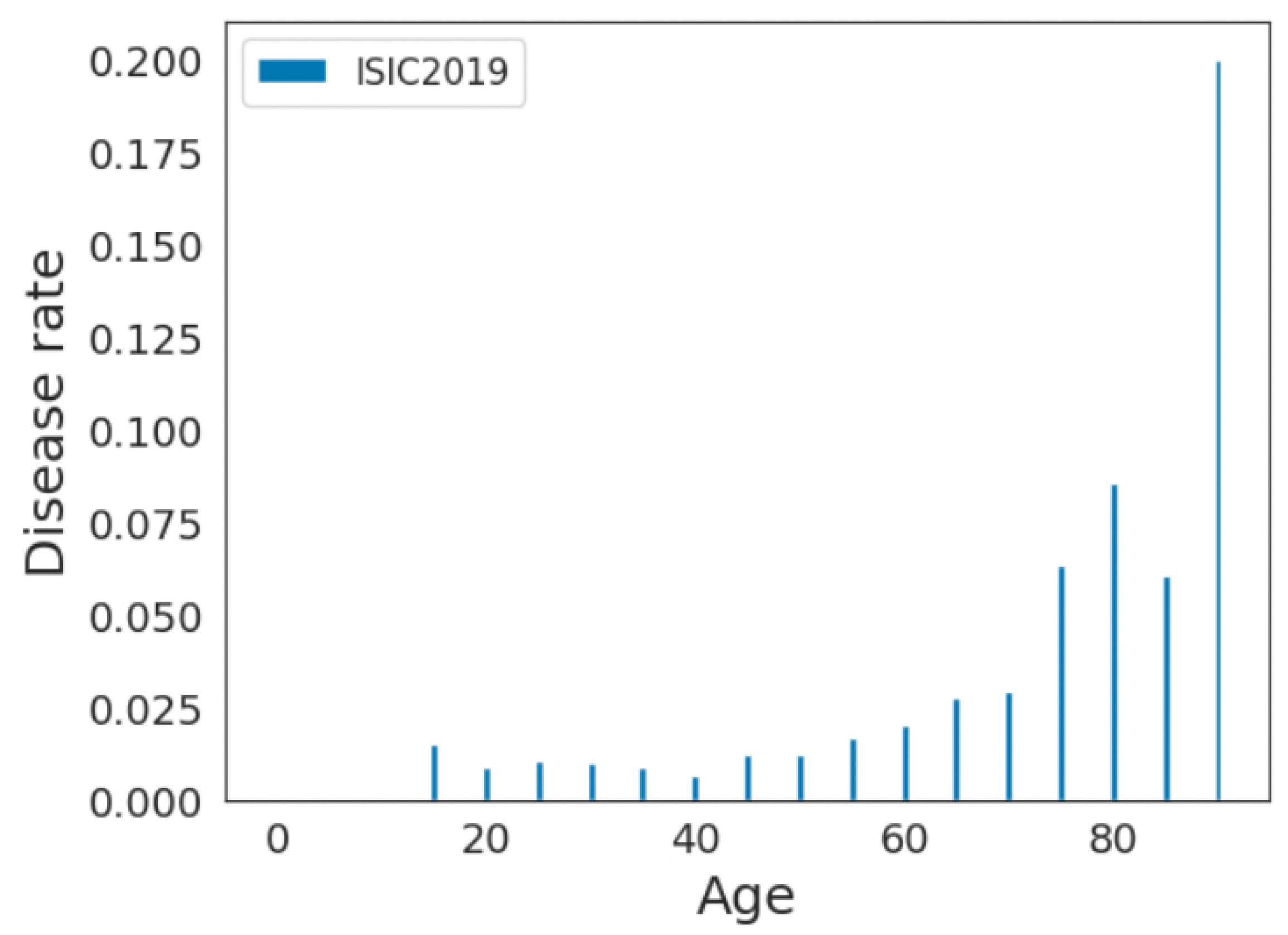
Furthermore, we analyzed the disease rate among each age group. Consider
n as the total number of individuals in the age group, and consider
d as the number of individuals in the age group who have the disease. We define the disease rate for the age group as
For example, if there are 100 individuals in the age group and 10 of them have the disease, the disease rate would be
. We plotted the disease rate among each age sample for these datasets. As shown in
Figure 5 and
Figure 6, the disease rate is not equally distributed within each dataset. For the ISIC2019 dataset, older adults have higher disease rates, whereas they are less represented in the data. For the PAD20 dataset, middle-aged adults have higher disease rates and there is better representation of older adults. Therefore, the distributions of the age and disease rates are not consistent in these datasets; as a result, age-related biases may be introduced when developing predictive models.
As pointed out by Mehrabi et al. [
1], different data collection protocols can induce measurement biases. According to Wu et al. [
17], the target prediction in skin lesion diagnosis should not depend on sensitive attributes, such as age. Furthermore, the training data should not be biased in terms of the disease samples per age category. As demonstrated in
Figure 6 and Table 3, age-related bias exists in these two datasets. As a result, the investigation of bias mitigation strategies for the continuous sensitive attribute is necessary before developing predictive models.
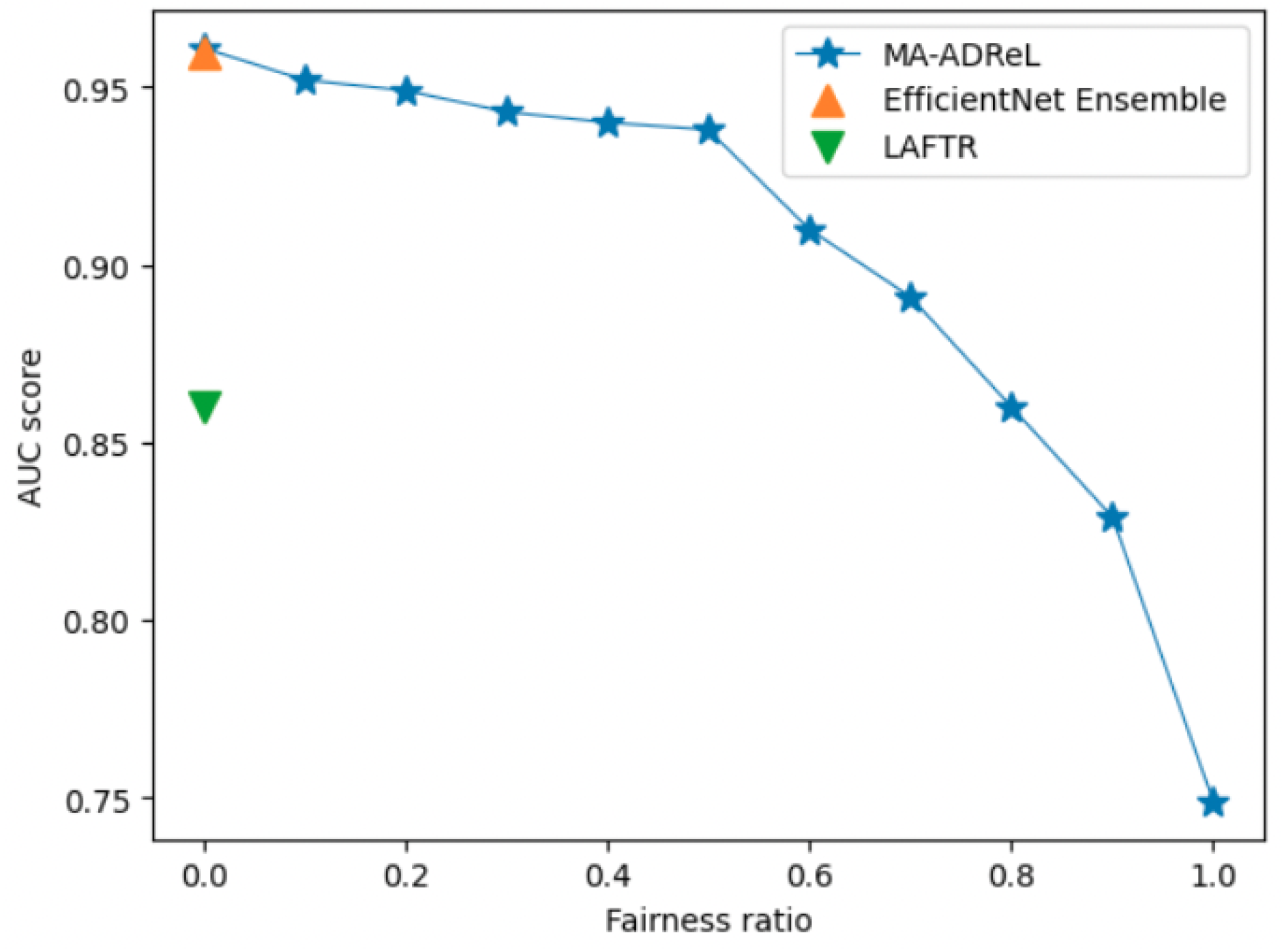
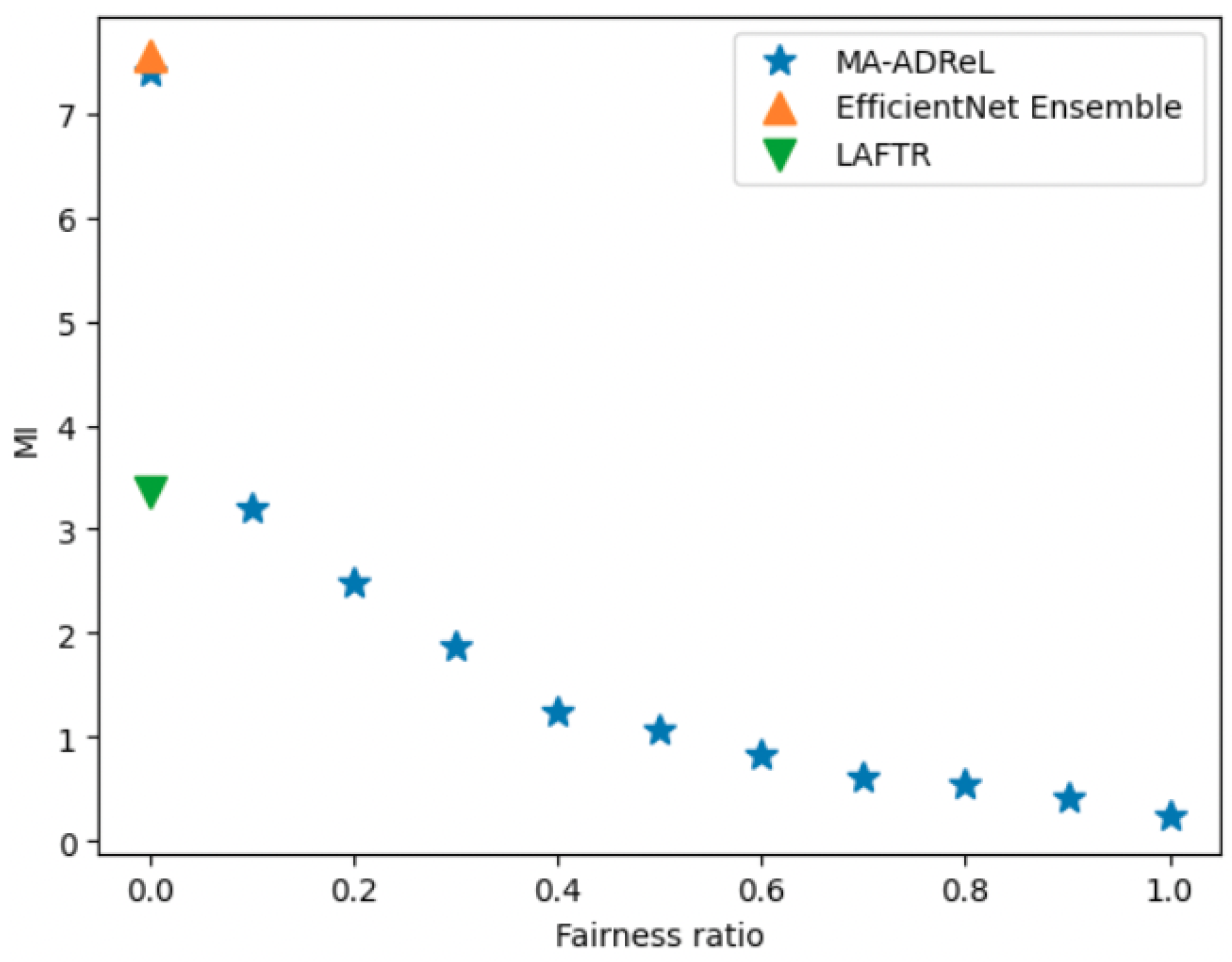
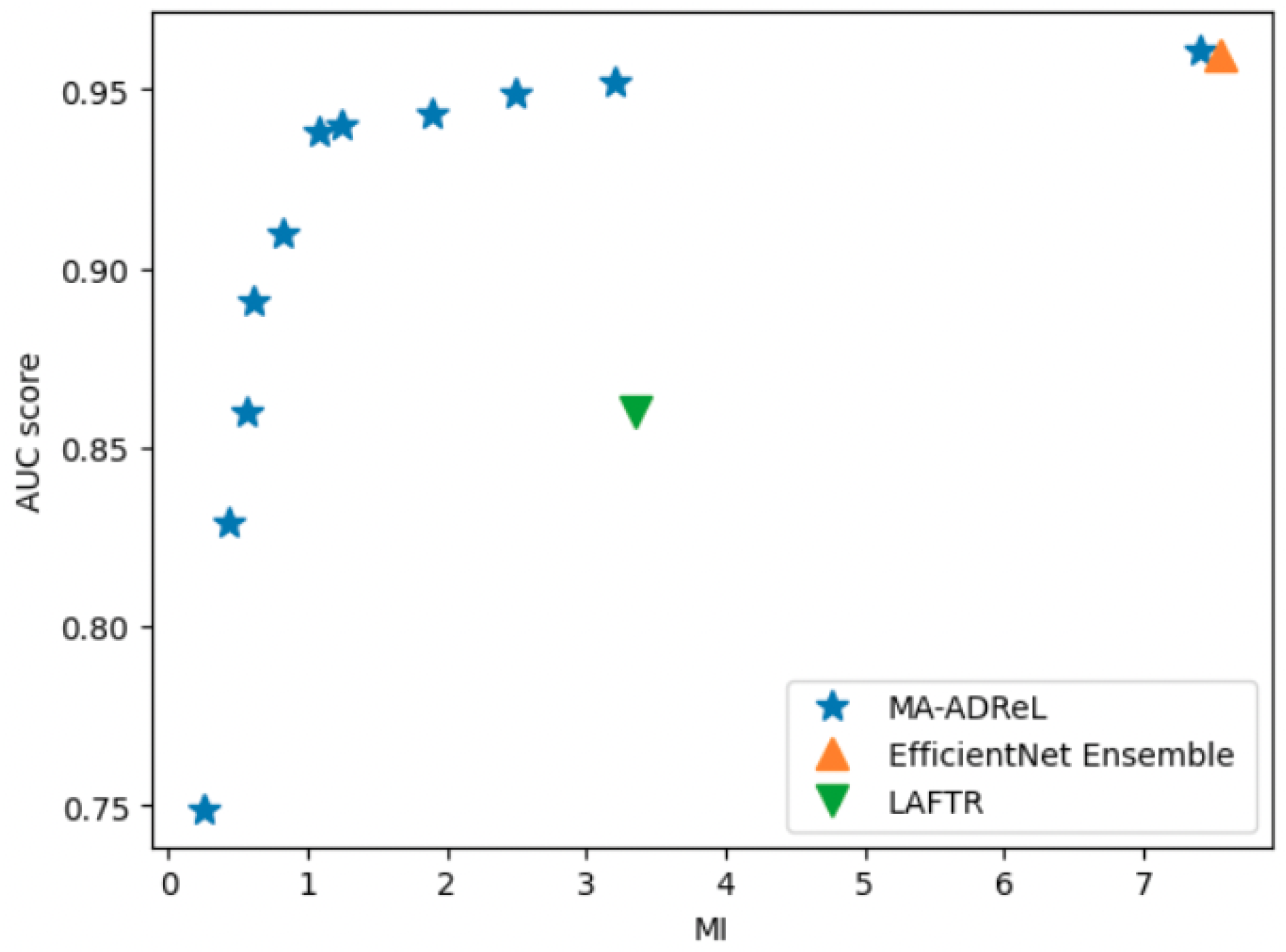
3.7. Baseline Setup
We compared MA-ADReL with several baselines, including (i) LAFTR learning [
14] and (ii) EfficientNet Ensemble, which is a vanilla training method without fairness constraints that achieved the best performance in the IIM-ISIC Melanoma Classification Challenge (i.e., the ISIC2019 dataset [
13]). We built upon their framework’s main classification backbone network.
We trained our model on 4 NVIDIA Tesla V100 GPUs with batch size 64 for all models using 5 random seeds. To schedule the training process, we employed cosine annealing with a single warm-up epoch [
36]. All models were trained for a total of 30 epochs. We report the average and standard deviation using the models with 5 random seeds on the test set. The performance metrics for evaluation are defined below.
3.8. Evaluation Criteria
We utilized the AUROC and AUPRC to evaluate the prediction performance, and we also utilized the MI score (as defined in Equation (
5)). To be more specific, the AUROC and AUPRC are defined as follows.
AUROC (Area Under the Receiver Operating Characteristic Curve). This is formulated as follows:
where TPR and FPR are the true positive rate and false positive rate at a threshold
t. The AUCROC is an integral of the TPR and FPR at all thresholds and quantifies the model’s ability to distinguish between the two classes (e.g., positive and negative) by calculating the area under the ROC curve. The AUCROC represents the probability that, if given a randomly chosen positive and negative sample, the model will rank the positive higher than the negative. The AUCROC of a perfect classifier is 1 and that of a random classifier is
.
AUPRC (Area Under the Precision–Recall Curve).
The precision–recall curve is another graphical representation of the model’s performance, particularly suitable for imbalanced datasets. It plots the precision against the recall at various classification thresholds
t and can be expressed mathematically as
The AUPRC quantifies the trade-off between the precision and recall across different classification thresholds, i.e., in terms of both not labeling negative samples as positive (precision) and correctly labeling the positive samples (recall). A higher AUCPR signifies a better-performing classifier. A perfect classifier will have an AUCPR of 1, and a random classifier’s AUCPR will be equal to the proportion of the number of positive samples in the data. As our dataset’s target variables are severely imbalanced, this can demonstrate the prediction performance from another perspective. We used Scikit-learn to calculate the AUROC and AUPRC criteria [
37].
5. Discussion and Future Work
Aimed at advancing the field of fair AI, our study presents MA-ADReL, a novel approach to counteracting age-related bias in skin lesion detection. Through the combination of adversarial learning and mutual information optimization, we have optimized the interplay between bias mitigation and performance retention. Nonetheless, our work is not without its limitations, which we acknowledge and discuss below.
One of the primary limitations of our study is the reliance on existing datasets, which, despite their utility, are not representative of the full demographic spectrum. The underrepresentation of certain age groups, particularly the elderly, in the ISIC2019 dataset poses a challenge in training and validating models that are equitable across all ages. This limitation is not unique to our study but is a common constraint in medical imaging research, which we hope that future data collection efforts will address. Future research could focus on training fair (and unfair) models on data from various younger age groups and testing them on various older age groups to develop an understanding of their performance. These experiments could establish the generalization capacities and limitations of models trained on younger patients’ skin lesions to detect older patients’ skin lesions.
Additionally, while our method has been effective in reducing age-related bias, it is possible that other forms of bias, such as those related to ethnicity, sex, or gender, may not be as effectively mitigated. Other types of bias, beyond age and demographics, may also be present in datasets due to selection bias, negative set bias, and category or labeling bias [
1,
2]. Therefore, it is very difficult to obtain a completely unbiased dataset in practical settings, especially those using human participants and different data collection protocols, instruments, and labeling strategies. Hypothetically, if a completely unbiased dataset existed, MA-ADRel would still perform comparably, with an additional functionality to manage future (age-related) bias. Our focus on age as a continuous attribute was intentional given the spotlight on digital ageism; however, a comprehensive assessment of all potential biases was beyond the scope of this study. We recommend that future research in this area should attempt to develop skin lesion models that can address different types of demographics and other data biases in one inclusive model. Other potential directions for research, besides adversarial learning to mitigate continuous variable-related bias (e.g., age), are to investigate deep imbalanced regression [
40] and supervised contrastive regression approaches [
41].
Lastly, our study focused on the technical aspects of bias mitigation and did not delve into the ethical and societal implications of deploying AI in healthcare. Future work should consider the broader ethical frameworks within which these technologies operate, including issues of consent, transparency, and accountability.
6. Conclusions
In this work, we introduced MA-ADReL, an innovative approach that utilizes adversarial learning to address the critical issue of age-related bias in the context of skin lesion detection. Our method differs from existing bias mitigation techniques, which predominately addresses discrete attributes (e.g., gender or race), by extending the focus to continuous attributes—specifically, age. By controlling the mutual information penalty term, MA-ADReL not only improves the fairness but also maintains high predictive accuracy, a delicate balance in the realm of AI fairness and performance. Our method’s innovation lies in its ability to manage continuous variables, which are often more complex to handle due to their inherent lack of natural categorization. This dual achievement is a significant milestone in the quest for fair AI. The implications of our research extend beyond technical advancements. As AI becomes increasingly integrated into healthcare, the need for algorithms that are fair, unbiased, and sensitive to demographic variables is important. The successful application of MA-ADReL on the ISIC2019 and PAD20 datasets illustrates its potential to transform the field of medical image analysis, ensuring that AI systems treat all patients equitably, regardless of age. Our work contributes to this critical discourse by providing a viable solution that can be potentially applied to other areas of medical diagnosis and beyond.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}