In Vitro Activity of Gentamicin-Loaded Bioabsorbable Beads against Different Microorganisms


Abstract
:1. Introduction
2. Objectives
3. Results and Discussion

{kind=link}
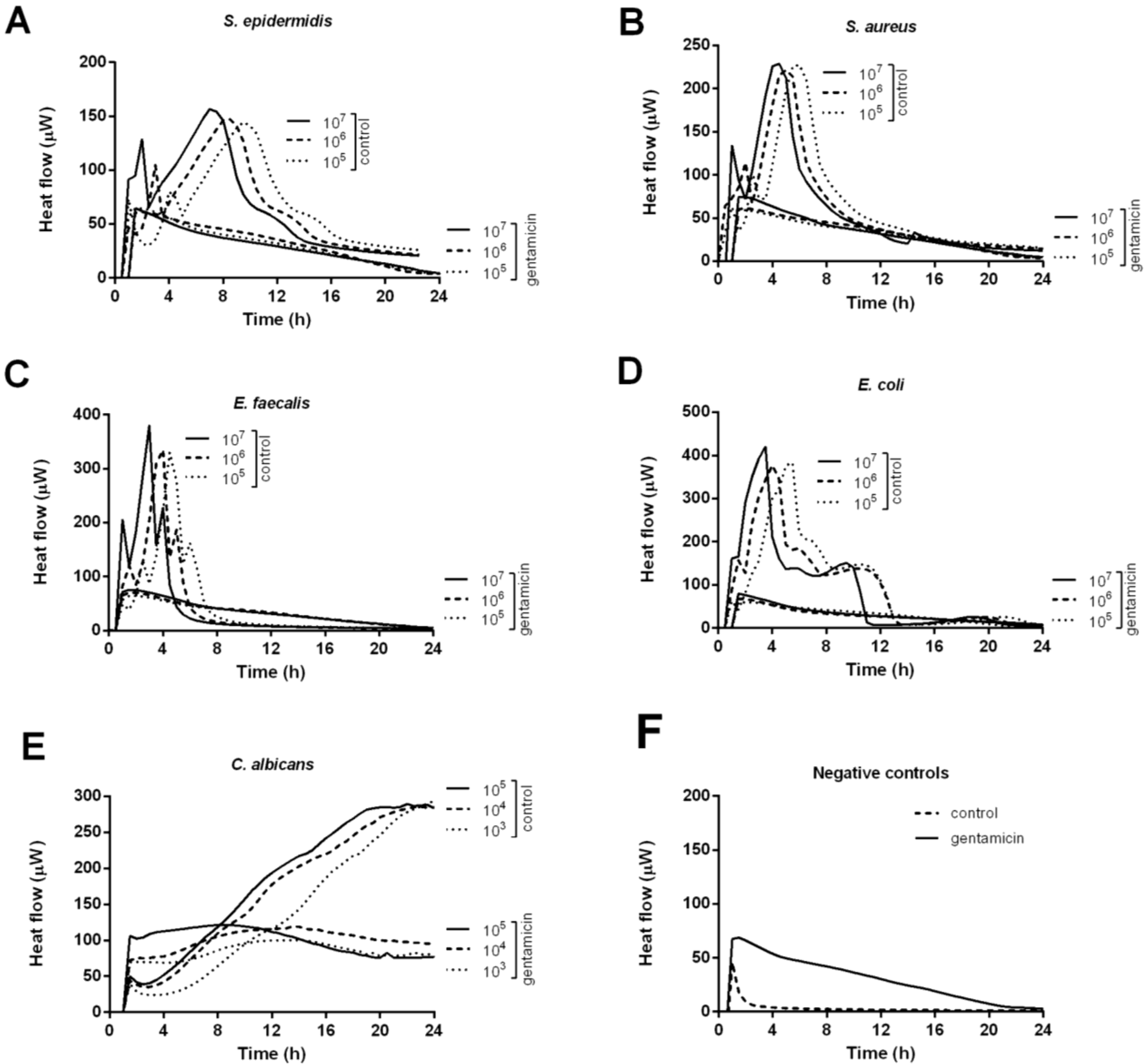
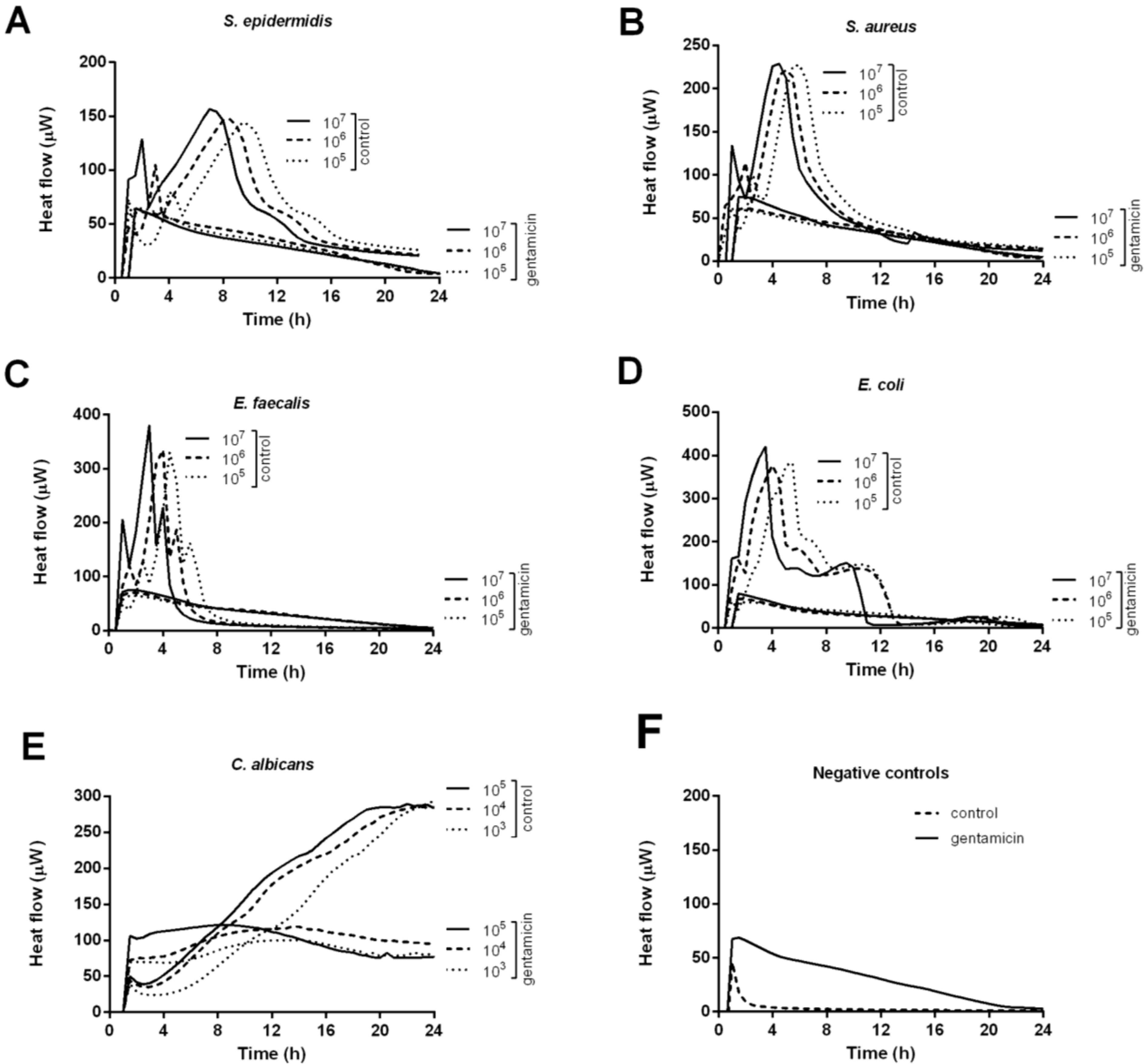
| Heat-flow peaks | Control | Gentamicin | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Peak (μW) | Time to peak (h) | Peak (μW) | |||||||
| Concentration (cfu/mL) | 107 | 106 | 105 | 107 | 106 | 105 | 107 | 106 | 105 |
| S. epidermidis | 111 | 102 | 98 | 7.1 | 8.2 | 9.4 | 0 | 0 | 0 |
| S. aureus | 184 | 175 | 183 | 4.4 | 4.9 | 5.7 | 8 | 0 | 0 |
| E. faecalis | 335 | 285 | 285 | 3.1 | 4.1 | 4.6 | 8 | 3 | 0 |
| E. coli | 375 | 325 | 338 | 3.4 | 3.9 | 5.2 | 12 | 0 | 0 |
| C. albicans * | 249 | 240 | 239 | 24 | 24 | 24 | 53 | 51 | 32 |
4. Experimental Section
4.1. Bone Graft Substitute
4.2. Study Organisms
4.3. Evaluation of Gentamicin Activity by Isothermal Microcalorimetry
5. Conclusions
Conflict of Interest
References
- Trampuz, A.; Zimmerli, W. Diagnosis and treatment of implant-associated septic arthritis and osteomyelitis. Curr. Infect. Dis. Rep. 2008, 10, 394–403. [Google Scholar] [CrossRef]
- Ostermann, P.A.; Henry, S.L.; Seligson, D. Timing of wound closure in severe compound fractures. Orthopedics 1994, 17, 397–399. [Google Scholar] [PubMed]
- Arciola, C.R.; Campoccia, D.; An, Y.H.; Baldassarri, L.; Pirini, V.; Donati, M.E.; Pegreffi, F.; Montanaro, L. Prevalence and antibiotic resistance of 15 minor staphylococcal species colonizing orthopedic implants. Int. J. Artif. Organs 2006, 29, 395–401. [Google Scholar] [PubMed]
- Von Eiff, C.; Arciola, C.R.; Montanaro, L.; Becker, K.; Campoccia, D. Emerging Staphylococcus species as new pathogens in implant infections. Int. J. Artif. Organs 2006, 29, 360–367. [Google Scholar] [PubMed]
- Del Pozo, J.L.; Patel, R. The challenge of treating biofilm-associated bacterial infections. Clin. Pharmacol. Ther. 2007, 82, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Mabry, R.L.; Holcomb, J.B.; Baker, A.M.; Cloonan, C.C.; Uhorchak, J.M.; Perkins, D.E.; Canfield, A.J.; Hagmann, J.H. United States Army Rangers in Somalia: An analysis of combat casualties on an urban battlefield. J. Trauma 2000, 49, 515–528; discussion 528–529. [Google Scholar] [CrossRef] [PubMed]
- Cierny, G., III; Mader, J.T.; Penninck, J.J. A clinical staging system for adult osteomyelitis. Clin. Orthop. Relat. Res. 2003, 414, 7–24. [Google Scholar] [CrossRef]
- Conterno, L.O.; da Silva Filho, C.R. Antibiotics for treating chronic osteomyelitis in adults. Cochrane. Database Syst. Rev. 2009. [CrossRef]
- Hermsen, E.D.; Hanson, M.; Sankaranarayanan, J.; Stoner, J.A.; Florescu, M.C.; Rupp, M.E. Clinical outcomes and nephrotoxicity associated with vancomycin trough concentrations during treatment of deep-seated infections. Expert. Opin. Drug Saf. 2010, 9, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Donlan, R.M. Biofilms: Microbial life on surfaces. Emerg. Infect. Dis. 2002, 8, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, H.W.; Engelbrecht, H. Über die Depotwirkung einiger Antibiotika bei Vermischung mit dem Kunstharz Palacos (in German). Chirurg 1970, 41, 511–515. [Google Scholar] [PubMed]
- Marks, K.E.; Nelson, C.L.; Lautenschlager, E.P. Antibiotic-impregnated acrylic bone cement. J. Bone Joint Surg. Am. 1976, 58, 358–364. [Google Scholar] [PubMed]
- Elson, R.A.; Jephcott, A.E.; McGechie, D.B.; Verettas, D. Antibiotic-loaded acrylic cement. J. Bone Joint Surg. Br. 1977, 59, 200–205. [Google Scholar] [PubMed]
- Neut, D.; van de Belt, H.; van Horn, J.R.; van der Mei, H.C.; Busscher, H.J. Residual gentamicin-release from antibiotic-loaded polymethylmethacrylate beads after 5 years of implantation. Biomaterials 2003, 24, 1829–1831. [Google Scholar] [CrossRef] [PubMed]
- Kendall, R.W.; Duncan, C.P.; Smith, J.A.; Ngui-Yen, J.H. Persistence of bacteria on antibiotic loaded acrylic depots. A reason for caution. Clin Orthop Relat Res. 1996, 329, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, H.W.; Elson, R.A.; Heinert, K. Antibiotic-loaded acrylic cement: current concepts. Clin. Orthop. Relat. Res. 1984, 190, 96–108. [Google Scholar] [PubMed]
- McLaren, A.C. Alternative materials to acrylic bone cement for delivery of depot antibiotics in orthopaedic infections. Clin. Orthop. Relat. Res. 2004, 427, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Cornell, C.N.; Tyndall, D.; Waller, S.; Lane, J.M.; Brause, B.D. Treatment of experimental osteomyelitis with antibiotic-impregnated bone graft substitute. J. Orthop. Res. 1993, 11, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, A.S.; Boden, S.D.; Goldberg, V.M.; Khan, Y.; Laurencin, C.T.; Rosier, R.N. American Academy of Orthopaedic Surgeons. The Committee on Biological, I. Bone-graft substitutes: Facts, fictions, and applications. J. Bone Joint Surg. Am. 2001, 83-A Suppl 2 Pt 2, 98–103. [Google Scholar]
- Dreesmann, H. Über Knochenplombierung (in German). Beitr. Klin. Chir. 1892, 9, 804–810. [Google Scholar]
- Kelly, C.M.; Wilkins, R.M.; Gitelis, S.; Hartjen, C.; Watson, J.T.; Kim, P.T. The use of a surgical grade calcium sulfate as a bone graft substitute: Results of a multicenter trial. Clin. Orthop. Relat. Res. 2001, 382, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Sidqui, M.; Collin, P.; Vitte, C.; Forest, N. Osteoblast adherence and resorption activity of isolated osteoclasts on calcium sulphate hemihydrate. Biomaterials 1995, 16, 1327–1332. [Google Scholar] [CrossRef] [PubMed]
- Turner, T.M.; Urban, R.M.; Gitelis, S.; Infanger, S.; Berzins, A.; Hall, D.J. Efficacy of calcium sulphate, a synthetic bone graft material, in healing a large canine medullary defect. In Proceesings of the 45th Annuual Meeting, Orethopedic Research Society, Anaheim, CA, USA, 1–4 February 1999. Abstract 522.
- Mackey, D.; Varlet, A.; Debeaumont, D. Antibiotic loaded plaster of Paris pellets: An in vitro study of a possible method of local antibiotic therapy in bone infection. Clin. Orthop. Relat. Res. 1982, 167, 263–268. [Google Scholar] [PubMed]
- Mousset, B.; Benoit, M.A.; Delloye, C.; Bouillet, R.; Gillard, J. Biodegradable implants for potential use in bone infection. An in vitro study of antibiotic-loaded calcium sulphate. Int. Orthop. 1995, 19, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Sulo, I. Gentamycin impregnated plaster beads in the treatment of bone infection. Rev. Chir. Orthop. Reparatrice Appar. Mot. 1993, 79, 299–305. [Google Scholar] [PubMed]
- Nelson, C.L.; McLaren, S.G.; Skinner, R.A.; Smeltzer, M.S.; Thomas, J.R.; Olsen, K.M. The treatment of experimental osteomyelitis by surgical debridement and the implantation of calcium sulfate tobramycin pellets. J. Orthop. Res. 2002, 20, 643–647. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.D.; Wild, L.M.; Schemitsch, E.H.; Waddell, J.P. The use of an antibiotic-impregnated, osteoconductive, bioabsorbable bone substitute in the treatment of infected long bone defects: early results of a prospective trial. J. Orthop. Trauma 2002, 16, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Beardmore, A.A.; Brooks, D.E.; Wenke, J.C.; Thomas, D.B. Effectiveness of local antibiotic delivery with an osteoinductive and osteoconductive bone-graft substitute. J. Bone Joint Surg. Am. 2005, 87, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Klemm, K. Septopal—A new way of local antibiotic therapy. In Local Antibiotic Treatment in Osteomyelitis and Soft Tissue Infections; Van Rens, T.J.G., Kayser, F.H., Eds.; Excerpta Medica: Amsterdam, The Netherlands, 1981; pp. 24–37. [Google Scholar]
- Wahlig, H.; Dingeldein, E.; Bergmann, R.; Reuss, K. The release of gentamicin from polymethylmethacrylate beads. An experimental and pharmacokinetic study. J. Bone Joint Surg. Br. 1978, 60B, 270–275. [Google Scholar]
- Wichelhaus, T.A.; Dingeldein, E.; Rauschmann, M.; Kluge, S.; Dieterich, R.; Schafer, V.; Brade, V. Elution characteristics of vancomycin, teicoplanin, gentamicin and clindamycin from calcium sulphate beads. J. Antimicrob. Chemother. 2001, 48, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Salzmann, S.; Antheaume, J.; Daniels, A.U. Microcalorimetry: A novel method for detection of microbial contamination in platelet products. Transfusion 2007, 47, 1643–1650. [Google Scholar] [CrossRef] [PubMed]
- Clauss, M.; Trampuz, A.; Borens, O.; Bohner, M.; Ilchmann, T. Biofilm formation on bone grafts and bone graft substitutes: comparison of different materials by a standard in vitro test and microcalorimetry. Acta Biomater. 2010, 6, 3791–3797. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, U.; Wirz, D.; Daniels, A.U. Isothermal micro calorimetry—A new method for MIC determinations: results for 12 antibiotics and reference strains of E. coli and S. aureus. BMC Microbiol. 2009. [Google Scholar] [CrossRef]
- Trampuz, A.; Steinhuber, A.; Wittwer, M.; Leib, S.L. Rapid diagnosis of experimental meningitis by bacterial heat production in cerebrospinal fluid. BMC Infect. Dis. 2007. [CrossRef]
- Kluin, O.S.; van der Mei, H.C.; Busscher, H.J.; Neut, D. Biodegradable vs. non-biodegradable antibiotic delivery devices in the treatment of osteomyelitis. Expert Opin. Drug Deliv. 2013, 10, 341–351. [Google Scholar] [CrossRef] [PubMed]
- Craig, W.A. Pharmacokinetic/pharmacodynamic parameters: Rationale for antibacterial dosing of mice and men. Clin. Infect. Dis. 1998, 26, 1–10; quiz 11–12. [Google Scholar] [CrossRef] [PubMed]
- Lerner, S.A.; Schmitt, B.A.; Seligsohn, R.; Matz, G.J. Comparative study of ototoxicity and nephrotoxicity in patients randomly assigned to treatment with amikacin or gentamicin. Am. J. Med. 1986, 80, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Miclau, T.; Edin, M.L.; Lester, G.E.; Lindsey, R.W.; Dahners, L.E. Bone toxicity of locally applied aminoglycosides. J. Orthop. Trauma 1995, 9, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Isefuku, S.; Joyner, C.J.; Simpson, A.H. Gentamicin may have an adverse effect on osteogenesis. J. Orthop. Trauma 2003, 17, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, A.D. Local antibiotic delivery vehicles in the treatment of musculoskeletal infection. Clin. Orthop. Relat. Res. 2005, 437, 91–96. [Google Scholar] [CrossRef] [PubMed]
- McLaren, A.C.; McLaren, S.G.; Nelson, C.L.; Wassell, D.L.; Olsen, K.M. The effect of sampling method on the elution of tobramycin from calcium sulfate. Clin. Orthop. Relat. Res. 2002, 403, 54–57. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Thein, E.; Tafin, U.F.; Betrisey, B.; Trampuz, A.; Borens, O. In Vitro Activity of Gentamicin-Loaded Bioabsorbable Beads against Different Microorganisms. Materials 2013, 6, 3284-3293. https://doi.org/10.3390/ma6083284
Thein E, Tafin UF, Betrisey B, Trampuz A, Borens O. In Vitro Activity of Gentamicin-Loaded Bioabsorbable Beads against Different Microorganisms. Materials. 2013; 6(8):3284-3293. https://doi.org/10.3390/ma6083284
Chicago/Turabian StyleThein, Eric, Ulrika Furustrand Tafin, Bertrand Betrisey, Andrej Trampuz, and Olivier Borens. 2013. "In Vitro Activity of Gentamicin-Loaded Bioabsorbable Beads against Different Microorganisms" Materials 6, no. 8: 3284-3293. https://doi.org/10.3390/ma6083284
APA StyleThein, E., Tafin, U. F., Betrisey, B., Trampuz, A., & Borens, O. (2013). In Vitro Activity of Gentamicin-Loaded Bioabsorbable Beads against Different Microorganisms. Materials, 6(8), 3284-3293. https://doi.org/10.3390/ma6083284