

Effect of a 4 mm vs. a 6 mm Diameter Mold on the Depth of Cure of 6 Bulk-Fill Resin-Based Composites



Abstract
1. Introduction
1.1. Tests Measuring Depth of Cure (DoC)
1.2. Limitations of the ISO 4049 Test
1.3. Clinical Relevance of a 4 mm Diameter Metal Mold to Test DoC of Bulk-Fill RBCs
1.4. Research Objectives and Hypotheses
- (1)
- Increasing the mold diameter from 4 to 6 mm will not significantly affect the DoC measurements of the six RBCs tested.
- (2)
- No significant difference will exist between DoC values obtained using single-wavelength or multi-wavelength light sources.
2. Materials and Methods
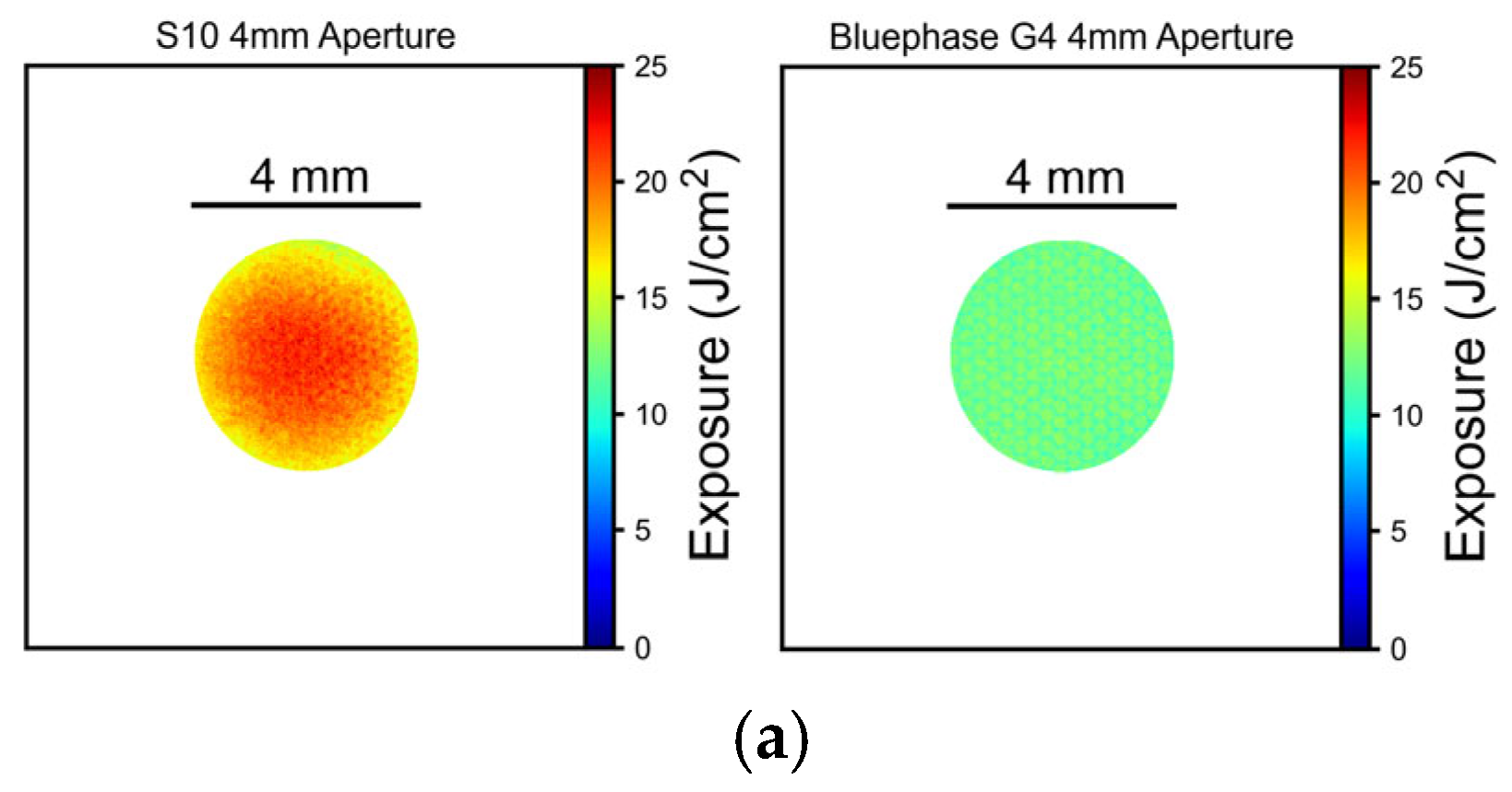
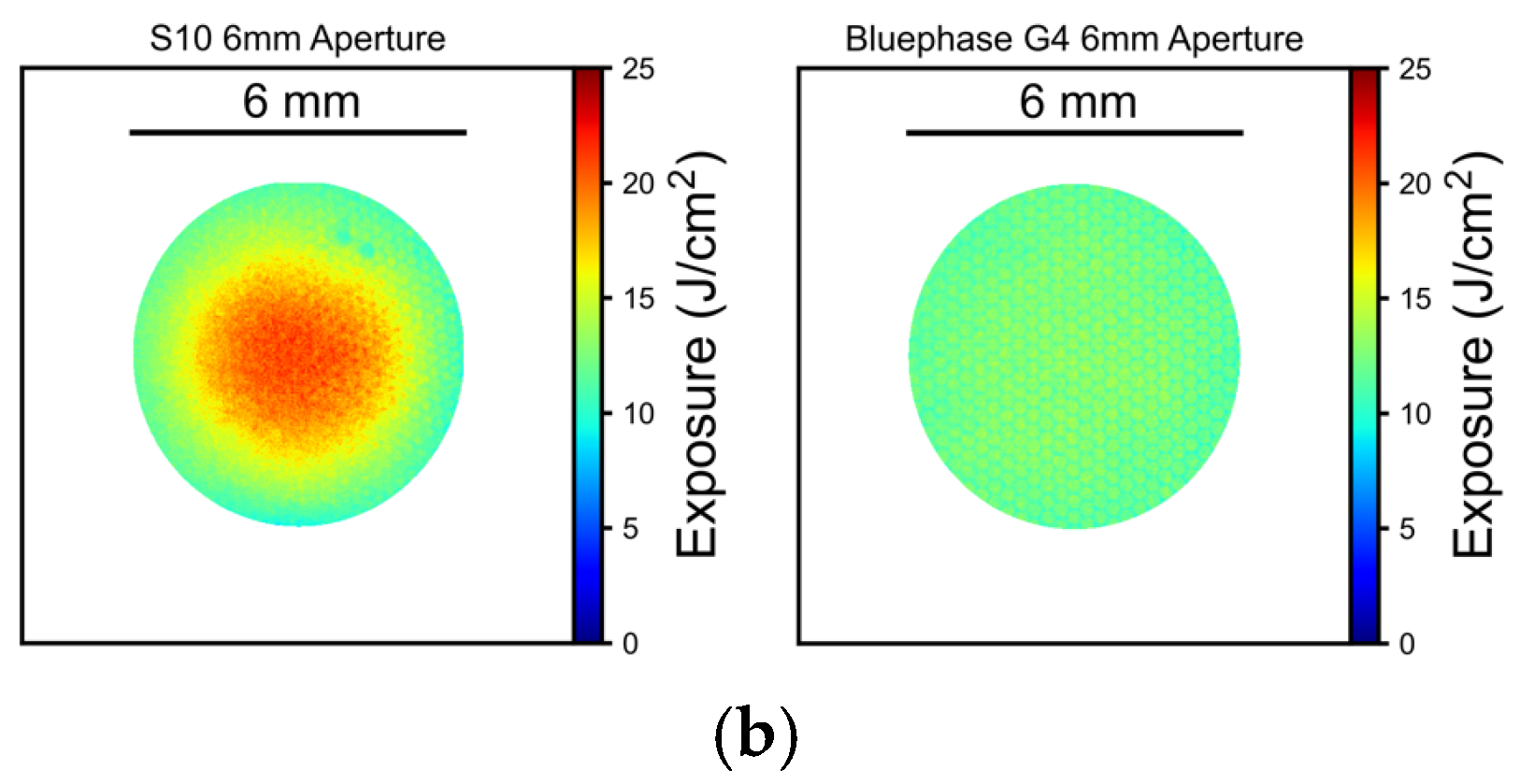
2.1. LCU Radiant Power and Beam Profile
2.2. Depth of Cure (DoC) of RBCs
2.3. Statistics
3. Results
3.1. Radiant Power and Beam Profile
3.2. Remaining Cured Composite Remnant Thickness and Depth of Cure (DoC)
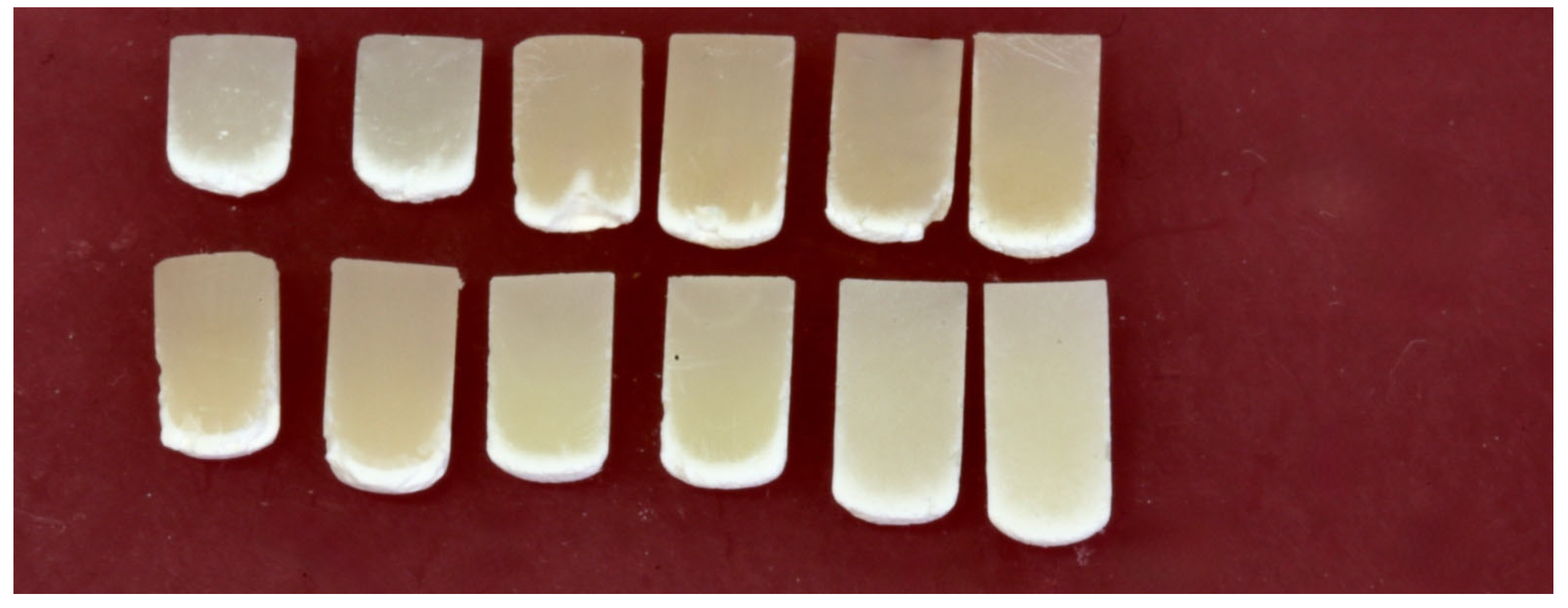
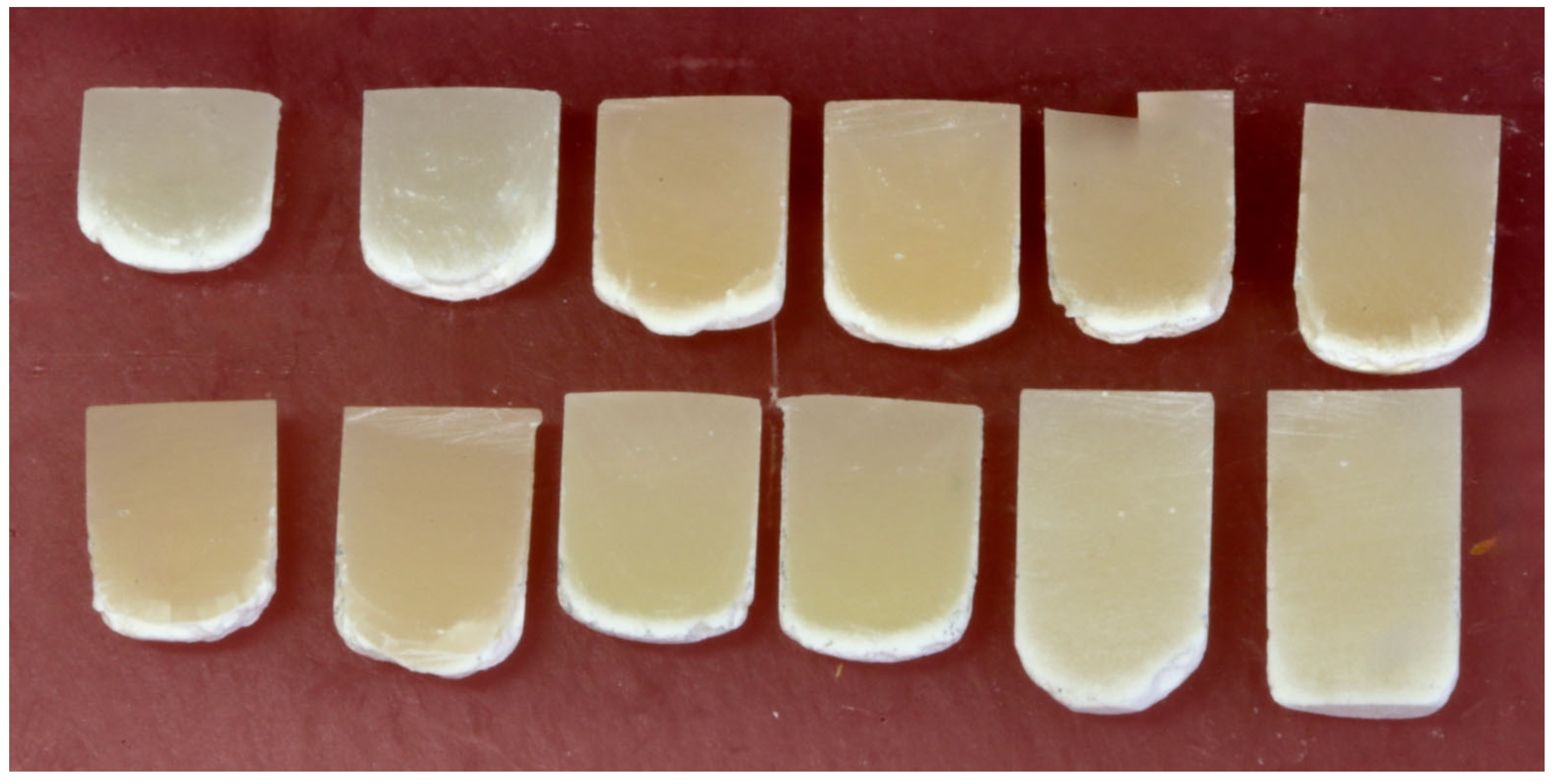
3.3. Bottom Surface Topography
4. Discussion
5. Conclusions
- The 6 mm diameter metal molds consistently produced greater depth-of-cure results than standard 4 mm diameter configurations specified in the ISO 4049 standard (p < 0.0001).
- The single-peak-wavelength LCU provided equivalent or superior performance compared to the multiple-peak-wavelength LCU tested in this study.
- The RBC polymerized in the metal molds consistently exhibited a dome-shaped morphology with a greater DoC at the center compared to the peripheral regions that were close to the metal walls.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| LCU | Light Curing Unit |
| RBC | Resin-based composite |
| DoC | Depth of Cure |
References
- FDI World Dental Federation. Dental amalgam phase down: Adopted by the FDI General Assembly: 7 September 2018, Buenos Aires, Argentina. Int. Dent. J. 2019, 69, 21–22. [Google Scholar] [CrossRef] [PubMed]
- European Commission Welcomes Provisional Agreement to Ban All Remaining Intentional Uses of Toxic Mercury in the EU. Available online: https://ec.europa.eu/commission/presscorner/detail/en/IP_24_679 (accessed on 28 February 2024).
- ISO 4049; Dentistry Polymer-Based Filling, Restorative Materials. International Standards Office: Geneva, Switzerland, 2019; p. 27.
- Ferracane, J.L.; Hilton, T.J.; Stansbury, J.W.; Watts, D.C.; Silikas, N.; Ilie, N.; Heintze, S.; Cadenaro, M.; Hickel, R. Academy of Dental Materials guidance-Resin composites: Part II-Technique sensitivity (handling, polymerization, dimensional changes). Dent. Mater. 2017, 33, 1171–1191. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaro, M.; Ferracane, J.L. Academy of Dental Materials guidance-Resin composites: Part I-Mechanical properties. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef]
- Durner, J.; Obermaier, J.; Draenert, M.; Ilie, N. Correlation of the degree of conversion with the amount of elutable substances in nano-hybrid dental composites. Dent. Mater. 2012, 28, 1146–1153. [Google Scholar] [CrossRef]
- Xu, X.; Sandras, D.A.; Burgess, J.O. Shear bond strength with increasing light-guide distance from dentin. J. Esthet. Restor. Dent. 2006, 18, 19–27; discussion 28. [Google Scholar] [CrossRef]
- Hass, V.; Dobrovolski, M.; Zander-Grande, C.; Martins, G.C.; Gordillo, L.A.; Rodrigues Accorinte Mde, L.; Gomes, O.M.; Loguercio, A.D.; Reis, A. Correlation between degree of conversion, resin-dentin bond strength and nanoleakage of simplified etch-and-rinse adhesives. Dent. Mater. 2013, 29, 921–928. [Google Scholar] [CrossRef]
- Vandewalle, K.S.; Ferracane, J.L.; Hilton, T.J.; Erickson, R.L.; Sakaguchi, R.L. Effect of energy density on properties and marginal integrity of posterior resin composite restorations. Dent. Mater. 2004, 20, 96–106. [Google Scholar] [CrossRef]
- Ilie, N.; Schmalz, G.; Fujioka-Kobayashi, M.; Lussi, A.; Price, R.B. Correlation of the mechanical and biological response in light-cured RBCs to receiving a range of radiant exposures: Effect of violet light. J. Dent. 2021, 105, 103568. [Google Scholar] [CrossRef]
- Ferracane, J.L.; Mitchem, J.C.; Condon, J.R.; Todd, R. Wear and marginal breakdown of composites with various degrees of cure. J. Dent. Res. 1997, 76, 1508–1516. [Google Scholar] [CrossRef]
- Kleverlaan, C.J.; de Gee, A.J. Curing efficiency and heat generation of various resin composites cured with high-intensity halogen lights. Eur. J. Oral Sci. 2004, 112, 84–88. [Google Scholar] [CrossRef]
- Fan, P.L.; Stanford, C.M.; Stanford, W.B.; Leung, R.; Stanford, J.W. Effects of backing reflectance and mold size on polymerization of photo-activated composite resin. J. Dent. Res. 1984, 63, 1245–1247. [Google Scholar] [CrossRef] [PubMed]
- Harrington, E.; Wilson, H.J. Depth of cure of radiation-activated materials--effect of mould material and cavity size. J. Dent. 1993, 21, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Erickson, R.L.; Barkmeier, W.W. Curing characteristics of a composite. Part 2: The effect of curing configuration on depth and distribution of cure. Dent. Mater. 2014, 30, e134–e145. [Google Scholar] [CrossRef]
- Erickson, R.L.; Barkmeier, W.W. Effect of mold diameter on the depth of cure of a resin-based composite material. Eur. J. Oral Sci. 2017, 125, 88–92. [Google Scholar] [CrossRef]
- AlShaafi, M.M.; AlQussier, A.; AlQahtani, M.Q.; Price, R.B. Effect of Mold Type and Diameter on the Depth of Cure of Three Resin-Based Composites. Oper. Dent. 2018, 43, 520–529. [Google Scholar] [CrossRef]
- Erickson, R.L.; Barkmeier, W.W. Comparisons of ISO depth of cure for a resin composite in stainless-steel and natural-tooth molds. Eur. J. Oral Sci. 2019, 127, 556–563. [Google Scholar] [CrossRef]
- Vandewalle, K.S.; Roberts, H.W.; Rueggeberg, F.A. Power distribution across the face of different light guides and its effect on composite surface microhardness. J. Esthet. Restor. Dent. 2008, 20, 108–117; discussion 118. [Google Scholar] [CrossRef]
- Shimokawa, C.; Turbino, M.L.; Giannini, M.; Braga, R.R.; Price, R.B. Effect of Curing Light and Exposure Time on the Polymerization of Bulk-Fill Resin-Based Composites in Molar Teeth. Oper. Dent. 2020, 45, E141–E155. [Google Scholar] [CrossRef]
- Price, R.B.; Rueggeberg, F.A.; Harlow, J.; Sullivan, B. Effect of mold type, diameter, and uncured composite removal method on depth of cure. Clin. Oral Investig. 2016, 20, 1699–1707. [Google Scholar] [CrossRef]
- Ribeiro, M.; Maucoski, C.; Price, R.B.; Soares, C.J. Effect of a 3-second Off-label Exposure on the Depth of Cure of Eight Resin-based Composites. Oper. Dent. 2024, 49, 421–431. [Google Scholar]
- McCabe, J.F.; Carrick, T.E. Output from visible-light activation units and depth of cure of light-activated composites. J. Dent. Res. 1989, 68, 1534–1539. [Google Scholar] [CrossRef] [PubMed]
- Asmussen, E.; Peutzfeldt, A. Polymer structure of a light-cured resin composite in relation to distance from the surface. Eur. J. Oral Sci. 2003, 111, 277–279. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.; Rueggeberg, F.A.; Looney, S.W.; Oxford, A.; Hassan, Z. Variation Comparison of Depth-of-Cure Between Scraping and Chemical Removal Methods. Abstract 2436. In Proceedings of the IADR General Session 2009, Miami, FL, USA, 1–4 April 2009. [Google Scholar]
- Miletic, V.; Pongprueksa, P.; De Munck, J.; Brooks, N.R.; Van Meerbeek, B. Curing characteristics of flowable and sculptable bulk-fill composites. Clin. Oral Investig. 2017, 21, 1201–1212. [Google Scholar] [CrossRef]
- Corciolani, G.; Vichi, A.; Davidson, C.L.; Ferrari, M. The influence of tip geometry and distance on light-curing efficacy. Oper. Dent. 2008, 33, 325–331. [Google Scholar] [CrossRef]
- Comisi, J.C.; Price, R.B.; Kinley-Howard, K.; Maucoski, C.; Rader, E. Ability of Six Curing Lights to Photocure Four Resin-Based Composites in a MOD-Mold: A Double-Blind Study. Eur. J. Prosthodont. Restor. Dent. 2024, 32, 301–313. [Google Scholar]
- Ash, M.M.; Nelson, S.J.; Ash, M.M. Wheeler’s Dental Anatomy, Physiology, and Occlusion, 8th ed.; W.B. Saunders: Philadelphia, PA, USA, 2003; 523p. [Google Scholar]
- Shimokawa, C.A.K.; Turbino, M.L.; Giannini, M.; Braga, R.R.; Price, R.B. Effect of light curing units on the polymerization of bulk fill resin-based composites. Dent. Mater. 2018, 34, 1211–1221. [Google Scholar] [CrossRef]
- Hadis, M.A.; Shortall, A.C.; Palin, W.M. The power of light—From dental materials processing to diagnostics and therapeutics. Biomater. Investig. Dent. 2024, 11, 40308. [Google Scholar] [CrossRef]
- Erickson, R.L.; Barkmeier, W.W.; Halvorson, R.H. Curing characteristics of a composite—Part 1: Cure depth relationship to conversion, hardness and radiant exposure. Dent. Mater. 2014, 30, e125–e133. [Google Scholar] [CrossRef]
- Thomaidis, S.; Kampouropoulos, D.; Antoniadou, M.; Kakaboura, A. Evaluation of the Depth of Cure by Microhardness of Bulk-Fill Composites with Monowave and Polywave LED Light-Curing Units. Appl. Sci. 2024, 14, 11532. [Google Scholar] [CrossRef]
- Contreras, S.C.M.; Jurema, A.L.B.; Claudino, E.S.; Bresciani, E.; Caneppele, T.M.F. Monowave and polywave light-curing of bulk-fill resin composites: Degree of conversion and marginal adaptation following thermomechanical aging. Biomater. Investig. Dent. 2021, 8, 72–78. [Google Scholar] [CrossRef]
- Menees, T.S.; Lin, C.P.; Kojic, D.D.; Burgess, J.O.; Lawson, N.C. Depth of cure of bulk fill composites with monowave and polywave curing lights. Am. J. Dent. 2015, 28, 357–361. [Google Scholar]
- 3s PowerCure: Scientific Documentation; Ivoclar Vivadent AG Research and Development Scientific Services; Ivoclar Vivadent: Schaan, Liechtenstein, 2019.
- Aura Ultra Universal Bulk Fill Restorative Material Instructions for Use; SDI Limited: Bayswater, VIC, Australia, 2016.
- Filtek One Bulk Fill Restorative: Technical Product Profile; 3M Oral Care: St. Paul, MN, USA, 2016.
- Hasslen, J.A.; Barkmeier, W.W.; Shaddy, R.S.; Little, J.R. Depth of cure of high-viscosity bulk-fill and conventional resin composites using varying irradiance exposures with a light-emitting diode curing unit. J. Oral Sci. 2019, 61, 425–430. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| RBC | Manufacturer | Lot Number | Shade | Initiator | Minimum Irradiance and Recommended Wavelength Range |
|---|---|---|---|---|---|
| Tetric plus Fill | Ivoclar Vivadent, Schaan, Liechtenstein | YM0206 | A3 | Camphorquinone plus Ivocerin | 900–1400 mW/cm2 for 10 s in the 400–500 nm range |
| Tetric plus Flow | Ivoclar Vivadent, Schaan, Liechtenstein | YM0210 | A3 | Camphorquinone plus Ivocerin | 900–1400 mW/cm2 for 10 s in the 400–500 nm range |
| Tetric PowerFill | Ivoclar Vivadent, Schaan, Liechtenstein | Z06955 | IVA | Camphorquinone plus Ivocerin | 900–1400 mW/cm2 for 10 s in the 400–500 nm range |
| Tetric PowerFlow | Ivoclar Vivadent, Schaan, Liechtenstein | Z06P1N | IVA | Camphorquinone plus Ivocerin | 900–1400 mW/cm2 for 10 s in the 400–500 nm range |
| Filtek One | 3 M, St. Paul, MN, USA | 4867A3 | A3 | Camphorquinone | 1000–2000 mW/cm2 for 20 s in the 400–500 nm range |
| Aura Bulk Fill | SDI, Bayswater, Victoria, Australia | 1222869 | Universal | Camphorquinone | High-power LED curing light for 20 s in the 460–480 nm range |
| RBC, Mold Diameter and LCU | Length (mm) | S.D. | Increase (%) Using the 6 mm Diameter Mold |
|---|---|---|---|
| PowerFlow, 6 mm, S10 | 5 | 0.01 | 19.0% |
| PowerFlow, 6 mm, G4 | 4.9 | 0.02 | 22.5% |
| Filtek One, 6 mm, S10 | 4.2 | 0.09 | 10.5% |
| PowerFlow, 4 mm, S10 | 4.2 | 0.08 | |
| PowerFill, 6 mm, S10 | 4.1 | 0.09 | 17.1% |
| Tetric plus Flow, 6 mm, S10 | 4.1 | 0.04 | 13.9% |
| PowerFlow, 4 mm, G4 | 4 | 0.04 | |
| Filtek One, 4 mm, S10 | 3.8 | 0.03 | |
| PowerFill, 6 mm, G4 | 3.8 | 0.08 | 15.2% |
| Tetric plus Fill, 6 mm, S10 | 3.8 | 0.08 | 11.8% |
| Tetric plus Flow, 6 mm, G4 | 3.8 | 0.05 | 11.8% |
| Filtek One, 6 mm, G4 | 3.7 | 0.04 | 10.8% |
| Tetric plus Fill, 6 mm, G4 | 3.6 | 0.13 | 12.5% |
| Tetric plus Flow, 4 mm, S10 | 3.6 | 0.12 | |
| PowerFill, 4 mm, S10 | 3.5 | 0.12 | |
| Tetric plus Fill, 4 mm, S10 | 3.4 | 0.11 | |
| Tetric plus Flow, 4 mm, G4 | 3.4 | 0.03 | |
| Filtek One, 4 mm, G4 | 3.3 | 0.04 | |
| PowerFill, 4 mm, G4 | 3.3 | 0.05 | |
| Tetric plus Fill, 4 mm, G4 | 3.2 | 0.06 | |
| AuraBulk, 6 mm, S10 | 3.1 | 0.07 | 14.8% |
| AuraBulk, 6 mm, G4 | 2.9 | 0.07 | 11.5% |
| AuraBulk, 4 mm, S10 | 2.7 | 0.08 | |
| AuraBulk, 4 mm, G4 | 2.6 | 0.04 |
| Factor | DF | Sum of Squares | Mean Square | F-Value | p-Value | Power |
|---|---|---|---|---|---|---|
| RBC | 5 | 29.35 | 5.87 | 1070.28 | <0.0001 | 1.0 |
| Mold Diameter | 1 | 7.72 | 7.72 | 1407.90 | <0.0001 | 1.0 |
| LCU | 1 | 1.88 | 1.88 | 342.79 | <0.0001 | 1.0 |
| RBC*Mold Diameter | 5 | 0.89 | 0.18 | 32.40 | <0.0001 | 1.0 |
| RBC*LCU | 5 | 0.32 | 0.06 | 11.67 | <0.0001 | 1.0 |
| Mold Diameter* Light | 1 | 0.00 | 0.00 | 0.37 | 0.55 | 0.09 |
| RBC*Mold Diameter* LCU | 5 | 0.06 | 0.01 | 2.26 | 0.05 | 0.71 |
| Residual | 96 | 0.53 | 0.01 | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulati, A.; Gareau, A.P.; Price, R.B. Effect of a 4 mm vs. a 6 mm Diameter Mold on the Depth of Cure of 6 Bulk-Fill Resin-Based Composites. Materials 2025, 18, 2548. https://doi.org/10.3390/ma18112548
Gulati A, Gareau AP, Price RB. Effect of a 4 mm vs. a 6 mm Diameter Mold on the Depth of Cure of 6 Bulk-Fill Resin-Based Composites. Materials. 2025; 18(11):2548. https://doi.org/10.3390/ma18112548
Chicago/Turabian StyleGulati, Anubhav, Alexandre P. Gareau, and Richard B. Price. 2025. "Effect of a 4 mm vs. a 6 mm Diameter Mold on the Depth of Cure of 6 Bulk-Fill Resin-Based Composites" Materials 18, no. 11: 2548. https://doi.org/10.3390/ma18112548
APA StyleGulati, A., Gareau, A. P., & Price, R. B. (2025). Effect of a 4 mm vs. a 6 mm Diameter Mold on the Depth of Cure of 6 Bulk-Fill Resin-Based Composites. Materials, 18(11), 2548. https://doi.org/10.3390/ma18112548