
Design of New Concept of Knitted Hernia Implant

 , ,
, ,  ,
,
Abstract
:1. Introduction
- the random arrangement of monofilament and the difference in the kind of the polymer in the hybrid knitted implants, resulting in a reduction in the assumed performance and safety and a significant rise in the risk of internal organ/implant adhesion if the hernia mesh is implanted using laparoscopic surgery [15,16,17];
- a significantly high surface density (e.g., for hernia meshes made entirely of PVDF monofilament, surface density >> 120 g/m2 relative to the surface density of knitted, polypropylene implants < 80 g/m2), resulting in a lack of biomimetics and risk of thick postoperative scar formation (reduction in patient comfort, complications long after surgery, breathing problems, pain, etc.) [15,17,18,19];
- the reduction of the risk of the implant to the viscera (if direct contact of the implant is necessary);
- acceleration of the connective tissue in-growth due to the enhancement of the implant surface promoting the fixation of the implant.
2. Materials and Methods
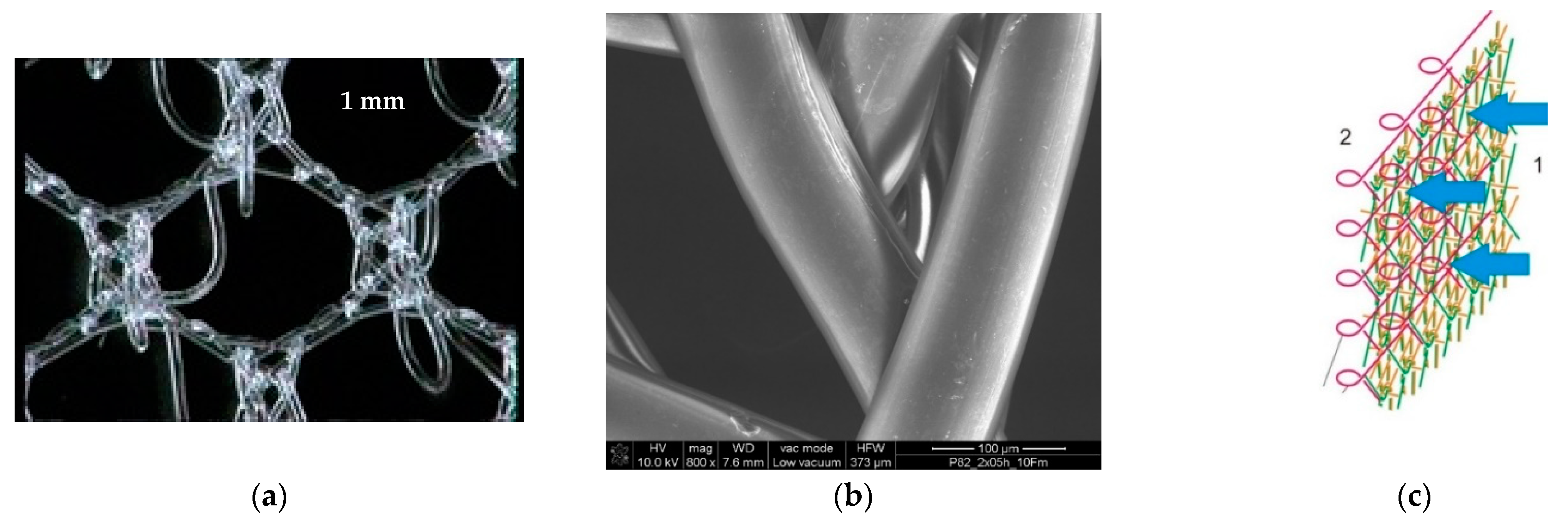
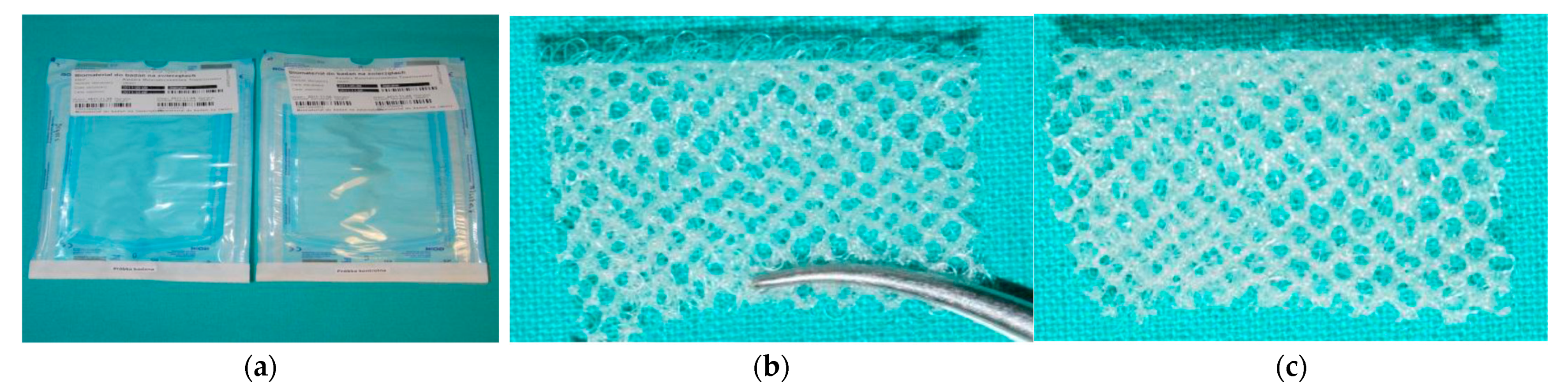
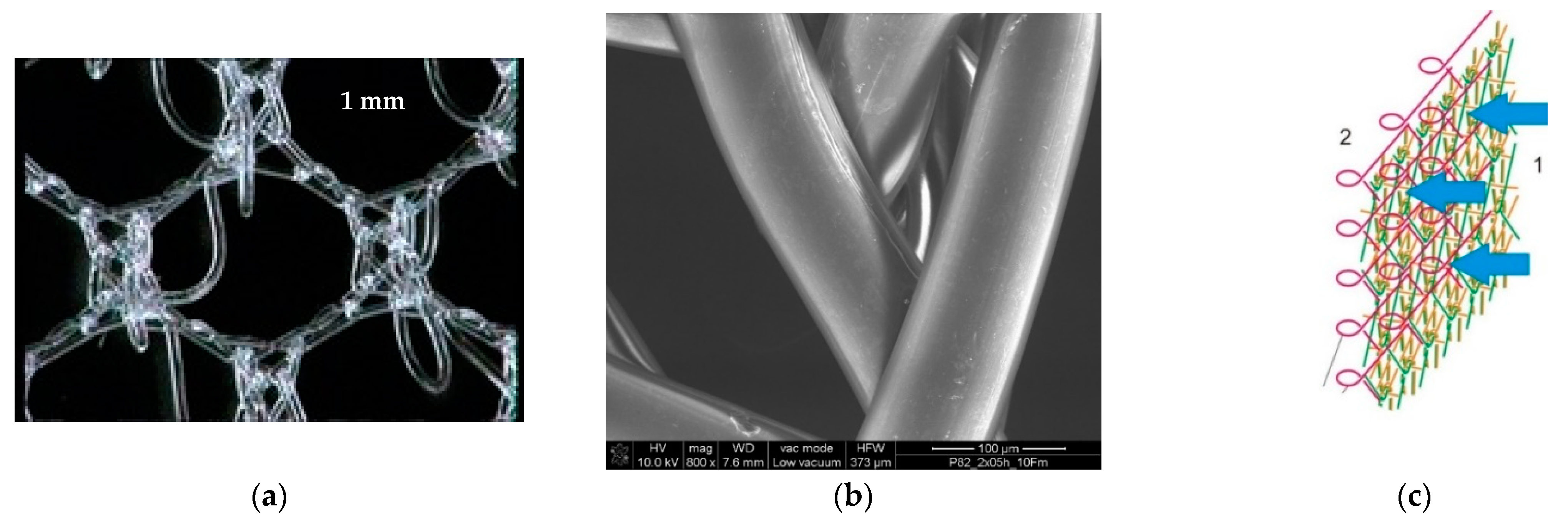
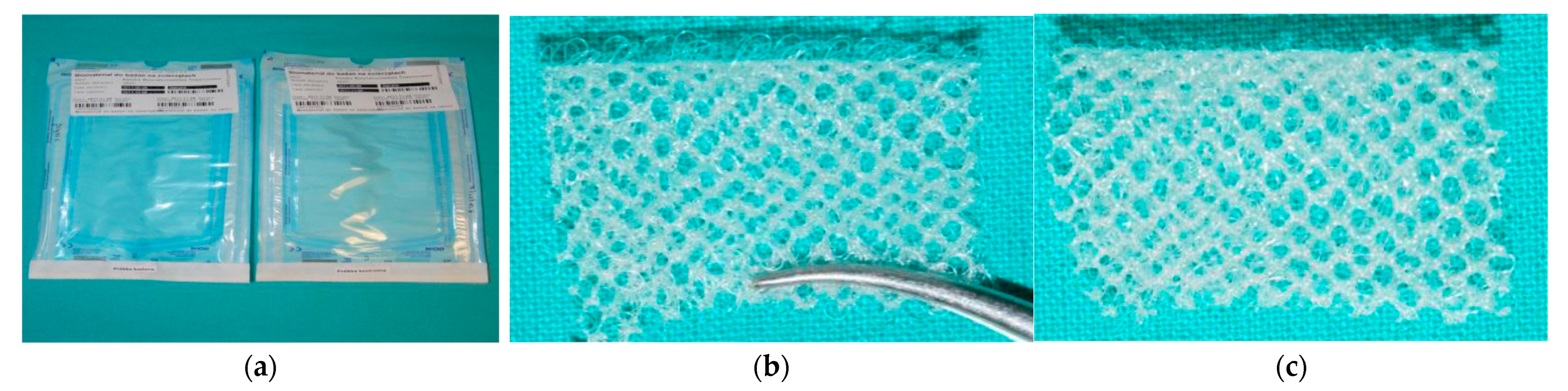
2.1. Knitted Implants
2.2. Methods
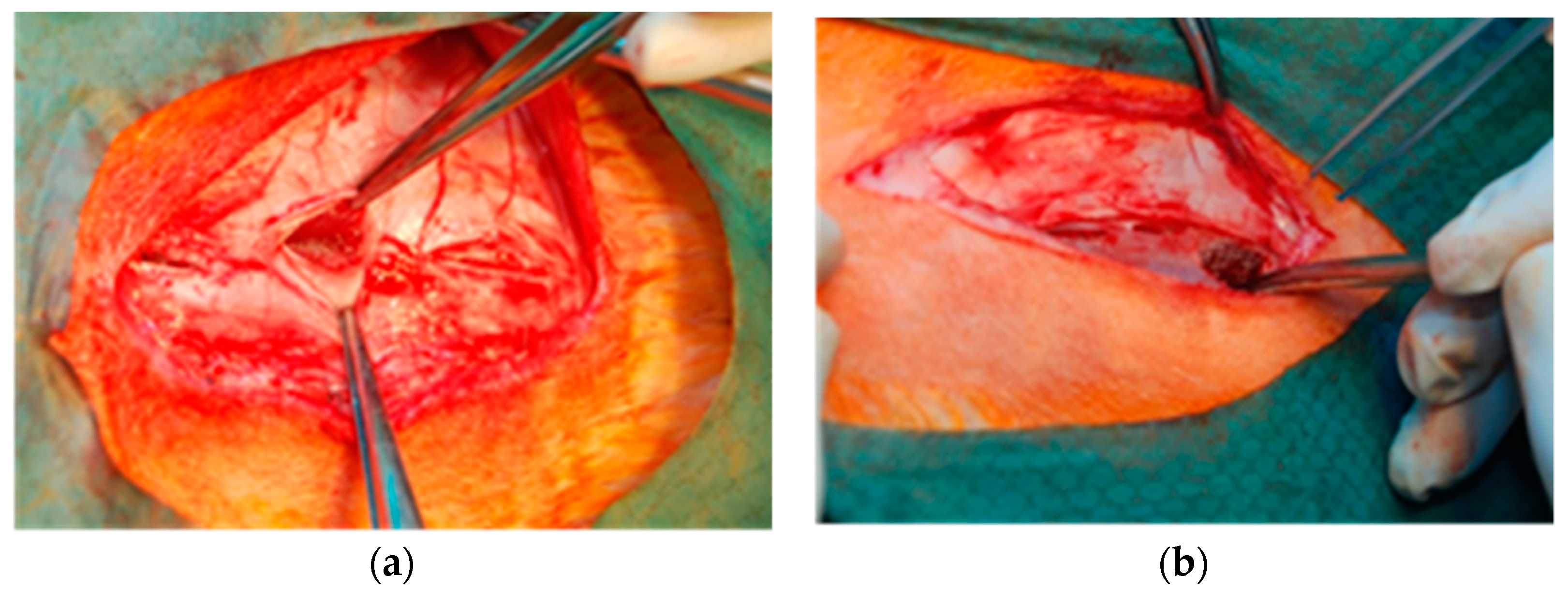
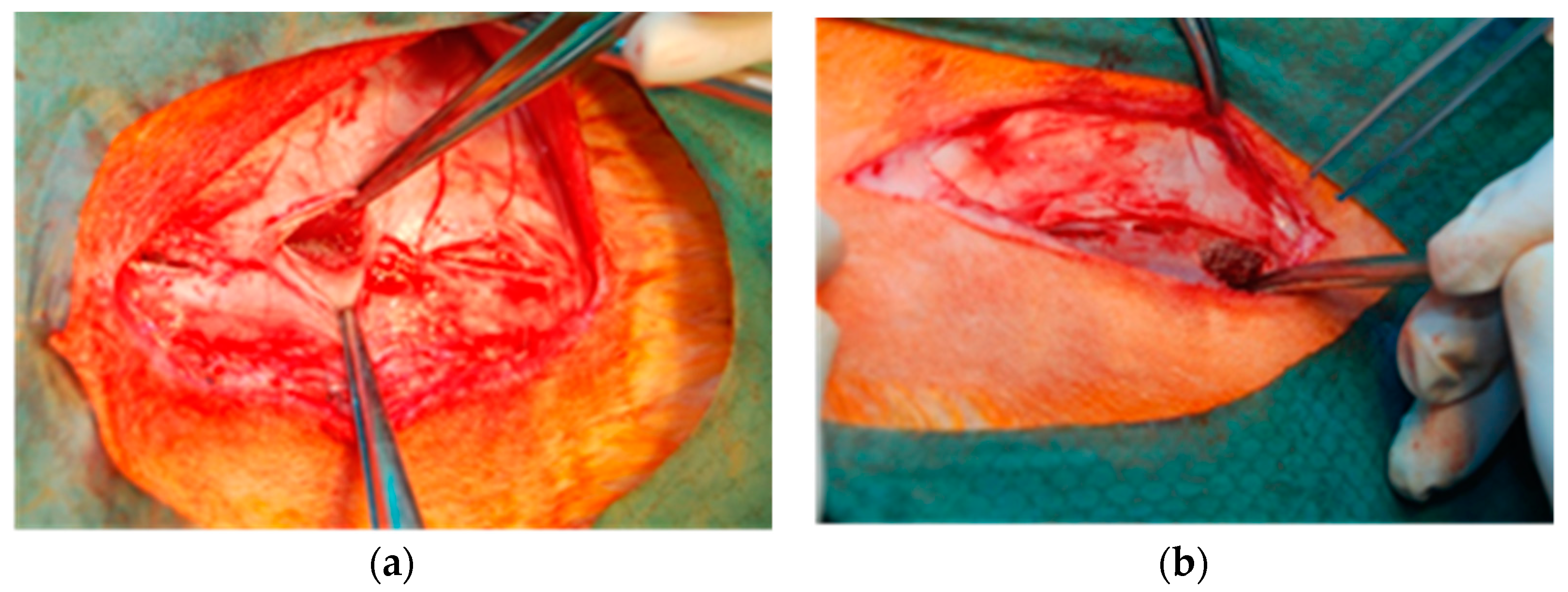
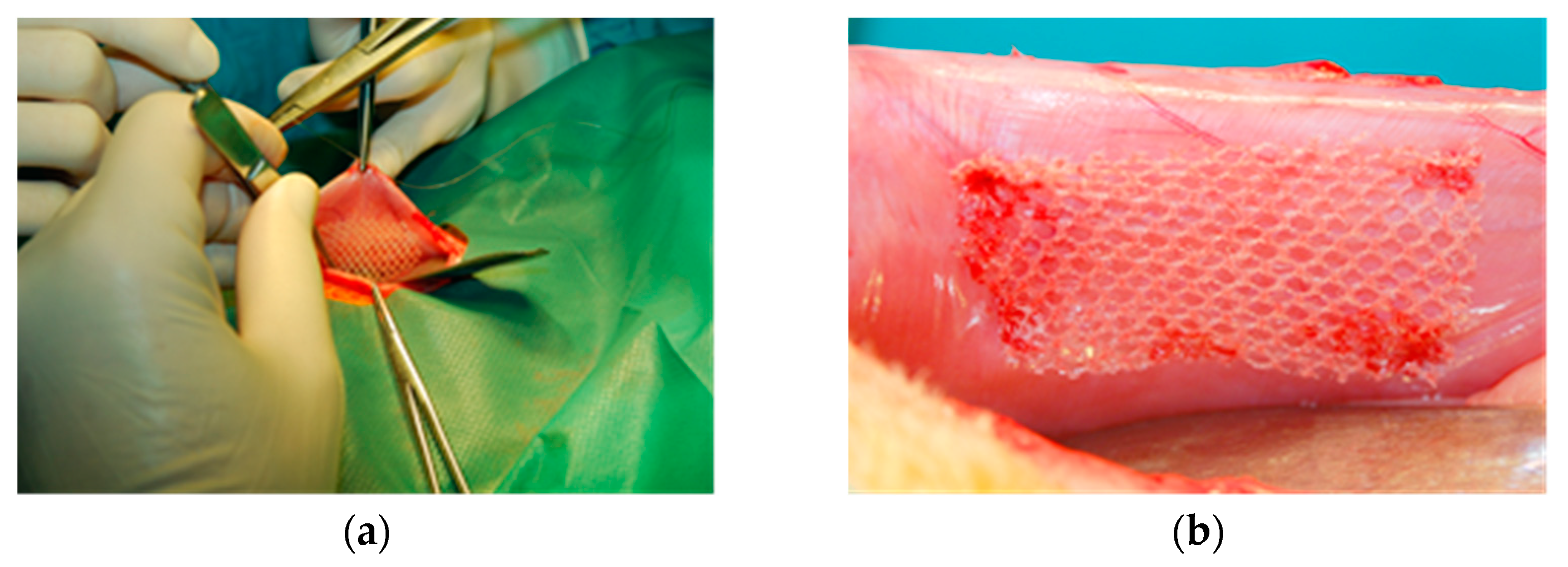
2.2.1. Local Effect after Implantation in Muscles
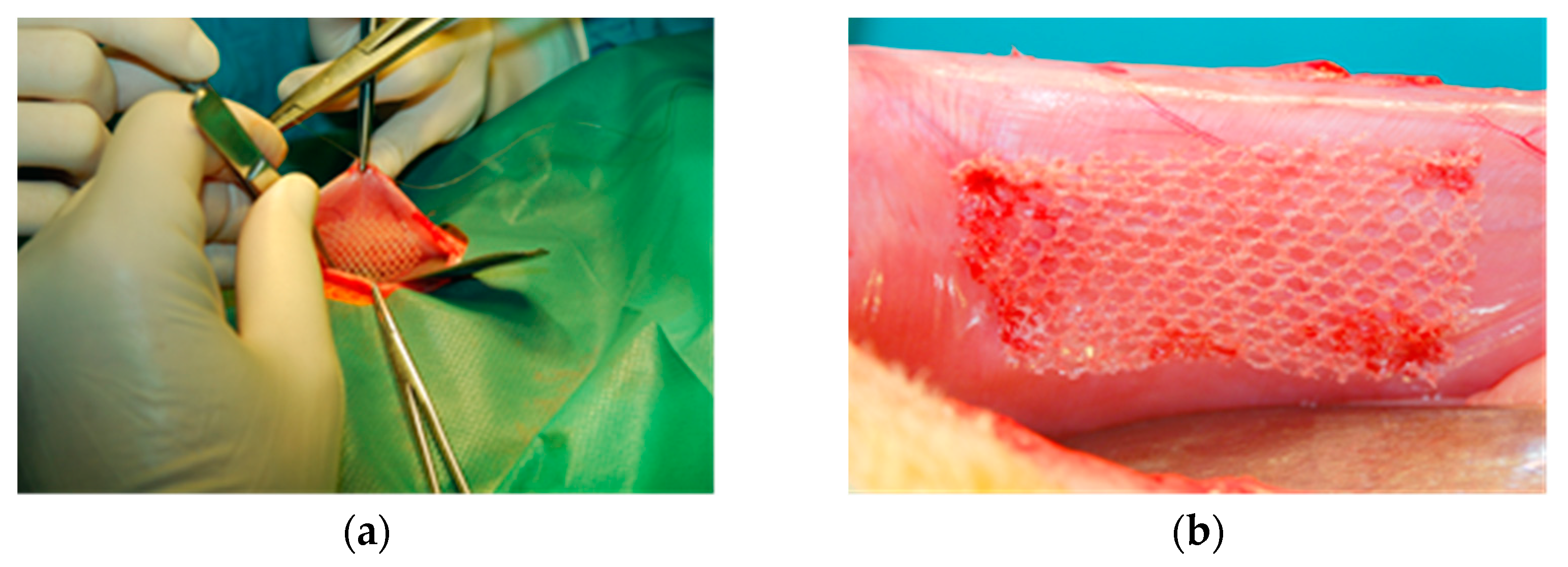
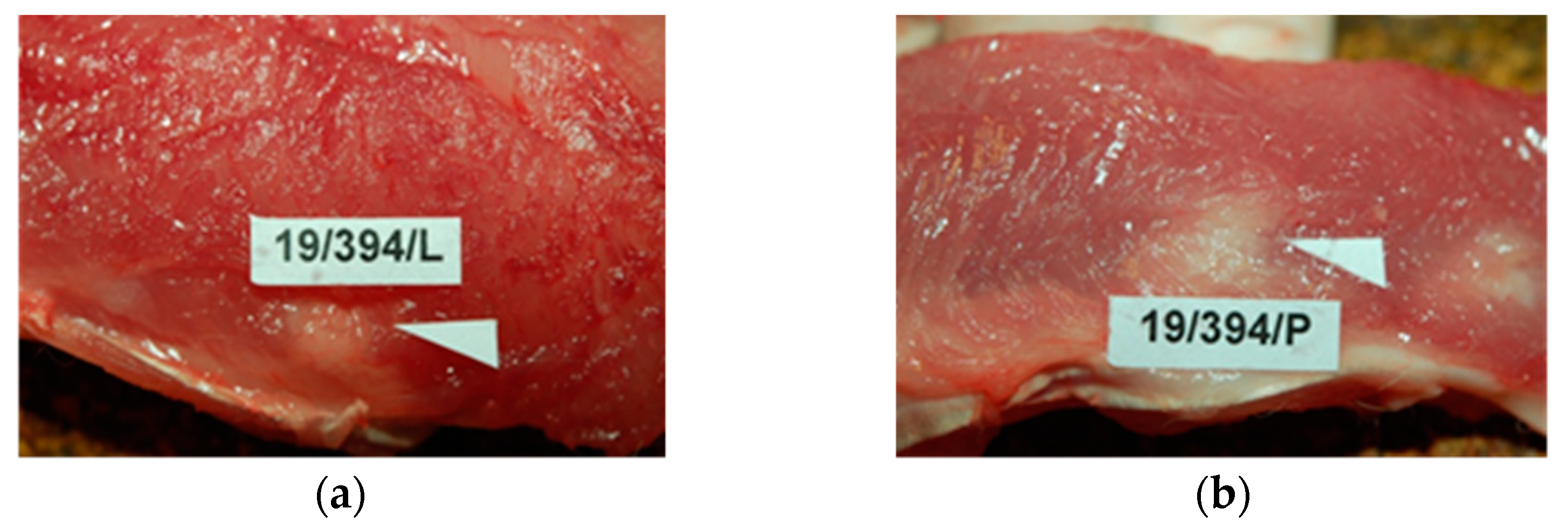
2.2.2. Local Effect after Implantation in the Abdominal Wall
- -
- adhesion of the tested sample to the viscera in direct contact of the surface with a nanolayer of PACVD originated fluoropolymer or non-modified reference with them as a result of intraperitoneal implantation;
- -
- local, potential biological incompatibility when the developed medical device is used as a textile implant for hernia reconstruction.
3. Results and Discussion
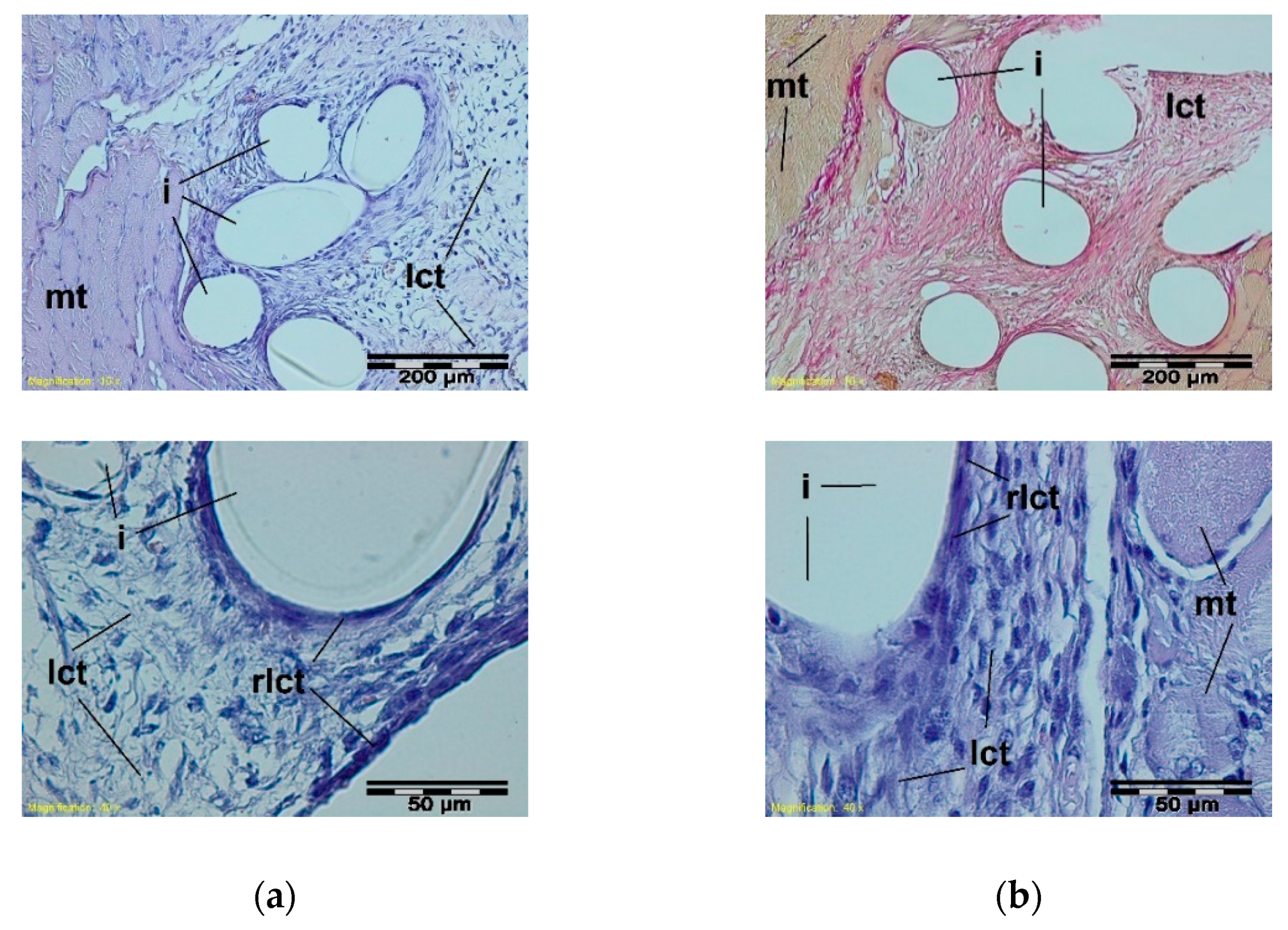
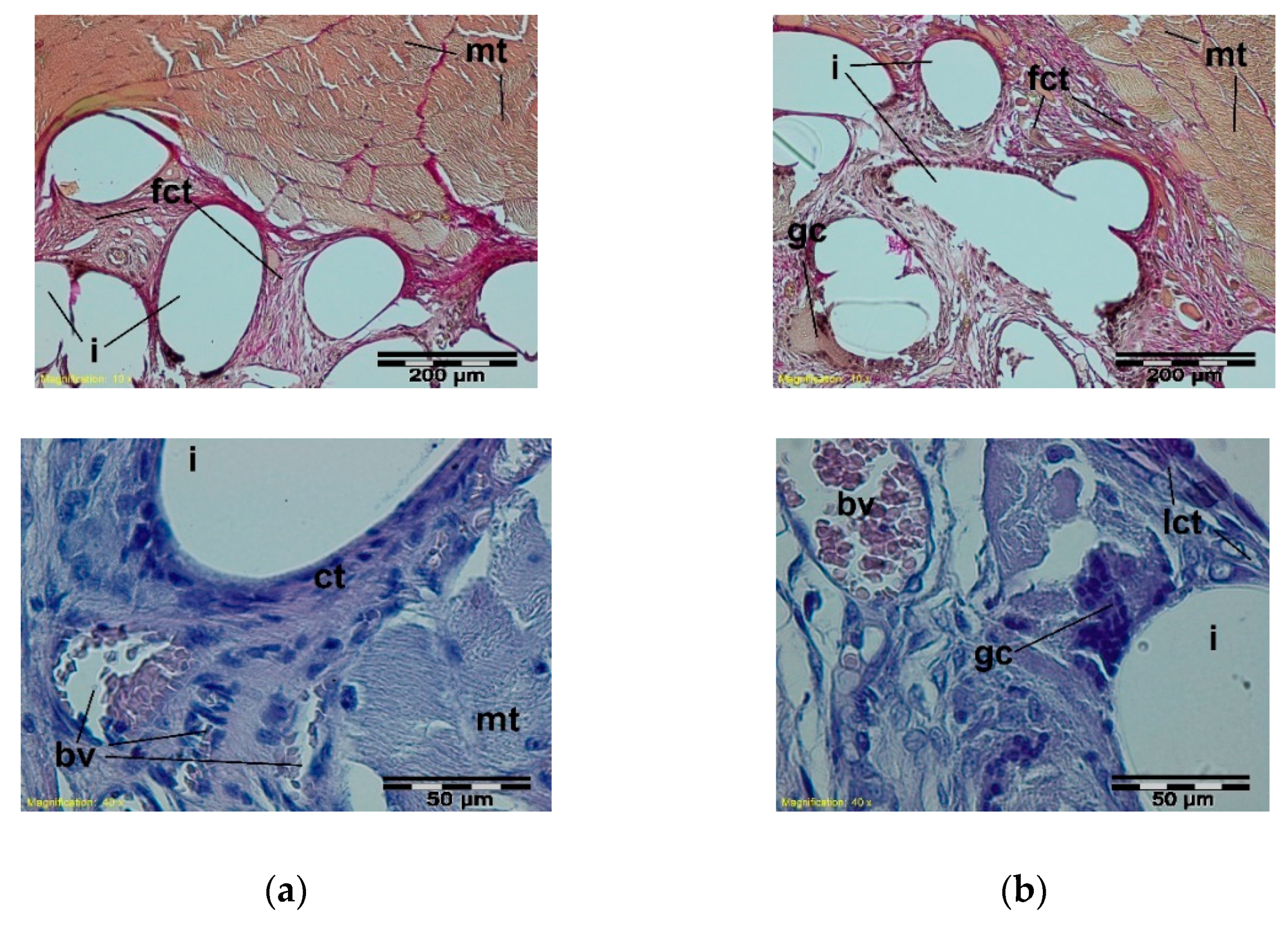
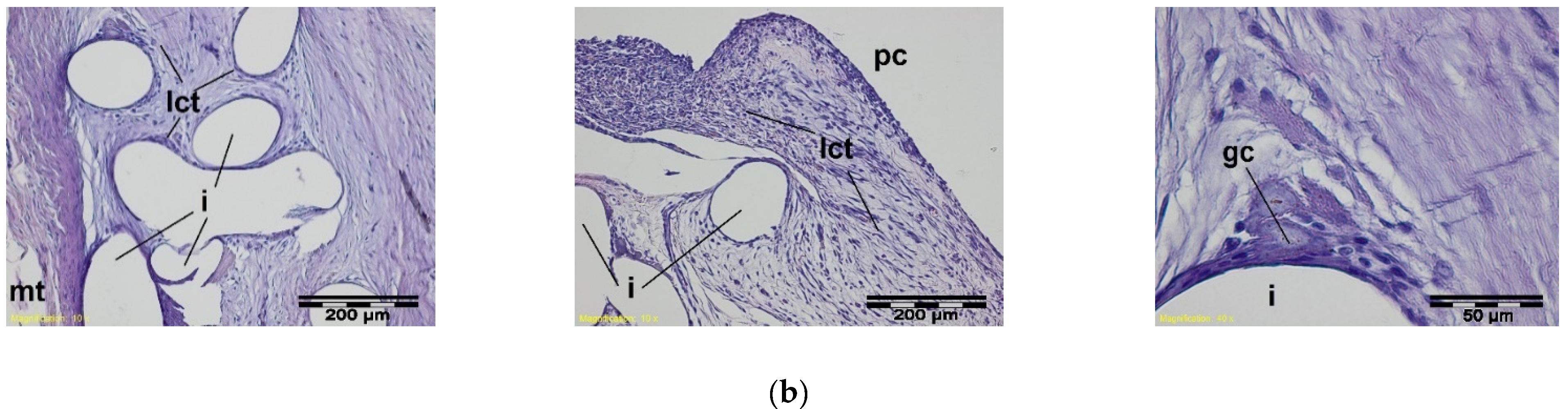
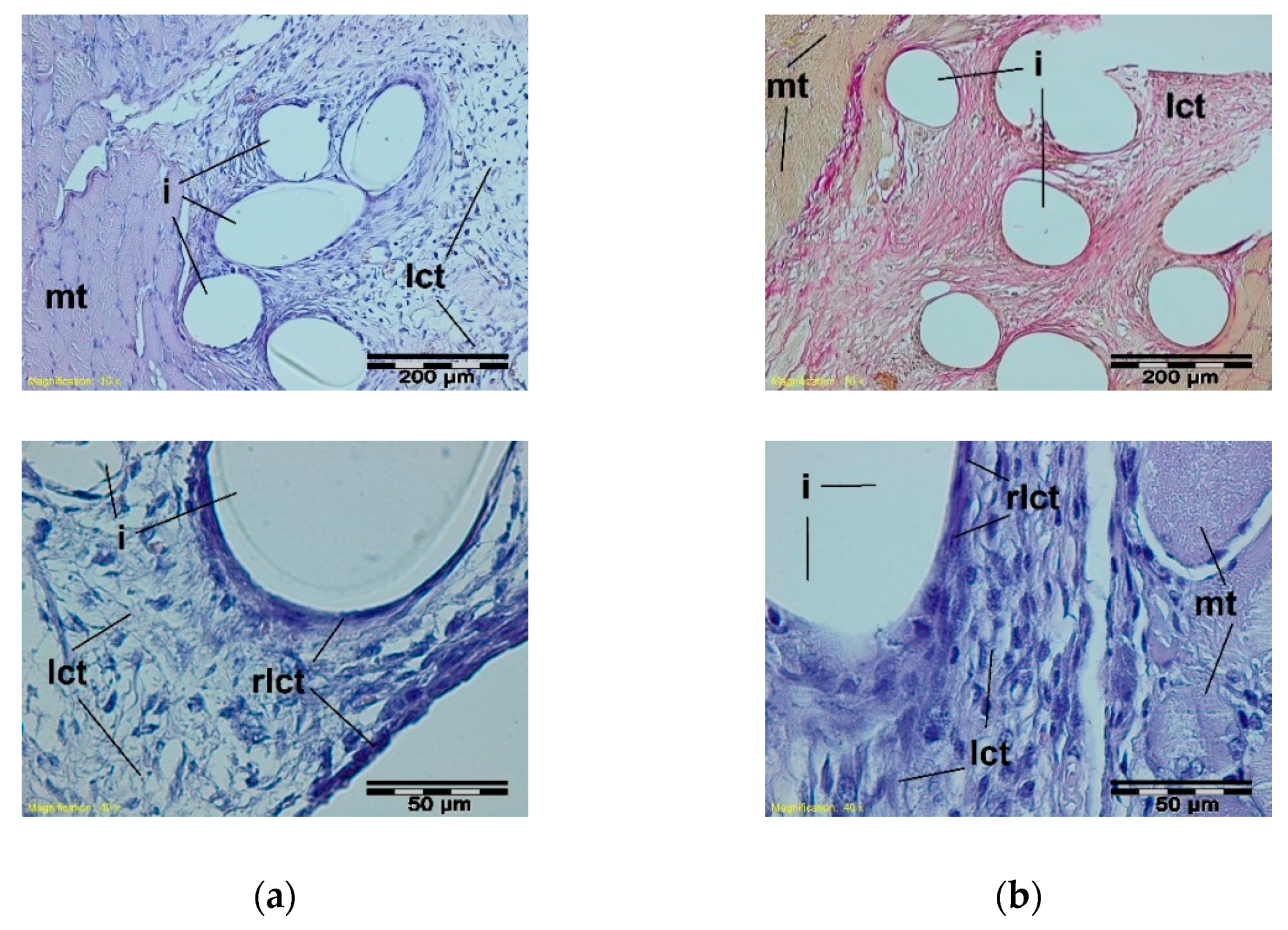
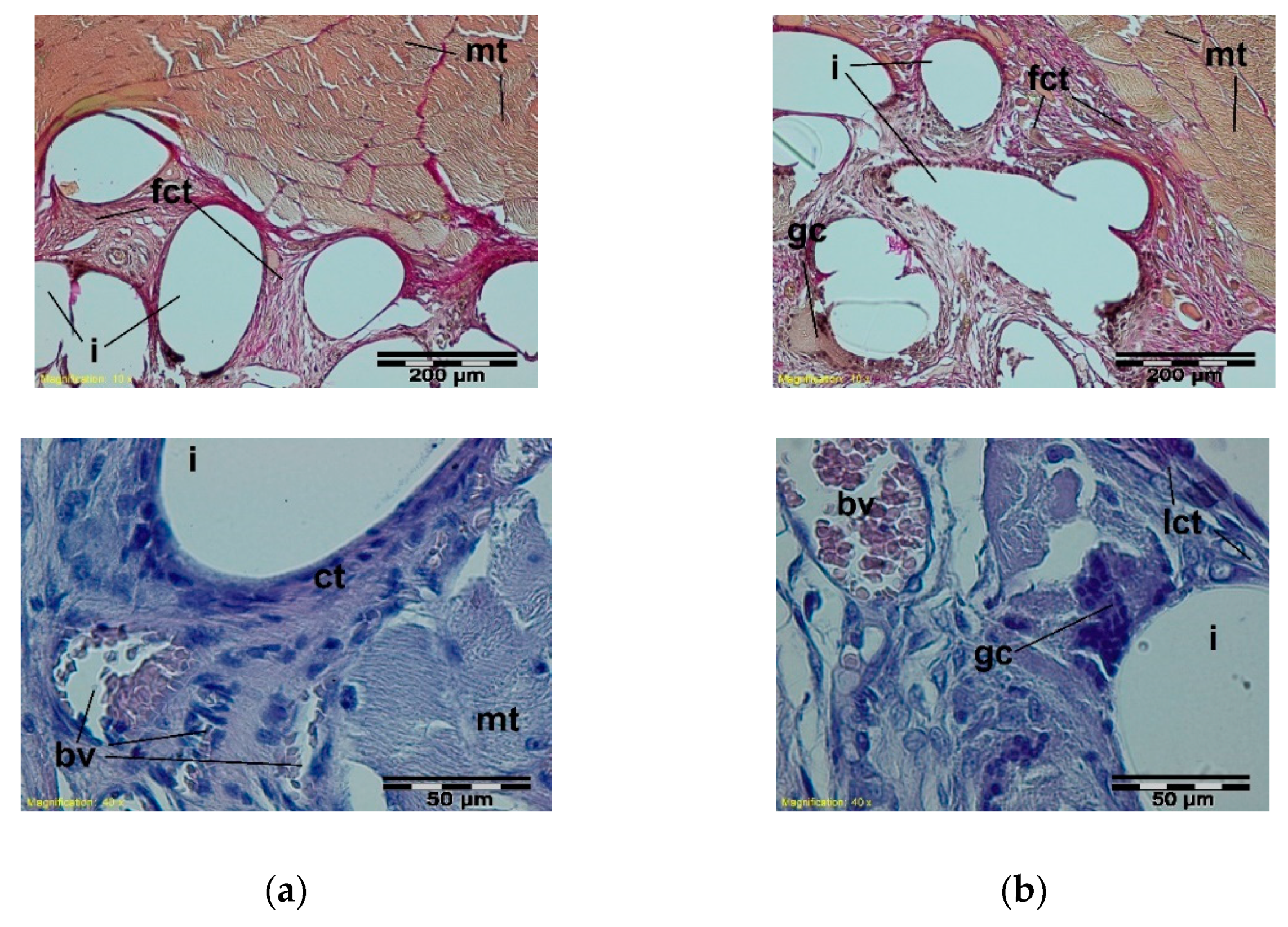
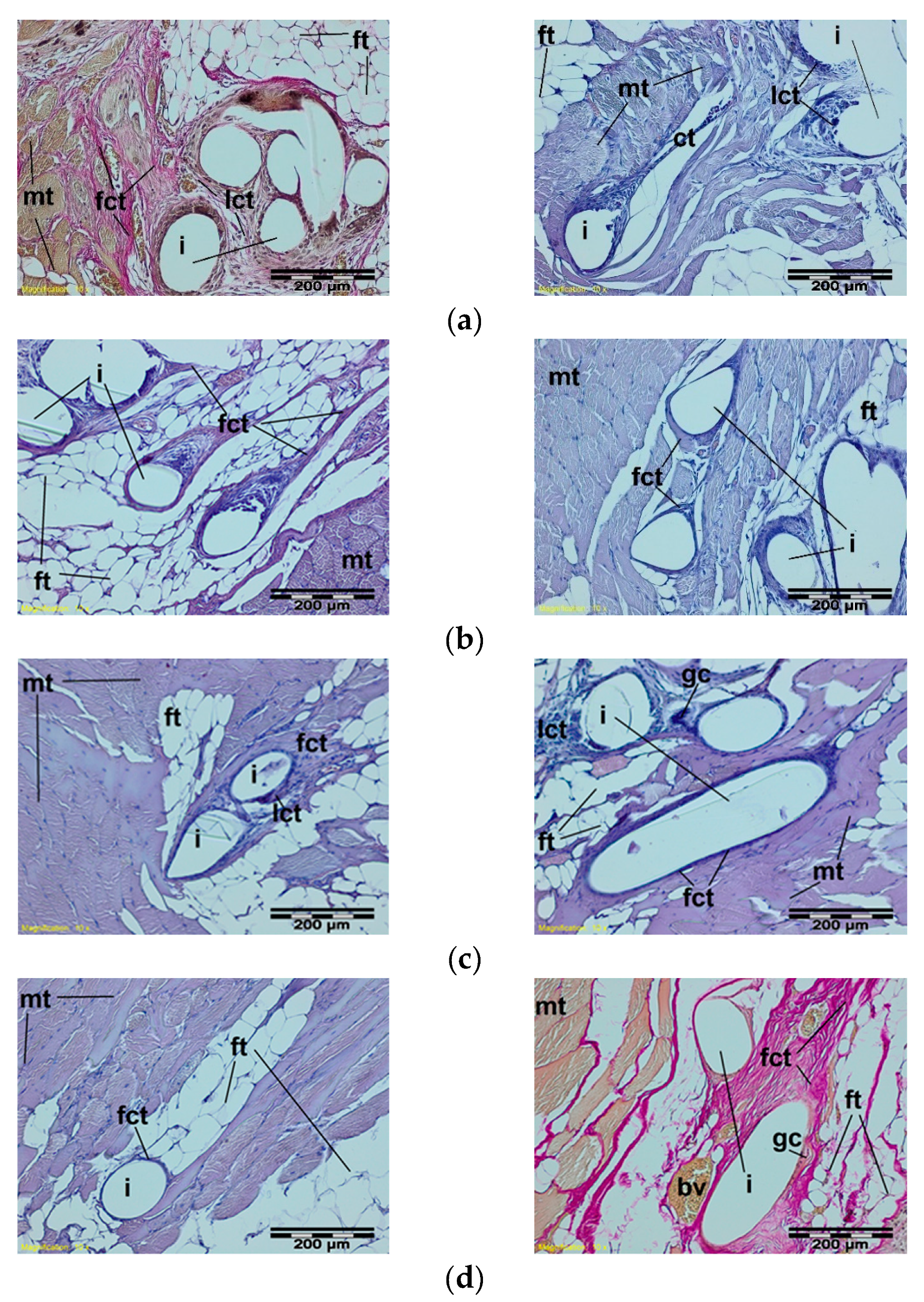
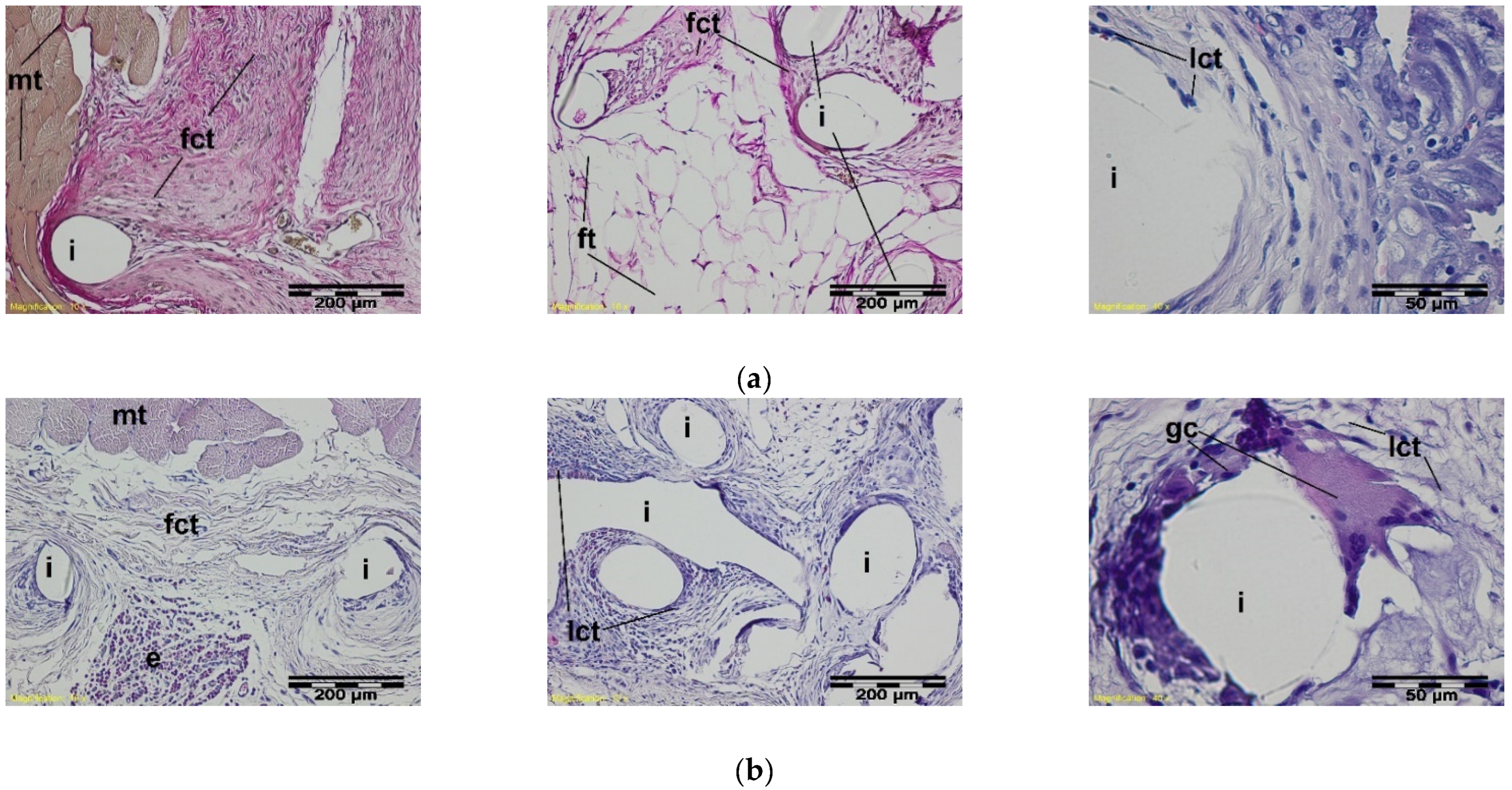
3.1. Study of the Local Effect after Implanting the Knitted Implants within the Muscles
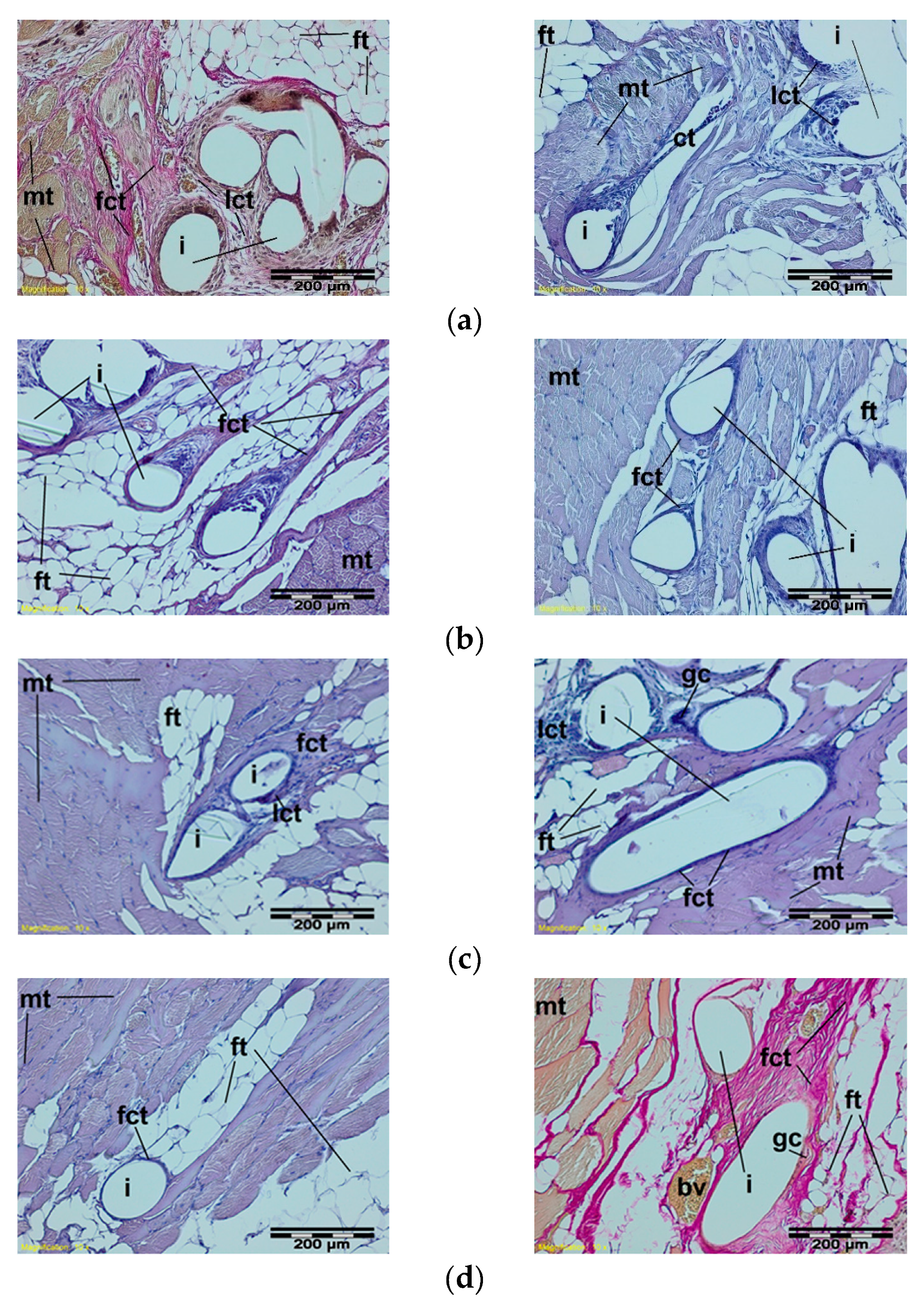
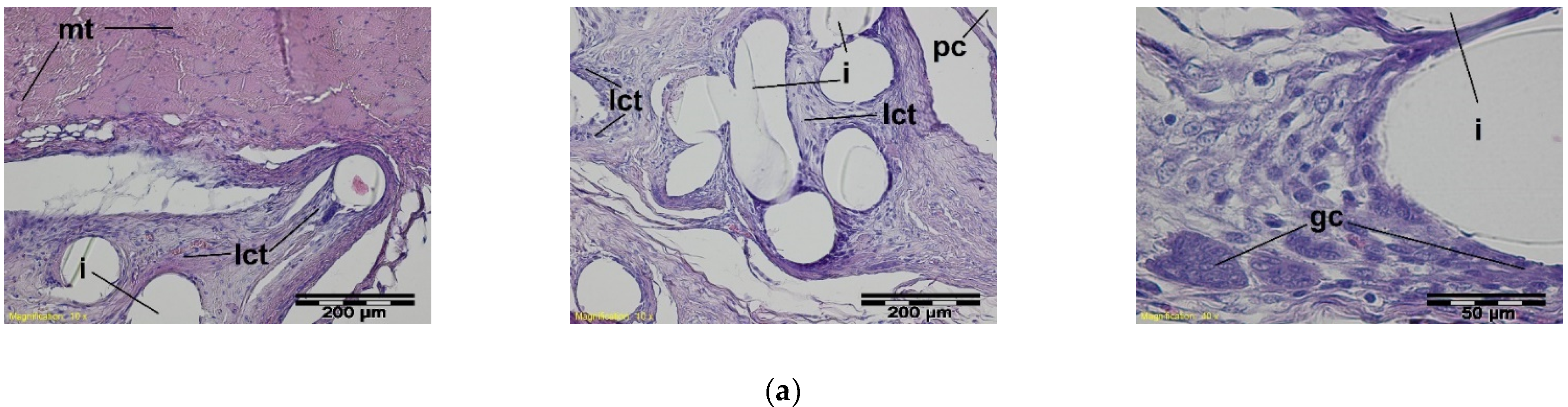
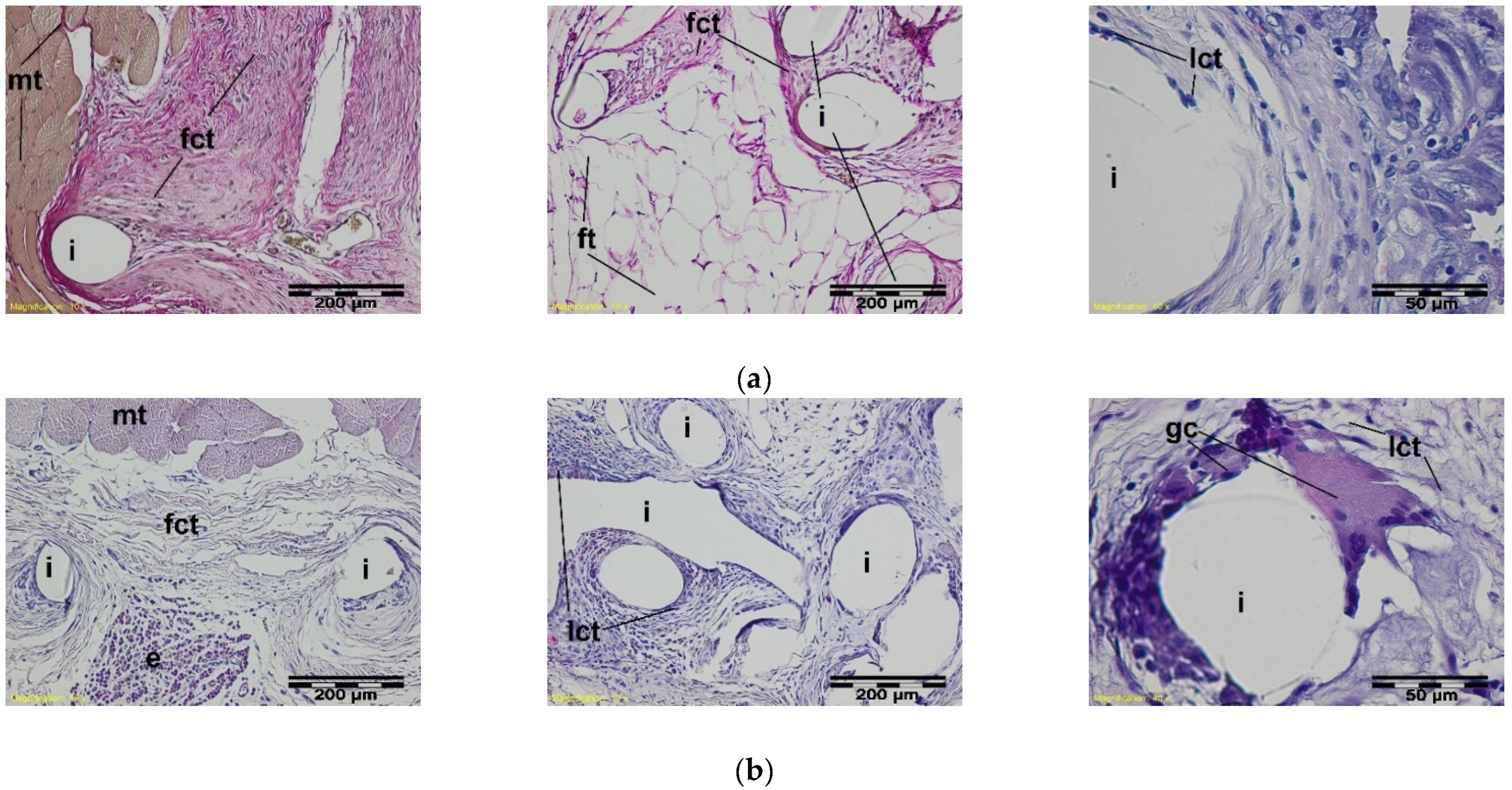
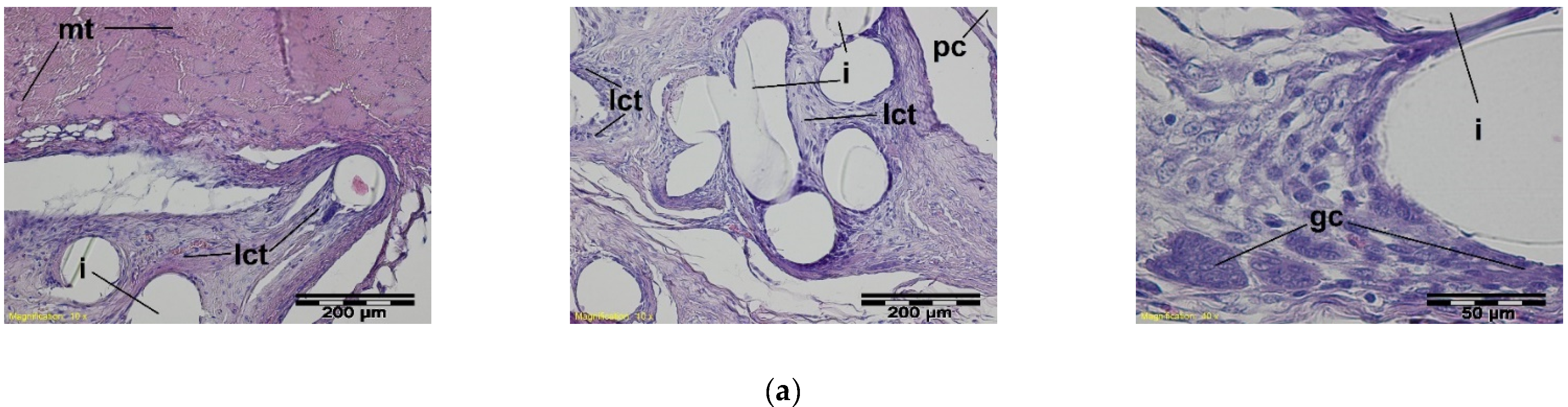
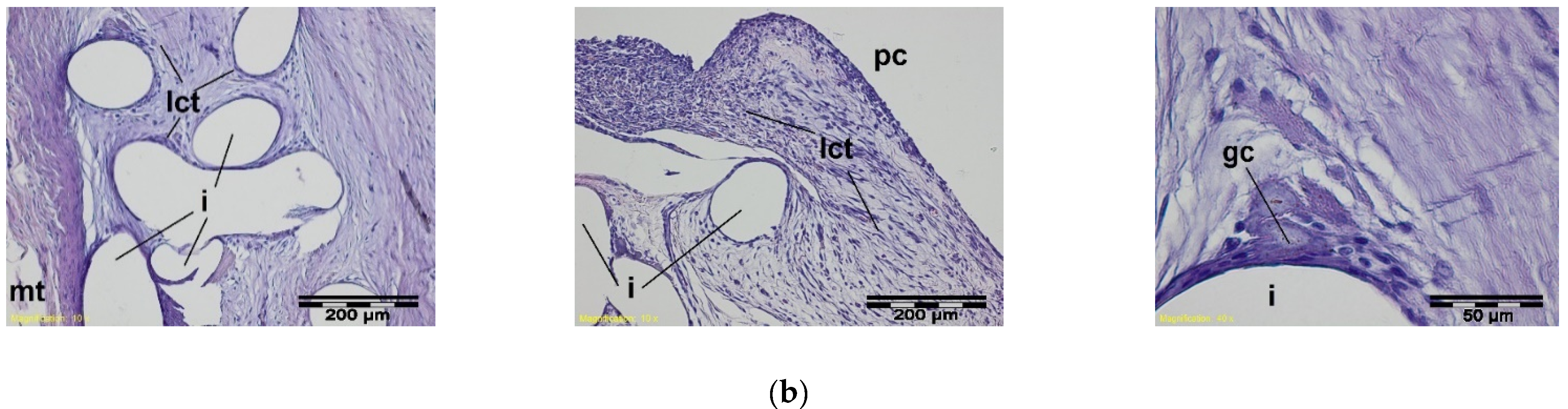
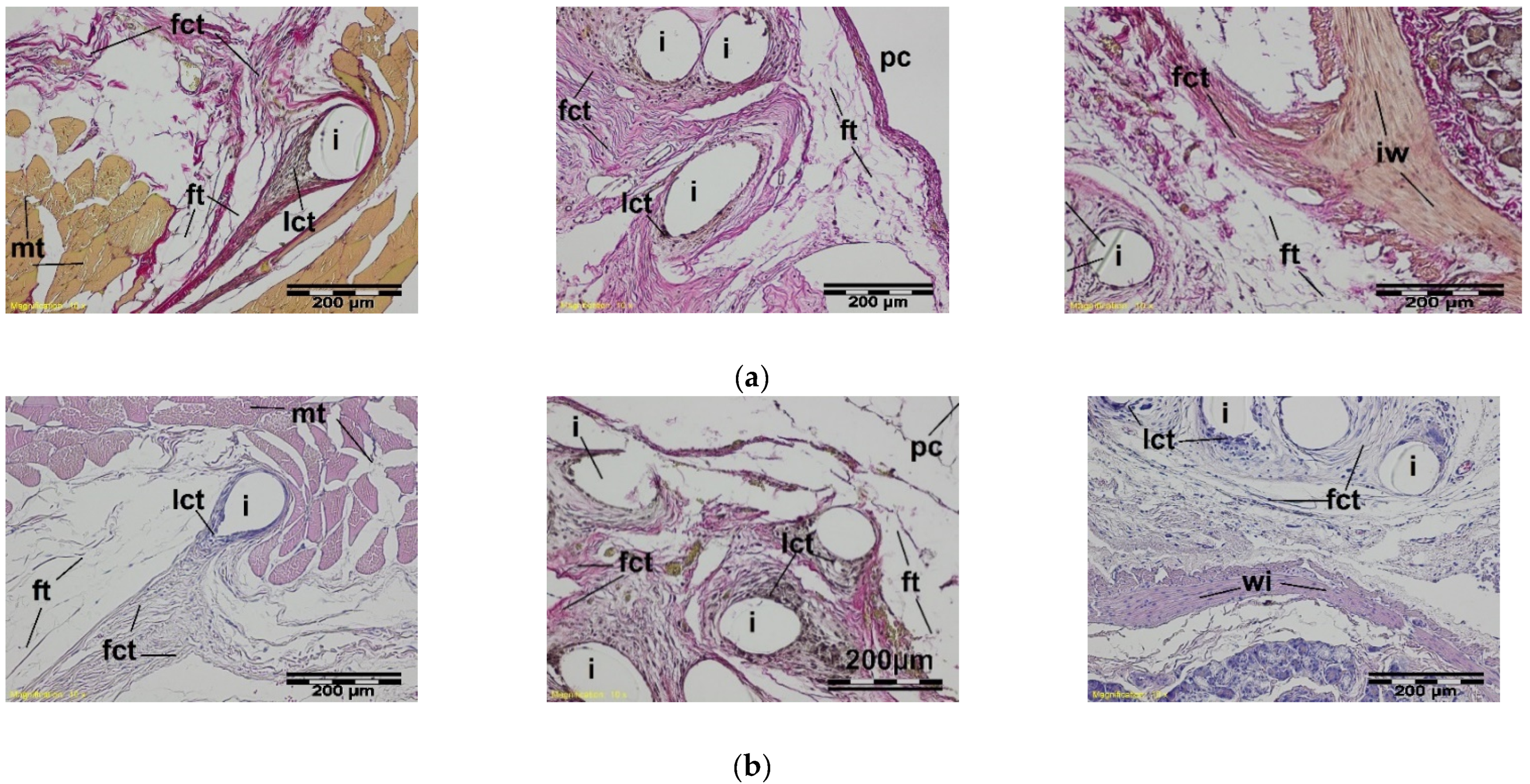
3.2. Study of the Local Effect after Intra-abdominal Implantation of the Knitted Implants
- -
- 2 weeks after the intra-abdominal implantation—0 points;
- -
- 4 weeks after the intra-abdominal implantation—(−1.4) points;
- -
- 12 weeks after the intra-abdominal implantation—(−0.6) points.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Otero, J.; Huber, A.T.; Heniford, B.T. Laparoscopic Hernia Repair. Adv. Surg. 2019, 53, 1–19. [Google Scholar] [CrossRef]
- Corthals, S.; van Cleven, S.; Uyttebroek, O.; de Carvalho, A.; Vanlander, A.; Berrevoet, F. Quality of Life After Open Versus Laparoscopic Preperitoneal Mesh Repair for Unilateral Inguinal Hernias. Asian J. Surg. 2021, 44, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Ma, P. Mechanical Properties of Warp-Knitted Hernia Repair Mesh with Various Boundary Conditions. J. Mech. Behav. Biomed. Mater. 2021, 114, 104192. [Google Scholar] [CrossRef] [PubMed]
- Turlakiewicz, K.; Puchalski, M.; Krucinska, I.; Sujka, W. The Role of Mesh Implants in Surgical Treatment of Parastomal Hernia. Materials 2021, 14, 1062. [Google Scholar] [CrossRef] [PubMed]
- Bendavid, R.; Abrahamson, J.; Arregui, M.E.; Flament, J.B.; Phillips, E.H. Abdominal Wall Hernias: Principles And Management; Springer: Cham, Switzerland, 2018; pp. 39–192. [Google Scholar]
- Conze, J.; Klinge, U.; Schumpelick, V. Surgical Treatment: Evidence-Based and Problem-Oriented; Zuckschwerdt Verlag GmbH: Munich, Germany, 2018. [Google Scholar]
- Guillaume, O.; Pérez-Tanoira, R.; Fortelny, R.; Redl, H.; Moriarty, T.F.; Richards, R.G.; Eglin, D.; Petter Puchner, A. Infections Associated with Mesh Repairs of Abdominal Wall Hernias: Are Antimicrobial Biomaterials the Longed-For Solution? Biomaterials 2018, 167, 15–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Xie, Y.; Zheng, Y.; He, W.; Qiao, W.; Meng, H. Regulatory Science for Hernia Mesh: Current Status and Future Perspectives. Bioact. Mater. 2021, 6, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Houshyar, S.; Sarker, A.; Jadhav, A.; Kumar, G.S.; Bhattacharyya, A.; Nayak, R.; Shanks, R.A.; Saha, T.; Rifai, A.; Padhye, R.; et al. Polypropylene-Nanodiamond Composite for Hernia Mesh. Mater. Sci. Eng. C 2020, 111, 110780. [Google Scholar] [CrossRef] [PubMed]
- Haigh, J.N.; Dargaville, T.R.; Dalton, P.D. Additive Manufacturing with Polypropylene Microfibers. Mater. Sci. Eng. C 2017, 77, 883–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rastegarpour, A.; Cheung, M.; Vardhan, M.; Ibrahim, M.M.; Butler, C.E.; Levinson, H. Surgical Mesh for Ventral Incisional Hernia Repairs: Understanding Mesh Design. Plast. Surg. 2016, 24, 41–50. [Google Scholar] [CrossRef]
- Wang See, C.; Kim, T.; Zhu, D. Hernia Mesh and Hernia Repair: A Review. Eng. Regen. 2020, 1, 19–33. [Google Scholar] [CrossRef]
- Lee, C.H.; Kim, H.; Han, I.W.; Kim, S.M.; Kwak, B.S.; Baik, Y.H.; Park, Y.J.; Oh, M.G. Effect of Polylactic Film (Surgi-Wrap) on Preventing Postoperative Ileus after Major Hepato-Pancreato-Biliary Surgery. Ann. Hepato Biliary Pancreat. Surg. 2016, 20, 191–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niekraszewicz, A.; Kucharska, M.; Struszczyk, M.H.; Rogaczewska, A.; Struszczyk, K. Investigation into Biological, Composite Surgical Meshes. Fibres Text. East. Eur. 2008, 16, 117–121. [Google Scholar]
- Tandon, A.; Shahzad, K.; Pathak, S.; Oommen, C.M.; Nunes, Q.M.; Smart, N. PARIETEX™ Composite Mesh Versus Dynamesh(®)-Ipom for Laparoscopic Incisional and Ventral Hernia Repair: A Retrospective Cohort Study. R. Coll. Surg. Engl. 2016, 98, 568–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikugawa, R.; Tsujinaka, S.; Tamaki, S.; Takenami, T.; Maemoto, R.; Fukuda, R.; Toyama, N.; Rikiyama, T. Successful Mesh Plug Repair Using a Hybrid Method for Recurrentinguinal Hernia after Laparoscopic Transabdominal Preperitoneal Approach: A Case Report. Int. J. Surg. Case Rep. 2019, 59, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Corduas, F.; Lamprou, D.A.; Mancuso, E. Next-Generation Surgical Meshes for Drug Delivery and Tissue Engineering Applications: Materials, Design And Emerging Manufacturing Technologies. Bio Design Manuf. 2021, 4, 278–310. [Google Scholar] [CrossRef]
- Kishor, R.J.; Kuppan, C.T.; Narayanan, C.D.; Vishnu, S. Laparoscopic Management of Mesh Migration into Urinary Bladder Following Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair—A Case Report. Int. J. Surg. Case Rep. 2021, 78, 401–404. [Google Scholar]
- Winsnes, A.; Haapamäki, M.M.; Gunnarsson, U.; Strigård, K. Surgical Outcome Of Mesh And Suture Repair In Primary Umbilical Hernia: Postoperative Complications And Recurrence. Hernia 2016, 20, 509–516. [Google Scholar] [CrossRef]
- Husain, S.G.; Cataldo, T.E. Late Stomal Complications. Clin. Colon Rectal Surg. 2008, 21, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, A.K. Surgical Perspectives Regarding Application of Biomaterials for the Management of Large Congenital Diaphragmatic Hernia Defects. Pediatric Surg. Int. 2018, 34, 475–489. [Google Scholar] [CrossRef]
- Grenadyorov, A.S.; Zhulkov, M.O.; Solovyev, A.A.; Oskomov, K.V.; Semenov, V.A.; Chernyavskiy, A.M.; Sirota, D.A.; Karmadonova, N.A.; Malashchenko, V.V.; Litvinova, L.S.; et al. Surface characterization and biological assessment of corrosion-resistant a-C:H:SiOx PACVD coating for Ti-6Al-4V alloy. Mater. Sci. Eng. C 2021, 123, 112002. [Google Scholar] [CrossRef]
- Grenadyorov, A.S.; Solovyev, A.A.; Ivanov, N.M.; Zhulkov, M.O.; Chernyavskiy, A.M.; Malashchenko, V.V.; Khlusov, A. Enhancement of the adhesive strength of antithrombogenic and hemocompatible a-C:H:SiOx films to polypropylene. Surf. Coat. Technol. 2020, 399, 126132. [Google Scholar] [CrossRef]
- Ghorbani, H.; Abdollah-zadeh, A.; Bagheri, F.; Poladi, A. Improving the bio-corrosion behavior of AISI316L stainless steel through deposition of Ta-based thin films using PACVD. Appl. Surf. Sci. 2018, 456, 398–402. [Google Scholar] [CrossRef]
- Yin, P.; Wei, X.; Shang, L.; Lu, Z.; Zhang, G. Design of low-friction and anti-corrosion a-C:H:SiOx films. Diam. Relat. Mater. 2021, 118, 108512. [Google Scholar] [CrossRef]
- He, W.; Cao, G.; Gan, X.; Fan, F.; Pei, B.; Li, X. Evaluation Methods for Mechanical Biocompatibility of Hernia Repair Meshes: Respective Characteristics, Application Scope and Future Perspectives. J. Mater. Res. Technol. 2021, 13, 1826–1840. [Google Scholar] [CrossRef]
- Struszczyk, M.H.; Gutowska, A.; Kowalski, K.; Kopias, K.; Pałys, B.; Komisarczyk, A.; Krucińska, I. Ultra-Light Knitted Structures for Application in Urologinecology and General Surgery—Optimisation of Structure in the Aspect of Physical Parameters. Fibres Text. East. Eur. 2011, 5, 92–98. [Google Scholar]
- Struszczyk, M.H.; Komisarczyk, A.; Krucińska, I. Ultra-Light Knitted Structures for Application in Urologinecology and General Surgery—Optimization of Structure. In Proceedings of FiberMed; Electronic Publishing: Tampere, Finland, 2011; Volume 11. [Google Scholar]
- Struszczyk, M.H.; Gutowska, A.; Pałys, B.; Cichecka, M.; Kostanek, K.; Wilbik-Hałgas, B.; Kowalski, K.; Kopias, K.; Krucińska, I. Accelerated Ageing of The Implantable, Ultra-Light, Knitted Medical Devices Modified by Low-Temperature Plasma Treatment—Part 1. Effects on the Physical Behaviour. Fibres Text. East. Eur. 2012, 6B, 121–127. [Google Scholar]
- Jozwicka, J.; Gzyra-Jagiela, K.; Struszczyk, M.H.; Gutowska, A.; Ciechańska, D.; Krucińska, I. Aspects of Chemical Characterisation of Leachables Profile from Ultra-Light Knitting Textiles for Uses as Medical Implants in Urogynaecology and General Surgery. Fibres Text. East. Eur. 2012, 6B, 128–134. [Google Scholar]
- Jozwicka, J.; Gzyra-Jagieła, K.; Gutowska, A.; Struszczyk, M.H.; Kostanek, K.; Cichecka, M.; Hałgas, B.; Kowalski, K.; Kopias, K.; Ciechańska, D.; et al. Accelerated Ageing of Implantable, Ultra-Light, Knitted Medical Devices Modified by Low-Temperature Plasma Treatment—Part 2. Effect on chemical purity. Fibres Text. East. Eur. 2014, 22, 133–139. [Google Scholar]
- Struszczyk, M.H.; Komisarczyk, A.; Krucinska, I.; Gutowska, A.; Pałys, B.; Ciechańska, D. Biomechanical Studies Of Novel Hernia Meshes With Enhanced Surface Behaviour. Fibres Text. East. Eur. 2014, 22, 129–134. [Google Scholar]
- Kostanek, K.; Struszczyk, M.H.; Chrzanowski, M.; Żywicka, B.; Paluch, D.; Szadkowski, M.; Gutowski, A.; Krucińska, I. Assessment of Modified Knitted Hernia Implants after Implantation: I. Biological Effect on the Structural and Usable Properties. Fibres Text. East. Eur. 2013, 21, 79–83. [Google Scholar]
- Garrard, C.L.; Clements, R.H.; Nanney, L.; Davidson, J.M.; Richards, W.O. Adhesion Formation Is Reduced after Laparoscopic Surgery. Surg. Endosc. 1999, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Kopias, K.; Golczyk, A.; Kowalski, K.; Struszczyk, M.H. Knitted Implant for Reconstruction of Connective Tissue Defects. Polish Patent 22221018, 20 April 2011. [Google Scholar]
- Kostanek, K.; Struszczyk, M.H.; Krucińska, I.; Urbaniak-Domagała, W.; Puchalski, M. Method of Modification of Three-Dimensional Implant for Curing Hernias in Low-Invasive Surgeries. Polish Patent Application P-395988, 17 August 2011. [Google Scholar]
- Gocławski, J.; Urbaniak-Domagała, W. The Measurement of Wetting Angle by Applying an ADSA Model of Sessile Drop on Selected Textile Surfaces. Fibres Text. East. Eur. 2008, 16, 84–88. [Google Scholar]
- Kostanek, K.; Struszczyk, M.H.; Domagała, W.; Krucińska, I. Surface Modification of the Implantable Knitted Structures for Potential Application in Laparoscopic Hernia Treatments. In Proceedings of FiberMed; Electronic Publishing: Tampere, Finlandia, 2011; Volume 11, pp. 28–30. ISBN 978-952-15-2607-7. [Google Scholar]
- Struszczyk, M.H.; Miklas, M.; Cichecka, M.; Wilbik-Hałgas, B.; Łandwijt, M.; Litwa, P.; Grabowska, G.; Błaszczyk, J.; Pawłowska, A.; Fejdyś, M.; et al. Research on the Functionalisation of Ballistic Materials—Optimisation of the Functionalisation Process. In Advanced Technologies And Materials In State Security; Struszczyk, M.H., Ed.; MORATEX: Lodz, Poland, 2018; pp. 63–128. ISBN 9788395166808. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Test Method | Reference Sample | PACVD Modified Prototype (Evaluated Sample) |
|---|---|---|---|
| Surface density (g/m2) | PN-EN 12127:2000 | 45.9 ± 0.8 | 46.1 ± 1.5 |
| Thickness (mm) | PN-EN ISO 5084:1999 | 1.08 ± 0.09 | 1.10 ± 0.01 |
| Longitudinal tensile strength (N) | PN-EN ISO13934-1:2002 | 114 ± 10.1 | 89.0 ± 23.7 |
| Vertical tensile strength (N) | 103.0 ± 8.8 | 110.0 ± 12.8 | |
| Longitudinal elongation (%) | 56.1 ± 12.4 | 76.4 ± 8.6 | |
| Vertical elongation (%) | 72.0 ± 5.2 | 62.7 ± 8.7 | |
| Longitudinal initial elasticity modulus (MPa) | 4.66 | 0.96 | |
| Vertical initial elasticity modulus (MPa) | 2.66 | 2.4 | |
| Bursting Strength (N) | PN-EN ISO 12236:2007 1 | 584.0 ± 53.8 | 564.0 ± 26.1 |
| Suture pullout in the corner (N) | ISO 7198:1998 2 | 20.7 ± 2.6 | 21.7 ± 3.8 |
| Fluorine content onto the surface (%) | determined by SEM-EDS | - | 4.98 |
| Crystallinity index (%) | determined by WAXS | 61.2 | 58.8 |
| Wetting angle (o) | [37] | 113 ± 8 | 143 ± 12 |
| Score (Difference in Score of the Tested Sample and the Reference) | Evaluation |
|---|---|
| 0–2.9 | No irritation |
| 3.0–8.9 | Slight irritation |
| 9.0–15.0 | Medium irritation |
| >15.1 | Strong irritation |
| Criteria | |||||
|---|---|---|---|---|---|
| Adhesion Quality (x1) | Adhesion Area (x2) | Mode of the Implant Covering (x3) | |||
| Absence | 0 | 0–20% of implant area | 0 | Absence | 0 |
| The place of the adhesion can be lightly removed | 1 | 20–45% of implant area | 1 | Point-to-point area | 1 |
| The place of the adhesion can be removed using additional strength (aggressive separation) | 2 | 45–70% of implant area | 2 | Multipoint adhesion in several places onto the implant | 2 |
| The place of the adhesion can be removed using sharp tools (by cutting) | 3 | >70% of implant area | 3 | Full adhesion | 3 |
| Importance (w1) | 1 | Importance (w2) | 2 | Importance (w3) | 1 |
| Time of the Implantation (Week) | Score 1 | Evaluation |
|---|---|---|
| 1 | 2.60 | No irritation |
| 3 | 2.42 | No irritation |
| 9 | −2.71 | No irritation |
| 12 | 2.99 | No irritation |
| 26 | −2.05 | No irritation |
| 56 | −2.71 | No irritation |
| Reference | PACVD Modified Knitted Implant | |||||
|---|---|---|---|---|---|---|
| Adhesion Quality | Adhesion Area | Mode of the Implant Covering | Adhesion Quality | Adhesion Area | Mode of the Implant Covering | |
| 2 | 0 | 2 | 3 | 0 | 2 | |
| 2 | 3 | 2 | 2 | 3 | 2 | |
| 2 | 0 | 2 | 2 | 3 | 2 | |
| 2 | 3 | 2 | 2 | 0 | 2 | |
| 2 | 2 | 2 | 2 | 2 | 2 | |
| Summary | 10 | 8 | 10 | 11 | 8 | 10 |
| Average | 2.0 | 1.6 | 2.0 | 2.2 | 1.6 | 2.0 |
| Sa1 | 0 | |||||
| Importance | 1 | 2 | 1 | 1 | 2 | 1 |
| Weighted average | 1.8 | 2.0 | ||||
| Sa2 | 0.20 | |||||
| Reference | PACVD-Modified Knitted Implant | |||||
|---|---|---|---|---|---|---|
| Adhesion Quality | Adhesion Area | Mode of the Implant Covering | Adhesion Quality | Adhesion Area | Mode of the Implant Covering | |
| 2 | 1 | 2 | 1 | 1 | 2 | |
| 1 | 1 | 2 | 2 | 0 | 1 | |
| 2 | 3 | 3 | 2 | 1 | 3 | |
| 2 | 3 | 3 | 2 | 1 | 3 | |
| 2 | 3 | 3 | 2 | 1 | 2 | |
| Summary | 9 | 11 | 13 | 9 | 4 | 11 |
| Average | 1.8 | 2.2 | 2.6 | 1.8 | 0.8 | 2.2 |
| Sa1 | −1.4 | |||||
| Importance | 1 | 2 | 1 | 1 | 2 | 1 |
| Weighted average | 2.2 | −1.4 | ||||
| Sa2 | −0.8 | |||||
| Reference | PACVD-Modified Knitted Implant | |||||
|---|---|---|---|---|---|---|
| Adhesion Quality | Adhesion Area | Mode of the Implant Covering | Adhesion Quality | Adhesion Area | Mode of the Implant Covering | |
| 3 | 1 | 3 | 3 | 0 | 3 | |
| 3 | 1 | 3 | 3 | 1 | 3 | |
| 3 | 3 | 2 | 3 | 0 | 2 | |
| 3 | 2 | 2 | 2 | 2 | 2 | |
| 2 | 1 | 3 | 2 | 2 | 2 | |
| Summary | 14 | 8 | 13 | 13 | 5 | 12 |
| Average | 2.8 | 1.6 | 2.6 | 2.6 | 1.0 | 2.4 |
| Sa1 | −0.6 | |||||
| Importance | 1 | 2 | 1 | 1 | 2 | 1 |
| Weighted average | 1.8 | 1.5 | ||||
| Sa2 | −0.3 | |||||
| Time of the Implantation (Week) | Score 1 | Evaluation |
|---|---|---|
| 2 | 1.79 | No irritation |
| 4 | −3.33 | No irritation |
| 12 | −2.01 | No irritation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Żywicka, B.; Struszczyk, M.H.; Paluch, D.; Kostanek, K.; Krucińska, I.; Kowalski, K.; Kopias, K.; Rybak, Z.; Szymonowicz, M.; Gutowska, A.; et al. Design of New Concept of Knitted Hernia Implant. Materials 2022, 15, 2671. https://doi.org/10.3390/ma15072671
Żywicka B, Struszczyk MH, Paluch D, Kostanek K, Krucińska I, Kowalski K, Kopias K, Rybak Z, Szymonowicz M, Gutowska A, et al. Design of New Concept of Knitted Hernia Implant. Materials. 2022; 15(7):2671. https://doi.org/10.3390/ma15072671
Chicago/Turabian StyleŻywicka, Bogusława, Marcin Henryk Struszczyk, Danuta Paluch, Krzysztof Kostanek, Izabella Krucińska, Krzysztof Kowalski, Kazimierz Kopias, Zbigniew Rybak, Maria Szymonowicz, Agnieszka Gutowska, and et al. 2022. "Design of New Concept of Knitted Hernia Implant" Materials 15, no. 7: 2671. https://doi.org/10.3390/ma15072671
APA StyleŻywicka, B., Struszczyk, M. H., Paluch, D., Kostanek, K., Krucińska, I., Kowalski, K., Kopias, K., Rybak, Z., Szymonowicz, M., Gutowska, A., & Kubiak, P. (2022). Design of New Concept of Knitted Hernia Implant. Materials, 15(7), 2671. https://doi.org/10.3390/ma15072671