
Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy

 , ,
, ,
Abstract
:1. Introduction
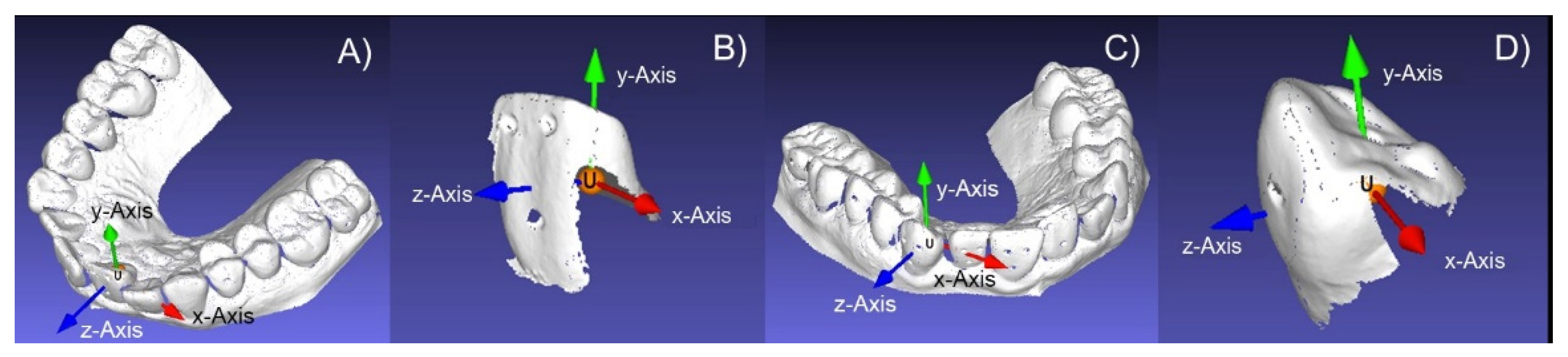
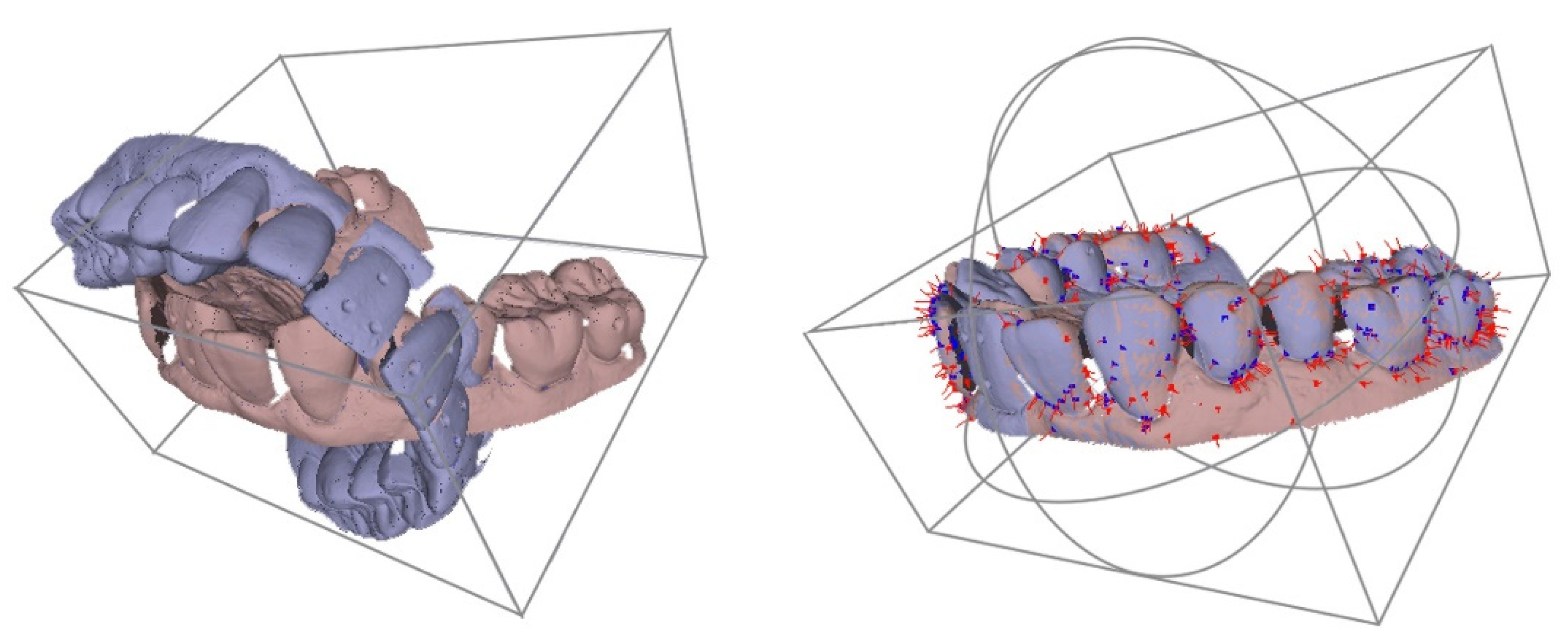
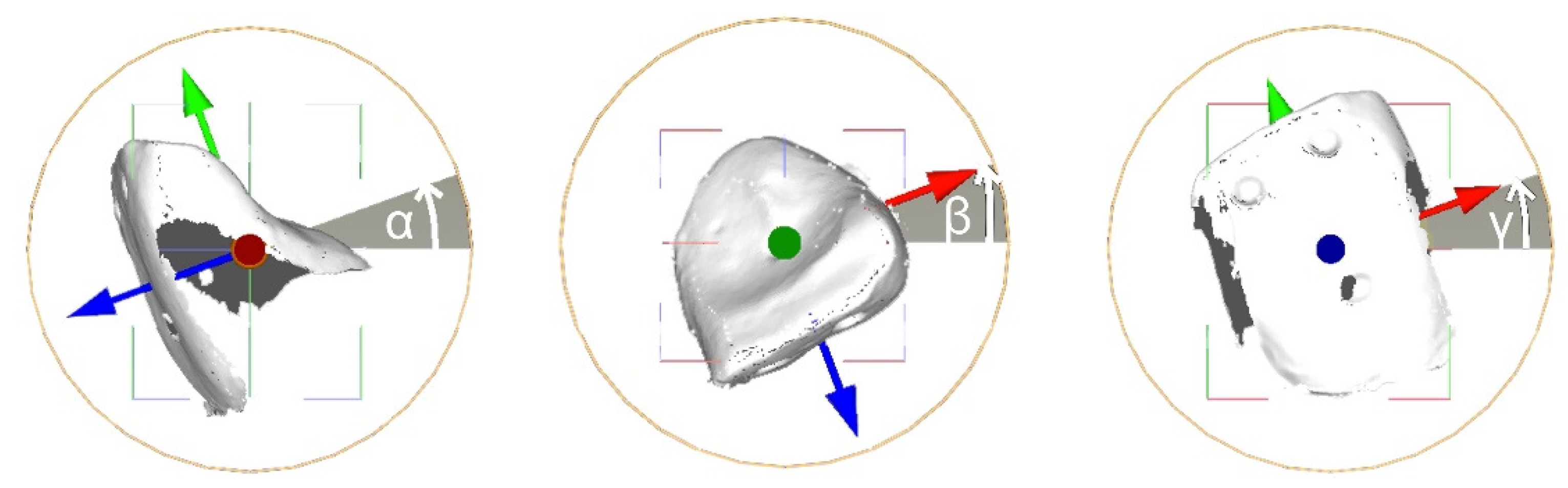
2. Materials and Methods
3. Results
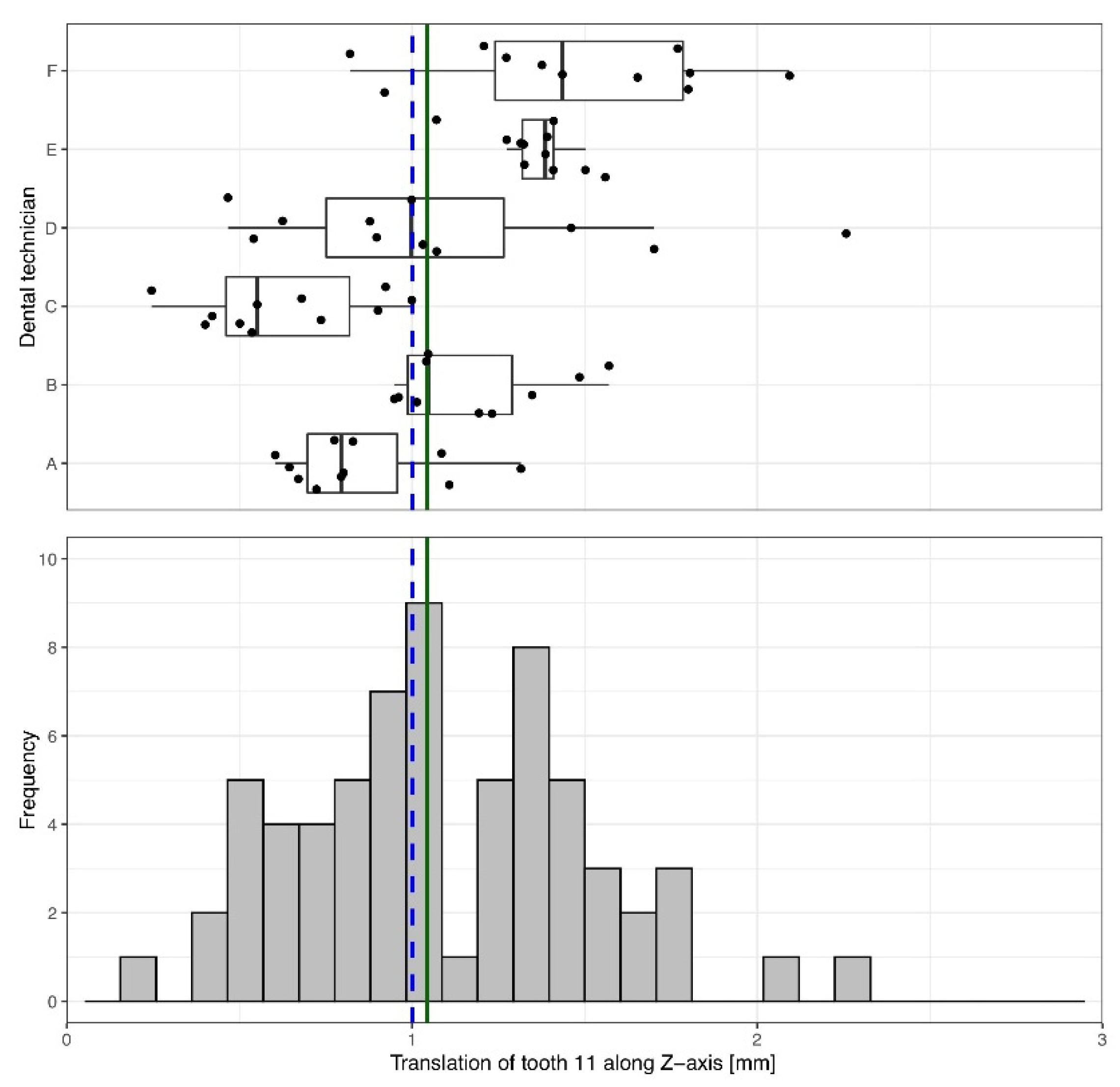
3.1. Orovestibular Translation of Tooth 11, 1 mm Vestibular
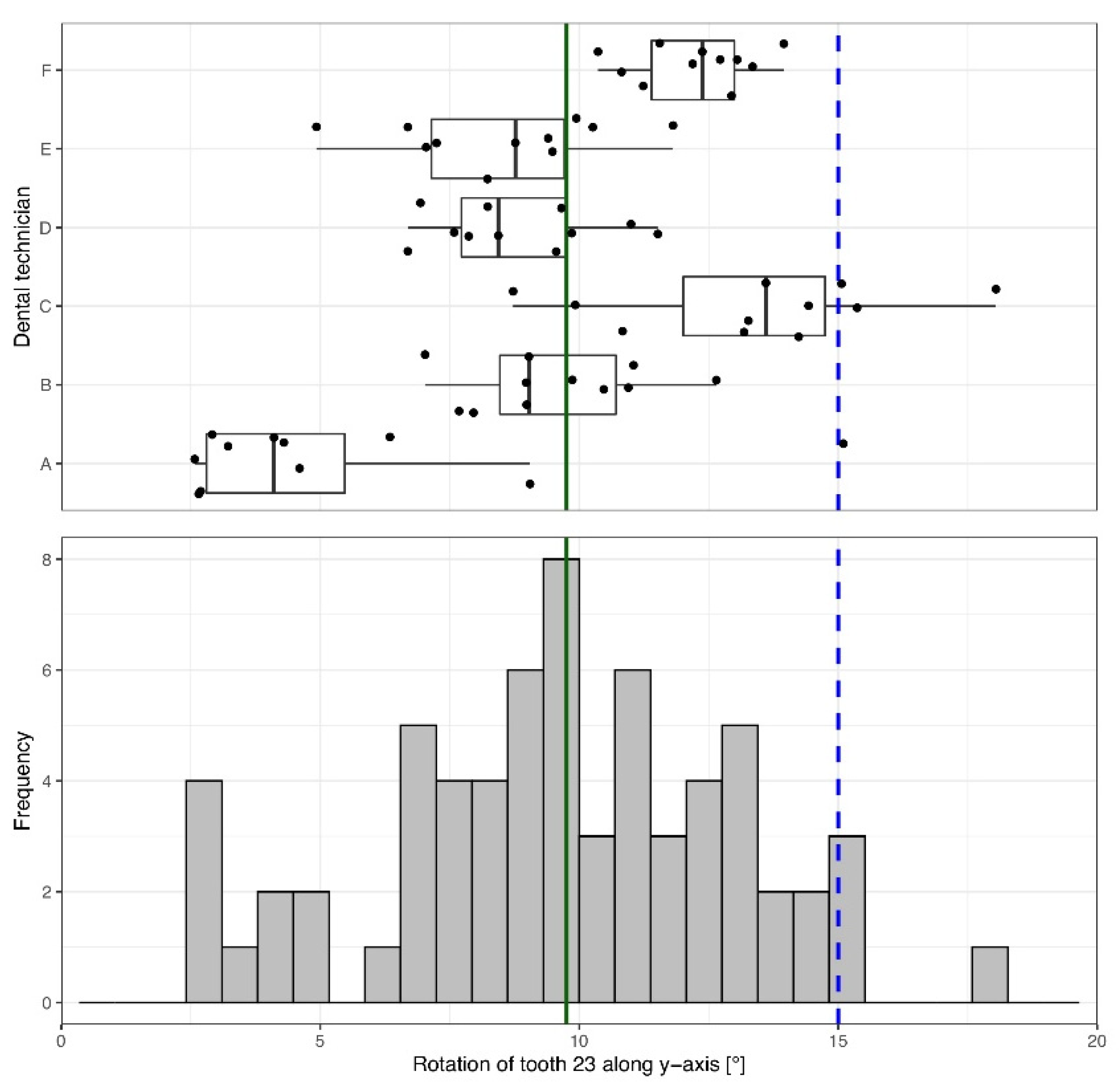
3.2. Mesio-Rotation Tooth 23, 15°
4. Discussion
5. Clinical Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Buschang, P.H.; Shaw, S.G.; Ross, M.; Crosby, D.; Campbell, P.M. Comparative time efficiency of aligner therapy and conventional edgewise braces. Angle Orthod. 2014, 84, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Chisari, J.R.; McGorray, S.P.; Nair, M.; Wheeler, T.T. Variables affecting orthodontic tooth movement with clear aligners. Am. J. Orthod. Dentofac. Orthop. 2014, 145, S82–S91. [Google Scholar] [CrossRef] [PubMed]
- Weir, T. Clear aligners in orthodontic treatment. Aust. Dent. J. 2017, 62 (Suppl. 1), 58–62. [Google Scholar] [CrossRef] [Green Version]
- Zheng, M.; Liu, R.; Ni, Z.; Yu, Z. Efficiency, effectiveness and treatment stability of clear aligners: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2017, 20, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Rossini, G.; Parrini, S.; Castroflorio, T.; Deregibus, A.; Debernardi, C.L. Efficacy of clear aligners in controlling orthodontic tooth movement: A systematic review. Angle Orthod. 2015, 85, 881–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, M.; Keilig, L.; Schwarze, J.; Jung, B.A.; Bourauel, C. Treatment outcome and efficacy of an aligner technique–regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014, 14, 68. [Google Scholar] [CrossRef] [Green Version]
- Kravitz, N.D.; Kusnoto, B.; BeGole, E.; Obrez, A.; Agran, B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 27–35. [Google Scholar] [CrossRef]
- Sterental, R. Staging. In The Invisalign System; Tuncay, O.C., Ed.; Quintessence: New Malden, UK, 2006; pp. 105–113. [Google Scholar]
- Kim, T.W.; Echarri, P. Clear aligner: An efficient, esthetic, and comfortable option for an adult patient. World J. Orthod. 2007, 8, 13–18. [Google Scholar]
- Sheridan, J.J.; Ledoux, W.; McMinn, R. Essix appliance: Minor tooth movement with divots and windows. J. Clin. Orthod. 1994, 28, 659–663. [Google Scholar]
- Barbagallo, L.J.; Shen, G.; Jones, A.S.; Swain, M.V.; Petocz, P.; Darendeliler, M.A. A novel pressure film approach for determining the force imparted by clear removable thermoplastic appliances. Ann. Biomed. Eng. 2008, 36, 335–341. [Google Scholar] [CrossRef] [Green Version]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Buschang, P.H.; Ross, M.; Shaw, S.G.; Crosby, D.; Campbell, P.M. Predicted and actual end-of-treatment occlusion produced with aligner therapy. Angle Orthod. 2015, 85, 723–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Im, J.; Cha, J.Y.; Lee, K.J.; Yu, H.S.; Hwang, C.J. Comparison of virtual and manual tooth setups with digital and plaster models in extraction cases. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Cignoni, P.; Callieri, M.; Corsini, M.; Dellepiane, M.; Ganovelli, F.; Ranzuglia, G. MeshLab: An Open-Source Mesh Processing Tool. In Eurographics Italian Chapter Conference; Scarano, V., De Chiara, R., Erra, U., Eds.; The Eurographics Association: Geneva, Switzerland, 2008; pp. 129–136. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Palone, M.; Longo, M.; Arveda, N.; Nacucchi, M.; Pascalis, F.; Spedicato, G.A.; Siciliani, G.; Lombardo, L. Micro-computed tomography evaluation of general trends in aligner thickness and gap width after thermoforming procedures involving six commercial clear aligners: An in vitro study. Korean J. Orthod. 2021, 51, 135–141. [Google Scholar] [CrossRef]
- Lombardo, L.; Arreghini, A.; Ramina, F.; Huanca Ghislanzoni, L.T.; Siciliani, G. Predictability of orthodontic movement with orthodontic aligners: A retrospective study. Prog. Orthod. 2017, 18, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, E.; Castroflorio, E.; Rossini, G.; Garino, F.; Cugliari, G.; Deregibus, A.; Castroflorio, T. Scanning electron microscopy evaluation of aligner fit on teeth. Angle Orthod. 2018, 88, 596–601. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Shin, Y.S.; Jung, H.D.; Hwang, C.J.; Baik, H.S.; Cha, J.Y. Precision and trueness of dental models manufactured with different 3-dimensional printing techniques. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 144–153. [Google Scholar] [CrossRef] [Green Version]
- Tomita, Y.; Uechi, J.; Konno, M.; Sasamoto, S.; Iijima, M.; Mizoguchi, I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent. Mater. J. 2018, 37, 628–633. [Google Scholar] [CrossRef] [Green Version]
- Koenig, N.; Choi, J.Y.; McCray, J.; Hayes, A.; Schneider, P.; Kim, K.B. Comparison of dimensional accuracy between direct-printed and thermoformed aligners. Korean J. Orthod. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Jaber, S.T.; Hajeer, M.Y.; Khattab, T.Z.; Mahaini, L. Evaluation of the fused deposition modeling and the digital light processing techniques in terms of dimensional accuracy of printing dental models used for the fabrication of clear aligners. Clin. Exp. Dent. Res. 2021, 7, 591–600. [Google Scholar] [CrossRef]
- Abduo, J.; Elseyoufi, M. Accuracy of intraoral scanners: A systematic review of influencing factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef] [PubMed]
- Fabels, L.N.; Nijkamp, P.G. Interexaminer and intraexaminer reliabilities of 3-dimensional orthodontic digital setups. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Hahn, W.; Zapf, A.; Dathe, H.; Fialka-Fricke, J.; Fricke-Zech, S.; Gruber, R.; Kubein-Meesenburg, D.; Sadat-Khonsari, R. Torquing an upper central incisor with aligners–acting forces and biomechanical principles. Eur. J. Orthod. 2010, 32, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, L.; Wichelhaus, A. Forces and moments delivered by the PET-G aligner to a maxillary central incisor for palatal tipping and intrusion. Angle Orthod. 2017, 87, 534–541. [Google Scholar] [CrossRef] [Green Version]
- Paquette, D.E.; Colville, C.; Wheeler, T. Clear Aligner Treatment. In Orthodontics—Current Principles and Techniques, 6th ed.; Graber, L.W., Vanarsdall, R.L., Jr., Vig, K.W.L., Huang, G.J., Eds.; Elsevier: St. Louis, MO, USA, 2017; pp. 778–811. [Google Scholar]
- Iwasaki, L.R.; Haack, J.E.; Nickel, J.C.; Morton, J. Human tooth movement in response to continuous stress of low magnitude. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 175–183. [Google Scholar] [CrossRef]
- Echarri, P. Clear-Aligner; Editoral Ripano S.A.: Madrid, Spain, 2013. [Google Scholar]
- Elkholy, F.; Mikhaiel, B.; Schmidt, F.; Lapatki, B.G. Mechanical load exerted by PET-G aligners during mesial and distal derotation of a mandibular canine: An in vitro study. J. Orofac. Orthop. 2017, 78, 361–370. [Google Scholar] [CrossRef]
- Alikhani, M.; Chou, M.Y.; Khoo, E.; Alansari, S.; Kwal, R.; Elfersi, T.; Almansour, A.; Sangsuwon, C.; Al Jearah, M.; Nervina, J.M.; et al. Age-dependent biologic response to orthodontic forces. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 632–644. [Google Scholar] [CrossRef]
- Tepedino, M.; Paoloni, V.; Cozza, P.; Chimenti, C. Movement of anterior teeth using clear aligners: A three-dimensional, retrospective evaluation. Prog. Orthod. 2018, 19, 9. [Google Scholar] [CrossRef] [Green Version]
- Reitan, K. Initial tissue behavior during apical root resorption. Angle Orthod. 1974, 44, 68–82. [Google Scholar] [CrossRef]
- Dudic, A.; Giannopoulou, C.; Meda, P.; Montet, X.; Kiliaridis, S. Orthodontically induced cervical root resorption in humans is associated with the amount of tooth movement. Eur. J. Orthod. 2017, 39, 534–540. [Google Scholar] [CrossRef]
- Wishney, M. Potential risks of orthodontic therapy: A critical review and conceptual framework. Aust. Dent. J. 2017, 62 (Suppl. 1), 86–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandhi, V.; Mehta, S.; Gauthier, M.; Mu, J.; Kuo, C.L.; Nanda, R.; Yadav, S. Comparison of external apical root resorption with clear aligners and pre-adjusted edgewise appliances in non-extraction cases: A systematic review and meta-analysis. Eur. J. Orthod. 2021, 43, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.W.; Wilhelmy, B.; Gaugel, H. CLEAR-ALIGNER—An Alternative Orthodontic Appliance. Available online: http://www.andersson-gaugel.de/pdf/SD_Clear-Aligner_klein.pdf (accessed on 21 April 2022).
- Proffit, W.R.; Fields, H.W.; Larson, B.; Sarver, D.M. Contemporary Orthodontics—E-Book; Elsevier Health Sciences: Philadelphia, PA, USA, 2018. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth | Type of Movement | Axis of Movement | Expected Movement | Mean (SD) | Median (IQR) | Range | One-Sample Wilcoxon Signed Rank Test | |
|---|---|---|---|---|---|---|---|---|
| Z | P | |||||||
| 11 | Rotation (°) | X | 0 | 3.32 (2.17) | 2.62 [1.77; 4.35] | −0.08 to 10.10 | 7.056 | <0.001 |
| Y | 0 | −1.26 (1.51) | −0.91 [−2.15; 0.05] | −5.16 to 1.64 | −5.350 | <0.001 | ||
| Z | 0 | −1.39 (1.43) | −1.38 [−2.39; −0.81] | −5.63 to 2.57 | −5.810 | <0.001 | ||
| Translation (mm) | X | 0 | 0.20 (0.13) | 0.18 [0.09; 0.28] | −0.01 to 0.58 | 7.043 | <0.001 | |
| Y | 0 | −0.16 (0.26) | −0.13 [−0.33; 0.02] | −1.02 to 0.37 | −4.532 | <0.001 | ||
| Z | 1 | 1.09 (0.42) | 1.04 [0.79; 1.39] | 0.25 to 2.26 | 1.434 | 0.152 | ||
| 23 | Rotation (°) | X | 0 | −1.13 (4.03) | −0.52 [−3.57; 1.70] | −10.38 to 7.58 | −1.607 | 0.108 |
| Y | 15 | 9.61 (3.46) | 9.76 [7.58; 12.19] | 2.58 to 18.04 | −6.915 | <0.001 | ||
| Z | 0 | 5.27 (2.99) | 4.47 [2.99; 7.02] | −0.32 to 13.21 | 7.056 | <0.001 | ||
| Translation (mm) | X | 0 | −0.26 (0.19) | −0.26 [−0.37; −0.14] | −0.77 to 0.08 | −6.749 | <0.001 | |
| Y | 0 | 0.16 (0.27) | 0.14 [−0.02; 0.33] | −0.34 to 0.77 | 4.124 | <0.001 | ||
| Z | 0 | −0.88 (0.40) | −1.01 [−1.16; −0.75] | −1.47 to 0.02 | −7.024 | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sabbagh, H.; Heger, S.M.; Stocker, T.; Baumert, U.; Wichelhaus, A.; Hoffmann, L. Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials 2022, 15, 3853. https://doi.org/10.3390/ma15113853
Sabbagh H, Heger SM, Stocker T, Baumert U, Wichelhaus A, Hoffmann L. Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials. 2022; 15(11):3853. https://doi.org/10.3390/ma15113853
Chicago/Turabian StyleSabbagh, Hisham, Sebastian Marcus Heger, Thomas Stocker, Uwe Baumert, Andrea Wichelhaus, and Lea Hoffmann. 2022. "Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy" Materials 15, no. 11: 3853. https://doi.org/10.3390/ma15113853
APA StyleSabbagh, H., Heger, S. M., Stocker, T., Baumert, U., Wichelhaus, A., & Hoffmann, L. (2022). Accuracy of 3D Tooth Movements in the Fabrication of Manual Setup Models for Aligner Therapy. Materials, 15(11), 3853. https://doi.org/10.3390/ma15113853