Abstract
Background: The purpose of this review was to analyze and correlate the findings for zirconia implants in clinical, preclinical and in vitro cell studies in relation to surface structure. Methods: Electronic searches were conducted to identify clinical, preclinical and in vitro cell studies on zirconia implant surfaces. The primary outcomes were mean bone loss (MBL) for clinical studies, bone-to-implant contact (BIC) and removal torque (RT) for preclinical studies and cell spreading, cell proliferation and gene expression for cell studies. The secondary outcomes included comparisons of data found for those surfaces that were investigated in all three study types. Results: From 986 screened titles, 40 studies were included for data extraction. In clinical studies, only micro-structured surfaces were investigated. The lowest MBL was reported for sandblasted and subsequently etched surfaces, followed by a sinter and slurry treatment and sandblasted surfaces. For BIC, no clear preference of one surface structure was observable, while RT was slightly higher for micro-structured than smooth surfaces. All cell studies showed that cell spreading and cytoskeletal formation were enhanced on smooth compared with micro-structured surfaces. Conclusions: No correlation was observed for the effect of surface structure of zirconia implants within the results of clinical, preclinical and in vitro cell studies, underlining the need for standardized procedures for human, animal and in vitro studies.
1. Introduction
Two-piece titanium dental implants with a roughened endosseous surface are frequently used to achieve fast and stable osseointegration [1,2,3,4]. The term osseointegration was introduced by Per-Ingvar Brånemark (Gothenburg, Sweden) for describing a direct structural and functional connection between living bone and the implant surface on a light microscopy level [5,6]. In the 1960s, Brånemark, working closely with the company Nobelpharma, considered a machined endosseous implant surface as appropriate. However, the group of André Schröder (Bern, Switzerland), cooperating with the company Straumann, introduced a rough surface that should stimulate the attachment of osteoblasts [7]. A wide range of different techniques has subsequently been developed by different implant manufacturers to equip the endosseous implant surface with unique features that would accelerate osseointegration [8,9,10]. The current consensus promotes an endosseous titanium implant surface with a moderately rough surface with an Sa of 1 to 2 µm for the highest osseointegration potential [11].
Hence, when zirconia implants were introduced, the endosseous surface was also structured in accordance with the consensus for titanium implants. Currently available zirconia implants are either made of 3 mol% yttria-stabilized tetragonal zirconia polycrystal (Y-TZP) or alumina-toughened zirconia (ATZ). The first zirconia implants on the market were sandblasted to create a rough surface. Currently available implants display moderately rough to rough features with smoothened edges created via sandblasting followed by acid etching, via laser ablation, additive sintering of small zirconia particles or injection molding [12,13,14,15]. Some implants are additionally heat-treated to retrieve the tetragonal phase and decelerate the aging procedure [13].
Clinical medium-term data are available for moderately rough zirconia implants [16,17,18,19]. For these implants, sandblasting followed by etching or optional heat-treatment or laser treatment is applied to create the moderately rough surface. Most studies report mean bone loss around the implant at different follow-ups based on radiographs. Survival or success rates are also commonly calculated.
Preclinical studies with zirconia implants have been conducted to compare mainly the bone-to-implant contact (BIC) or removal torque (RT) of zirconia with titanium implants [14]. The chosen animal models included rats, rabbits, sheep, pigs and monkeys [14,15]. A review of preclinical data with zirconia implant surfaces revealed that the BIC is rather dependent on the animal model than the surface roughness [14]. The osseointegration potential of zirconia was assessed in vitro by conducting experiments with a wide range of osteoblastic cells and stem cell lines [20,21]. Different parameters such as cell spreading, cell proliferation, cell viability or expression of a wide range of inflammation or osteogenic differentiation genes were evaluated. Reviews considering in vitro data of cell studies mainly compared zirconia with titanium surfaces [20,21], and only limited information is available about the influence of surface topography on cell behavior [22].
No review analyzed if the findings from in vitro cell studies are consistent with preclinical data and are consequently relevant for conducting clinical studies for the respective surface structures of zirconia. Hence, the purpose of this review was to analyze and correlate the findings for zirconia implants in clinical with preclinical and in vitro cell studies to evaluate the influence of the surface structure on the outcome.
2. Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P [23]) statement using the Population, Intervention, Comparison and Outcome (PICO) method [24].
2.1. Focused Question
For the present review, the focused (PICO) question to be addressed was as follows: “In clinical, preclinical and in vitro studies, what are the outcomes (marginal bone loss, first bone-to-implant contact (BIC), removal torque (RT), cell behavior) of zirconia dental implant surfaces with regard to the surface structure?”
2.2. Search Strategy
A systematic electronic search of Medline via Pubmed and Embase was performed between June and August 2021. Articles in English and German were considered. The following terms and combinations were applied: ((“Dental implants” [MeSH] AND (“zirconium oxide” OR “yttria-stabilized tetragonal zirconia” OR “zirconia”)) OR “zirconia implant” OR “ceramic implant”) AND ((“osseointegration” [MeSH] OR “bone-implant-interface” [MeSH] OR “survival rate” [MeSH] OR “success rate” OR “marginal bone loss”) OR (“bone implant contact” OR “removal torque”) OR (“osteoblasts” OR “cell proliferation” OR “cell spreading” OR “gene expression”)). Additionally, recent systematic reviews [14,20,21,25,26,27] were screened for publications. Reference management software (Zotero, V 5.0.96.3) was used.
2.3. Inclusion Criteria
The inclusion criteria were defined as follows:
- Human trials, preclinical and in vitro osteoblastic cell studies investigating zirconia implant surfaces that were published between January 2000 and December 2021;
- Randomized clinical trials or cohort studies with at least 10 patients included [26];
- Details on the surface structure of zirconia and implant manufacturer are given;
- Reported details of marginal bone loss of clinical trials, BIC or RT of preclinical studies, osteoblastic cell behavior (spreading, proliferation, gene expression) for in vitro studies comparing two different zirconia surfaces.
2.4. Exclusion Criteria
Studies that did not meet the inclusion criteria were excluded from this work. Data from multiple publications on the same patient population were summarized, and the last published work was cited.
2.5. Selection of Studies
After elimination of duplicates, the reviewers (BH, NR) independently screened titles, abstracts and full texts meeting the selection criteria. Disagreements regarding the inclusion and exclusion of studies were resolved by discussion between the reviewers.
2.6. Data Extraction and Outcome Measures
Data extraction into Excel tables was independently performed for all included studies (BH, NR). From the included full-text articles, the following data were extracted: author(s), year of publication, number of included patients and implants, implant material (yttria-stabilized zirconia (Y-TZP)/alumina-toughened zirconia (ATZ), controls, implant design (1-piece/2-piece), specimen dimension, implant manufacturer, implant surface treatment, surface roughness, time period between implant placement and prosthetic treatment, type of restoration (single crown (SC)/fixed dental prostheses (FDP)), number of implant failures, observation period (months), implant survival (%), mean bone loss (MBL, mm), bone-to-implant contact (BIC, %), removal torque (RT, Ncm), animal, cell line, cell spreading, cell proliferation and gene expression.
Primary outcomes were MBL for clinical studies, BIC and RT for preclinical studies, and cell spreading, cell proliferation and gene expression for cell studies. Secondary outcomes included comparisons of data found for those surfaces that were investigated in all three study types.
2.7. Data Analysis
The mean MBL values from clinical studies of the same study population were collected for each follow-up. Data of studies using the same implant type were then pooled when data were extracted at the same follow-up. Further, data of implants with similar surface treatments were pooled at each follow-up. The BIC values and RT values of the included preclinical studies were listed for each intervention point. Values were further pooled by surface treatment and animal model for each intervention point. Minipig and pig were considered as species pig. Findings for cell spreading, cell proliferation and gene expression of in vitro cell studies were analyzed descriptively by comparing the results of the investigated surfaces within each study.
3. Results
The electronic data base search and the respective results are displayed in Figure 1. For the clinical studies, only those displaying the latest results of the same study population are listed by the first authors’ name (n = 10). However, short-term data were extracted from previous studies of the respective population whenever data on MBL were missing in the latest reports.
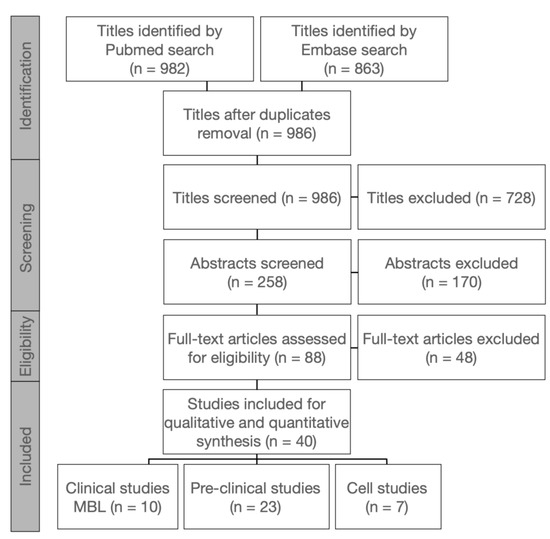
Figure 1.
Search strategy and study selection process.
Details on clinical studies are given in Table 1. Implants with sandblasted surfaces that were inserted in five of the studies [18,28,29,30,31] displayed survival rates between 77.3 and 100%. The survival rates of implants with sinter and slurry on the endosseous surface ranged from 94.3 to 98.2% [17,32,33]. The survival of sandblasted and etched surfaces that were used in two prospective studies ranged from 97.5 to 98.4% [16,19]. The MBL obtained at the respective follow-ups is displayed in Figure 2a. Following the consensus for titanium implants, an MBL of 2 mm at most was considered a threshold value for success [34]. The data of the same implant types were pooled in Figure 2b. The lowest MBL was observed with the implant ceramic.implant (Vita, Germany). The MBL was pooled by surface treatments in Figure 2c. Overall, the lowest MBL was reported for sandblasted and subsequently etched surfaces, followed by a sinter and slurry treatment and sandblasted surfaces. However, data of up to 11 years were included for sandblasted surfaces, while for the others, data between 3 and 5.5 years are currently published.

Table 1.
Overview of clinical trials with zirconia implants.
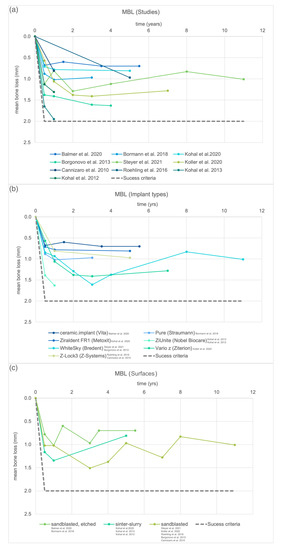
Figure 2.
Mean bone loss (MBL) reported in clinical studies with zirconia implants at the respective follow-up. The threshold value included as success criteria was defined by Misch et al. 2008 [34]. (a) Mean bone loss of all included clinical trials, (b) mean bone loss pooled by implant type and (c) mean bone loss pooled by implant surface treatment.
An overview of the animal studies is given in Table 2 (n = 23). Within those studies, the results of BIC and RT obtained within the same set-up were published separately for two preclinical studies [45,46,47,48]. The BIC was obtained in 19 and RT in 8 of the studies. Only one study compared the BIC of two different implant materials within one trial, however, with varying surface treatments [49]. The BIC values in studies directly comparing zirconia implants with different surfaces with the same set-up were either significantly higher [50], similar [51,52,53] or lower [54] for smoother surfaces.
Table 2.
Overview of preclinical studies that measured bone-to-implant contact or removal torque (mean with standard deviations) of zirconia implants.
The BIC at the respective intervention time for each study is displayed in Figure 3a. Similar surface treatments were pooled in Figure 3b. No clear preference of one surface treatment is observable. Figure 3c shows the BIC pooled by the animal model for zirconia implants. The rabbit and rat models display a short intervention time with a fast osseointegration; however, with the rabbit model, higher BIC values were reported. The BIC with the pig model decreased again after 8 weeks. For the dog model, osseointegration progressed slower and required observation periods of up to 48 weeks.
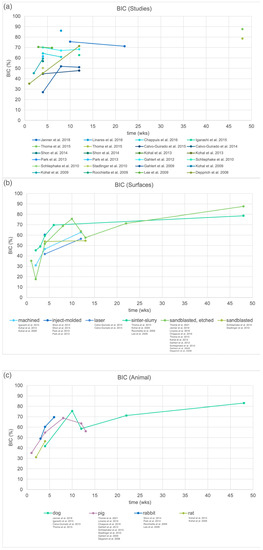
Figure 3.
Bone-to-implant contact (BIC) around zirconia implants obtained in preclinical studies. (a) BIC of all included studies, (b) BIC pooled by surface treatment of zirconia implants and (c) BIC pooled by animal model.
Figure 4a reveals the RT at the different intervention times for each included preclinical study. Similar surfaces were pooled in Figure 4b. For machined surfaces, a lower RT was reported than for modified surfaces that were sandblasted or etched. Studies comparing the RT of zirconia implants with different surfaces within the same set-up found higher values for rougher surfaces [53,61,67]. When the RT was pooled by the animal model in Figure 4c, the RT in the rabbit model strongly increased between 3 and 4 weeks. For the pig model, a slight increase was reported between 8 and 12 weeks that progressed further afterward.
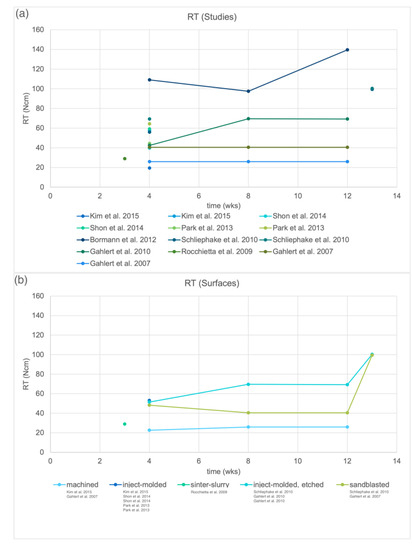
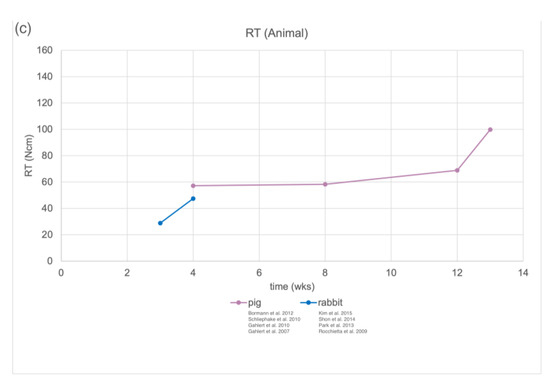
Figure 4.
Removal torque (RT) around zirconia implants obtained in preclinical studies. (a) RT of all included studies, (b) RT pooled by surface treatment of zirconia implants and (c) RT pooled by animal model.
Cell studies with osteoblastic cells comparing two differing zirconia implant surfaces are presented descriptively in Table 3 (n = 7). Six of the studies compared a micro-structured (sandblasted and subsequently etched [50,68,69,70,71] or sinter and slurry-modified [72]) surface with a machined surface. All studies showed that cell spreading and cytoskeletal formation were enhanced on machined compared with micro-structured surfaces [50,68,69,70,72]. Cell proliferation was either enhanced [72], similar [50] or lower [71] on machined surfaces compared with micro-structured surfaces. For gene expression, no conclusive results were observable as all studies investigated different time intervals, gene expression and cell lines.
Table 3.
Overview of cell studies with osteoblast that compared two different zirconia implant surfaces by measuring cell spreading, cell proliferation or gene expression.
4. Discussion
The purpose of this review was to analyze and correlate the findings for zirconia implants in clinical with preclinical and in vitro cell studies to evaluate the influence of the surface structure on the outcome. As only sandblasted, sinter and slurry-modified, as well as sandblasted and subsequently etched surfaces were investigated in the included clinical trials, only those findings could be compared with preclinical and in vitro cell studies. The best performance with the highest survival rates and the lowest MBL in the clinic were observed for sandblasted and subsequently etched surfaces, followed by sinter and slurry-modified and sandblasted surfaces. In preclinical studies, the BIC values reported for sandblasted and subsequently etched and sinter and slurry-modified surfaces seemed similar, deviating slightly at each intervention point. Osseointegration of sandblasted surfaces progressed slower; however, data were only available for two intervention time points. Unfortunately, none of these surfaces were compared with each other regarding the RT and in cell studies with osteoblasts.
The zirconia implants currently on the market with clinical studies included in this review are either one-piece Y-TZP implants that are sandblasted by Bredent [28,30], sandblasted and etched by Straumann and Vita [16,19] or ATZ implants with surfaces modified with sinter and slurry by Fairimplant [17]. Implants of Z-System [29,31] are still available, but surfaces were changed from sandblasted to laser-modified. The two-piece implant system of Ziterion with clinical studies available [18] was acquired by Sirona Dentsply but is at present not on the market. For the clinical performance of two-piece implants, only limited clinical data are currently available. Besides the study with Ziterion implants [18], another clinical trial was conducted with Zeramex ATZ implants reporting a survival rate of 83% after almost a 7-year follow-up [74]. Within the currently available systems, the highest survival rates were reported for one-piece zirconia implants with sandblasted and subsequently etched surfaces of 97.5 to 98.4% [16,19]. In addition, the MBL is promising with values below 1 mm after 3 and 5.5 years, respectively, for those studies that evaluated 102 implants in total. The results of implants modified with sinter and slurry achieved high survival rates in two different studies of 95.4% to 98.2% after 1 year [32,33] and 94.3% after 5 years [17], respectively. All three studies were conducted by one group. The MBL of the most recent study with 35 evaluated ATZ implants after 5 years (Ziraldent FR1, Metoxit) was within the range of sandblasted and subsequently etched implants, i.e., below 1 mm [17]. However, the MBL of Y-TZP implants by Nobel Biocare with the same surface showed an MBL of 1.3 mm after 1 year for implants restored with single crowns [33]. A higher MBL of almost 2 mm was reported for those implants restored with fixed dental prostheses (FDP) [32]. Follow-ups in both studies were only conducted up to one year. The restorative treatment (single crowns or FDPs) affected the MBL in all studies with sinter and slurry-modified surfaces [17,32], but not for sandblasted and subsequently etched zirconia implants [16]. Implants with sandblasted surfaces displayed lower survival rates, varying between 77.3 and 100% [18,28,29,30,31], confirmed by a tendency towards higher MBL values than for other implant surfaces.
Overall, the clinical outcome of zirconia implants irrespective of the surface can be considered promising confirming previous reviews [21,25,26,27], and all implant surfaces resulted in an MBL below the threshold value for clinical success of 2 mm [34]. In clinical studies, only the micro-structured implant surfaces are investigated. However, it has been found that clinical bone formation on zirconia implants occurs and remains stable up to 5 years on the endosseous sandblasted and subsequently etched, as well as on the polished transmucosal part [75]. The current review confirms findings of a review with titanium implants demonstrating that very good long-term results can be achieved with all types of endosseous implant surfaces (turned, titanium plasma sprayed, blasted, anodized, blasted and acid-etched) [76]. Hence, the surface structure of the endosseous part of implants may not be the decisive factor for osseointegration but might affect osseointegration speed. Such a hypothesis is, however, not supported by the available results.
In preclinical studies, no clear preference of one surface structure could be identified. Surprisingly, surfaces with lower surface roughness that were machined or injection-molded provided comparable BIC to modified surfaces. When smooth surfaces were directly compared with rougher surfaces within the same set-up, even higher [50], similar [51,52,53] or lower [54] BICs were measured. Hence, the current dogma for titanium implants, that an Sa value between 1 and 2 µm roughness promotes osseointegration [11], may not be applicable for zirconia implants. The surface roughness value Sa is mainly used to describe the roughness of implants. However, this value only provides information on the arithmetical mean roughness and the actual topography, while factors such as kurtosis and skewness that may impact osseointegration are not considered. As obtaining the surface roughness of dental implants was not performed in a standardized manner for the included studies, the authors refrained from using the surface roughness parameter Sa as a comparative factor in this review.
The RT values were lower for machined compared with rougher surfaces [53,61,67]; hence, a machined implant may be easier retrieved in the case of removal. However, the effect of a smooth surface on the long-term stability of the implant is currently not known.
As previously observed, BIC and RT were highly affected by the selected animal model [27]. Osseointegration occurred faster in the rabbit and rat models; hence, shorter investigation times seemed applicable. Higher BIC values can be expected from the rabbit model compared with the rat model for zirconia implants (Figure 3c). Larger animal models with dogs or pigs are commonly chosen, as they would provide an ossseointegration speed similar to the human species [77]. However, longer observation periods and higher costs are to be expected for those studies. Consequently, BIC and RT values of the different surfaces could only be truly evaluated within the same study set-up due to varying effects of the animal model, observation time, implant material and implant dimensions. Hence, before considering performing an animal study, those parameters should be as standardized as possible to retrieve a valuable outcome on the effect of surface structure.
Cell studies should be a prerequisite for conducting animal studies. Only one group considered comparing the outcome of their cell study with a preclinical model with rats using the same surfaces [50]. Machined surfaces were compared with sandblasted and subsequently etched surfaces. For cell proliferation and gene expression of human fetal osteoblast cells hFOB 1.19, no correlation between the outcome of cell and animal study could be determined between the two investigated surfaces. However, cytoskeletal organization and focal contact formation were faster on machined than on sandblasted and subsequently etched surfaces. In addition, the BIC in the rat model was significantly higher on the machined surface after 4 and 8 weeks [50]. The finding that cell spreading and cytoskeletal formation are enhanced on machined compared with micro-structured surfaces was confirmed by all other included studies with osteoblast cells [50,68,69,70,72].
Unfortunately, no clinical study with machined zirconia implants exists to further investigate the potential of this surface structuring method. Only the fact that radiological long-term data from a clinical study prove a tight contact between the polished zirconia transmucosal part and bone [75] supports the hypothesis that smooth surfaces might provide osseointegration in the long run. Smooth surfaces are of high interest to improve cleanability, increase implant quality and decrease production costs.
Although a great effort is made to conduct in vitro, preclinical and clinical studies, no correlation can be observed within the respective results, underlining the need for standardized procedures for animal and human studies, especially concerning ethics. Additional attention should be focused on choosing an appropriate control group for animal and human research having only one varying parameter from the test group. The tested materials and surfaces are to be properly characterized using scanning electron microscopy and more parameters of surface roughness than the arithmetical mean. In vitro cell and preclinical studies using the same implant surfaces should be mandatory prior to a clinical trial to validate the study designs. In addition, there is a strong need for guidelines for conducting clinical trials with implants and for the parameters to be obtained and reported.
5. Conclusions
The conclusion must be interpreted with care as the study designs of the included clinical, preclinical and cell studies are highly heterogenous and vary regarding the follow-up time and implant design. Within the limitations of this review that investigated the impact of surface structure of zirconia implants it can be concluded that:
- In clinical studies, the lowest MBL was reported for sandblasted and subsequently etched surfaces, followed by a sinter and slurry treatment and sandblasted surfaces;
- In preclinical studies analyzing BIC, no clear preference of one surface structure was observable. The RT was slightly higher for micro-structured than smooth surfaces. The BIC and RT values were highly influenced by the chosen animal model;
- All cell studies showed that cell spreading and cytoskeletal formation were enhanced on machined compared with micro-structured surfaces;
- No correlation was observed between the outcomes, underlining the need for standardized procedures for animal and human studies.
Author Contributions
Conceptualization, N.R. and J.F.; methodology, N.R., B.H. and J.F.; formal analysis, N.R.; investigation, N.R. and B.H.; data curation, N.R. and B.H.; writing—original draft preparation, N.R.; writing—review and editing, N.R. and J.F.; visualization, N.R.; supervision, J.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request from the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Buser, D.; Janner, S.F.M.; Wittneben, J.-G.; Brägger, U.; Ramseier, C.A.; Salvi, G.E. 10-Year Survival and Success Rates of 511 Titanium Implants with a Sandblasted and Acid-Etched Surface: A Retrospective Study in 303 Partially Edentulous Patients. Clin. Implant. Dent. Relat. Res. 2012, 14, 839–851. [Google Scholar] [CrossRef] [PubMed]
- Ravald, N.; Dahlgren, S.; Teiwik, A.; Gröndahl, K. Long-Term Evaluation of Astra Tech and Brånemark Implants in Patients Treated with Full-Arch Bridges. Results after 12–15 Years. Clin. Oral Implant. Res. 2013, 24, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Östman, P.-O.; Hellman, M.; Sennerby, L. Ten Years Later. Results from a Prospective Single-Centre Clinical Study on 121 Oxidized (TiUniteTM) Brånemark Implants in 46 Patients. Clin. Implant. Dent. Relat Res. 2012, 14, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Stenberg, T. Prospective 10-Year Cohort Study Based on a Randomized Controlled Trial (RCT) on Implant-Supported Full-Arch Maxillary Prostheses. Part 1: Sandblasted and Acid-Etched Implants and Mucosal Tissue. Clin. Implant. Dent. Relat Res. 2012, 14, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Chrcanovic, B.; Östman, P.-O.; Sennerby, L. Initial and Long-Term Crestal Bone Responses to Modern Dental Implants. Periodontol. 2000 2017, 73, 41–50. [Google Scholar] [CrossRef]
- The Osseointegration Book: From Calvarium to Calcaneus. Available online: http://www.quintpub.com/display_detail.php3?psku=BG063#.YYlA7VMxnOQ (accessed on 8 November 2021).
- Abraham, C.M. A Brief Historical Perspective on Dental Implants, Their Surface Coatings and Treatments. Open Dent. J. 2014, 8, 50–55. [Google Scholar] [CrossRef]
- Nobles, K.P.; Janorkar, A.V.; Williamson, R.S. Surface Modifications to Enhance Osseointegration-Resulting Material Properties and Biological Responses. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 1909–1923. [Google Scholar] [CrossRef]
- Souza, J.C.M.; Sordi, M.B.; Kanazawa, M.; Ravindran, S.; Henriques, B.; Silva, F.S.; Aparicio, C.; Cooper, L.F. Nano-Scale Modification of Titanium Implant Surfaces to Enhance Osseointegration. Acta Biomater. 2019, 94, 112–131. [Google Scholar] [CrossRef]
- Rupp, F.; Liang, L.; Geis-Gerstorfer, J.; Scheideler, L.; Hüttig, F. Surface Characteristics of Dental Implants: A Review. Dent. Mater. 2018, 34, 40–57. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. Effects of Titanium Surface Topography on Bone Integration: A Systematic Review. Clin. Oral Implant. Res. 2009, 20, 172–184. [Google Scholar] [CrossRef]
- Schünemann, F.H.; Galárraga-Vinueza, M.E.; Magini, R.; Fredel, M.; Silva, F.; Souza, J.C.M.; Zhang, Y.; Henriques, B. Zirconia Surface Modifications for Implant Dentistry. Mater. Sci. Eng. C 2019, 98, 1294–1305. [Google Scholar] [CrossRef]
- Fischer, J.; Schott, A.; Märtin, S. Surface Micro-Structuring of Zirconia Dental Implants. Clin. Oral Implant. Res. 2016, 27, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Pieralli, S.; Kohal, R.-J.; Lopez Hernandez, E.; Doerken, S.; Spies, B.C. Osseointegration of Zirconia Dental Implants in Animal Investigations: A Systematic Review and Meta-Analysis. Dent. Mater. 2018, 34, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Nishihara, H.; Haro Adanez, M.; Att, W. Current Status of Zirconia Implants in Dentistry: Pre-clinical Tests. J. Prosthodont. Res. 2019, 63, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Balmer, M.; Spies, B.C.; Kohal, R.; Hämmerle, C.H.; Vach, K.; Jung, R.E. Zirconia Implants Restored with Single Crowns or Fixed Dental Prostheses: 5-year Results of a Prospective Cohort Investigation. Clin. Oral Implant. Res. 2020, 31, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.-J.; Spies, B.C.; Vach, K.; Balmer, M.; Pieralli, S. A Prospective Clinical Cohort Investigation on Zirconia Implants: 5-Year Results. J. Clin. Med. 2020, 9, 2585. [Google Scholar] [CrossRef]
- Koller, M.; Steyer, E.; Theisen, K.; Stagnell, S.; Jakse, N.; Payer, M. Two-Piece Zirconia versus Titanium Implants after 80 Months: Clinical Outcomes from a Prospective Randomized Pilot Trial. Clin. Oral Implant. Res. 2020, 31, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Bormann, K.-H.; Gellrich, N.-C.; Kniha, H.; Schild, S.; Weingart, D.; Gahlert, M. A Prospective Clinical Study to Evaluate the Performance of Zirconium Dioxide Dental Implants in Single-Tooth Edentulous Area: 3-Year Follow-Up. BMC Oral Health 2018, 18, 181. [Google Scholar] [CrossRef] [Green Version]
- Hanawa, T. Zirconia versus Titanium in Dentistry: A Review. Dent. Mater. J. 2020, 39, 24–36. [Google Scholar] [CrossRef] [Green Version]
- Sivaraman, K.; Chopra, A.; Narayan, A.I.; Balakrishnan, D. Is Zirconia a Viable Alternative to Titanium for Oral Implant? A Critical Review. J. Prosthodont. Res. 2018, 62, 121–133. [Google Scholar] [CrossRef]
- Han, A.; Tsoi, J.K.H.; Lung, C.Y.K.; Matinlinna, J.P. An Introduction of Biological Performance of Zirconia with Different Surface Characteristics: A Review. Dent. Mater. J. 2020, 39, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO Framework to Improve Searching PubMed for Clinical Questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afrashtehfar, K.I.; Del Fabbro, M. Clinical Performance of Zirconia Implants: A Meta-Review. J. Prosthet. Dent. 2020, 123, 419–426. [Google Scholar] [CrossRef]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Performance and Outcome of Zirconia Dental Implants in Clinical Studies: A Meta-analysis. Clin. Oral Implant. Res. 2018, 29, 135–153. [Google Scholar] [CrossRef]
- Pieralli, S.; Kohal, R.J.; Jung, R.E.; Vach, K.; Spies, B.C. Clinical Outcomes of Zirconia Dental Implants: A Systematic Review. J. Dent. Res. 2017, 96, 38–46. [Google Scholar] [CrossRef]
- Steyer, E.; Herber, V.; Koller, M.; Végh, D.; Mukaddam, K.; Jakse, N.; Payer, M. Immediate Restoration of Single-Piece Zirconia Implants: A Prospective Case Series-Long-Term Results after 11 Years of Clinical Function. Materials 2021, 14, 6738. [Google Scholar] [CrossRef]
- Roehling, S.; Woelfler, H.; Hicklin, S.; Kniha, H.; Gahlert, M. A Retrospective Clinical Study with Regard to Survival and Success Rates of Zirconia Implants up to and after 7 Years of Loading. Clin. Implant. Dent. Relat Res. 2016, 18, 545–558. [Google Scholar] [CrossRef]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Dolci, M.; Calvo-Guirado, J.L.; Delgado Ruiz, R.A.; Maiorana, C. Evaluation of the Success Criteria for Zirconia Dental Implants: A Four-Year Clinical and Radiological Study. Int. J. Dent. 2013, 2013, 463073. [Google Scholar] [CrossRef]
- Cannizzaro, G.; Torchio, C.; Felice, P.; Leone, M.; Esposito, M. Immediate Occlusal versus Non-Occlusal Loading of Single Zirconia Implants. A Multicentre Pragmatic Randomised Clinical Trial. Eur. J. Oral Implantol. 2010, 3, 111–120. [Google Scholar]
- Kohal, R.-J.; Patzelt, S.B.M.; Butz, F.; Sahlin, H. One-Piece Zirconia Oral Implants: One-Year Results from a Prospective Case Series. 2. Three-Unit Fixed Dental Prosthesis (FDP) Reconstruction. J. Clin. Periodontol. 2013, 40, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.-J.; Knauf, M.; Larsson, B.; Sahlin, H.; Butz, F. One-Piece Zirconia Oral Implants: One-Year Results from a Prospective Cohort Study. 1. Single Tooth Replacement. J. Clin. Periodontol. 2012, 39, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Perel, M.L.; Wang, H.-L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant Success, Survival, and Failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payer, M.; Arnetzl, V.; Kirmeier, R.; Koller, M.; Arnetzl, G.; Jakse, N. Immediate Provisional Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Results after 24 Months of Clinical Function. Clin. Oral Implant. Res. 2013, 24, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Spies, B.C.; Sperlich, M.; Fleiner, J.; Stampf, S.; Kohal, R.-J. Alumina Reinforced Zirconia Implants: 1-Year Results from a Prospective Cohort Investigation. Clin. Oral Implant. Res. 2016, 27, 481–490. [Google Scholar] [CrossRef]
- Spies, B.C.; Balmer, M.; Patzelt, S.B.M.; Vach, K.; Kohal, R.J. Clinical and Patient-Reported Outcomes of a Zirconia Oral Implant: Three-Year Results of a Prospective Cohort Investigation. J. Dent. Res. 2015, 94, 1385–1391. [Google Scholar] [CrossRef]
- Payer, M.; Heschl, A.; Koller, M.; Arnetzl, G.; Lorenzoni, M.; Jakse, N. All-Ceramic Restoration of Zirconia Two-Piece Implants—A Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2015, 26, 371–376. [Google Scholar] [CrossRef]
- Balmer, M.; Spies, B.C.; Vach, K.; Kohal, R.-J.; Hämmerle, C.H.F.; Jung, R.E. Three-Year Analysis of Zirconia Implants Used for Single-Tooth Replacement and Three-Unit Fixed Dental Prostheses: A Prospective Multicenter Study. Clin. Oral Implant. Res. 2018, 29, 290–299. [Google Scholar] [CrossRef] [Green Version]
- Jung, R.E.; Grohmann, P.; Sailer, I.; Steinhart, Y.-N.; Fehér, A.; Hämmerle, C.; Strub, J.R.; Kohal, R. Evaluation of a One-Piece Ceramic Implant Used for Single-Tooth Replacement and Three-Unit Fixed Partial Dentures: A Prospective Cohort Clinical Trial. Clin. Oral Implant. Res. 2016, 27, 751–761. [Google Scholar] [CrossRef]
- Gahlert, M.; Kniha, H.; Weingart, D.; Schild, S.; Gellrich, N.-C.; Bormann, K.-H. A Prospective Clinical Study to Evaluate the Performance of Zirconium Dioxide Dental Implants in Single-Tooth Gaps. Clin. Oral Implant. Res. 2016, 27, e176–e184. [Google Scholar] [CrossRef]
- Borgonovo, A.-E.; Fabbri, A.; Vavassori, V.; Censi, R.; Maiorana, C. Multiple Teeth Replacement with Endosseous One-Piece Yttrium-Stabilized Zirconia Dental Implants. Med. Oral Patol. Oral Cir. Bucal. 2012, 17, e981–e987. [Google Scholar] [CrossRef] [PubMed]
- Borgonovo, A.; Censi, R.; Dolci, M.; Vavassori, V.; Bianchi, A.; Maiorana, C. Use of Endosseous One-Piece Yttrium-Stabilized Zirconia Dental Implants in Premolar Region: A Two-Year Clinical Preliminary Report. Minerva Stomatol. 2011, 60, 229–241. [Google Scholar] [PubMed]
- Borgonovo, A.E.; Arnaboldi, O.; Censi, R.; Dolci, M.; Santoro, G. Edentulous Jaws Rehabilitation with Yttrium-Stabilized Zirconium Dioxide Implants: Two Years Follow-up Experience. Minerva Stomatol. 2010, 59, 381–392. [Google Scholar] [PubMed]
- Gahlert, M.; Roehling, S.; Sprecher, C.M.; Kniha, H.; Milz, S.; Bormann, K. In Vivo Performance of Zirconia and Titanium Implants: A Histomorphometric Study in Mini Pig Maxillae. Clin. Oral Implant. Res. 2012, 23, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Bormann, K.-H.; Gellrich, N.-C.; Kniha, H.; Dard, M.; Wieland, M.; Gahlert, M. Biomechanical Evaluation of a Microstructured Zirconia Implant by a Removal Torque Comparison with a Standard Ti-SLA Implant. Clin. Oral Implant. Res. 2012, 23, 1210–1216. [Google Scholar] [CrossRef]
- Gahlert, M.; Röhling, S.; Wieland, M.; Eichhorn, S.; Küchenhoff, H.; Kniha, H. A Comparison Study of the Osseointegration of Zirconia and Titanium Dental Implants. A Biomechanical Evaluation in the Maxilla of Pigs. Clin. Implant. Dent. Relat. Res. 2010, 12, 297–305. [Google Scholar] [CrossRef]
- Gahlert, M.; Röhling, S.; Wieland, M.; Sprecher, C.M.; Kniha, H.; Milz, S. Osseointegration of Zirconia and Titanium Dental Implants: A Histological and Histomorphometrical Study in the Maxilla of Pigs. Clin. Oral Implant. Res. 2009, 20, 1247–1253. [Google Scholar] [CrossRef]
- Thoma, D.S.; Benic, G.I.; Muñoz, F.; Kohal, R.; Sanz Martin, I.; Cantalapiedra, A.G.; Hämmerle, C.H.F.; Jung, R.E. Histological Analysis of Loaded Zirconia and Titanium Dental Implants: An Experimental Study in the Dog Mandible. J. Clin. Periodontol. 2015, 42, 967–975. [Google Scholar] [CrossRef] [Green Version]
- Kohal, R.J.; Bächle, M.; Att, W.; Chaar, S.; Altmann, B.; Renz, A.; Butz, F. Osteoblast and Bone Tissue Response to Surface Modified Zirconia and Titanium Implant Materials. Dent. Mater. 2013, 29, 763–776. [Google Scholar] [CrossRef]
- Schliephake, H.; Hefti, T.; Schlottig, F.; Gédet, P.; Staedt, H. Mechanical Anchorage and Peri-Implant Bone Formation of Surface-Modified Zirconia in Minipigs. J. Clin. Periodontol. 2010, 37, 818–828. [Google Scholar] [CrossRef]
- Park, Y.-S.; Chung, S.-H.; Shon, W.-J. Peri-Implant Bone Formation and Surface Characteristics of Rough Surface Zirconia Implants Manufactured by Powder Injection Molding Technique in Rabbit Tibiae. Clin. Oral Implant. Res. 2013, 24, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Shon, W.-J.; Chung, S.H.; Kim, H.-K.; Han, G.-J.; Cho, B.-H.; Park, Y.-S. Peri-Implant Bone Formation of Non-Thermal Atmospheric Pressure Plasma-Treated Zirconia Implants with Different Surface Roughness in Rabbit Tibiae. Clin. Oral Implant. Res. 2014, 25, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Kohal, R.J.; Wolkewitz, M.; Hinze, M.; Han, J.-S.; Bächle, M.; Butz, F. Biomechanical and Histological Behavior of Zirconia Implants: An Experiment in the Rat. Clin. Oral Implant. Res. 2009, 20, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Thomé, G.; Sandgren, R.; Bernardes, S.; Trojan, L.; Warfving, N.; Bellón, B.; Pippenger, B.E. Osseointegration of a Novel Injection Molded 2-Piece Ceramic Dental Implant: A Study in Minipigs. Clin. Oral Investig. 2021, 25, 603–615. [Google Scholar] [CrossRef] [PubMed]
- Janner, S.F.M.; Gahlert, M.; Bosshardt, D.D.; Roehling, S.; Milz, S.; Higginbottom, F.; Buser, D.; Cochran, D.L. Bone Response to Functionally Loaded, Two-Piece Zirconia Implants: A Pre-clinical Histometric Study. Clin. Oral Implant. Res. 2018, 29, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Liñares, A.; Grize, L.; Muñoz, F.; Pippenger, B.E.; Dard, M.; Domken, O.; Blanco-Carrión, J. Histological Assessment of Hard and Soft Tissues Surrounding a Novel Ceramic Implant: A Pilot Study in the Minipig. J. Clin. Periodontol. 2016, 43, 538–546. [Google Scholar] [CrossRef]
- Chappuis, V.; Cavusoglu, Y.; Gruber, R.; Kuchler, U.; Buser, D.; Bosshardt, D.D. Osseointegration of Zirconia in the Presence of Multinucleated Giant Cells. Clin. Implant. Dent. Relat Res. 2016, 18, 686–698. [Google Scholar] [CrossRef]
- Igarashi, K.; Nakahara, K.; Haga-Tsujimura, M.; Kobayashi, E.; Watanabe, F. Hard and Soft Tissue Responses to Three Different Implant Materials in a Dog Model. Dent. Mater. J. 2015, 34, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Guirado, J.L.; Aguilar-Salvatierra, A.; Delgado-Ruiz, R.A.; Negri, B.; Fernández, M.P.R.; Maté Sánchez de Val, J.E.; Gómez-Moreno, G.; Romanos, G.E. Histological and Histomorphometric Evaluation of Zirconia Dental Implants Modified by Femtosecond Laser versus Titanium Implants: An Experimental Study in Fox Hound Dogs. Clin. Implant. Dent. Relat. Res. 2015, 17, 525–532. [Google Scholar] [CrossRef]
- Kim, H.-K.; Woo, K.M.; Shon, W.-J.; Ahn, J.-S.; Cha, S.; Park, Y.-S. Comparison of Peri-Implant Bone Formation around Injection-Molded and Machined Surface Zirconia Implants in Rabbit Tibiae. Dent. Mater. J. 2015, 34, 508–515. [Google Scholar] [CrossRef] [Green Version]
- Calvo-Guirado, J.L.; Aguilar-Salvatierra, A.; Gomez-Moreno, G.; Guardia, J.; Delgado-Ruiz, R.A.; Mate-Sanchez de Val, J.E. Histological, Radiological and Histomorphometric Evaluation of Immediate vs. Non-Immediate Loading of a Zirconia Implant with Surface Treatment in a Dog Model. Clin. Oral Implant. Res. 2014, 25, 826–830. [Google Scholar] [CrossRef] [PubMed]
- Stadlinger, B.; Hennig, M.; Eckelt, U.; Kuhlisch, E.; Mai, R. Comparison of Zirconia and Titanium Implants after a Short Healing Period. A Pilot Study in Minipigs. Int. J. Oral Maxillofac. Surg. 2010, 39, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Rocchietta, I.; Fontana, F.; Addis, A.; Schupbach, P.; Simion, M. Surface-Modified Zirconia Implants: Tissue Response in Rabbits. Clin. Oral Implant. Res. 2009, 20, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Sieweke, J.H.; Rodriguez, N.A.; Schüpbach, P.; Lindström, H.; Susin, C.; Wikesjö, U.M.E. Evaluation of Nano-Technology-Modified Zirconia Oral Implants: A Study in Rabbits. J. Clin. Periodontol. 2009, 36, 610–617. [Google Scholar] [CrossRef]
- Depprich, R.; Zipprich, H.; Ommerborn, M.; Naujoks, C.; Wiesmann, H.-P.; Kiattavorncharoen, S.; Lauer, H.-C.; Meyer, U.; Kübler, N.R.; Handschel, J. Osseointegration of Zirconia Implants Compared with Titanium: An in Vivo Study. Head Face Med. 2008, 4, 30. [Google Scholar] [CrossRef] [Green Version]
- Gahlert, M.; Gudehus, T.; Eichhorn, S.; Steinhauser, E.; Kniha, H.; Erhardt, W. Biomechanical and Histomorphometric Comparison between Zirconia Implants with Varying Surface Textures and a Titanium Implant in the Maxilla of Miniature Pigs. Clin. Oral Implant. Res. 2007, 18, 662–668. [Google Scholar] [CrossRef]
- Rohr, N.; Bergemann, C.; Nebe, B.J.; Fischer, J. Crystal Structure of Zirconia Affects Osteoblast Behavior. Dent. Mater. 2020, 36, 905–913. [Google Scholar] [CrossRef]
- Bergemann, C.; Duske, K.; Nebe, J.B.; Schöne, A.; Bulnheim, U.; Seitz, H.; Fischer, J. Microstructured Zirconia Surfaces Modulate Osteogenic Marker Genes in Human Primary Osteoblasts. J. Mater. Sci. Mater. Med. 2015, 26, 26. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.; Bohner, L.; Hanisch, M.; Kleinheinz, J.; Sielker, S. Influence of Implant Material and Surface on Mode and Strength of Cell/Matrix Attachment of Human Adipose Derived Stromal Cell. Int. J. Mol. Sci. 2020, 21, 4110. [Google Scholar] [CrossRef]
- Jung, S.; Bohner, L.; Hanisch, M.; Kleinheinz, J.; Sielker, S. Influence of Implant Material and Surface on Differentiation and Proliferation of Human Adipose-Derived Stromal Cells. Int. J. Mol. Sci. 2018, 19, 4033. [Google Scholar] [CrossRef] [Green Version]
- Setzer, B.; Bächle, M.; Metzger, M.C.; Kohal, R.J. The Gene-Expression and Phenotypic Response of HFOB 1.19 Osteoblasts to Surface-Modified Titanium and Zirconia. Biomaterials 2009, 30, 979–990. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Ruíz, R.A.; Gomez Moreno, G.; Aguilar-Salvatierra, A.; Markovic, A.; Mate-Sánchez, J.E.; Calvo-Guirado, J.L. Human Fetal Osteoblast Behavior on Zirconia Dental Implants and Zirconia Disks with Microstructured Surfaces. An Experimental in Vitro Study. Clin. Oral Implant. Res. 2016, 27, e144–e153. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Two-piece zirconia implants supporting all-ceramic crowns: Six-year results of a prospective cohort study. Clin. Oral Implant. Res. 2021, 32, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Rohr, N.; Balmer, M.; Jung, R.E.; Kohal, R.J.; Spies, B.C.; Hämmerle, C.H.F.; Fischer, J. Influence of Zirconia Implant Surface Topography on First Bone Implant Contact within a Prospective Cohort Study. Clin. Implant. Dent. Relat. Res. 2021, 23, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Wennerberg, A.; Albrektsson, T.; Chrcanovic, B. Long-Term Clinical Outcome of Implants with Different Surface Modifications. Eur. J. Oral Implantol. 2018, 11 (Suppl. S1), S123–S136. [Google Scholar]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of Titanium, Titanium Alloy and Zirconia Dental Implants: Current Knowledge and Open Questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).