
Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
2. Zirconia Applications and Variations
2.1. Structural Properties (Crystalline Phases and Stabilization)
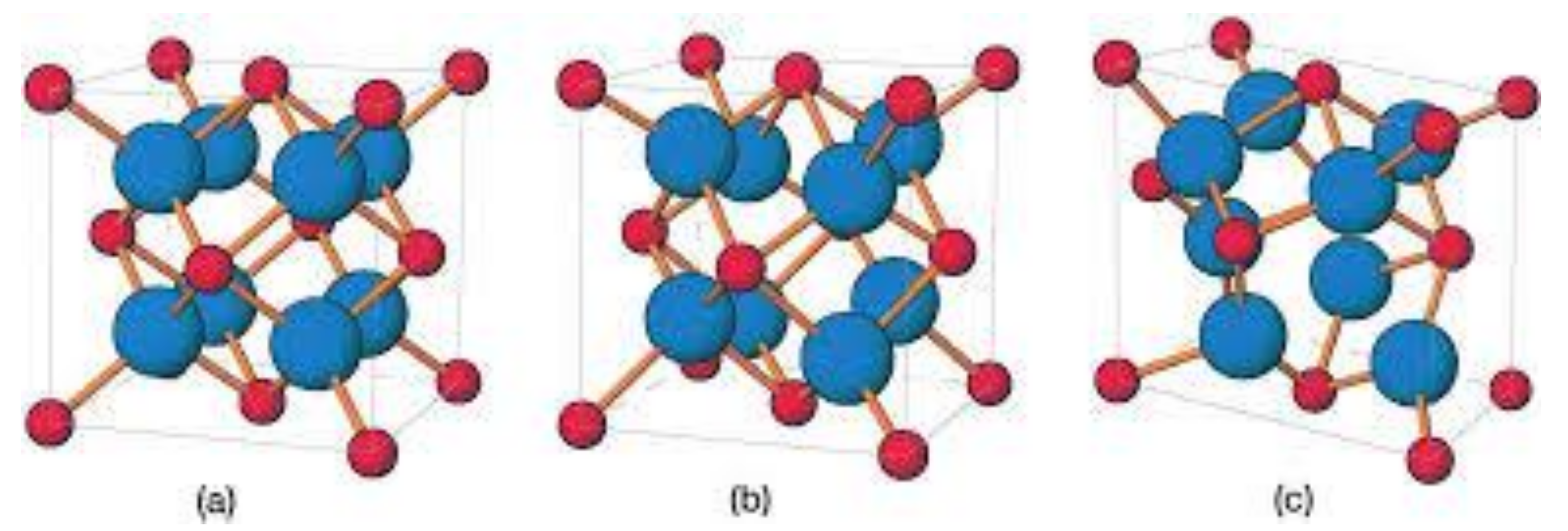
2.1.1. Monoclinic Zirconia
2.1.2. Tetragonal Zirconia
2.1.3. Cubic Zirconia
3. Surface Modifications Aiming at Improved Biological Responses
3.1. Sand Blasting
3.2. Acid Etching
3.3. Selective Infiltration Technique
3.4. Polishing
3.5. Laser Treatment
3.6. Ultraviolet Light Treatment
3.7. Coating
3.8. Biofunctionalization
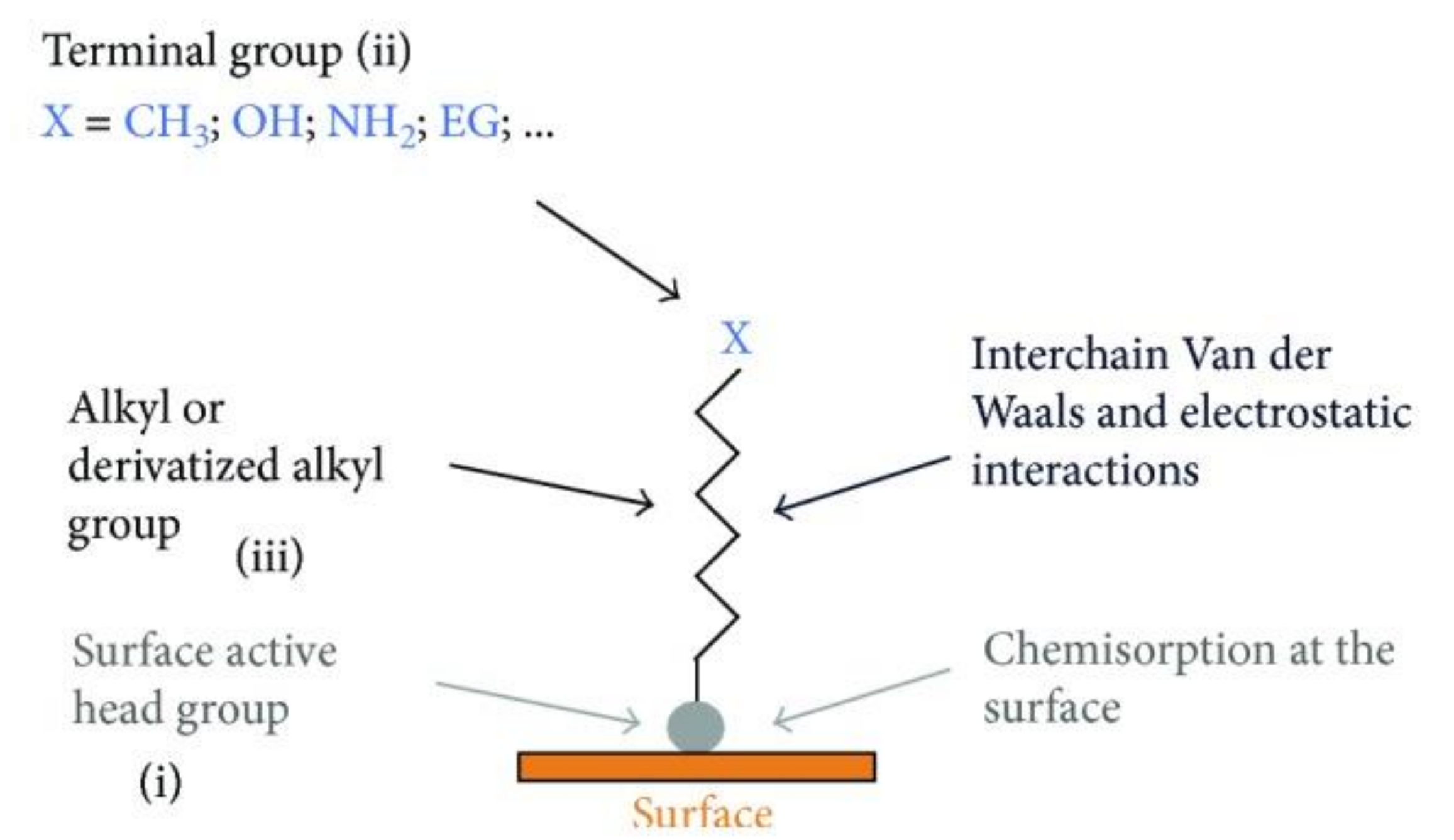
3.9. Self-Assembly
4. Biological Responses
4.1. Blood-Surface Biological Interactions
4.2. Osteoprogenitor Cells
4.3. Fibroblasts and Macrophages
4.4. Epithelial Cells
4.5. Bacterial Cells
5. Clinical Benefits
5.1. Osseointegration of Zirconia Implants
5.2. Clinical Stability of Zirconia Implants
5.3. Clinical Cytotoxicity and Soft Tissue Response to Zirconia Implants
5.4. Limitations
6. Conclusions and Future Challenges
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.; Lawn, B.R. Evaluating dental zirconia. Dent. Mater. 2019, 35, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Moussi, J.; Drury, J.L.; Wataha, J.C. Zirconia in biomedical applications. Expert Rev. Med. Devices 2016, 13, 945–963. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontol. 2000 2017, 73, 22–40. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific trends in clinical research on zirconia dental implants: A bibliometric review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Scarano, A.; Stoppaccioli, M.; Casolino, T. Zirconia crowns cemented on titanium bars using CAD/CAM: A five-year follow-up prospective clinical study of 9 patients. BMC Oral Health 2019, 19, 286. [Google Scholar] [CrossRef]
- Kunrath, M.F. Customized dental implants: Manufacturing processes, topography, osseointegration and future perspectives of 3D fabricated implants. Bioprinting 2020, e00107. [Google Scholar] [CrossRef]
- Wang, W.; Yu, H.; Liu, Y.; Jiang, X.; Gao, B. Trueness analysis of zirconia crowns fabricated with 3-dimensional printing. J. Prosthet. Dent. 2019, 121, 285–291. [Google Scholar] [CrossRef]
- Gupta, S.; Noumbissi, S.; Kunrath, M.F. Nano modified zirconia dental implants: Advances and the frontiers for rapid osseointegration. Med. Devices Sens. 2020, 3, e10076. [Google Scholar] [CrossRef]
- Gnilitskyi, I.; Pogorielov, M.; Viter, R.; Ferraria, A.M.; Carapeto, A.P.; Oleshko, O.; Orazi, L.; Mishchenko, O. Cell and tissue response to nanotextured Ti6Al4V and Zr implants using high-speed femtosecond laser-induced periodic surface structures. Nanomed. Nanotechnol. Biol. Med. 2019, 21, 102036. [Google Scholar] [CrossRef]
- De la Hoz, M.F.T.; Katunar, M.R.; González, A.; Sanchez, A.G.; Díaz, A.O.; Ceré, S. Effect of anodized zirconium implants on early osseointegration process in adult rats: A histological and histomorphometric study. Prog. Biomater. 2019, 8, 249–260. [Google Scholar] [CrossRef]
- Pobloth, A.-M.; Mersiowsky, M.J.; Kliemt, L.; Schell, H.; Dienelt, A.; Pfitzner, B.M.; Burgkart, R.; Detsch, R.; Wulsten, D.; Boccaccini, A.R. Bioactive coating of zirconia toughened alumina ceramic implants improves cancellous osseointegration. Sci. Rep. 2019, 9, 1–16. [Google Scholar] [CrossRef]
- Kunrath, M.F.; Diz, F.M.; Magini, R.; Galárraga-Vinueza, M.E. Nanointeraction: The profound influence of nanostructured and nano-drug delivery biomedical implant surfaces on cell behavior. Adv. Colloid Interface Sci. 2020, 102265. [Google Scholar] [CrossRef]
- Altmann, B.; Rabel, K.; Kohal, R.J.; Proksch, S.; Tomakidi, P.; Adolfsson, E.; Bernsmann, F.; Palmero, P.; Fürderer, T.; Steinberg, T. Cellular transcriptional response to zirconia-based implant materials. Dent. Mater. 2017, 33, 241–255. [Google Scholar] [CrossRef]
- Hanawa, T. Zirconia versus titanium in dentistry: A review. Dent. Mater. J. 2020, 39, 24–36. [Google Scholar] [CrossRef]
- Rottmar, M.; Müller, E.; Guimond-Lischer, S.; Stephan, M.; Berner, S.; Maniura-Weber, K. Assessing the osteogenic potential of zirconia and titanium surfaces with an advanced in vitro model. Dent. Mater. 2019, 35, 74–86. [Google Scholar] [CrossRef]
- Iinuma, Y.; Hirota, M.; Hayakawa, T.; Ohkubo, C. Surrounding tissue response to surface-treated zirconia implants. Materials 2020, 13, 30. [Google Scholar] [CrossRef]
- Da Cruz, M.B.; Marques, J.F.; Fernandes, B.F.; Costa, M.; Miranda, G.; da Mata, A.D.S.P.; Carames, J.M.M.; Silva, F.S. Gingival fibroblasts behavior on bioactive zirconia and titanium dental implant surfaces produced by a functionally graded technique. J. Appl. Oral Sci. 2020, 28. [Google Scholar] [CrossRef]
- Kunrath, M.F.; Monteiro, M.S.; Gupta, S.; Hubler, R.; de Oliveira, S.D. Influence of titanium and zirconia modified surfaces for rapid healing on adhesion and biofilm formation of staphylococcus epidermidis. Arch. Oral Biol. 2020, 117, 104824. [Google Scholar] [CrossRef]
- Roehling, S.; Astasov-Frauenhoffer, M.; Hauser-Gerspach, I.; Braissant, O.; Woelfler, H.; Waltimo, T.; Kniha, H.; Gahlert, M. In vitro biofilm formation on titanium and zirconia implant surfaces. J. Periodontol. 2017, 88, 298–307. [Google Scholar] [CrossRef]
- Pieralli, S.; Kohal, R.-J.; Lopez Hernandez, E.; Doerken, S.; Spies, B.C. Osseointegration of zirconia dental implants in animal investigations: A systematic review and meta-analysis. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2018, 34, 171–182. [Google Scholar] [CrossRef]
- Koller, M.; Steyer, E.; Theisen, K.; Stagnell, S.; Jakse, N.; Payer, M. Two-piece zirconia versus titanium implants after 80 months: Clinical outcomes from a prospective randomized pilot trial. Clin. Oral Implants Res. 2020, 31, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Di Carlo, F.; Quaranta, M.; Piattelli, A. Bone response to zirconia ceramic implants: An experimental study in rabbits. J. Oral Implantol. 2003, 29, 8–12. [Google Scholar] [CrossRef]
- Ekfeldt, A.; Fürst, B.; Carlsson, G.E. Zirconia abutments for single-tooth implant restorations: A 10-to 11-year follow-up study. Clin. Oral Implants Res. 2017, 28, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Rashad, M.M.; Baioumy, H.M. Effect of thermal treatment on the crystal structure and morphology of zirconia nanopowders produced by three different routes. J. Mater. Process. Technol. 2008, 195, 178–185. [Google Scholar] [CrossRef]
- Kelly, J.R.; Denry, I. stabilized zirconia as a structural ceramic: An overview. Dent. Mater. 2008, 24, 289–298. [Google Scholar] [CrossRef]
- Vagkopoulou, T.; Koutayas, S.O.; Koidis, P.; Strub, J.R. Zirconia in dentistry: Part 1. Discovering the nature of an upcoming bioceramic. Eur. J. Esthet. Dent. 2009, 4. [Google Scholar]
- Piconi, C.; Maccauro, G. Zirconia as a ceramic biomaterial. Biomaterials 1999, 20, 1–25. [Google Scholar] [CrossRef]
- Denry, I.; Kelly, J.R. State of the art of zirconia for dental applications. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2008, 24, 299–307. [Google Scholar] [CrossRef]
- Hannink, R.H.J.; Kelly, P.M.; Muddle, B.C. Transformation toughening in zirconia-containing ceramics. J. Am. Ceram. Soc. 2004, 83, 461–487. [Google Scholar] [CrossRef]
- Koutayas, S.O.; Vagkopoulou, T.; Pelekanos, S.; Koidis, P.; Strub, J.R. Zirconia in dentistry: Part 2. evidence-based clinical breakthrough. Eur. J. Esthet. Dent. Off. J. Eur. Acad. Esthet. Dent. 2009, 4, 348–380. [Google Scholar]
- Hempel, U.; Hefti, T.; Kalbacova, M.; Wolf-Brandstetter, C.; Dieter, P.; Schlottig, F. Response of osteoblast-like SAOS-2 Cells to zirconia ceramics with different surface topographies. Clin. Oral Implants Res. 2010, 21, 174–181. [Google Scholar] [CrossRef]
- Strickstrock, M.; Rothe, H.; Grohmann, S.; Hildebrand, G.; Zylla, I.M.; Liefeith, K. Influence of surface roughness of dental zirconia implants on their mechanical stability, cell behavior and osseointegration. BioNanoMaterials 2017, 18. [Google Scholar] [CrossRef]
- Roehling, S.K.; Meng, B.; Cochran, D.L. Sandblasted and acid-etched implant surfaces with or without high surface free energy: Experimental and clinical background. In Implant Surfaces and Their Biological and Clinical Impact; Springer: Berlin/Heidelberg, Germany, 2015; pp. 93–136. [Google Scholar]
- Kohal, R.J.; Bächle, M.; Att, W.; Chaar, S.; Altmann, B.; Renz, A.; Butz, F. Osteoblast and bone tissue response to surface modified zirconia and titanium implant materials. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2013, 29, 763–776. [Google Scholar] [CrossRef]
- Iwaya, Y.; Machigashira, M.; Kanbara, K.; Miyamoto, M.; Noguchi, K.; Izumi, Y.; Ban, S. Surface properties and biocompatibility of acid-etched titanium. Dent. Mater. J. 2008, 27, 415–421. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Freire-Maia, B.; Gomez, R.S. Small central odontogenic fibroma mimicking hyperplastic dental follicle and dentigerous cyst. J. Maxillofac. Oral Surg. 2014, 13, 332–336. [Google Scholar] [CrossRef]
- Hoshing, U.A.; Patil, S.; Medha, A.; Bandekar, S.D. Comparison of shear bond strength of composite resin to enamel surface with laser etching versus acid etching: An in vitro evaluation. J. Conserv. Dent. JCD 2014, 17, 320–324. [Google Scholar] [CrossRef]
- Langhoff, J.D.; Voelter, K.; Scharnweber, D.; Schnabelrauch, M.; Schlottig, F.; Hefti, T.; Kalchofner, K.; Nuss, K.; von Rechenberg, B. Comparison of chemically and pharmaceutically modified titanium and zirconia implant surfaces in dentistry: A study in sheep. Int. J. Oral Maxillofac. Surg. 2008, 37, 1125–1132. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Selective infiltration-etching technique for a strong and durable bond of resin cements to zirconia-based materials. J. Prosthet. Dent. 2007, 98, 379–388. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Osman, E.; Jansen, I.; Everts, V.; Feilzer, A.J. Influence of a nanoporous zirconia implant surface of on cell viability of human osteoblasts. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2013, 22, 190–195. [Google Scholar] [CrossRef]
- Klinge, B.; Meyle, J. Working group 2 soft-tissue integration of implants. consensus report of working group 2. Clin. Oral Implant. Res. 2006, 17, 93–96. [Google Scholar] [CrossRef]
- Kimura, Y.; Matsuzaka, K.; Yoshinari, M.; Inoue, T. Initial attachment of human oral keratinocytes cultured on zirconia or titanium. Dent. Mater. J. 2012, 31, 346–353. [Google Scholar] [CrossRef]
- Yasuno, K.; Kakura, K.; Taniguchi, Y.; Yamaguchi, Y.; Kido, H. Zirconia implants with laser surface treatment peri implant bone response and enhancement of osseointegration. J. Hard Tissue Biol. 2014, 23, 93–100. [Google Scholar] [CrossRef]
- Hao, L.; Lawrence, J. Effects of CO2 laser irradiation on the wettability and human sin fibroblast cell response of magnesia partially stabilized zirconia. Mater. Sci. Eng. C Mater. Biol. Appl. 2003, 23, 627–639. [Google Scholar] [CrossRef]
- Hao, L.; Ma, D.R.; Lawrence, J.; Zhu, X. Enhancing osteoblast functions on a magnesia partially stabilized zirconia bioceramic by means of laser irradiation. Mater. Sci. Eng. C Mater. Biol. Appl. 2005, 25, 496–502. [Google Scholar] [CrossRef]
- Ogawa, T. Ultraviolet photofunctionalization of titanium implants. Int. J. Oral Maxillofac. Implant. 2014, 29, e95-102. [Google Scholar] [CrossRef]
- Hsu, S.K.; Hsu, H.C.; Ho, W.F.; Yao, C.H.; Chang, P.L.; Wu, S.C. Biomolecular modification of zirconia surfaces for enhanced biocompatibility. Thin Solid Films 2014, 572, 91–98. [Google Scholar] [CrossRef]
- Sawase, T.; Jimbo, R.; Baba, K.; Shibata, Y.; Ikeda, T.; Atsuta, M. Photo-induced hydrophilicity enhances initial cell behavior and early bone apposition. Clin. Oral Implant. Res. 2008, 19, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Tengvall, P.; Lundström, I. Physico-chemical considerations of titanium as a biomaterial. Clin. Mater. 1992, 9, 115–134. [Google Scholar] [CrossRef]
- Zhao, G.; Schwartz, Z.; Wieland, M.; Rupp, F.; Geis-Gerstorfer, J.; Cochran, D.L.; Boyan, B.D. High surface energy enhances cell response to titanium substrate microstructure. J. Biomed. Mater. Res. A 2005, 74, 49–58. [Google Scholar] [CrossRef]
- Sartoretto, S.C.; Alves, A.T.N.N.; Resende, R.F.B.; Calasans-Maia, J.; Granjeiro, J.M.; Calasans-Maia, M.D. early osseointegration driven by the surface chemistry and wettability of dental implants. J. Appl. Oral Sci. 2015, 23, 279–287. [Google Scholar] [CrossRef]
- Tuna, T.; Wein, M.; Swain, M.; Fischer, J.; Att, W. Influence of ultraviolet photofunctionalization on the surface characteristics of zirconia-based dental implant materials. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2015, 31, e14–e24. [Google Scholar] [CrossRef]
- Herman, H. Plasma spray deposition processes. MRS Bull. 1988, 13, 60–67. [Google Scholar] [CrossRef]
- Yang, Y.; Kim, K.-H.; Ong, J.L. A Review on Calcium Phosphate Coatings Produced Using a Sputtering Process--an Alternative to Plasma Spraying. Biomaterials 2005, 26, 327–337. [Google Scholar] [CrossRef]
- Pardun, K.; Treccani, L.; Volkmann, E.; Streckbein, P.; Heiss, C.; Li Destri, G.; Marletta, G.; Rezwan, K. Mixed zirconia calcium phosphate coatings for dental implants: Tailoring coating stability and bioactivity potential. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 48, 337–346. [Google Scholar] [CrossRef]
- Zhang, B.; Kwok, C.T.; Cheng, F.T.; Man, H.C. Fabrication of nano-structured HA/CNT coatings on Ti6Al4V by electrophoretic deposition for biomedical applications. J. Nanosci. Nanotechnol. 2011, 11, 10740–10745. [Google Scholar] [CrossRef]
- Sandhyarani, M.; Rameshbabu, N.; Venkateswarlu, K.; Rama Krishna, L. Fabrication, Characterization and in-vitro evaluation of nano structured zirconia/hydroxyapatite composite film on zirconium. Surf. Coat. Technol. 2014, 238, 58–67. [Google Scholar]
- Stanic, V.; Aldini, N.N.; Fini, M.; Giavaresi, G.; Giardino, R.; Krajewski, A.; Ravaglioli, A.; Mazzocchi, M.; Dubini, B.; Bossi, M.G.P.; et al. Osteointegration of bioactive glass-coated zirconia in healthy bone: An in vivo evaluation. Biomaterials 2002, 23, 3833–3841. [Google Scholar] [CrossRef]
- Bosetti, M.; Vernè, E.; Ferraris, M.; Ravaglioli, A.; Cannas, M. In vitro characterisation of zirconia coated by bioactive glass. Biomaterials 2001, 22, 987–994. [Google Scholar] [CrossRef]
- Frandsen, C.J.; Noh, K.; Brammer, K.S.; Johnston, G.; Jin, S. Hybrid micro/nano-topography of a TiO2 nanotube-coated commercial zirconia femoral knee implant promotes bone cell adhesion in vitro. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 2752–2756. [Google Scholar] [CrossRef]
- Morra, M. Biochemical modification of titanium surfaces: Peptides and ECM proteins. Eur. Cells Mater. 2006, 12, 1–15. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Sager, M.; Wieland, M.; Dard, M.; Becker, J. Histological and immunohistochemical analysis of initial and early osseous integration at chemically modified and conventional SLA titanium implants: Preliminary results of a pilot study in dogs. Clin. Oral Implants Res. 2007, 18, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Ruoslahti, E.; Pierschbacher, M.D. New perspectives in cell adhesion: RGD and integrins. Science 1987, 238, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Whitesides, G.M.; Grzybowski, B. Self-assembly at all scales. Science 2002, 295, 2418–2421. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.C.; Correa-Uribe, A.; Martins, M.C.L.; Pelaez-Vargas, A. Self-assembled monolayers for dental implants. Int. J. Dent. 2018, 2018, 4395460. [Google Scholar] [CrossRef]
- Love, J.C.; Estroff, L.A.; Kriebel, J.K.; Nuzzo, R.G.; Whitesides, G.M. Self-assembled monolayers of thiolates on metals as a form of nanotechnology. Chem. Rev. 2005, 105, 1103–1169. [Google Scholar] [CrossRef] [PubMed]
- Ulman, A. Formation and structure of self-assembled monolayers. Chem. Rev. 1996, 96, 1533–1554. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, F.; Quaresima, R.; Canullo, L.; Scarano, A.; Muzio, L.L.; Piattelli, A. Effects of Novel laser dental implant microtopography on human osteoblast proliferation and bone deposition. Int. J. Oral Maxillofac. Implant. 2020, 35, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Shahramian, K.; Abdulmajeed, A.; Kangasniemi, I.; Söderling, E.; Närhi, T. TiO2 coating and UV photofunctionalization enhance blood coagulation on zirconia surfaces. BioMed Res. Int. 2019, 2019, 8078230. [Google Scholar] [CrossRef] [PubMed]
- Traini, T.; Caputi, S.; Gherlone, E.; Degidi, M.; Piattelli, A. Fibrin clot extension on zirconia surface for dental implants: A quantitative in vitro study. Clin. Implant Dent. Relat. Res. 2014, 16, 718–727. [Google Scholar] [CrossRef]
- Mödinger, Y.; Teixeira, G.Q.; Neidlinger-Wilke, C.; Ignatius, A. Role of the complement system in the response to orthopedic biomaterials. Int. J. Mol. Sci. 2018, 19, 3367. [Google Scholar] [CrossRef] [PubMed]
- Campelo, C.S.; Chevallier, P.; Vaz, J.M.; Vieira, R.S.; Mantovani, D. Sulfonated chitosan and dopamine based coatings for metallic implants in contact with blood. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 72, 682–691. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.; Mozafari, M. A critical review on the cellular and molecular interactions at the interface of zirconia-based biomaterials. Ceram. Int. 2018, 44, 16137–16149. [Google Scholar] [CrossRef]
- Bharate, V.; Kumar, Y.; Koli, D.; Pruthi, G.; Jain, V. Effect of different abutment materials (zirconia or titanium) on the crestal bone height in 1 year. J. Oral Biol. Craniofacial Res. 2020, 10, 372–374. [Google Scholar] [CrossRef]
- Kolaczkowska, E.; Kubes, P. Neutrophil recruitment and function in health and inflammation. Nat. Rev. Immunol. 2013, 13, 159–175. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The role of nutrition in periodontal health: An update. Nutrients 2016, 8. [Google Scholar] [CrossRef]
- Munro, T.; Miller, C.M.; Antunes, E.; Sharma, D. Interactions of osteoprogenitor cells with a novel zirconia implant surface. J. Funct. Biomater. 2020, 11, 50. [Google Scholar] [CrossRef]
- Da Costa Fernandes, C.J.; Ferreira, M.R.; Bezerra, F.J.B.; Zambuzzi, W.F. Zirconia stimulates ECM-remodeling as a prerequisite to pre-osteoblast adhesion/proliferation by possible interference with cellular anchorage. J. Mater. Sci. Mater. Med. 2018, 29, 41. [Google Scholar] [CrossRef]
- Katunar, M.R.; Gomez Sanchez, A.; Santos Coquillat, A.; Civantos, A.; Martinez Campos, E.; Ballarre, J.; Vico, T.; Baca, M.; Ramos, V.; Cere, S. In vitro and in vivo characterization of anodised zirconium as a potential material for biomedical applications. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 75, 957–968. [Google Scholar] [CrossRef]
- Mostafa, D.; Aboushelib, M. Bioactive-hybrid-zirconia implant surface for enhancing osseointegration: An in vivo study. Int. J. Implant Dent. 2018, 4, 20. [Google Scholar] [CrossRef]
- Rezaei, N.M.; Hasegawa, M.; Ishijima, M.; Nakhaei, K.; Okubo, T.; Taniyama, T.; Ghassemi, A.; Tahsili, T.; Park, W.; Hirota, M.; et al. Biological and osseointegration capabilities of hierarchically (Meso-/Micro-/Nano-Scale) roughened zirconia. Int. J. Nanomed. 2018, 13, 3381–3395. [Google Scholar] [CrossRef]
- Roehling, S.; Gahlert, M.; Janner, S.; Meng, B.; Woelfler, H.; Cochran, D.L. Ligature-Induced peri-implant bone loss around loaded zirconia and titanium implants. Int. J. Oral Maxillofac. Implants 2019, 34, 357–365. [Google Scholar] [CrossRef]
- Rabel, K.; Kohal, R.-J.; Steinberg, T.; Tomakidi, P.; Rolauffs, B.; Adolfsson, E.; Palmero, P.; Fürderer, T.; Altmann, B. Controlling osteoblast morphology and proliferation via surface micro-topographies of implant biomaterials. Sci. Rep. 2020, 10, 12810. [Google Scholar] [CrossRef]
- Atsuta, I.; Ayukawa, Y.; Kondo, R.; Oshiro, W.; Matsuura, Y.; Furuhashi, A.; Tsukiyama, Y.; Koyano, K. Soft tissue sealing around dental implants based on histological interpretation. J. Prosthodont. Res. 2016, 60, 3–11. [Google Scholar] [CrossRef]
- Yang, Y.; Zheng, M.; Liao, Y.; Zhou, J.; Li, H.; Tan, J. Different behavior of human gingival fibroblasts on surface modified zirconia: A comparison between ultraviolet (UV) light and plasma. Dent. Mater. J. 2019, 38, 756–763. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, Y.; Sculean, A.; Bosshardt, D.D.; Miron, R.J. Macrophage behavior and interplay with gingival fibroblasts cultured on six commercially available titanium, zirconium, and titanium-zirconium dental implants. Clin. Oral Investig. 2019, 23, 3219–3227. [Google Scholar] [CrossRef]
- Fischer, N.G.; Wong, J.; Baruth, A.; Cerutis, D.R. Effect of clinically relevant CAD/CAM zirconia polishing on gingival fibroblast proliferation and focal adhesions. Materials 2017, 10, 1358. [Google Scholar] [CrossRef]
- Rohr, N.; Zeller, B.; Matthisson, L.; Fischer, J. Surface structuring of zirconia to increase fibroblast viability. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2020, 36, 779–786. [Google Scholar] [CrossRef]
- Nishihara, H.; Haro Adanez, M.; Att, W. Current status of zirconia implants in dentistry: Preclinical tests. J. Prosthodont. Res. 2019, 63, 1–14. [Google Scholar] [CrossRef]
- Naveau, A.; Rignon-Bret, C.; Wulfman, C. Zirconia abutments in the anterior region: A systematic review of mechanical and esthetic outcomes. J. Prosthet. Dent. 2019, 121, 775–781. [Google Scholar] [CrossRef]
- Igarashi, K.; Nakahara, K.; Kobayashi, E.; Watanabe, F.; Haga-Tsujimura, M. Hard and soft tissue responses to implant made of three different materials with microgrooved collar in a dog model. Dent. Mater. J. 2018, 37, 964–972. [Google Scholar] [CrossRef]
- Rigolin, M.S.M.; Basso, F.G.; Hebling, J.; de Costa, C.A.S.; de Assis Mollo Junior, F.; Dorigatti de Avila, E. Effect of different implant abutment surfaces on OBA-09 epithelial cell adhesion. Microsc. Res. Tech. 2017, 80, 1304–1309. [Google Scholar] [CrossRef]
- Okabe, E.; Ishihara, Y.; Kikuchi, T.; Izawa, A.; Kobayashi, S.; Goto, H.; Kamiya, Y.; Sasaki, K.; Ban, S.; Noguchi, T.; et al. Adhesion properties of human oral epithelial-derived cells to zirconia. Clin. Implant Dent. Relat. Res. 2016, 18, 906–916. [Google Scholar] [CrossRef]
- Nothdurft, F.P.; Fontana, D.; Ruppenthal, S.; May, A.; Aktas, C.; Mehraein, Y.; Lipp, P.; Kaestner, L. Differential behavior of fibroblasts and epithelial cells on structured implant abutment materials: A comparison of materials and surface topographies. Clin. Implant Dent. Relat. Res. 2015, 17, 1237–1249. [Google Scholar] [CrossRef] [PubMed]
- Atsuta, I.; Ayukawa, Y.; Furuhashi, A.; Narimatsu, I.; Kondo, R.; Oshiro, W.; Koyano, K. Epithelial sealing effectiveness against titanium or zirconia implants surface. J. Biomed. Mater. Res. A 2019, 107, 1379–1385. [Google Scholar] [CrossRef] [PubMed]
- Madeira, S.; Barbosa, A.; Moura, C.G.; Buciumeanu, M.; Silva, F.S.; Carvalho, O. Aunps and Agμps-functionalized zirconia surfaces by hybrid laser technology for dental implants. Ceram. Int. 2020, 46, 7109–7121. [Google Scholar] [CrossRef]
- Riivari, S.; Shahramian, K.; Kangasniemi, I.; Willberg, J.; Närhi, T.O. TiO2-modified zirconia surface improves epithelial cell attachment. Int. J. Oral Maxillofac. Implants 2019, 34, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.-J.; Ryu, J.-S.; Shimono, M.; Lee, K.-W.; Lee, J.-M.; Jung, H.-S. differential healing patterns of mucosal seal on zirconia and titanium implant. Front. Physiol. 2019, 10, 796. [Google Scholar] [CrossRef]
- Shahramian, K.; Gasik, M.; Kangasniemi, I.; Walboomers, X.F.; Willberg, J.; Abdulmajeed, A.; Närhi, T. Zirconia implants with improved attachment to the gingival tissue. J. Periodontol. 2020, 91, 1213–1224. [Google Scholar] [CrossRef]
- Tetè, S.; Zizzari, V.L.; Borelli, B.; De Colli, M.; Zara, S.; Sorrentino, R.; Scarano, A.; Gherlone, E.; Cataldi, A.; Zarone, F. Proliferation and adhesion capability of human gingival fibroblasts onto zirconia, lithium disilicate and feldspathic veneering ceramic in vitro. Dent. Mater. J. 2014, 33, 7–15. [Google Scholar] [CrossRef]
- Singh, B.N.; Veeresh, V.; Mallick, S.P.; Jain, Y.; Sinha, S.; Rastogi, A.; Srivastava, P. Design and evaluation of chitosan/chondroitin sulfate/nano-bioglass based composite scaffold for bone tissue engineering. Int. J. Biol. Macromol. 2019, 133, 817–830. [Google Scholar] [CrossRef]
- Kunrath, M.F.; Dos Santos, R.P.; de Oliveira, S.D.; Hubler, R.; Sesterheim, P.; Teixeira, E.R. Osteoblastic cell behavior and early bacterial adhesion on macro-, micro-, and nanostructured titanium surfaces for biomedical implant applications. Int. J. Oral Maxillofac. Implants 2020, 35, 773–781. [Google Scholar] [CrossRef]
- Degidi, M.; Artese, L.; Scarano, A.; Perrotti, V.; Gehrke, P.; Piattelli, A. Inflammatory infiltrate, microvessel density, nitric oxide synthase expression, vascular endothelial growth factor expression, and proliferative activity in peri-implant soft tissues around titanium and zirconium oxide healing caps. J. Periodontol. 2006, 77, 73–80. [Google Scholar] [CrossRef]
- Scarano, A.; Piattelli, M.; Caputi, S.; Favero, G.A.; Piattelli, A. Bacterial adhesion on commercially pure titanium and zirconium oxide disks: An in vivo human study. J. Periodontol. 2004, 75, 292–296. [Google Scholar] [CrossRef]
- Do Nascimento, C.; Pita, M.S.; Fernandes, F.H.N.C.; Pedrazzi, V.; de Albuquerque, R.F., Jr.; Ribeiro, R.F. Bacterial adhesion on the titanium and zirconia abutment surfaces. Clin. Oral Implants Res. 2014, 25, 337–343. [Google Scholar] [CrossRef]
- Moritz, J.; Abram, A.; Čekada, M.; Gabor, U.; Garvas, M.; Zdovc, I.; Kocjan, A. Nanoroughening of sandblasted 3Y-TZP surface by alumina coating deposition for improved osseointegration and bacteria reduction. J. Eur. Ceram. Soc. 2019, 39, 4347–4357. [Google Scholar] [CrossRef]
- Pérez-Tanoira, R.; Horwat, D.; Kinnari, T.J.; Pérez-Jorge, C.; Gómez-Barrena, E.; Migot, S.; Esteban, J. Bacterial adhesion on biomedical surfaces covered by yttria stabilized zirconia. J. Mater. Sci. Mater. Med. 2016, 27, 6. [Google Scholar] [CrossRef][Green Version]
- Han, A.; Tsoi, J.K.H.; Lung, C.Y.K.; Matinlinna, J.P. An introduction of biological performance of zirconia with different surface characteristics: A review. Dent. Mater. J. 2020, 39, 523–530. [Google Scholar] [CrossRef]
- Han, A.; Tsoi, J.K.; Rodrigues, F.P.; Leprince, J.G.; Palin, W.M. Bacterial adhesion mechanisms on dental implant surfaces and the influencing factors. Int. J. Adhes. Adhes. 2016, 69, 58–71. [Google Scholar] [CrossRef]
- Zechner, W.; Tangl, S.; Fürst, G.; Tepper, G.; Thams, U.; Mailath, G.; Watzek, G. Osseous healing characteristics of three different implant types. Clin. Oral Implants Res. 2003, 14, 150–157. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 2—Review focusing on clinical knowledge of different surfaces. Int. J. Prosthodont. 2004, 17, 544–564. [Google Scholar]
- Sollazzo, V.; Pezzetti, F.; Scarano, A.; Piattelli, A.; Bignozzi, C.A.; Massari, L.; Brunelli, G.; Carinci, F. Zirconium oxide coating improves implant osseointegration in vivo. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2008, 24, 357–361. [Google Scholar] [CrossRef]
- Akagawa, Y.; Ichikawa, Y.; Nikai, H.; Tsuru, H. Interface histology of unloaded and early loaded partially stabilized zirconia endosseous implant in initial bone healing. J. Prosthet. Dent. 1993, 69, 599–604. [Google Scholar] [CrossRef]
- Akagawa, Y.; Hosokawa, R.; Sato, Y.; Kamayama, K. Comparison between freestanding and tooth-connected partially stabilized zirconia implants after two years’ function in monkeys: A clinical and histologic study. J. Prosthet. Dent. 1998, 80, 551–558. [Google Scholar] [CrossRef]
- Stadlinger, B.; Hennig, M.; Eckelt, U.; Kuhlisch, E.; Mai, R. Comparison of zirconia and titanium implants after a short healing period. a pilot study in minipigs. Int. J. Oral Maxillofac. Surg. 2010, 39, 585–592. [Google Scholar] [CrossRef]
- Dubruille, J.H.; Viguier, E.; Le Naour, G.; Dubruille, M.T.; Auriol, M.; Le Charpentier, Y. Evaluation of combinations of titanium, zirconia, and alumina implants with 2 bone fillers in the dog. Int. J. Oral Maxillofac. Implants 1999, 14, 271–277. [Google Scholar]
- Kohal, R.-J.; Papavasiliou, G.; Kamposiora, P.; Tripodakis, A.; Strub, J.R. Three-dimensional computerized stress analysis of commercially pure titanium and yttrium-partially stabilized zirconia implants. Int. J. Prosthodont. 2002, 15, 189–194. [Google Scholar]
- Gahlert, M.; Röhling, S.; Wieland, M.; Sprecher, C.M.; Kniha, H.; Milz, S. Osseointegration of zirconia and titanium dental implants: A histological and histomorphometrical study in the maxilla of pigs. Clin. Oral Implants Res. 2009, 20, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Gahlert, M.; Roehling, S.; Sprecher, C.M.; Kniha, H.; Milz, S.; Bormann, K. In vivo performance of zirconia and titanium implants: A histomorphometric study in mini pig maxillae. Clin. Oral Implants Res. 2012, 23, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Noumbissi, S.; Scarano, A.; Gupta, S. A Literature review study on atomic ions dissolution of titanium and its alloys in implant dentistry. Materials 2019, 12, 368. [Google Scholar] [CrossRef] [PubMed]
- Klokkevold, P.R.; Nishimura, R.D.; Adachi, M.; Caputo, A. Osseointegration enhanced by chemical etching of the titanium surface. a torque removal study in the rabbit. Clin. Oral Implants Res. 1997, 8, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Sennerby, L.; Dasmah, A.; Larsson, B.; Iverhed, M. Bone tissue responses to surface-modified zirconia implants: A histomorphometric and removal torque study in the rabbit. Clin. Implant Dent. Relat. Res. 2005, 7, S13–S20. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Scarano, A.; Piattelli, M. Detection of alkaline and acid phosphatases around titanium implants: A light microscopical and histochemical study in rabbits. Biomaterials 1995, 16, 1333–1338. [Google Scholar] [CrossRef]
- Alzubaydi, T.L.; Alameer, S.S.; Ismaeel, T.; Alhijazi, A.Y.; Geetha, M. In vivo studies of the ceramic coated titanium alloy for enhanced osseointegration in dental applications. J. Mater. Sci. Mater. Med. 2009, 20, S35–S42. [Google Scholar] [CrossRef]
- Ferguson, S.J.; Langhoff, J.D.; Voelter, K.; von Rechenberg, B.; Scharnweber, D.; Bierbaum, S.; Schnabelrauch, M.; Kautz, A.R.; Frauchiger, V.M.; Mueller, T.L.; et al. Biomechanical comparison of different surface modifications for dental implants. Int. J. Oral Maxillofac. Implants 2008, 23, 1037–1046. [Google Scholar]
- Liagre, B.; Moalic, S.; Vergne, P.; Charissoux, J.L.; Bernache-Assollant, D.; Beneytout, J.L. Effects of alumina and zirconium dioxide particles on arachidonic acid metabolism and proinflammatory interleukin production in osteoarthritis and rheumatoid synovial cells. J. Bone Jt. Surg. Br. 2002, 84, 920–930. [Google Scholar] [CrossRef]
- Ito, A.; Tateishi, T.; Niwa, S.; Tange, S. In-vitro evaluation of the cytocompatibility of wear particles generated by UHMWPE/zirconia friction. Clin. Mater. 1993, 12, 203–209. [Google Scholar] [CrossRef]
- Hisbergues, M.; Vendeville, S.; Vendeville, P. Zirconia: Established facts and perspectives for a biomaterial in dental implantology. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 519–529. [Google Scholar] [CrossRef]
- Christel, P.; Meunier, A.; Heller, M.; Torre, J.P.; Peille, C.N. Mechanical properties and short-term in-vivo evaluation of yttrium-oxide-partially-stabilized zirconia. J. Biomed. Mater. Res. 1989, 23, 45–61. [Google Scholar] [CrossRef]
- Ichikawa, Y.; Akagawa, Y.; Nikai, H.; Tsuru, H. Tissue compatibility and stability of a new zirconia ceramic in vivo. J. Prosthet. Dent. 1992, 68, 322–326. [Google Scholar] [CrossRef]
- Helmer, J.C.; Driskell, T.D. Research on Bioceramics: Symposium on Use of Ceramics as Surgical Implants; Clemson University: Clemson, SC, USA, 1969. [Google Scholar]
- Gredes, T.; Kubasiewicz-Ross, P.; Gedrange, T.; Dominiak, M.; Kunert-Keil, C. comparison of surface modified zirconia implants with commercially available zirconium and titanium implants: A histological study in pigs. Implant Dent. 2014, 23, 502–507. [Google Scholar] [CrossRef]
- Tetè, S.; Mastrangelo, F.; Bianchi, A.; Zizzari, V.; Scarano, A. collagen fiber orientation around machined titanium and zirconia dental implant necks: An animal study. Int. J. Oral Maxillofac. Implants 2009, 24, 52–58. [Google Scholar]
- Van Brakel, R.; Meijer, G.J.; Verhoeven, J.W.; Jansen, J.; de Putter, C.; Cune, M.S. Soft tissue response to zirconia and titanium implant abutments: An in vivo within-subject comparison. J. Clin. Periodontol. 2012, 39, 995–1001. [Google Scholar] [CrossRef]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implants Res. 2008, 19, 635–641. [Google Scholar] [CrossRef]
- Zembic, A.; Sailer, I.; Jung, R.E.; Hämmerle, C.H.F. Randomized-controlled clinical trial of customized zirconia and titanium implant abutments for single-tooth implants in canine and posterior regions: 3-year results. Clin. Oral Implants Res. 2009, 20, 802–808. [Google Scholar] [CrossRef]
- Kajiwara, N.; Masaki, C.; Mukaibo, T.; Kondo, Y.; Nakamoto, T.; Hosokawa, R. soft tissue biological response to zirconia and metal implant abutments compared with natural tooth: Microcirculation monitoring as a novel bioindicator. Implant Dent. 2015, 24, 37–41. [Google Scholar] [CrossRef]
- Liñares, A.; Grize, L.; Muñoz, F.; Pippenger, B.E.; Dard, M.; Domken, O.; Blanco-Carrión, J. Histological assessment of hard and soft tissues surrounding a novel ceramic implant: A pilot study in the Minipig. J. Clin. Periodontol. 2016, 43, 538–546. [Google Scholar] [CrossRef]
- Han, J.; Zhang, F.; van Meerbeek, B.; Vleugels, J.; Braem, A.; Castagne, S. Laser surface texturing of zirconia-based ceramics for dental applications: A review. Mater. Sci. Eng. C 2021, 112034. [Google Scholar] [CrossRef]
- Lorenz, J.; Giulini, N.; Hölscher, W.; Schwiertz, A.; Schwarz, F.; Sader, R. Prospective controlled clinical study investigating long-term clinical parameters, patient satisfaction, and microbial contamination of zirconia implants. Clin. Implant Dent. Rel. Res. 2019, 21, 263–271. [Google Scholar] [CrossRef]
- Preis, V.; Kammermeier, A.; Handel, G.; Rosentritt, M. In vitro performance of two-piece zirconia implant systems for anterior application. Dent. Mater. 2016, 32, 765–774. [Google Scholar] [CrossRef]
- Peters, O.A.; Du, D.; Ho, M.Y.; Chu, R.; Moule, A. Assessing the cutting efficiency of different burs on zirconia substrate. Aust. Endod. J. 2019, 45, 289–297. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Zirconia Implants Surface Treatments | ||||
|---|---|---|---|---|
| Treatment | Procedure | Disadvantages | Characteristics | References |
| Sandblasting | High pressure alumina (Al2O3) release | Surface micro-cracks, Structural stress, contaminations | Low cost, hardness and needle-like shape | [31,33] |
| Acid etching | Combinations of: (1) ≃48% hydrofluoric acid (HF) (2) ≃70% nitric acid (HNO3) (3) ≃98% Sulfuric acid (H2SO4) | Undesired chemical changes | Remove the alumina contamination. Micro scale surface texture for bone to implant contact interface | [35,36,37] |
| Selective infiltration technique | Coating and glass heating procedure | Extended only to the surface grains | Nano-porous surface | [39,40] |
| Polishing | Silicon carbide polishing paper with diamond or silica suspension | Smoother surface compared to acid etching and sandblasting | Average surface roughness between 8 and 200 nm. No surface chemistry modifications. | [40,41,42] |
| Laser treatment | (1) CO2 laser (2) ER:YAG (3) Cr:YSGG | Disrupts chemical structure | No surface contamination. Improve material wettability | [43,44,45] |
| Ultraviolet light treatment (UVC) | UVC photons | No effects on surface roughness and surface chemistry | Effect of superhydrophilicity | [46,47,48,49,50,51,52] |
| Coating | Obtained by electrophoretic deposition (EPD) and plasma-spraying: (1) Reinforced hydroxyapatite (HA) (2) Calcium Phosphate (Ca(PO)4) (3) Bioglaze (RKKP) | Coating-implant bond strength and modification of chemical structure | Low cost and a high deposition rate. Good biocompatibility, corrosion resistance, and bioactivity | [53,54,55,56,57,58,59,60] |
| Biofunctionalization | (1) Immobilized arginine—glycine—aspartate (RGD) | Structural chemical changes | Improved biochemical properties and biological responses | [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63] |
| Self-assembly | Self-assembled monolayers of active organic compound and terminal functionalization | Van der Waals layer interactions | Surface vapor deposition of active organic compound and molecule adhesion | [64,65,66,67,68] |
| ZrO2-Derivates Interactions | ||||
|---|---|---|---|---|
| Cellular and Tissular Response | Tissue | Cells | Effects | References |
| Connective tissue cells | Fibroblasts Macrophages | -Increased cells migration and proliferation. -Fibronectin and vitronectin release. -Collagen and extracellular matrix proteins release. -Better cellular activity with hydrophilic surfaces. | [85,86,87,88,89,90,91,92] | |
| Blood cells | Erythrocytes Platelets | -Fibrinogen cascade activation. -Plasma proteins activation. | [71,72,73,74] | |
| Defense cells | Neutrophils, Leukocytes | -Histamine release. -Mast cell degranulation. | [71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101] | |
| Epithelium tissue | Epithelial cells | -Increased differentiation and proliferation. -Faster healing process and protective scarring. | [93,94,95,96,97] | |
| Osteoprogenitors | Osteoblasts | -Increased migration and proliferation. -Increased activity of osteopontin, osteocalcin, BMP-2 genes.-Osteoprogenitors sells adherence and proliferation. | [77,78,79,80,81,82,83,84] | |
| Oral biofilms cells | Bacteria cells | -Lower bacterial adhesion and proliferation. -Reduced bacteria activity. | [102,103,104,105,106,107,108,109,110] | |
| Bone Tissue Response to ZrO2 | |||
|---|---|---|---|
| Effect | Author | Effectiveness | Reference |
| Implant Loading | Akagawa et al. Stadlinger et al. | No bone-implant contact (BIC) with significant difference between the loaded and unloaded zirconia implants (BIC loaded: 81.9%; BIC unloaded: 69.8%). No BIC significant difference submerged zirconia and the non-submerged zirconia implants. | [114,116] |
| Chemical Property | Gahlert et al. Noumbissi et al. Sollazzo et al. | No difference of bone formation pattern in direct contact with zirconia and surface-modified titanium implant surfaces. Zirconia oxide high resistance to corrosion and ions release. Higher BIC percentage of zirconia implant compared to titanium implant. | [113,119,121] |
| Surface Treatments | Sennerby et al. | Sandblasted zirconia implants can achieve a higher stability in bone than machined zirconia implants. | [123] |
| Biocompatibility | Liagre et al. Hisbergues et al. Helmer et al. | No pseudo-teratogen effect. No evidence of high cytotoxicity or inflammation. No evidence of local bone reaction associated to the alumina treatment. | [127,129,132] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kunrath, M.F.; Gupta, S.; Lorusso, F.; Scarano, A.; Noumbissi, S. Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review. Materials 2021, 14, 2825. https://doi.org/10.3390/ma14112825
Kunrath MF, Gupta S, Lorusso F, Scarano A, Noumbissi S. Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review. Materials. 2021; 14(11):2825. https://doi.org/10.3390/ma14112825
Chicago/Turabian StyleKunrath, Marcel F., Saurabh Gupta, Felice Lorusso, Antonio Scarano, and Sammy Noumbissi. 2021. "Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review" Materials 14, no. 11: 2825. https://doi.org/10.3390/ma14112825
APA StyleKunrath, M. F., Gupta, S., Lorusso, F., Scarano, A., & Noumbissi, S. (2021). Oral Tissue Interactions and Cellular Response to Zirconia Implant-Prosthetic Components: A Critical Review. Materials, 14(11), 2825. https://doi.org/10.3390/ma14112825