Design of 3D Additively Manufactured Hybrid Structures for Cranioplasty



 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Modified Bone Cement
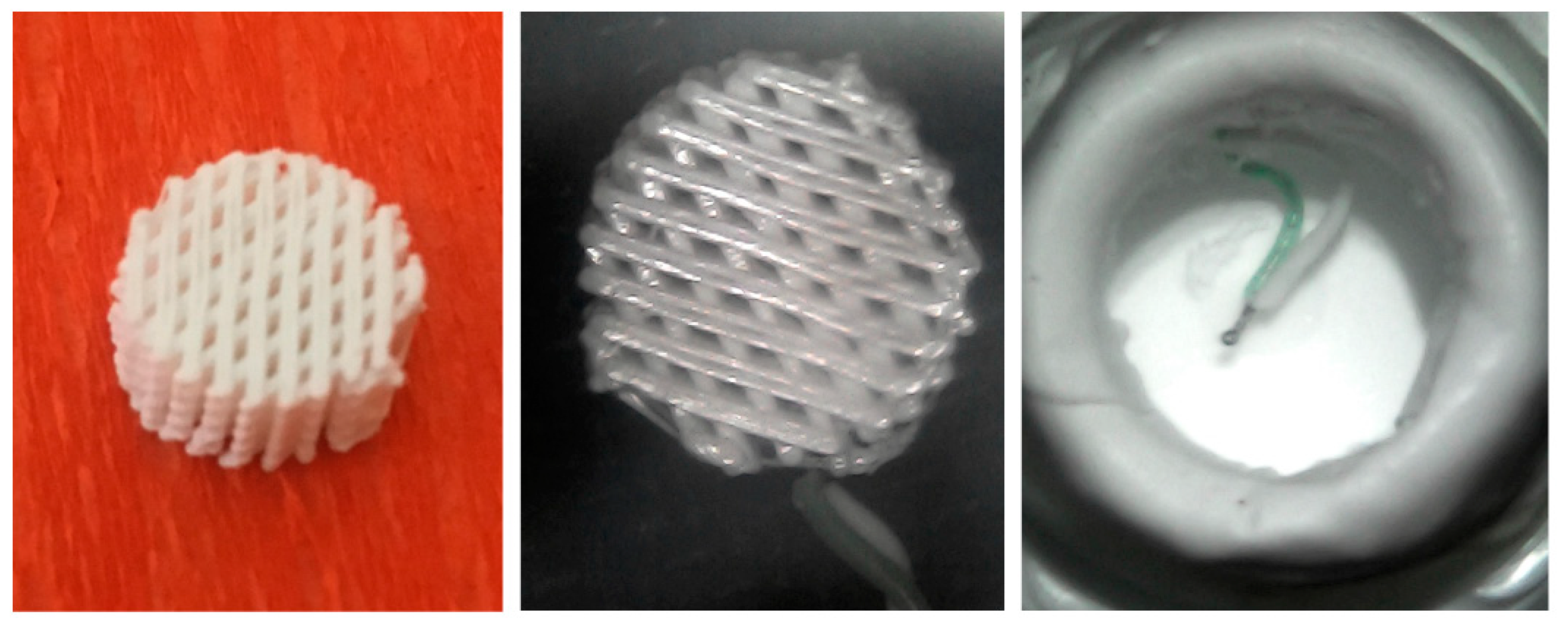
2.2. Design and Fabrication of 3D Additive Manufactured Porous Structures
2.3. Temperature Profile Evaluation
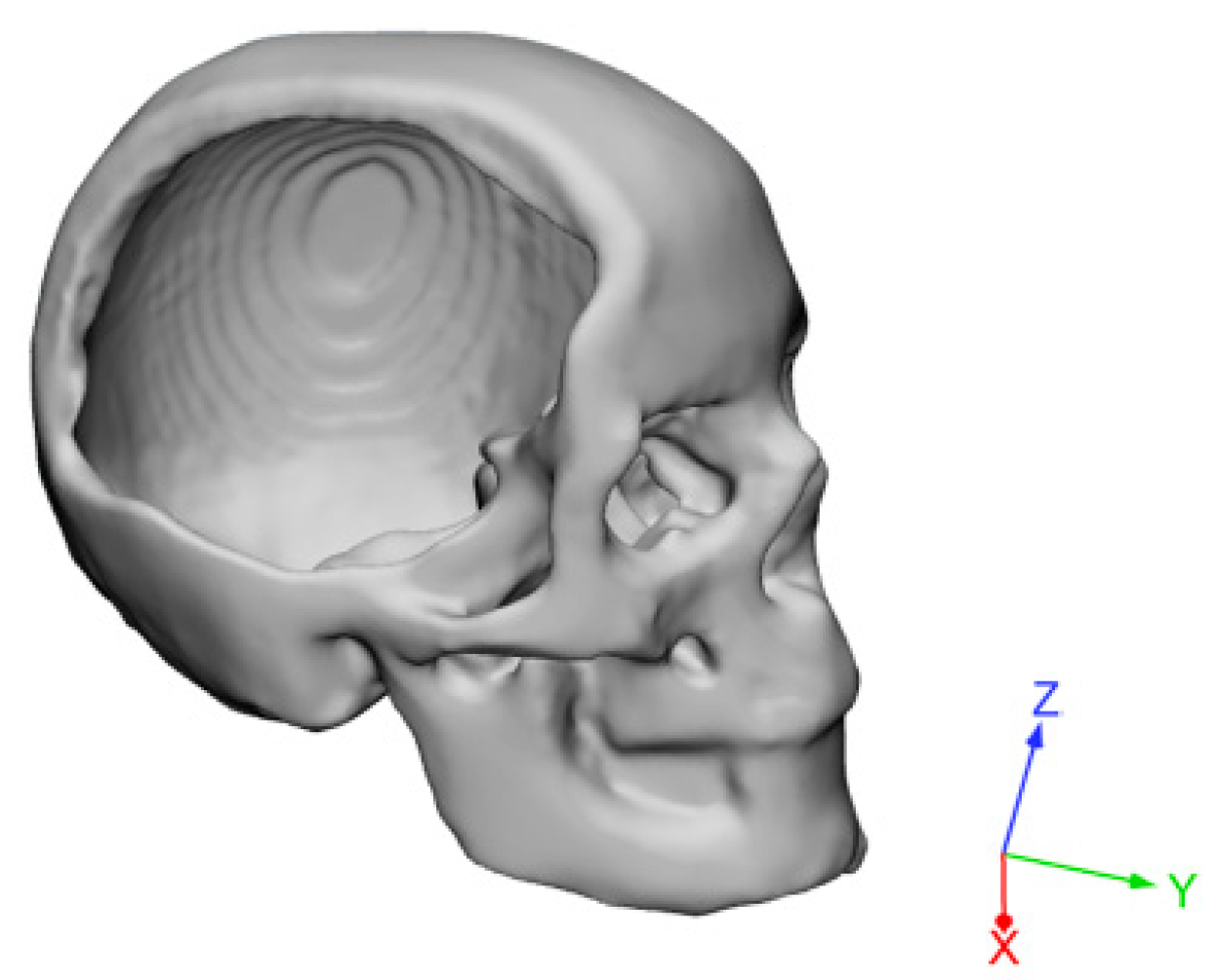
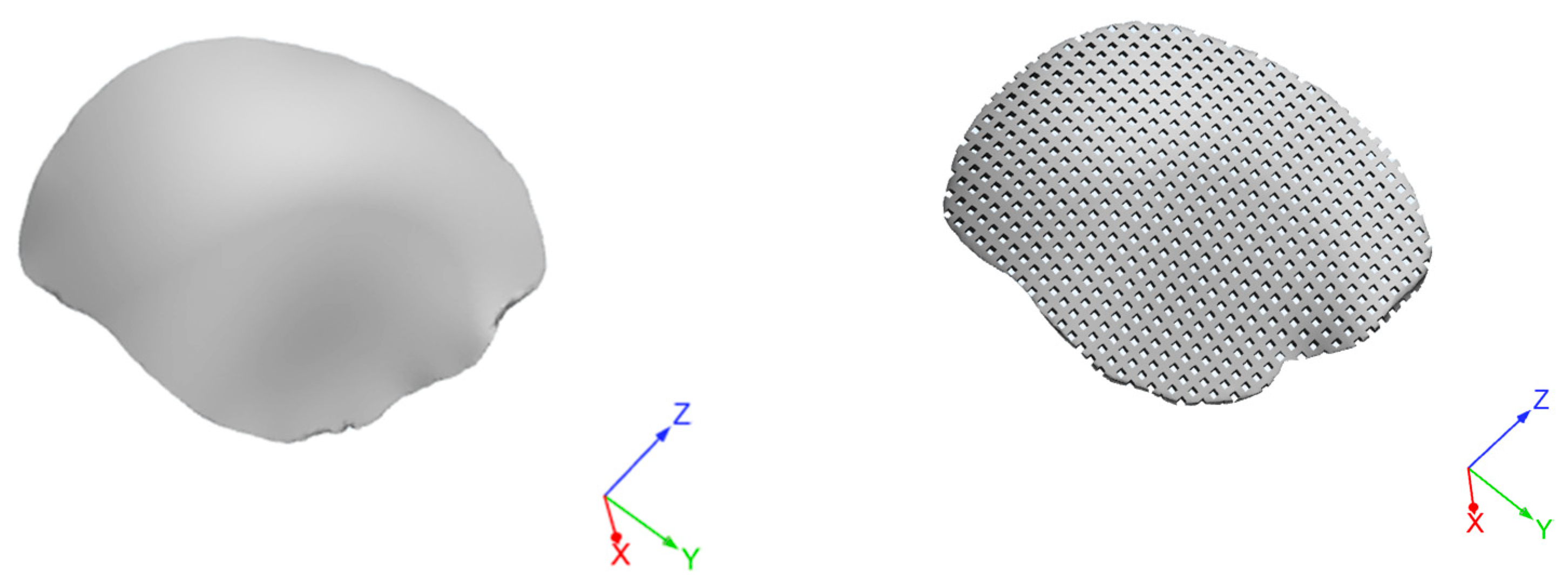
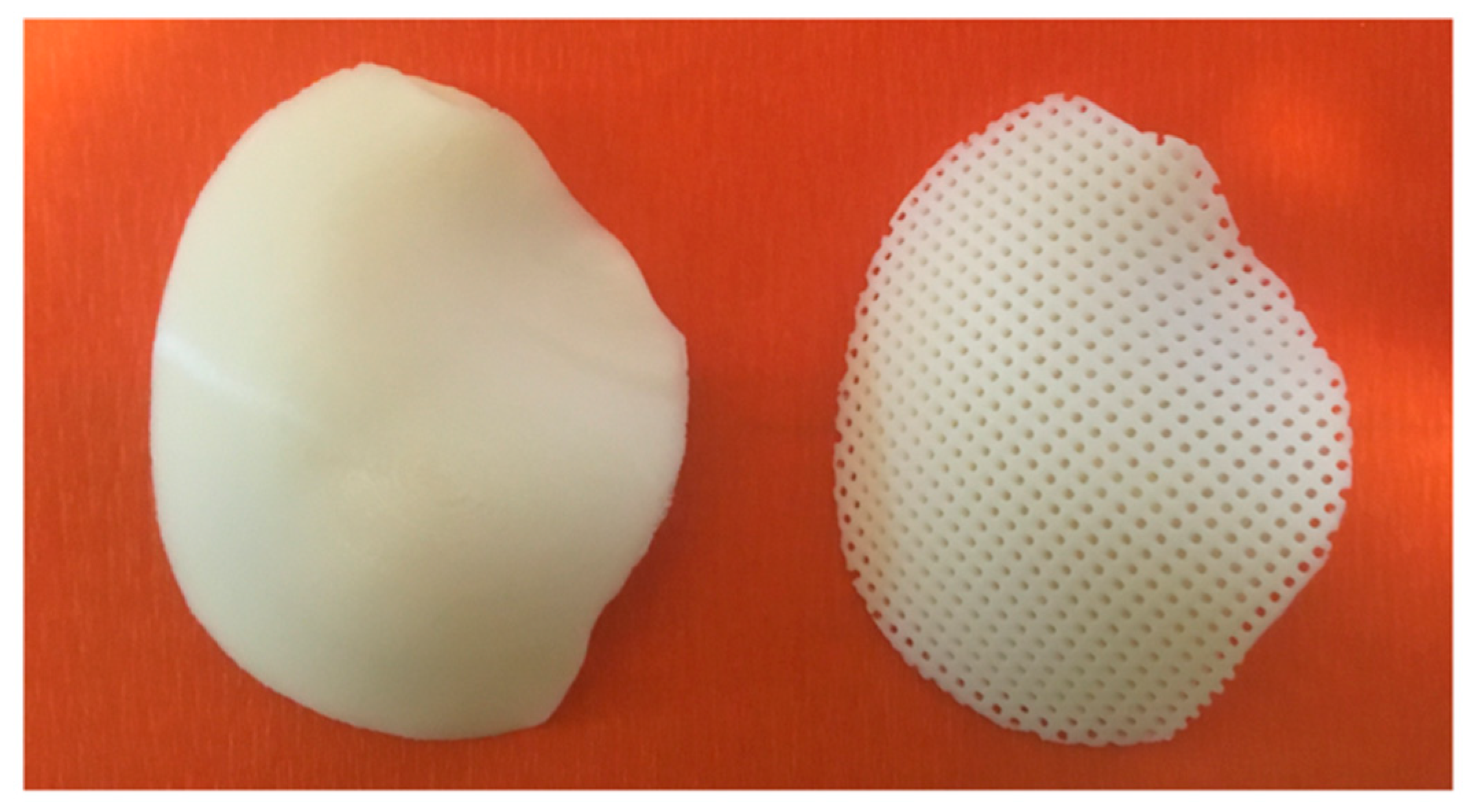
2.4. Design and Fabrication of 3D Customized Hybrid Devices for Large Cranial Defects
2.5. Theoretical Impact Analysis
3. Results and Discussion
4. Conclusions
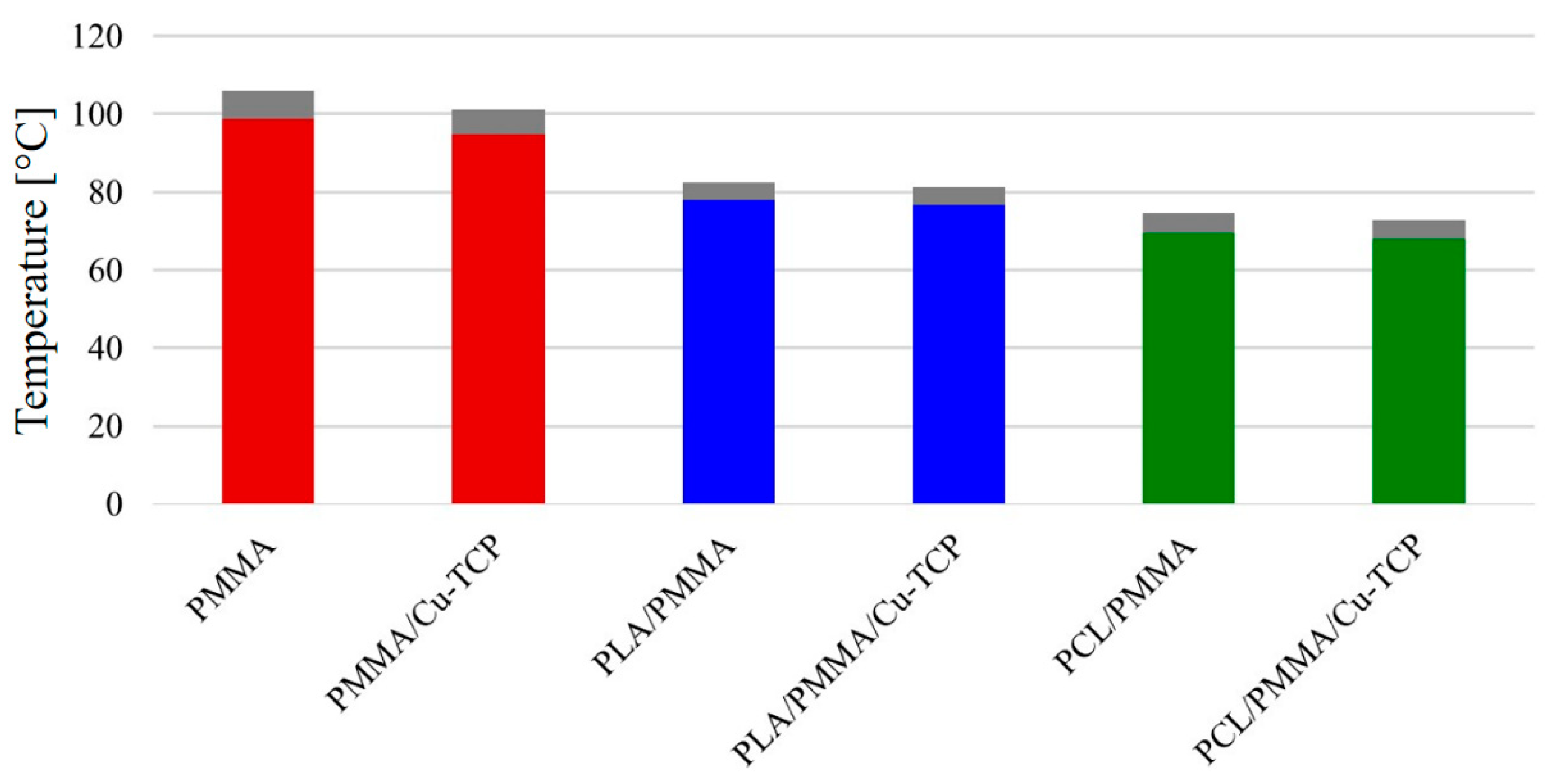
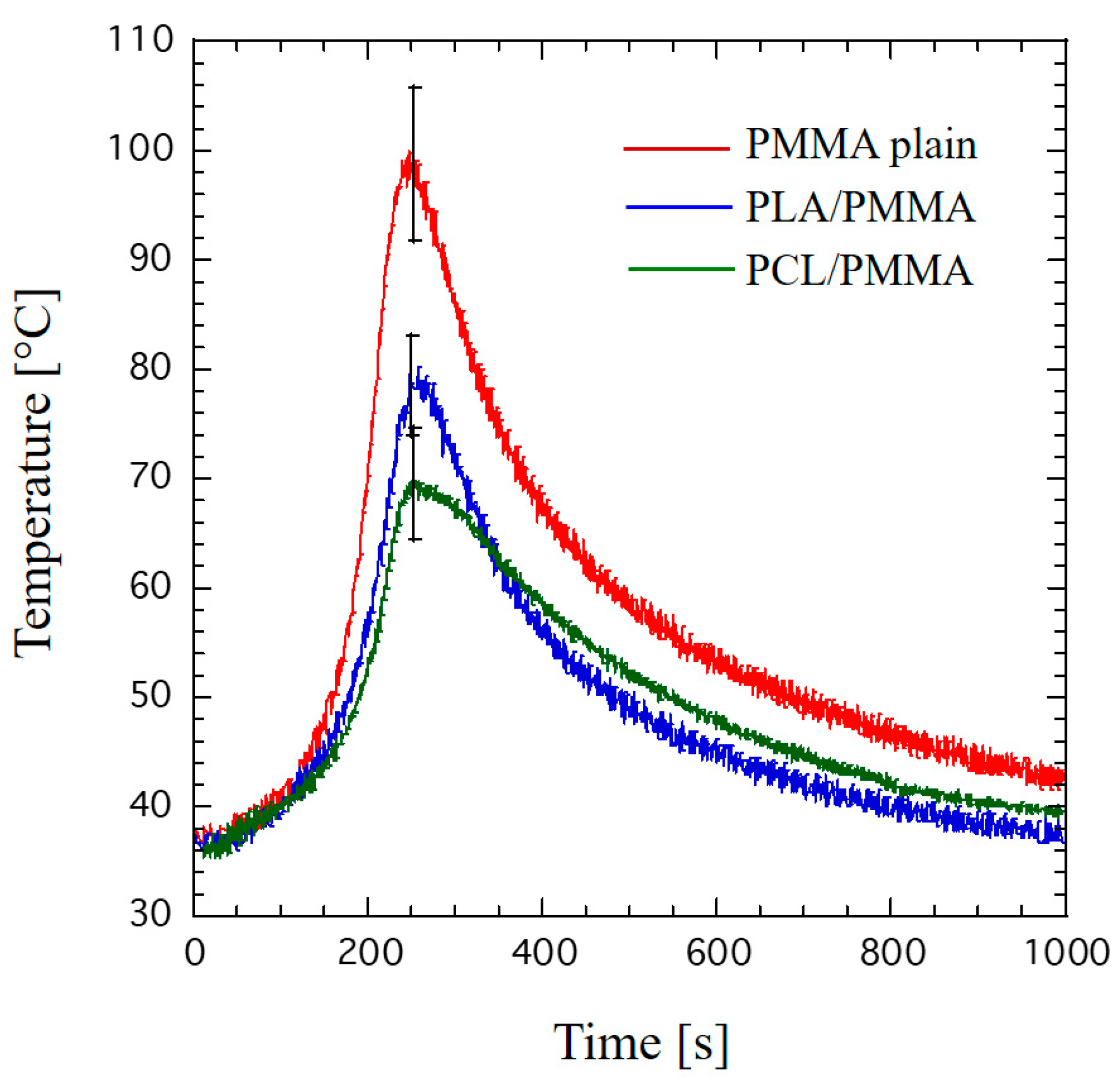
- Peak temperatures measured for hybrid PCL/PMMA (69.5 ± 5.1 °C) and PCL/PMMA/Cu-TCP (67.8 ± 4.9 °C) were lower than those found for the PLA-based ones.
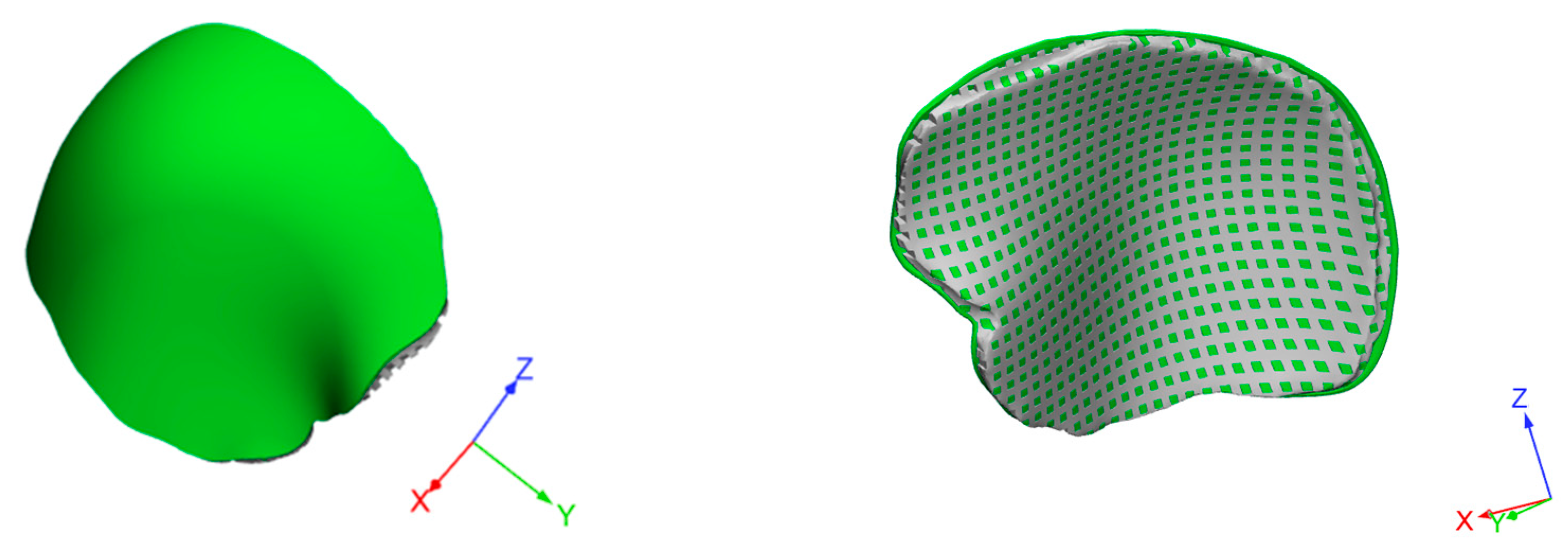
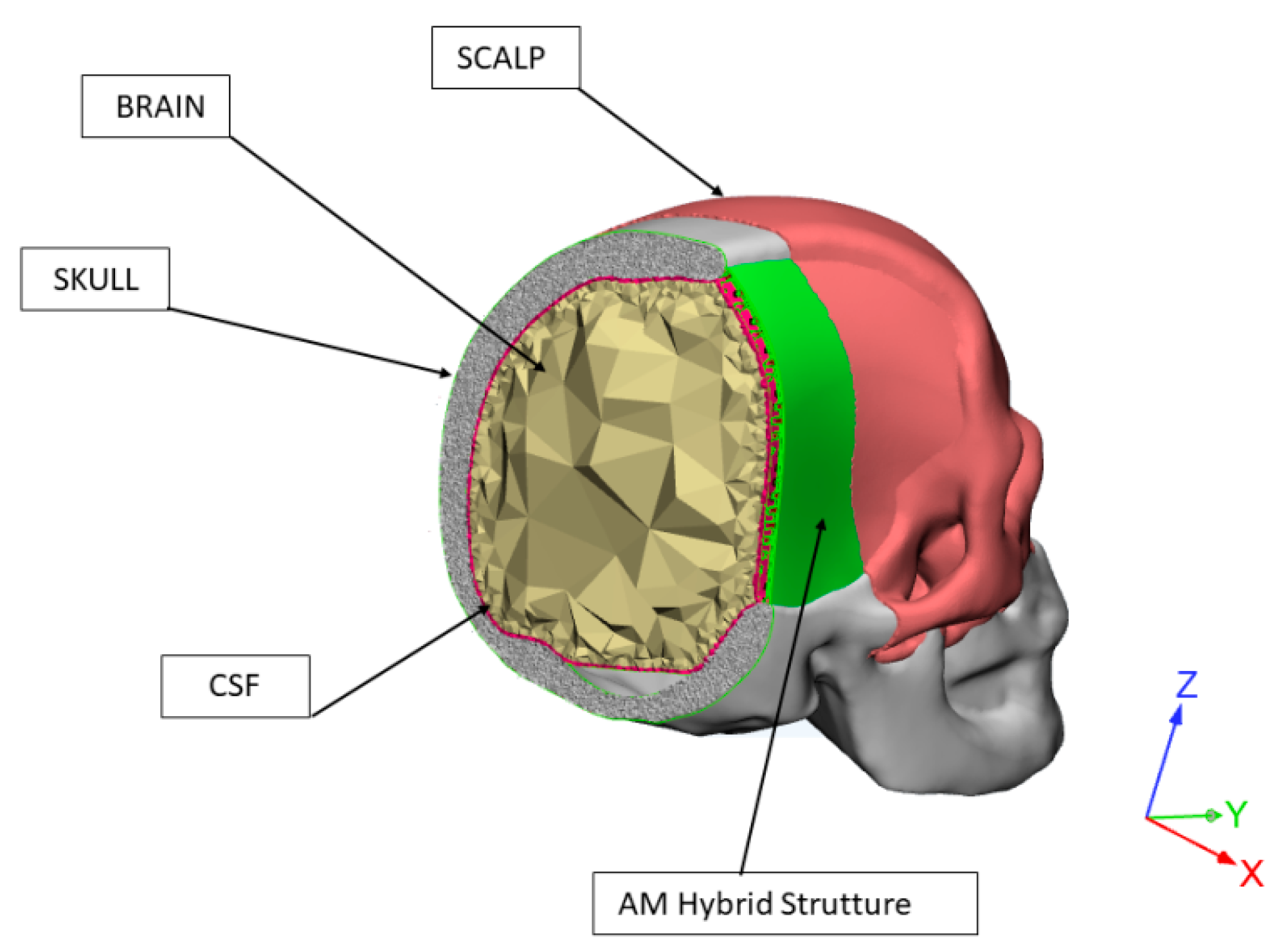
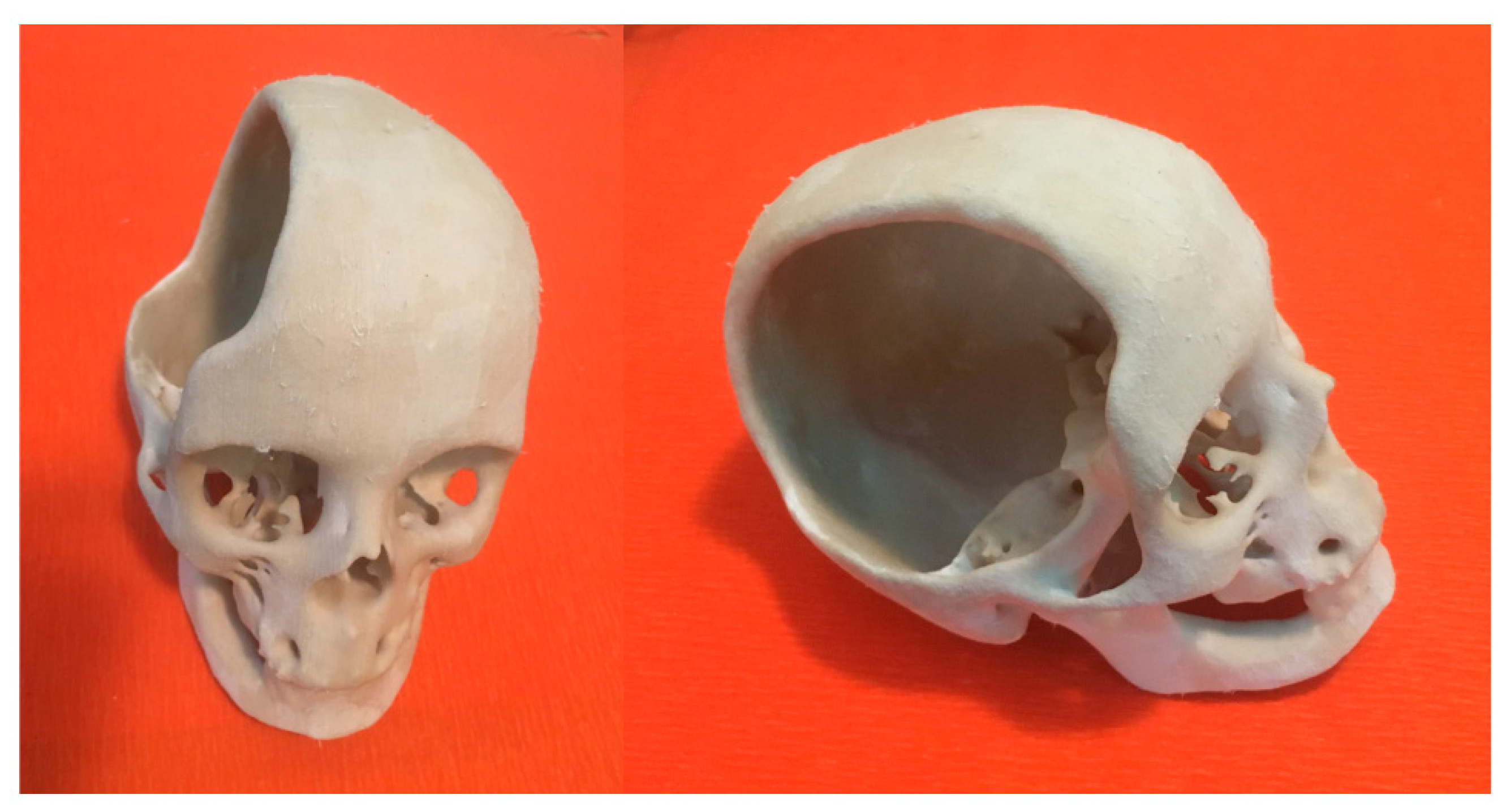
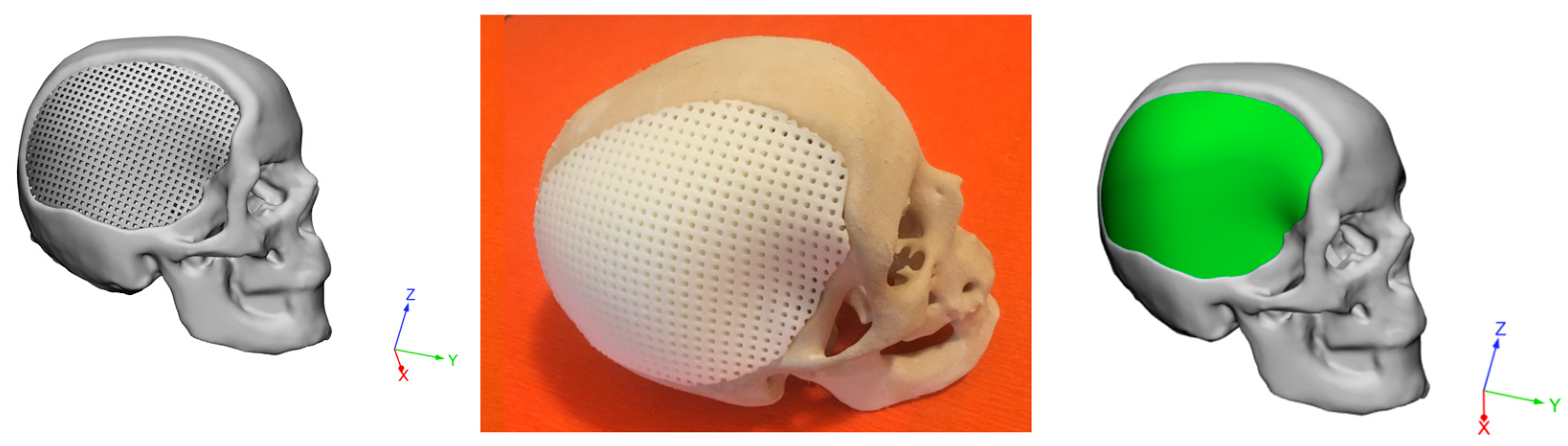
- An integrated design strategy was employed to develop 3D hybrid devices for large cranial defects, involving RE, AM and a modified PMMA bone cement (PMMA/Cu-TCP 97.5/2.5 w/w). The feasibility of the proposed technical solutions was validated through virtual and physical models.
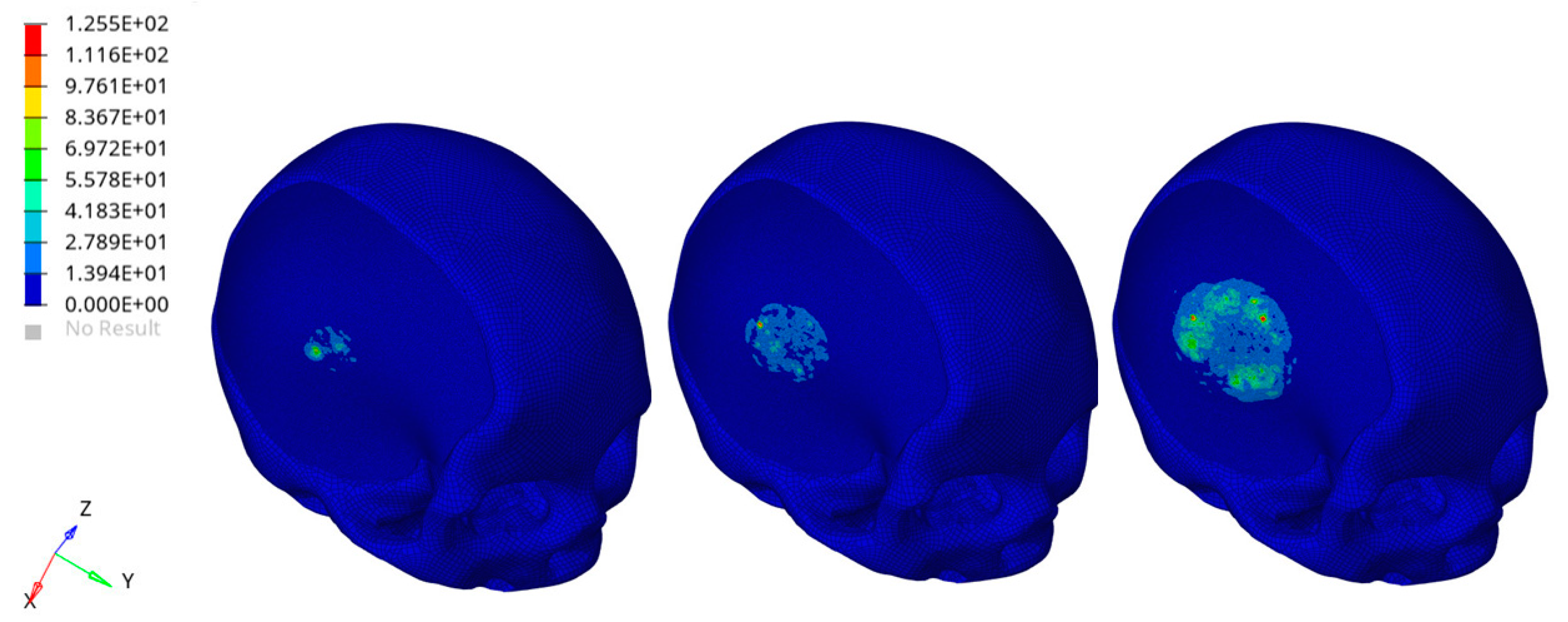
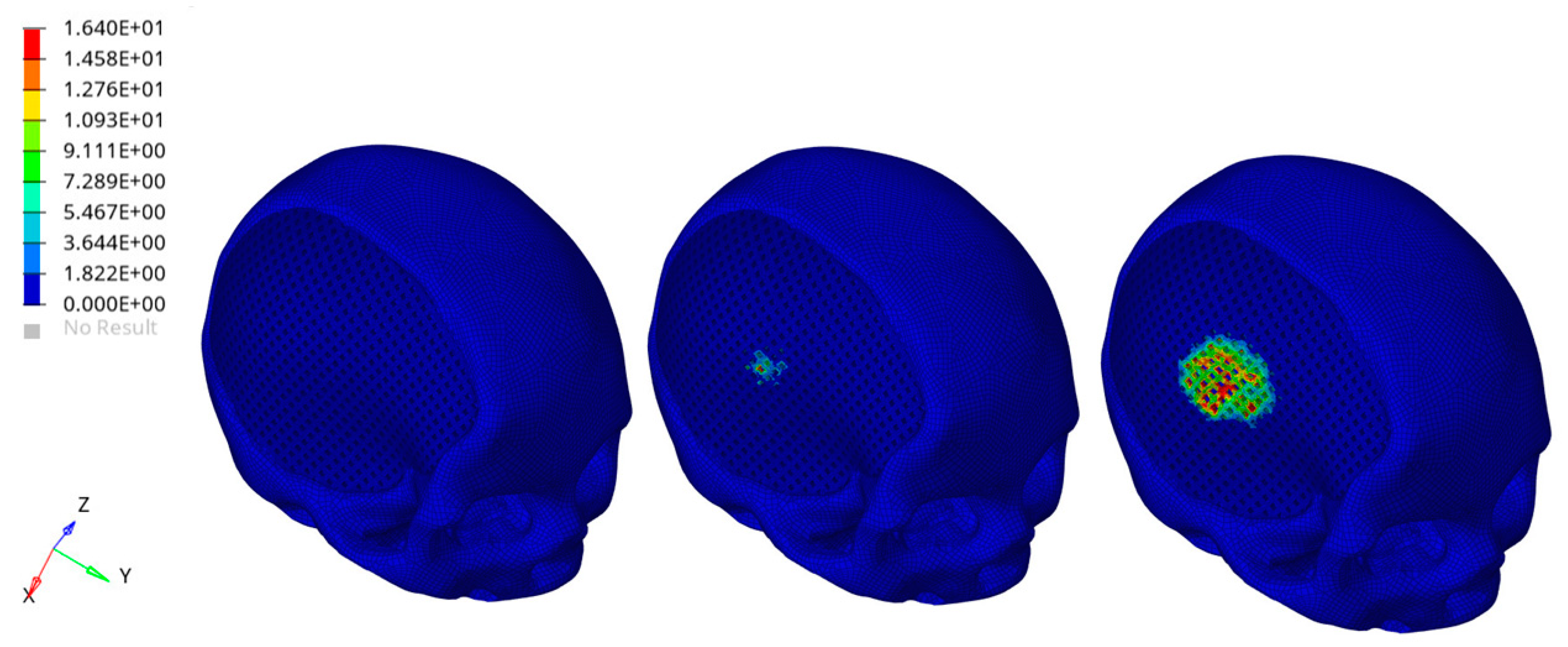
- A theoretical impact analysis was preliminarily carried out on the entire head model. Severe conditions were simulated considering a rigid sphere impacting the implant zone of the head for people with the customized PCL/PMMA/Cu-TCP device. FEA results suggested that the impact caused the failure of some elements of the external cement layer, without significantly altering the mechanical of the underneath PCL structure infiltrated with the cement.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Santis, R.; Gloria, A.; Ambrosio, L. Materials and technologies for craniofacial tissue repair and regeneration. Top. Med. 2010, 16, 1–6. [Google Scholar]
- Piitulainen, J.M.; Kauko, T.; Aitasalo, K.M.; Vuorinen, V.; Vallittu, P.K.; Posti, J.P. Outcomes of Cranioplasty with Synthetic Materials and Autologous Bone Grafts. World Neurosurg. 2015, 83, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Unterhofer, C.; Wipplinger, C.; Verius, M.; Recheis, W.; Thomé, C.; Ortler, M. Reconstruction of large cranial defects with poly-methyl-methacrylate (PMMA) using a rapid prototyping model and a new technique for intraoperative implant modeling. Neurol. Neurochir. Polska 2017, 51, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Wu, C.T.; Lee, S.T.; Chen, P.J. Cranioplasty using polymethyl methacrylate prostheses. J. Clin. Neurosci. 2009, 16, 56–63. [Google Scholar] [CrossRef]
- Harris, D.A.; Fong, A.J.; Buchanan, E.P.; Monson, L.; Khechoyan, D.; Lam, S. History of synthetic materials in alloplastic cranioplasty. Neurosurg. Focus 2014, 36, E20. [Google Scholar] [CrossRef]
- De Santis, R.; Mollica, F.; Ambrosio, L.; Nicolais, L.; Ronca, D. Dynamic mechanical behavior of PMMA based bone cements in wet environment. J. Mater. Sci. Mater. Electron. 2003, 14, 583–594. [Google Scholar] [CrossRef]
- Spence, W.T. Form-Fitting Plastic Cranioplasty. J. Neurosurg. 2009, 11, 219–225. [Google Scholar] [CrossRef]
- Bloch, O.; McDermott, M.W. In situ cranioplasty for hyperostosing meningiomas of the cranial vault. Can. J. Neurol. Sci. J. Can. Sci. Neurol. 2011, 38, 59–64. [Google Scholar] [CrossRef][Green Version]
- McElhaney, J.H.; Fogle, J.L.; Melvin, J.W.; Haynes, R.R.; Roberts, V.L.; Alem, N.M. Mechanical properties on cranial bone. J. Biomech. 1970, 3, 495–511. [Google Scholar] [CrossRef]
- Ronca, D.; Gloria, A.; De Santis, R.; Russo, T.; D’Amora, U.; Chierchia, M.; Nicolais, L.; Ambrosio, L. Critical analysis on dynamic-mechanical performance of spongy bone: The effect of an acrylic cement. Hard Tissue 2014, 3, 9–16. [Google Scholar]
- Caro-Osorio, E.; Ramos, R.D.L.G.; Martínez-Sánchez, S.R.; Olazarán-Salinas, F. Cranioplasty with polymethylmethacrylate prostheses fabricated by hand using original bone flaps: Technical note and surgical outcomes. Surg. Neurol. Int. 2013, 4, 136. [Google Scholar] [CrossRef] [PubMed]
- Matsuno, A.; Tanaka, H.; Iwamuro, H.; Takanashi, S.; Miyawaki, S.; Nakashima, M.; Nakaguchi, H.; Nagashima, T. Analyses of the factors influencing bone graft infection after delayed cranioplasty. Acta Neurochir. 2006, 148, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Minelli, E.B.; Della Bora, T.; Benini, A. Different microbial biofilm formation on polymethylmethacrylate (PMMA) bone cement loaded with gentamicin and vancomycin. Anaerobe 2011, 17, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Worm, P.V.; Nascimento, T.L.D.; Nicola, F.D.C.; Sanches, E.F.; Moreira, C.F.D.S.; Rogério, L.P.W.; Dos Reis, M.M.; Finger, G.; Collares, M.V.M. Polymethylmethacrylate imbedded with antibiotics cranioplasty: An infection solution for moderate and large defects reconstruction. Surg. Neurol. Int. 2016, 7, 746–S751. [Google Scholar] [CrossRef]
- Oei, J.D.; Zhao, W.W.; Chu, L.; DeSilva, M.N.; Ghimire, A.; Ralph, R.H.; Whang, K. Antimicrobial acrylic materials with in situ generated silver nanoparticles. J. Biomed. Mater. Res. Part B Appl. Biomater. 2011, 100, 409–415. [Google Scholar] [CrossRef]
- Russo, T.; Gloria, A.; De Santis, R.; D’Amora, U.; Balato, G.; Vollaro, A.; Oliviero, O.; Improta, G.; Triassi, M.; Ambrosio, L. Preliminary focus on the mechanical and antibacterial activity of a PMMA-based bone cement loaded with gold nanoparticles. Bioact. Mater. 2017, 2, 156–161. [Google Scholar] [CrossRef]
- Russo, T.; De Santis, R.; Gloria, A.; Barbaro, K.; Altigeri, A.; Fadeeva, I.V.; Rau, J.V. Modification of PMMA Cements for Cranioplasty with Bioactive Glass and Copper Doped Tricalcium Phosphate Particles. Polymer 2019, 12, 37. [Google Scholar] [CrossRef]
- Jaberi, J.; Gambrell, K.; Tiwana, P.; Madden, C.; Finn, R. Long-Term Clinical Outcome Analysis of Poly-Methyl-Methacrylate Cranioplasty for Large Skull Defects. J. Oral Maxillofac. Surg. 2013, 71, e81–e88. [Google Scholar] [CrossRef]
- Saringer, W.; Nöbauer-Huhmann, I.; Knosp, E. Cranioplasty with Individual Carbon Fibre Reinforced Polymere (CFRP) Medical Grade Implants Based on CAD/CAM Technique. Acta Neurochir. 2002, 144, 1193–1203. [Google Scholar] [CrossRef]
- Peltola, M.J.; Vallittu, P.K.; Vuorinen, V.; Aho, A.A.J.; Puntala, A.; Aitasalo, K.M.J. Novel composite implant in craniofacial bone reconstruction. Eur. Arch. Oto-Rhino-Laryngol. 2011, 269, 623–628. [Google Scholar] [CrossRef]
- Msallem, B.; Beiglboeck, F.; Honigmann, P.; Jaquiéry, D.M.C.; Thieringer, M.D.M.F. Craniofacial Reconstruction by a Cost-Efficient Template-Based Process Using 3D Printing. Plast. Reconstr. Surg.-Glob. Open 2017, 5, e1582. [Google Scholar] [CrossRef] [PubMed]
- Van Putten, M.C., Jr.; Yamada, S. Alloplastic cranial implants made from computed tomographic scan-generated casts. J. Prosthet. Dent. 1992, 68, 103–108. [Google Scholar] [CrossRef]
- Arridge, S.; Moss, J.P.; Linney, A.D.; James, D.R. Three dimensional digitization of the face and skull. J. Maxillofac. Surg. 1985, 13, 136–143. [Google Scholar] [CrossRef]
- Mertens, C.; Wessel, E.; Berger, M.; Ristow, O.; Hoffmann, J.; Kansy, K.; Freudlsperger, C.; Bächli, H.; Engel, M. The value of three-dimensional photogrammetry in isolated sagittal synostosis: Impact of age and surgical technique on intracranial volume and cephalic index─a retrospective cohort study. J. Cranio-Maxillofac. Surg. 2017, 45, 2010–2016. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-H.; Chuang, H.-Y.; Lin, H.-L.; Liu, C.-L.; Yao, C.-H. Surgical results of cranioplasty using three-dimensional printing technology. Clin. Neurol. Neurosurg. 2018, 168, 118–123. [Google Scholar] [CrossRef]
- Dean, D.; Min, K.-J.; Bond, A. Computer Aided Design of Large-Format Prefabricated Cranial Plates. J. Craniofacial Surg. 2003, 14, 819–832. [Google Scholar] [CrossRef]
- De Santis, R.; D’Amora, U.; Russo, T.; Ronca, A.; Gloria, A.; Ambrosio, L. 3D fibre deposition and stereolithography techniques for the design of multifunctional nanocomposite magnetic scaffolds. J. Mater. Sci. Mater. Med. 2015, 26, 250. [Google Scholar] [CrossRef]
- Maricevich, J.P.B.R.; Cezar-Junior, A.B.; de Oliveira-Junior, E.X.; Silva, J.A.M.; da Silva, J.V.L.; Nunes, A.A.; Almeida, N.S.; Azevedo-Filho, H.R.C. Functional and aesthetic evaluation after cranial reconstruction with polymethyl methacrylate prostheses using low-cost 3D printing templates in patients with cranial defects secondary to decompressive craniectomies: A prospective study. Surg. Neurol. Int. 2019, 117, 443–452. [Google Scholar] [CrossRef]
- Chim, H.; Schantz, J.-T. New Frontiers in Calvarial ReconstructionS: Integrating Computer-Assisted Design and Tissue Engineering in Cranioplasty. Plast. Reconstr. Surg. 2005, 116, 1726–1741. [Google Scholar] [CrossRef]
- Espalin, D.; Arcaute, K.; Rodriguez, D.; Medina, F.; Posner, M.; Wicker, R. Fused deposition modeling of patient-specific polymethylmethacrylate implants. Rapid Prototyp. J. 2010, 16, 164–173. [Google Scholar] [CrossRef]
- Hassan, M.N.; Yassin, M.A.; Suliman, S.; Lie, S.A.; Gjengedal, H.; Mustafa, K. The bone regeneration capacity of 3D-printed templates in calvarial defect models: A systematic review and meta-analysis. Acta Biomater. 2019, 91, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Gloria, A.; De Santis, R.; Ambrosio, L. Polymer-based composite scaffolds for tissue engineering. J. Appl. Biomater. Biomech. 2010, 8, 57–67. [Google Scholar] [PubMed]
- Sinikovic, B.; Schumann, P.; Winkler, M.; Kuestermeyer, J.; Tavassol, F.; Von See, C.; Carvalho, C.; Mülhaupt, R.; Bormann, K.-H.; Kokemueller, H.; et al. Calvaria bone chamber-A new model for intravital assessment of osseous angiogenesis. J. Biomed. Mater. Res. Part A 2011, 99, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Gephart, M.G.H.; Woodard, J.I.; Arrigo, R.T.; Lorenz, H.P.; Schendel, S.A.; Edwards, M.S.B.; Guzman, R. Using bioabsorbable fixation systems in the treatment of pediatric skull deformities leads to good outcomes and low morbidity. Child’s Nerv. Syst. 2012, 29, 297–301. [Google Scholar] [CrossRef]
- Chao, M.T.; Jiang, S.; Smith, D.; DeCesare, G.E.; Cooper, G.M.; Pollack, I.F.; Girotto, J.; Losee, J.E. Demineralized Bone Matrix and Resorbable Mesh Bilaminate Cranioplasty: A Novel Method for Reconstruction of Large-Scale Defects in the Pediatric Calvaria. Plast. Reconstr. Surg. 2009, 123, 976–982. [Google Scholar] [CrossRef]
- De Santis, R.; Gloria, A.; Russo, T.; D’Amora, U.; Zeppetelli, S.; Tampieri, A.; Herrmannsdörfer, T.; Ambrosio, L. A route toward the development of 3D magnetic scaffolds with tailored mechanical and morphological properties for hard tissue regeneration: Preliminary study. Virtual Phys. Prototyp. 2011, 6, 189–195. [Google Scholar] [CrossRef]
- Russo, L.; Gloria, A.; Russo, T.; D’Amora, U.; Taraballi, F.; De Santis, R.; Ambrosio, L.; Nicotra, F.; Cipolla, L. Glucosamine grafting on poly(ε-caprolactone): A novel glycated polyester as a substrate for tissue engineering. RSC Adv. 2013, 3, 6286–6289. [Google Scholar] [CrossRef]
- Schantz, J.T.; Teoh, S.H.; Lim, T.C.; Endres, M.; Lam, C.X.F.; Hutmacher, D.W. Repair of Calvarial Defects with Customized Tissue-Engineered Bone Grafts, I. Evaluation of Osteogenesis in a Three-Dimensional Culture System. Tissue Eng. 2003, 9, 113–126. [Google Scholar] [CrossRef]
- Schantz, J.T.; Hutmacher, D.W.; Lam, C.X.F.; Brinkmann, M.; Wong, K.M.; Lim, T.C.; Chou, N.; Guldberg, R.E.; Teoh, S.H. Repair of Calvarial Defects with Customised Tissue-Engineered Bone Grafts II. Evaluation of Cellular Efficiency and Efficacyin Vivo. Tissue Eng. 2003, 9, 127–139. [Google Scholar] [CrossRef]
- Askari, M.; Naniz, M.A.; Kouhi, M.; Saberi, A.; Zolfagharian, A.; Bodaghi, M. Recent progress in extrusion 3D bioprinting of hydrogel biomaterials for tissue regeneration: A comprehensive review with focus on advanced fabrication techniques. Biomater. Sci. 2020. [Google Scholar] [CrossRef]
- Bodaghi, M.; Liao, W.-H. 4D printed tunable mechanical metamaterials with shape memory operations. Smart Mater. Struct. 2019, 28, 045019. [Google Scholar] [CrossRef]
- Bodaghi, M.; Serjouei, A.; Zolfagharian, A.; Fotouhi, M.; Rahman, H.; Durand, D. Reversible energy absorbing meta-sandwiches by FDM 4D printing. Int. J. Mech. Sci. 2020, 173, 105451. [Google Scholar] [CrossRef]
- Domingos, M.; Chiellini, F.; Gloria, A.; Ambrosio, L.; Bartolo, P. Effect of process parameters on the morphological and mechanical properties of 3D Bioextruded poly(ε-caprolactone) scaffolds. Rapid Prototyp. J. 2012, 18, 56–67. [Google Scholar] [CrossRef]
- Domingos, M.; Intranuovo, F.; Russo, T.; De Santis, R.; Gloria, A.; Ambrosio, L.; Ciurana, J.; Bartolo, P. The first systematic analysis of 3D rapid prototyped poly(ε-caprolactone) scaffolds manufactured through BioCell printing: The effect of pore size and geometry on compressive mechanical behaviour and in vitro hMSC viability. Biofabrication 2013, 5, 045004. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, F.A.M.M.; Fonseca, A.C.; Domingos, M.; Gloria, A.; Serra, A.C.; Coelho, J.F.J. The potential of unsaturated polyesters in biomedicine and tissue engineering: Synthesis, structure-properties relationships and additive manufacturing. Prog. Polym. Sci. 2017, 68, 1–34. [Google Scholar] [CrossRef]
- Moxon, S.; Ferreira, M.J.S.; Dos Santos, P.; Popa, B.; Gloria, A.; Katsarava, R.; Tugushi, D.; Serra, A.C.; Hooper, N.M.; Kimber, S.J.; et al. A Preliminary Evaluation of the Pro-Chondrogenic Potential of 3D-Bioprinted Poly(ester urea) Scaffolds. Polymer 2020, 12, 1478. [Google Scholar] [CrossRef]
- Rocco, N.; Papallo, I.; Nava, M.B.; Catanuto, G.; Accurso, A.; Onofrio, I.; Oliviero, O.; Improta, G.; Speranza, D.; Domingos, M.; et al. Additive manufacturing and technical strategies for improving outcomes in breast reconstructive surgery. Acta IMEKO 2020, 9, 74–79. [Google Scholar] [CrossRef]
- Caroline, D.; Rémy, W. Head injury prediction tool for protective systems optimisation. In Proceedings of the 7th European LS-DYNA Conference, Salzburg, Austria, 14–15 May 2009. [Google Scholar]
- Zhihua, C.; Yun, X.; Zheng, B.; Haojie, M. Creating a human head finite element model using a multi-block approach for predicting skull response and brain pressure. Comput. Methods Biomech. Biomed. Eng. 2019, 22, 169–179. [Google Scholar]
- Takhounts, E.G.; Ridella, S.A.; Hasija, V.; Tannous, R.E.; Campbell, J.Q.; Malone, D.; Danelson, K.; Stitzel, J.; Rowson, S.; Duma, S. Investigation of traumatic brain injuries using the next generation of simulated injury monitor (SIMon) finite element head model. Stapp. Car Crash J. 2008, 52, 1–31. [Google Scholar]
- De Santis, R.; Ambrogi, V.; Carfagna, C.; Ambrosio, L.; Nicolais, L. Effect of microencapsulated phase change materials on the thermo-mechanical properties of poly(methyl-methacrylate) based biomaterials. J. Mater. Sci. Mater. Med. 2006, 17, 1219–1226. [Google Scholar] [CrossRef]
- Lanzotti, A.; Martorelli, M.; Maietta, S.; Gerbino, S.; Penta, F.; Gloria, A. A comparison between mechanical properties of specimens 3D printed with virgin and recycled PLA. Procedia CIRP 2019, 79, 143–146. [Google Scholar] [CrossRef]
- Tse, K.M.; Lim, S.P.; Tan, V.; Lee, H. A review of head injury and finite element head models. Am. J. Eng. Technol. Soc. 2014, 1, 28–52. [Google Scholar]
- Lee, S.H.; Lee, K.-S.; Sorcar, S.; Razzaq, A.; Lee, M.-G.; In, S.-I. Novel Porous Brain Electrodes for Augmented Local Field Potential Signal Detection. Materials 2019, 12, 542. [Google Scholar] [CrossRef] [PubMed]
- Yoganandan, N.; Pintar, F.A.; Sances, A., Jr.; Walsh, P.R.; Ewing, C.L.; Thomas, D.J.; Snyder, R.G. Biomechanics of skull fracture. J. Neurotrauma. 1995, 12, 659–668. [Google Scholar] [CrossRef]
- Yoganandan, N.; Zhang, J.; Pintar, F.A. Force and Acceleration Corridors from Lateral Head Impact. Traffic Inj. Prev. 2004, 5, 368–373. [Google Scholar] [CrossRef]
- Raymond, D.; Van Ee, C.; Crawford, G.; Bir, C. Tolerance of the skull to blunt ballistic temporo-parietal impact. J. Biomech. 2009, 42, 2479–2485. [Google Scholar] [CrossRef]
- Sahoo, D.; Robbe, C.; Deck, C.; Meyer, F.; Papy, A.; Willinger, R. Head injury assessment of non-lethal projectile impacts: A combined experimental/computational method. Injury 2016, 47, 2424–2441. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, K.H.; Dwarampudi, R.; Omori, K.; Li, T.; Chang, K.; Hardy, W.N.; Khalil, T.B.; King, A.I. Recent advances in brain injury research: A new human head model development and validation. Stapp. Car Crash J. 2001, 45, 369–394. [Google Scholar] [CrossRef]
- Mao, H.; Gao, H.; Cao, L.; Genthikatti, V.V.; Yang, K.H. Development of high-quality hexahedral human brain meshes using feature-based multi-block approach. Comput. Methods Biomech. Biomed. Eng. 2011, 16, 271–279. [Google Scholar] [CrossRef]
- Deck, C.; Willinger, R. Improved head injury criteria based on head FE model. Int. J. Crashworthiness 2008, 13, 667–678. [Google Scholar] [CrossRef]
- Hardy, W.N.; Foster, C.D.; Mason, M.J.; Yang, K.H.; King, A.I.; Tashman, S. Investigation of Head Injury Mechanisms Using Neutral Density Technology and High-Speed Biplanar X-ray. Stapp. Car Crash J. 2001, 45, 337–368. [Google Scholar] [CrossRef] [PubMed]
- Hardy, W.N.; Mason, M.J.; Foster, C.D.; Shah, C.S.; Kopacz, J.M.; Yang, K.H.; King, A.I.; Bishop, J.; Bey, M.; Anderst, W.; et al. A study of the response of the human cadaver head to impact. Stapp. Car Crash J. 2007, 51, 17–80. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E.; Urban, J.E.; Stitzel, J.D. Validation performance comparison for finite element models of the human brain. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 1273–1288. [Google Scholar] [CrossRef] [PubMed]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Santis, R.; Russo, T.; Rau, J.V.; Papallo, I.; Martorelli, M.; Gloria, A. Design of 3D Additively Manufactured Hybrid Structures for Cranioplasty. Materials 2021, 14, 181. https://doi.org/10.3390/ma14010181
De Santis R, Russo T, Rau JV, Papallo I, Martorelli M, Gloria A. Design of 3D Additively Manufactured Hybrid Structures for Cranioplasty. Materials. 2021; 14(1):181. https://doi.org/10.3390/ma14010181
Chicago/Turabian StyleDe Santis, Roberto, Teresa Russo, Julietta V. Rau, Ida Papallo, Massimo Martorelli, and Antonio Gloria. 2021. "Design of 3D Additively Manufactured Hybrid Structures for Cranioplasty" Materials 14, no. 1: 181. https://doi.org/10.3390/ma14010181
APA StyleDe Santis, R., Russo, T., Rau, J. V., Papallo, I., Martorelli, M., & Gloria, A. (2021). Design of 3D Additively Manufactured Hybrid Structures for Cranioplasty. Materials, 14(1), 181. https://doi.org/10.3390/ma14010181