High Potential of Bacterial Adhesion on Block Bone Graft Materials

 , , and
, , and 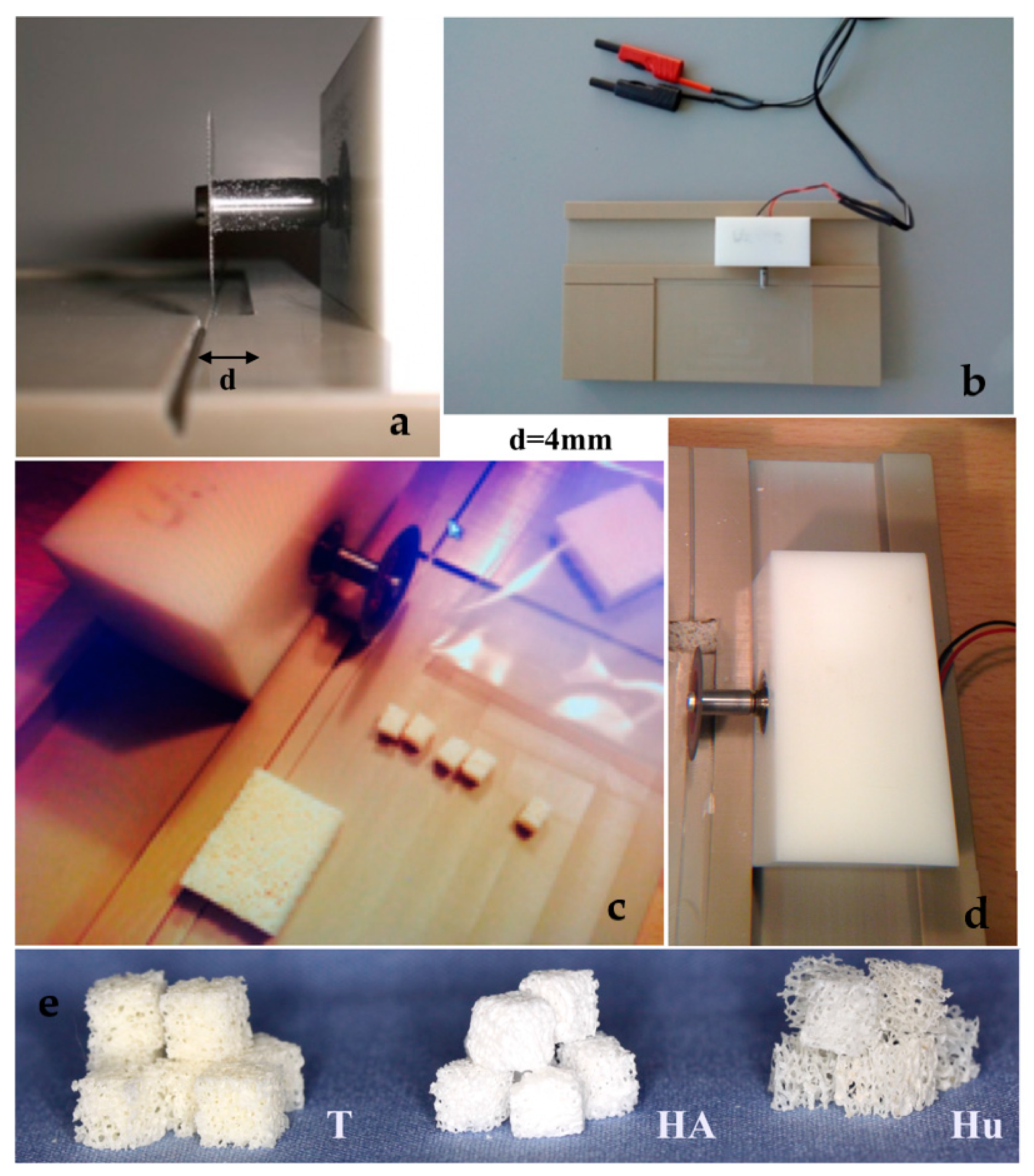{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
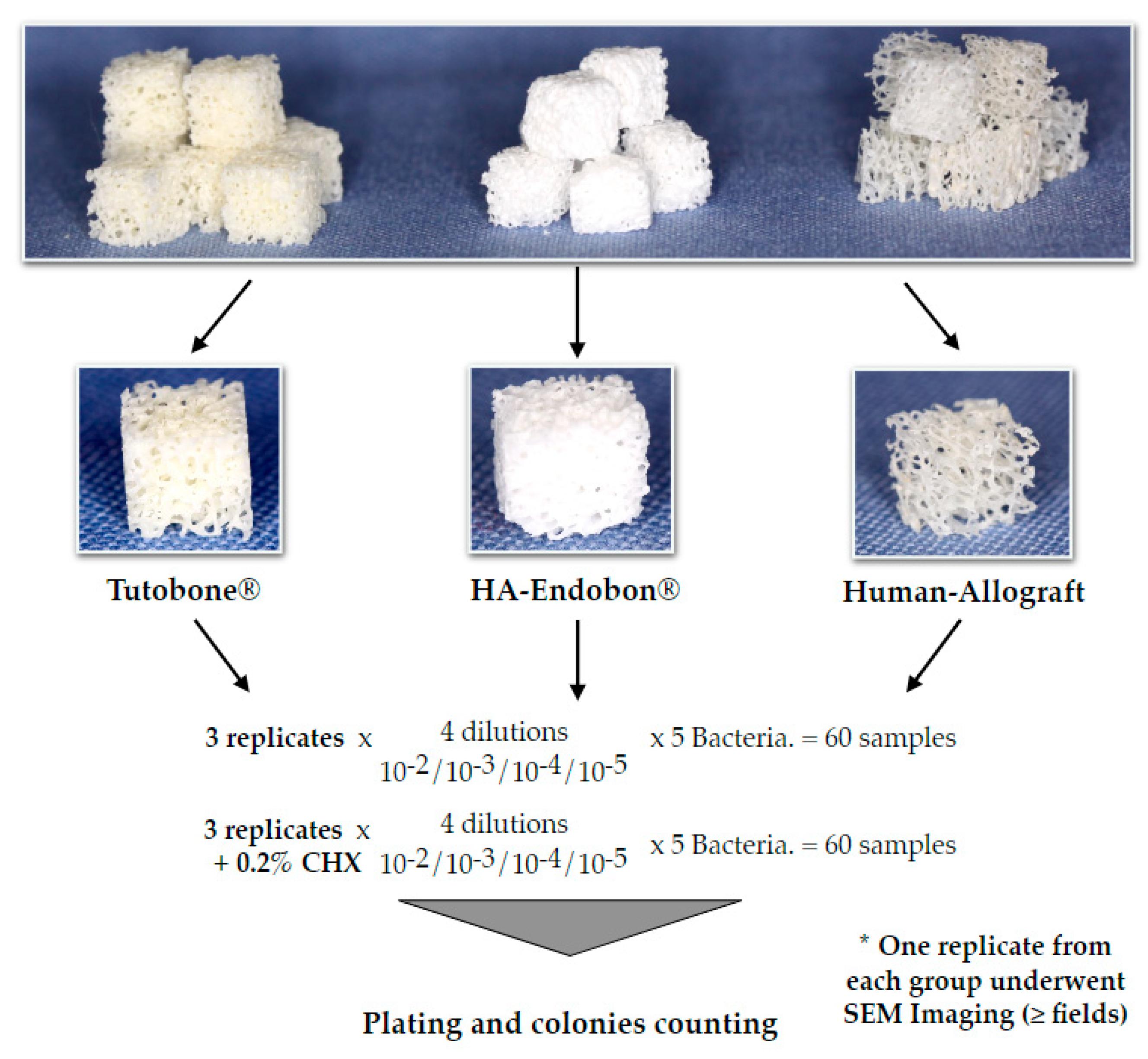
2.1. Selection and Preparation of Biomaterials
2.2. Bacterial Strains
2.3. Quantification of the Initial Microbial Adhesion
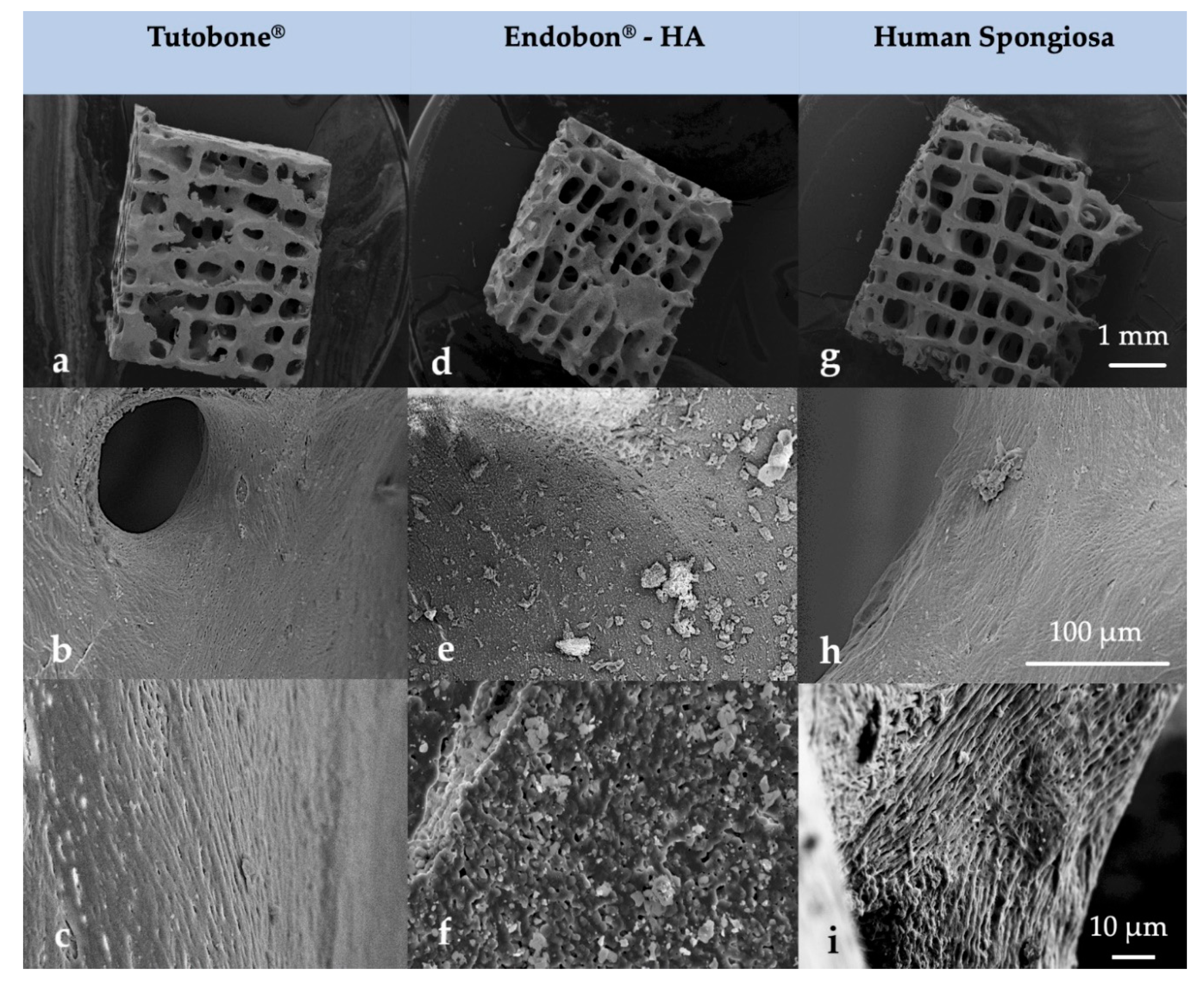
2.4. Scanning Electron Microscopy—SEM
2.5. Statistical Analysis
3. Results
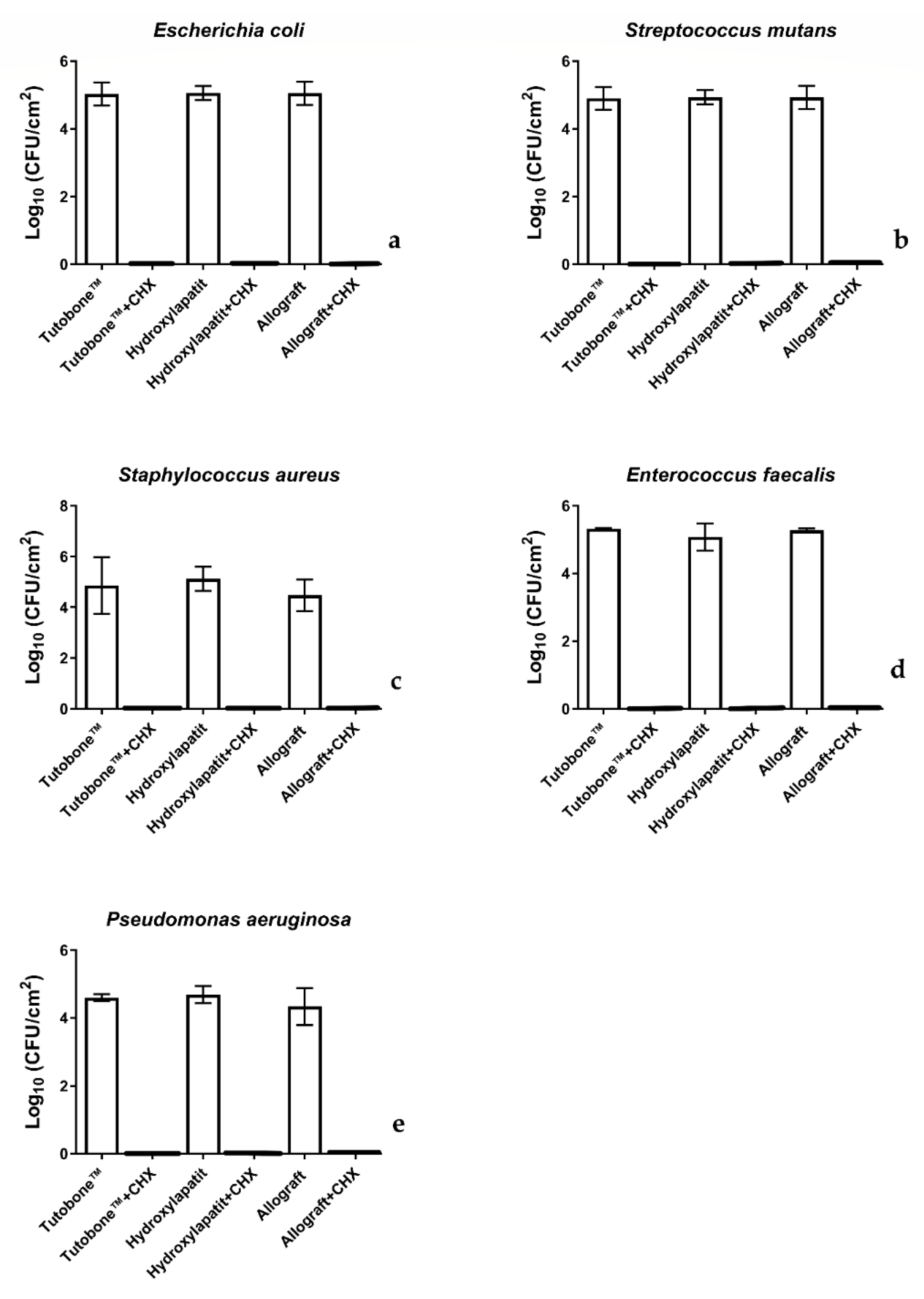
3.1. All Bone Graft Materials Presented a Comparable Initial Bacterial Adhesion for the Five Selected Bacterial Species
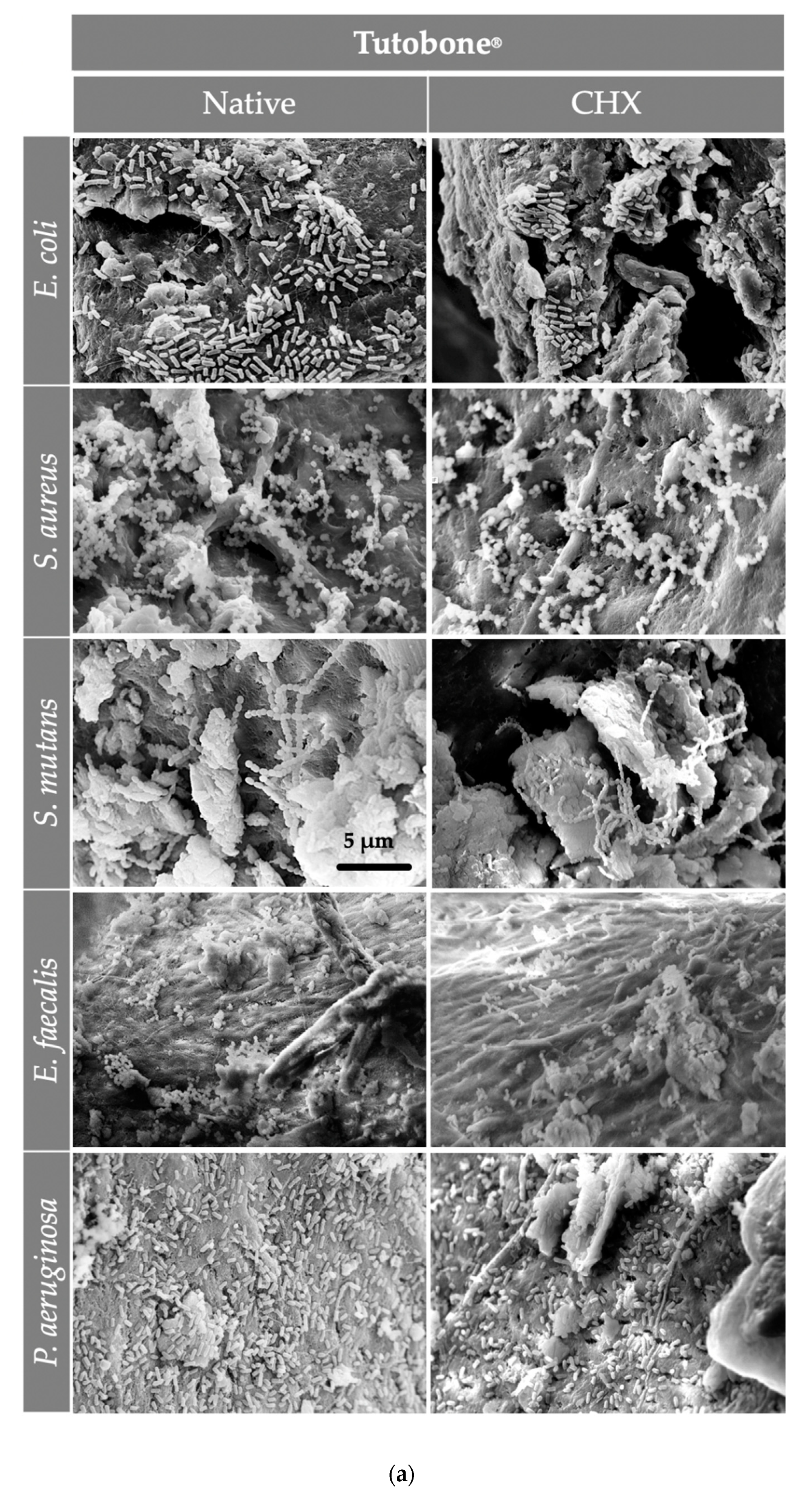
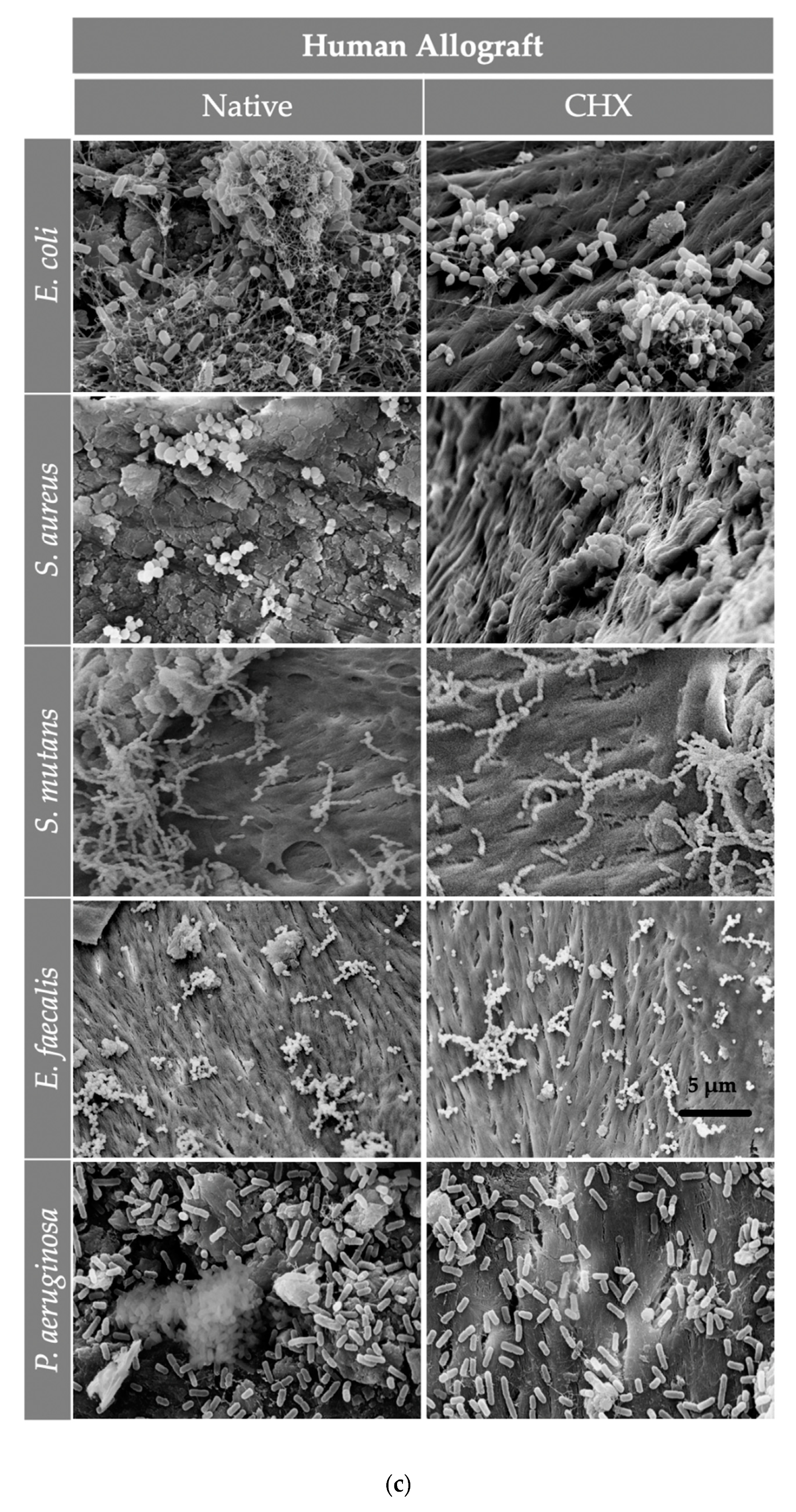
3.2. Pretreatment of the Bone Graft Material with CHX Killed the Adhered Bacteria
3.3. The Morphology of the Scaffolds Allowed for the Organization of the Adherent Bacterial Cells in Grape-Like Clusters
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dorosz, N.; Dominiak, M. Mandibular ridge reconstruction: A review of contemporary methods. Adv. Clin. Exp. Med. 2018, 27, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Nguyen, K. Complex bone augmentation in alveolar ridge defects. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 227–244. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Dietsh, F. Bone-grafting materials in implant dentistry. Implant Dent. 1993, 2, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone substitutes: An update. Injury 2005, 36 (Suppl. 3), S20–S27. [Google Scholar] [CrossRef]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone grafts: Which is the ideal biomaterial? J. Clin. Periodontol. 2019. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone tissue engineering: Recent advances and challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef]
- Boyce, T.; Edwards, J.; Scarborough, N. Allograft bone. The influence of processing on safety and performance. Orthop. Clin. N. Am. 1999, 30, 571–581. [Google Scholar] [CrossRef]
- Bostrom, M.P.G.; Seigerman, D.A. The clinical use of allografts, demineralized bone matrices, synthetic bone graft substitutes and osteoinductive growth factors: A survey study. HSS J. 2005, 1, 9–18. [Google Scholar] [CrossRef]
- Block, M.S. The Processing of Xenografts Will Result in Different Clinical Responses. J. Oral Maxillofac. Surg. 2019, 77, 690–697. [Google Scholar] [CrossRef]
- Soltan, M.; Smiler, D.; Prasad, H.S.; Rohrer, M.D. Bone block allograft impregnated with bone marrow aspirate. Implant Dent. 2007, 16, 329–339. [Google Scholar] [CrossRef]
- Charwat-Pessler, J.; Musso, M.; Petutschnigg, A.; Entacher, K.; Plank, B.; Wernersson, E.; Tangl, S.; Schuller-Götzburg, P. A Bone Sample Containing a Bone Graft Substitute Analyzed by Correlating Density Information Obtained by X-ray Micro Tomography with Compositional Information Obtained by Raman Microscopy. Materials 2015, 8, 3831–3853. [Google Scholar] [CrossRef] [PubMed]
- Precheur, H.V. Bone graft materials. Dent. Clin. N. Am. 2007, 51, 729–746. [Google Scholar] [CrossRef] [PubMed]
- Rodella, L.F.; Favero, G.; Labanca, M. Biomaterials in maxillofacial surgery: Membranes and grafts. Int. J. Biomed. Sci. 2011, 7, 81–88. [Google Scholar] [PubMed]
- Kao, S.T.; Scott, D.D. A review of bone substitutes. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 513–521. [Google Scholar] [CrossRef]
- Chaushu, G.; Mardinger, O.; Peleg, M.; Ghelfan, O.; Nissan, J. Analysis of complications following augmentation with cancellous block allografts. J. Periodontol. 2010, 81, 1759–1764. [Google Scholar] [CrossRef]
- Busscher, H.J.; van der Mei, H.C.; Subbiahdoss, G.; Jutte, P.C.; van den Dungen, J.J.A.M.; Zaat, S.A.J.; Schultz, M.J.; Grainger, D.W. Biomaterial-associated infection: Locating the finish line in the race for the surface. Sci. Transl. Med. 2012, 4, 153rv10. [Google Scholar] [CrossRef]
- Clauss, M.; Trampuz, A.; Borens, O.; Bohner, M.; Ilchmann, T. Biofilm formation on bone grafts and bone graft substitutes: Comparison of different materials by a standard in vitro test and microcalorimetry. Acta Biomater. 2010, 6, 3791–3797. [Google Scholar] [CrossRef]
- Hashemi, H.M.; Beshkar, M. Bacterial contamination of autogenous bone collected by rongeur compared with that collected by bone filter during implant surgery. Br. J. Oral Maxillofac. Surg. 2011, 49, 474–477. [Google Scholar] [CrossRef]
- Zamborsky, R.; Svec, A.; Bohac, M.; Kilian, M.; Kokavec, M. Infection in Bone Allograft Transplants. Exp. Clin. Transpl. 2016, 14, 484–490. [Google Scholar]
- Delloye, C.; Cornu, O.; Druez, V.; Barbier, O. Bone allografts: What they can offer and what they cannot. J. Bone Joint Surg. Br. 2007, 89, 574–579. [Google Scholar] [CrossRef]
- Nary Filho, H.; Pinto, T.F.; de Freitas, C.P.; Ribeiro-Junior, P.D.; dos Santos, P.L.; Matsumoto, M.A. Autogenous bone grafts contamination after exposure to the oral cavity. J. Craniofac. Surg. 2014, 25, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Crawford, R.J.; Webb, H.K.; Truong, V.K.; Hasan, J.; Ivanova, E.P. Surface topographical factors influencing bacterial attachment. Adv. Colloid Interface Sci. 2012, 179–182, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Blay, A.; Tunchel, S.; Sendyk, W.R. Viability of autogenous bone grafts obtained by using bone collectors: Histological and microbiological study. Pesqui. Odontol. Bras. 2003, 17, 234–240. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sharif-Abdullah, S.S.B.; Chong, M.C.; Surindar-Kaur, S.S.; Kamaruzzaman, S.B.; Ng, K.H. The effect of chlorhexidine in reducing oral colonisation in geriatric patients: A randomised controlled trial. Singap. Med. J. 2016, 57, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Pommer, B.; Georgopoulos, A.; Dvorak, G.; Ulm, C. Decontamination of autogenous bone grafts: Systematic literature review and evidence-based proposal of a protocol. Quintessence Int. 2014, 45, 145–150. [Google Scholar] [CrossRef]
- Maekawa, S.; Yoshioka, M.; Kumamoto, Y. Proposal of a new scheme for the serological typing of Enterococcus faecalis strains. Microbiol. Immunol. 1992, 36, 671–681. [Google Scholar] [CrossRef]
- Yaman, F.; Unlü, G.; Atilgan, S.; Celik, Y.; Ozekinci, T.; Yaldiz, M. Microbiologic and histologic assessment of intentional bacterial contamination of bone grafts. J. Oral Maxillofac. Surg. 2007, 65, 1490–1494. [Google Scholar] [CrossRef]
- Ketonis, C.; Barr, S.; Adams, C.S.; Hickok, N.J.; Parvizi, J. Bacterial colonization of bone allografts: Establishment and effects of antibiotics. Clin. Orthop. Relat. Res. 2010, 468, 2113–2121. [Google Scholar] [CrossRef]
- Elnayef, B.; Monje, A.; Gargallo-Albiol, J.; Galindo-Moreno, P.; Wang, H.-L.; Hernández-Alfaro, F. Vertical Ridge Augmentation in the Atrophic Mandible: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, 291–312. [Google Scholar] [CrossRef]
- Deluiz, D.; Oliveira, L.; Fletcher, P.; Pires, F.R.; Nunes, M.A.; Tinoco, E.M.B. Fresh-Frozen Bone Allografts in Maxillary Alveolar Augmentation: Analysis of Complications, Adverse Outcomes, and Implant Survival. J. Periodontol. 2016, 87, 1261–1267. [Google Scholar] [CrossRef]
- Rice, S.A.; Wuertz, S.; Kjelleberg, S. Next-generation studies of microbial biofilm communities. Microb. Biotechnol. 2016, 9, 677–680. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawas, B.; Schiegnitz, E. Augmentation procedures using bone substitute materials or autogenous bone - a systematic review and meta-analysis. Eur. J. Oral Implantol. 2014, 7 (Suppl. 2), S219–S234. [Google Scholar] [PubMed]
- Khojasteh, A.; Hassani, A.; Motamedian, S.R.; Saadat, S.; Alikhasi, M. Cortical Bone Augmentation Versus Nerve Lateralization for Treatment of Atrophic Posterior Mandible: A Retrospective Study and Review of Literature. Clin. Implant Dent. Relat. Res. 2016, 18, 342–359. [Google Scholar] [CrossRef] [PubMed]
- Araújo, P.P.T.; Oliveira, K.P.; Montenegro, S.C.L.; Carreiro, A.F.P.; Silva, J.S.P.; Germano, A.R. Block allograft for reconstruction of alveolar bone ridge in implantology: A systematic review. Implant Dent. 2013, 22, 304–308. [Google Scholar] [CrossRef]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef]
- Khoury, F.; Antoun, H.; Missika, P. Bone Augmentation in Oral Implantology; Quintessence Publishing Company: Chicago, IL, USA, 2007. [Google Scholar]
- Nkenke, E.; Neukam, F.W. Autogenous bone harvesting and grafting in advanced jaw resorption: Morbidity, resorption and implant survival. Eur. J. Oral Implantol. 2014, 7 (Suppl. 2), S203–S217. [Google Scholar]
- Nyström, E.; Nilson, H.; Gunne, J.; Lundgren, S. A 9–14 year follow-up of onlay bone grafting in the atrophic maxilla. Int. J. Oral Maxillofac. Surg. 2009, 38, 111–116. [Google Scholar] [CrossRef]
- Von Arx, T.; Cochran, D.L.; Hermann, J.S.; Schenk, R.K.; Buser, D. Lateral ridge augmentation using different bone fillers and barrier membrane application. A histologic and histomorphometric pilot study in the canine mandible. Clin. Oral Implant. Res. 2001, 12, 260–269. [Google Scholar] [CrossRef]
- Elnayef, B.; Porta, C.; Suárez-López Del Amo, F.; Mordini, L.; Gargallo-Albiol, J.; Hernández-Alfaro, F. The Fate of Lateral Ridge Augmentation: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 622–635. [Google Scholar] [CrossRef]
- Barone, A.; Varanini, P.; Orlando, B.; Tonelli, P.; Covani, U. Deep-frozen allogeneic onlay bone grafts for reconstruction of atrophic maxillary alveolar ridges: A preliminary study. J. Oral Maxillofac. Surg. 2009, 67, 1300–1306. [Google Scholar] [CrossRef]
- Nissan, J.; Marilena, V.; Gross, O.; Mardinger, O.; Chaushu, G. Histomorphometric analysis following augmentation of the posterior mandible using cancellous bone-block allograft. J. Biomed. Mater. Res. A 2011, 97, 509–513. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xuan, F.; Choi, B.-H.; Jeong, S.-M. Minimally invasive ridge augmentation using xenogenous bone blocks in an atrophied posterior mandible: A clinical and histological study. Implant Dent. 2013, 22, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Wolford, L.M.; Wardrop, R.W.; Hartog, J.M. Coralline porous hydroxylapatite as a bone graft substitute in orthognathic surgery. J. Oral Maxillofac. Surg. 1987, 45, 1034–1042. [Google Scholar] [CrossRef]
- Kattimani, V.S.; Chakravarthi, P.S.; Prasad, L.K. Biograft Block Hydroxyapatite: A Ray of Hope in the Reconstruction of Maxillofacial Defects. J. Craniofac. Surg. 2016, 27, 247–252. [Google Scholar] [CrossRef]
- Nunes, C.R.; Simske, S.J.; Sachdeva, R.; Wolford, L.M. Long-term ingrowth and apposition of porous hydroxylapatite implants. J. Biomed. Mater. Res. 1997, 36, 560–563. [Google Scholar] [CrossRef]
- Ayers, R.A.; Simske, S.J.; Nunes, C.R.; Wolford, L.M. Long-term bone ingrowth and residual microhardness of porous block hydroxyapatite implants in humans. J. Oral Maxillofac. Surg. 1998, 56, 1297–1301. [Google Scholar] [CrossRef]
- Silvestri, D.L.; McEnery-Stonelake, M. Chlorhexidine: Uses and adverse reactions. Dermatitis 2013, 24, 112–118. [Google Scholar] [CrossRef]
- Young, M.P.J.; Korachi, M.; Carter, D.H.; Worthington, H.V.; McCord, J.F.; Drucker, D.B. The effects of an immediately pre-surgical chlorhexidine oral rinse on the bacterial contaminants of bone debris collected during dental implant surgery. Clin. Oral Implant. Res. 2002, 13, 20–29. [Google Scholar] [CrossRef]
- Tezulas, E.; Dilek, O.C.; Topcuoglu, N.; Kulekci, G. Decontamination of autogenous bone grafts collected during dental implant site preparation: A pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 656–660. [Google Scholar] [CrossRef]
- Kuttenberger, J.J.; Hardt, N.; Rutz, T.; Pfyffer, G.E. Bone collected with a bone collector during dental implant surgery. Mund Kiefer Gesichtschir. 2005, 9, 18–23. [Google Scholar] [CrossRef]
- Verdugo, F.; Sáez-Rosón, A.; Uribarri, A.; Martínez-Conde, R.; Cabezas-Olcoz, J.; Moragues, M.D.; Pontón, J. Bone microbial decontamination agents in osseous grafting: An in vitro study with fresh human explants. J. Periodontol. 2011, 82, 863–871. [Google Scholar] [CrossRef]
- Lai, P.; Coulson, C.; Pothier, D.D.; Rutka, J. Chlorhexidine ototoxicity in ear surgery, part 1: Review of the literature. J. Otolaryngol. Head Neck Surg. 2011, 40, 437–440. [Google Scholar] [PubMed]
- Cieplik, F.; Jakubovics, N.S.; Buchalla, W.; Maisch, T.; Hellwig, E.; Al-Ahmad, A. Resistance Toward Chlorhexidine in Oral Bacteria—Is There Cause for Concern? Front. Microbiol. 2019, 10, 587. [Google Scholar] [CrossRef] [PubMed]
- Mauceri, R.; Campisi, G.; Matranga, D.; Mauceri, N.; Pizzo, G.; Melilli, D. The Role of Antibiotic Prophylaxis in Reducing Bacterial Contamination of Autologous Bone Graft Collected from Implant Site. Biomed. Res. Int. 2017, 2017, 2175019. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.-A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- Renwick, M.J.; Simpkin, V.; Mossialos, E. Targeting innovation in antibiotic drug discovery and development: The need for a One Health—One Europe—One World Framework. In Series European Observatory Health Policy Series; WHO Regional Office for Europe: København, Danmark, 2016. [Google Scholar]
- Al-Ahmad, A.; Zou, P.; Solarte, D.L.G.; Hellwig, E.; Steinberg, T.; Lienkamp, K. Development of a standardized and safe airborne antibacterial assay, and its evaluation on antibacterial biomimetic model surfaces. PLoS ONE 2014, 9, e111357. [Google Scholar] [CrossRef] [PubMed]
- Choy, M.H.; Stapleton, F.; Willcox, M.D.P.; Zhu, H. Comparison of virulence factors in Pseudomonas aeruginosa strains isolated from contact lens- and non-contact lens-related keratitis. J. Med. Microbiol. 2008, 57, 1539–1546. [Google Scholar] [CrossRef]
- Zimmerli, W.; Trampuz, A.; Ochsner, P.E. Prosthetic-joint infections. N. Engl. J. Med. 2004, 351, 1645–1654. [Google Scholar] [CrossRef]
- Wilkins, M.; Hall-Stoodley, L.; Allan, R.N.; Faust, S.N. New approaches to the treatment of biofilm-related infections. J. Infect. 2014, 69 (Suppl. 1), S47–S52. [Google Scholar] [CrossRef]
- Al-Ahmad, A.; Wiedmann-Al-Ahmad, M.; Carvalho, C.; Lang, M.; Follo, M.; Braun, G.; Wittmer, A.; Mülhaupt, R.; Hellwig, E. Bacterial and Candida albicans adhesion on rapid prototyping-produced 3D-scaffolds manufactured as bone replacement materials. J. Biomed. Mater. Res. A 2008, 87, 933–943. [Google Scholar] [CrossRef]
- Cieplik, F.; Tabenski, L.; Buchalla, W.; Maisch, T. Antimicrobial photodynamic therapy for inactivation of biofilms formed by oral key pathogens. Front. Microbiol. 2014, 5, 405. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K. Riddle of Biofilm Resistance. Antimicrob. Agents Chemother. 2001, 45, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Mah, T.-F.C.; O’Toole, G.A. Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 2001, 9, 34–39. [Google Scholar] [CrossRef]
- Stewart, P.S.; William Costerton, J. Antibiotic resistance of bacteria in biofilms. Lancet 2001, 358, 135–138. [Google Scholar] [CrossRef]
- Chambless, J.D.; Hunt, S.M.; Stewart, P.S. A Three-Dimensional Computer Model of Four Hypothetical Mechanisms Protecting Biofilms from Antimicrobials. Appl. Environ. Microbiol. 2006, 72, 2005–2013. [Google Scholar] [CrossRef]
- Hazan, R.; Que, Y.-A.; Maura, D.; Rahme, L.G. A method for high throughput determination of viable bacteria cell counts in 96-well plates. BMC Microbiol. 2012, 12, 259. [Google Scholar] [CrossRef]
- Shah, S.R.; Tatara, A.M.; D’Souza, R.N.; Mikos, A.G.; Kasper, F.K. Evolving strategies for preventing biofilm on implantable materials. Mater. Today 2013, 16, 177–182. [Google Scholar] [CrossRef]
- Carinci, F.; Lauritano, D.; Bignozzi, C.A.; Pazzi, D.; Candotto, V.; Santos de Oliveira, P.; Scarano, A. A New Strategy Against Peri-Implantitis: Antibacterial Internal Coating. Int. J. Mol. Sci. 2019, 20, 3897. [Google Scholar] [CrossRef]
- Venkatesan, N.; Perumal, G.; Doble, M. Bacterial resistance in biofilm-associated bacteria. Future Microbiol. 2015, 10, 1743–1750. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisyrios, T.; Karygianni, L.; Fretwurst, T.; Nelson, K.; Hellwig, E.; Schmelzeisen, R.; Al-Ahmad, A. High Potential of Bacterial Adhesion on Block Bone Graft Materials. Materials 2020, 13, 2102. https://doi.org/10.3390/ma13092102
Nisyrios T, Karygianni L, Fretwurst T, Nelson K, Hellwig E, Schmelzeisen R, Al-Ahmad A. High Potential of Bacterial Adhesion on Block Bone Graft Materials. Materials. 2020; 13(9):2102. https://doi.org/10.3390/ma13092102
Chicago/Turabian StyleNisyrios, Themistoklis, Lamprini Karygianni, Tobias Fretwurst, Katja Nelson, Elmar Hellwig, Rainer Schmelzeisen, and Ali Al-Ahmad. 2020. "High Potential of Bacterial Adhesion on Block Bone Graft Materials" Materials 13, no. 9: 2102. https://doi.org/10.3390/ma13092102
APA StyleNisyrios, T., Karygianni, L., Fretwurst, T., Nelson, K., Hellwig, E., Schmelzeisen, R., & Al-Ahmad, A. (2020). High Potential of Bacterial Adhesion on Block Bone Graft Materials. Materials, 13(9), 2102. https://doi.org/10.3390/ma13092102