
Social Simulation Model of the Spread and Prevention of the Omicron SARS-CoV-2 Variant

Abstract
1. Introduction
2. Multi-Agent Behavior Design
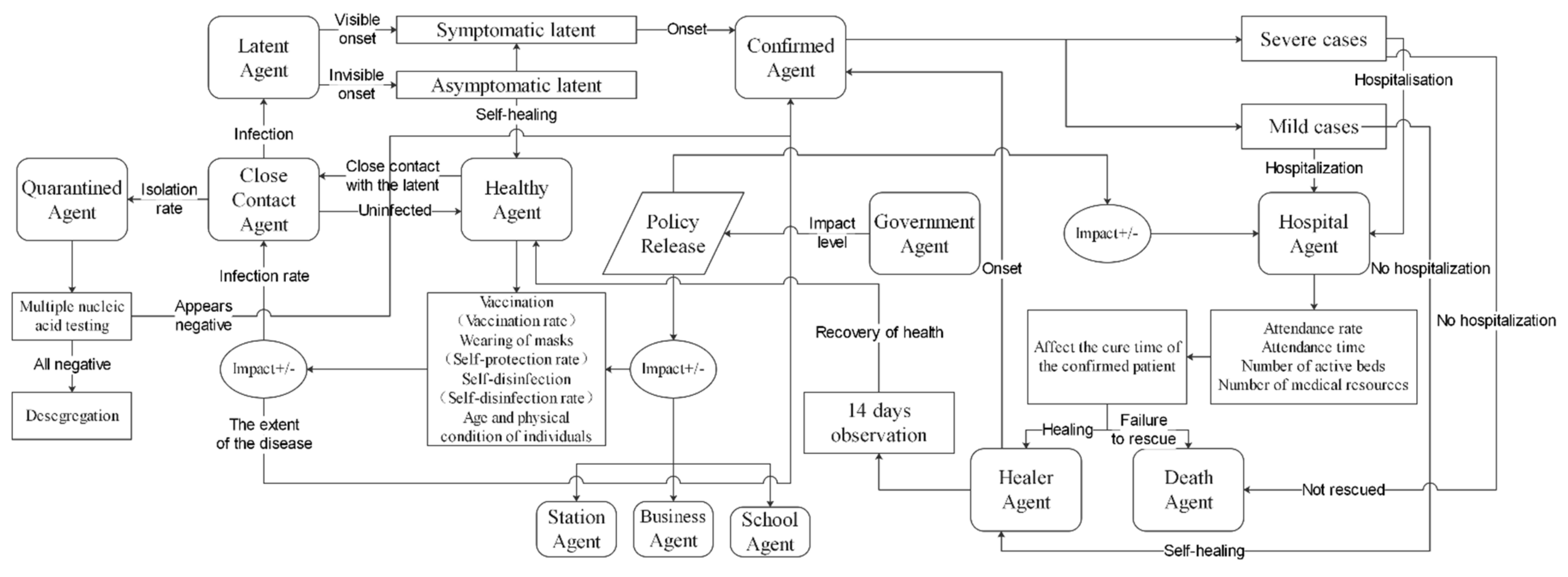
2.1. Overview of Agent Behavior
2.2. Resident Agent Flow Behavior Rules
2.3. State Transition Rules for Resident Agents
2.4. Contact Propagation Rules between Agents
2.5. Rules of Conduct for the Admission of Patients to Hospital Agents
3. Implementation of a Multi-Agent-Based Model for the Spread and Control of Omicron Strains
Model Validation
4. Analysis of Simulation Scenarios and Experimental Results
4.1. No-Intervention Scenario
4.2. Non-Pharmacological Intervention Scenarios
Self-Hygiene Prevention and Control
4.3. Drug Intervention Scenarios
4.3.1. Hospital Treatment
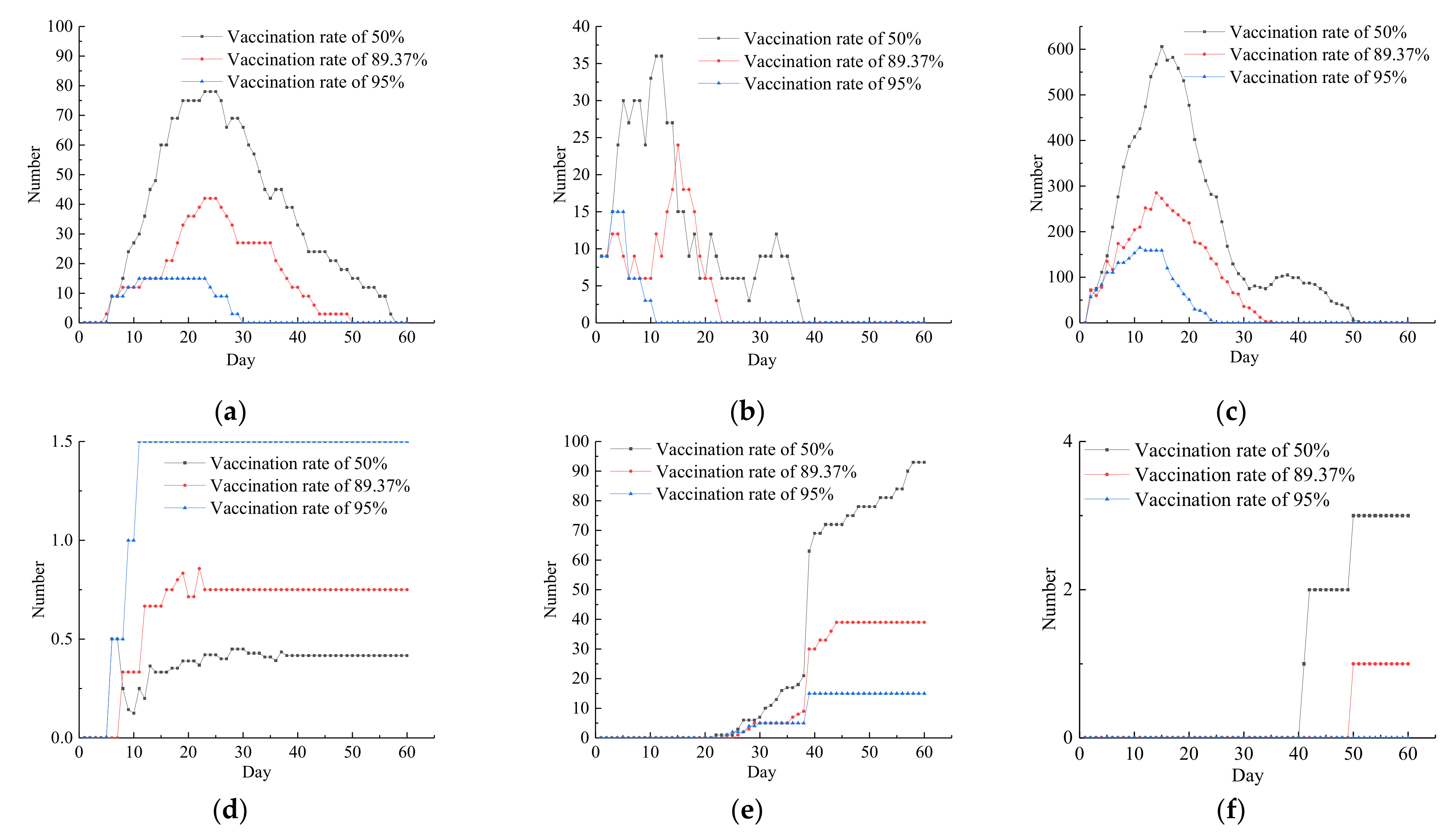
4.3.2. Vaccine Interventions
4.4. Combination of Multiple Interventions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, J.; Zhang, L.; Liu, X.; Wei, Y.; Liu, C.; Lian, X.; Huang, Z.; Chou, J.; Liu, X.; Li, X.; et al. Global prediction system for COVID-19 pandemic. Sci. Bull. 2020, 65, 1884–1887. [Google Scholar] [CrossRef] [PubMed]
- Sanyaolu, A.; Marinkovic, A.; Prakash, S.; Haider, N.; Williams, M.; Okorie, C.; Badaru, O.; Smith, S. SARS-CoV-2 Omicron variant (B.1.1.529): A concern with immune escape. World J. Virol. 2022, 11, 137–143. [Google Scholar] [CrossRef] [PubMed]
- WHO. Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern. Available online: https://www.who.int/news/item/26-11-2021-classification-of-omicron-(b.1.1.529)-sars-cov-2-variant-of-concern (accessed on 26 November 2021).
- Ren, S.-Y.; Wang, W.-B.; Gao, R.-D.; Zhou, A.-M. Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity, transmission, and vaccine resistance. World J. Clin. Cases 2022, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.; Wang, X.; Li, Q.; Bragazzi, N.L.; Tang, S.; Xiao, Y.; Wu, J. Estimation of the Transmission Risk of the 2019-nCoV and Its Implication for Public Health Interventions. J. Clin. Med. 2020, 9, 462. [Google Scholar] [CrossRef]
- Suryawanshi, R.K.; Chen, I.P.; Ma, T.; Syed, A.M.; Brazer, N.; Saldhi, P.; Simoneau, C.R.; Ciling, A.; Khalid, M.M.; Sreekumar, B.; et al. Limited cross-variant immunity from SARS-CoV-2 Omicron without vaccination. Nature 2022, 607, 351–355. [Google Scholar] [CrossRef]
- Chekol Abebe, E.; Tiruneh, G.; Medhin, M.; Behaile, T.; Mariam, A.; Asmamaw Dejenie, T.; Mengie Ayele, T.; Tadele Admasu, F.; Tilahun Muche, Z.; Asmare Adela, G. Mutational Pattern, Impacts and Potential Preventive Strategies of Omicron SARS-CoV-2 Variant Infection. Infect Drug Resist. 2022, 15, 1871–1887. [Google Scholar] [CrossRef]
- Liu, M.; Shi, L.; Chen, H.; Wang, X.; Yang, M.; Jiao, J.; Yang, J.; Sun, G. Comparison Between China and Brazil in the Two Waves of COVID-19 Prevention and Control. J. Epidemiol. Glob. Health 2022, 12, 168–181. [Google Scholar] [CrossRef]
- Jin, H.; Lu, L.; Liu, J.; Cui, M. COVID-19 emergencies around the globe: China’s experience in controlling COVID-19 and lessons learned. Int. J. Qual. Health Care 2021, 33, mzaa143. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.B.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M.; et al. Estimated Effectiveness of COVID-19 Vaccines Against Omicron or Delta Symptomatic Infection and Severe Outcomes. JAMA Netw. Open 2022, 5, e2232760. [Google Scholar] [CrossRef]
- Chen, Z.; Deng, X.; Fang, L.; Sun, K.; Wu, Y.; Che, T.; Zou, J.; Cai, J.; Liu, H.; Wang, Y.; et al. Epidemiological characteristics and transmission dynamics of the outbreak caused by the SARS-CoV-2 Omicron variant in Shanghai, China: A descriptive study. Lancet Reg. Health West. Pac. 2022, 29, 100592. [Google Scholar] [CrossRef]
- Alzahrani, S.I.; Aljamaan, I.A.; Al-Fakih, E.A. Forecasting the spread of the COVID-19 pandemic in Saudi Arabia using ARIMA prediction model under current public health interventions. J. Infect. Public Health 2020, 13, 914–919. [Google Scholar] [CrossRef]
- Sheng, H.; Wu, L.; Xiao, C. Modeling Analysis and Prediction on NCP Epidemic Transmission. J. Syst. Simul. 2020, 32, 759–766. [Google Scholar] [CrossRef]
- Annas, S.; Pratama, M.I.; Rifandi, M.; Sanusi, W.; Side, S. Stability analysis and numerical simulation of SEIR model for pandemic COVID-19 spread in Indonesia. Chaos Solitons Fractals 2020, 139, 110072. [Google Scholar] [CrossRef]
- Cao, W.J.; Liu, X.F.; Han, Z.; Feng, X.; Zhang, L.; Liu, X.F.; Xu, X.K.; Wu, Y. Statictical analysis and autoregressive modeling of confirmed coronavirus disease 2019 epidemic case. Acta Phys. Sin. 2020, 69, 40–46. [Google Scholar] [CrossRef]
- Chen, B.; Yang, M.; Ai, C.; Ma, L.; Zhu, Z.; Chen, H.; Zhu, M.; Xu, W. Prediction of Epidemic Transmission and Evaluation of Prevention and Control Measures Based on Artificial Society. J. Syst. Simul. 2020, 32, 2507–2514. [Google Scholar] [CrossRef]
- Saikia, D.; Bora, K.; Bora, M.P. COVID-19 outbreak in India: An SEIR model-based analysis. Nonlinear Dyn. 2021, 104, 4727–4751. [Google Scholar] [CrossRef]
- Fan, R.G.; Wang, Y.B.; Luo, M.; Zhang, Y.Q.; Zhu, C.P. SEIR-Based COVID-19 Transmission Model and Inflection Point Prediction Analysis. J. Univ. Electron. Sci. Technol. China 2020, 49, 369–374. [Google Scholar]
- Li, D.; Bai, R.R. Combined model of novel coronavirus transmission simulation. Stat. Decis. 2020, 36, 5–10. [Google Scholar] [CrossRef]
- Ma, X.; Zhang, X.; Qin, C. Research of the Sudden Public Health Incidents Response Policies Based on Policy Tools: Taking COVID-19 as an Example. Inf. Stud. Theory Appl. 2020, 43, 29–37. [Google Scholar]
- Li, C.J.; Liu, G.P. Data-driven consensus for non-linear networked multi-agent systems with switching topology and time-varying delays. IET Control Theory Appl. 2018, 12, 1773–1779. [Google Scholar] [CrossRef]
- Pan, L.; Qin, S.; Li, X.; Lu, F.; Yang, F. Multi-agent Simulation Model for COVID-19 Virus Prevention and Control. J. Syst. Simul. 2020, 32, 2244–2257. [Google Scholar] [CrossRef]
- Yin, L.; Liu, K.; Zhang, H.; Xi, G.; Li, X.; Li, Z.; Xue, J. Integrating Human Mobility into the Epidemiological Models of COVID-19: Progress and Challenges. J. Geo Inf. Sci. 2021, 23, 1894–1909. [Google Scholar]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Mkolesia, A. On the Estimation of a Univariate Gaussian Distribution: A Comparative Approach. Open J. Stats 2015, 5, 445–454. [Google Scholar] [CrossRef]
- Prevention and Control Plan for Novel Coronavirus Pneumonia (Seventh Edition). Chin. J. Infect. Control 2020, 19, 1042–1048.
- Taiyuan Bureau of Statistics. Taiyuan Statistical Yearbook; China Statistics Press: Taiyuan, China, 2020. [Google Scholar]
- Kim, M.-K.; Lee, B.; Choi, Y.Y.; Um, J.; Lee, K.-S.; Sung, H.K.; Kim, Y.; Park, J.-S.; Lee, M.; Jang, H.-C.; et al. Clinical Characteristics of 40 Patients Infected With the SARS-CoV-2 Omicron Variant in Korea. J. Korean Med. Sci. 2022, 37, e31. [Google Scholar] [CrossRef]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.who.int/publications-detail-redirect/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19) (accessed on 15 July 2021).
- General Office of the National Health Care Commission. Notice on the Issuance of the Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 8). Available online: http://www.nhc.Gov.cn/yzygj/s7653p/202008/0a7bdf12bd4b46e5bd28ca7f9a7f5e5a.html (accessed on 15 September 2020).
- Liu, Y.; Rocklöv, J. The effective reproductive number of the Omicron variant of SARS-CoV-2 is several times relative to Delta. J. Travel Med. 2022, 29, taac037. [Google Scholar] [CrossRef]
- Pan, L.; Li, X.; Qin, S.; Zhang, Y.; Yan, H. Multi-Agent Simulation Model of Urban Safety Livability Change. J. Syst. Simul. 2019, 31, 1321–1333. [Google Scholar]
- The People’s Government of Shanxi Province. Status of Vaccination in Shanxi Province. Available online: http://www.shanxi.gov.cn/yw/sxyw/202203/t20220331_960920.shtml (accessed on 31 March 2022).
- Zhang, J.; Huimin, X.U.E.; Yaxin, G.O.N.G.; Qi, Q.I.N.; Changhua, N.I.N.G.; Lei, C.A.O.; Yongxiao, C.A.O. Analysis of death time of patients with coronavirus disease 2019. J. Xi’an Jiaotong Univ. Med. Sci. 2021, 42, 123–127. [Google Scholar]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-Harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unit: Person, Household | |||
|---|---|---|---|
| Serial | Municipal District | Population | Total Households |
| 1 | Yingze | 547,718 | 161,954 |
| 2 | Xinghualing | 619,463 | 190,583 |
| 3 | Wanbailin | 592,184 | 177,510 |
| 4 | Jiancaoping | 333,077 | 113,440 |
| 5 | Jinyuan | 215,551 | 68,512 |
| 6 | Xiaodian | 694,166 | 206,339 |
| Total | 3,002,159 | 918,338 | |
| Serial | Hospital Name | Number of Medical and Nursing Staff | Number of Beds | Municipal District |
|---|---|---|---|---|
| 1 | First hospital of Shanxi Medical University | 3985 | 2419 | Yingze |
| 2 | Second hospital of Shanxi Medical University | 3800 | 2700 | Xinghualing |
| 3 | Fourth People’s Hospital of Taiyuan | 359 | 440 | Wanbailin |
| 4 | The Third People’s Hospital of Shanxi province | 616 | 850 | Yingze |
| 5 | Shanxi Norman Bethune Hospital | 2720 | 3533 | Xiaodian |
| 6 | Armed Police Hospital | 300 | 500 | Xiaodian |
| 7 | Shanxi provincial People’s Hospital | 2405 | 2000 | Yingze |
| 8 | Taiyuan Seventh People’s Hospital | 369 | 300 | Xinghualing |
| 9 | Taigang General Hospital | 2396 | 1800 | Jiancaoping |
| 10 | Children’s Hospital of Shanxi Province | 2943 | 1611 | Xinghualing |
| 11 | Taiyuan Central Hospital | 1500 | 1076 | Xiaodian |
| Total | 21,393 | 17,178 |
| Name of Parameter | Source of Initial Value | Description |
|---|---|---|
| Total population in Taiyuan Municipality | Taiyuan City Statistical Yearbook 2020 [27] | 300.2159 million people |
| Age composition of Taiyuan’s population | Data from the 7th Census of Taiyuan in 2020 | 0–14 years: 15.55%, 15–59 years: 68.34%, 60 years and over: 16.11% |
| Vaccination rate | Complete vaccination coverage in China as of 24 June 2022 | 89.37% |
| Case fatality rate (CFR) | Case fatality rate in China as of 24 June 2022 | 2.3% |
| Latency time | Clinical characteristics of 40 patients infected with the SARS-CoV-2 omicron variant in Korea [28] | 3.5 days |
| Mean time to healing | Report of the WHO–China Joint Mission on Coronavirus Disease 2019 (COVID-19) [29] | Approximately 2 weeks for mild cases, 3–6 weeks for severe and critical cases |
| Hospital admission response time | Average admission time to tertiary and above hospitals in Taiyuan | 2 to 3 days |
| Hospital beds | Total beds in Taiyuan’s tertiary and above hospitals | 17,178 |
| Number of medical and nursing staff | General medical staff of tertiary and above hospitals in Taiyuan | 2.1393 |
| Mean number of nucleic acid tests during isolation | Prevention and control program for novel coronavirus pneumonia (8th edition) [30] | 4 times |
| Average number of effective reproduction (Re) | The effective reproductive number for the Omicron variant of SARS-CoV-2 is several times relative to Omicron [31]. | 3.4 (0.88~9.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.; Pan, L.; Yan, H.; Zhang, G.; Zhang, R. Social Simulation Model of the Spread and Prevention of the Omicron SARS-CoV-2 Variant. Axioms 2022, 11, 660. https://doi.org/10.3390/axioms11120660
Su Y, Pan L, Yan H, Zhang G, Zhang R. Social Simulation Model of the Spread and Prevention of the Omicron SARS-CoV-2 Variant. Axioms. 2022; 11(12):660. https://doi.org/10.3390/axioms11120660
Chicago/Turabian StyleSu, Ya, Lihu Pan, Huimin Yan, Guoyou Zhang, and Rui Zhang. 2022. "Social Simulation Model of the Spread and Prevention of the Omicron SARS-CoV-2 Variant" Axioms 11, no. 12: 660. https://doi.org/10.3390/axioms11120660
APA StyleSu, Y., Pan, L., Yan, H., Zhang, G., & Zhang, R. (2022). Social Simulation Model of the Spread and Prevention of the Omicron SARS-CoV-2 Variant. Axioms, 11(12), 660. https://doi.org/10.3390/axioms11120660