Betel nut chewing is a prevalent habit among the Indian population which predisposes to the development of oral sub-mucus fibrosis (OSMF). OSMF is a premalignant condition resulting in progressive and irreversible trismus. Surgical management is indicated in severe cases [
1]. Oral cavity cancers in association with OSMF is a common clinical scenario. The idea of simultaneously treating the two has led to the adoption of cross-cheek flap design in free flap transfer [
1,
2]. Lee and coworker had previously described a cross-cheek anterolateral thigh flap (ALT) for simultaneous correction of trismus and oral cancer [
2]. The use of two small radial forearm free flaps (RFFF) has proved to be effective and reliable in the literature [
3]. We report, in two patients, a novel technique of a single dumbbell-shaped, cross-cheek RFFF to repair bilateral defects.
Case Reports
The dumbbell-shaped RFFF was used in two patients who underwent ablative surgery for oral cancer and severe trismus.
Case 1
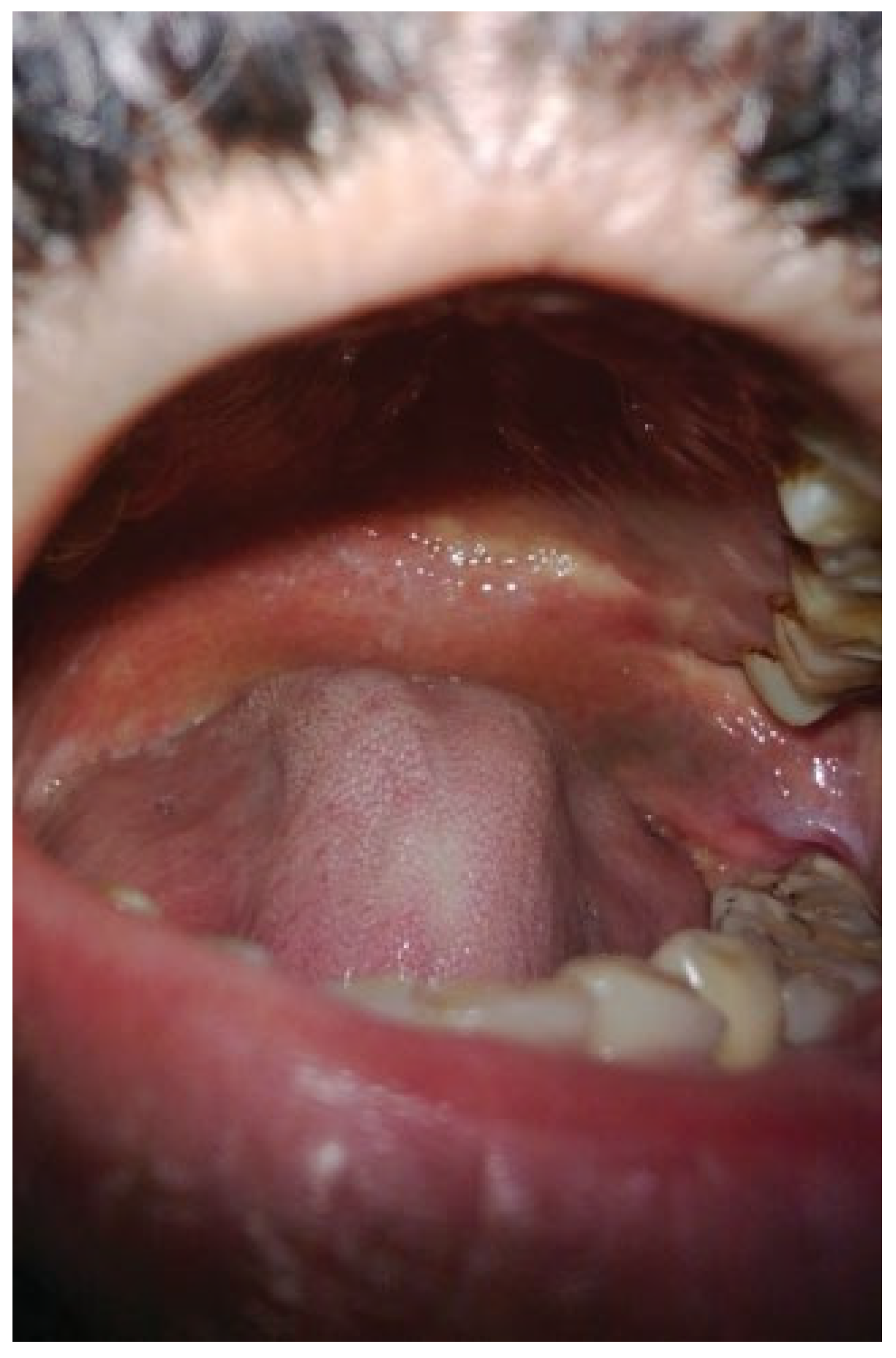
A 37-year-old male patient, chronic betel nut chewer, presented with right buccal mucosa carcinoma abutting the mandible with OSMF. His preoperative interincisor distance (IID) was 5 mm (
Figure 1). He underwent wide local excision with marginal mandibulectomy and bilateral trismus release with coronoidectomy. A dumbbell-shaped RFFF was used to cover this defect spanning across bilateral buccal mucosa and palate.
Case 2
A 47-year-old man, a habitual betel nut consumer, presented with recurrent carcinoma left buccal mucosa and chronic trismus with an IID of 2 mm. His left RFFF had been previously used during the first cancer surgery. Presently, he underwent wide local excision including marginal mandibulectomy and infrastructure maxillectomy and bilateral trismus release with coronoidectomy. A dumbbell-shaped RFFF was harvested from the right forearm and anastomosed to the contralateral facial vessels.
Surgical Anatomy of the Flap
The skin of the RFFF is supplied by 9 to 17 septocutaneous perforators of the radial artery, emerging in the lateral intermuscular septum between the brachioradialis and flexor carpi radialis. The distal skin is supplied by the numerous distal perforators, whereas the proximal skin receives perforators from the middle third of the forearm, which may be few in number [
4]. This may raise some doubt regarding the reliability of an independent proximal skin paddle. However, ink injection studies have revealed that vessels in the distal zone are capable of supplying a fasciocutaneous flap extending proximally up to the elbow, making this technique quite robust [
4].
Surgical Technique
The operation was performed by two teams simultaneously. Tumor was excised with adequate margins (
Figure 2) followed by the release of fibrotic tissue in the buccal mucosa on both sides and the soft palate. The palatal mucosa was further denuded to accommodate the bridging segment of the flap. Palpation of soft, pliable tissue at the resultant defect verified the complete release. A myotomy of fibrotic buccinator, temporalis, and masseter muscles followed by bilateral coronoidectomy was done. A dumbbell-shaped RFFF was marked according to the intraoral defect. The dimensions of the distal and proximal skin paddles were designed to match the corresponding bilateral buccal defects and intervening segment to the palate. The RFFF was raised in the conventional manner. The dumbbell-shaped flap covered the cancer resection defect on one side and the defect created by the OSMF release on the other side and the intervening divided soft palate mucosa (
Figure 3 and
Figure 4). The proximal skin covered the defect on the same side as of the recipient vessels. During inset, prolene sutures are drilled through the palatal bone to ensure snug attachment of the bridging segment. After careful inset and passage of the pedicle into the neck, anastomosis was performed. The donor site was skin grafted. Early initiation of jaw opening exercises in the postoperative period was encouraged. Absolute cessation of betel nut consumption was initiated.
Results
The intraoperative IID increased from 5 to 40 mm in the first patient and from 2 to 35 mm in the second. At 12-month follow-up, the IID was 38 and 30 mm, respectively, amounting to the average increment in IID of 30 or 3 cm (
Figure 5). Neither of the patients received adjuvant radiotherapy. There was no significant donor site morbidity. The first patient required third molar extraction postoperatively due to the bulky flap impinging on the tooth. The second patient was reexplored for venous thrombosis but was successfully salvaged. Both the patients had no significant speech problems and both could take regular diet.
Discussion
Trismus complicates oral cancer surgery and interferes with postoperative surveillance [
2]. Submucous fibrosis is the most common cause of trismus associated with oral cancer in the Indian subcontinent [
5]. There are reports of the use of double free flaps for treatment of OSMF [
1]. Wei et al. were the first to use two small RFFF for bilateral buccal mucosa defects [
3]. The drawback of this approach is the need for two microsurgeries which is more time consuming and technically demanding. Also, sacrifice of both the radial arteries with questionable limb ischemia and exhausting both the forearm donor sites and two sets of recipient vessels may be detrimental in cases of recurrence. Besides, this approach cannot be used in already vessel-depleted necks. Tsao et al. presented a technique of harvesting two independent RFFF from the same radial artery [
6]. This method of splitting a fasciocutaneous flap based on individual perforators still requires two anastomoses. Similarly, Chou et al. used two ALTs based on one descending branch of lateral femoral circumflex vessel [
7]. A tripaddled ALT flap with three independent sets of perforators was harvested by Jiang et al. [
8]. However, these flaps are highly perforator dependent and bulky.
The use of single RFFF for bilateral defects has been described earlier. This technique requires splitting of the lower gingivolabial sulcus to accommodate the bridging skin paddle, which causes the lower lip to prolapse and an unsightly appearance [
6]. Lee et al. modified this technique and used bipaddled RFFF using only one donor site [
9]. The bridging skin was skeletonized and the “bridge pedicle” was placed submucosally under the anterior vestibule. There is also a possibility of pedicle compression due to inadequate space, especially where OSMF may result in an already firm and shallow sulcus.
Other methods of resurfacing post–trismus release defects include split skin graft and local flaps [
1]. Reports in the literature have been disappointing owing to scar contracture and inadequacy in tissue supply, more so in coexistent cancer cases [
10]. Intraoral local flaps such as tongue flap, buccal fat, and palatal flaps are exposed to the same field change in OSMF. They are bulky and require additional divisional surgery. Bilateral tongue flaps can result in significant functional impairment in speech and swallowing [
9]. Extra-oral flaps such as nasolabial flap and submental flap are limited in their reach posteriorly with the additional morbidity of facial and neck scars [
9,
10].
The advantages of the RFFF for reconstructing such sizable defects are manifold. It has a constant vascular anatomy, thin and pliable skin, technical ease of harvest, and long pedicle. This dumbbell-shaped modification integrates three anatomically distinct sites into a single unit, which can be repaired with a solitary flap and one anastomosis. Hence, the other donor sites and vessels are spared as possible salvage portals.
This surgical technique has its drawbacks. The first and foremost is the donor site morbidity. With large amounts of forearm skin harvested, the donor site has to be almost always skin grafted. The issues of complete or partial graft loss and unacceptable appearance of the forearm are of definite concern. In recurrent or salvage situations with vessel depleted necks, pedicle length may appear to be insufficient. Rarely, excessive bulkiness of the flap may cause problems which can be solved by flap thinning or dental extraction at a subsequent stage. Finally, the mean increment of 3 cm in IID must be considered with caution, as both these cases had no adjuvant radiation which is known to affect the results adversely.
Conclusion
A single dumbbell-shaped RFFF is a useful option for reconstructing complex defects following trismus release and cancer resection. The dumbbell shape provided tissue for both the buccal mucosa defects and central released soft palate preventing fibrosis and reapproximation. This preserves one forearm donor site and one set of recipient vessels for further reconstruction, with acceptable donor site morbidity.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}