Abstract
Facial fracture patients are seen in a Level 1 trauma hospital. In our institution, we manage many patients with facial fractures and carry out more than 150 surgical procedures every year. Open reduction and internal fixation is our management of choice. All surgical procedures involve drilling of bone and implant insertion to keep the fractured bones in an anatomically reduced position to aid healing. Occasionally, drill bits used to create the pilot hole break and are embedded in the bone. We present a situation in which such an incident occurred and review the literature on retained broken implants and devices.
Patients with facial fractures are commonly treated in a Level 1 trauma hospital. In most of these cases, there will be bony union as long as the fragments are in contact with one another. The complexity of the fracture and the degree of displacement will contribute to the rate of nonunion, if there is no surgical reduction performed. However, the rate of nonunion and malunion remains low [1]. In our institution, we manage many patients with facial fractures and carry out more than 150 surgical procedures every year. Open reduction and internal fixation (ORIF) is our management of choice unless contraindications, for example, recent myocardial infarction, stroke, or bleeding tendencies preclude surgery. All surgical procedures involve drilling of bone and implant insertion to keep the fractured bones in an anatomically reduced position until healing is completed [2].
Occasionally, drill bits used to create the pilot hole break and are embedded in the bone. We present a situation in which such an incident occurred and review the literature on retained broken implants and devices.
Case Report
T.S., a 25-year-old man, was admitted after being involved in a road traffic accident. He had sustained multiple rib fractures, left scapula fracture, cervical spinal processes fracture, and a small subdural hemorrhage, in addition to the left-sided orbitozygomatic fracture. The zygomatic fragment was displaced and rotated medially (Knight and North type 4 fracture [3]). The patient underwent surgery for reduction and fixation of the fracture. During fixation, a 1.1-mm diameter, 6-mm length drill bit with stop (Matrix Midface, Depuy-Synthes, Paoli, Philadelphia, PA) broke and the distal tip was retained in the zygomatic body. The decision was made to leave the drill bit in situ. Fortunately, that was the second hole to be drill for that particular plate. Therefore, the plate needs to be only adjusted slightly (< 1 mm) medially, pivoting on the first partially inserted screw. The surgery was completed without any other difficulties. The patient recovered well and was discharged. A 1-year follow-up visit did not show any complications. T.S., however, is not our only case. Over the last 10-year period, there have been more than 10 such cases. All of whom did not have complications related to the retained dril bit/implant, on short- and long-term follow-up appointments. Table 1 summarizes the details of some of the above-mentioned cases. Figure 1 and Figure 2 represent a photograph and computed tomography scan image of a retained screw.

Table 1.
Summary of five cases.

Figure 1.
Retained broken screw within frontal bone.
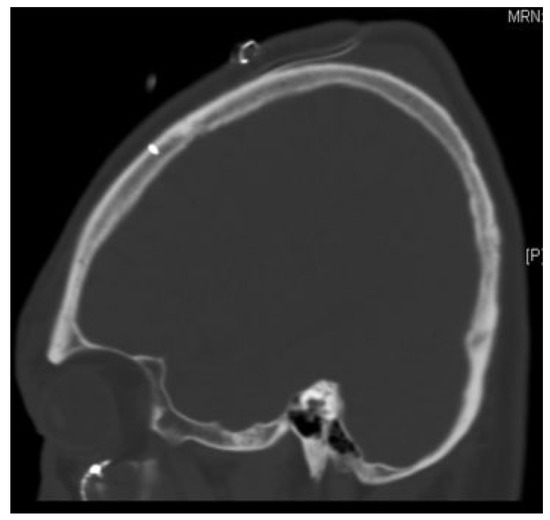
Figure 2.
Computed tomography scan image of Figure 1.
Discussion
A long-term review of our cases revealed many instances of retained broken implants. On follow-up, there were no reports of complications directly related to the broken implant.
A literature search was conducted on PubMed and Ovid for broken/retained drill bits or screws in facial fracture patients. To our knowledge, there is no publication on retained broken implants in the facial skeleton. The literature for broken drill bits and screws are either on animals, long bone fixation or spinal fixation [4,5]. In all of these publications, the most common type of broken implant is the broken drill bit.
Drilling bone is an essential part of ORIF, where a pilot hole is created to receive a fixation device such as a screw (threaded) or a wire (nonthreaded). It is done perpendicular to the bony surface. However, the natural geometry of bone, especially the facial skeleton, is irregular and curved. This makes it difficult to create a perpendicular drill hole and gives rise to higher rates of skiving, skimming, walking, and wandering of the drill bit just before purchase is achieved [6]. It is during this process the drill bit breaks due to torsional and/or canting forces. In addition, the probability of craniomaxillofacial surgery drill bits breaking is higher as their diameter is much smaller than those used for orthopedic surgery. The bit sizes are as small as 0.8 mm and up to 1.8 mm in diameter. Longer drill bits are more likely to fracture compared with shorter ones. The longer drill bits are used in deep cavity or bicortical bone drilling, where canting and torsional forces tend to be present, especially in inexperienced hands.
Another possible cause for drill bit fracture is wear and tear. The drill bits are made of stainless steel (316L), containing a mixture of iron (62.5%), chromium (17.6%), nickel (14.5%), molybdenum (2.8%), and smaller amounts of other metals [7]. This alloy is more rigid and strong compared with the titanium alloy and thus has less tendency to yield or bend. As a result, canting and/or torsional forces acting on it would more likely lead to surface damage [8]. These minute surface damage would contribute to the weakening of the integrity of the drill bit. This would accumulate during the surgery after each drilling episode and increase the probability of drill bit fracture.
It is documented that during the drilling process, there are multiple mechanical forces that are converted to thermal energy, for example, the shear deformation of bone, friction between bone chips and the drill bit, and friction between the cutting edge and underlying bone. These temperatures can go as high as above 100°C. There is a linear relationship between the significant wear to the cutting edge of the drill bit, especially after 600 drilled holes, and a rise in temperature of the surrounding bone, which can go up an additional 54.5°C [9]. In our hospital, the reuse of drill bits is practiced. This practice is both US Food Drug Administration approved and Depuy-Synthes sanctioned as long as standards or the original manufacturer is maintained [10]. The process of sterilizing these drill bits, at temperatures of 121 or 135°C, and the repeated usage will cause further wear and tear to the implant, leaving it vulnerable to fracture during the subsequent usage. In addition, the drill bits become more corrosive over time.
The second most common broken implant during ORIF is the screw. Screws used in facial fracture fixation are small and in the diameter of 1.0 to 2.0 mm. Similar to the drill bit, canting and torsional forces act on the screw, particularly between the head and shaft of the screw. This can lead to screw head fracture during insertion of the screw. In addition, the use of the wrong drill bit size, that is, a smaller one, can lead to excessive force placed on the screw during the insertion process. These shear forces cause defacement of the screw head or fracture of the screw, especially if it is a non-self-tapping screw. Finally, doing everything the right way may still lead to difficulty in insertion of the screw. The bone chips can get impacted between the pilot hole wall and the screw flutes. More force will be required to insert the screw, increasing the risk of screw fracture. One way to circumvent this is to reverse the insertion process two to three revolutions when there is resistance in putting in the screw, and then continue the insertion. This would loosen the impacted bone chips and allow for easier insertion of the screw.
All implants used in our hospital are made of 99.99% pure titanium by Depuy-Synthes. These are inert and do not cause adverse reactions in patients [11]. The titanium forms a protective oxide, which improves tissue biocompatibility and osseointegration. However, its tribocorrosion rate is higher on its own. Tribocorrosion is the degradation process due to a combination of wear and corrosion. Therefore, it is made in combination with other materials such as aluminum and niobium and other trace elements (Ti6AL7Nb) [12]. The drill bits are made of grade 316L austenitic stainless steel. The molybdenum it contains gives it a better overall corrosive resistant property and stiffness.
The next question that arises is what will happen if the implants were retained?
The main issue about leaving in situ broken drill bits is if part of it is sticking out of the bone, that is, not flush with the bone surface. This will undoubtedly cause more harm especially erosion through the skin. In addition to that, the attempted drilled hole was strategically made for placement of the plate. In cases of simple, noncomminuted fractures, slightly relocating the plate by 1 to 2 mm can rectify this problem. However, in comminuted fracture, one may only have “one bite of the cherry.” Attempting to remove the bit from a small bony fragment will more than likely cause it to further comminute or at the very least create a larger hole diameter preventing good purchase of the screw. These would be similar complications if the screw were to break.
The stainless steel drill bit, despite having molybdenum in its alloy, may undergo corrosion and induce an inflammatory response or foreign body reaction. The titanium alloy has a higher tribocorrosion resistance. However, Depuy-Synthes, the maker of the implants and drill bits, cautions against mixed metals in vivo [13]. These metals, each with its own corrosion potential, can react together and produce conduction currents if they are in contact in an electrochemically conductive fluid, like bodily fluid. In turn, this can lead to accelerated corrosion of both metals, reduce their individual strengths, and stimulate an inflammatory or hypersensitivity response. However, both can be present in the bone or soft tissue as long as both are not in direct contact with each other.
The potential complications do not stop with electrochemical reactions only. If the two implants are in contact with one another, micromotion can increase wear to the implants. This can lead to the release of metal ions into the surrounding area. Due to enlarged particle size, macrophages may not be able to ingest and remove them. The presence of these ions can stimulate an inflammatory reaction, which may not only result in osteolysis but also inhibition of bone formation [14,15].
The most common reasons for the removal of implant are palpability, erosion, pain, and thermal sensitivity [16]. In the case of broken implants, the recommendation was to remove it if it was in a joint or in a position which made removal easy [17]. The presence of infection would of course mandate the removal of the implants. Facial fracture fixation often involves piecing together many small fragments of bone. Any attempt at removing a retained broken drill bit or screw shaft would undoubtedly lead to further breaking up of the small fragment of bone, in an already comminuted fracture. Our practice is to not retrieve broken parts that are embedded in bone.
To our knowledge, we do not have complications after facial fracture fixation as a result of broken implants. It is our recommendation that broken implants, including drill bits, should be left in situ as long as it is not overtly protruding off the surface or left in a joint.
References
- Klotch, D.W.; Gilliland, R. Internal fixation vs. conventional therapy in midface fractures. J Trauma 1987, 27, 1136–1145. [Google Scholar] [PubMed]
- Gilardino, M.S.; Chen, E.; Bartlett, S.P. Choice of internal rigid fixation materials in the treatment of facial fractures. Craniomaxillofac Trauma Reconstr 2009, 2, 49–60. [Google Scholar] [PubMed]
- Knight, J.S.; North, J.F. The classification of malar fractures: an analysis of displacement as a guide to treatment. Br J Plast Surg 1961, 13, 325–339. [Google Scholar] [CrossRef] [PubMed]
- Fothi, U.; Perren, S.M.; Auer, J.A. Drill bit failure with implant involvement—an intraoperative complication in orthopaedic surgery. Injury 1992, 23 (Suppl 2), S17–S29. [Google Scholar] [CrossRef] [PubMed]
- Price, M.V.; Molloy, S.; Solan, M.C.; Sutton, A.; Ricketts, D.M. The rate of instrument breakage during orthopaedic procedures. Int Orthop 2002, 26, 185–187. [Google Scholar] [PubMed]
- Bertollo, N.; Walsh, W.R. Drilling of bone: practicality, limitations and complications associated with surgical drill-bits. In Biomechanics in Applications; Klika, V., Ed.; 2011; Chapter 3; pp. 53–82. Available online: http://www.intechopen.com/books/biomechanics-in-applications/drilling-of-bone-practicality-limitations-and-complications-associated-with-surgical-drill-bits (accessed on 26 February 2014).
- Navarro, M.; Michiardi, A.; Castaño, O.; Planell, J.A. Biomaterials in orthopaedics. J R Soc Interface 2008, 5, 1137–1158. [Google Scholar] [PubMed]
- Steinemann, S. Metal for craniomaxillofacial internal fixation implants and its physiologic implications. In Craniomaxillofacial Reconstructive and Corrective Bone Surgery; Greenberg, A., Prein, J., Eds.; Springer: New York, NY, USA, 2006; pp. 107–12. [Google Scholar]
- Jochum, R.M.; Reichart, P.A. Influence of multiple use of Timedur-titanium cannon drills: thermal response and scanning electron microscopic findings. Clin Oral Implants Res 2000, 11, 139–143. [Google Scholar] [PubMed]
- Available online: http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/ucm073758.htm (accessed on 26 February 2014).
- Steinmann, S.G.; Eulenberger, J.; Mausli, P.A.; Schroeder, A. Biological and Biomechanical Performance of Biomaterials; Elsevier Science: Amsterdam, 1986. [Google Scholar]
- Plecko, M.; Sievert, C.; Andermatt, D.; et al. Osseointegration and biocompatibility of different metal implants—a comparative experimental investigation in sheep. BMC Musculoskelet Disord 2012, 13, 32. [Google Scholar]
- Available online: http://sites.synthes.com/intl/vet/support_contact/faq/Pages/faq.aspx (accessed on 26 February 2014).
- Olmedo, D.; Fernández, M.M.; Guglielmotti, M.B.; Cabrini, R.L. Macrophages related to dental implant failure. Implant Dent 2003, 12, 75–80. [Google Scholar] [PubMed]
- Adya, N.; Alam, M.; Ravindranath, T.; Mubeen, A.; Saluja, B. Corrosion in titanium dental implants: literature review. J Indian Prosthodont Soc 2005, 5, 126–131. [Google Scholar]
- Orringer, J.S.; Barcelona, V.; Buchman, S.R. Reasons for removal of rigid internal fixation devices in craniofacial surgery. J Craniofac Surg 1998, 9, 40–44. [Google Scholar] [PubMed]
- Hirt, U.; Auer, J.A.; Perren, S.M. Drill bit failure without implant involvement—an intraoperative complication in orthopaedic surgery. Injury 1992, 23 (Suppl 2), S5–S16. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the author. The Author(s) 2014.