The Comprehensive AOCMF Classification: Skull Base and Cranial Vault Fractures—Level 2 and 3 Tutorial
Abstract
:Level 2 and Level 3 Classification System for Skull Base and Cranial Vault Fractures
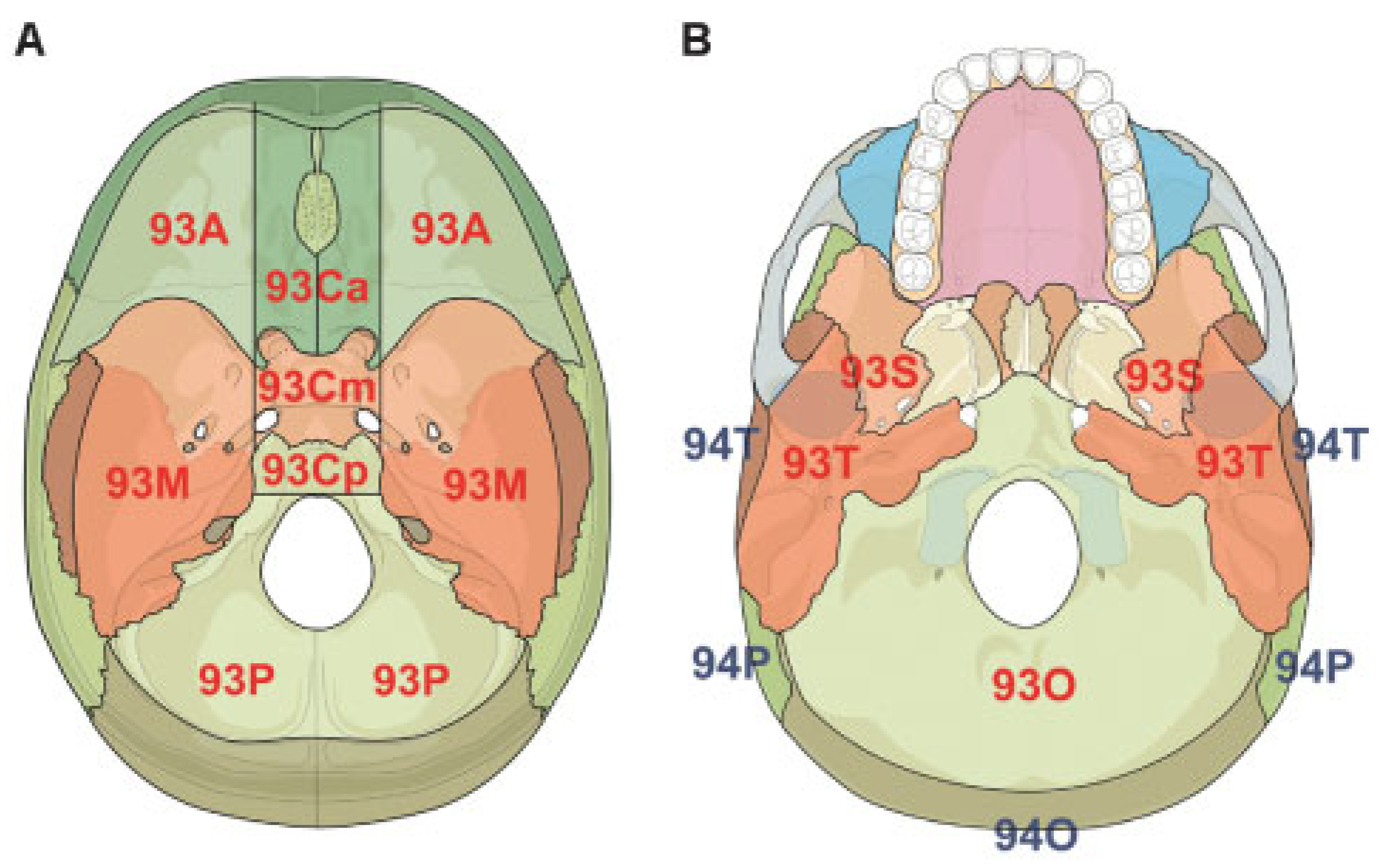
Level 2 System for Fracture Location
Level 3 System for Fracture Morphology
- 1 = Nonfragmented (single fracture line [linear and branched], ignoring small fracture cracks), or
- 2 = Fragmented
- 0 = Nondisplaced
- 1 = Displaced but not depressed
- 2 = Depressed (when the broken bones are displaced inward toward the meninges and brain for more than 3 mm)
Associated Intracranial Features
Fracture Coding and Topographical Distribution
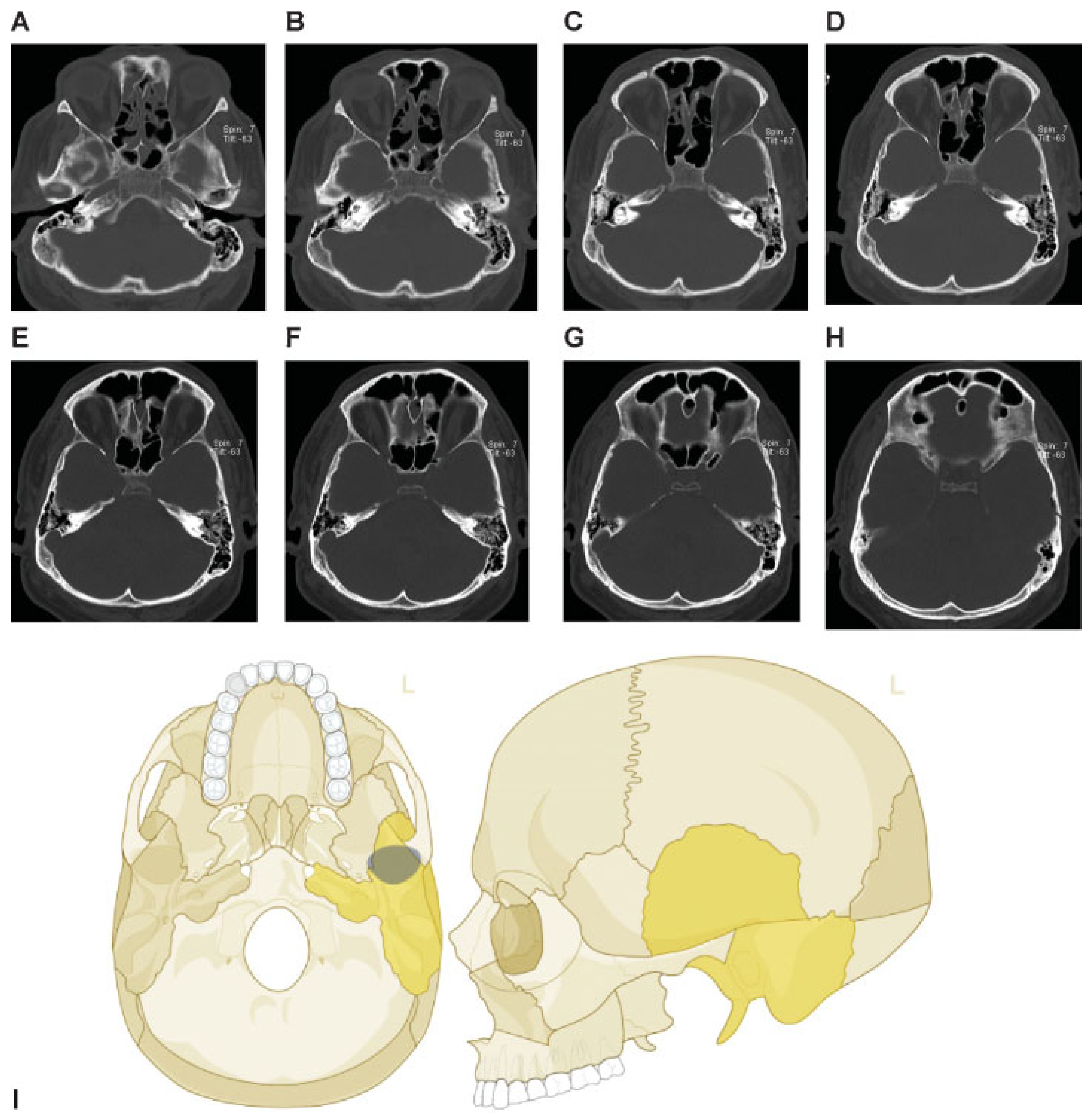
Case Examples
Discussion
Conclusion
Acknowledgments
References
- Audigé, L.; Cornelius, C.P.; Di Ieva, A.; Prein, J. CMF Classification Group. The first AO classification system for fractures of the craniomaxillofaxial skeleton: rationale, methodological background, developmental process and objectives. Craniomaxillofac Trauma Reconstr 2014, 7 (Suppl 1), S6–S14. [Google Scholar]
- Cornelius, C.P.; Audigé, L.; Kunz, C.; et al. The comprehensive AOCMF classification system: mandible fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr 2014, 7 (Suppl 1), S15–S30. [Google Scholar] [CrossRef] [PubMed]
- Masson, F.; Vecsey, J.; Salmi, L.R.; et al. Disability and handicap 5 years after a head injury: a population-based study. J Clin Epidemiol 1997, 50, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Annegers, J.F.; Grabow, J.D.; Kurland, L.T.; Laws, E.R., Jr. The incidence, causes, and secular trends of head trauma in Olmsted County, Minnesota, 1935-1974. Neurology 1980, 30, 912–919. [Google Scholar] [CrossRef] [PubMed]
- Kraus, J.F.; Black, M.A.; Hessol, N.; et al. The incidence of acute brain injury and serious impairment in a defined population. Am J Epidemiol 1984, 119, 186–201. [Google Scholar] [CrossRef] [PubMed]
- Samii, M.; Tatagiba, M. Skull base trauma: diagnosis and management. Neurol Res 2002, 24, 147–156. [Google Scholar] [CrossRef] [PubMed]
- de Boussard, C.N.; Bellocco, R.; af Geijerstam, J.L.; et al. Delayed intracranial complications after concussion. J Trauma 2006, 61, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Di Ieva, A.; Gaetani, P.; Matula, C.; et al. Berengario da Carpi: a pioneer in neurotraumatology. J Neurosurg 2011, 114, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Le Fort, R. Étude expérimentale sur les fractures de la machoire supérieure (Part l). Rev Chir 1901, 23, 208–227. [Google Scholar]
- Le Fort, R. Étude expérimentale sur les fractures de la machoire supérieure (Part II). Rev Chir 1901, 23, 360–379. [Google Scholar]
- Le Fort, R. Étude expérimentale sur les fractures de la machoire supérieure (Part lll). Rev Chir 1901, 23, 479–507. [Google Scholar]
- Sakas, D.E.; Beale, D.J.; Ameen, A.A.; et al. Compound anterior cranial base fractures: classification using computerized tomography scanning as a basis for selection of patients for dural repair. J Neurosurg 1998, 88, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Sherif, C.; Di Ieva, A.; Gibson, D. A management algorithm for cerebrospinal fluid leak associated with anterior skull base fractures: detailed clinical and radiological follow-up. Neurosurg Rev 2012, 35, 227–237, discussion 237–238. [Google Scholar] [CrossRef] [PubMed]
- Madhusudan, G.; Sharma, R.K.; Khandelwal, N.; Tewari, M.K. Nomenclature of frontobasal trauma: a new clinicoradiographic classification. Plast Reconstr Surg 2006, 117, 2382–2388. [Google Scholar] [CrossRef] [PubMed]
- Buitrago-Téllez, C.H.; Schilli, W.; Bohnert, M.; et al. A comprehensive classification of craniofacial fractures: postmortem and clinical studies with twoand three-dimensional computed tomography. Injury 2002, 33, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Bächli, H.; Leiggener, C.; Gawelin, P.; et al. Skull base and maxillofacial fractures: two centre study with correlation of clinical findings with a comprehensive craniofacial classification system. J Craniomaxillofac Surg 2009, 37, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Manson, P.N.; Stanwix, M.G.; Yaremchuk, M.J.; et al. Frontobasal fractures: anatomical classification and clinical significance. Plast Reconstr Surg 2009, 124, 2096–2106. [Google Scholar] [CrossRef] [PubMed]
- Kunz, C.; Cornelius, C.P.; Prein, J.; et al. The comprehensive AOCMF classification system: midface fractures - level 2 tutorial. Craniomaxillofac Trauma Reconstr 2014, 7 (Suppl 1), S59–S67. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code | Subdivisions | Level 3 items | Categories |
|---|---|---|---|
| All | Fracture line(s) | 1 = Single fracture line (ignoring associated cracks) | |
| 2 = Multiple fracture lines | |||
| Displacement | 0 = Nondisplaced | ||
| 1 = Displaced but not depressed | |||
| 2 = Depressed (displaced toward the brain) | |||
| 93A | Anterior SB | ||
| Frontal sinus | Fracture | 0 = No; 1 = Yes | |
| Opacification | 0 = No; 1 = Yes | ||
| 93M | Middle SB | ||
| Ethmoid sinus | Fracture | 0 = No; 1 = Yes | |
| Opacification | 0 = No; 1 = Yes | ||
| 93Ca | Central anterior SB | ||
| Cribriform | Fracture | 0 = No; 1 = Yes | |
| 93Cm | Central middle SB | ||
| Sphenoid sinus | Fracture | 0 = No; 1 = Yes | |
| Opacification | 0 = No; 1 = Yes | ||
| 93O | Occipital bone | ||
| Occipital condylar process | Fracture | 0 = No; 1 = Yes | |
| 94F | Frontal bone | ||
| Frontal sinus | Fracture | 0 = No; 1 = Yes | |
| Opacification | 0 = No; 1 = Yes | ||
| 93S | Sphenoid bone | ||
| 93T | Temporal bone | ||
| Glenoid fossaa | Fracture | 0 = No; 1 = Yes |
| Item groups | Items | Categories |
|---|---|---|
| Intracranial air a | 0 = None | |
| 1 = Bubbles (up to 3 mm diameter) | ||
| 2 = Pneumocephalus (>3 mm diameter) | ||
| Intracranial mass lesion | Epidural hematoma | 0 = No; 1 = Yes |
| Subdural hematoma | 0 = No; 1 = Yes | |
| Intracerebral hematoma | 0 = No; 1 = Yes | |
| Traumatic SAH | 0 = No; 1 = Yes | |
| Intraventricular | 0 = No; 1 = Yes | |
| Contusion | 0 = No; 1 = Yes | |
| Foreign bodies | 0 = No; 1 = Yes | |
| Cranial nerve involvement | Nerve 1 | 0 = No; 1 = Yes |
| Nerve 2 | 0 = No; 1 = Yes | |
| Nerve 3 | 0 = No; 1 = Yes | |
| Nerve 4 | 0 = No; 1 = Yes | |
| Nerve 5 | 0 = No; 1 = Yes | |
| Nerve 6 | 0 = No; 1 = Yes | |
| Nerve 7 | 0 = No; 1 = Yes | |
| Nerve 8 | 0 = No; 1 = Yes | |
| Nerve 9 | 0 = No; 1 = Yes | |
| Nerve 10 | 0 = No; 1 = Yes | |
| Nerve 11 | 0 = No; 1 = Yes | |
| Nerve 12 | 0 = No; 1 = Yes | |
| Vascular structure involvement | Traumatic aneurysm | 0 = No; 1 = Yes |
| Traumatic CCF | 0 = No; 1 = Yes | |
| Traumatic occlusion | 0 = No; 1 = Yes | |
| Venous sinuses | Transverse sinus | 0 = No; 1 = Yes |
| Sigmoid sinus | 0 = No; 1 = Yes | |
| Superior sagittal sinusa | 0 = No; 1 = Yes | |
| Confluence sinusa | 0 = No; 1 = Yes | |
| Cerebrospinal fluid leak | ||
| Previous | Rhinorrhea | 0 = No; 1 = Yes |
| Otorrhea | 0 = No; 1 = Yes | |
| Other location | 0 = No; 1 = Yes | |
| Active | Rhinorrhea | 0 = No; 1 = Yes |
| Otorrhea | 0 = No; 1 = Yes | |
| Other location | 0 = No; 1 = Yes | |
© 2014 by the author. The Author(s) 2014.
Share and Cite
Di Ieva, A.; Audigé, L.; Kellman, R.M.; Shumrick, K.A.; Ringl, H.; Prein, J.; Matula, C. The Comprehensive AOCMF Classification: Skull Base and Cranial Vault Fractures—Level 2 and 3 Tutorial. Craniomaxillofac. Trauma Reconstr. 2014, 7, 103-113. https://doi.org/10.1055/s-0034-1389563
Di Ieva A, Audigé L, Kellman RM, Shumrick KA, Ringl H, Prein J, Matula C. The Comprehensive AOCMF Classification: Skull Base and Cranial Vault Fractures—Level 2 and 3 Tutorial. Craniomaxillofacial Trauma & Reconstruction. 2014; 7(s1):103-113. https://doi.org/10.1055/s-0034-1389563
Chicago/Turabian StyleDi Ieva, Antonio, Laurent Audigé, Robert M. Kellman, Kevin A. Shumrick, Helmut Ringl, Joachim Prein, and Christian Matula. 2014. "The Comprehensive AOCMF Classification: Skull Base and Cranial Vault Fractures—Level 2 and 3 Tutorial" Craniomaxillofacial Trauma & Reconstruction 7, no. s1: 103-113. https://doi.org/10.1055/s-0034-1389563
APA StyleDi Ieva, A., Audigé, L., Kellman, R. M., Shumrick, K. A., Ringl, H., Prein, J., & Matula, C. (2014). The Comprehensive AOCMF Classification: Skull Base and Cranial Vault Fractures—Level 2 and 3 Tutorial. Craniomaxillofacial Trauma & Reconstruction, 7(s1), 103-113. https://doi.org/10.1055/s-0034-1389563